Phys · gastrointestinal
Colorectal Cancer
Also known as colorectal cancer · CRC · colon cancer · rectal cancer · bowel cancer · colorectal carcinoma · adenoma-carcinoma sequence · APC · KRAS · TP53 · microsatellite instability · Lynch syndrome · hereditary nonpolyposis colorectal cancer · HNPCC · familial adenomatous polyposis · FAP · faecal immunochemical test · FIT · total mesorectal excision · TME · FOLFOX · CAPOX · FOLFIRI · cetuximab · panitumumab · bevacizumab · pembrolizumab · CEA
Consultant-physician guide to colorectal cancer — the third most common cancer worldwide, whose prevention rests on the adenoma-carcinoma sequence and whose treatment hangs on TNM/Dukes staging. Covers the molecular pathway (APC, KRAS, TP53 and the microsatellite instability/Lynch pathway), risk factors (age, family history, IBD, diet, the hereditary syndromes), FIT-based screening and surveillance intervals, clinical presentation by tumour site, the surgical principles (colectomy with lymph node dissection, total mesorectal excision for rectal cancer), adjuvant chemotherapy by stage (FOLFOX/CAPOX for stage III, selective stage II), metastatic management (chemotherapy plus biologic by RAS/MSI status, metastasectomy, pembrolizumab for MSI-high), and the hereditary syndromes (Lynch, FAP, MUTYH, Peutz-Jeghers, juvenile polyposis). Structured for FRACP DWE and DCE, MRCP, and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Colorectal Cancer

The answer first
Colorectal cancer (CRC) is a malignancy of the colonic or rectal epithelium and the third most commonly diagnosed cancer worldwide and a leading cause of cancer death. Its central importance to a physician is that it is preventable and curable when caught early — and the entire field turns on two ideas: the adenoma-carcinoma sequence (cancer develops slowly from a benign polyp, so removing polyps prevents cancer), and stage-directed treatment (the depth of wall invasion and the nodal status determine surgery alone versus surgery plus chemotherapy). [1]
The single organising principle: CRC management is driven by the TNM stage and the molecular profile (RAS and MSI status). Know the staging and the molecular tests and you know CRC. Everything else — screening, the surgical approach, the chemotherapy backbone, the biologic — feeds into those two frameworks [2][3].
The treatment ladder, by stage: [1]
- Stage I and most stage II colon cancer — surgery alone is curative.
- High-risk stage II — selective adjuvant FOLFOX or CAPOX (small absolute benefit).
- Stage III (node-positive) — surgery then adjuvant FOLFOX or CAPOX for 3 to 6 months (the MOSAIC and IDEA data).
- Locally advanced rectal cancer (T3/T4 or node-positive) — neoadjuvant chemoradiotherapy or short-course radiotherapy, then total mesorectal excision (TME).
- Metastatic (stage IV) — palliative chemotherapy (FOLFOX or FOLFIRI) plus a biologic chosen by RAS status (anti-EGFR for RAS wild-type, bevacizumab for any), with first-line pembrolizumab for MSI-high disease and metastasectomy when disease is resectable. [1]
DWE high-yield: The answer to almost every CRC management question is "stage the tumour with TNM and test the molecular profile (RAS, BRAF, MMR/MSI)." Stage I and II colon cancer: surgery. Stage III: surgery then FOLFOX or CAPOX. Rectal cancer: neoadjuvant chemoradiotherapy then TME. Metastatic and RAS wild-type: chemotherapy plus cetuximab or panitumumab. Metastatic and MSI-high: first-line pembrolizumab [6][8][10].
Epidemiology and the preventable cancer
CRC is the third most commonly diagnosed cancer worldwide and the second leading cause of cancer death. Global estimates for 2022 recorded approximately 1.9 million new cases and 900 000 deaths, with the burden rising in low- and middle-income countries adopting a Western lifestyle and in younger adults in high-income countries [1].
The age-standardised incidence is highest in Australasia, Europe, and North America — populations with diets high in red and processed meat, lower fibre intake, higher rates of obesity, and sedentary lifestyles. The most important epidemiological fact for the physician is the rising incidence in adults under 50, which has prompted several countries (including the United States) to lower the average-risk screening start age to 45. [1]
Risk factors
| Risk factor | Mechanism / magnitude |
|---|---|
| Age above 50 | The strongest risk factor — over 90 percent of cases occur after age 50, though young-onset CRC is rising |
| Family history | One first-degree relative roughly doubles the risk; the risk is higher the younger the relative was at diagnosis |
