Phys · gastrointestinal
Obstructive (Surgical) Jaundice
Also known as obstructive jaundice · surgical jaundice · post-hepatic jaundice · extrahepatic biliary obstruction · cholestatic jaundice · choledocholithiasis · malignant biliary obstruction · ascending cholangitis
Consultant-physician-depth guide to obstructive (surgical) jaundice — bilirubin above 50 micromol per litre with predominant conjugated hyperbilirubinaemia, elevated alkaline phosphatase and gamma-GT, pale stools, dark urine, and pruritus. Causes classified by the level of obstruction: extrahepatic (choledocholithiasis as the most common cause, pancreatic head cancer, cholangiocarcinoma, ampullary cancer, biliary stricture, parasitic obstruction, biliary atresia, Mirizzi syndrome, pancreatitis) and intrahepatic cholestasis (drugs, PBC, PSC, viral hepatitis, sepsis, Dubin-Johnson and Rotor, intrahepatic cholestasis of pregnancy). The diagnostic approach from history (biliary colic versus painless jaundice, weight loss, Charcot triad) and examination (Courvoisier sign, scratch marks, asterixis) through investigations (LFT pattern, GGT, coagulation, CA 19-9, ultrasound first-line, MRCP gold-standard, CT for pancreatic mass, EUS-FNA, ERCP therapeutic). Management of the underlying cause, biliary drainage, the Tokyo Guidelines 2018 for cholangitis, pre-operative optimisation with vitamin K, and palliative care for advanced malignancy. Structured for FRACP DWE and DCE, MRCP, and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Obstructive (Surgical) Jaundice

The answer first
Obstructive (surgical) jaundice is the syndrome of impaired bile flow from the liver to the duodenum, producing a predominantly conjugated (direct) hyperbilirubinaemia above 50 micromol per litre, a markedly elevated alkaline phosphatase and gamma-glutamyl transferase, pale (acholic) stools, dark urine, and intractable pruritus. The obstruction may be extrahepatic — a physical blockage anywhere from the right and left hepatic ducts through the common hepatic duct, common bile duct, and ampulla of Vater — or it may reflect intrahepatic cholestasis, where the hepatocyte or canalicular secretory machinery fails without a mechanical blockage. The distinction is the central diagnostic task, because the two groups share an identical biochemistry but demand entirely different management [2].
The single most important clinical pivot is the history. Jaundice preceded by biliary colic (right upper quadrant pain radiating to the back or shoulder, lasting hours, with nausea) points to choledocholithiasis — a gallstone that has migrated from the gallbladder into the common bile duct — which is the most common cause of obstructive jaundice overall. Painless, progressive jaundice with weight loss in an older patient points to malignancy — most often pancreatic head adenocarcinoma, but also cholangiocarcinoma and ampullary cancer. Fever, rigors, jaundice, and right upper quadrant pain (Charcot triad) herald acute ascending cholangitis, a life-threatening infection of an obstructed biliary tree that mandates urgent drainage [1].
DCE trap: The biggest error in obstructive jaundice is stopping at the biochemical diagnosis of cholestasis and forgetting to localise the obstruction. Every jaundiced patient with a cholestatic liver function pattern requires imaging to distinguish extrahepatic obstruction (which needs drainage or surgery) from intrahepatic cholestasis (which needs a cause-directed workup and never an ERCP). Ultrasound is the first-line test; MRCP is the gold-standard non-invasive biliary imaging; CT stages malignancy; ERCP is therapeutic. [1]
Definition and pathophysiology — why the pattern arises
Jaundice (icterus) is clinically visible when the serum bilirubin exceeds approximately 40 to 50 micromol per litre. The classification into pre-hepatic (haemolytic), hepatic (hepatocellular), and post-hepatic (obstructive) is based on where in the bilirubin metabolic pathway the disruption occurs. [1]
Bilirubin metabolism — the pathway every candidate must draw
Bilirubin is the end-product of heme catabolism. Senescent red cells are phagocytosed by reticuloendothelial (Kupffer) cells, and heme is converted by heme oxygenase to biliverdin and then to unconjugated bilirubin. Unconjugated bilirubin is lipid-soluble, bound to albumin in plasma, and cannot be excreted by the kidney (it does not appear in urine). In the hepatocyte, bilirubin is conjugated by UDP-glucuronosyltransferase on the smooth endoplasmic reticulum to form conjugated (direct) bilirubin, which is water-soluble and actively secreted into the bile canaliculus against a concentration gradient. [1]
