Phys · gastrointestinal
Gastrointestinal Bleeding
Also known as GI bleed · upper GI bleed · UGIB · haematemesis · melaena · lower GI bleed · LGIB · haematochezia · variceal bleed · peptic ulcer bleed · obscure GI bleed · acute gastrointestinal haemorrhage
Consultant-physician-depth guide to acute upper and lower gastrointestinal bleeding — risk stratification (Glasgow-Blatchford, Rockall), resuscitation, restrictive transfusion, endoscopic therapy, variceal management and obscure GI bleed — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Gastrointestinal Bleeding
The answer first
Acute gastrointestinal (GI) bleeding is a time-critical medical emergency. Resuscitation always comes before diagnosis. Two questions drive every decision in the first hour: [1]
- Is the patient haemodynamically stable? If not — two large-bore cannulae, crystalloid bolus, cross-match blood, activate the massive transfusion protocol if shocked.
- Is this likely a variceal or non-variceal source? The answer changes the drug pathway (vasoactive agent + antibiotics for variceal; PPI infusion for non-variceal) and the urgency of endoscopy. [1]
The five non-negotiable actions in suspected upper GI bleed (UGIB):
- Resuscitate (ABCDE): protect airway in haematemesis, IV access, fluid resuscitate, transfuse restrictively.
- Risk-stratify with the Glasgow-Blatchford Score (GBS) before endoscopy — it decides who can wait and who is high-risk.
- Give a proton-pump inhibitor (PPI) infusion (esomeprazole/omeprazole 80 mg bolus then 8 mg/h) if a non-variceal bleed is suspected — though give it early regardless, before the source is confirmed.
- Give a vasoactive drug (terlipressin or octreotide) plus prophylactic antibiotics if variceal bleeding is possible (any known/suspected cirrhosis).
- Arrange upper GI endoscopy within 24 hours — it is both diagnostic and therapeutic. [1]
The transfusion target that changed practice: restrictive transfusion (Hb threshold 70 g/L, transfuse to 70–90 g/L) improves survival compared with a liberal strategy — established by Villanueva et al. (NEJM 2013). The exception is the patient with concomitant acute coronary syndrome or severe vascular disease, where a higher threshold (around 80–90 g/L) is reasonable. [1]
