Phys · gastrointestinal
Chronic Pancreatitis
Also known as chronic pancreatitis · chronic calcific pancreatitis · fibrocalculous pancreatic diabetes · tropical calcific pancreatitis · autoimmune pancreatitis · hereditary pancreatitis · pancreatogenic diabetes · type 3c diabetes
Consultant-physician-depth guide to chronic pancreatitis — the irreversible fibroinflammatory destruction of pancreatic parenchyma, the TIGAR-O mechanistic aetiology (alcohol 70 per cent, hereditary PRSS1/SPINK1/CFTR, autoimmune IgG4-related type 1, tropical calcific, obstructive), the clinical triad of chronic epigastric pain, steatorrhoea from exocrine insufficiency, and type 3c brittle diabetes, the investigations (faecal elastase below 200, CT calcification, MRCP ductal anatomy, EUS Rosemont early changes), the analgesic ladder and endoscopic-surgical drainage (Puestow, Frey, Beger, Whipple, Cahen trial), pancreatic enzyme replacement, and pancreatic cancer surveillance. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Chronic Pancreatitis

The answer first
Chronic pancreatitis is an irreversible, progressive fibroinflammatory syndrome of the pancreas in which recurrent injury destroys acinar and islet cells and replaces them with fibrosis, ultimately producing permanent exocrine insufficiency (steatorrhoea, malabsorption, malnutrition) and endocrine insufficiency (type 3c, pancreatogenic, diabetes). The 2016 mechanistic consensus redefined it as a pathological fibroinflammatory syndrome rather than a purely morphological diagnosis, emphasising that the disease is a continuous inflammatory process driven by identifiable mechanisms rather than simply the late end-stage of scarring [1].
The clinical triad that every physician must know is chronic recurrent epigastric pain radiating to the back, steatorrhoea, and new-onset diabetes in the context of chronic alcohol use. Alcohol is responsible for about 70 per cent of cases. The single most important concept is that chronic pancreatitis is irreversible but manageable: the fibrosis cannot be undone, so management is structured around the four pillars of pain control, replacement of exocrine function (pancreatic enzymes), control of endocrine insufficiency (insulin), and treatment of complications including pancreatic cancer surveillance [3].
DCE trap: The biggest pivot in chronic pancreatitis is recognising that the disease moves through phases. Early disease is dominated by recurrent painful attacks that mimic acute pancreatitis; as the gland burns out, the pain often abates while steatorrhoea (appearing only after 90 per cent of enzyme secretory capacity is lost) and brittle type 3c diabetes dominate. In every long case, state the aetiology using the TIGAR-O classification, quantify both exocrine and endocrine insufficiency, and always exclude pancreatic cancer in any patient with an inflammatory head mass or a change in symptoms. [1]
Definition and pathophysiology — the mechanistic framework
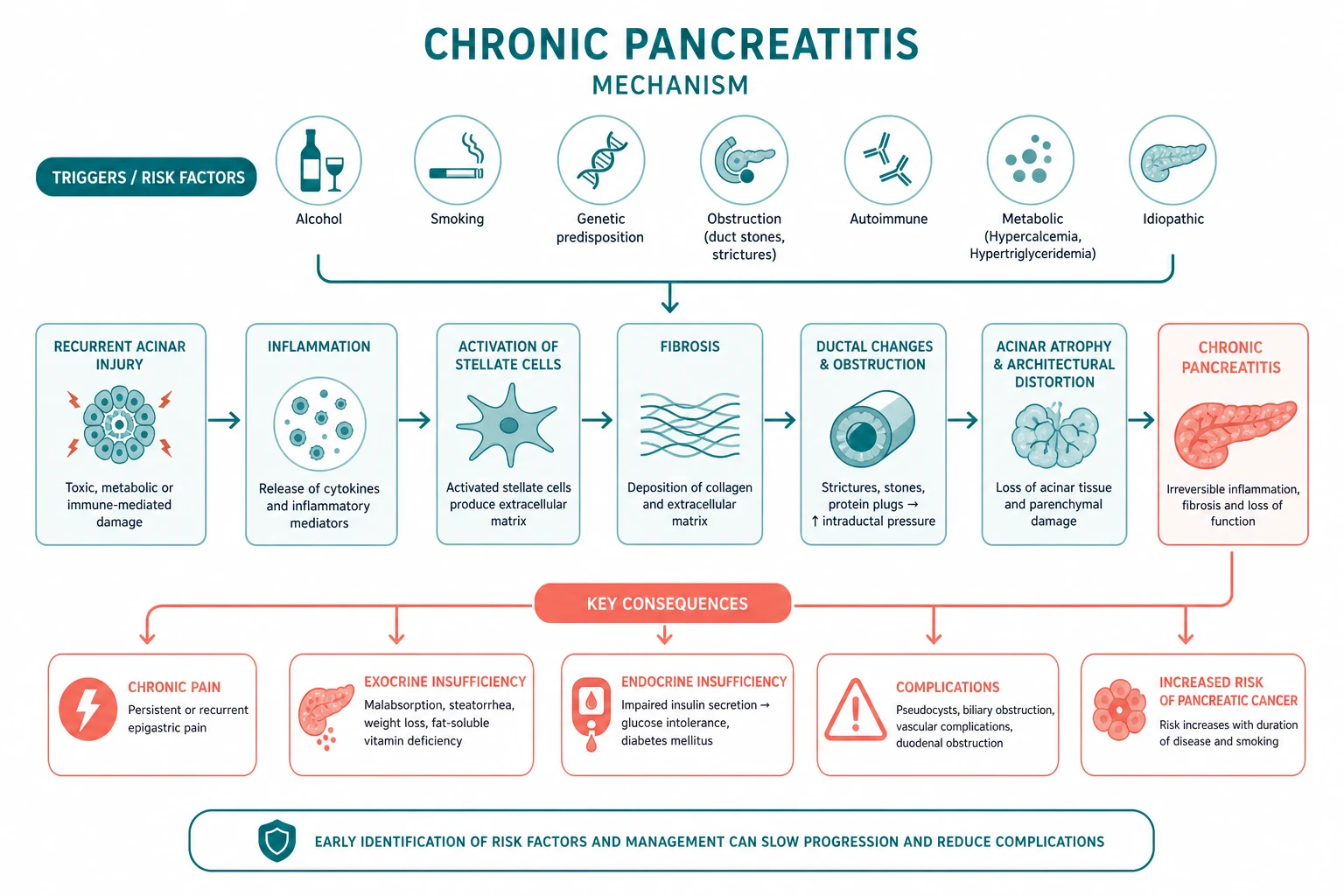
The traditional morphological definition — irreversible destruction of pancreatic parenchyma with fibrosis — has been superseded by the 2016 mechanistic consensus, which defines chronic pancreatitis as a pathological fibroinflammatory syndrome of the pancreas in which persistent injury produces irreversible structural damage with permanent loss of exocrine and endocrine function [1]. This shift matters because it allows the disease to be diagnosed and managed earlier, before the end-stage calcification and ductal distortion that the old definition required.