Conjugated bilirubin travels through the biliary tree to the duodenum, where gut bacteria convert it to urobilinogen and then to stercobilin (the brown pigment of stool). A fraction of urobilinogen is reabsorbed and re-excreted by the kidney (the enterohepatic circulation). [1]
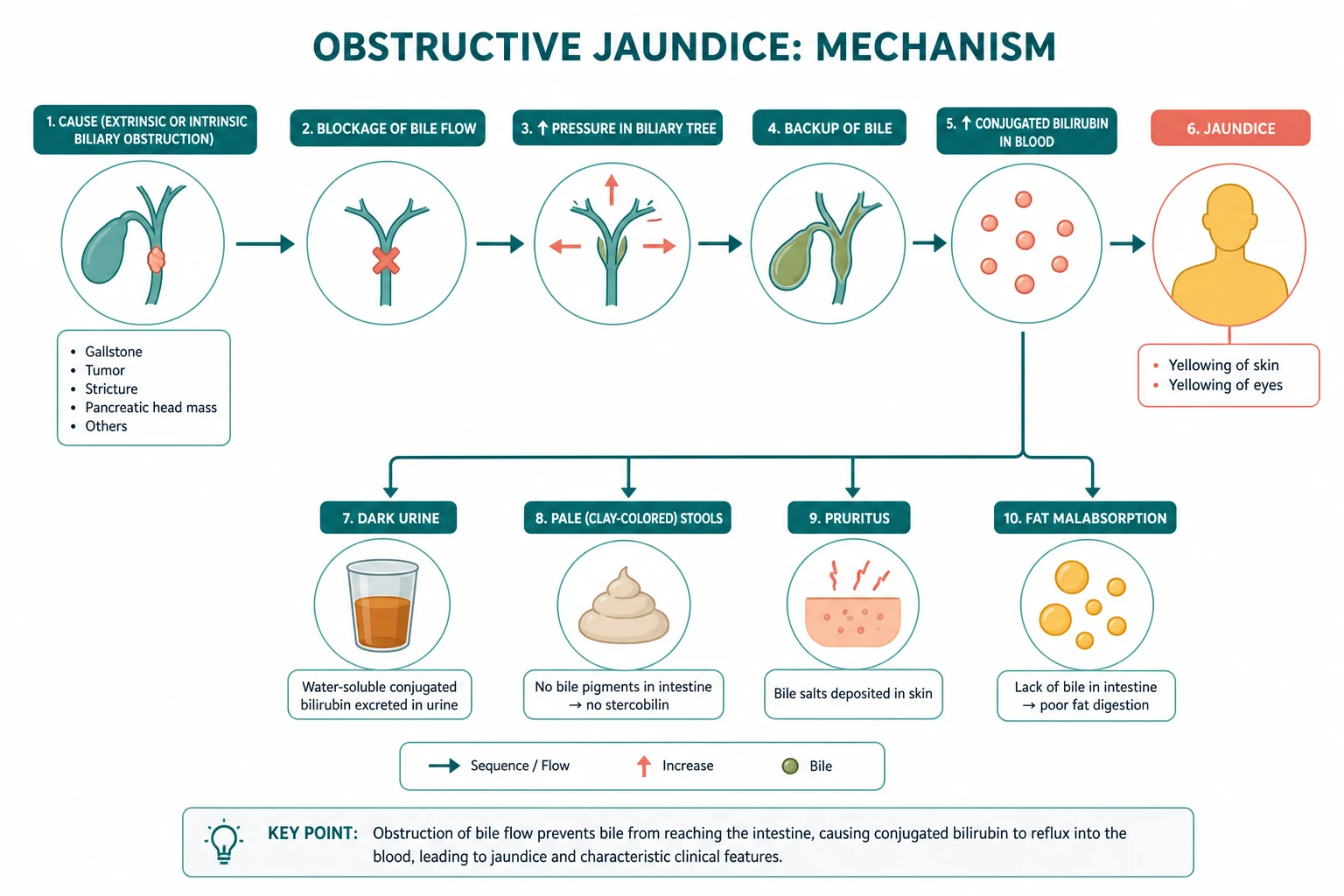
Where obstruction interrupts the pathway
When the common bile duct is obstructed, conjugated bilirubin cannot reach the gut. It refluxes back into the bloodstream (because hepatic conjugation continues but biliary excretion is blocked), producing a predominantly conjugated hyperbilirubinaemia. Because conjugated bilirubin is water-soluble and loosely albumin-bound, it is filtered by the glomerulus and appears in the urine — giving the dark (tea-coloured) urine that is the hallmark of obstructive jaundice. At the same time, because little or no bilirubin reaches the gut, stercobilin is absent and the stools become pale (acholic, clay-coloured). [1]
DWE high-yield mechanism question: "Why does obstructive jaundice produce dark urine and pale stools, while haemolytic jaundice produces normal-coloured stools and urine that is only positive for urobilinogen?" Answer: In obstruction, conjugated bilirubin is water-soluble, refluxes into blood, and is excreted in urine (dark urine); none reaches the gut to form stercobilin (pale stools). In haemolysis, the excess unconjugated bilirubin is conjugated and normally excreted into the gut, producing excess stercobilin (dark stools) and excess reabsorbed urobilinogen (urine urobilinogen positive), but no bilirubinuria because unconjugated bilirubin is albumin-bound and not filtered. [1]
The cholestatic enzyme pattern
Biliary obstruction causes the cholestatic pattern: a markedly elevated alkaline phosphatase (ALP), an elevated gamma-glutamyl transferase (GGT), and a mildly elevated or normal bilirubin, with only modest transaminase elevation. ALP rises because biliary obstruction induces the synthesis of ALP by hepatocytes and canalicular cells and impairs its secretion. The GGT is useful because it confirms the hepatic origin of an elevated ALP — bone ALP does not raise the GGT. The transaminases (ALT, AST) rise only modestly because the hepatocytes themselves are not the primary site of injury (unless there is superimposed hepatocellular damage from prolonged obstruction or cholangitis). [1]
The coagulopathy of obstruction
Bile is required for the absorption of fat-soluble vitamins A, D, E, and K. In prolonged obstruction, vitamin K malabsorption depletes the vitamin K-dependent clotting factors (II, VII, IX, and X), producing a prolonged prothrombin time (elevated INR). This is a critical pre-operative consideration: a jaundiced patient going to surgery or ERCP must have the coagulation profile checked and corrected. The key teaching point is that vitamin K corrects the coagulopathy of obstructive jaundice (because the liver can still synthesise the factors if given vitamin K), whereas the coagulopathy of hepatocellular failure does not correct with vitamin K (because the liver cannot synthesise the factors at all). This distinction is a classic DWE discriminator. [1]
Causes — classified by the level of obstruction
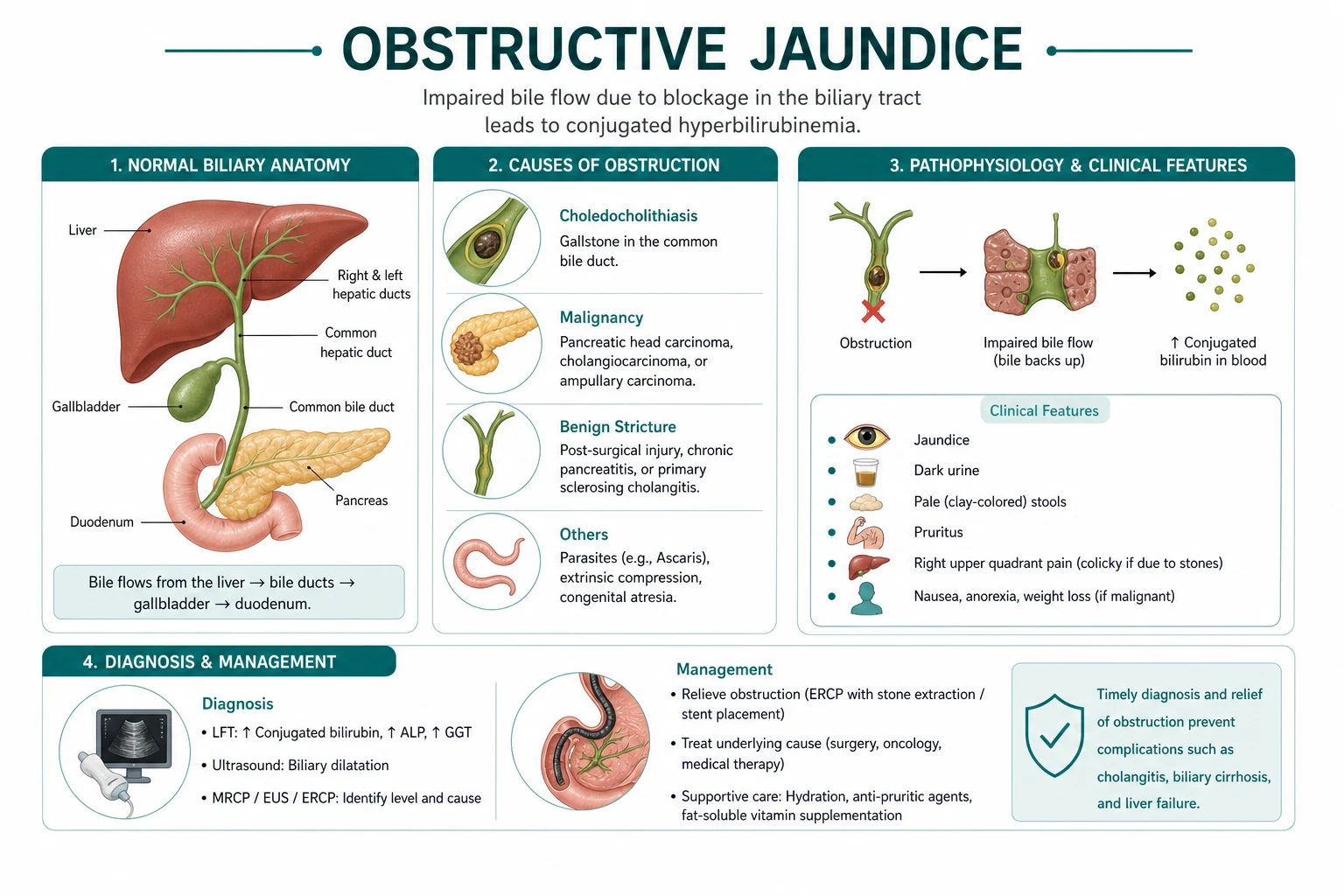
The causes of obstructive jaundice are classified by whether the obstruction is extrahepatic (a mechanical blockage of the bile ducts, potentially amenable to drainage or surgery) or intrahepatic (cholestasis at the hepatocyte or canalicular level, without a ductal blockage). The two share an identical biochemistry, so the distinction is made by imaging — dilated ducts indicate extrahepatic obstruction; non-dilated ducts indicate intrahepatic cholestasis. [1]
Extrahepatic causes — the surgical jaundice
| Cause | Key features | Exam-relevant points |
|---|---|---|
| Choledocholithiasis | Most common cause; biliary colic followed by jaundice; RUQ pain | Stone in CBD from gallbladder migration; ERCP extraction + cholecystectomy [2] |
| Pancreatic head cancer | Painless progressive jaundice, weight loss, Courvoisier sign | Head of pancreas; Whipple if resectable; poor prognosis [3] |
| Cholangiocarcinoma | Painless jaundice, pruritus; may arise anywhere in biliary tree | Klatskin tumour at bifurcation; PSC is a risk factor [7] |