Classification by anatomical source
GI bleeding is divided by the ligament of Treitz: upper GI bleed is proximal, lower GI bleed is distal. A third category — obscure GI bleed — is bleeding that remains unlocalised after standard upper and lower endoscopy. [1]
| Category | Definition | Classic features |
|---|---|---|
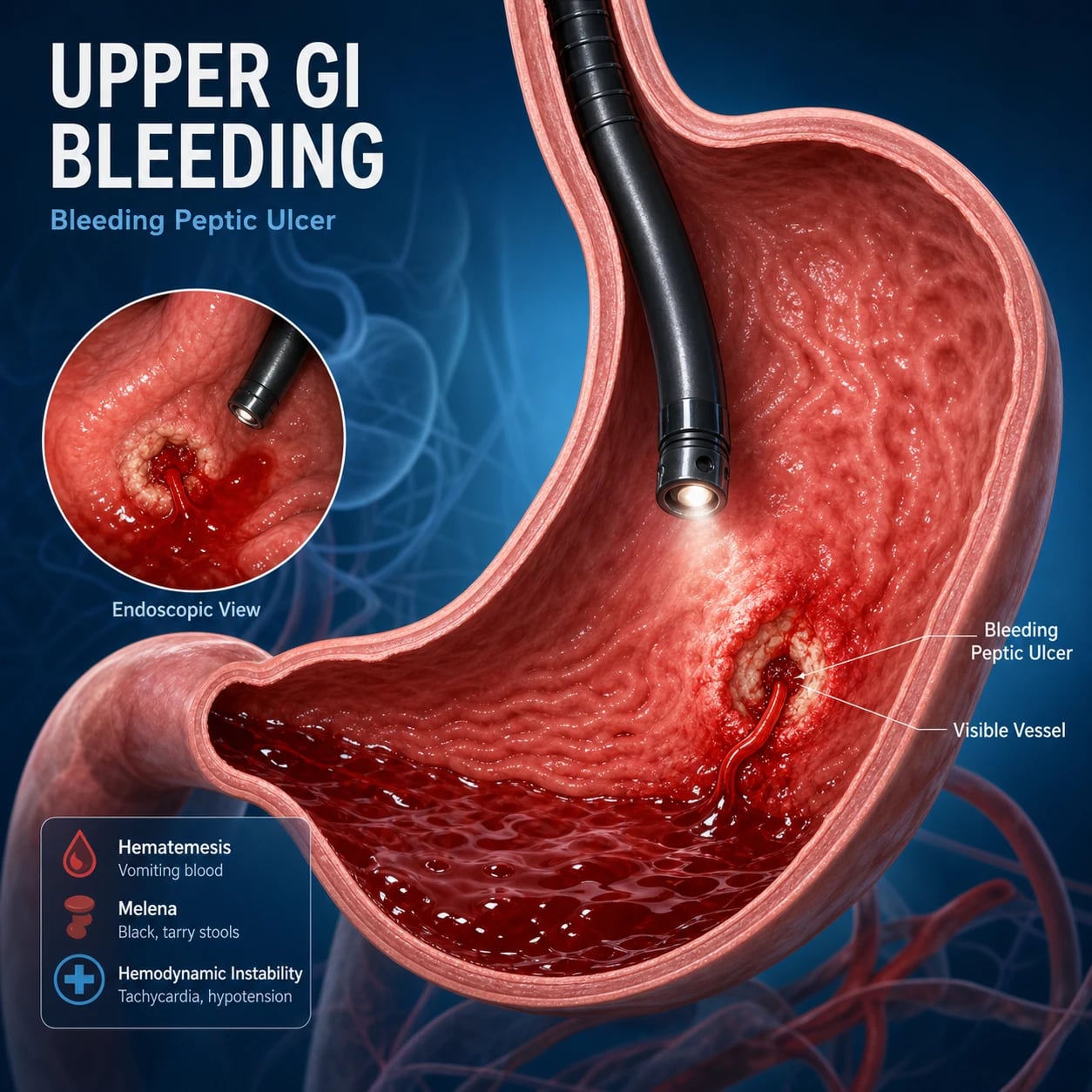
| Upper GI bleed | Bleeding proximal to the ligament of Treitz | Haematemesis, coffee-ground vomit, melaena |
| Lower GI bleed | Bleeding distal to the ligament of Treitz | Haematochezia (bright red blood per rectum), sometimes melaena from right colon |
| Obscure GI bleed | No source found on OGD + colonoscopy | Overt (visible bleeding) or occult (iron deficiency anaemia, positive FOBT) |
DWE trap: Haematochezia does not always mean lower GI bleed. A massive, brisk upper GI bleed can pass rapidly through the gut and present as bright red blood per rectum with haemodynamic instability. The clue is shock out of proportion to the apparent source — always place an NG tube or proceed to upper endoscopy if the patient is unstable. [1]
Risk stratification
Risk stratification determines who needs admission, who needs urgent endoscopy, and who can be safely discharged. Two scores are central — and they are used at different stages. [1]
Glasgow-Blatchford Score (GBS) — pre-endoscopy
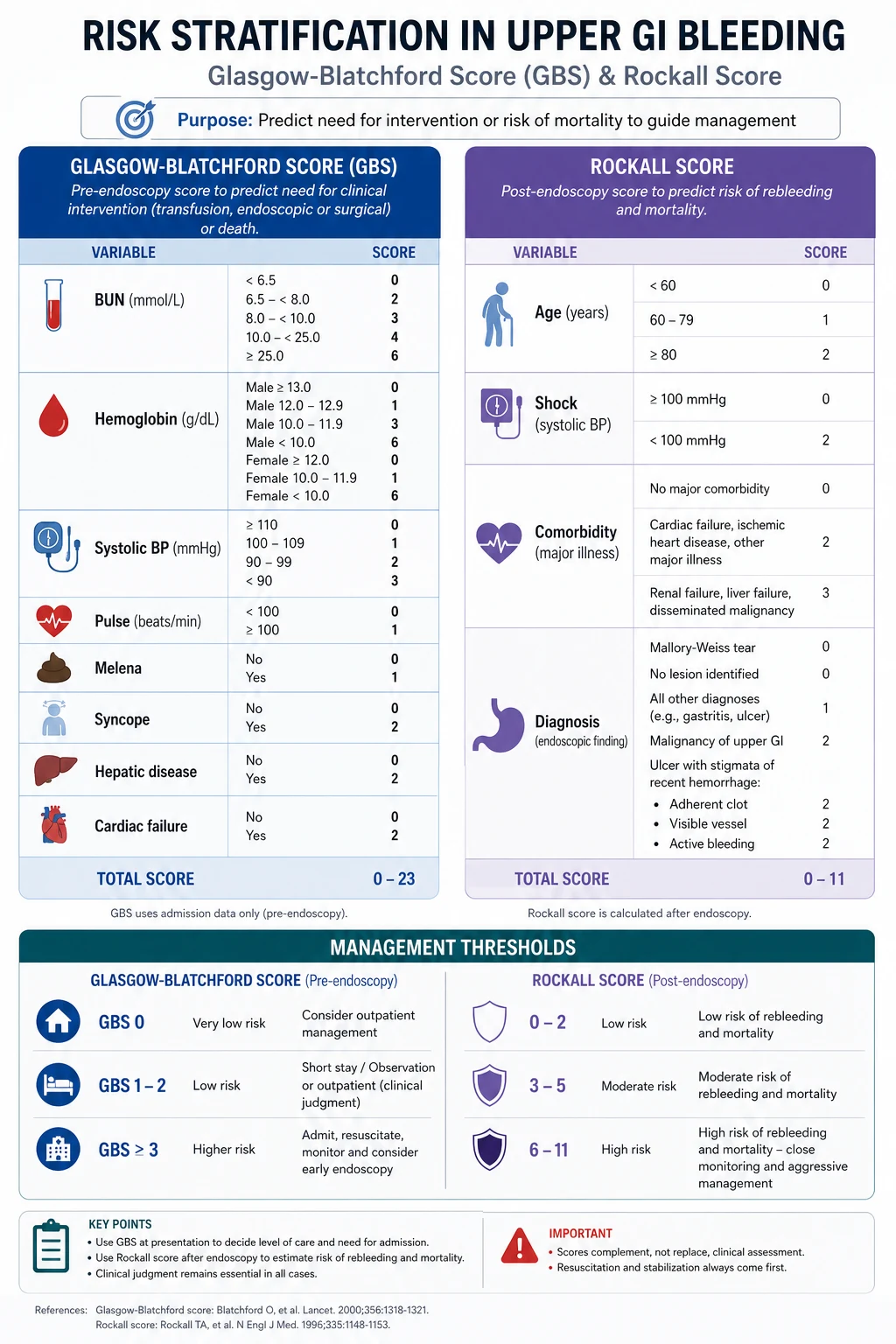
The GBS is calculated at presentation, before endoscopy, using only history, observations and bloods. It predicts the need for intervention (transfusion, endoscopic therapy, surgery) — not mortality. Its strength is its negative predictive value: a low score identifies patients safe for outpatient management. [1]
| Component | Points |
|---|---|
| Urea (mmol/L) | 6.5–7.9 → 2; 8.0–9.9 → 3; 10.0–25.0 → 4; >25 → 6 |
| Haemoglobin men (g/L) | 120–129 → 1; 100–119 → 3; <100 → 6 |
| Haemoglobin women (g/L) | 100–119 → 1; <100 → 6 |
| Systolic BP (mmHg) | 100–109 → 1; 90–99 → 2; <90 → 3 |
| Pulse (beats/min) | >100 → 1 |
| Other markers (present = each adds) | Syncope +2; hepatic disease +2; cardiac failure +2 |
Interpretation:
- GBS 0–1: low risk. Consider outpatient management with early endoscopy clinic follow-up — these patients very rarely need intervention.
