Phys · gastrointestinal
Acute Pancreatitis
Also known as acute pancreatitis · haemorrhagic pancreatitis · necrotising pancreatitis · gallstone pancreatitis · alcoholic pancreatitis · interstitial oedematous pancreatitis · walled-off necrosis · pseudocyst · autoimmune pancreatitis
Consultant-physician-depth guide to acute pancreatitis — premature intracellular trypsin activation and the I GET SMASHED aetiology, classic epigastric pain radiating to the back, lipase above 3x ULN as the diagnostic anchor, the Revised Atlanta Classification severity tiers, BISAP and Ranson scoring, goal-directed fluid resuscitation after the WATERFALL trial, early enteral feeding within 24 to 48 hours, ERCP for cholangitis only, the step-up approach for infected necrosis after PANTER, and same-admission cholecystectomy for gallstone pancreatitis. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Acute Pancreatitis

The answer first
Acute pancreatitis is an acute inflammatory process of the pancreas caused by premature intracellular activation of digestive enzymes — principally trypsin — within pancreatic acinar cells, leading to autodigestion of the gland and a variable systemic inflammatory response. It is diagnosed when two of three criteria are met: characteristic epigastric pain radiating to the back, serum lipase or amylase more than three times the upper limit of normal, and characteristic imaging findings [2].
The two dominant causes are gallstones (40 to 50 per cent) and alcohol (25 to 35 per cent), together accounting for 75 to 80 per cent of all cases. Mortality ranges from 1 per cent in mild disease to 30 per cent in infected necrotising pancreatitis. The single most important paradigm shift in the last decade is the move away from uncontrolled aggressive fluid resuscitation (the WATERFALL trial showed harm) and the abandonment of prolonged bowel rest in favour of early enteral feeding [3] [2].
DCE trap: The biggest pivot in modern pancreatitis management is that the old dogmas have been overturned: prophylactic antibiotics do not help, aggressive fluids cause harm, NPO is wrong, and open necrosectomy is a last resort. In every long case, state the severity using the Revised Atlanta Classification, give the goal-directed fluid plan, state the nutrition plan (early oral feeding), and justify your decisions with the trial evidence. [1]
Pathophysiology — why premature trypsin activation matters clinically
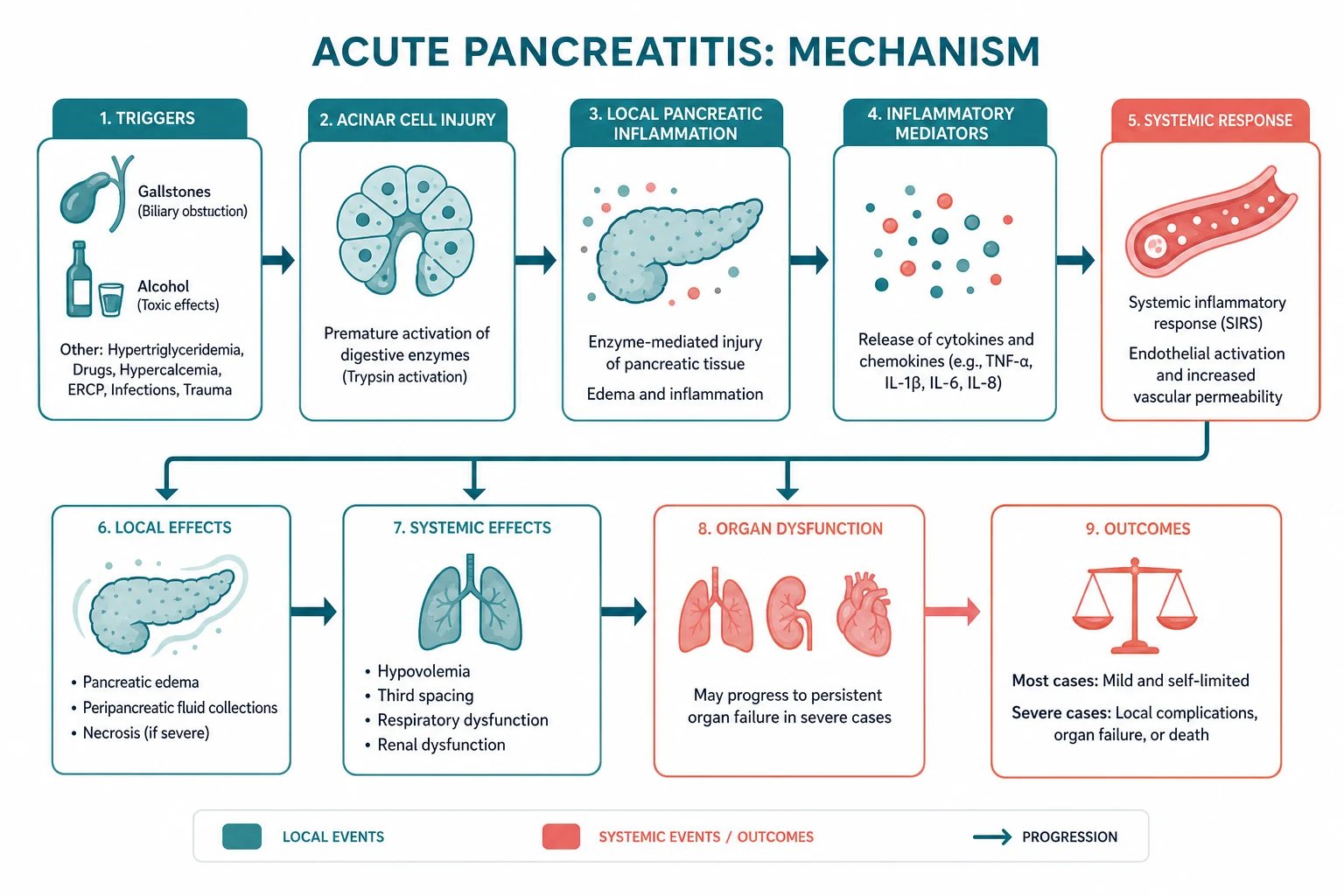
The pancreas synthesises digestive enzymes as inactive zymogens (trypsinogen, chymotrypsinogen, proelastase, prophospholipase, procarboxypeptidase). These are normally activated only after reaching the duodenal lumen, where enteropeptidase on the brush border converts trypsinogen to trypsin, which then activates the other zymogens. This compartmentalisation — zymogen granules, trypsinogen activation only in the duodenum, and intracellular trypsin inhibitor (serine protease inhibitor Kazal type 1, SPINK1) — is the central protective mechanism. [1]
In acute pancreatitis, this compartmentalisation fails. Trypsinogen is prematurely activated to trypsin within the pancreatic acinar cell. Once trypsin is intracellularly active, it activates the entire enzyme cascade: phospholipase A2 damages cell membranes, elastase destroys vascular walls (causing haemorrhage), and lipase causes fat necrosis. Autodigestion follows. The process also activates the complement and kinin cascades, producing the systemic inflammatory response syndrome (SIRS) that drives distant organ failure [1].