| Ampullary cancer | Painless jaundice, may have intermittent jaundice and anaemia (GI blood loss) | Arises at ampulla of Vater; better prognosis than pancreatic cancer if resected early |
| Biliary stricture | Post-cholecystectomy (most common), chronic pancreatitis, PSC | Distinguish benign from malignant with imaging and brushings [7] |
| Parasitic obstruction | Ascaris lumbricoides, liver flukes (Clonorchis, Opisthorchis) | Endemic in Asia; causes recurrent cholangitis and cholangiocarcinoma |
| Biliary atresia | Neonatal jaundice, pale stools, dark urine | Kasai portoenterostomy before 60 days of life; paediatric emergency |
| Mirizzi syndrome | Stone impacted in cystic duct or Hartmann pouch compressing CHD | Risk of cholecystocholedochal fistula; identifies cystic duct carefully at surgery |
| Pancreatitis | Acute (oedematous head compressing CBD) or chronic (fibrotic stricture) | Resolves with acute episode; chronic stricture may need stenting |
Intrahepatic cholestasis — the medical jaundice
Intrahepatic cholestasis produces the same biochemistry (conjugated hyperbilirubinaemia, elevated ALP and GGT) but without ductal dilatation on imaging. The causes are diverse: [1]
- Drug-induced cholestasis — flucloxacillin, chlorpromazine, anabolic steroids, amoxicillin-clavulanate, erythromycin, oral contraceptives, ciclosporin. A careful drug history is essential and the cholestasis usually resolves on withdrawal.
- Primary biliary cholangitis (PBC) — middle-aged woman, fatigue and pruritus, antimitochondrial antibody (AMA) positive, elevated IgM, small bile duct destruction.
- Primary sclerosing cholangitis (PSC) — young man with inflammatory bowel disease (ulcerative colitis), multifocal biliary strictures and beading on MRCP, ANCA positive, markedly elevated ALP, and a markedly increased risk of cholangiocarcinoma [7].
- Viral hepatitis — hepatocellular pattern with cholestatic features, especially hepatitis A and E.
- Sepsis — systemic infection can impair hepatocellular bile secretion; the cholestasis resolves with treatment of the infection.
- Dubin-Johnson syndrome — benign inherited defect in canalicular excretion of conjugated bilirubin (MRP2), producing chronic mild conjugated hyperbilirubinaemia with a black liver. Rotor syndrome is similar without the black pigment.
- Intrahepatic cholestasis of pregnancy (ICP) — third trimester pruritus and elevated bile acids, resolves after delivery, associated with fetal prematurity and stillbirth.
DCE trap: The cardinal error is performing an ERCP on a patient with intrahepatic cholestasis. A patient with a cholestatic LFT pattern and a non-dilated biliary tree on ultrasound and MRCP does not have a mechanical obstruction and will not benefit from ERCP — in fact, ERCP risks pancreatitis and cholangitis for no therapeutic gain. Pursue the intrahepatic cause (drugs, PBC, PSC, sepsis) with serology and biopsy instead. [1]
Clinical presentation — the history is the diagnostic compass
The history is the single most powerful discriminator in obstructive jaundice, because the tempo and associated symptoms narrow the differential before any imaging is done. [1]
The painful versus painless distinction
Biliary colic preceding jaundice is the hallmark of choledocholithiasis. The pain is typically in the right upper quadrant or epigastrium, may radiate to the right shoulder tip or the back, builds to a crescendo over minutes, plateaus for several hours, and is often associated with nausea and vomiting. The jaundice develops as the stone obstructs the common bile duct; if the stone disimpacts and passes, the jaundice and pain may resolve spontaneously, producing the intermittent jaundice that is characteristic of ampullary obstruction (stone or tumour). [1]
Painless progressive jaundice is the hallmark of malignancy — most often pancreatic head adenocarcinoma. The jaundice is typically deep and progressive, accompanied by weight loss, anorexia, and new-onset diabetes (the pancreatic cancer may destroy islet cells or produce paraneoplastic glucose intolerance). Pruritus may be severe and precede the visible jaundice by weeks. Courvoisier sign — a palpable, non-tender gallbladder in a jaundiced patient — strongly suggests a malignant obstruction distal to the cystic duct, because the slow, progressive obstruction distends a thin-walled, compliant gallbladder [5].