- GBS >= 1 (per most guidelines, threshold evolving): admission for endoscopy. Some ANZ/UK pathways use a threshold of 0 only for safe discharge.
- GBS >= 7: high risk — needs admission, early endoscopy, high intervention rate. [1]
DWE high-yield: The GBS is the only validated score usable before endoscopy. Examiners will give you the components and ask for the score and the disposition decision. Memorise the components; you cannot calculate it without urea, haemoglobin, systolic BP, pulse and the three comorbidity markers. [1]
Rockall score — post-endoscopy
The Rockall score is calculated after endoscopy because it incorporates endoscopic findings. It predicts mortality (and rebleeding risk). The full Rockall ranges from 0 to 11. [1]
| Component | 0 | 1 | 2 | 3 |
|---|---|---|---|---|
| Age | <60 | 60–79 | >=80 | — |
| Shock | No shock (SBP >=100, pulse <100) | Tachycardia (SBP >=100, pulse >=100) | Hypotension (SBP <100) | — |
| Comorbidity | None | — | Cardiac failure, ischaemic heart disease, any major comorbidity | Renal failure, liver failure, disseminated malignancy |
| Diagnosis (endoscopic) | Mallory-Weiss, no lesion | All other diagnoses (malignancy included in some versions) | Upper GI malignancy | — |
| Stigmata of recent haemorrhage | None, dark spot | — | Blood in upper GI tract, adherent clot, visible/spurting vessel | — |
Interpretation:
- Score 0–2: low mortality (<1%), low rebleeding risk.
- Score >= 3: significant rebleeding and mortality risk.
- Score >= 8: mortality approaches 40% despite therapy. [1]
The pre-endoscopic (clinical) Rockall uses only the first three components (age, shock, comorbidity) and gives a partial score out of 7. It is less accurate than the GBS for pre-endoscopy decisions but still appears in guidelines and exams. [1]
DCE trap: Know when to use which score. The examiner asks "how will you decide who can go home from the ED?" → GBS. The examiner asks "after his endoscopy showed a visible vessel, what is his risk and what do you do?" → full Rockall. Mixing them up is a common short-case error. [1]
Upper GI bleed — management algorithm
Immediate management (first 30 minutes)
-
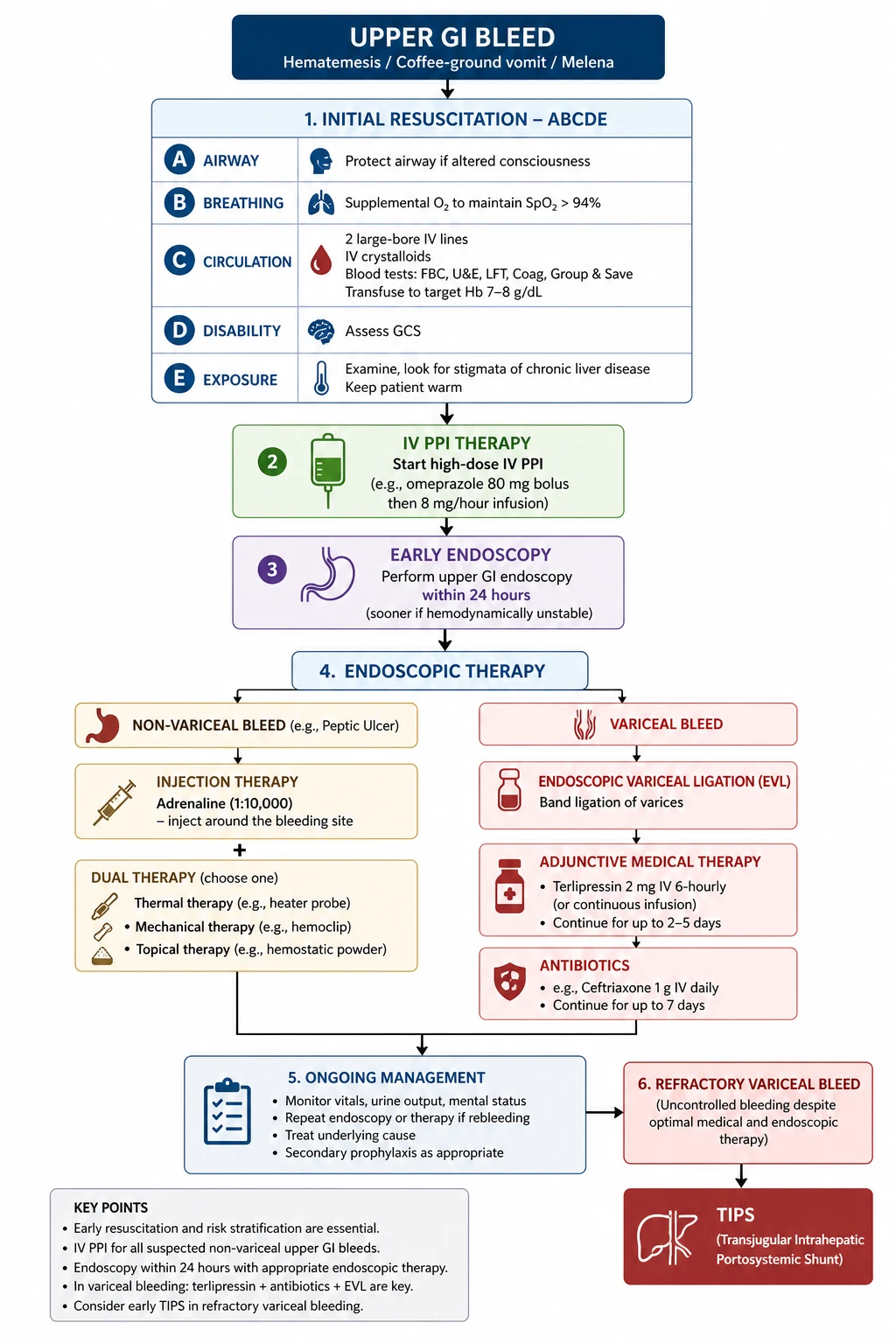
Assess and resuscitate (ABCDE):
- Airway: protect the airway in active haematemesis — risk of aspiration, especially if encephalopathic or intoxicated. Consider early intubation if the airway is not safe or if massive ongoing bleeding is anticipated for endoscopy.
- Breathing: high-flow oxygen if hypoxic or shocked.
- Circulation: two large-bore (14–16 G) cannulae. Take bloods (FBC, U&E, LFTs, coagulation, group and hold/cross-match 2–4 units, lipase, troponin if cardiac history). Restore volume with crystalloid (0.9% sodium chloride or balanced crystalloid) boluses. Avoid over-resuscitation in cirrhosis — it raises portal pressure and worsens variceal bleeding.
- Disability: check conscious state; altered mentation suggests shock, hepatic encephalopathy, or both.
- Exposure/examination: look for stigmata of chronic liver disease (palmar erythema, spider naevi, jaundice, ascites, caput medusae), lymphadenopathy, abdominal tenderness (peritonism = perforation), and rectal examination for melaena/haematochezia. [1]
-
Calculate the GBS to confirm this is a bleed needing admission and intervention. [1]