The two dominant mechanisms by which this premature activation occurs: [1]
-
Gallstones and biliary obstruction — a gallstone (or microlithiasis or biliary sludge) transiently obstructs the ampulla of Vater. The shared channel theory holds that obstruction raises intraductal pressure, forcing bile or pancreatic juice into the pancreatic duct, or simply obstructing pancreatic outflow so that enzymes accumulate and activate intracellularly. The mechanism is transient — most gallstones pass spontaneously into the duodenum within hours to days. [1]
-
Alcohol — ethanol causes direct toxic injury to acinar cells, alters intracellular signalling (sensitising cells to cholecystokinin), increases digestive enzyme content relative to protective enzymes, and forms protein plugs in small pancreatic ducts. Alcohol is also a cofactor for hypertriglyceridaemia. Chronic alcohol exposure causes recurrent acute attacks that may progress to chronic pancreatitis. [1]
The less common but exam-favoured mechanisms: [1]
-
Hypertriglyceridaemia — when serum triglycerides exceed 11 mmol per litre (approximately 1000 mg per dL), pancreatic lipase hydrolyses triglycerides to free fatty acids that are directly toxic to the pancreatic vascular endothelium and acinar cells, triggering inflammation. This is the mechanism in familial chylomicronaemia, poorly controlled diabetes, alcohol excess, and oestrogen or retinoic acid therapy. The serum is lactescent (milky), and pseudohyponatraemia may occur because the large lipid fraction displaces the aqueous phase. [1]
-
ERCP — endoscopic instrumentation of the ampulla causes mechanical, hydrostatic, or chemical injury to the pancreatic duct. Post-ERCP pancreatitis occurs in 3 to 10 per cent of procedures, usually within 24 hours. [1]
-
Autoimmune — type 1 autoimmune pancreatitis (IgG4-related disease) causes lymphoplasmacytic inflammation and fibrosis of the pancreas. Unlike other forms, it may present as painless jaundice or a pancreatic mass rather than classical acute pain. [1]
DWE high-yield mechanism question: "Why does hypertriglyceridaemia cause pancreatitis but hypercholesterolaemia does not?" Answer: Pancreatic lipase hydrolyses triglycerides (not cholesterol) to free fatty acids. The free fatty acids are unbound and directly toxic to the vascular endothelium and acinar cell membranes, triggering inflammation and microvascular thrombosis. Cholesterol is not a lipase substrate and does not generate toxic free fatty acids. [1]
Causes — the I GET SMASHED mnemonic

The mnemonic I GET SMASHED captures the full aetiological list. Commit the relative frequencies. [1]
| Letter | Cause | Key facts for the exam |
|---|---|---|
| I | Idiopathic | 10 to 20 per cent. Consider occult microlithiasis, sphincter of Oddi dysfunction, autoimmune, or genetic (PRSS1, SPINK1 mutations). Repeat the biliary imaging (EUS, MRCP) after recovery. |
| G | Gallstones | Most common cause — 40 to 50 per cent. Consider when ALT is elevated (above 150 IU per L has a positive predictive value of 95 per cent for gallstone pancreatitis), female, over 50, or with a sonographic stone. |
| E | Ethanol | Second most common — 25 to 35 per cent. Male predominance, chronic heavy intake. Risk of progression to chronic pancreatitis. |
| T | Trauma | Blunt abdominal trauma causing duct injury. Consider when amylase is elevated after a seatbelt injury or handlebar injury. |
| S | Steroids | Glucocorticoids are a recognised drug cause. Also consider autoimmune diseases treated with steroids as the underlying cause. |
| M | Mumps and Mycoplasma | Viral and atypical infectious causes. Also Coxsackie, CMV, HSV, HIV, and VZV. |
| A | Autoimmune | Type 1 (IgG4-related) and Type 2 (idiopathic duct-centric). See the dedicated section below. |
| S | Scorpion sting | Tityus trinitatis envenomation is the classic exam favourite. Exotic cause included for completeness. |
| H | Hypertriglyceridaemia and Hypercalcaemia | Triglycerides above 11 mmol per litre (type I, IV, V hyperlipidaemia). Hypercalcaemia (usually above 12 mmol per litre or from hyperparathyroidism). |
| E | ERCP and Endoscopic | Post-ERCP pancreatitis in 3 to 10 per cent of procedures. Prevent with rectal NSAIDs and prophylactic pancreatic stent in high-risk patients. |
| D | Drugs | Azathioprine, 6-mercaptopurine, mesalazine, didanosine, sulphonamides, thiazides, valproate, oestrogens, tetracyclines, L-asparaginase. |
DWE trap: The two most tested drug causes are azathioprine and mesalazine (IBD patients), followed by thiazides. When an IBD patient on azathioprine presents with epigastric pain and elevated lipase, stop the drug. When a hypertensive patient on a thiazide presents with pancreatitis, switch the antihypertensive. [1]
Clinical presentation
The classic triad is severe constant epigastric pain radiating to the back, vomiting that does not relieve the pain, and low-grade fever. The pain is typically relieved by sitting forward (the pancreatic retroperitoneal position is decompressed in the flexed position). [1]
Physical signs
Most patients have only mild epigastric tenderness and guarding. The paucity of abdominal signs relative to the severity of the pain is a hallmark: the inflammation is retroperitoneal, so the peritoneal surface is largely spared. Abdominal distension from paralytic ileus is common in severe disease. [1]
The two eponymous periumbilical signs indicate haemorrhagic necrotising pancreatitis — blood tracking along fascial planes from the retroperitoneum: [1]
- Cullen sign — periumbilical bluish discolouration. Blood tracks from the retroperitoneum via the falciform ligament to the periumbilical region.