| Hereditary syndromes | Lynch syndrome (3 to 5 percent of all CRC), FAP (1 percent), MUTYH-associated polyposis, Peutz-Jeghers, juvenile polyposis |
| Inflammatory bowel disease | Long-standing (over 8 years) extensive ulcerative colitis and Crohn's colitis — colitis-associated CRC via inflammation-driven dysplasia |
| Diet — red and processed meat | Heterocyclic amines and N-nitroso compounds; processed meat is a Group 1 carcinogen (IARC) |
| Low dietary fibre | Reduced stool bulk and transit time increases mucosal contact with carcinogens |
| Smoking and alcohol | Both increase CRC risk in a dose-dependent manner |
| Obesity and physical inactivity | Insulin resistance, hyperinsulinaemia, and chronic inflammation |
| Type 2 diabetes | Shared metabolic risk factors; CRC incidence is increased |
| Prior abdominal radiation | A weaker but recognised risk factor |
| Acromegaly / ureterosigmoidostomy | Rare but classic associations |
DWE trap: A family history of a single affected relative does not automatically mean a hereditary syndrome — but it does move the patient into a higher-risk screening category (colonoscopy from age 40, or 10 years before the relative's age at diagnosis). The hereditary syndromes have specific patterns: Lynch (early-onset, right-sided, mismatch repair loss), FAP (hundreds of polyps, APC mutation). [1]
Pathogenesis — the adenoma-carcinoma sequence
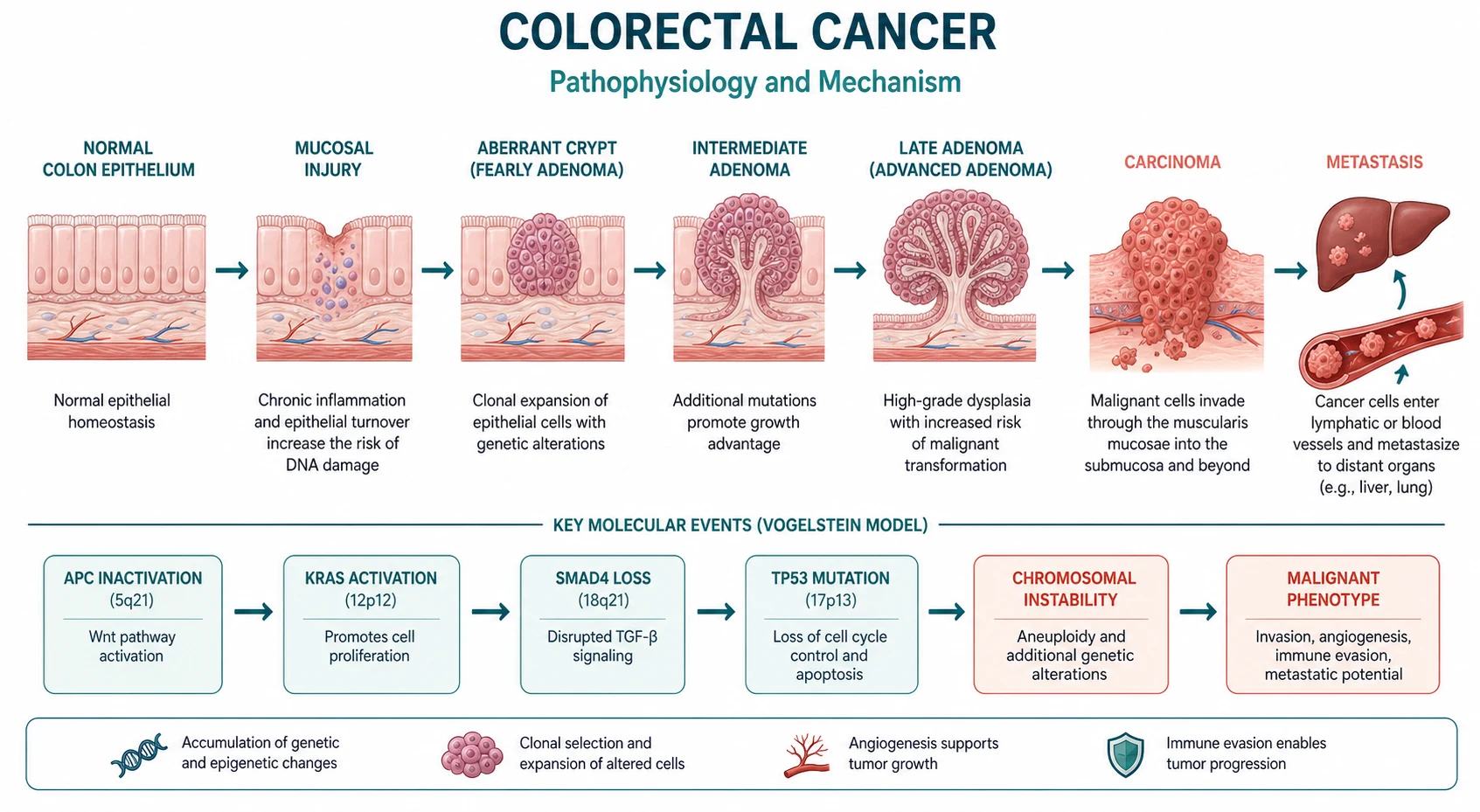
The dominant model of colorectal carcinogenesis is the adenoma-carcinoma sequence, formalised by Fearon and Vogelstein in 1990 [2]. Most colorectal cancers do not arise de novo; they develop slowly from a benign adenomatous polyp over 10 to 15 years, through the stepwise accumulation of genetic alterations. This long window is the biological basis for screening and polypectomy — find and remove the adenoma, and you prevent the cancer.

The classic chromosomal instability pathway
The sequence proceeds through characteristic molecular hits, in roughly this order (though the total accumulation matters more than the exact sequence): [1]
-
APC loss (chromosome 5q) — the gatekeeper. Loss of the APC tumour suppressor is the initiating event in most sporadic CRC and the inherited defect in familial adenomatous polyposis. APC normally degrades beta-catenin in the Wnt signalling pathway; without it, beta-catenin accumulates and drives uncontrolled crypt cell proliferation. The result is an early adenoma. [1]
-
KRAS mutation — the oncogenic driver. An activating KRAS mutation (about 40 percent of CRC) turns on proliferative signalling (MAPK pathway), driving the adenoma from a small tubular adenoma to a larger, more dysplastic intermediate adenoma. KRAS mutation also predicts resistance to anti-EGFR antibodies (cetuximab, panitumumab), which is why RAS testing is mandatory before using these drugs [8].
-
Chromosome 18 loss (SMAD4/DCC) — progression. Loss of tumour suppressors on 18q drives the adenoma toward higher-grade dysplasia. [1]
-
TP53 loss (chromosome 17p) — the malignant transition. Loss of p53, the guardian of the genome, permits the late adenoma to breach the basement membrane and become an invasive carcinoma. This is the defining step from adenoma to cancer. [1]
The microsatellite instability (MSI) pathway
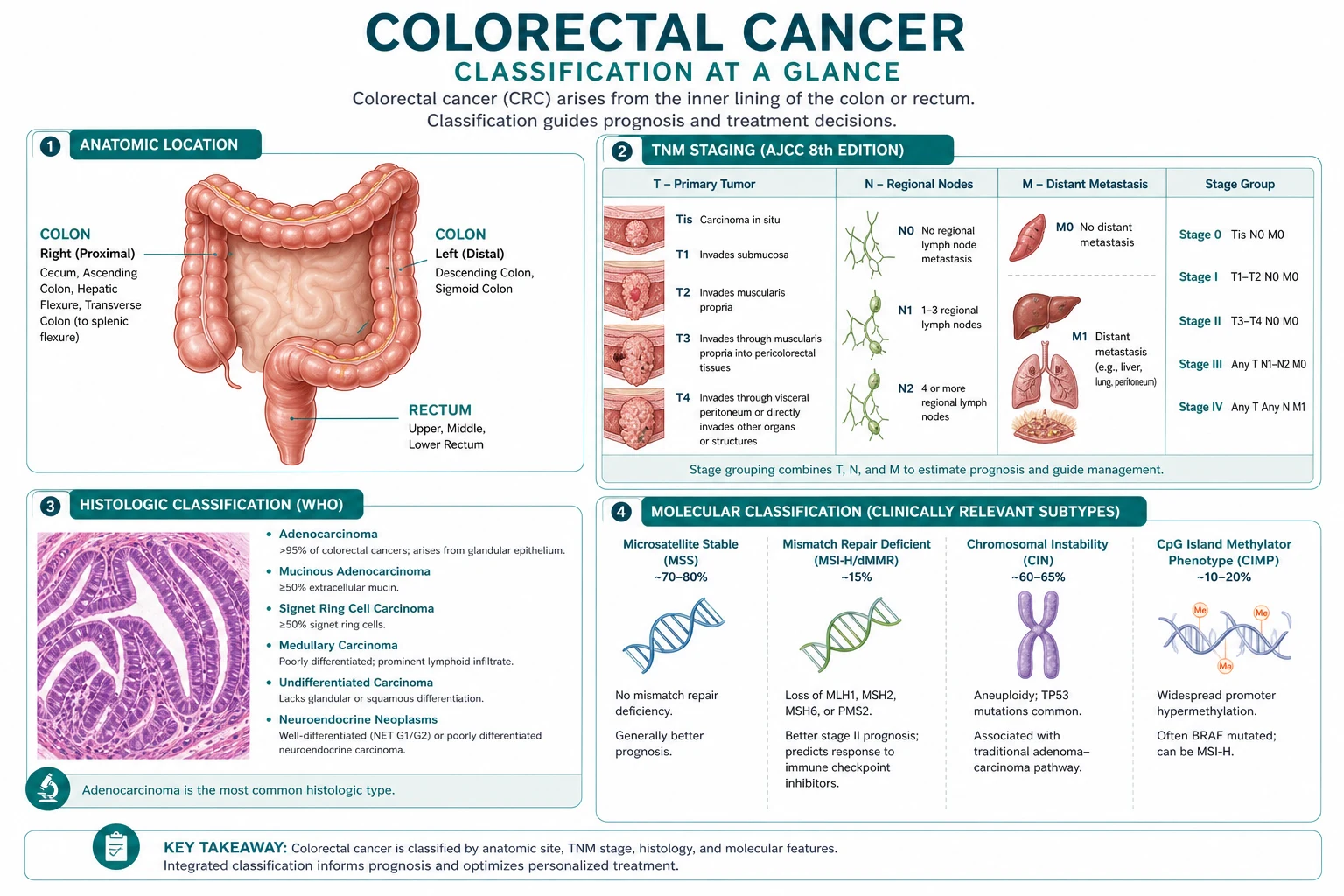
A separate carcinogenesis route produces about 15 percent of CRC through defective DNA mismatch repair (MMR) [3]. The MMR system corrects single-base mismatches and short insertion-deletion loops that arise during DNA replication. When MMR is lost, errors accumulate preferentially in microsatellites — short repetitive DNA sequences — producing microsatellite instability (MSI).
MSI arises in two ways: [1]
- Germline (Lynch syndrome, 3 percent of CRC): an inherited mutation in one of the MMR genes — MLH1, MSH2, MSH6, PMS2, or a deletion in EPCAM (which silences MSH2). The patient is born with one defective copy; loss of the remaining copy in a colonic cell disables MMR and accelerates carcinogenesis. Lynch cancers are often right-sided, early-onset, and have a better stage-for-stage prognosis but a high rate of synchronous and metachronous tumours.
- Sporadic (12 percent of CRC): acquired hypermethylation of the MLH1 promoter, usually in the setting of the CpG island methylator phenotype (CIMP) and a BRAF mutation, arising from a sessile serrated lesion (the serrated pathway). Sporadic MSI-high tumours are not inherited. [1]