The SAPE and necrosis-fibrosis sequence
Three converging hypotheses explain how recurrent injury becomes irreversible fibrosis [1] [2]:
- The sentinel acute pancreatitis event (SAPE) hypothesis — a first, often subclinical, attack of acute pancreatitis primes the gland. Persistent or recurrent stressors (alcohol, smoking, genetic susceptibility) then drive a chronic fibroinflammatory response.
- The necrosis-fibrosis sequence — repeated episodes of necrosis heal by fibrosis; the more severe and frequent the necrosis, the more extensive the eventual scarring. This is why severe necrotising acute pancreatitis and recurrent acute pancreatitis both predispose to chronic disease.
- The ductal hypertension and protein-plug hypothesis — in alcoholic disease, hyperconcentrated protein-rich pancreatic juice precipitates as protein plugs in the small ducts. These plugs calcify into stones, obstruct ducts, raise intraductal pressure, and drive periductular fibrosis and acinar atrophy. [1]
The final common pathway is the activation of pancreatic stellate cells, the fibroblast-like cells of the pancreas. Once activated by injury, alcohol metabolites, or cytokines, they proliferate and deposit collagen, producing the dense fibrosis that is the histological hallmark and the substrate for the irreversible loss of function. [1]
DWE high-yield mechanism question: "Why does steatorrhoea appear late in chronic pancreatitis?" Answer: The pancreas has enormous functional reserve. Lipase and colipase secretion must fall to less than 10 per cent of normal (more than 90 per cent loss of secretory capacity) before fat malabsorption becomes clinically apparent. This is why early disease presents with pain alone and steatorrhoea is a feature of established, burnt-out disease. [1]
Causes — the TIGAR-O classification
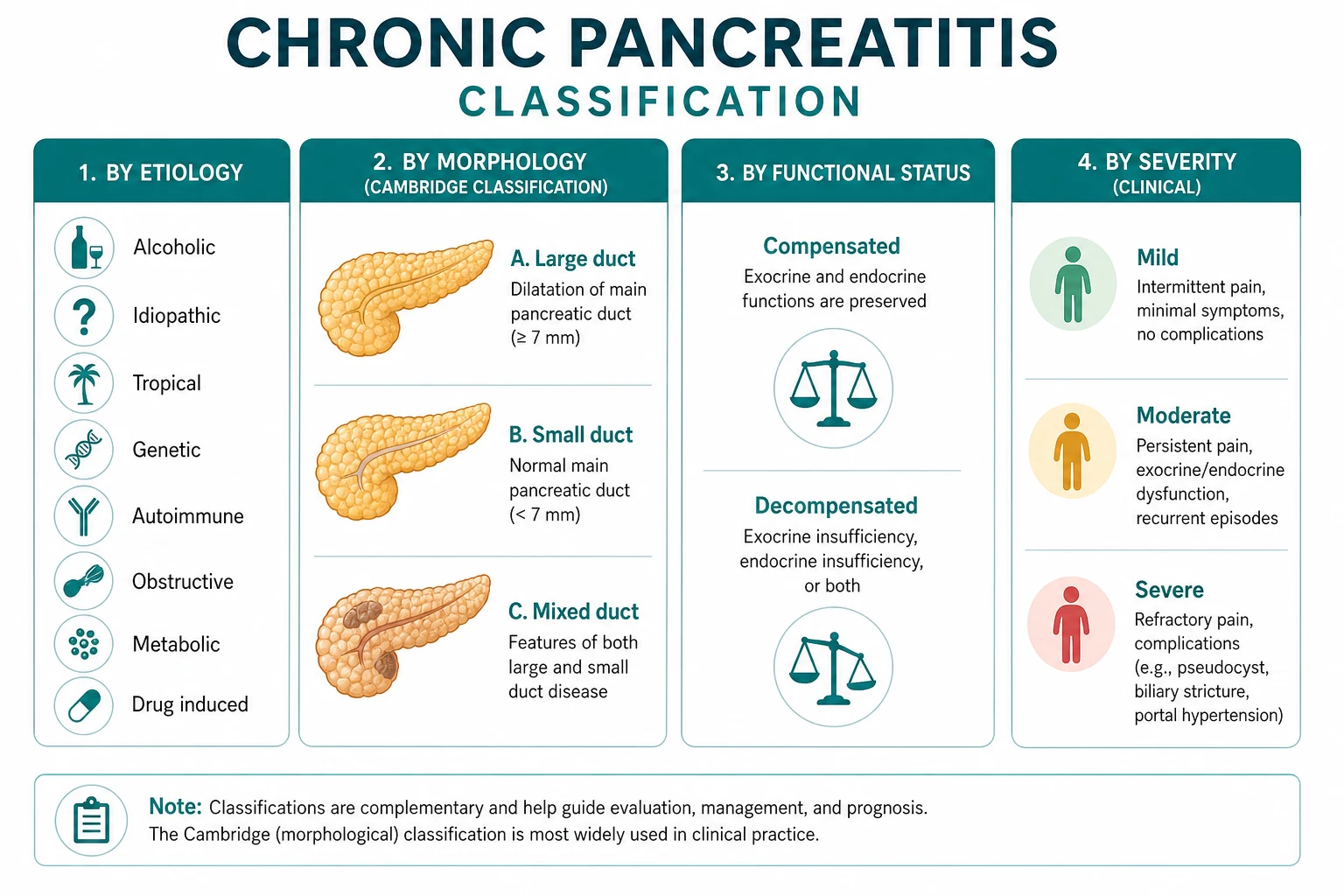
The TIGAR-O mechanistic classification, revised in 2019 (version 2), is the framework the examiner expects. It classifies risk factors into six mechanistic categories and supersedes the older, purely descriptive aetiological lists [2].