- Grey Turner sign — flank discolouration. Blood tracks from the retroperitoneum to the flanks. [1]
Both are rare (under 3 per cent of cases) but, when present, indicate severe haemorrhagic disease with high mortality. They are not pathognomonic — Cullen sign also occurs in ruptured ectopic pregnancy and haemorrhagic ascites. [1]
Severity clues at the bedside
Signs that the disease is severe or progressing to organ failure:
- Tachycardia, hypotension, and cool peripheries (third-space fluid loss, SIRS)
- Tachypnoea and hypoxia (early acute respiratory distress syndrome or pleural effusion)
- Oliguria (prerenal acute kidney injury from hypovolaemia and SIRS)
- Confusion (hypoxia, electrolyte disturbance, SIRS encephalopathy)
- A rigid or silent abdomen (peritonitis from necrosis or perforation) [1]
Diagnosis — the two of three rule
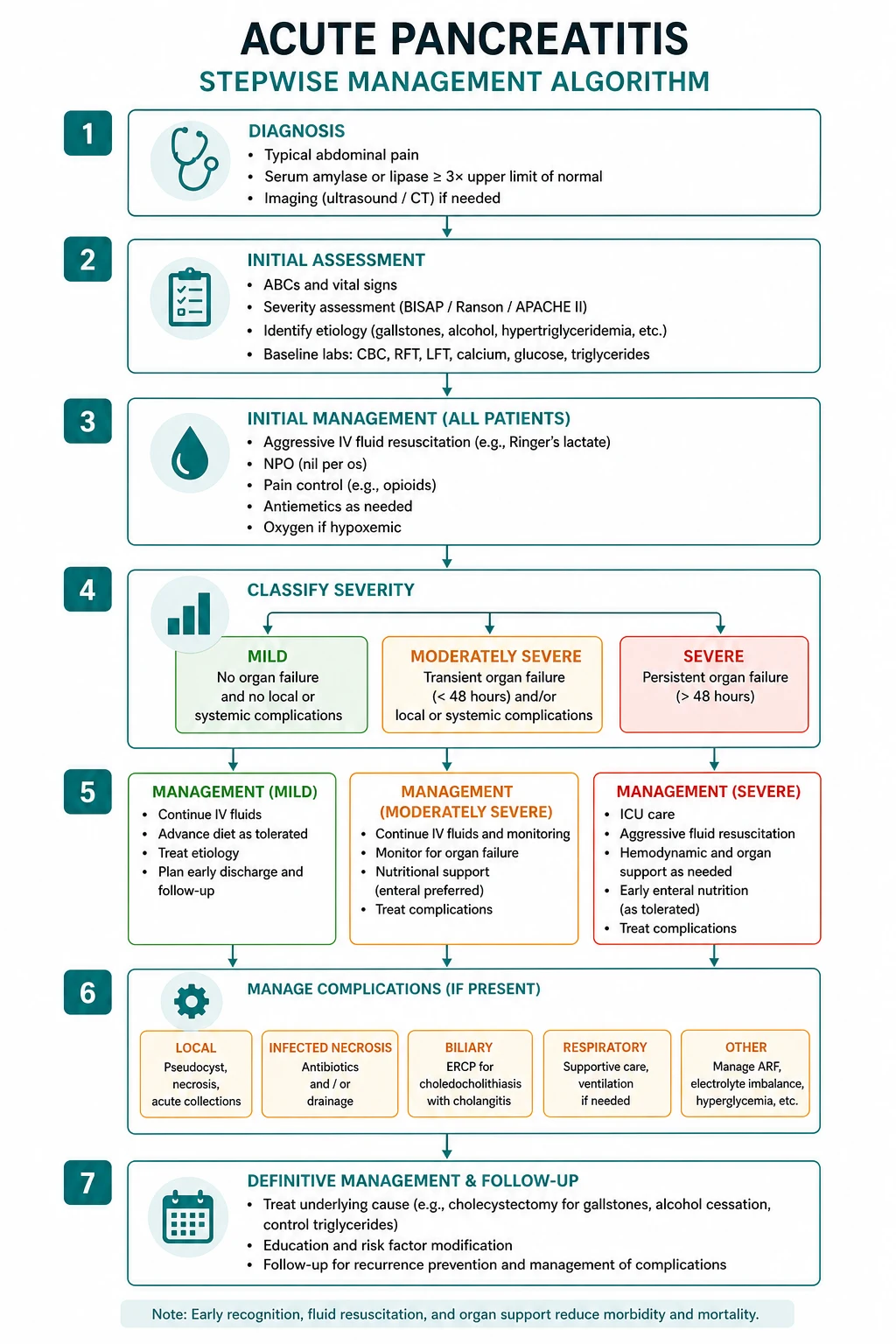
Diagnosis requires two of three [2]:
- Characteristic abdominal pain — acute onset of severe, persistent epigastric pain, often radiating to the back.
- Serum lipase (or amylase) more than three times the upper limit of normal.
- Characteristic imaging findings on contrast-enhanced CT, MRI, or transabdominal ultrasound. Imaging is not required for diagnosis when the first two criteria are met. [1]
Why lipase over amylase
Serum lipase is the preferred enzyme for three reasons: it has a longer half-life (remains elevated for days, whereas amylase normalises within 24 to 72 hours), it is more sensitive (raised in 90 to 100 per cent of cases versus 80 to 85 per cent for amylase), and it is more specific (amylase is also raised in salivary gland disease, tubo-ovarian disease, intestinal ischaemia, and diabetic ketoacidosis). Lipase above three times the upper limit of normal is the diagnostic threshold. [1]
Lipase may be falsely normal in hypertriglyceridaemia (the lactescent serum interferes with the assay) — in this situation, dilute the serum and re-test, or use clinical and imaging criteria. [1]
DWE trap: A normal or only mildly elevated amylase does NOT exclude pancreatitis. Amylase normalises within 24 to 72 hours. If the patient presents late, the lipase is more reliable. Conversely, a lipase less than three times the upper limit of normal with a compatible story is still consistent with pancreatitis if the imaging is characteristic — the diagnosis is two of three, not all three. [1]
Severity assessment — scoring systems and the Revised Atlanta Classification

Severity assessment drives the level of care, the intensity of monitoring, and the threshold for imaging and intervention. The Revised Atlanta Classification is the current international standard for severity, supplemented by the BISAP score for early bedside risk stratification [1] [6].