The clinical importance of MSI is threefold: it screens for Lynch syndrome (with cascade family testing), it is a favourable prognostic factor (MSI-high tumours have better stage-adjusted survival), and it is a predictive marker for immunotherapy — MSI-high tumours carry a high tumour mutational burden, generate neoantigens, and respond dramatically to checkpoint blockade [10].
DWE high-yield — test MMR and MSI on every new colorectal cancer. Universal testing is now standard: immunohistochemistry for the four MMR proteins (loss of one or more = dMMR) and/or PCR/next-generation sequencing for MSI. This single test screens for Lynch syndrome, informs prognosis, and identifies candidates for pembrolizumab. Omitting it is a serious and common error [3].
Screening — finding the polyp before it becomes cancer
Screening works because the adenoma-carcinoma sequence gives a 10 to 15 year window in which a polyp can be found and removed before it turns into cancer, or a cancer can be found at a curable stage. The landmark Minnesota trial established that annual faecal occult blood testing reduced CRC mortality by 33 percent at 13 years [4]. Modern screening has moved to the more sensitive and specific faecal immunochemical test (FIT).
Who, how, and how often
| Risk group | Screening strategy |
|---|---|
| Average risk (age 50 and over, no family history) | FIT every 1 to 2 years from age 50 (ANZ and UK); the US lowered the start age to 45. Colonoscopy every 10 years is an alternative direct-screening option |
| One first-degree relative with CRC at age 60 or over | Colonoscopy every 5 years from age 40 (or 10 years before the relative's age at diagnosis) |
| One first-degree relative with CRC before age 60, or two relatives | Colonoscopy every 5 years from age 40 (or 10 years before the earliest diagnosis), or age 30 for some guidelines |
| Lynch syndrome | Colonoscopy every 1 to 2 years from age 20 to 25 (or 2 to 5 years before the earliest family cancer) |
| Familial adenomatous polyposis (FAP) | Flexible sigmoidoscopy annually from age 10 to 12 (puberty); switch to colonoscopy once polyps appear |
| MUTYH-associated polyposis | Colonoscopy every 1 to 2 years from age 18 (homozygotes) or 25 to 30 (heterozygotes) |
| Inflammatory bowel disease (extensive UC/Crohn's colitis for over 8 years) | Surveillance colonoscopy with chromoendoscopy and targeted biopsies every 1 to 2 years for dysplasia |
The faecal immunochemical test (FIT)
FIT uses an antibody against human haemoglobin to detect occult blood in stool. It has higher sensitivity than the older guaiac-based FOBT (which required dietary restriction and was less specific for human blood), and it requires only a single small stool sample with no diet or medication changes. A positive FIT prompts colonoscopy. A quantitative FIT threshold also allows risk-stratified referral. [1]
When screening finds a polyp — surveillance
After polypectomy, surveillance colonoscopy intervals depend on the polyp findings, balancing the risk of metachronous neoplasia against the harm of repeated procedures: [1]
| Finding at colonoscopy | Surveillance interval |
|---|---|
| Low-risk adenoma (1 to 2 small tubular adenomas under 10 mm) | 5 years |
| High-risk adenoma (3 or more adenomas, any adenoma 10 mm or larger, or villous histology / high-grade dysplasia) | 3 years |
| Sessile serrated lesion or piecemeal resection | 3 to 6 months (incomplete resection) then 1 to 3 years |
| No adenoma (hyperplastic polyps only) | Return to routine screening (10 years) |
DWE high-yield: Low-risk adenoma = 5-year surveillance; high-risk adenoma (3 or more, or 10 mm or larger, or villous) = 3-year surveillance. These intervals are among the most frequently tested facts in gastroenterology exams. Over-surveillance is a common real-world error that consumes resource and increases procedural harm. [1]
The NordICC trial — colonoscopy screening in perspective
The NordICC trial randomised over 84 000 Europeans aged 55 to 64 to an invitation for a once-only screening colonoscopy versus no screening [5]. At 10 years, the intention-to-screen analysis showed an 18 percent reduction in CRC incidence, with no statistically significant mortality reduction — a sobering result driven by low uptake (42 percent of those invited actually had the colonoscopy) and the relatively short follow-up. The per-protocol analysis (those who actually underwent colonoscopy) showed a 31 percent incidence reduction and a 50 percent mortality reduction. The lesson: colonoscopy works when it is performed to a high standard and the patient actually has it, but population-level effectiveness depends on uptake. FIT-based programmes achieve higher participation.