-
Transfuse restrictively. Transfuse red cells when Hb < 70 g/L, aiming for 70–90 g/L. For the patient with acute coronary syndrome, decompensated heart failure, or critical vascular disease, use a threshold of 80 g/L (aim 80–90 g/L, some up to 100). Do not transfuse a stable patient simply because they have bled — Villanueva et al. (NEJM 2013) showed a liberal strategy (threshold 90 g/L) increased mortality and rebleeding compared with a restrictive (threshold 70 g/L) strategy. [1]
-
Correct coagulopathy cautiously. Reverse warfarin or major anticoagulation only as part of the bleeding plan — do not reflexively give vitamin K or fresh frozen plasma in stable patients, because rapid full reversal can be harmful and is not routinely recommended in guidelines. Manage anticoagulants per their specific reversal pathway (e.g., specific reversal agents for DOACs where appropriate, discuss with haematology). Platelet transfusion is reserved for active bleeding with thrombocytopenia (platelets < 50 × 10⁹/L) or antiplatelet-related bleeding. [1]
Pharmacotherapy before endoscopy
- Suspected non-variceal bleed: start an IV PPI infusion — esomeprazole or omeprazole 80 mg IV bolus, then 8 mg/hour infusion for 72 hours after endoscopic haemostasis for high-risk ulcers. Give the bolus early, before endoscopy, in unselected suspected UGIB.
- Suspected variceal bleed (any cirrhosis/portal hypertension): start a vasoactive drug — terlipressin 2 mg IV every 4 hours (the only vasoactive agent shown to reduce mortality in variceal bleeding; Ioannou Cochrane 2003), or octreotide 50 microgram bolus then 50 microgram/hour infusion (somatostatin is an alternative where available). Continue for 2–5 days.
- Plus prophylactic antibiotics in all cirrhotic patients with GI bleeding — ceftriaxone 1 g IV daily for up to 7 days (or oral quinolone if low-risk). Antibiotics reduce bacterial infections and mortality (Bernard meta-analysis, Hepatology 1999). This is one of the few interventions proven to lower mortality in variceal bleeding. [1]
Endoscopy
- Timing: upper GI endoscopy within 24 hours of admission for most UGIB. Very early endoscopy (within 6–12 hours) has not shown a mortality benefit in unselected patients and may worsen outcomes in unstable patients resuscitated inadequately. For suspected variceal bleeding, endoscopy should occur within 12 hours once resuscitation is underway.
- Resuscitate before scoping. Endoscopy in an under-resuscitated, shocked patient carries a high risk of cardiovascular collapse and aspiration. The exception is uncontrolled bleeding needing emergency endoscopic control. [1]
Endoscopic therapy by source
- Bleeding peptic ulcer (high-risk stigmata — active spurting, oozing, or non-bleeding visible vessel): combination therapy — adrenaline (epinephrine) submucosal injection plus a mechanical or thermal method (haemoclips, heater probe, bipolar coagulation). Adrenaline alone has a high rebleeding rate; dual modal therapy is standard. Follow with the 72-hour PPI infusion (Lau et al., NEJM 2000). [1]- Oesophageal varices: endoscopic band ligation (EVL) is first-line — superior to sclerotherapy with fewer complications (Stiegmann et al., NEJM 1992). Sclerotherapy (e.g., cyanoacrylate for gastric varices) is reserved for lesions not amenable to banding.