Revised Atlanta Classification (2012) — three severity tiers
| Severity | Definition | Organ failure | Local or systemic complications | Mortality |
|---|---|---|---|---|
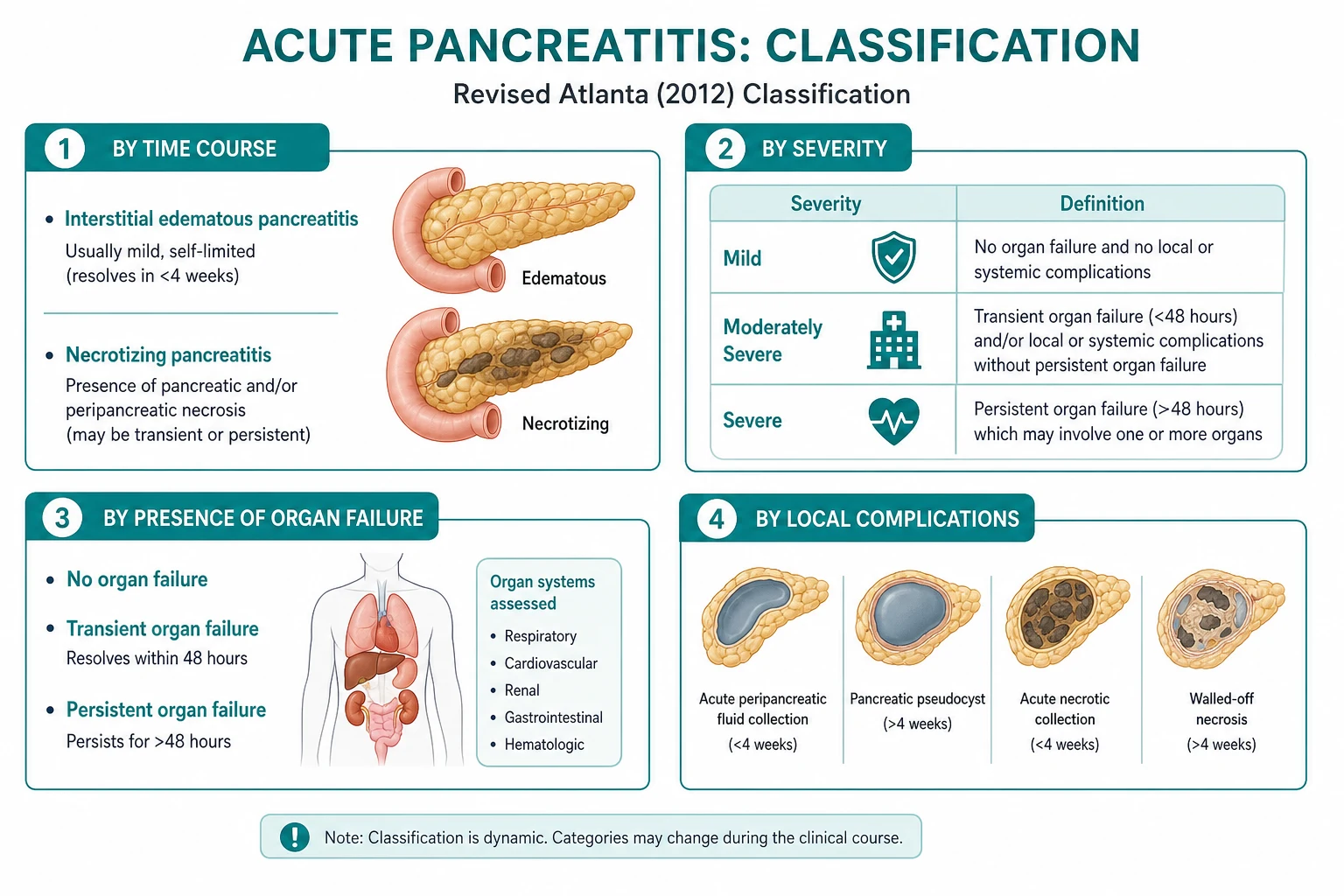
| Mild | No organ failure, no local or systemic complications | Absent | Absent | Under 1 per cent |
| Moderately severe | Transient organ failure (resolves within 48 hours) and/or local or systemic complications without persistent organ failure | Transient (less than 48 hours) | Present (necrosis, fluid collections, exacerbation of comorbid disease) | 3 to 5 per cent |
| Severe | Persistent organ failure (more than 48 hours) — may involve one or more of respiratory, cardiovascular, or renal systems | Persistent (more than 48 hours) | Present | 15 to 30 per cent |
The critical discriminator between moderately severe and severe is persistent organ failure beyond 48 hours, defined using the modified Marshall scoring system. A single persistent organ failure (for example, a creatinine above 170 micromol per litre or a PaO2 below 60 mmHg persisting for more than 48 hours) qualifies the patient as severe. [1]
BISAP — the bedside score (within 24 hours)
The Bedside Index of Severity in Acute Pancreatitis (BISAP) was derived from a population of nearly 18,000 patients to provide early risk stratification using data available within 24 hours of admission [6]. One point is allocated for each of five parameters; a score of 3 or above identifies severe disease:
| B | Blood urea nitrogen | Greater than 8.9 mmol per litre (25 mg per dL) |
|---|---|---|
| I | Impaired mental status | Disorientation, GCS below 15 |
| S | SIRS | Two or more of temperature, heart rate, respiratory rate or PaCO2, white cell count |
| A | Age | Greater than 60 years |
| P | Pleural effusion | On imaging (chest X-ray or CT) |
A BISAP score of 3 to 5 carries a mortality of 5 to 20 per cent, compared with under 1 per cent for a score of 0 to 1 [6] [7].
Ranson criteria — at admission and at 48 hours
Ranson criteria are scored at admission and at 48 hours. The limitation is that the full score can only be calculated at 48 hours, which limits its usefulness for early decisions. Three or more criteria indicate severe disease. [1]
At admission (non-gallstone):
- Age greater than 55 years
- White cell count greater than 16 times 10 to the 9 per litre
- Glucose greater than 10 mmol per litre
- AST greater than 250 IU per litre
- LDH greater than 350 IU per litre [1]
At 48 hours (non-gallstone):
- Haematocrit fall greater than 10 percentage points
- Urea increase greater than 1.8 mmol per litre despite fluids [1]- Calcium below 2 mmol per litre
- PaO2 below 60 mmHg
- Base deficit greater than 4
- Estimated fluid sequestration greater than 6 litres [1]
Gallstone Ranson modifies three parameters: age greater than 70, white cell count greater than 18, and LDH greater than 400 at admission; AST greater than 250 replaced by a different cut-off. [1]
APACHE II — the ICU score
APACHE II is the most accurate score but requires 12 to 14 physiological variables and is impractical without a calculator. It is used in ICU settings and in research. An APACHE II score of 8 or above at admission predicts severe disease. [1]
CRP at 48 hours — the single best late marker
A CRP above 150 mg per litre at 48 hours is the single most useful individual laboratory marker for pancreatic necrosis. CRP is low early (rises over 48 to 72 hours), so it is not useful for early triage but is excellent for the day 2 to 3 reassessment. [1]
DCE long-case trap: When asked to assess severity, state the severity using the Revised Atlanta Classification (mild, moderately severe, or severe), support it with the BISAP score and the CRP, and explain that the definitive determinant of severe disease is persistent organ failure beyond 48 hours. Do not say "Ranson 3 equals severe" without explaining the timing limitation. [1]
Investigations
First-line investigations at admission
| Investigation | Purpose |
|---|---|
| Serum lipase | Diagnostic — above 3 times ULN. Preferred over amylase (longer half-life, higher sensitivity and specificity). |
| Full blood count | Leukocytosis indicates inflammation and infection risk. Haematocrit for haemoconcentration (third-space loss) or anaemia (haemorrhage). |
| Urea and electrolytes | Urea above 8.9 mmol per litre is a BISAP criterion and a marker of hypovolaemia. Monitor creatinine for acute kidney injury. |
| Calcium | Hypocalcaemia is a marker of severity (saponification of calcium in fat necrosis). Hypercalcaemia suggests the cause. |
| Triglycerides | Above 11 mmol per litre identifies hypertriglyceridaemic pancreatitis. The serum is lactescent. |
| Arterial or venous blood gas | For pH, PaO2, and base deficit (Ranson criteria). Assess for metabolic acidosis and hypoxia. |
| Blood glucose | Hyperglycaemia is common (impaired insulin release from inflamed gland). Glucose above 10 mmol per litre is a Ranson criterion. |
| Abdominal ultrasound | Look for gallstones (the cause in 40 to 50 per cent). Often limited by ileus and body habitus, but should always be attempted at admission. |
| ECG | Exclude myocardial infarction (epigastric pain can be cardiac). |
Second-line and selective investigations
| Investigation | When to order |
|---|---|
| Contrast-enhanced CT abdomen | When the diagnosis is uncertain, when the patient fails to improve at 48 to 72 hours, or to assess for necrosis after the first week. NOT routinely at admission — the gland may look normal early, and contrast may worsen the ischaemia. |
| MRCP | For suspected biliary obstruction, choledocholithiasis, or biliary anatomy definition. Preferred over ERCP for diagnosis without the risk of post-procedure pancreatitis. |
| EUS | For occult biliary disease (microlithiasis, sludge) after recovery. The most sensitive test for small gallstones. |
| IgG4 | If autoimmune pancreatitis is suspected (painless jaundice, diffuse pancreatic enlargement, elevated IgG4). |
| Lipid panel | In all patients, but specifically when the serum is lactescent or the presentation is atypical. |
DWE trap: The most common imaging error is ordering a CT at admission for a patient with a clear clinical and biochemical diagnosis of pancreatitis. The ACG and IAP guidelines recommend AGAINST routine CT at admission. The CT is reserved for diagnostic uncertainty, failure to improve at 48 to 72 hours, or suspected complications. Early CT may underestimate the severity because necrosis takes 72 hours to fully develop, and contrast may theoretically worsen pancreatic perfusion. [1]
Management — the evidence-based bundle
1. Goal-directed fluid resuscitation (the WATERFALL revolution)
This is the single area where modern evidence has overturned the old dogma. For decades, the standard teaching was aggressive fluid resuscitation with Ringer lactate at 250 to 500 mL per hour initially, based on the rationale that aggressive fluids prevent necrosis by maintaining pancreatic perfusion. The WATERFALL trial (de Madaria, NEJM 2022) tested this directly and stopped early for harm [3].