Clinical presentation — the site changes the symptom
The presentation of CRC is determined by the tumour site. The colon is a tube; a tumour in the liquid-content right colon behaves differently from a tumour in the solid-stool left colon or rectum. [1]
| Site | Classic presentation |
|---|---|
| Right colon (caecum, ascending) | Iron deficiency anaemia from chronic occult bleeding, vague right-sided abdominal discomfort, a palpable right iliac fossa mass, weight loss, fatigue. Bleeding is dark and mixed with stool, often unnoticed |
| Left colon (descending, sigmoid) | Change in bowel habit (increasing constipation, alternating constipation and diarrhoea, pencil-thin stools), obstructive symptoms (colicky pain, distension), visible dark red blood mixed with stool |
| Rectum | Fresh rectal bleeding (bright red, often on the surface of the stool or on toilet paper), tenesmus, a sensation of incomplete evacuation, mucus per rectum. Palpable on digital rectal examination |
The red flags that demand urgent investigation (colonoscopy): new rectal bleeding over age 40; iron deficiency anaemia in an older man or postmenopausal woman; a persistent change in bowel habit (looser stools or increased frequency) for over 6 weeks in a patient over 50 (any age if accompanied by weight loss); a palpable abdominal or rectal mass; unexplained weight loss with bowel symptoms. [1]
DWE trap: The single most dangerous habit is attributing rectal bleeding to haemorrhoids without examining or scoping. Haemorrhoids are common and coexist with cancer; any new bleeding in a patient over 40 (or with alarm features) is cancer until proven otherwise. Equally, iron deficiency anaemia in an older adult is colorectal cancer until excluded — never simply prescribe iron without investigating the source. [1]
Diagnosis and staging
Colonoscopy — the diagnostic standard
Colonoscopy with biopsy is the gold standard: it visualises the entire colon, obtains tissue for histology, and can resect polyps therapeutically. A complete examination to the caecum (documented by photo of the appendiceal orifice and ileocaecal valve) is required, because synchronous lesions occur in up to 5 percent. If colonoscopy is incomplete or contraindicated, CT colonography (virtual colonoscopy) is the alternative. [1]
Baseline bloods and tumour marker
A full blood count identifies anaemia; iron studies confirm iron deficiency. Liver function tests may suggest liver metastases. Serum CEA (carcinoembryonic antigen) is measured at baseline — it is not a diagnostic test (it can be normal in CRC and elevated in non-malignant disease, especially smoking and liver disease), but it is invaluable for monitoring treatment response and detecting recurrence after curative surgery. A rising CEA post-resection prompts cross-sectional imaging for recurrence. [1]
Staging scans
- CT chest-abdomen-pelvis is the standard staging scan — assessing local invasion, regional nodes, and distant metastases (liver, lung, peritoneum).
- MRI pelvis is mandatory for rectal cancer — it defines the depth of invasion through the muscularis propria (T stage), the distance to the mesorectal fascia (which predicts whether the circumferential resection margin will be clear), and involvement of the sphincter complex and pelvic sidewall. The MRI drives the neoadjuvant decision. [1]
Molecular testing — non-negotiable on every new CRC
Every colorectal cancer must have: [1]
- MMR status by immunohistochemistry and/or MSI by PCR/NGS — screens for Lynch syndrome and identifies immunotherapy candidates [3].
- KRAS, NRAS, and BRAF mutation analysis — determines eligibility for anti-EGFR therapy (cetuximab, panitumumab), which only works in RAS wild-type tumours [8]. BRAF mutation (V600E) is a poor prognostic marker and, in metastatic disease, opens the option of combined BRAF plus EGFR inhibition.