- Mallory-Weiss tear: usually self-limiting; endotherapy only if actively bleeding.
- Gastric antral vascular ectasia (GAVE, watermelon stomach): argon plasma coagulation.
- Dieulafoy lesion: endoscopic clipping or thermal coagulation — these are large-calibre submucosal arteries that can re-bleed catastrophically if not secured.
- Angiodysplasia: argon plasma coagulation or thermal contact. [1]
Refractory or massive bleeding
If endoscopic therapy fails or bleeding is uncontrolled:
- Re-attempt endoscopy once — a second endoscopic attempt is appropriate before surgery or radiology.
- Transjugular intrahepatic portosystemic shunt (TIPS) for refractory variceal bleeding, ideally as early (pre-emptive) TIPS within 72 hours in high-risk cirrhotic patients (Child-Pugh B with active bleeding, or Child-Pugh C 10–13) to reduce treatment failure and mortality.
- Surgical or interventional radiology (IR) management for refractory non-variceal bleeding — oversew of the ulcer (under-run vessel) or mesenteric angiography with embolisation. Balloon tamponade (Sengstaken-Blakemore tube) is a temporary bridge (max ~24 hours) to definitive therapy in massive variceal bleeding, with high complication rates (aspiration, oesophageal rupture). [1]
Causes of upper GI bleeding
Rank the causes by frequency and severity — examiners expect a structured list with discriminating features. [1]
| Cause | Key discriminators | Relative frequency |
|---|---|---|
| Peptic ulcer (gastric or duodenal) | Epigastric pain, NSAID/aspirin use, H. pylori; most common cause (~40–50%) | Highest |
| Oesophageal/gastric varices | Cirrhosis, portal hypertension signs; high mortality, massive bleed | ~10–20% |
| Erosive gastritis/oesophagitis | NSAIDs, alcohol, critical illness (stress ulcers), severe reflux | Common |
| Mallory-Weiss tear | Retching/vomiting preceding haematemesis; usually self-limiting | ~5% |
| Gastric/oesophageal cancer | Weight loss, dysphagia, older patient, anaemia | ~5% |
| Angiodysplasia / GAVE | Elderly, chronic occult bleeding, aortic stenosis (Heyde syndrome), renal failure | Variable |
| Dieulafoy lesion | Painless massive haematemesis in an otherwise well patient; large submucosal artery | Rare but dangerous |
| Aortoenteric fistula | Prior aortic graft/surgery + sentinel (herald) bleed — see below | Rare, lethal |
| Haemobilia | Biliary colic, jaundice, GI bleeding (Quincke triad) | Rare |
DWE trap: The Dieulafoy lesion classically presents as painless, massive haematemesis in a patient with no prior GI history and a normal-looking mucosa between bleeds — easy to miss at endoscopy unless actively bleeding. Dieulafoy = painless massive bleed, no ulcer. [1]
Aortoenteric fistula — the must-not-miss diagnosis
An aortoenteric fistula is a direct communication between the aorta (often an abdominal aortic aneurysm repair or graft) and the GI tract, usually the third/fourth part of the duodenum. It carries an extremely high mortality if missed. [1]
Clinical triad:
- Prior aortic surgery or graft (sometimes primary in an unrepairsed aneurysm, but graft is the classic).
- Herald (sentinel) bleed — a self-limiting minor haematemesis/melaena hours to days before catastrophic exsanguination.
- Massive, uncontrolled GI bleeding that follows. [1]