WATERFALL trial design and results:
- Multicentre randomised trial of aggressive versus moderately aggressive fluid resuscitation.
- Aggressive group: bolus of 20 mL per kg over 2 hours, then 3 mL per kg per hour.
- Moderate group: bolus of 10 mL per kg only if hypovolaemic, then 1.5 mL per kg per hour.
- Result: aggressive resuscitation did NOT reduce the rate of moderately severe or severe pancreatitis, and caused significantly more fluid overload (including pulmonary oedema). [1]
The 2024 ACG guideline now recommends moderately aggressive, goal-directed fluid resuscitation with Ringer lactate, with frequent reassessment of volume status (every 6 hours) aiming to reduce the blood urea [2]. A practical approach:
- Initial: Ringer lactate 5 to 10 mL per kg per hour for the first 24 to 48 hours (not the old 250 to 500 mL per hour).
- Reassess every 6 hours: target a falling blood urea, stable haematocrit, and adequate urine output (0.5 to 1 mL per kg per hour).
- Reduce the rate once the urea is normalising or if fluid overload develops.
- Avoid boluses unless the patient is hypotensive or clearly hypovolaemic. [1]
Ringer lactate is preferred over normal saline because it reduces the systemic inflammatory response (the chloride in normal saline may worsen pancreatic perfusion via splanchnic vasoconstriction and is associated with metabolic acidosis). [1]
DWE high-yield question: "What fluid and rate for acute pancreatitis?" The 2024 answer: Ringer lactate, moderately aggressive (5 to 10 mL per kg per hour), with goal-directed reassessment every 6 hours. The old answer of "250 to 500 mL per hour of normal saline" is now wrong — WATERFALL showed it causes fluid overload. [1]
2. Analgesia
Pain control is essential. Opioids are first-line: morphine 2.5 to 5 mg IV every 4 hours, or a patient-controlled analgesia pump for severe pain. The historical concern that morphine causes sphincter of Oddi spasm and worsens pancreatitis is not supported by clinical evidence — there is no demonstrable difference in outcomes between morphine, fentanyl, or buprenorphine. Do not withhold adequate analgesia for this outdated concern. [1]
3. Nutrition — early enteral feeding within 24 to 48 hours
This is the second area where the dogma has been overturned. The traditional approach was "bowel rest with NPO and total parenteral nutrition" to rest the inflamed pancreas. Multiple randomised trials have shown that early enteral feeding (within 24 to 48 hours) is safe, reduces infectious complications, reduces the need for surgery, and reduces mortality compared with NPO and parenteral nutrition [2].
The practical approach:
- Mild pancreatitis: start a low-fat solid or liquid oral diet within 24 to 48 hours as pain and vomiting settle.
- Moderately severe or severe: if the patient cannot tolerate oral feeding, start nasogastric (or nasojejunal) enteral feeding within 48 to 72 hours. Nasogastric feeding is as effective as nasojejunal in most trials — the jejunum is not required unless there is intolerance to gastric feeding.
- Parenteral nutrition: reserved only for patients who cannot meet their nutritional needs enterally after 5 to 7 days (prolonged ileus, complex fistulae, or failed enteral feeding). [1]
DWE trap: The most common nutrition error in MCQs is choosing "keep NPO and start total parenteral nutrition." The correct answer for mild pancreatitis is to start an oral diet within 24 to 48 hours. For severe pancreatitis, the correct answer is enteral (not parenteral) feeding via a nasogastric or nasojejunal tube. [1]
4. ERCP — only for cholangitis or persistent biliary obstruction
Early ERCP (within 24 hours) is indicated in acute biliary pancreatitis only when there is concomitant cholangitis (fever, jaundice, right upper quadrant pain, or rigors with a dilated common bile duct and stone) or persistent biliary obstruction (a stone confirmed on imaging with rising bilirubin and ongoing obstruction) [2].
ERCP is NOT indicated for:
- Severe pancreatitis without cholangitis or obstruction.
- Mild or resolving biliary pancreatitis without obstruction (the stone has usually passed).
- Prophylactic sphincterotomy in patients who will undergo cholecystectomy. [1]
The ASGE and ACG guidelines converge on this point: the gallstone has usually passed into the duodenum by the time the patient presents with pancreatitis, so ERCP is unnecessary unless there is evidence of ongoing obstruction or cholangitis. [1]
5. Antibiotics — NOT prophylactic; only for infected necrosis
Prophylactic antibiotics are NOT recommended in acute pancreatitis, including severe necrotising disease. This is one of the most tested and most commonly mismanaged areas. Multiple randomised trials and meta-analyses (including the PROPATRIA-era trials) have shown that prophylactic antibiotics (whether carbapenems, quinolones, or beta-lactams) do not reduce infected necrosis, do not reduce mortality, and increase the risk of fungal infection and antibiotic resistance [2] [5].