TNM and Dukes staging
The TNM system (tumour depth, nodes, metastasis) is the modern staging language. The older Dukes classification persists in exams and clinical shorthand: [1]
| TNM | Description | Dukes equivalent |
|---|---|---|
| T1 | Tumour invades submucosa | — |
| T2 | Tumour invades muscularis propria | — |
| T3 | Tumour invades through muscularis propria into subserosa or pericolic fat | Dukes B (if node-negative) |
| T4 | Tumour penetrates visceral peritoneum or invades adjacent organs | Dukes B |
| N0 | No regional lymph node metastasis | — |
| N1 | 1 to 3 regional nodes | Dukes C |
| N2 | 4 or more regional nodes | Dukes C |
| M0 | No distant metastasis | — |
| M1 | Distant metastasis | Dukes D |
In Dukes terms: A = limited to the bowel wall (muscularis propria), node-negative; B = through the wall, node-negative; C = any depth with node positivity; D = distant metastases. Stage groupings combine these into the familiar stage I (T1-T2 N0), stage II (T3-T4 N0), stage III (any T N1-N2), and stage IV (M1) that drive treatment. [1]
Surgical management
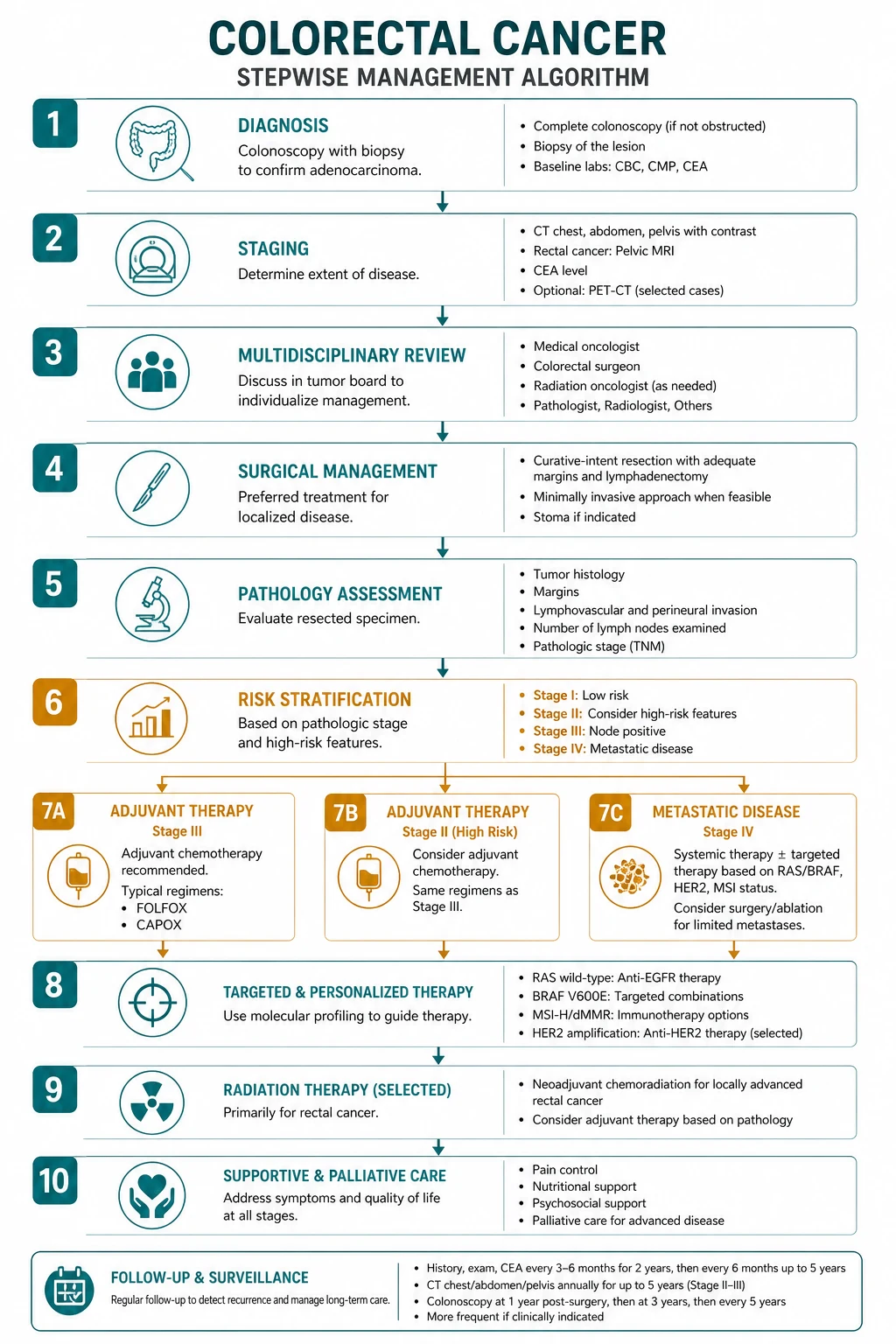
Surgery is the cornerstone of curative treatment for non-metastatic CRC. The oncological principle is an en-bloc resection of the tumour-bearing segment of bowel together with its mesentery and draining lymph nodes (at least 12 nodes must be examined for accurate staging), with high ligation of the feeding vessels. [1]
Colon cancer
The operation depends on the tumour site: right hemicolectomy (caecum, ascending colon, hepatic flexure) with ligation of the ileocolic and right colic vessels; extended right hemicolectomy for transverse colon lesions; left hemicolectomy (descending colon) or sigmoid colectomy with ligation of the inferior mesenteric vessels. Primary anastomosis is usually possible. [1]
Laparoscopic (minimally invasive) colectomy is oncologically equivalent to open surgery for colon cancer, with faster recovery, less pain, and shorter stay — it is now the default for suitable cases. [1]
Rectal cancer — total mesorectal excision (TME)
For rectal cancer, the surgical standard is total mesorectal excision — sharp dissection in the avascular mesorectal plane that removes the rectum and its enveloping mesorectum (containing the lymphatic drainage) as an intact specimen. TME, pioneered by Heald, dramatically reduced local recurrence from over 20 percent to under 10 percent by ensuring a clear circumferential resection margin. The MRI-defined threatened mesorectal fascia is the trigger for neoadjuvant therapy to shrink the tumour away from that margin. [1]
Whether the sphincters can be preserved determines whether the patient has an anterior resection (with a colo-anal anastomosis) or an abdominoperineal excision of rectum (APER) with a permanent end colostomy. A low anastomosis is typically protected by a temporary defunctioning loop ileostomy to reduce the consequence of an anastomotic leak. [1]
Emergency surgery — obstruction and perforation
A left-sided CRC is the commonest cause of malignant large bowel obstruction. The emergency options are a self-expanding metal stent (as a bridge to elective surgery in a fit patient, or for palliation), a Hartmann's procedure (resection with an end colostomy and a rectal stump), or resection with primary anastomosis in a selected, stable patient. Perforation with peritonitis mandates emergency laparotomy, resection, and usually a stoma. Caecal blowout — ischaemic perforation proximal to an obstructing distal tumour — is a feared, high-mortality presentation. [1]

Adjuvant and neoadjuvant therapy
Stage III colon cancer — adjuvant FOLFOX or CAPOX
Stage III (node-positive) colon cancer benefits from adjuvant chemotherapy after resection. The standard is an oxaliplatin plus fluoropyrimidine doublet — either FOLFOX (oxaliplatin, leucovorin, infusional 5-FU every 2 weeks) or CAPOX (oxaliplatin plus oral capecitabine every 3 weeks). The MOSAIC trial established that adding oxaliplatin to fluorouracil and leucovorin improved disease-free and overall survival in stage III disease — 5-year DFS 73.3 percent with FOLFOX4 versus 67.4 percent with LV5FU2 [6].