| Category | Examples | Exam-relevant points |
|---|---|---|
| Toxic-metabolic | Alcohol (the dominant cause, about 70 per cent), tobacco smoking, hypercalcaemia, hypertriglyceridaemia, chronic renal failure | Alcohol is dose-related but not deterministic — only a minority of heavy drinkers develop chronic pancreatitis, indicating cofactors (smoking is the most important). Smoking independently accelerates fibrosis and markedly increases pancreatic cancer risk. |
| Idiopathic | Early-onset (young adults, pain-predominant) and late-onset (older, painless, insufficiency-predominant) | Consider occult genetic causes and autoimmune disease before labelling idiopathic. Tropical calcific pancreatitis is a distinct entity. |
| Genetic | PRSS1 (hereditary pancreatitis), SPINK1, CFTR, CTRC | Hereditary PRSS1 pancreatitis: autosomal dominant, recurrent acute pancreatitis from childhood, a strong family history, and a markedly elevated lifetime pancreatic cancer risk. SPINK1 is a modifier (loss of trypsin inhibition) and is enriched in tropical and idiopathic disease. CFTR causes duct obstruction. |
| Autoimmune | Type 1 (IgG4-related disease), Type 2 (idiopathic duct-centric pancreatitis) | Type 1 is the pancreatic manifestation of IgG4-related disease: an older man with painless obstructive jaundice, a sausage-shaped gland, elevated serum IgG4, other organ involvement, and a dramatic response to steroids. It is the one form that is reversible. |
| Recurrent and severe acute pancreatitis | After gallstone, alcoholic, or hypertriglyceridaemic acute pancreatitis | The SAPE and necrosis-fibrosis pathways. Recurrent acute pancreatitis is a recognised precursor. |
| Obstructive | Pancreatic ductal adenocarcinoma, pancreas divisum, ampullary stenosis, post-traumatic duct strictures | Obstructive chronic pancreatitis improves when the obstruction is relieved, distinguishing it from the irreversible toxic-metabolic forms. Pancreas divisum is a controversial cause — symptomatic disease requires dorsal duct changes. |
Tropical calcific (fibrocalculous pancreatic) pancreatitis
This is a distinct form seen in young, thin, non-drinking patients from southern India (Kerala), tropical Africa, and south-east Asia. It is characterised by large, dense intraductal calculi in a markedly dilated main pancreatic duct, early and severe insulin-requiring diabetes (fibrocalculous pancreatic diabetes, a form of type 3c diabetes), and marked malnutrition. The cassava (cyanogenic glycoside) hypothesis, chronic protein-calorie malnutrition, and a high prevalence of SPINK1 mutations are implicated. It is a high-yield MRCP and DWE entity because its radiological and demographic picture is unmistakable. [1]
Autoimmune pancreatitis — the reversible exception
Type 1 autoimmune pancreatitis must never be missed because, unlike every other form of chronic pancreatitis, it is steroid-responsive. It is the pancreatic manifestation of IgG4-related disease and typically presents in an older man with painless obstructive jaundice, a diffusely enlarged sausage-shaped pancreas with a capsule-like rim on imaging, irregular narrowing of the main pancreatic duct, elevated serum IgG4, and other organ involvement (sclerosing cholangitis, retroperitoneal fibrosis, salivary and lacrimal gland enlargement, renal lesions). Diagnosis is made with the International Consensus Diagnostic Criteria (ICDC), which integrate imaging, serology, other organ involvement, histology (lymphoplasmacytic sclerosing pancreatitis with storiform fibrosis and abundant IgG4-positive plasma cells), and an optional steroid response [8]. Treatment is prednisolone 0.6 to 1 mg per kg per day for two to four weeks with a taper; the response is dramatic and is itself diagnostic. Relapse is common (40 to 50 per cent) and requires maintenance immunosuppression (azathioprine, mycophenolate, or rituximab). Type 2 is separate (idiopathic duct-centric, IgG4-negative, younger patients, associated with inflammatory bowel disease).
