Phys · gastrointestinal
Inflammatory Bowel Disease
Also known as ulcerative colitis · Crohn's disease · UC · IBD · regional enteritis · Crohn disease · indeterminate colitis · IBD-U · colitis-associated neoplasia · acute severe ulcerative colitis
Consultant-physician-depth guide to inflammatory bowel disease — pathophysiology (NOD2, ATG16L1, Th1/Th17, TNF, IL-12/23), UC versus Crohn's discrimination, clinical phenotypes, extraintestinal manifestations, investigation strategy, stepwise biologic and surgical management, colitis-associated neoplasia surveillance, and pregnancy. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Inflammatory Bowel Disease
The answer first
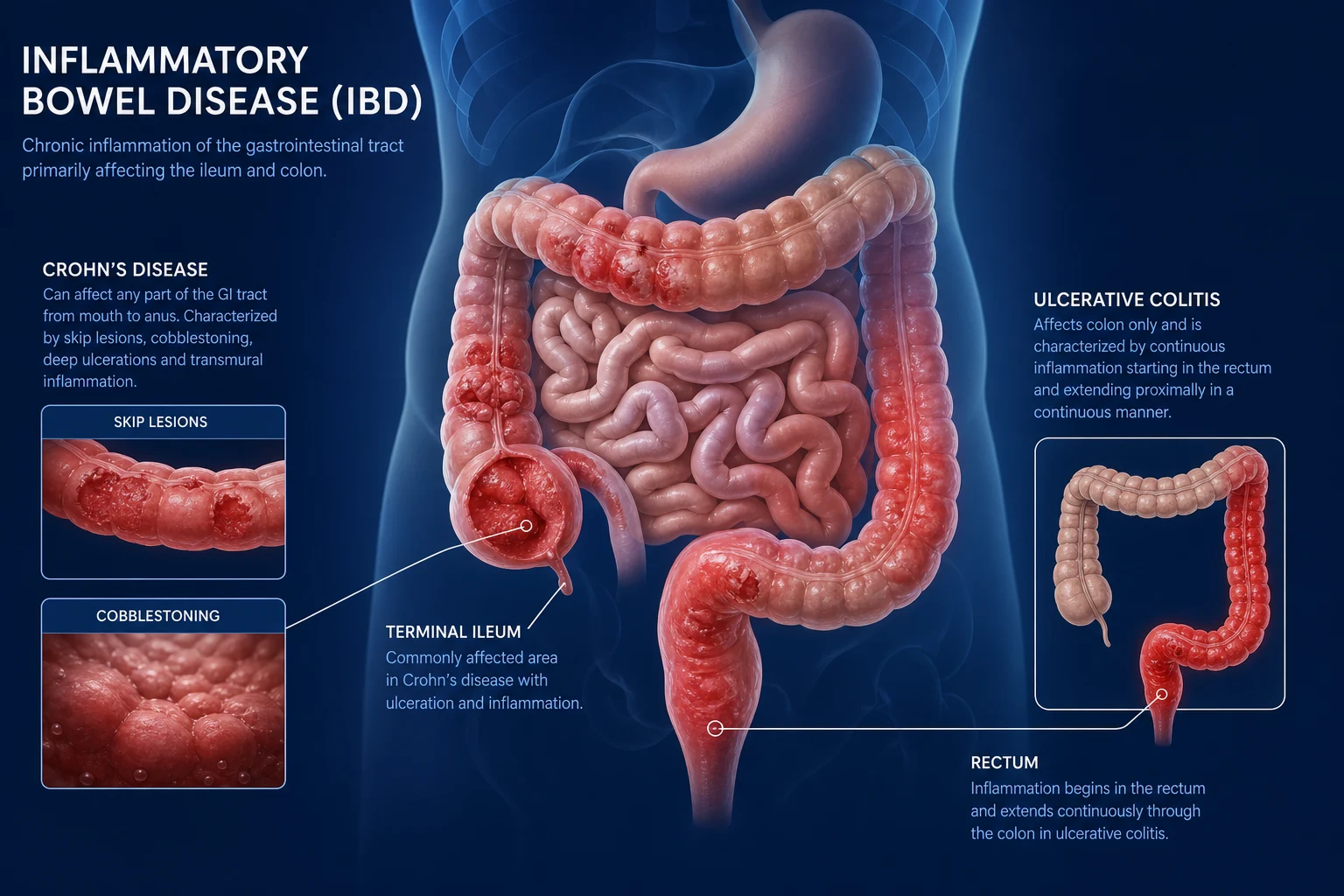
Inflammatory bowel disease (IBD) is chronic, immune-mediated intestinal inflammation arising from a dysregulated mucosal immune response to gut microbiota in a genetically susceptible host. The two major subtypes are ulcerative colitis (UC), a mucosal disease limited to the colon and rectum with continuous proximal spread, and Crohn's disease, a transmural disease that can affect any segment of the gastrointestinal tract from mouth to anus with skip lesions. [1]
The single most important concept for the exam is that treatment has moved to a treat-to-target paradigm targeting mucosal or endoscopic healing, not just symptom control [10]. Steroids induce remission but do not maintain it; maintenance requires 5-ASA, immunomodulators, biologics, or small molecules. The right drug depends on the disease type (UC versus Crohn's), the phenotype (luminal versus fistulising), the severity, and the patient's comorbidities and preferences.