The IDEA collaboration pooled six trials (over 12 800 patients) comparing 3 versus 6 months of oxaliplatin-based adjuvant therapy. The overall result was non-inferiority borderline; in practice, 3 months is preferred for low-risk stage III (T1-T3 N1) and 6 months for high-risk stage III (T4 or N2), trading the lower neuropathy of the shorter course against the marginal efficacy gain of the longer course. [1]
Stage II colon cancer — selective adjuvant therapy
The overall benefit of adjuvant chemotherapy in stage II colon cancer is small (an absolute survival benefit of 3 to 5 percent at best), and routine treatment is not recommended. Adjuvant FOLFOX or CAPOX is offered selectively to patients with high-risk features: T4 tumour, fewer than 12 lymph nodes examined, bowel perforation or obstruction, poorly differentiated histology, lymphovascular or perineural invasion. The MOSAIC subgroup analysis showed no overall survival benefit in stage II but a signal in high-risk subsets [6]. The decision must be shared with the patient, honestly disclosing the small absolute benefit against oxaliplatin neuropathy.
Rectal cancer — neoadjuvant chemoradiotherapy
For locally advanced rectal cancer (T3/T4 or node-positive), preoperative (neoadjuvant) chemoradiotherapy is the standard. The German CAO/ARO/AIO-94 trial established neoadjuvant over postoperative chemoradiotherapy: preoperative treatment improved local control (10-year local relapse 7.1 percent versus 10.1 percent), was better tolerated, and enabled more sphincter-preserving surgery, with no difference in overall survival [9].
The two neoadjuvant approaches are long-course chemoradiotherapy (45 to 50 Gy over 5 weeks with concurrent capecitabine or 5-FU, then surgery after 6 to 8 weeks) and short-course radiotherapy (25 Gy in 5 fractions, then surgery within a week, or with a delayed interval). For early, favourable rectal cancer, surgery alone or total neoadjuvant therapy then a watch-and-wait (non-operative) approach after a clinical complete response is an emerging option. [1]
Total neoadjuvant therapy (TNT)
Giving all the chemotherapy and chemoradiotherapy before surgery (rather than some after) is now preferred for high-risk rectal cancer, based on the RAPIDO and PRODIGE 23 trials, which improved disease-free survival and distant metastasis rates compared with standard chemoradiotherapy then surgery then adjuvant chemotherapy. TNT delivers the systemic treatment earlier, tackling micrometastatic disease and improving compliance. [1]
Metastatic disease — chemotherapy, biologics, and immunotherapy
Metastatic (stage IV) CRC is treated with palliative combination chemotherapy plus a biologic agent, with curative-intent metastasectomy for selected patients with limited, resectable disease. [1]
The chemotherapy backbone
The two interchangeable first-line doublets are FOLFOX (oxaliplatin-based) and FOLFIRI (irinotecan-based), both built on infusional 5-FU and leucovorin. They have equivalent efficacy, so the choice is often driven by toxicity and the plan for later lines (using oxaliplatin first then irinotecan on progression, or vice versa). CAPOX (capecitabine plus oxaliplatin) is an oral alternative. A single-agent fluoropyrimidine (capecitabine or 5-FU) is reasonable for a frail patient. [1]
Biologic selection — by RAS status
The biologic added to the chemotherapy doublet depends on the RAS mutation status: [1]
- RAS wild-type tumours can receive an anti-EGFR antibody — cetuximab (chimeric) or panitumumab (fully human) — added to FOLFOX or FOLFIRI. The Karapetis / CO.17 analysis established that cetuximab benefits only patients with KRAS wild-type tumours (median OS 9.5 versus 4.8 months with best supportive care); patients with KRAS-mutant tumours derive no benefit [8]. Anti-EGFR therapy works best in left-sided (distal to the splenic flexure) RAS/BRAF wild-type tumours. The characteristic toxicity is an acneiform rash, the severity of which correlates with efficacy.
- RAS mutant (or any status) tumours can receive bevacizumab, an anti-VEGF antibody, which works independently of RAS status. The Hurwitz trial (IFL plus bevacizumab versus IFL plus placebo) showed improved overall survival (median 20.3 versus 15.6 months), establishing anti-angiogenic therapy in first-line metastatic CRC [7]. Bevacizumab toxicities are hypertension, proteinuria, bleeding, thromboembolism, and impaired wound healing (hold before elective surgery).
Immunotherapy for MSI-high metastatic CRC
For the 15 percent of metastatic CRC with MSI-high or mismatch repair-deficient biology, first-line pembrolizumab (anti-PD-1) transformed outcomes. The KEYNOTE-177 trial randomised 307 patients with previously untreated MSI-high/dMMR metastatic CRC to pembrolizumab versus investigator's choice chemotherapy (FOLFOX or FOLFIRI plus a biologic): pembrolizumab nearly doubled median progression-free survival (16.5 versus 8.2 months; HR 0.60) with a far better toxicity profile (grade 3 to 4 adverse events 22 percent versus 66 percent) [10]. MSI-high tumours are exquisitely sensitive to checkpoint blockade because their high mutational burden generates abundant neoantigens that the immune system can attack once PD-1 inhibition releases the brakes. This is one of the great recent wins in precision oncology.
Metastasectomy — the curative option in stage IV
Selected patients with limited, resectable liver or lung metastases can be cured by metastasectomy, often after chemotherapy to shrink the disease. Five-year survival after complete resection of colorectal liver metastases is 30 to 50 percent. The criteria for resectability have broadened: the goal is complete (R0) resection of all disease with an adequate liver remnant, regardless of the number or size of metastases. This means no patient with metastatic CRC should be labelled "palliative only" without assessment by a hepatobiliary or thoracic MDT. [1]
Later-line and refractory options
For disease refractory to first and second-line therapy, options include regorafenib (a multi-kinase inhibitor), TAS-102 (trifluridine/tipiracil, an oral nucleoside combination), and, for BRAF V600E-mutant metastatic CRC, encorafenib plus cetuximab. These confer a modest but real survival benefit. [1]
Hereditary syndromes — recognise, test, and cascade-screen
About 5 to 10 percent of CRC is hereditary. Recognising a syndrome changes the patient's surveillance and treatment and triggers cascade genetic testing of at-risk relatives. [1]
Lynch syndrome (HNPCC)
Lynch syndrome (formerly hereditary nonpolyposis colorectal cancer, HNPCC) is the commonest hereditary CRC syndrome, caused by a germline mutation in a mismatch repair gene — MLH1, MSH2, MSH6, PMS2, or an EPCAM deletion that silences MSH2. It is autosomal dominant with high penetrance. Lynch cancers arise (unlike FAP) from few or no polyps, are often right-sided and early-onset (median age around 45), and are associated with extra-colonic cancers — endometrial (the commonest extra-colonic), ovarian, gastric, urothelial, small bowel, hepatobiliary, brain, and sebaceous. [1]
The Amsterdam II criteria (the "3-2-1-1" rule) identify families likely to have Lynch: 3 or more relatives with a Lynch-associated cancer, 2 or more successive generations affected, 1 or more diagnosed under age 50, with 1 a first-degree relative of the other two. The revised Bethesda guidelines are broader and guide which tumours to test for MSI. But the modern standard is universal MMR/MSI testing of every new CRC — which catches Lynch regardless of family history or age [3].