Antibiotics are indicated when:
- Infected necrosis is proven or strongly suspected (gas in the necrotic collection on CT, clinical deterioration with fever and rising inflammatory markers, or a positive culture from fine-needle aspiration).
- There is a concomitant infection (cholangitis, pneumonia, bacteraemia, urinary tract infection).
- An extrapancreatic infection is driving the clinical picture. [1]
When antibiotics are indicated for infected necrosis, the preferred agents cover enteric gram-negatives and anaerobes: a carbapenem (meropenem 1 g IV every 8 hours) or piperacillin-tazobactam 4.5 g IV every 8 hours. The duration should be limited, and the antibiotics should be stopped once the infection source is controlled. [1]
6. The step-up approach for infected necrosis

The PANTER trial (van Santvoort, NEJM 2010) established the step-up approach as the standard for infected or symptomatic necrotising pancreatitis [4]. The trial randomised 88 patients with infected necrotising pancreatitis to either primary open necrosectomy or a step-up approach (percutaneous or endoscopic drainage first, with minimally invasive retroperitoneal necrosectomy only if drainage failed).
PANTER results:
- The step-up approach reduced the primary composite endpoint (major complications or death) from 69 per cent to 40 per cent.
- About 35 per cent of patients in the step-up group were managed with drainage alone and never needed necrosectomy.
- Fewer new-onset organ failures, fewer incisional hernias, and less exocrine insufficiency in the step-up group. [1]
The modern step-up algorithm:
- Antibiotics and supportive care first. Many patients with suspected infected necrosis improve with antibiotics alone, and the decision to intervene should be delayed until the collection is walled-off (usually after 4 weeks).
- Percutaneous or endoscopic catheter drainage. The first intervention when a walled-off collection is symptomatic or infected. Endoscopic drainage (transgastric or transduodenal via EUS-guided cystgastrostomy) is increasingly preferred because it avoids external fistulae and allows direct endoscopic necrosectomy.
- Endoscopic or minimally invasive necrosectomy. If drainage alone does not resolve the infection, proceed to endoscopic necrosectomy (via the transgastric route) or video-assisted retroperitoneal debridement (VARD).
- Open necrosectomy — the last resort, reserved for patients who fail all minimally invasive approaches or who require laparotomy for another reason. [1]
Timing is critical: intervene late, not early. The collection should be allowed to become walled-off (a defined capsule, usually after 4 weeks) before drainage is attempted. Early intervention before walling-off risks bleeding, uncontrolled infection, and enteric fistula formation. [1]
DWE trap: The most common MCQ error on necrosis management is choosing "open necrosectomy" or "immediate surgical debridement" for infected necrosis. The correct answer is the step-up approach: antibiotics, then percutaneous or endoscopic drainage, then minimally invasive necrosectomy. Open necrosectomy is the last resort, not the first. [1]
7. Gallstone pancreatitis — cholecystectomy timing
For mild gallstone pancreatitis, cholecystectomy should be performed during the index admission (once pain and inflammatory markers are settling) or within 2 weeks of discharge [8]. Meta-analyses of randomised trials show that same-admission cholecystectomy reduces recurrent biliary events (recurrent pancreatitis, biliary colic, cholangitis) without increasing surgical complications. The risk of recurrent pancreatitis is 20 to 25 per cent within 6 months if the gallbladder is left in situ.
For severe gallstone pancreatitis with necrosis or ongoing organ failure, cholecystectomy is deferred until recovery (usually 3 to 6 months) because the inflammation makes the dissection hazardous. In these patients, an intraoperative cholangiogram or pre-operative MRCP should be performed to exclude retained common bile duct stones. [1]
For patients who are not fit for surgery (advanced age, severe comorbidity), endoscopic sphincterotomy alone reduces recurrent biliary events as a bridge to cholecystectomy or as definitive therapy. [1]
Local complications — the Revised Atlanta morphological framework
The Revised Atlanta Classification standardises the terminology for local complications, which previously used overlapping and confusing terms ("phlegmon," "pancreatic abscess"). The key organising principles are: is there necrosis? and has the collection been present for more or less than 4 weeks? [1].
Interstitial oedematous pancreatitis (about 90 per cent)
In this subtype, the pancreatic parenchyma is inflamed but not necrotic. The local complications are fluid collections: [1]
| Collection | Timing | Composition | Management |
|---|---|---|---|
| Acute peripancreatic fluid collection (APFC) | Less than 4 weeks | Fluid only, no necrosis, no capsule | Usually resolves spontaneously; observe. |
| Pancreatic pseudocyst | More than 4 weeks | Fluid enclosed by a defined capsule (no epithelium), no necrosis | Drain only if symptomatic (pain, infection, gastric outlet obstruction). |
Necrotising pancreatitis (about 10 per cent)
In this subtype, there is necrosis of the pancreatic parenchyma, the peripancreatic tissue, or both. The local complications involve necrotic material: [1]
| Collection | Timing | Composition | Management |
|---|---|---|---|
| Acute necrotic collection (ANC) | Less than 4 weeks | Fluid and necrotic tissue, no defined wall | Observe if sterile; antibiotics and step-up drainage if infected. |
| Walled-off necrosis (WON) | More than 4 weeks | Necrotic material enclosed by a defined capsule | Drain (endoscopic preferred) if symptomatic or infected; may require necrosectomy. |
Infected versus sterile necrosis
The critical distinction is whether the necrosis is sterile or infected. Infected necrosis is the single most important determinant of mortality in necrotising pancreatitis (mortality 20 to 30 per cent versus 5 to 10 per cent for sterile necrosis). [1]
Features suggesting infected necrosis:
- Gas bubbles within the necrotic collection on CT (pathognomonic, from gas-forming organisms).
- Clinical deterioration after initial improvement (new fever, rising inflammatory markers, haemodynamic instability).
- Persistent fever and leukocytosis despite supportive care beyond the first week. [1]
When infection is suspected but not proven (no gas on CT, indeterminate clinical course), image-guided fine-needle aspiration for Gram stain and culture can confirm the diagnosis. However, this is performed less frequently now, as a deteriorating patient with necrosis is usually treated empirically with antibiotics and the step-up approach regardless of the aspiration result. [1]
Autoimmune pancreatitis
Autoimmune pancreatitis (AIP) is a distinct entity that every fellowship candidate must recognise because it mimics pancreatic cancer and is dramatically steroid-responsive. There are two subtypes: [1]
Type 1 (IgG4-related disease)
Type 1 AIP is the pancreatic manifestation of IgG4-related disease, a systemic fibroinflammatory disorder characterised by dense lymphoplasmacytic infiltrates rich in IgG4-positive plasma cells. It affects older men (sixth to seventh decade) and presents classically as painless obstructive jaundice (from a swollen pancreatic head compressing the common bile duct) with a discrete pancreatic mass on imaging — a presentation that is indistinguishable from pancreatic adenocarcinoma without biopsy. [1]
Diagnostic features (HISORt criteria):
- Histology: dense periductal lymphoplasmacytic infiltrate, storiform fibrosis, obliterative phlebitis, and more than 10 IgG4-positive plasma cells per high-power field.