DCE trap: The biggest pivot in IBD management is the move from "step-up" (escalate through steroids then immunomodulators then biologics) to "top-down" (early aggressive therapy with combination biologic plus immunomodulator in high-risk patients). In every long case, classify the disease, state the severity, state the phenotype, and justify your treatment intensity by the risk of complications — not just symptom relief. [1]
Pathophysiology — why the immune cascade matters clinically
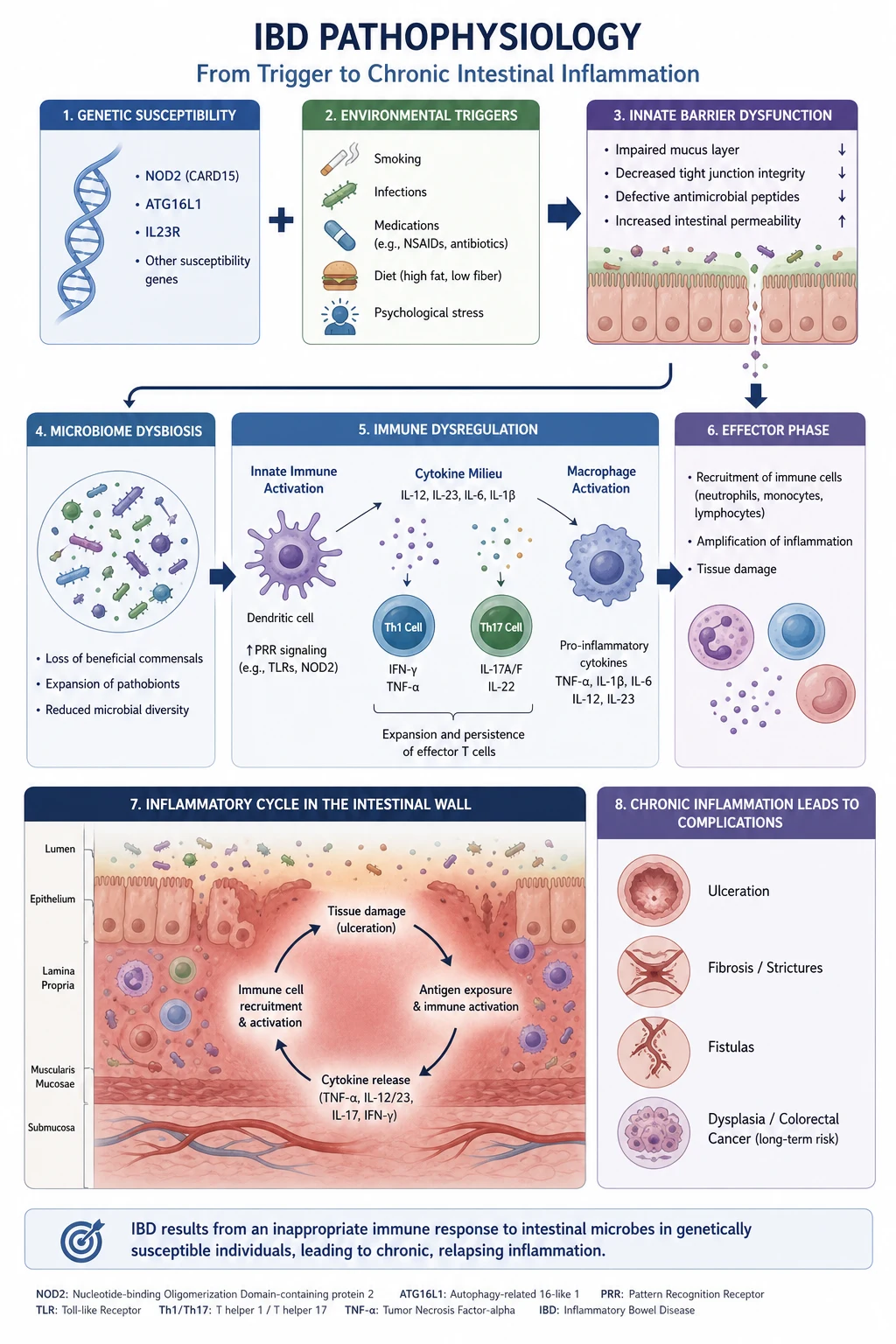
IBD results from an inappropriate, sustained mucosal immune response to commensal gut bacteria in a genetically predisposed person. Four interactive pillars produce disease: genetic susceptibility, barrier dysfunction, microbiome dysbiosis, and immune dysregulation [1].
Genetic susceptibility
Over 200 IBD susceptibility loci have been identified through genome-wide association studies. The two most important genes for the exam: [1]
-
NOD2 (nucleotide-binding oligomerisation domain 2) — the strongest genetic risk factor for Crohn's disease. NOD2 is an intracellular pattern recognition receptor for muramyl dipeptide (MDP), a component of bacterial cell walls. When NOD2 detects MDP, it activates nuclear factor-kappa B and autophagy pathways. Loss-of-function NOD2 variants (three common mutations in people of European ancestry) impair bacterial sensing and clearance, allowing intracellular organisms to persist and drive chronic inflammation. Homozygous or compound heterozygous carriage confers a 2- to 4-fold increased risk of Crohn's, and predicts ileal disease, stricturing, and fistulising behaviour. [1]
-
ATG16L1 (autophagy-related 16-like 1) — the T300A variant impairs autophagy, the process by which cells engulf and degrade intracellular pathogens and damaged organelles. NOD2 and ATG16L1 converge on the same biological pathway: defective autophagic handling of intracellular bacteria in Paneth cells (specialised antimicrobial cells of the ileal crypts) [1]. This convergence explains why both genes predispose specifically to Crohn's disease with ileal involvement.
Other notable loci include IL23R (protective variant reduces IL-23 signalling), IRGM (autophagy), and HLA region genes (stronger association with UC). However, most IBD risk is polygenic and non-Mendelian — a family history increases risk 5- to 10-fold, but concordance in identical twins is only 30 to 50 per cent for Crohn's and 10 to 15 per cent for UC, confirming that environmental triggers are essential. [1]
Barrier dysfunction
The intestinal epithelium forms a single-cell barrier separating the luminal microbiota (roughly 100 trillion organisms) from the mucosal immune system. Tight junction proteins (claudins, occludin, zonula occludens) regulate paracellular permeability. In IBD, barrier integrity is compromised by cytokines (notably TNF and interferon-gamma), which cause tight junction reorganisation. Increased permeability allows bacterial antigens to penetrate the mucosa and activate lamina propria immune cells, perpetuating the inflammatory cycle. This is why some therapies — notably anti-TNF — work partly by restoring barrier function ("mucosal healing"), not just by suppressing inflammation. [1]
Microbiome dysbiosis
Patients with IBD have reduced microbial diversity, a depletion of beneficial short-chain-fatty-acid producers (notably Faecalibacterium prausnitzii), and an expansion of facultative anaerobes and mucosa-associated adherent-invasive Escherichia coli. The dysbiosis is not a single-pathogen cause; rather, the community structure shifts toward a pro-inflammatory configuration. Antibiotics and diet modulate the microbiome and may influence disease activity, though no single probiotic or dietary intervention reproducibly induces or maintains remission. [1]
Immune dysregulation — the cytokine cascade
The adaptive immune response in IBD is dominated by T-helper subsets: [1]
-
Crohn's disease is driven primarily by a Th1 and Th17 response. Naive T cells differentiate into Th1 cells under IL-12 stimulation, producing interferon-gamma and TNF-alpha. Th17 cells develop under TGF-beta plus IL-6 and IL-23 stimulation, producing IL-17A, IL-17F, and IL-22. Both pathways converge on tissue-damaging inflammation. [1]
-
Ulcerative colitis has a more atypical Th2-like response, with increased IL-13 production from natural killer T cells, though Th17 also contributes. [1]
The clinically pivotal cytokines are TNF-alpha (central to both UC and Crohn's — the target of infliximab, adalimumab, golimumab, certolizumab), IL-12/23 (the shared p40 subunit targeted by ustekinumab, and the IL-23-specific p19 subunit targeted by risankizumab and mirikizumab), and the integrin-mediated lymphocyte trafficking pathway (alpha-4 beta-7 integrin targeted by vedolizumab). [1]
DWE high-yield mechanism question: "Why does targeting TNF help both UC and Crohn's?" Answer: TNF-alpha is a central pro-inflammatory cytokine in both Th1 and Th17 pathways; it amplifies inflammation, upregulates adhesion molecules, increases epithelial permeability, and drives tissue destruction. Blocking it interrupts the cascade at multiple points — which is why anti-TNF agents work across the full IBD spectrum. [1]