Charcot triad and Reynolds pentad — cholangitis
Charcot triad — fever (often with rigors), jaundice, and right upper quadrant pain — is the classic clinical presentation of acute ascending cholangitis, present in about 50 to 70 per cent of cases. The addition of hypotension and altered mental state constitutes Reynolds pentad, indicating severe disease with septic shock. Cholangitis is a medical and biliary emergency: the obstructed biliary tree is colonised by gut organisms (principally Escherichia coli, Klebsiella, Enterococcus, and anaerobes), and the raised intrabiliary pressure forces bacteria and endotoxin into the systemic circulation (cholangio-venous reflux), producing systemic sepsis [1].
Other key historical features
- Pale stools and dark urine — the cardinal features of complete biliary obstruction. The patient may notice that the urine is the colour of strong tea or cola and that the stool is pale, putty-coloured, and difficult to flush.
- Pruritus — may be severe and intractable, worse at night, caused by bile salt deposition in the skin. It may precede visible jaundice.
- Weight loss and anorexia — suggest malignancy but are non-specific.
- Fever and rigors — suggest cholangitis.
- Drug history — flucloxacillin, chlorpromazine, anabolic steroids, amoxicillin-clavulanate, erythromycin, oral contraceptives.
- Travel history — parasitic obstruction (Ascaris, liver flukes) in endemic regions.
- Past medical history — inflammatory bowel disease (PSC), previous biliary surgery (stricture), chronic pancreatitis (stricture), biliary colic (stones).
- Family history — hereditary syndromes (Dubin-Johnson), pancreatic cancer kindreds. [1]
Physical examination
The physical examination of a jaundiced patient serves two purposes: to assess the severity (signs of hepatic failure, sepsis) and to narrow the differential (signs of chronic liver disease, malignancy, or a palpable gallbladder). [1]
General inspection and vital signs
Inspect for the depth of jaundice (scleral icterus first, then cutaneous), scratch marks and excoriations (pruritus), cachexia (malignancy, chronic disease), and the stigmata of chronic liver disease (spider naevi, palmar erythema, gynaecomastia, caput medusae, testicular atrophy, parotid enlargement) which, if present, suggest a hepatocellular rather than a purely obstructive cause. Check the vital signs meticulously: fever and tachycardia suggest cholangitis; hypotension and confusion signal Reynolds pentad and septic shock. [1]
Abdominal examination — the critical signs
- Courvoisier sign — a palpable, non-tender, distended gallbladder in a jaundiced patient. The law states that in the presence of jaundice, a palpable gallbladder is unlikely to be due to gallstones (because chronic stone disease thickens and fibroses the gallbladder wall, preventing distension) and is more likely due to malignancy (which causes slow, progressive obstruction of a compliant gallbladder). The modern evidence is that Courvoisier sign has low sensitivity (about 26 to 55 per cent) but moderate-to-high specificity (83 to 90 per cent) for malignancy [5]. The absence of a palpable gallbladder does not exclude malignancy; its presence strongly suggests it.
- Right upper quadrant tenderness — suggests acute cholecystitis or cholangitis (Murphy sign).
- Epigastric mass — may represent a pancreatic head tumour.
- Hepatomegaly — a smooth, enlarged liver may reflect biliary obstruction or metastatic infiltration; a hard, nodular liver suggests malignancy.
- Ascites — suggests peritoneal malignancy, portal hypertension, or hepatic failure.
- Splenomegaly — suggests portal hypertension or haemolysis.
Signs of hepatic failure and encephalopathy
Assess for asterixis (the flapping tremora of hepatic encephalopathy), constructional apraxia (inability to draw a five-pointed star or write legibly), and the grade of encephalopathy. These signs indicate hepatocellular failure rather than simple obstruction and dramatically alter the prognosis and management. [1]
Investigations — the staged imaging strategy
The investigation of obstructive jaundice follows a staged imaging strategy that proceeds from the least invasive and most accessible to the most definitive and potentially therapeutic. The goal is to (1) confirm the cholestatic biochemistry, (2) determine whether the obstruction is extrahepatic or intrahepatic, (3) localise the level and characterise the cause of an extrahepatic obstruction, and (4) obtain tissue for a malignant diagnosis. [1]
Blood tests — the foundation
- Liver function tests — the cholestatic pattern: conjugated bilirubin (elevated, often above 50 micromol per litre), ALP (markedly elevated, typically more than three times the upper limit of normal), GGT (elevated, confirming hepatic ALP origin), ALT and AST (mildly elevated or normal). The ratio of ALP to transaminases is high in obstruction.
- Coagulation studies — prothrombin time and INR. Prolonged in obstructive jaundice from vitamin K malabsorption; corrects with vitamin K.
- Full blood count — leucocytosis suggests cholangitis; anaemia may indicate malignancy or haemolysis.
- Amylase or lipase — elevated in gallstone pancreatitis complicating ampullary obstruction.
- Tumour markers — CA 19-9 for pancreatic and biliary malignancy. It has a sensitivity of approximately 79 to 81 per cent and a specificity of 82 to 90 per cent for pancreatic adenocarcinoma in symptomatic patients, but it is falsely elevated in cholangitis and biliary obstruction and falsely normal in Lewis-antigen-negative individuals (5 to 10 per cent of the population) who cannot synthesise CA 19-9 [4]. It is therefore a monitoring, not a screening, marker. CEA may be modestly useful in cholangiocarcinoma.
- Viral and autoimmune serology — hepatitis A, B, C, E serology; antimitochondrial antibody (PBC); ANA, ANCA, immunoglobulins (PSC, autoimmune hepatitis) — performed when intrahepatic cholestasis is suspected.
Ultrasound — the first-line imaging
Abdominal ultrasound is the first-line imaging modality in any patient with obstructive jaundice. It is cheap, widely available, non-invasive, and does not use radiation. Its key tasks are to (1) identify gallbladder stones, (2) detect common bile duct dilatation (a CBD above 6 to 7 mm, increasing with age and post-cholecystectomy), (3) assess the gallbladder wall and identify signs of acute cholecystitis, and (4) screen for hepatic metastases or a pancreatic mass. The principal limitation of ultrasound is poor visualisation of the distal common bile duct (obscured by overlying bowel gas), so a normal ultrasound does not exclude a distal CBD stone or a small pancreatic head lesion [2].