- Imaging: diffuse (sausage-shaped) pancreatic enlargement with a capsule-like rim, and irregular narrowing of the main pancreatic duct. There may be associated IgG4-related sclerosing cholangitis (mimicking cholangiocarcinoma).
- Serology: elevated serum IgG4 (above 1.4 g per litre; sensitivity 76 per cent, specificity 93 per cent). Note that IgG4 can be elevated in pancreatic cancer and cholangiocarcinoma, so it is not diagnostic alone.
- Other organ involvement: the defining feature of IgG4-related disease. Look for sclerosing cholangitis, retroperitoneal fibrosis, salivary and lacrimal gland enlargement (Mikulicz syndrome), renal lesions, and hilar lymphadenopathy.
- Response to steroids: dramatic. A 2-week trial of prednisolone 0.6 to 1 mg per kg per day produces objective radiological and biochemical improvement. This response is so characteristic that it is used diagnostically. [1]
Management: prednisolone 0.6 to 1 mg per kg per day (typically 30 to 40 mg daily) for 2 to 4 weeks, then taper over weeks to months. About 40 to 50 per cent of patients relapse, requiring maintenance immunosuppression with azathioprine or mycophenolate. [1]
Type 2 (idiopathic duct-centric pancreatitis)
Type 2 AIP is a separate entity that is NOT IgG4-related. It affects younger patients (third to fourth decade), is equally common in men and women, is often associated with inflammatory bowel disease (especially ulcerative colitis), and has a normal serum IgG4. Histology shows granulocytic epithelial lesions (neutrophilic infiltration of the duct epithelium) without IgG4-positive plasma cells. It is also steroid-responsive but relapses less frequently than Type 1. [1]
DWE high-yield discriminator: The exam favourite is the older man with painless jaundice, a pancreatic mass, and an elevated IgG4. The trap is to assume pancreatic cancer and proceed to surgery without considering autoimmune pancreatitis. The answer is to check IgG4, perform EUS with core biopsy or FNA, and consider a steroid trial if the histology and imaging are characteristic. Cancer must always be excluded first, but a dramatic steroid response is the clinical hallmark. [1]
Prognosis and follow-up
Mortality and recovery
- Mild pancreatitis: mortality under 1 per cent. Most patients recover in 3 to 7 days.
- Moderately severe pancreatitis: mortality 3 to 5 per cent. Recovery over 1 to 3 weeks.
- Severe pancreatitis with persistent organ failure: mortality 15 to 30 per cent. Recovery is prolonged, often months, and may involve rehabilitation for deconditioning, ongoing exocrine and endocrine pancreatic insufficiency, and psychological sequelae of a critical illness. [1]
Exocrine and endocrine insufficiency
After necrotising pancreatitis, especially when the gland has lost more than 50 per cent of its parenchyma, exocrine insufficiency (steatorrhoea, weight loss, fat-soluble vitamin deficiency) develops in 20 to 40 per cent of patients. Treat with pancreatic enzyme replacement (pancreatin 25,000 to 40,000 units with meals). Endocrine insufficiency (diabetes) develops in 15 to 30 per cent and may be brittle (difficult to control) because of the loss of both insulin and glucagon secretion. [1]
Recurrence and prevention
- Gallstone pancreatitis: the risk of recurrence is 20 to 25 per cent within 6 months without cholecystectomy. Cholecystectomy during the index admission or within 2 weeks is the standard [8].
- Alcohol pancreatitis: counsel for complete abstinence. Continued drinking leads to recurrent attacks and progression to chronic pancreatitis (with chronic pain, exocrine and endocrine insufficiency, and an elevated risk of pancreatic cancer).
- Hypertriglyceridaemia: treat with a fibrate (fenofibrate), omega-3 fatty acids, dietary modification, diabetic control, and avoidance of alcohol and oestrogen. Target triglycerides below 5 mmol per litre.
DCE long-case approach: severe necrotising pancreatitis
For a long case of severe pancreatitis, structure the presentation as follows: [1]
Opening statement (SASPOP): "Doctor, my patient is a 58-year-old man presenting with severe acute gallstone pancreatitis complicated by persistent organ failure (acute kidney injury and acute respiratory distress syndrome) and infected walled-off necrosis requiring endoscopic drainage, who has developed new-onset diabetes. He is a heavy drinker. His problems are: severe acute pancreatitis (Revised Atlanta severe); infected walled-off necrosis; acute kidney injury (recovering); persistent pleural effusion; alcohol use disorder; new-oncentred diabetes; and malnutrition." [1]
Problem list (numbered and prioritised):
- Severe necrotising gallstone pancreatitis with infected walled-off necrosis.
- Organ failure (acute kidney injury, resolving; respiratory, resolved).
- Malnutrition requiring nasojejunal feeding.
- Alcohol use disorder and alcohol withdrawal risk.
- New-onset diabetes (pancreoprivic, likely brittle).
- Future cholecystectomy once recovered.
- Rehabilitation and deconditioning. [1]
Integrated management plan:
- Ongoing source control: continue endoscopic drainage of the walled-off necrosis; repeat endoscopic necrosectomy if the collection re-accumulates. Meropenem for infected necrosis, with a plan to de-escalate and stop once source-controlled.
- Nutrition: nasojejunal enteral feeding; aim for positive nitrogen balance; plan transition to oral diet as ileus resolves. Pancreatic enzyme replacement for steatorrhoea.
- Diabetes: endocrinology input; likely to require insulin (often basal-bolus); monitor for hypoglycaemia (loss of glucagon counter-regulation makes it brittle).
- Alcohol: alcohol withdrawal prophylaxis (thiamine, benzodiazepines as needed); addiction counselling; plan for supervised detoxification.
- Surgical: cholecystectomy once the patient has recovered from the acute episode (3 to 6 months), with intraoperative cholangiogram to exclude retained stones.
- Rehabilitation: early mobilisation, physiotherapy, and functional recovery. [1]
DCE short-case approach: abdominal examination
When asked to examine the abdomen of a patient recovering from pancreatitis, the systematic routine is: [1]
- End of bed inspection: assess for distress, pain posture (sitting forward), jaundice, and signs of chronic alcohol use (spider naevi, palmar erythema, parotid enlargement, gynaecomastia, muscle wasting). Look for the periumbilical and flank discolouration (Cullen and Grey Turner signs) in severe disease.
- Hands and arms: look for clubbing, palmar erythema, asterixis (in hepatic encephalopathy), and track marks (IV drug use). Check for Dupuytren contracture (alcohol association).
- Face: conjunctival pallor, scleral icterus, parotid enlargement, and perioral signs of hyperlipidaemia (xanthelasma, corneal arcus).
- Neck: jugular venous pressure (hypovolaemia), cervical lymphadenopathy.