UC versus Crohn's — the discrimination table
This table is the core discriminator for the DWE and the DCE short case. Commit it to memory. [1]
| Feature | Ulcerative colitis | Crohn's disease |
|---|---|---|
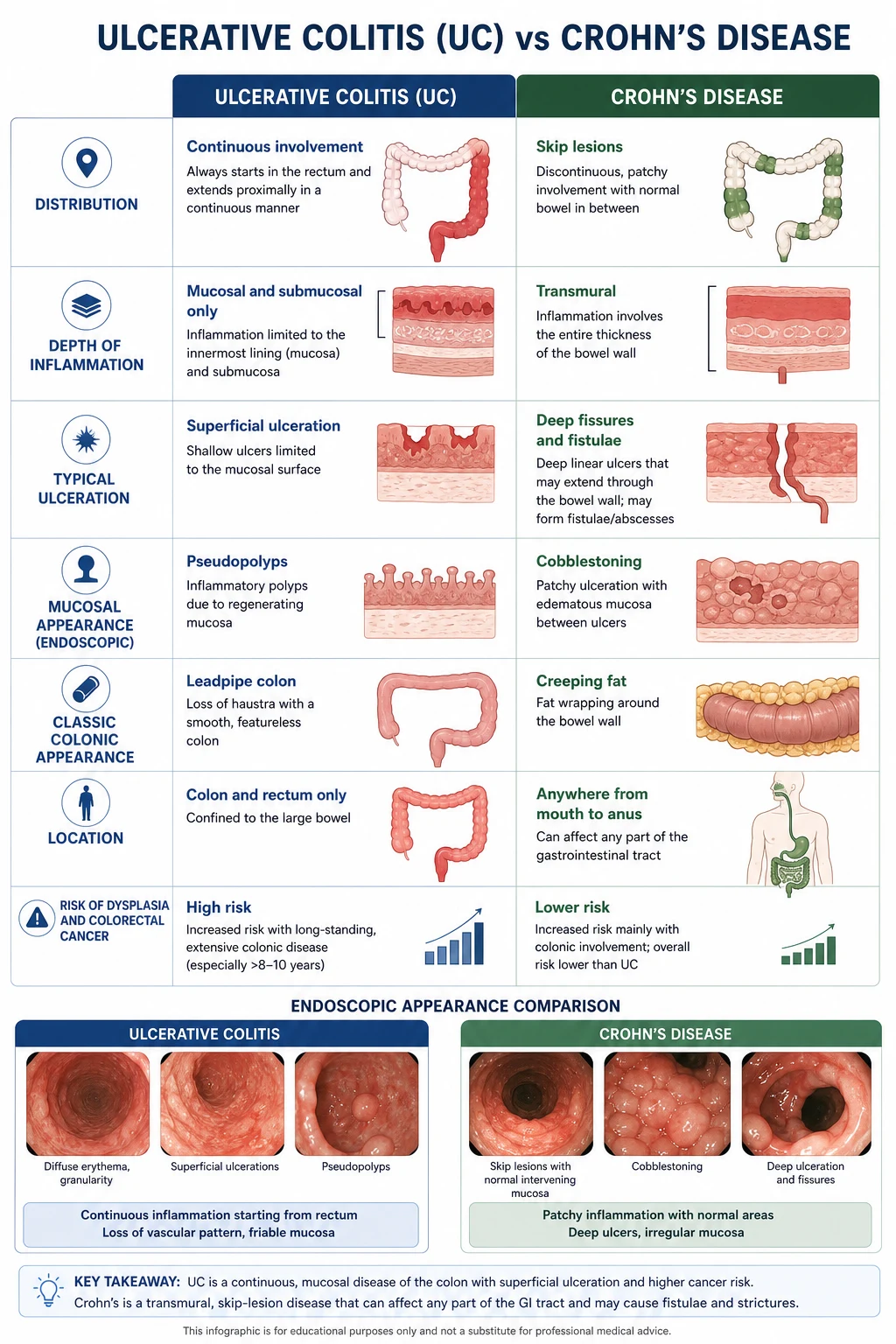
| Distribution | Continuous from rectum, proximal spread. Rectum always involved (proctitis, procotsigmoiditis, left-sided, extensive/pancolitis). Colon only. | Skip lesions, any segment from mouth to anus. Rectal sparing in up to 40 per cent. Ileal involvement common. |
| Depth of inflammation | Mucosal and submucosal only | Transmural — through all bowel wall layers |
| Endoscopy | Loss of vascular pattern, granularity, friability, superficial ulceration, pseudopolyps. Continuous from rectum. | Aphthous ulcers, deep linear or serpiginous ulcers, cobblestoning, skip areas. |
| Histology | Crypt abscesses, mucosal neutrophilic infiltrate, goblet cell mucin depletion, basal plasmacytosis. Inflammation limited to mucosa. | Patchy transmural inflammation, non-caseating granulomas (in about 30 per cent), fissuring ulceration, creeping fat. |
| Imaging (CTE/MRE) | Not diagnostic; may show colonic wall thickening. | Bowel wall thickening, mural stratification, strictures, fistulae, abscess, fat wrapping (creeping fat), comb sign (engorged vasa recta). |
| Perianal disease | Uncommon | Common — skin tags, fissures, fistulae, abscesses in up to one-third. |
| Strictures | Rare; suggests carcinoma or severe inflammation | Common — may be inflammatory or fibrotic |
| Fistulae | Very rare | Common — perianal, enterovesical, enterocutaneous, enteroenteric |
| Surgery | Curative (proctocolectomy removes all disease) | Not curative — recurrence common at anastomosis |
| Smoking | Protective (quitters risk flare); ex-smokers over-represented | Worsens disease; increases flare and surgery risk |
| PSC association | Strong (male predominance, pancolitis, low cancer risk per duration) | Weak |
| Serology | pANCA positive in 60 to 70 per cent; ASCA negative | ASCA positive in 40 to 60 per cent; pANCA negative |
The smoking paradox is a perennial exam favourite: smoking appears to protect against UC (risk is lower in smokers; quitting can trigger onset) but worsens Crohn's disease (smokers have more flares, more strictures, and more surgery). [1]
DWE trap: "Non-caseating granulomas are pathognomonic of Crohn's." This is true when present, but they are found in only about 30 per cent of Crohn's biopsies — their absence does not exclude Crohn's. They are also found in intestinal tuberculosis and sarcoidosis, so context matters, especially in TB-endemic regions. [1]
Clinical presentation
Ulcerative colitis
The cardinal symptom is bloody diarrhoea, often with mucus, urgency and tenesmus. The presentation ranges from mild proctitis (rectal bleeding and urgency with formed stools) to fulminant colitis with toxic megacolon. [1]
Truelove and Witts severity criteria classify an acute UC attack at diagnosis or flare. A severe attack is defined by any one of the following, with more than six bloody stools daily: [1]
| Criterion | Severe threshold |
|---|---|
| Stool frequency | More than 6 per day |
| Blood in stool | Macroscopic blood (frank) |
| Temperature | Greater than 37.8 degrees C |
| Heart rate | Greater than 90 bpm |
| Haemoglobin | Less than 105 g/L |
| ESR | Greater than 30 mm/h |
A moderate attack falls between mild (fewer than 4 stools daily with no systemic features) and severe. This classification drives the threshold for hospital admission and IV steroids. [1]
DCE long-case trap: Any patient meeting Truelove-Witts severe criteria requires same-day hospital admission, stool testing (including C. difficile toxin and culture), abdominal X-ray to exclude toxic megacolon, and IV hydrocortisone. Assess on day 3 — the response dictates whether rescue therapy (infliximab or ciclosporin) or surgery is needed. [1]
Crohn's disease
Crohn's presents more variably because of its diverse location and transmural nature. The Montreal classification organises the phenotype by age, location (L1 ileal, L2 colonic, L3 ileocolonic, L4 isolated upper GI) and behaviour (B1 non-stricturing non-penetrating, B2 stricturing, B3 penetrating). [1]
Two dominant phenotypes: [1]
-
Luminal (B1/B2) Crohn's — chronic diarrhoea (may be non-bloody), abdominal pain (classically right iliac fossa), weight loss, fatigue, and features of malabsorption if extensive small bowel involvement. Stricturing disease (B2) presents with obstructive symptoms — cramping, distension, vomiting — and must be distinguished from inflammatory disease, because steroids worsen fibrotic strictures. [1]
-
Fistulising (B3) Crohn's — perianal fistulae (the most common), internal fistulae (enterovesical causing pneumaturia and recurrent UTI; enterocutaneous), and intra-abdominal abscess. Perianal disease may precede luminal symptoms by years and is a major cause of morbidity and surgery. Examine the perineum in every suspected Crohn's patient — this is the most commonly missed bedside finding in exams. [1]
Growth failure and delayed puberty may be the presenting feature in adolescent Crohn's. [1]