DWE trap: The most common imaging error is concluding that obstruction is excluded because ultrasound showed a non-dilated CBD. The distal CBD is often not seen on ultrasound, and an obstructing stone may be present without marked dilatation (especially if the obstruction is recent or intermittent). A patient with a cholestatic LFT pattern and gallstones requires further imaging (MRCP or EUS) to exclude choledocholithiasis even if the ultrasound shows no CBD dilatation. [1]
MRCP — the gold-standard non-invasive biliary imaging
Magnetic resonance cholangiopancreatography (MRCP) is the gold-standard non-invasive test for the biliary tree. It uses heavily T2-weighted sequences to image the static fluid in the biliary and pancreatic ducts without requiring contrast or cannulation. It has a sensitivity above 90 per cent for common bile duct stones and strictures and excellent specificity. MRCP is preferred over diagnostic ERCP because it carries no risk of pancreatitis, bleeding, perforation, or cholangitis — the complications that limit ERCP. It is the test of choice to confirm or exclude choledocholithiasis in a patient with an intermediate pre-test probability, and to characterise biliary strictures (PSC beading, cholangiocarcinoma, post-surgical) [2].
CT — staging malignancy
Contrast-enhanced triple-phase (pancreatic protocol) computed tomography is the investigation of choice when a pancreatic mass is suspected or confirmed. It stages the tumour for resectability by assessing (1) the size and location of the primary, (2) vascular involvement — particularly encasement of the superior mesenteric artery, superior mesenteric vein, and portal vein (which renders the tumour locally advanced and unresectable for cure), and (3) distant metastases (liver, peritoneum, lungs). CT is more reliable than ultrasound for visualising the pancreas and the distal CBD and is essential for the staging workup of pancreatic and biliary malignancy [3].
EUS — small lesions and tissue
Endoscopic ultrasound (EUS) has the highest sensitivity for small pancreatic head lesions (especially those under 2 cm that may be missed on CT) and for ampullary tumours. It also allows fine-needle aspiration (FNA) or fine-needle biopsy (FNB) of pancreatic masses, regional lymph nodes, and submucosal lesions for tissue diagnosis — essential before committing to chemotherapy, neoadjuvant therapy, or a palliative pathway. Meta-analyses report EUS-FNA sensitivity of approximately 85 to 92 per cent and specificity of 95 to 98 per cent for solid pancreatic lesions, making it the primary tissue-acquisition modality [8]. EUS is also used to assess the depth of biliary strictures and to place fiducial markers for subsequent radiotherapy.
ERCP — diagnostic and therapeutic
Endoscopic retrograde cholangiopancreatography (ERCP) combines endoscopic visualisation of the ampulla with radiological imaging of the biliary tree after cannulation and contrast injection. In the modern era, ERCP is primarily therapeutic — its diagnostic role has been superseded by MRCP and EUS. The therapeutic capabilities of ERCP include:
- CBD stone extraction with a balloon catheter or Dormia basket, after sphincterotomy (incision of the sphincter of Oddi to enlarge the ductal orifice) [2].
- Biliary stenting — placement of a plastic (temporary) or self-expanding metal stent (for longer patency in malignancy) across a malignant stricture to relieve obstruction and jaundice.
- Stricture dilation and brushing for cytology to distinguish benign from malignant strictures.
- Nasobiliary drainage for decompression in cholangitis.
The complications of ERCP are significant and must be discussed in consent: post-ERCP pancreatitis (about 5 per cent), bleeding (after sphincterotomy), duodenal perforation, and cholangitis (from failed or incomplete drainage). Periprocedural rectal diclofenac or indomethacin and prophylactic pancreatic duct stenting reduce the risk of pancreatitis in high-risk patients. [1]
Percutaneous transhepatic cholangiography (PTC)
When ERCP fails or is anatomically impossible (after Roux-en-Y gastric bypass, gastrectomy, or when the ampulla is inaccessible), PTC provides percutaneous access to the biliary tree via a transhepatic route. It allows diagnostic cholangiography, biliary drainage (external or internal-external), and stenting. PTC is also the preferred approach for intrahepatic or hilar (Klatskin) strictures, where endoscopic access to the affected ducts may be difficult. [1]
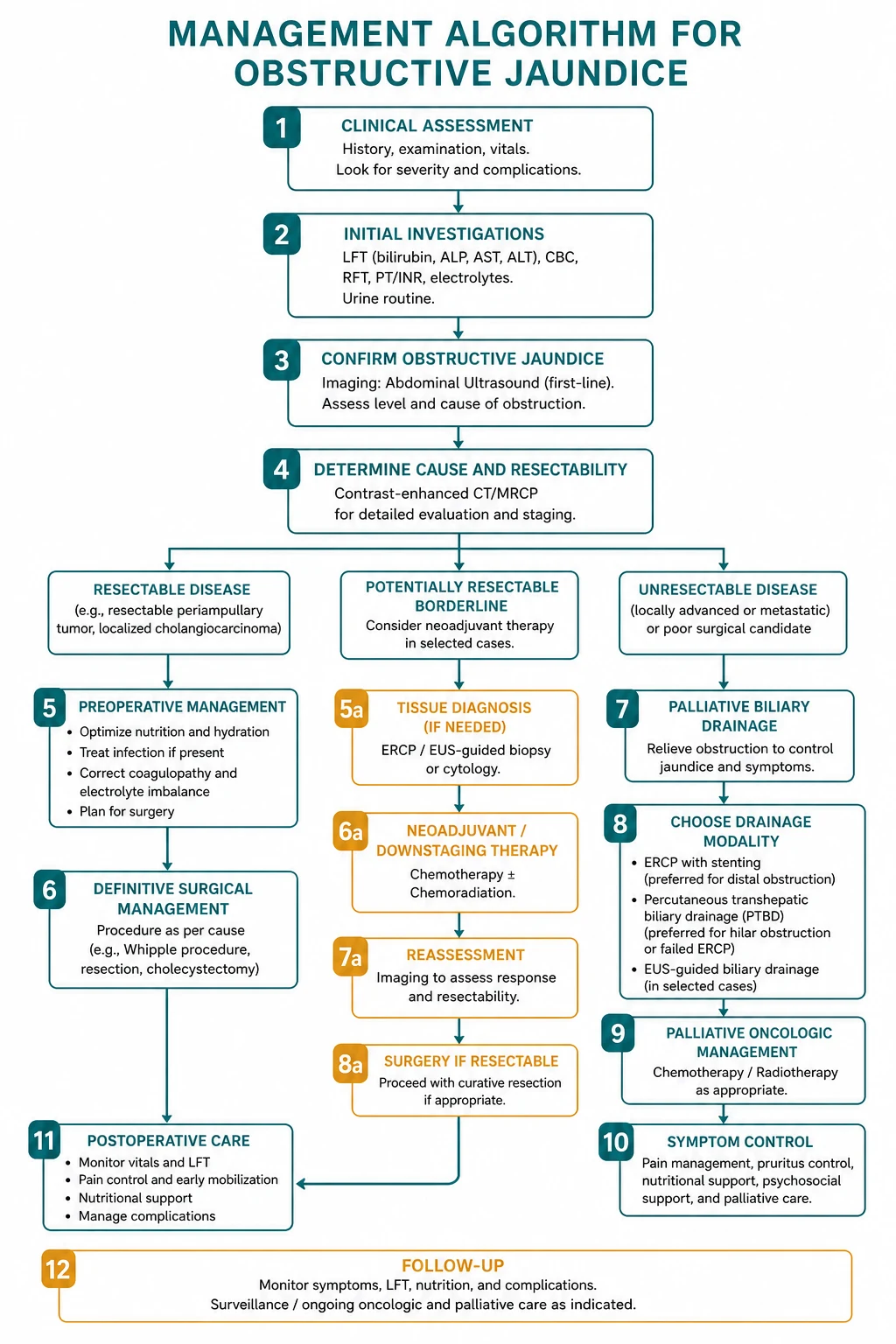
Management — treat the cause and restore drainage
The overarching principle of management is to treat the underlying cause and, where there is extrahepatic obstruction, to restore biliary drainage. The specific approach depends on the cause. [1]
Choledocholithiasis
The standard management of choledocholithiasis is ERCP with sphincterotomy and stone extraction (balloon trawl or basket), followed by laparoscopic cholecystectomy during the same admission to prevent recurrence (the source of the stones remains the gallbladder). The 2019 ASGE guidelines risk-stratify patients with gallstones to determine who needs pre-operative ERCP versus proceeding directly to cholecystectomy [2]:
- High risk (CBD stone on imaging, clinical cholangitis, or bilirubin above 4 mg per dL with a dilated CBD) — proceed to ERCP.
- Intermediate risk (abnormal liver biochemical tests, age above 55, or a dilated CBD on imaging) — evaluate with EUS, MRCP, or intraoperative cholangiography (IOC) before deciding on ERCP.
- Low risk — cholecystectomy without pre-operative ERCP. [1]
For large or impacted CBD stones, mechanical lithotripsy, extracorporeal shock wave lithotripsy, or cholangioscopy with electrohydraulic lithotripsy may be required. If endoscopic extraction fails, surgical common bile duct exploration (laparoscopic or open) is performed. [1]
Pancreatic head cancer
The management of pancreatic head adenocarcinoma depends on resectability, which is determined by CT staging [3]:
- Resectable (no vascular encasement, no metastases) — pancreaticoduodenectomy (Whipple procedure) with curative intent, followed by adjuvant chemotherapy (gemcitabine or FOLFIRINOX). Surgery is the only potential cure, but only 15 to 20 per cent of patients present with resectable disease.
- Locally advanced (superior mesenteric artery or vein encasement, unresectable) — chemotherapy (FOLFIRINOX or gemcitabine/nab-paclitaxel) with or without chemoradiotherapy; biliary drainage by ERCP stenting for symptomatic jaundice.
- Metastatic — palliative chemotherapy and biliary stenting for symptomatic relief.
Pre-operative biliary drainage was once routine for deep jaundice before pancreaticoduodenectomy, but the landmark randomised trial by van der Gaag (NEJM 2010) showed that routine PBD was associated with a higher rate of serious complications (74 versus 39 per cent) compared with early surgery [6]. PBD is now reserved for specific indications: cholangitis, surgery that must be delayed, or neoadjuvant chemotherapy.
DWE trap: The most common management error in pancreatic head cancer is routinely performing preoperative biliary drainage before Whipple. The van der Gaag NEJM 2010 trial showed that PBD increased serious complications from 39 to 74 per cent. Reserve PBD for cholangitis, when surgery is delayed, or for patients undergoing neoadjuvant therapy. Proceed to early surgery in the operable patient. [1]
Cholangiocarcinoma and ampullary cancer
Cholangiocarcinoma may arise in the intrahepatic ducts, the perihilar region (Klatskin tumour at the bifurcation — the most common and most challenging), or the distal CBD. Management is determined by location and resectability: surgical resection (hepatectomy for intrahepatic, hilar resection with hepaticojejunostomy for Klatskin, Whipple for distal) for localised disease, and palliative biliary stenting (ERCP or PTC, with self-expanding metal stents for longer patency) for unresectable disease. Ampullary cancer arises at the ampulla of Vater and, because it obstructs early, presents with painless jaundice at a smaller size and a better prognosis than pancreatic cancer if resected early (Whipple). [1]
Biliary strictures
Benign strictures (post-cholecystectomy, chronic pancreatitis, PSC) are managed with endoscopic balloon dilation and stenting (plastic stents exchanged every 3 to 6 months), reserving surgical bypass (hepaticojejunostomy or choledochoenterostomy) for endoscopic failure or recurrent disease. PSC strictures must be brushed for cytology at every ERCP to exclude superimposed cholangiocarcinoma, which occurs in 10 to 15 per cent of PSC patients [7].
Parasitic obstruction
Ascaris lumbricoides may migrate into the biliary tree causing obstruction and cholangitis; management is anthelmintics (mebendazole or albendazole) with endoscopic extraction of the worm. Liver flukes (Clonorchis sinensis, Opisthorchis viverrini), endemic in south-east Asia, cause recurrent cholangitis and are a major risk factor for cholangiocarcinoma; management is praziquantel plus management of complications. [1]
Acute ascending cholangitis — the emergency
Acute ascending cholangitis is a life-threatening infection of an obstructed biliary tree and a true biliary emergency. The obstruction is most often due to a CBD stone, but may be from any cause (stricture, tumour, stent occlusion). The pathophysiology is cholangio-venous reflux: the obstructed, bacteria-laden bile is under pressure, and bacteria and endotoxin are forced through the bile canaliculi into the systemic circulation, producing bacteraemia and septic shock. [1]
Diagnosis — the Tokyo Guidelines 2018
The Tokyo Guidelines 2018 (TG18) provide the standard diagnostic criteria and severity grading [1]. The diagnostic criteria combine three domains:
- A. Systemic inflammation — fever (above 38 degrees Celsius) or rigors, and laboratory evidence (white cell count abnormal, CRP elevated).
- B. Cholestasis — jaundice (bilirubin above the normal range) or abnormal liver function tests (ALP, GGT, AST, ALT elevated).