DCE trap: The cardinal error is operating on an autoimmune pancreatitis mass for presumed pancreatic cancer without considering the diagnosis. A diffusely enlarged gland with elevated IgG4 and capsule-like rim should trigger a steroid trial, not a Whipple — a dramatic response is the clinical hallmark. [1]
Clinical presentation
Chronic pancreatitis evolves through two phases that determine the clinical picture at any given time. [1]
Early disease — the painful phase
The hallmark is chronic, recurrent epigastric pain radiating to the back, often precipitated by alcohol or fatty food, lasting hours to days, and severe enough to require opioids. Attacks resemble acute pancreatitis (nausea, vomiting, tenderness) and may be complicated by acute-on-chronic inflammation. Between attacks there may be background constant pain. Weight loss from anorexia, food avoidance, and malabsorption begins insidiously. [1]
A subset (especially late-onset idiopathic and autoimmune) is painless, presenting with steatorrhoea, diabetes, or an incidental radiological finding — painlessness is therefore not a reliable exclusion. [1]
Late (burnt-out) disease — the insufficiency phase
As the gland is progressively destroyed, two things happen: the pain often abates (the pain-generating parenchyma and nerves are destroyed), and exocrine and endocrine insufficiency dominate [3].
Exocrine insufficiency manifests as:
- Steatorrhoea — foul-smelling, bulky, greasy stools that are difficult to flush, the cardinal sign that appears only after 90 per cent of enzyme secretory capacity is lost.
- Weight loss and malnutrition — from fat and protein malabsorption combined with reduced oral intake from pain and alcohol.
- Fat-soluble vitamin deficiency — vitamin A (night blindness), D (osteomalacia, osteoporosis), E (neuropathy, ataxia), and K (coagulopathy, easy bruising). [1]
Endocrine insufficiency manifests as type 3c (pancreatogenic) diabetes, which is different from type 2 in several important ways (see below). [1]
Bedside signs
Physical examination is often unremarkable. Look for:
- Cachexia and muscle wasting from malnutrition.
- Epigastric tenderness, and occasionally a palpable mass (a pseudocyst or an inflammatory head mass).
- Signs of chronic alcoholic liver disease (spider naevi, palmar erythema, parotid enlargement) when alcohol is the cause.
- Signs of malabsorption (easy bruising, koilonychia).
- Stigmata of chronic insulin-requiring diabetes and its complications. [1]
Investigations — function and imaging are complementary
Diagnosis requires evidence of pancreatic dysfunction or characteristic irreversible morphological change. No single test is sufficient, particularly in early disease where both function and imaging may be subtle. The M-ANNHEIM criteria integrate aetiology, clinical course, and severity, and the Cambridge (and EUS Rosemont) criteria grade morphological severity [4] [3].
Pancreatic function tests
- Faecal elastase-1 is the best non-invasive marker of exocrine insufficiency. It is a stool test, requires a single sample, and is not affected by pancreatic enzyme replacement therapy (because the enzyme measured is human pancreatic elastase, not the porcine enzyme in replacement preparations). A level below 200 micrograms per gram indicates exocrine insufficiency, and below 100 indicates severe insufficiency. The crucial limitation is that it is insensitive in mild disease — sensitivity may be as low as 40 to 50 per cent in early chronic pancreatitis, rising above 85 per cent in severe disease. A normal faecal elastase does not exclude exocrine insufficiency in a patient with a compatible clinical picture [3].
- Faecal fat (72-hour collection on a 100 g per day fat diet), with faecal fat exceeding 7 g per day indicating steatorrhoea, is now rarely used because it is unpleasant, requires dietary compliance, and is less specific (any cause of fat malabsorption raises it).
- The 13C-mixed triglyceride breath test is a sensitive indirect test of lipase function but is not widely available.
- Direct pancreatic function tests (secretin or cholecystokinin stimulation with duodenal aspiration) are the gold standard but are invasive and largely research tools.
Imaging
Imaging is graded by the Cambridge classification (normal, equivocal, mild, moderate, marked), which correlates with the severity of ductal and parenchymal change. [1]
- Abdominal X-ray — pancreatic calcification is highly specific when present but is seen in only about 30 per cent of cases. A normal film does not exclude chronic pancreatitis.
- Contrast-enhanced CT — the first-line cross-sectional modality in established disease, showing ductal dilatation, parenchymal calcification, gland atrophy, and complications (pseudocyst, inflammatory mass, splenic vein thrombosis).
- MRCP — the best non-invasive assessment of ductal anatomy, defining strictures, stones, ductal dilatation, and side-branch changes without radiation. Secretin-enhanced MRCP improves ductal visualisation and can detect early disease.
- Endoscopic ultrasound (EUS) — the most sensitive modality for early chronic pancreatitis, detecting subtle parenchymal and ductal changes before they are visible on CT or MRCP. The Rosemont criteria grade parenchymal (hyperechoic foci with shadowing, lobularity with honeycombing) and ductal (main duct irregularity, calculi, visible side branches) features. The limitation is inter-observer variability and the risk of over-diagnosing early change in older patients.
- ERCP — now reserved for therapeutic intervention (stenting, stone removal) rather than diagnosis, given its invasiveness and the availability of MRCP and EUS. [1]
Endocrine assessment
Every patient should be screened for diabetes with fasting glucose and HbA1c; an oral glucose tolerance test is used when equivocal. When diabetes is present, the Ewald criteria confirm type 3c diabetes: exocrine insufficiency (faecal elastase), pathological pancreatic imaging, and the absence of type 1 diabetes-associated autoimmunity [5] [6].
The aetiological workup
Identify the cause to guide targeted therapy and surveillance: a detailed alcohol and smoking history, serum IgG4 (autoimmune), a lipid panel and calcium (hypertriglyceridaemia, hypercalcaemia), and, when indicated, genetic testing (PRSS1, SPINK1, CFTR) — particularly in young patients, those with a family history, and those without an obvious toxic cause [2].