Extragastrointestinal manifestations
Extragastrointestinal manifestations (EIMs) affect up to 40 per cent of IBD patients and may precede, accompany or follow the intestinal disease. Group them into those that parallel gut inflammation (activity-related) and those that run an independent course (activity-independent). [1]
Activity-related (track bowel inflammation)
| Manifestation | Key features | Association |
|---|---|---|
| Peripheral arthritis (Type 1) | Asymmetric, oligoarticular, large joints (knees, ankles). Self-limited; resolves with gut treatment. | More common in UC and Crohn's colitis |
| Erythema nodosum | Tender red nodules on anterior shins. Mirrors disease activity. | Common; correlates with bowel flares |
| Aphthous stomatitis | Painful shallow oral ulcers. | Common in Crohn's |
| Episcleritis | Red, burning eyes without visual loss. | Resolves with bowel treatment |
Activity-independent (run their own course)
| Manifestation | Key features | Association |
|---|---|---|
| Axial arthropathy (sacroiliitis, ankylosing spondylitis) | Inflammatory back pain, morning stiffness. HLA-B27 positive in many. Does not respond to gut treatment. | Independent of bowel activity; may precede IBD by years |
| Primary sclerosing cholangitis (PSC) | Cholestatic LFTs, stricturing of intra- and extrahepatic bile ducts. Male predominance. Independently increases colitis-associated cancer risk. | Strongly associated with UC (about 5 per cent of UC patients); rectal sparing and backwash ileitis common |
| Uveitis (anterior) | Eye pain, photophobia, blurred vision. Urgent ophthalmology referral. | Independent of bowel activity; can cause permanent visual loss |
| Pyoderma gangrenosum | Painful ulcer with undermined edges, usually on legs. Pathergy. | Activity-independent; may precede IBD diagnosis |
| Peripheral arthritis (Type 2) | Symmetric polyarticular, small joints. Independent of bowel activity. | More common in Crohn's |
DCE short-case trap: The short-case examiner will ask you to classify an extraintestinal manifestation as activity-related or activity-independent. State the distinction clearly: "Erythema nodosum and Type 1 peripheral arthritis track gut inflammation and resolve with bowel treatment. Axial spondyloarthritis, PSC, and pyoderma gangrenosum run an independent course and require separate management." This distinction earns marks. [1]
Investigations
First-line (confirm diagnosis and assess severity)
| Investigation | Purpose |
|---|---|
| Full blood count | Anaemia (chronic disease, iron deficiency, B12 in terminal ileal Crohn's), leukocytosis, thrombocytosis in active disease |
| CRP and ESR | Inflammatory markers; CRP correlates with endoscopic activity and predicts anti-TNF response. About 15 per cent are CRP non-responders. |
| Iron studies, B12, folate | Iron deficiency from bleeding or malabsorption; B12 deficiency from terminal ileal disease or resection |
| Stool microscopy and culture, C. difficile toxin | Exclude infectious colitis (Campylobacter, Salmonella, Shigella, E. coli, C. difficile) — the most important differential in acute presentation |
| Faecal calprotectin | Neutrophil-derived protein; correlates with mucosal inflammation. High NPV for excluding IBD in IBS-like presentations. Cut-off typically 50 microg/g. |
Faecal calprotectin — the non-invasive gatekeeper
Faecal calprotectin is a calcium-binding protein released by activated neutrophils at sites of intestinal inflammation. Its concentration in stool directly reflects the degree of mucosal neutrophilic infiltration. A meta-analysis confirmed it is the single best non-invasive test for excluding IBD in adults with symptoms suggestive of irritable bowel syndrome, with a pooled sensitivity around 80 per cent and specificity around 90 per cent — far superior to CRP or ESR alone [9].
Key practical points:
- To exclude IBD: a normal faecal calprotectin (below 50 microg/g) has a high negative predictive value, safely avoiding colonoscopy in many patients with functional symptoms.
- To monitor disease: rising calprotectin predicts relapse weeks before symptoms recur, enabling proactive therapy escalation.
- To assess treatment response: a falling calprotectin correlates with mucosal healing — the treat-to-target biomarker of choice for follow-up between colonoscopies.
- Limitations: not specific to IBD. Elevated in infectious enteritis, colorectal cancer, diverticulitis, and with NSAID use. PPI use may mildly elevate it. [1]
Colonoscopy with biopsies — the diagnostic gold standard
Ileocolonoscopy with multiple biopsies from each segment (caecum, ascending, transverse, descending, sigmoid, rectum, terminal ileum) is the cornerstone of IBD diagnosis. It establishes the diagnosis, defines the extent and severity, and excludes infection and malignancy. [1]
In acute severe colitis, a flexible sigmoidoscopy (unprepared or limited preparation) is safer than full colonoscopy to avoid perforation in an inflamed, thin-walled colon. [1]
Histological features that discriminate:
- UC: continuous mucosal inflammation, crypt abscesses, goblet cell depletion, basal plasmacytosis, distortion of crypt architecture.