- C. Imaging — biliary dilatation or evidence of a cause (stone, stricture, stent).
A suspected diagnosis requires one item from A plus one item from B or C; a definite diagnosis requires one item from each of A, B, and C. [1]
Severity grading and the timing of drainage
TG18 grades severity to guide the timing of biliary drainage [1]:
- Grade III (severe) — organ dysfunction (hypotension requiring vasopressors, disturbed consciousness, PaO2/FiO2 below 300, oliguria or creatinine above 2 mg per dL, INR above 1.5, platelets below 100,000). Emergent biliary drainage is required as soon as the patient is resuscitated and stable.
- Grade II (moderate) — any two of: high fever (above 39 degrees), marked jaundice (bilirubin above 5 mg per dL), age above 75, marked leucocytosis, hypoalbuminaemia. Early biliary drainage within 48 hours.
- Grade I (mild) — does not meet Grade II or III criteria. Antibiotics first; drainage only if there is no response within 24 hours.
Management — the three pillars
- Resuscitation — intravenous fluids, oxygen, vasopressors for shock, and supportive care for organ dysfunction.
- Broad-spectrum antibiotics — covering Gram-negative organisms and enterococci. First-line is piperacillin-tazobactam or a third-generation cephalosporin (ceftriaxone) with metronidazole. Antibiotics are continued until the infection is controlled and the biliary tree is drained; the duration is tailored to the adequacy of drainage and the clinical response [1]. Blood cultures are taken before antibiotics.
- Biliary drainage — the definitive treatment. Without drainage, antibiotics alone are insufficient because they cannot sterilise an obstructed, pressurised biliary tree. Drainage is achieved by ERCP (sphincterotomy, stone extraction, stent placement, or nasobiliary drainage) as the first choice, with PTC if ERCP fails or is inaccessible, and surgical decompression as a last resort. The timing is determined by the severity grade [1].
DCE integration point: A candidate who recognises Charcot triad, applies the Tokyo Guidelines 2018 diagnostic criteria and severity grading, initiates resuscitation and broad-spectrum antibiotics, and arranges urgent biliary drainage (ERCP as first-line) will pass the cholangitis long case. The cardinal error is delaying drainage for further imaging or for the antibiotics to work — without decompression of the obstructed tree, the patient will deteriorate. [1]
Pre-operative optimisation
Before any biliary surgery or ERCP in a jaundiced patient, several pre-operative measures are essential: [1]
- Correct the coagulopathy — check the PT/INR in every jaundiced patient. A prolonged INR from vitamin K malabsorption is corrected with vitamin K 10 mg intravenously or orally (acts within 24 to 48 hours as new clotting factors are synthesised). If the INR fails to correct with vitamin K, suspect hepatocellular failure (the liver cannot synthesise factors even when given vitamin K) and use fresh frozen plasma before invasive procedures. A platelet count and bleeding time should also be checked.
- Treat cholangitis — if present, with resuscitation, antibiotics, and drainage before elective surgery.
- Optimise nutrition and hydration — correct dehydration and electrolyte disturbances; consider nutritional support in the malnourished or cachectic cancer patient.
- Decompress severe jaundice — in a deeply jaundiced patient (bilirubin above 200 to 300 micromol per litre) or one with cholangitis, pre-operative biliary drainage (ERCP stent or PTC) may be considered, though routine PBD before pancreaticoduodenectomy is not recommended because of the increased complication rate demonstrated by the van der Gaag trial [6].
- Renal protection — jaundiced patients are at risk of hepatorenal syndrome and acute kidney injury from endotoxaemia; ensure adequate hydration and avoid nephrotoxic drugs.
Pruritus of cholestasis
Intractable pruritus is one of the most distressing symptoms of obstructive jaundice and may significantly impair quality of life, particularly in malignancy and PBC. The mechanism involves the deposition of bile salts and other pruritogens in the skin. Management is stepped:
- Cholestyramine — a bile acid sequestrant that binds bile acids in the gut, interrupting the enterohepatic circulation. It is first-line for PBC and other cholestatic conditions.
- Rifampicin (150 to 300 mg twice daily) — second-line; acts by inducing hepatic enzyme systems and altering bile acid metabolism. Monitor liver function. [1]3. Sertraline and ondansetron — adjunctive options for refractory pruritus.
- Nasobiliary drainage — temporary but highly effective for refractory pruritus in PBC and other chloestatic disorders.
- Definitive relief of the obstruction — the most effective treatment for the pruritus of mechanical obstruction (ERCP stone extraction, stenting, surgery). [1]
Palliative care for advanced malignancy
For patients with unresectable or metastatic pancreatic, biliary, or ampullary cancer, the goals shift from cure to symptom control and quality of life. The key interventions are:
- Biliary drainage — ERCP with a self-expanding metal stent (longer patency than plastic, appropriate for the expected survival of months) relieves jaundice, pruritus, and the risk of cholangitis. If ERCP fails, PTC or surgical bypass (choledochoenterostomy or hepaticojejunostomy) provides alternative drainage.
- Duodenal stenting — for the 10 to 20 per cent of pancreatic cancer patients who develop duodenal obstruction from tumour invasion.
- Pain control — celiac plexus block or neurolysis (percutaneous or EUS-guided) for the severe epigastric and back pain of pancreatic cancer; opioid analgesia.
- Palliative chemotherapy — FOLFIRINOX or gemcitabine/nab-paclitaxel to extend survival and maintain quality of life.
- Nutritional support — pancreatic enzyme replacement for exocrine insufficiency; dietetic input.
- Psychological and social support — early involvement of palliative care and oncology teams; advance care planning. [1]
Prognosis
The prognosis of obstructive jaundice depends entirely on the cause. Choledocholithiasis has an excellent prognosis with timely ERCP and cholecystectomy. Pancreatic head adenocarcinoma has a dismal prognosis — overall five-year survival is under 10 per cent, and only 15 to 20 per cent present with resectable disease; even after a successful Whipple, the median survival is 18 to 24 months [3]. Ampullary cancer has a markedly better prognosis if resected early (five-year survival 40 to 60 per cent). Cholangiocarcinoma has a poor prognosis overall, worse for hilar (Klatskin) tumours than for distal. Acute ascending cholangitis carries a mortality of 2 to 10 per cent depending on severity and the timeliness of drainage; Grade III cholangitis with multi-organ failure has a mortality approaching 30 per cent [1]. Drug-induced intrahepatic cholestasis usually resolves on withdrawal of the offending agent, though chronic cholestasis (vanishing bile duct syndrome) may rarely occur.