DWE trap: A normal faecal elastase and a normal CT do not exclude early chronic pancreatitis. If the clinical suspicion is high (recurrent typical pain in a heavy drinker), EUS with the Rosemont criteria is the investigation of choice because it detects parenchymal change before calcification or ductal dilatation appears on CT. [1]
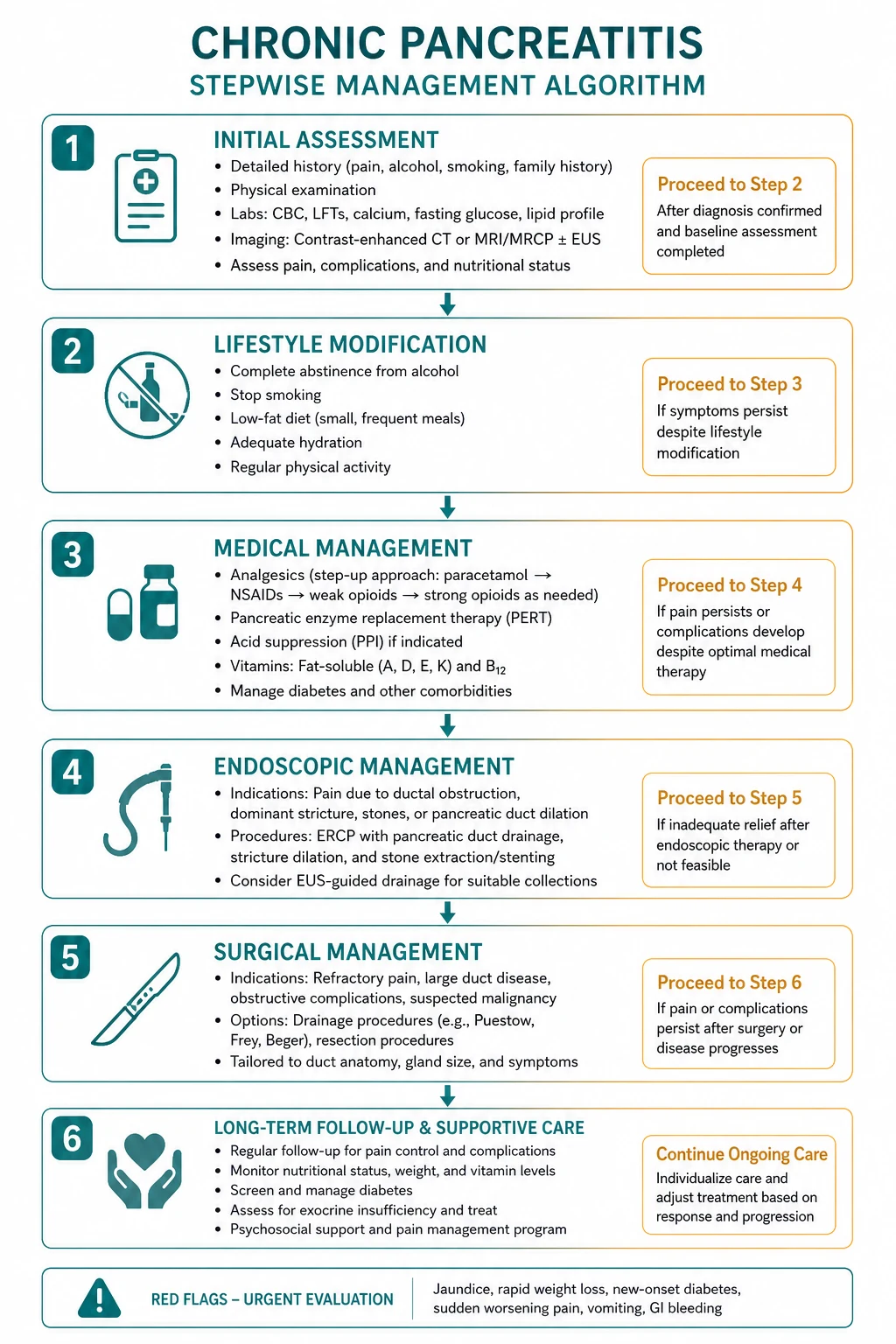
Management — the four pillars
Management is structured around four pillars: (1) pain control, (2) replacement of exocrine function, (3) control of endocrine insufficiency, and (4) treatment of complications and surveillance [3]. The first step in every patient is the elimination of precipitants — complete alcohol abstinence and smoking cessation — which slow progression and reduce pancreatic cancer risk.
Pillar 1 — pain control
Pain is the dominant problem in early disease and the principal driver of disability and opioid dependence. Management follows a stepped approach [3]:
- Eliminate precipitants — alcohol abstinence and smoking cessation are first-line and may reduce pain frequency.
- Non-opioid analgesics — paracetamol and NSAIDs (with gastroprotection and renal monitoring).
- Weak opioids — tramadol, then low-dose strong opioids (oral morphine, oxycodone), titrated with a clear plan to minimise dependence.
- Adjunct neuropathic agents — pregabalin, gabapentin, and tricyclic antidepressants, which target the neuropathic component of chronic pancreatic pain (neural inflammation and perineural fibrosis are part of the pathology).