- Crohn's: patchy inflammation, transmural involvement, granulomas (30 per cent), fissuring. [1]
Small bowel assessment in Crohn's
Because standard colonoscopy reaches only the terminal ileum, dedicated small bowel imaging is essential when Crohn's is suspected with small bowel symptoms (right lower quadrant pain, obstructive features, B12 deficiency, weight loss). [1]
| Modality | Role |
|---|---|
| MR enterography (MRE) | Preferred first-line. No radiation. Excellent for mural oedema, strictures, fistulae, abscess, and comb sign. Repeatable for monitoring. |
| CT enterography (CTE) | Faster; preferred in acute presentations (suspected abscess, acute obstruction). Radiation limits serial use. |
| Capsule endoscopy | Most sensitive for small bowel mucosal lesions. Useful when MRE/CTE negative and suspicion remains. Contraindicated in known or suspected strictures (retention risk). |
| Intestinal ultrasound | Emerging, radiation-free, bedside tool for assessing bowel wall thickness and disease activity; growing role in monitoring. |
Perianal assessment in Crohn's
Examination under anaesthesia (EUA) is the gold standard for perianal Crohn's, combined with pelvic MRI. Endoanal ultrasound is an alternative. These map fistula anatomy (using the Parks classification) and guide surgical drainage and seton placement. Never start a biologic in suspected perianal Crohn's without first excluding abscess by imaging. [1]
Treat-to-target — the framework for all management decisions
The STRIDE-II consensus from the International Organization for the Study of IBD (IOIBD) formalised treat-to-target for IBD [10]. The targets are:
Short-term targets (within 3 months):
- Clinical remission (normal stool frequency, no bleeding, no urgency)
- Normalisation of CRP and faecal calprotectin [1]
Long-term targets (within 9 to 12 months):
- Endoscopic healing (Mayo endoscopic subscore 0 to 1 in UC; absence of ulceration in Crohn's)
- Absence of disability, restoration of quality of life, normal growth in children [1]
Adjunctive assessments (not formal targets but measured): transmural healing in Crohn's (by MRE or intestinal ultrasound), and histological healing in UC (Robarts Histopathology Index or Geboes score). [1]
DWE paradigm shift: The treat-to-target approach means steroids are no longer an endpoint — they are a bridge to maintenance therapy that achieves mucosal healing. A patient on long-term steroids without an endoscopic assessment is being under-treated. Every steroid course must have an exit strategy. [1]
Management — ulcerative colitis
Induction of remission
| Severity | Induction therapy |
|---|---|
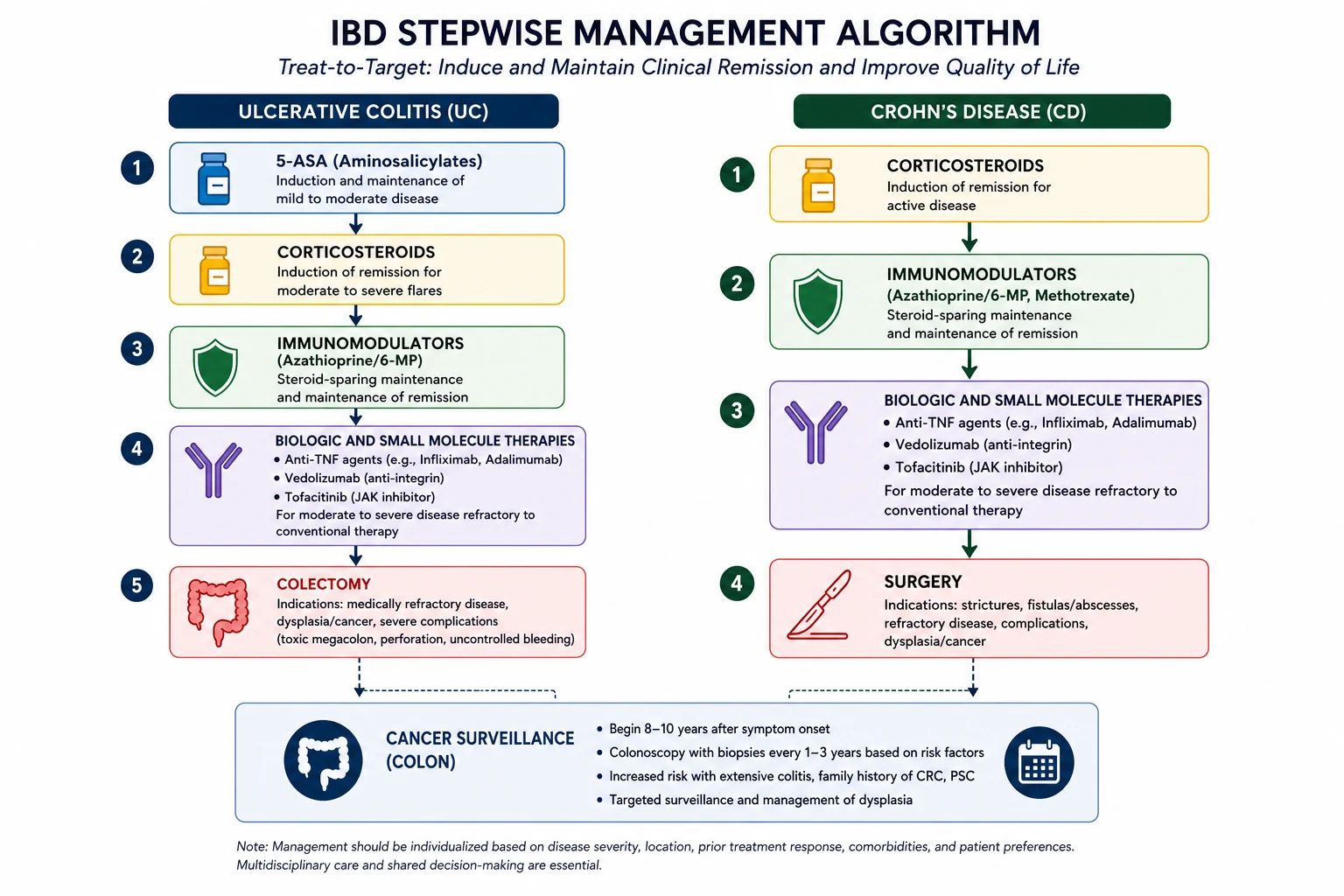
| Mild (proctitis, procotsigmoiditis) | Topical 5-ASA (mesalazine suppository for proctitis, enema for procotsigmoiditis) 1 g daily. Combine with oral 5-ASA if inadequate response. |
| Moderate | Oral prednisone 40 mg daily (taper over 8 to 12 weeks) if 5-ASA fails within 2 to 4 weeks. Budesonide-MMX 9 mg daily is a lower-systemic-side-effect alternative for mild-moderate. |
| Severe (Truelove-Witts severe) | Hospital admission. IV hydrocortisone 100 mg QID (or 100 mg every 6 hours) or methylprednisolone 60 mg daily. Assess response at 72 hours. |
The 5-ASA agents (mesalazine, sulfasalazine, balsalazide, olsalazine) are first-line for mild to moderate UC. They work topically on the colonic mucosa by inhibiting NF-kappaB and prostaglandin/leukotriene synthesis. Sulfasalazine (5-ASA linked to sulfapyridine) is especially useful when arthropathy coexists because the sulfapyridine moiety has independent anti-inflammatory effects. Dose: 2 to 4 g/day. Side effects of sulfasalazine: headache, nausea, reversible male infertility (oligospermia), rash, and Heinz body haemolytic anaemia in G6PD deficiency. [1]
Maintenance of remission
| Agent | Role |
|---|---|
| 5-ASA | First-line maintenance for all extents. At least 2 g/day. Reduces relapse and colorectal cancer risk. |
| Azathioprine / 6-MP | For steroid-dependent or frequently relapsing UC. Thiopurine methyltransferase (TPMT) testing before starting. Dose: AZA 2 to 2.5 mg/kg/day, 6-MP 1 to 1.5 mg/kg/day. Monitor FBC and LFTs regularly (myelosuppression, hepatotoxicity, pancreatitis). |
| Anti-TNF: infliximab | For moderate-severe UC refractory to immunomodulators. 5 mg/kg at weeks 0, 2, 6, then every 8 weeks. The ACT trials established efficacy for induction and maintenance [3]. Also used as rescue therapy in acute severe UC (see below). |
| Anti-TNF: adalimumab | Alternative anti-TNF. 160 mg SC, then 80 mg at week 2, then 40 mg every other week. |
| Anti-TNF: golimumab | UC only. 200 mg SC at weeks 0 and 2, then 100 mg every 4 weeks. |
| Vedolizumab | Gut-selective anti-integrin (alpha-4 beta-7). No systemic immunosuppression — preferred when anti-TNF contraindicated or malignancy/infection risk. 300 mg IV at weeks 0, 2, 6, then every 8 weeks. GEMINI I confirmed efficacy [7]. Slower onset (8 to 14 weeks). |
| Tofacitinib | Oral JAK1/3 inhibitor. 10 mg BID for 8 weeks induction, then 5 mg BID maintenance. OCTAVE trials established efficacy [8]. Rapid onset. Monitor lipids and herpes zoster. Avoid in older patients with cardiovascular or malignancy risk (post-marketing safety signal from ORAL Surveillance in rheumatoid arthritis). |
| Colectomy | Curative for UC. Indicated for refractory acute severe colitis, steroid dependence with no medical options, dysplasia or carcinoma, or toxic megacolon. J-pouch (ileoanal anastomosis) is the preferred reconstruction, avoiding permanent stoma. |
Acute severe ulcerative colitis — the emergency pathway
Acute severe UC is a medical emergency requiring inpatient management. The algorithm: [1]
-
Admit, stabilise and investigate. IV fluids, DVT prophylaxis (IBD is a prothrombotic state), stool for culture and C. difficile, abdominal X-ray to exclude toxic megacolon (transverse colon diameter greater than 6 cm), and a limited flexible sigmoidoscopy to confirm severity. [1]
-
IV corticosteroids. Hydrocortisone 100 mg QID or methylprednisolone 60 mg/day for 3 to 5 days. [1]
-
Assess response at day 3. Use objective criteria — stool frequency, CRP, and radiographic assessment. The Oxford criteria: stool frequency greater than 8/day on day 3, or CRP greater than 45 and stool frequency 3 to 8/day, predicts colectomy in 85 per cent — these patients should proceed to rescue therapy or surgery. [1]
-
Rescue therapy if steroid-refractory. Either infliximab 5 mg/kg single dose (the Järnerot study demonstrated reduced colectomy at 3 months compared to placebo [4]) or ciclosporin 2 mg/kg/day IV (or 4 mg/kg/day if lower dose not tolerated). The CYSIF trial and the CONSTRUCT trial demonstrated equipoise between infliximab and ciclosporin for short-term outcomes — the choice depends on centre experience and patient factors [5]. Ciclosporin requires monitoring of levels, renal function, magnesium, and blood pressure. Infliximab is simpler logistically and is the preferred rescue therapy in most ANZ units.