Management: colonoscopy every 1 to 2 years from age 20 to 25; aspirin (the CAPP2 trial showed a reduction in CRC incidence); risk-reducing hysterectomy and bilateral salpingo-oophorectomy for women after family completion; and cascade testing of first-degree relatives (each has a 50 percent chance of carrying the mutation). [1]
Familial adenomatous polyposis (FAP)
FAP is caused by a germline mutation in the APC gene on chromosome 5q (the gatekeeper of the adenoma-carcinoma sequence). Affected individuals develop hundreds to thousands of adenomatous polyps from adolescence; without intervention, CRC is virtually inevitable by age 40. The management is annual flexible sigmoidoscopy from age 10 to 12 (puberty), switching to colonoscopy once polyps appear, and prophylactic colectomy in the late teens to early twenties — typically a restorative proctocolectomy or colectomy with ileorectal anastomosis. Patients need lifelong surveillance of the rectal or pouch remnant, duodenal surveillance (duodenal adenomas and cancer are the leading cause of death after colectomy), and screening for desmoid tumours. Attenuated FAP (AFAP) has fewer polyps (under 100), a later onset, and a more right-sided distribution. [1]
MUTYH-associated polyposis
An autosomal recessive polyposis syndrome from biallelic MUTYH mutations, causing tens to hundreds of adenomas and a CRC risk of around 80 percent by age 70. Surveillance colonoscopy begins at age 18 (homozygotes) or 25 to 30 (heterozygotes). [1]
Peutz-Jeghers syndrome
An autosomal dominant STK11 (LKB1) mutation causing mucocutaneous pigmentation (lips, buccal mucosa, fingers) and hamartomatous gastrointestinal polyps. There is a markedly increased risk of CRC and of cancers throughout the GI tract, breast, ovary (sex cord tumour with annular tubules), pancreas, and testis (Sertoli cell tumours). Surveillance is multi-organ and begins in adolescence. [1]
Juvenile polyposis syndrome
An autosomal dominant syndrome (SMAD4 or BMPR1A mutations) of multiple juvenile (hamartomatous) polyps in the colon and throughout the GI tract, with an increased CRC risk. Surveillance colonoscopy begins in the early teens; prophylactic colectomy is considered for a heavy polyp burden. [1]
DWE high-yield: The hereditary syndromes are distinguished by polyp type and count and by the inheritance pattern. FAP: hundreds to thousands of adenomas, APC, autosomal dominant, prophylactic colectomy. Lynch: few polyps, MMR gene loss, right-sided early cancers, universal MSI testing. MUTYH: autosomal recessive, tens of adenomas. Peutz-Jeghers: hamartomas with mucocutaneous pigmentation. Juvenile polyposis: hamartomas, SMAD4/BMPR1A. [1]
Follow-up and surveillance after curative treatment
After curative-intent resection, surveillance aims to detect resectable recurrence (local or metastatic). A typical programme for stage II and III disease is: [1]
- Review and CEA every 3 to 6 months for 2 years, then 6-monthly to 5 years.
- CT chest-abdomen-pelvis annually for 3 to 5 years.
- Surveillance colonoscopy at 1 year post-resection (to clear anastomotic and synchronous lesions), then at 3 years, then every 5 years (or per Lynch/polyposis protocol if hereditary). [1]
A rising CEA post-resection, in the absence of symptoms, prompts cross-sectional (and sometimes PET) imaging to localise recurrence, with a view to resection if disease is limited. Surveillance is tapered for patients in whom recurrence would not change management (frailty, comorbidity). [1]
Prognosis
CRC prognosis depends on the stage at diagnosis and the treatment received. The five-year survival figures are high-yield: [1]
| Stage (TNM group) | Five-year survival |
|---|---|
| Stage I (T1-T2 N0 M0) | Around 90 percent |
| Stage IIA (T3 N0) | Around 87 percent |
| Stage IIB/IIC (T4 N0) | 63 to 73 percent |
| Stage IIIA (T1-T2 N1) | Around 88 percent |
| Stage IIIB | 64 to 78 percent |
| Stage IIIC | Around 48 percent |
| Stage IV (metastatic) | Around 14 percent (median OS on modern therapy 24 to 36 months) |
Prognosis is modified by molecular profile — MSI-high tumours have a better stage-adjusted prognosis but respond less to single-agent 5-FU; BRAF V600E mutation is a poor prognostic marker in metastatic disease; RAS mutation does not, by itself, worsen prognosis but removes the anti-EGFR option. The site matters: left-sided tumours (splenic flexure to rectum) have a better prognosis and respond better to anti-EGFR therapy than right-sided tumours, which are more often MSI-high and BRAF-mutant. [1]
The common exam traps
- Attributing rectal bleeding to haemorrhoids without examining or scoping — any new bleeding over 40 (or with alarm features) is cancer until proven otherwise.
- Missing iron deficiency anaemia as the presentation of a right-sided colon cancer — investigate the source; do not simply prescribe iron.
- Giving anti-EGFR antibodies to a RAS-mutant tumour — they only work in RAS wild-type disease; test RAS before use [8].
- Failing to test MMR/MSI on every new CRC — universal testing screens for Lynch, informs prognosis, and identifies immunotherapy candidates [3][10].
- Over-treating stage II colon cancer — only high-risk stage II benefits from adjuvant chemotherapy; routine stage II treatment is an error.
- Using postoperative (adjuvant) chemoradiotherapy for rectal cancer when neoadjuvant is standard — the German trial established preoperative treatment for better local control [9].
- Confusing Dukes with TNM — Dukes A (wall, node-negative), B (through wall, node-negative), C (node-positive), D (metastatic); know both systems.
- Defaulting all metastatic CRC to palliation — selected patients with resectable liver or lung metastases can be cured by metastasectomy; assess in an MDT.