- Interventional and definitive therapy for refractory pain (see below). [1]
Pancreatic enzyme replacement for pain: enteric-coated enzymes may benefit a subset with small-duct, non-obstructive disease, thought to work by suppressing cholecystokinin-mediated pancreatic stimulation (negative feedback). They are not effective for the pain of large-duct obstructive disease, and they are never the sole analgesic. [1]
Antioxidants (selenium, beta-carotene, vitamin C, vitamin E, methionine) have modest and inconsistent evidence for pain reduction and are sometimes trialled. [1]
Interventional options when oral therapy fails:
- Coeliac plexus block (percutaneous or EUS-guided) — provides temporary relief in a subset; benefit is often short-lived.
- Thoracoscopic splanchnicectomy — division of the splanchnic nerves; reserved for carefully selected patients with refractory pain.
- Endoscopic therapy — ERCP with stent placement for a single dominant stricture with upstream duct dilatation, and pancreatic duct stone removal; extracorporeal shock wave lithotripsy (ESWL) is combined with ERCP to fragment large obstructing ductal calculi.
- Surgery — the definitive option for refractory pain and obstructive disease (see below). [1]
Pillar 2 — exocrine insufficiency
Pancreatic enzyme replacement therapy (PERT) with enteric-coated porcine pancreatin (Creon, Pancreatin) is the cornerstone. The meta-analysis by de la Iglesia-García confirmed that PERT significantly improves the coefficient of fat absorption (from about 67 per cent to 83 per cent), reduces faecal fat and nitrogen excretion, improves nutritional parameters, and improves quality of life [9].
Practical prescribing [3] [9]:
- Dose — 25,000 to 40,000 units of lipase with each main meal, and half that (about 10,000 to 25,000 units) with snacks.
- Timing — take during or immediately after food, never before, so the enzymes are present in the duodenum when chyme arrives.
- Acid suppression — add a proton pump inhibitor (omeprazole 20 mg, pantoprazole 40 mg) to protect the enzymes from gastric acid degradation and improve their efficacy. [1]- Titrate to symptoms — increase the dose until steatorrhoea and weight stabilise; a poor response should prompt a review of adherence and timing and consideration of a higher dose or acid suppression, not abandonment.
- Fat-soluble vitamin supplementation — vitamins A, D, E, and K, with bone density monitoring (DEXA) for osteoporosis and osteomalacia.
- Nutritional support — a diet with adequate calories and reduced fat (but not fat-free), with medium-chain triglycerides as a calorie source because they are absorbed directly without micellar solubilisation.
Pillar 3 — endocrine insufficiency — type 3c diabetes
Diabetes develops in 25 to 80 per cent of patients with chronic pancreatitis depending on duration and severity [5]. Type 3c (pancreatogenic) diabetes is distinct from type 2 because the gland loses both insulin-secreting beta cells and glucagon-secreting alpha cells. The consequences are clinically critical [5] [6]:
- The diabetes is brittle, with wide glucose excursions that are difficult to control.
- Hypoglycaemia is particularly dangerous because the loss of glucagon counter-regulation means there is no endogenous recovery from insulin-induced hypoglycaemia. Severe hypoglycaemia is a leading cause of death in type 3c diabetes.
- Insulin requirements may be lower than in type 2 (because of reduced insulin resistance), but the risk of hypoglycaemia is higher.
- Insulin is the mainstay of therapy. Metformin should generally be avoided in malnourished, exocrine-insufficient patients because of the risk of lactic acidosis and weight loss, though it may be considered early when insulin resistance coexists. Sulphonylureas risk hypoglycaemia and are rarely used.
- Pancreatic enzyme replacement improves glycaemic control by restoring nutrient absorption and reducing the mismatch between insulin and absorbed glucose. [1]
Every patient requires structured diabetes education, regular self-monitoring of blood glucose (with attention to hypoglycaemia), and a relaxed HbA1c target that prioritises avoidance of hypoglycaemia over tight control. [1]
DWE trap: The most common error is treating type 3c diabetes like type 2 — choosing metformin or sulphonylureas as first-line and targeting tight glycaemic control. Insulin is the mainstay, the diabetes is brittle, and hypoglycaemia avoidance (not tight control) is the priority. [1]
Pillar 4 — endoscopic and surgical therapy
Endoscopic and surgical therapy are reserved for refractory pain, obstructive complications, and the management of an inflammatory head mass or pseudocyst. The choice is individualised to the ductal anatomy and the presence of a mass [3] [10].
Endoscopic therapy (ERCP) is appropriate for:
- A single dominant ductal stricture with upstream dilatation — stent placement with serial exchange.
- Main duct stones — removal, often combined with ESWL to fragment large calculi.
- Biliary obstruction — biliary stenting for a fibrotic pancreatic head stricture causing cholestasis. [1]
Surgical options are chosen by the ductal anatomy and the presence of an inflammatory head mass:
- Puestow procedure (longitudinal pancreaticojejunostomy) — for a dilated main pancreatic duct (above 7 mm) with multiple strictures and stones; the duct is filleted open along its length and anastomosed to a Roux loop of jejunum to decompress the entire duct. It relieves pain by decompression but does not remove diseased parenchyma.
- Frey procedure — combines a longitudinal pancreaticojejunostomy with a coring out of the fibrotic pancreatic head, suited to an enlarged, diseased head with a dilated duct.
- Beger procedure (duodenum-preserving pancreatic head resection) — resects the diseased head while preserving the duodenum and biliary tree; favoured in Europe for an inflammatory head mass.