-
If rescue therapy fails, colectomy. Delaying surgery in a deteriorating patient increases mortality. The decision should be shared between gastroenterology, colorectal surgery, and the patient from admission. [1]
DWE high-yield: Infliximab and ciclosporin are equally effective as rescue therapy for steroid-refractory acute severe UC. The most common exam error is waiting too long before colectomy — early surgical involvement from admission is mandatory. [1]
Management — Crohn's disease
Induction of remission
| Phenotype | Induction therapy |
|---|---|
| Mild ileocaecal | Budesonide 9 mg daily (ileal-release formulation). Local action, low systemic bioavailability, fewer steroid side effects than prednisone. |
| Fistulising / perianal | Antibiotics: metronidazole 500 mg TDS and/or ciprofloxacin 500 mg BD for 2 to 4 weeks for sepsis control. Combined with surgical drainage and seton placement. |
| Severe or refractory | Anti-TNF (infliximab preferred for rapid control and fistulising disease), or ustekinumab, or vedolizumab. |
Maintenance of remission
| Agent | Role |
|---|---|
| Azathioprine / 6-MP / methotrexate | First-line immunomodulators for steroid-dependent or frequently relapsing Crohn's. AZA 2 to 2.5 mg/kg/day, 6-MP 1 to 1.5 mg/kg/day, methotrexate 25 mg IM/SC weekly (in patients intolerant of or not responding to thiopurines). Check TPMT before thiopurines. |
| Anti-TNF: infliximab | 5 mg/kg at weeks 0, 2, 6, then every 8 weeks. Preferred for fistulising disease and rapid control. The SONIC trial showed combination therapy (infliximab plus azathioprine) is superior to either alone for steroid-free remission and mucosal healing in immunomodulator-naive patients [2]. |
| Anti-TNF: adalimumab | 160 mg SC, then 80 mg at week 2, then 40 mg every other week. Alternative to infliximab; no infusion reactions, self-administered. |
| Anti-TNF: certolizumab pegol | Available in some regions; less commonly used in ANZ. |
| Ustekinumab | Anti-IL-12/23 (p40). IV induction (weight-based about 6 mg/kg), then 90 mg SC every 8 to 12 weeks. UNITI trials established efficacy in both anti-TNF-naive and anti-TNF-experienced patients [6]. Favorable safety profile. |
| Vedolizumab | Gut-selective. Useful when anti-TNF contraindicated. Slower onset limits use in very active disease. |
| Surgery | Not curative. Indicated for strictures (resection or strictureplasty), fistulae not responding to medical therapy, abscess drainage, and refractory disease. Over 50 per cent of Crohn's patients require at least one surgery within 10 years. Post-operative recurrence is common; start anti-TNF or immunomodulator early after resection in high-risk patients. |
Combination therapy versus monotherapy
The SONIC trial is the pivotal evidence: in biologic- and immunomodulator-naive Crohn's patients, infliximab plus azathioprine achieved steroid-free remission at week 26 in 56.8 per cent, versus 44.4 per cent for infliximab alone and 30.0 per cent for azathioprine alone [2]. Mucosal healing rates were similarly superior with combination. This underpins the "top-down" strategy for high-risk patients — those with young age, extensive disease, stricturing or penetrating behaviour, perianal disease, or rapid progression.
DWE high-yield combination therapy question: "When should you start combination anti-TNF plus immunomodulator rather than monotherapy?" Answer: combination therapy is preferred in immunomodulator-naive patients with high-risk features (young age, extensive ileocolonic disease, perianal disease, stricturing or penetrating behaviour). The SONIC trial demonstrated superiority of combination over monotherapy for steroid-free remission and mucosal healing in this group. [1]
Perianal Crohn's disease
Perianal fistulising disease is one of the most disabling complications of Crohn's and requires combined medical and surgical management. The algorithm: [1]
- Sepsis control first. EUA with drainage of abscess and loose seton placement. Never start anti-TNF in suspected undrained abscess — it will fail and may worsen sepsis.
- Pelvic MRI to map the fistula anatomy (simple versus complex, Parks classification).
- Anti-TNF therapy. Infliximab is first-line for complex perianal fistulae (adalinumab is an alternative). Antibiotics (ciprofloxacin, metronidazole) bridge to biologic response.
- Seton maintenance until the fistula closes, combined with serial EUA and imaging.
- Consider fecal diversion or proctectomy in refractory cases — up to 10 to 20 per cent of perianal Crohn's patients ultimately require proctectomy. [1]
Colitis-associated neoplasia — surveillance and dysplasia
Long-standing extensive UC and Crohn's colitis increase the risk of colorectal cancer. The risk depends on duration (begins 8 to 10 years after diagnosis), extent (pancolitis greater than left-sided greater than proctitis), concomitant PSC (markedly higher risk, start surveillance at diagnosis), family history of colorectal cancer, and ongoing active inflammation. [1]
Surveillance strategy
- Start surveillance at 8 years after diagnosis for extensive colitis (or from diagnosis if PSC is present).
- Interval: every 1 to 2 years (annually if PSC, previous dysplasia, or stricture).
- Technique: high-definition colonoscopy with dye-spray chromoendoscopy (methylene blue or indigo carmine) — this increases dysplasia detection 2- to 3-fold compared to white-light alone and is now the standard of care in high-quality units. Targeted biopsies of visible lesions plus random biopsies (though chromoendoscopy reduces the need for random biopsies). [1]
Managing dysplasia
- DALM (dysplasia-associated lesion or mass): an older term now replaced by the concept of visible dysplasia — categorised as polypoid or non-polypoid, with or without ulceration. Most visible dysplastic lesions can be removed endoscopically by EMR or ESD. Colectomy is reserved for dysplasia that cannot be resected endoscopically, multifocal high-grade dysplasia, or confirmed carcinoma.
- Invisible dysplasia (flat): confirmed by a second expert pathologist and repeat chromoendoscopy. If confirmed, colectomy is generally recommended for multifocal or high-grade lesions.