- Missing Lynch syndrome — Amsterdam/Bethesda identify who to test; universal MSI testing is now the standard; a CRC under 50, synchronous or metachronous Lynch-associated cancers, or a suggestive family history must trigger testing and cascade screening of relatives.
- Stopping surveillance colonoscopy too soon or too often — follow the polyp-based intervals (low-risk 5 years, high-risk 3 years); over-surveillance causes harm.
Regional guideline anchoring
- ANZ (Cancer Council Australia, Cancer Council NHMRC) — FIT-based screening biennially for the average-risk population from age 50 (the National Bowel Cancer Screening Program); colonoscopy for positive FIT and for increased-risk groups; MDT management; surveillance per the polyp and cancer guidelines.
- UK (NICE NG151, UK Bowel Cancer Screening Programme) — biennial FIT from age 60 (lowering to 50); quantitative FIT to triage suspected-cancer referrals; colonoscopy for positive FIT; two-week-wait referral pathways for symptomatic patients.
- US (USPSTF, USMSTF, NCCN) — screening from age 45 for average risk (USPSTF 2021, grade B); FIT annually, colonoscopy every 10 years, stool DNA, CT colonography, or flexible sigmoidoscopy all acceptable; NCCN drives staging and treatment algorithms.
- Europe (ESMO) — staging, adjuvant and metastatic treatment algorithms; RAS/BRAF/MSI testing mandated; biologic sequencing. [1]
Drug doses are verified; the ANZ regimen is primary where it differs. FOLFOX every 2 weeks; CAPOX (oxaliplatin 130 mg/m2 plus capecitabine 1000 mg/m2 twice daily days 1 to 14) every 3 weeks; FOLFIRI every 2 weeks; bevacizumab 5 to 7.5 mg/kg every 2 weeks; cetuximab loading 400 mg/m2 then 250 mg/m2 weekly; panitumumab 6 mg/kg every 2 weeks; pembrolizumab 200 mg every 3 weeks (or weight-based). [1]
Summary
Colorectal cancer is the third most common cancer worldwide and a leading cause of cancer death, yet it is preventable and curable when caught early because it develops slowly through the adenoma-carcinoma sequence (APC, then KRAS, then TP53) over 10 to 15 years. Screening with the faecal immunochemical test (FIT) targets the average-risk population from age 50 (45 in the US), with colonoscopy surveillance guided by polyp findings (low-risk adenoma 5 years, high-risk 3 years). Presentation varies by site: iron deficiency anaemia for right-sided tumours, change in bowel habit and obstruction for left-sided, fresh rectal bleeding for rectal. Every new cancer requires colonoscopy with biopsy, CT staging, MRI for rectal cancer, and universal MMR/MSI plus RAS/BRAF molecular testing. Treatment is stage-directed: stage I and most stage II colon cancer need surgery alone; high-risk stage II is selective; stage III gets surgery then FOLFOX or CAPOX; locally advanced rectal cancer gets neoadjuvant chemoradiotherapy then total mesorectal excision; metastatic disease gets chemotherapy plus a biologic by RAS status, first-line pembrolizumab for MSI-high, and metastasectomy when resectable. The hereditary syndromes (Lynch, FAP, MUTYH-associated, Peutz-Jeghers, juvenile polyposis) demand recognition, genetic testing, and cascade screening of relatives. [1]
One-line answer for the viva: "I manage colorectal cancer by the TNM stage and the molecular profile. Stage I and most stage II colon cancer: surgery alone. High-risk stage II: selective FOLFOX or CAPOX. Stage III: surgery then FOLFOX or CAPOX. Locally advanced rectal cancer: neoadjuvant chemoradiotherapy or short-course radiotherapy, then total mesorectal excision. Metastatic disease: FOLFOX or FOLFIRI plus a biologic — anti-EGFR for RAS wild-type, bevacizumab for any — with first-line pembrolizumab for MSI-high disease and metastasectomy when disease is resectable. I screen universally with FIT from age 50, I test MMR/MSI and RAS on every new tumour to find Lynch syndrome and guide therapy, and I counsel and cascade-test relatives for any hereditary syndrome I find." [1]
Sources
Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates. CA Cancer J Clin 2024 [1]; Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell 1990;61:759-767 [2]; Boland CR, Goel A. Microsatellite instability in colorectal cancer. Gastroenterology 2010;138:2073-2087 [3]; Mandel JS, Bond JH, Church TR, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med 1993;328:1365-1371 [4]; Bretthauer M, Loberg M, Wieszczy P, et al. NordICC trial — effect of colonoscopy screening on CRC risks. N Engl J Med 2022;387:1546-1556 [5]; Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer (MOSAIC). N Engl J Med 2004;350:2343-2351 [6]; Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic CRC. N Engl J Med 2004;350:2335-2342 [7]; Karapetis CS, Khambata-Ford S, Jonker DJ, et al. K-ras mutations and benefit from cetuximab in advanced CRC. N Engl J Med 2008;359:1757-1765 [8]; Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351:1731-1740 [9]; Andre T, Diaz LA, Pasmantires N, et al. Pembrolizumab versus chemotherapy for MSI-high/dMMR metastatic CRC (KEYNOTE-177). N Engl J Med 2020;383:2207-2218 [10].
Cancer Council Australia / NHMRC Clinical Practice Guidelines for Colorectal Cancer; US Preventive Services Task Force 2021; NICE Guideline NG151; NCCN Colon and Rectal Cancer Guidelines; ESMO metastatic CRC guidelines. [1]
References
- [1]Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J Clin, 2024.PMID 38572751
- [2]Fearon ER, Vogelstein B A genetic model for colorectal tumorigenesis Cell, 1990.PMID 2188735
- [3]Boland CR, Goel A Microsatellite instability in colorectal cancer Gastroenterology, 2010.PMID 20420947
- [4]Mandel JS, Bond JH, Church TR, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study N Engl J Med, 1993.PMID 8474513
- [5]Bretthauer M, Loberg M, Wieszczy P, et al. Effect of Colonoscopy Screening on Risks of Colorectal Cancer and Related Death N Engl J Med, 2022.PMID 36214590
- [6]Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer N Engl J Med, 2004.PMID 15175436
- [7]Hurwitz H, Fehrenbacher L, Novotny W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer N Engl J Med, 2004.PMID 15175435
- [8]Karapetis CS, Khambata-Ford S, Jonker DJ, et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer N Engl J Med, 2008.PMID 18946061
- [9]Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer N Engl J Med, 2004.PMID 15496622
- [10]Andre T, Diaz LA, Pasmantires N, et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer N Engl J Med, 2020.PMID 33264544