- Pancreaticoduodenectomy (Whipple) — reserved for an inflammatory head mass suspicious for or coexisting with pancreatic cancer, or where malignancy cannot be excluded preoperatively. [1]
The endoscopic-versus-surgical decision is informed by the landmark randomised trial by Cahen (NEJM 2007), which compared endoscopic transampullary drainage with operative pancreaticojejunostomy for obstructive chronic pancreatitis. Surgery provided superior durable pain relief (complete or partial relief in 75 per cent versus 32 per cent at two years; 80 per cent versus 38 per cent at five years) and better quality of life, with similar complication rates, although endoscopy required more repeat procedures [10]. The practical interpretation is that endoscopic therapy is a reasonable first step in selected patients (dominant stricture, limited disease, those unfit for surgery), but surgery offers superior long-term pain control in fit patients with obstructive dilated-duct disease. The decision is individualised and made in a multidisciplinary setting.
Complications
- Pseudocyst formation — differentiate from walled-off necrosis (which contains solid debris). Observe if asymptomatic; drain (endoscopic, percutaneous, or surgical) if symptomatic, infected, or persistently large (above 6 cm). Endoscopic cystgastrostomy is the usual approach for a mature, adherent collection.
- Biliary obstruction — a fibrotic pancreatic head or stricture compresses the common bile duct, causing cholestasis and jaundice. Manage with endoscopic biliary stenting or, for definitive management, surgical bypass or resection.
- Splenic vein thrombosis — chronic peripancreatic inflammation thromboses the splenic vein, producing left-sided (sinistral) portal hypertension with gastric and oesophageal varices (the gastric fundal varices are characteristic). When variceal bleeding occurs, splenectomy is curative because it removes the distal venous bed. This is a classic exam point.
- Pancreatic cancer — a long-term increased risk, addressed below.
- Malnutrition and osteoporosis — the consequences of chronic malabsorption: fat-soluble vitamin deficiency, osteomalacia and osteoporosis (monitor bone density), sarcopenia, and impaired quality of life.
- Duodenal obstruction — rarely, a fibrotic pancreatic head obstructs the duodenum, causing gastric outlet obstruction. [1]
Pancreatic cancer risk and surveillance
Chronic pancreatitis is a modest but real risk factor for pancreatic ductal adenocarcinoma. The systematic review and meta-analysis by Kirkegård (2017) found that the risk is highest in the first two years after diagnosis (effect estimate about 16, partly reflecting surveillance bias and undiagnosed cancer), remains elevated at five years (effect estimate about 8), and persists long-term at a lower level (effect estimate about 3.5 after nine or more years) [7].
Two principles follow. First, any change in symptoms in established chronic pancreatitis — new weight loss, a change in the pain pattern, or new jaundice — mandates investigation to exclude pancreatic cancer, because the two diseases coexist and mimic each other. An inflammatory head mass must be distinguished from carcinoma with Ca 19-9, EUS-fine-needle aspiration, and PET-CT where needed. Second, surveillance is selective, not universal. The American Gastroenterological Association and American Pancreatic Association recommend surveillance only for high-risk groups — principally hereditary pancreatitis (PRSS1), genetic syndromes, and selected familial clusters — because the absolute cancer risk in ordinary alcoholic chronic pancreatitis is too low to justify universal imaging. Smoking is the most important modifiable cofactor that magnifies the cancer risk and must be addressed [2].
DCE trap: A patient with chronic pancreatitis who develops a new, different pain pattern or unexplained weight loss has pancreatic cancer until proven otherwise. Never attribute a change in symptoms to a flare of chronic pancreatitis without imaging. [1]
Prognosis and quality of life
Chronic pancreatitis is an irreversible, progressive disease, and the prognosis is determined by four interacting factors: the underlying cause (alcohol and smoking drive the worst outcomes and the highest cancer risk), the adequacy of replacement therapy (enzyme and insulin), the success of pain control, and the avoidance of complications [3].
Mortality is increased two- to three-fold over the general population. The principal causes of death are, in rough order: pancreatic cancer, complications of type 3c diabetes (especially severe hypoglycaemia from loss of glucagon counter-regulation), malnutrition and its sequelae, cardiovascular disease (accelerated by diabetes and smoking), and continuing alcohol-related harm. Notably, the pain of early disease often burns out as the gland is destroyed — a pyrrhic victory, because the absence of late pain simply marks the progression to exocrine and endocrine failure [1].
Quality of life is dominated by chronic pain, opioid dependence, and the burden of a brittle, hypoglycaemia-prone diabetes. The most impactful interventions are often the simplest — sustained alcohol and smoking cessation, adequate and correctly timed pancreatic enzyme replacement with a proton pump inhibitor, and a pain strategy that avoids iatrogenic opioid use disorder. A multidisciplinary model (gastroenterology, endocrinology, pain medicine, dietetics, addiction medicine, and pancreatic surgery) is the standard of care [3].
Goals of care for the long case. In every patient, the physician should be able to state: the aetiology (TIGAR-O), the degree of exocrine insufficiency (faecal elastase, weight trend, fat-soluble vitamin status), the degree of endocrine insufficiency and the hypoglycaemia risk, the pain strategy and its opioid component, and the plan for cancer surveillance and complications. The realistic message to the patient is that the disease cannot be cured, but its progression can be slowed and its consequences managed. [1]
DCE integration point: A long-case candidate who presents a coherent four-pillar plan (pain, exocrine replacement, endocrine control, complications and surveillance), names the aetiology by TIGAR-O, justifies the endoscopic-versus-surgical decision with the Cahen evidence, and actively excludes pancreatic cancer will pass the pancreatitis long case comfortably. [1]
High-yield DWE points and exam traps
- Steatorrhoea appears only after 90 per cent of enzyme secretory capacity is lost. Early chronic pancreatitis presents with pain, not malabsorption.
- Alcohol is the cause in about 70 per cent; smoking is the key cofactor and independently increases both fibrosis and pancreatic cancer risk.