- Low-grade dysplasia: more controversial; may be managed with intensified surveillance or colectomy depending on multifocality and patient factors. [1]
5-ASA maintenance may have a chemopreventive effect, reducing colorectal cancer risk — another reason to optimise maintenance therapy. [1]
DCE long-case trap: PSC-IBD is a special phenotype. The colitis is often mild or quiescent but carries a markedly elevated colorectal cancer risk — surveillance starts at the time of PSC diagnosis and continues annually regardless of colitis activity. The colitis often shows rectal sparing and backwash ileitis. [1]
Bone health — osteoporosis
Chronic inflammation (IL-1, IL-6, TNF activating osteoclasts), corticosteroid use, hypogonadism, malnutrition, and low body mass index all contribute to osteoporosis and fracture risk in IBD. The risk is highest in post-menopausal women, those on repeated steroid courses, and those with extensive small bowel Crohn's (malabsorption of calcium and vitamin D). [1]
Management:
- DEXA scan at diagnosis and periodically for patients on long-term steroids or with other risk factors.
- Calcium 1000 to 1200 mg/day and vitamin D 800 to 1000 IU/day supplementation.
- Bisphosphonate (alendronate 70 mg weekly, or zoledronic acid 5 mg IV annually) for patients on long-term steroids (greater than 3 months at prednisone 5 mg or more) or with T-score below -2.5.
- Minimise corticosteroid exposure by optimising maintenance therapy — this is the single most effective bone-preserving strategy. [1]
Nutritional support
Malnutrition affects up to 70 per cent of Crohn's patients and 20 to 40 per cent of UC patients at some point. Causes include reduced oral intake (food fear), malabsorption (extensive small bowel disease or resection), increased metabolic demands (inflammation), and medication effects. [1]
Specific deficiencies:
- Iron deficiency: oral iron poorly tolerated in active colitis (worsens oxidative stress); IV iron (ferric carboxymaltose or iron isomaltoside) preferred for moderate-severe deficiency.
- B12 deficiency: terminal ileal disease or resection of more than 60 cm. Check levels; supplement 1000 microg IM every 3 months if deficient.
- Vitamin D and calcium: as above.
- Zinc, magnesium, fat-soluble vitamins: in extensive small bowel disease or short bowel syndrome. [1]
Exclusive enteral nutrition (EEN) has a specific role in paediatric Crohn's — an 8-week liquid diet (polymeric or elemental formula) induces remission in 60 to 80 per cent, with the advantage of promoting growth (no steroid suppression). Less used in adults but a steroid-sparing option. [1]
Pregnancy in IBD
Most women with well-controlled IBD have normal fertility and pregnancy outcomes. The key principles: [1]
- Control disease before conception. Active disease at conception increases the risk of flare during pregnancy, preterm delivery, low birth weight, and miscarriage. Aim for remission for 3 to 6 months before conceiving. Quiescent IBD at conception usually stays quiescent through pregnancy.
- Continue maintenance therapy. Most IBD medications are safe in pregnancy and lactation: 5-ASA, azathioprine/6-MP (low thiopurine metabolite levels, no teratogenicity signal), anti-TNF agents (infliximab, adalimumab — continue through pregnancy; stop vedolizumab and ustekinumab data is growing and reassuring), and methotrexate (strictly contraindicated — abortifacient and teratogenic). Tofacitinib has limited pregnancy safety data — avoid if possible.
- Anti-TNF transfer to fetus. Infliximab and adalimumab cross the placenta in the third trimester (active transplacental transport). The infant may have detectable drug levels for up to 6 months. Defer live vaccines (rotavirus, BCG) for the first 6 months in infants exposed in utero to anti-TNF; killed vaccines are safe.
- Delivery mode. Vaginal delivery is preferred. Caesarean section is recommended for patients with active perianal Crohn's disease (to avoid sphincter trauma and fistula recurrence) and may be considered for patients with a J-pouch (to protect the anal sphincter and pouch function).
- Colonoscopy during pregnancy is reserved for strong indications (severe flare, suspected malignancy); flexible sigmoidoscopy with minimal sedation is safer. [1]
DWE high-yield pregnancy question: "Which IBD medications must be stopped in pregnancy?" Answer: methotrexate (teratogenic and abortifacient, stop 3 to 6 months before conception) and thalidomide. Continue 5-ASA, thiopurines, and anti-TNF agents throughout pregnancy. Defer live vaccines in infants exposed to anti-TNF in utero for the first 6 months. [1]
Prognosis
IBD is a chronic relapsing-remitting disease. With modern treat-to-target therapy aiming for mucosal healing, outcomes have improved substantially. [1]
| Outcome | UC | Crohn's |
|---|---|---|
| Colectomy at 10 years | About 10 per cent overall; 20 to 30 per cent for those presenting with acute severe colitis | 40 to 50 per cent require at least one bowel resection |
| Mortality | Near-normal with optimal treatment | Slightly increased (surgery, malignancy, sepsis) |
| Colorectal cancer | Increased after 8 to 10 years of extensive colitis; higher with PSC | Increased in colonic Crohn's |
| Quality of life | Good with remission; J-pouch restores near-normal bowel function | Variable; perianal disease and short bowel syndrome are major burdens |
The life expectancy of well-managed IBD patients now approaches that of the general population. [1]
DCE long-case approach
Opening statement (SASPOP)
"Ms Sarah Williams is a 32-year-old primary school teacher who presents with a 6-week history of bloody diarrhoea (8 to 10 stools per day), cramping lower abdominal pain, urgency and 4 kg weight loss. She has a past history of ulcerative colitis (pancolitis) diagnosed 6 years ago, currently managed with mesalazine 2 g daily. She also has a 2-year history of erythema nodosum and mild peripheral arthritis affecting her knees. [1]
Her main problems are:
- Moderately severe ulcerative colitis flare — Truelove-Witts severe (more than 6 bloody stools, HR 96, Hb 102)
- Extraintestinal manifestations — erythema nodosum and peripheral arthritis tracking bowel activity
- Anaemia of chronic disease with iron deficiency
- Risk of colitis-associated neoplasia (6 years pancolitis — surveillance due in 2 years)
- Psychosocial impact — time off work, anxiety about flare progression [1]
My immediate management priorities are stool studies to exclude infection (especially C. difficile), hospital admission for IV hydrocortisone, flexible sigmoidoscopy to assess severity, and a plan for step-up to anti-TNF or vedolizumab if steroid-refractory. I will also address her iron deficiency, DVT prophylaxis, and bone health." [1]
Integrated management plan
- Admit and investigate — stool culture and C. difficile toxin; FBC, CRP, iron studies, albumin; abdominal X-ray to exclude toxic megacolon; limited flexible sigmoidoscopy.
- IV hydrocortisone 100 mg QID; assess response at day 3. [1]3. If steroid-refractory — infliximab 5 mg/kg as rescue therapy (or ciclosporin per local protocol).
- Iron repletion — IV ferric carboxymaltose (oral iron poorly tolerated in active colitis).
- DVT prophylaxis — enoxaparin 40 mg SC daily (IBD is a prothrombotic state; acute flare increases VTE risk). [1]6. Maintenance escalation — plan to move from 5-ASA to azathioprine or anti-TNF if steroid-dependent or frequently relapsing.
- Extraintestinal manifestations — will resolve with bowel treatment (activity-related).
- Bone health — DEXA and calcium/vitamin D if steroid course prolonged.