Management: this is a surgical emergency, not an endoscopic diagnosis. Do not rely on endoscopy to diagnose it — request urgent CT angiography and involve vascular surgery immediately. Endoscopy may be performed to exclude another source if the patient is stable, but the diagnosis and treatment are surgical (graft excision and extra-anatomic bypass or in-situ repair). Missing the herald bleed and attributing it to a benign cause is the classic fatal error. [1]
Lower GI bleeding
Causes
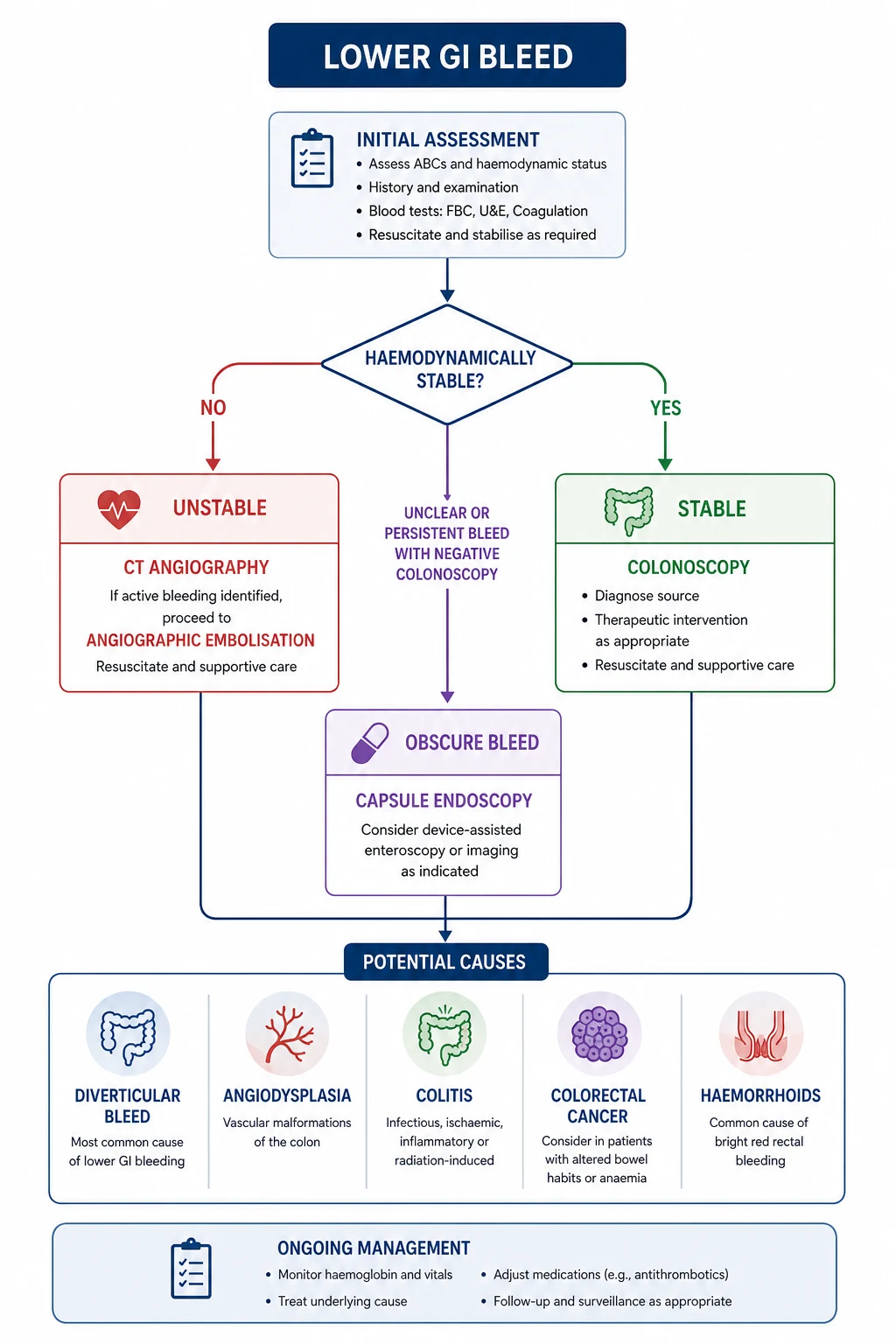
Lower GI bleeding is bleeding distal to the ligament of Treitz, presenting most often as haematochezia (bright red blood or clots per rectum). The common causes differ from upper GI bleeding: [1]
| Cause | Key discriminators |
|---|---|
| Diverticular bleed | Most common cause in older adults; painless, profuse bright red blood; usually stops spontaneously (~75%) but rebleeds |
| Haemorrhoids | Bright red blood on toilet paper/dripping, not mixed with stool; rarely causes major haemorrhage |
| Inflammatory bowel disease (UC/Crohn's) | Bloody diarrhoea, tenesmus, cramping, systemic features |
| Colorectal cancer / polyps | Older patient, change in bowel habit, weight loss, iron deficiency; occult more often than massive |
| Angiodysplasia | Elderly, painless, often right-sided colon; recurrent minor bleeds, renal failure, aortic stenosis |
| Ischaemic colitis | Painful — left-sided abdominal pain then bloody diarrhoea; classic "pain out of proportion"; watershed areas (splenic flexure, rectosigmoid) |
| Post-polypectomy bleed | Recent colonoscopy; can be immediate or delayed up to 2 weeks |
DWE discriminator: Diverticular bleeding is painless; ischaemic colitis is painful. This single contrast separates the two most-tested lower GI bleed causes. Diverticular bleeds are profuse, painless and bright red; ischaemic colitis follows mesenteric hypoperfusion with cramping pain and bloody stools. [1]
Management approach
The principles are the same — resuscitate first, risk-stratify, then localise and treat — but the diagnostic pathway differs. [1]
- Exclude an upper GI source first if the patient is unstable or the bleeding is massive (a brisk UGIB can present as haematochezia). Upper endoscopy if any doubt.
- Risk-stratify — there is no single validated score as universal as the GBS for lower GI bleed, but several (e.g., the Oakland score) help identify low-risk patients suitable for outpatient management. Haemodynamic instability, active bleeding, and comorbidity drive admission and urgency.
- Colonoscopy is the diagnostic test of choice in stable patients — ideally after a bowel preparation, usually within 24 hours of admission for ongoing bleeding. It allows both diagnosis and therapy (clipping, epinephrine injection, argon plasma coagulation).
- CT angiography is the test of choice for haemodynamically unstable patients with active, massive lower GI bleeding — it localises the bleeding site and guides therapy. Active bleeding at >0.5 mL/min is detectable.
- Mesenteric angiography with embolisation is the definitive intervention for massive or refractory lower GI bleeding not controlled endoscopically — it can target the bleeding vessel (e.g., a diverticular artery) with coils or particles.
- Surgery (segmental colectomy) is reserved for refractory, unlocalisable, or recurrent life-threatening bleeding despite angiographic and endoscopic attempts. [1]
Obscure GI bleeding
Obscure GI bleeding is persistent or recurrent bleeding for which no source has been found on upper endoscopy and colonoscopy. It is divided into:
- Overt: visible bleeding (melaena, haematochezia) — small bowel source is the most likely culprit.