High-yield DWE points and exam traps
- Obstructive jaundice is conjugated hyperbilirubinaemia with elevated ALP and GGT, dark urine, and pale stools. The first diagnostic task is to distinguish extrahepatic (needs imaging and drainage) from intrahepatic (needs serology and biopsy) by ultrasound.
- Ultrasound is first-line; MRCP is the gold-standard non-invasive biliary tree; CT stages pancreatic cancer; ERCP is therapeutic. Know the role of each modality and when to escalate.
- Courvoisier sign: a palpable gallbladder in a jaundiced patient suggests malignancy, not stones — low sensitivity (26 to 55 per cent), high specificity (83 to 90 per cent) [5].
- Charcot triad (fever, jaundice, RUQ pain) is present in only 50 to 70 per cent of cholangitis. Apply the Tokyo Guidelines 2018 criteria (systemic inflammation plus cholestasis plus imaging) and grade the severity to time the drainage.
- Acute cholangitis needs urgent biliary drainage — antibiotics alone cannot sterilise an obstructed, pressurised biliary tree. Grade III (organ dysfunction) needs emergent drainage.
- CA 19-9 is a monitoring marker, not a screening marker. Falsely elevated in cholangitis and obstruction; falsely normal in Lewis-antigen-negative individuals [4].
- Vitamin K corrects the coagulopathy of obstruction; failure to correct suggests hepatocellular failure. This is the classic DWE discriminator between cholestatic and hepatocellular jaundice.
- Routine preoperative biliary drainage before Whipple is harmful — the van der Gaag NEJM 2010 trial showed higher complications (74 versus 39 per cent). Reserve PBD for cholangitis, delayed surgery, or neoadjuvant therapy [6].
- Do not perform ERCP for intrahepatic cholestasis. A non-dilated biliary tree on ultrasound and MRCP, with a cholestatic LFT pattern, points to an intrahepatic cause (drugs, PBC, PSC, sepsis) that will not benefit from and may be harmed by ERCP.
- Drug-induced cholestasis is easily missed. Always take a careful drug history — flucloxacillin, chlorpromazine, anabolic steroids, amoxicillin-clavulanate, erythromycin, oral contraceptives.
- PSC presents in a young man with inflammatory bowel disease and a cholestatic LFT pattern. MRCP shows multifocal strictures and beading; there is a markedly increased risk of cholangiocarcinoma [7].
References and further reading
The Tokyo Guidelines 2018 (TG18) provide the current standard for the diagnosis, severity grading, and management of acute cholangitis, including the timing of biliary drainage by severity grade [1]. The 2019 ASGE guideline risk-stratifies choledocholithiasis and guides the use of ERCP versus MRCP, EUS, and intraoperative cholangiography [2]. The Lancet seminar on pancreatic cancer (Vincent 2011) remains the authoritative overview of epidemiology, biology, and management [3]. The clinical utility and limitations of CA 19-9 are reviewed by Ballehaninna and Chamberlain [4]. The modern evidence for Courvoisier sign — its low sensitivity and moderate specificity — is summarised by Fitzgerald [5]. The landmark randomised trial by van der Gaag (NEJM 2010) established that routine preoperative biliary drainage for pancreatic head cancer is harmful [6]. The ACG Clinical Guideline on Primary Sclerosing Cholangitis (Lindor 2015) covers diagnosis, the lack of effective medical therapy, and cancer surveillance [7]. The diagnostic accuracy of EUS-FNA for solid pancreatic lesions is established by meta-analysis [8].
References
- [1]Kiriyama S, Kozaka K, Takada T, Strasberg SM, Pitt HA, Gabata T, Yoshida M, Miura F, Horiguchi A, Wada K, Mayumi T, Gomi H, Yokoe M, Hata J, Inui K, Itoi T, Kimura Y, Takaoka M, Wakabayashi G, Chan ACW, Lau WY, Endo I, Asaka T, Kusachi S, Aoki T, Higuchi R, Okamoto K, Tajima Y, Ichihara T, Takagi K, Yamamoto M, Hirota M, Matsuyama Y, Kubota K, Kure S, Kayahara M, Maeda A, Murata A, Tanaka A, Yamakawa T, Palanisamy S, Chen MF, Suzuki K, Yamaue H, Miyazaki M, Takahashi K, Uchida E, Gouma DJ, de Castro SMM, Suwa A, Yasuda H, Niwa H, Horiguchi M, Murakami Y, Sumiyama Y, Sugiyama M, Sata N, Konishi H, Sado H, Nakanishi Y, Kawaguchi Y, Okamoto Y, Ogata T, Hanyu F, Kusano H, Todo S, Park AE, Gigot JF, Fan ST, Pawlik TM, Buchler MW, Ponchon T, Kruskal JB, Hodiwala A, Garden OJ, Cherqui D, Yamamoto J, Han HS, Yoon YS, Choi IS, Lee SE, Honda G, Sugiyama M, Asai K, Amano H, Yoshida EM Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholangitis (with videos) J Hepatobiliary Pancreat Sci, 2018.PMID 29032610
- [2]Maple JT, Ikenberry SO, Anderson MA, Appalaneni V, Banerjee S, Cash BD, Fisher L, Harrison ME, Fanelli RD, Fukami N, Khashab MA, Krinsky ML, Lichtenstein DR, Kaul V, Strohmeyer L, Shergill AK, Dominitz JA ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis Gastrointest Endosc, 2019.PMID 30979521
- [3]Vincent A, Herman J, Schulick R, Hruban RH, Goggins M Pancreatic cancer Lancet, 2011.PMID 21620466
- [4]Ballehaninna UK, Chamberlain RS The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal J Gastrointest Oncol, 2012.PMID 22811878
- [5]Fitzgerald JE, White MJ, Lobo DN Courvoisier's gallbladder: law or sign? World J Surg, 2009.PMID 19190960
- [6]van der Gaag NA, Rauws EA, van Eijck CH, Bruno MJ, van der Harst E, Kubben FJ, Gerritsen JJ, Greve JW, Gerhards MF, de Hingh IH, Klinkenbijl JH, Nio CY, de Castro SM, Busch OR, van Gulik TM, Bossuyt PM, Gouma DJ Preoperative biliary drainage for cancer of the head of the pancreas N Engl J Med, 2010.PMID 20071702
- [7]Lindor KD, Kowdley KV, Harrison ME; American College of Gastroenterology ACG Clinical Guideline: Primary Sclerosing Cholangitis Am J Gastroenterol, 2015.PMID 25869391
- [8]Puli SR, Bechtold ML, Buxbaum JL, Eloubeidi MA Endoscopic ultrasound guided fine needle aspiration for the diagnosis of pancreatic cystic neoplasms: a meta-analysis Pancreatology, 2013.PMID 23395570