- Chest: look for pleural effusion (especially left-sided — a sign of severity).
- Abdomen: inspect for scars (previous surgery), distension (ileus, ascites), and visible peristalsis. Palpate for epigastric tenderness, guarding, and a palpable mass (pseudocyst or inflammatory mass). Check for shifting dullness (ascites). Auscultate bowel sounds (absent or tinkling in ileus).
- Back: look for Grey Turner sign (flank discolouration). Examine for spinal tenderness if relevant. [1]
Presentation template: [1]
"I examined Mr Smith's abdominal system. He is comfortable at rest but is sitting forward, consistent with pain. There is no jaundice, pallor, or stigmata of chronic liver disease. The abdomen is soft with marked epigastric tenderness but no guarding or rigidity. There is no palpable mass, hepatosplenomegaly, or ascites. Bowel sounds are sparse, consistent with a paralytic ileus. There is no Cullen or Grey Turner sign. These findings are consistent with acute pancreatitis without evidence of haemorrhagic or necrotising complications. I would like to review the observations, confirm the diagnosis with a serum lipase, and organise an abdominal ultrasound to look for gallstones." [1]
Key DWE MCQ patterns
- Which fluid and rate for acute pancreatitis? Ringer lactate, moderately aggressive (5 to 10 mL per kg per hour), goal-directed with reassessment every 6 hours — NOT 250 to 500 mL per hour (WATERFALL showed harm). [1]2. When are prophylactic antibiotics indicated? Never — prophylactic antibiotics are NOT recommended, including in severe necrotising disease.
- When is early ERCP indicated in biliary pancreatitis? Only for cholangitis or persistent biliary obstruction — NOT for severity alone.
- When should a CT be ordered? For diagnostic uncertainty or failure to improve at 48 to 72 hours — NOT routinely at admission.
- What is the preferred initial management of infected necrosis? The step-up approach (antibiotics, then percutaneous or endoscopic drainage) — NOT open necrosectomy.
- What nutrition for mild pancreatitis? Oral diet within 24 to 48 hours — NOT NPO with parenteral nutrition.
- When should cholecystectomy be performed after mild gallstone pancreatitis? During the index admission or within 2 weeks.
- Which enzyme is preferred for diagnosis? Lipase (more sensitive and specific, longer half-life) over amylase.
- What is the BISAP score threshold for severe disease? 3 or above (of 5).
- What defines severe pancreatitis per the Revised Atlanta Classification? Persistent organ failure (more than 48 hours).
- Which probiotics are recommended? None — probiotics are contraindicated (PROPATRIA showed increased mortality and bowel ischaemia).
- Which ALT level strongly suggests gallstone pancreatitis? Above 150 IU per litre (PPV 95 per cent). [1]
References
[1] Banks, Bollen, Dervenis, et al. (2013) — Revised Atlanta Classification: two morphological types (interstitial oedematous and necrotising), three severity tiers (mild, moderately severe, severe), and standardised terminology for fluid collections (APFC, pseudocyst, ANC, WON) based on necrosis and timing.
[2] Tenner, Baillie, DeWitt, Vege, et al. (2024) — ACG Guideline: moderately aggressive goal-directed Ringer lactate fluids, early enteral nutrition within 24 to 48 hours, no prophylactic antibiotics, ERCP within 24 hours only for cholangitis or persistent obstruction, and the step-up approach for infected necrosis.
[3] de-Madaria, Buxbaum, Maisonneuve, et al. (WATERFALL, 2022) — Aggressive fluid resuscitation (20 mL per kg bolus then 3 mL per kg per hour) did not improve outcomes and caused significantly more fluid overload than moderate resuscitation (10 mL per kg bolus only if hypovolaemic, then 1.5 mL per kg per hour). Trial stopped early for harm.
[4] van Santvoort, Besselink, Bakker, et al. (PANTER, 2010) — The step-up approach (percutaneous or endoscopic drainage first, with minimally invasive necrosectomy only if drainage failed) reduced major complications or death from 69 to 40 per cent versus primary open necrosectomy; 35 per cent needed drainage alone.
[5] Besselink, van Santvoort, Buskens, et al. (PROPATRIA, 2008) — Probiotic prophylaxis in predicted severe acute pancreatitis did not reduce infectious complications and significantly increased mortality (16 versus 6 per cent) and bowel ischaemia. Probiotics are contraindicated in acute pancreatitis.
[6] Wu, Johannes, Sun, Tabak, Conwell, Banks (2008) — Derivation of the BISAP score from a population of nearly 18,000 patients: five parameters (BUN, impaired mental status, SIRS, age, pleural effusion) available within 24 hours; a score of 3 or above identifies severe disease with a mortality of 5 to 20 per cent.
[7] Papachristou, Muddana, Yadav, et al. (2010) — Prospective comparison of BISAP, Ranson, APACHE II, and CTSI scores: BISAP performs comparably to Ranson and APACHE II for predicting organ failure, complications, and mortality, and is superior for early (within 24 hours) risk stratification.
[8] Moody, Yadav, Hossain, Haque, Adler (2020) — Meta-analysis of five randomised trials: early (same-admission) cholecystectomy for mild biliary pancreatitis reduces recurrent biliary events without increasing surgical complications compared with delayed (interval) cholecystectomy.
GESA (Gastroenterological Society of Australia) clinical practice guidelines; IAP and APA (International Association of Pancreatology and American Pancreatic Association) evidence-based guidelines; BSG (British Society of Gastroenterology) guidelines on the management of acute pancreatitis. [1]
References
- [1]Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus Gut, 2013.PMID 23100216
- [2]Tenner S, Baillie J, DeWitt J, Vege SS, et al. American College of Gastroenterology Guidelines: Management of Acute Pancreatitis Am J Gastroenterol, 2024.PMID 38857482
- [3]de-Madaria E, Buxbaum JL, Maisonneuve P, et al. Aggressive or Moderate Fluid Resuscitation in Acute Pancreatitis N Engl J Med, 2022.PMID 36103415
- [4]van Santvoort HC, Besselink MG, Bakker OJ, et al. A step-up approach or open necrosectomy for necrotizing pancreatitis N Engl J Med, 2010.PMID 20410514
- [5]Besselink MG, van Santvoort HC, Buskens E, et al. Probiotic prophylaxis in predicted severe acute pancreatitis: a randomised, double-blind, placebo-controlled trial Lancet, 2008.PMID 18279948
- [6]Wu BU, Johannes RS, Sun X, Tabak Y, Conwell DL, Banks PA The early prediction of mortality in acute pancreatitis: a large population-based study Gut, 2008.PMID 18519429
- [7]Papachristou GI, Muddana V, Yadav D, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis Am J Gastroenterol, 2010.PMID 19861954
- [8]Moody N, Yadav A, Hossain E, Haque K, Adler DG Meta-analysis of randomized clinical trials of early versus delayed cholecystectomy for mild gallstone pancreatitis Br J Surg, 2019.PMID 31268184