- Occult: iron deficiency anaemia and/or positive faecal occult blood, no visible bleeding. [1]
The small bowel is the most common site of obscure bleeding (angiodysplasia, small bowel tumours, Crohn's disease, Meckel diverticulum). [1]
Diagnostic pathway:
- Repeat and review the upper endoscopy and colonoscopy — up to 25% of "obscure" bleeds are missed lesions in the reach of standard endoscopes (e.g., gastric angiodysplasia, caecal cancer).
- Capsule endoscopy is the first-line investigation for the small bowel in obscure bleeding — it has the highest diagnostic yield (~60%) compared with push enteroscopy or barium studies (Triester meta-analysis, Am J Gastroenterol 2005). It localises the bleeding to a small bowel segment but cannot biopsy or treat.
- Device-assisted (double-balloon) enteroscopy is used to confirm, biopsy and treat lesions found on capsule endoscopy — it can reach deep into the small bowel from oral or anal routes and allows haemostasis (clipping, argon plasma coagulation).
- CT or MR enterography for structural lesions (tumours, strictures, Crohn's).
- Meckel scan (technetium-99m pertechnetate) in younger patients with obscure overt bleeding — Meckel diverticulum with ectopic gastric mucosa. [1]
DWE high-yield: The sequence is capsule endoscopy first (localise), then double-balloon enteroscopy (treat). Capsule endoscopy has the highest yield but is non-therapeutic; double-balloon enteroscopy reaches the lesion for haemostasis. [1]
Investigations
| Test | Purpose | When |
|---|---|---|
| FBC | Baseline Hb (may lag true loss), platelets, MCV (chronic blood loss = microcytic) | All patients |
| U&E | Urea (raised disproportionately to creatinine suggests UGIB — blood digested in gut raises urea), creatinine | All patients |
| LFTs, coagulation | Liver disease/coagulopathy (suggests variceal source) | All patients |
| Group and cross-match | Transfusion readiness | All significant bleeds; 2–4 units |
| Upper GI endoscopy | Diagnosis + therapy (ulcers, varices) | Within 24 h; within 12 h for suspected varices |
| Colonoscopy | Lower GI source — diagnosis + therapy | Stable LGIB, after bowel prep |
| CT angiography | Localise active bleeding | Unstable/massive bleeding, obscure |
| Mesenteric angiography | Localise + embolise | Refractory massive bleeding |
| Capsule endoscopy | Obscure bleed — small bowel source | After negative OGD + colonoscopy |
Why does urea rise in upper GI bleeding? Digested blood proteins are absorbed in the upper small bowel and converted to urea by the liver, producing a disproportionately high urea-to-creatinine ratio (typically urea : creatinine > 30 in SI units). This is a classic exam discriminator and helps confirm an upper GI source when the bleeding is occult. [1]
Pharmacology — drug doses at a glance
| Drug | Dose / route | Indication | Rationale |
|---|---|---|---|
| PPI (esomeprazole or omeprazole) | 80 mg IV bolus, then 8 mg/h infusion x 72 h | Non-variceal ulcer bleed (after endoscopic haemostasis) | Reduces rebleeding (Lau 2000). Post-endoscopy for high-risk stigmata. |
| Octreotide | 50 microgram IV bolus, then 50 microgram/h infusion | Variceal bleed (alternative to terlipressin) | Somatostatin analogue; widely available where terlipressin is not. |
| Ceftriaxone | 1 g IV daily, up to 7 days | Cirrhotic with any GI bleed (prophylaxis) | Reduces bacterial infection and mortality (Bernard 1999). |
| Vitamin K | 5–10 mg IV slow (only if indicated) | Reversal of warfarin (cautious) | Not routine; discuss with haematology. |
| Sucralfate / misoprostol | Per local protocol | Stress ulcer prophylaxis in ICU | For ventilated/coagulopathic ICU patients. |
Long-term management and secondary prevention
After the acute episode, address the underlying cause to prevent recurrence: [1]
- Peptic ulcer: test and treat H. pylori (urea breath test or biopsy at endoscopy; serology if recent antibiotics/PPI). Continue a maintenance PPI for high-risk patients (prior bleeding ulcer on aspirin/clopidogrel, or multiple bleeds). Address NSAID use — switch to paracetamol or add a PPI if NSAIDs unavoidable. Resume low-dose aspirin for secondary cardiovascular prevention as soon as haemostasis is secured (the thrombotic risk of stopping outweighs the bleeding risk after 2–3 days); manage dual antiplatelet therapy with cardiology input.
- Variceal bleeding: secondary prophylaxis with non-selective beta-blocker (propranolol or carvedilol) titrated to heart rate, plus repeat EVL sessions to obliterate varices (every 1–2 weeks until eradicated). Address underlying liver disease; consider transplant referral in decompensated cirrhosis. Refer to the related chronic liver disease topic for full portal hypertension management.
- Diverticular bleed: most stop spontaneously; no specific drug prophylaxis. Educate about rebleeding risk (~25% at 4 years); surgery considered for recurrent severe bleeds.
- Angiodysplasia: consider the aortic stenosis — angiodysplasia (Heyde syndrome) association; recurrent bleeding may improve after aortic valve replacement. Thalidomide or octreotide have evidence for refractory cases.
- Colorectal cancer: stage-appropriate oncology referral and surveillance. [1]
Multi-morbidity, anticoagulation and shared decisions
The complex GI bleed patient is common in the DCE long case — they have atrial fibrillation on a DOAC, a recent stent on dual antiplatelet therapy, CKD, and ischaemic heart disease. The decisions: [1]
- Anticoagulation: for a life-threatening bleed, withhold and consider specific reversal (idarucizumab for dabigatran, andexanet for apixaban/rivaroxaban — discuss with haematology given cost and thrombotic risk). Restart anticoagulation as soon as bleeding is controlled — the optimal window is 7–14 days for most bleeds, balancing thromboembolic and rebleeding risk. Premature permanent cessation is a common and harmful error.