- Type 3c diabetes is brittle; insulin is the mainstay; hypoglycaemia is the danger. Avoid metformin in malnourished exocrine-insufficient patients.
- Faecal elastase is the best non-invasive marker but is insensitive in mild disease (sensitivity as low as 40 to 50 per cent). A normal result does not exclude exocrine insufficiency.
- Pancreatic calcification on plain X-ray is specific but present in only about 30 per cent. A normal film does not exclude chronic pancreatitis.
- EUS with the Rosemont criteria is the investigation of choice for early disease before calcification or ductal dilatation appears on CT.
- Autoimmune pancreatitis (type 1, IgG4-related) is the reversible exception. A sausage-shaped gland with capsule-like rim, elevated IgG4, and a dramatic steroid response should trigger the diagnosis — do not operate for presumed cancer.
- Tropical calcific pancreatitis — young, thin, non-drinker from southern India, large intraductal calculi, early severe insulin-requiring diabetes.
- Splenectomy is curative for gastric variceal bleeding from splenic vein thrombosis (left-sided portal hypertension).
- Surgery provides superior durable pain relief to endoscopy for obstructive dilated-duct disease (Cahen, NEJM 2007) — the endoscopic-versus-surgical decision is individualised in a multidisciplinary setting [10].
References and further reading
The HaPanEU (United European Gastroenterology) 2017 evidence-based guidelines are the current European reference standard for diagnosis and therapy [3]. The mechanistic definition (Whitcomb 2016) and the revised TIGAR-O classification (Majumder/Whitcomb 2019) provide the aetiological framework [1] [2]. The M-ANNHEIM criteria integrate aetiology, clinical course, and severity [4]. Type 3c diabetes is reviewed by Ewald and colleagues [5] [6]. Pancreatic cancer risk is quantified by Kirkegård (2017) [7]. Autoimmune pancreatitis is defined by the International Consensus Diagnostic Criteria (Shimosegawa 2011) [8]. Pancreatic enzyme replacement efficacy is established by the de la Iglesia-García meta-analysis (2017) [9]. The endoscopic-versus-surgical decision is informed by the Cahen randomised trial (NEJM 2007) [10].
References
- [1]Whitcomb DC, Frulloni L, Garg P, Greer JB, Schneider A, Yadav D, Shimosegawa T Chronic pancreatitis: An international draft consensus proposal for a new mechanistic definition Pancreatology, 2016.PMID 26924663
- [2]Majumder S, Gierisch LM, Bolinger JM, Arora M, Topazian M, Roberts K, Chari ST, Whitcomb DC, Yadav D Pancreatitis: TIGAR-O Version 2 Risk/Etiology Checklist With Topic Reviews, Updates, and Use Primers Clin Transl Gastroenterol, 2019.PMID 31166201
- [3]Löhr JM, Dominguez-Munoz E, Rosendahl J, Besselink M, Mayerle J, Junge F, ... HaPanEU/UEG Working Group United European Gastroenterology evidence-based guidelines for the diagnosis and therapy of chronic pancreatitis (HaPanEU) United European Gastroenterol J, 2017.PMID 28344786
- [4]Schneider A, Löhr JM, Singer MV The M-ANNHEIM classification of chronic pancreatitis: introduction of a unifying classification system based on a review of previous classifications of the disease J Gastroenterol, 2007.PMID 17351799
- [5]Ewald N, Hardt PD Diagnosis and treatment of diabetes mellitus in chronic pancreatitis World J Gastroenterol, 2013.PMID 24259958
- [6]Ewald N, Bretzel RG Diabetes mellitus secondary to pancreatic diseases (Type 3c)--are we neglecting an important disease? Eur J Intern Med, 2013.PMID 23375619
- [7]Kirkegård J, Mortensen FV, Cronin-Fenton D Chronic Pancreatitis and Pancreatic Cancer Risk: A Systematic Review and Meta-analysis Am J Gastroenterol, 2017.PMID 28762376
- [8]Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, Kim MH, Klöppel G, Ko SB, Lerch MM, Lohr M, Notohara K, Okazaki K, Schneider A, Webster LD, Yamaguchi T, Yoshida M, International Association of Pancreatology International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology Pancreas, 2011.PMID 21412117
- [9]de la Iglesia-García D, Huang W, Szatmary P, Baston-Rey I, González-López O, Alvarez-Castro A, González-Pérez C, NaIK W, Sabbagh L, Puga M, Macias-Garcia F, Whiston R, Larino-Noia J, Iglesias-Garcia J, de-Madaria E, Besselink M, Banks PA, Windsor JA, Duggan S, O'Suilleabhain C, Vazquez-Iglesias JL, Sans MD, Barthet M, Delhaye M, Deviere J, Dumonceau JM, Marra-Lopez C, Robles-Díaz M, Mariani A, Clain JE, Gleeson FC, Pelaez-Luna M, Capurso G, Perri F, Frulloni L, D'Onofrio M, Gabbrielli A, Zamboni G, Salvia R, Pederzoli P, Bassi C, Bocus P, Ciccotto F, Manfredi R, Costamagna G, Brighi N, Fusaroli P, Kamisawa T, Okamoto A, Kawa S, Hart PA, Chari ST, Gleeson F, Takahashi N, Vege SS, Kamisawa T, Lerch MM, Mayerle J Efficacy of pancreatic enzyme replacement therapy in chronic pancreatitis: systematic review and meta-analysis Gut, 2017.PMID 27941156
- [10]Cahen DL, Gouma DJ, Nio Y, Rauws EA, Boermeester MA, Busch OR, Stoker J, Lameris JS, Dijkgraaf MG, Huibregtse K, Bruno MJ Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis N Engl J Med, 2007.PMID 17301298