- Communication — explain the flare, the treatment plan, the role of biologics, and the surveillance timeline. Address her anxiety about work and disease progression. [1]
DCE examiner probing questions you must anticipate:
- "How would you assess her response at day 3?" → Oxford criteria: stool frequency more than 8/day, or CRP more than 45 with stool frequency 3 to 8/day, predicts colectomy in 85 per cent — proceed to rescue therapy.
- "Why is she at risk of VTE?" → IBD is a prothrombotic state (inflammation, thrombocytosis, immobilisation); acute severe colitis carries a VTE risk comparable to post-surgical patients.
- "How would her management change if she were pregnant?" → Continue 5-ASA and anti-TNF; avoid methotrexate; defer live vaccines in the infant if anti-TNF used in third trimester.
- "What is her colorectal cancer surveillance strategy?" → Start at 8 years after diagnosis (2 years from now); chromoendoscopy every 1 to 2 years; annual if PSC. [1]
DCE short-case approach: abdominal and skin examination
Instruction: "Examine this patient's abdominal system." [1]
Systematic routine
- End of bed — cachexia, pallor (anaemia), signs of steroid use (moon face, central obesity, striae, bruising), aphthous ulcers (oral Crohn's), erythema nodosum on shins.
- Hands — clubbing (Crohn's, PSC-UC), palmar erythema, aphthous ulceration, peripheral arthritis (swollen knee joints).
- Eyes — episcleritis (red conjunctiva), uveitis (painful red eye with photophobia).
- Skin — erythema nodosum (tender red nodules on anterior shins), pyoderma gangrenosum (ulcer with undermined edges on legs), aphthous stomatitis.
- Abdomen — scars from previous surgery (right hemicolectomy scar in Crohn's), palpable mass (Crohn's phlegmon or abscess in right iliac fossa), tenderness, hepatomegaly or splenomegaly (PSC), stoma site.
- Perineum — skin tags, fissures, fistulae, abscess, scarring from previous surgery (the most commonly missed area).
- Joints — sacroiliitis (sacroiliac joint tenderness, decreased lumbar spine mobility), peripheral arthritis. [1]
Presentation template
"I examined Ms Williams' abdominal system. She has a moon face and central obesity consistent with corticosteroid use. There are tender erythematous nodules on the anterior shins consistent with erythema nodosum, and an aphthous ulcer on the buccal mucosa. There is no clubbing, episcleritis or uveitis. The abdomen is soft with mild left iliac fossa tenderness. There is no palpable mass, hepatosplenomegaly or stoma. Bowel sounds are normal. On perianal examination there is no fissure, fistula or skin tag. There is no peripheral arthritis or sacroiliitis today. [1]
These findings are consistent with an ulcerative colitis flare with an activity-related extraintestinal manifestation (erythema nodosum). I would like to take a full medication and surgical history, organise a stool panel and inflammatory markers, and proceed to flexible sigmoidoscopy to assess severity." [1]
Key DWE MCQ patterns
- Which agent is contraindicated in pregnancy? Methotrexate (not 5-ASA, thiopurines, or anti-TNF).
- Which rescue therapy for steroid-refractory acute severe UC? Infliximab 5 mg/kg or ciclosporin 2 mg/kg/day IV — both equally effective. [1]3. Which drug combination is superior in immunomodulator-naive Crohn's? Infliximab plus azathioprine (SONIC).
- Which gene is the strongest susceptibility locus for Crohn's? NOD2.
- Which extraintestinal manifestation runs an independent course? Axial spondyloarthritis, PSC, uveitis, pyoderma gangrenosum (not erythema nodosum or Type 1 peripheral arthritis).
- Which small molecule is an oral JAK inhibitor for UC? Tofacitinib.
- Which biologic targets IL-12/23? Ustekinumab.
- Which imaging is preferred for small bowel Crohn's? MR enterography.
- Which technique improves dysplasia detection in colitis surveillance? Dye-spray chromoendoscopy.
- How does smoking affect UC versus Crohn's? Protective in UC, worsens Crohn's. [1]
References
[1] Khor, Gardet, Xavier (2011) — IBD genetics and pathogenesis: NOD2 and ATG16L1 converge on autophagy; over 200 susceptibility loci identified. [2] SONIC (Colombel, 2010) — Combination infliximab plus azathioprine superior to monotherapy for steroid-free remission and mucosal healing in immunomodulator-naive Crohn's. [3] ACT 1 and ACT 2 (Rutgeerts, 2005) — Infliximab effective for induction and maintenance in moderate-severe UC. [4] Järnerot (2005) — Infliximab as rescue therapy reduces 3-month colectomy in steroid-refractory acute severe UC. [5] CYSIF (Laharie, 2012) — Ciclosporin and infliximab equally effective for steroid-refractory acute severe UC. [6] UNITI (Feagan, 2016) — Ustekinumab (anti-IL-12/23) effective for induction and maintenance in Crohn's. [7] GEMINI I (Feagan, 2013) — Vedolizumab (gut-selective anti-integrin) effective for induction and maintenance in UC. [8] OCTAVE (Sandborn, 2017) — Tofacitinib (oral JAK inhibitor) effective for induction and maintenance in UC. [9] Menees (2015) — Meta-analysis: faecal calprotectin is the best non-invasive test to exclude IBD in IBS-like presentations. [10] STRIDE-II (Turner, 2021) — Treat-to-target for IBD: clinical remission plus endoscopic healing as long-term targets; CRP and calprotectin normalisation as short-term targets.
GESA consensus on IBD management; ECCO guidelines on UC, Crohn's and perianal disease; BSG consensus on IBD management; ACG clinical guidelines on UC and Crohn's. [1]
References
- [1]Khor B, Gardet A, Xavier RJ Genetics and pathogenesis of inflammatory bowel disease Nature, 2011.PMID 21677747
- [2]Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn's disease N Engl J Med, 2010.PMID 20393175
- [3]Rutgeerts P, Sandborn WJ, Feagan BG, et al. Infliximab for induction and maintenance therapy for ulcerative colitis N Engl J Med, 2005.PMID 16339095
- [4]Järnerot G, Hertervig E, Friis-Liby I, et al. Infliximab as rescue therapy in severe to moderately severe ulcerative colitis: a randomized, placebo-controlled study Gastroenterology, 2005.PMID 15940615
- [5]Laharie D, Bourreille A, Branche J, et al. Ciclosporin versus infliximab in patients with severe ulcerative colitis refractory to intravenous steroids: a parallel, open-label randomised controlled trial Lancet, 2012.PMID 23063316
- [6]Feagan BG, Sandborn WJ, Gasink C, et al. Ustekinumab as Induction and Maintenance Therapy for Crohn's Disease N Engl J Med, 2016.PMID 27959607
- [7]Feagan BG, Rutgeerts P, Sands BE, et al. Vedolizumab as induction and maintenance therapy for ulcerative colitis N Engl J Med, 2013.PMID 23964932
- [8]Sandborn WJ, Su C, Sands BE, et al. Tofacitinib as Induction and Maintenance Therapy for Ulcerative Colitis N Engl J Med, 2017.PMID 28467869
- [9]Menees SB, Powell C, Kurlander J, et al. A meta-analysis of the utility of C-reactive protein, erythrocyte sedimentation rate, fecal calprotectin, and fecal lactoferrin to exclude inflammatory bowel disease in adults with IBS Am J Gastroenterol, 2015.PMID 25732419
- [10]Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD Gastroenterology, 2021.PMID 33359090