- Antiplatelets: continue aspirin for secondary prevention through the bleed where possible; withhold clopidogrel/ticagrelor during active bleeding and resume after haemostasis. Never stop dual antiplatelet therapy in a patient with a recent (within 6 months) stent without cardiology input — stent thrombosis is catastrophic.
- Cardiovascular comorbidity: the restrictive transfusion threshold shifts up (80–90 g/L) in acute coronary syndrome; over-transfusion causes volume overload in heart failure.
- Renal disease: uraemia impairs platelet function; angiodysplasia is more common and refractory in CKD. [1]
Communication and consent
- Explain the procedure and risks of endoscopy (perforation, aspiration, sedation in a haemodynamically unstable patient) and obtain consent where possible — but in life-threatening bleeding, proceed under implied consent and document the clinical urgency.
- Discuss prognosis honestly with cirrhotic patients — variceal bleeding is a marker of decompensation with significant 1-year mortality; transplant referral conversations should begin early.
- Involve the patient and family in goals of care discussions for the frail, multi-morbid patient where the burden of ICU, repeated endoscopy, and surgery may outweigh benefit. [1]
Exam traps and high-yield discriminators
- Transfuse restrictively. A liberal strategy (threshold 90 g/L) increases mortality in UGIB (Villanueva 2013). The MCQ answer is Hb threshold 70 g/L, except in ACS where it is higher. [1]2. GBS is pre-endoscopy; Rockall is post-endoscopy. Do not conflate them. GBS predicts need for treatment; Rockall predicts mortality.
- Urea disproportionately raised relative to creatinine = upper GI source. The ratio is a classic discriminator.
- Haematochezia with shock = consider brisk UGIB, not necessarily a lower source. Place an NG tube or scope from above first.
- Aortoenteric fistula in any patient with prior aortic graft surgery and a herald bleed — CT angiography and vascular surgery, not endoscopy.
- Dieulafoy lesion = painless massive haematemesis in a well patient, no visible ulcer.
- Cirrhotic bleed = antibiotics + vasoactive agent + early endoscopy. Antibiotics reduce mortality — never omit them.
- Capsule first, then double-balloon enteroscopy for obscure GI bleed.
- Diverticular bleed is painless; ischaemic colitis is painful — the single contrast for lower GI bleed MCQs.
- Endoscopic dual therapy (adrenaline + clip/thermal) for bleeding ulcers — adrenaline alone rebleeds. [1]
DCE long-case integration
A typical GI bleed long case is a 70-year-old with melaena, a background of atrial fibrillation on apixaban, ischaemic heart disease on aspirin, CKD, and a recent aspirin/NSAID increase for osteoarthritis. You will be expected to: [1]
- Present a structured problem list (acute UGIB, anticoagulation management, cardiovascular risk, renal function, polypharmacy).
- Justify your resuscitation (restrictive transfusion, PPI infusion, hold apixaban, discuss reversal with haematology).
- Give an integrated management plan (endoscopy timing, endoscopic therapy, secondary prevention, safe anticoagulant resumption, H. pylori testing).
- Discuss communication and shared decision-making — when to resume anticoagulation, goals of care if frail. [1]
Refer to the SAQ, viva, and case artifacts for worked examples at this depth. [1]
References and guidelines
ACG Clinical Guideline: Management of Patients with Ulcer Bleeding (2021); Baveno VII consensus on portal hypertension (2022); NICE CG141 Acute upper gastrointestinal bleeding; GESA (Gastroenterological Society of Australia) clinical guidance; AASLD/BSG liver and variceal bleeding guidance. Key trials: Villanueva 2013 (transfusion strategy), Lau 2000 (PPI infusion), Stiegmann 1992 (EVL), Bernard 1999 (antibiotic prophylaxis), Ioannou 2003 (terlipressin), Triester 2005 (capsule endoscopy). [1]
References
- [1]Blatchford O, Murray WR, Blatchford M A risk score to predict need for treatment for upper-gastrointestinal haemorrhage Lancet, 2000.PMID 11073021
- [2]Rockall TA, Logan RF, Devlin HB, Northfield TC Risk assessment after acute upper gastrointestinal haemorrhage Gut, 1996.PMID 8675081
- [3]Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding N Engl J Med, 2013.PMID 23281973
- [4]Lau JY, Sung JJ, Lee KK, et al. Effect of intravenous omeprazole on recurrent bleeding after endoscopic treatment of bleeding peptic ulcers N Engl J Med, 2000.PMID 10922420
- [5]Bernard B, Grange JD, Khac EN, Amiot X, Opolon P, Poynard T Antibiotic prophylaxis for the prevention of bacterial infections in cirrhotic patients with gastrointestinal bleeding: a meta-analysis Hepatology, 1999.PMID 10347104
- [6]Ioannou GN, Doust J, Rockey DC Terlipressin for acute esophageal variceal hemorrhage Cochrane Database Syst Rev, 2003.PMID 12535432
- [7]Stiegmann GV, Goff JS, Michaletz-Onody PA, et al. Endoscopic sclerotherapy as compared with endoscopic ligation for bleeding esophageal varices N Engl J Med, 1992.PMID 1579136
- [8]Triester SL, Leighton JA, Leontiadis GI, et al. A meta-analysis of the yield of capsule endoscopy compared to other diagnostic modalities in patients with obscure gastrointestinal bleeding Am J Gastroenterol, 2005.PMID 16279893