Phys · gastrointestinal
Oesophageal Disorders
Also known as GORD · GERD · reflux · heartburn · Barrett's oesophagus · Barrett's esophagus · eosinophilic oesophagitis · EoE · achalasia · oesophageal cancer · dysphagia · odynophagia · Schatzki ring · Boerhaave syndrome · Zenker diverticulum
Consultant-physician-depth guide to oesophageal disorders — the dysphagia discrimination framework, GORD and the refractory-reflux workup, Barrett's surveillance and endoscopic eradication, eosinophilic oesophagitis from PPI-first to dupilumab, achalasia subtypes and subtype-matched treatment, oesophageal cancer staging and neoadjuvant therapy, and the oesophageal emergencies — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Oesophageal Disorders

The answer first
Almost everything an examiner can ask about the oesophagus hangs off one history question: what does the patient struggle to swallow, and how has it evolved? Dysphagia that begins with solids and progresses is a mechanical narrowing (stricture, ring, cancer) until proven otherwise; dysphagia that involves liquids from the very first day is a motility disorder (achalasia, spasm) until proven otherwise. Get that distinction out loud in the first thirty seconds and the rest of the work-up — endoscopy, barium swallow, manometry — falls into place behind it [1].
Three further rules carry the DWE and the long case [2]:
- Alarm features change the first test. Progressive dysphagia, weight loss, anaemia, haematemesis or persistent vomiting means endoscopy now — not a PPI trial and a review in eight weeks [1].
- Prove the disease before you escalate the treatment. Refractory "reflux" deserves objective pH-impedance testing off PPI before anyone reaches for a fundoplication; suspected achalasia deserves manometry before anyone dilates anything [2] [19].
- Dysplasia ends surveillance. A Barrett's patient with confirmed dysplasia has crossed from watching to treating — endoscopic eradication with resection of visible lesions plus radiofrequency ablation is the standard, backed by randomised trials [5] [8] [9].
The dysphagia framework — the single most discriminating question
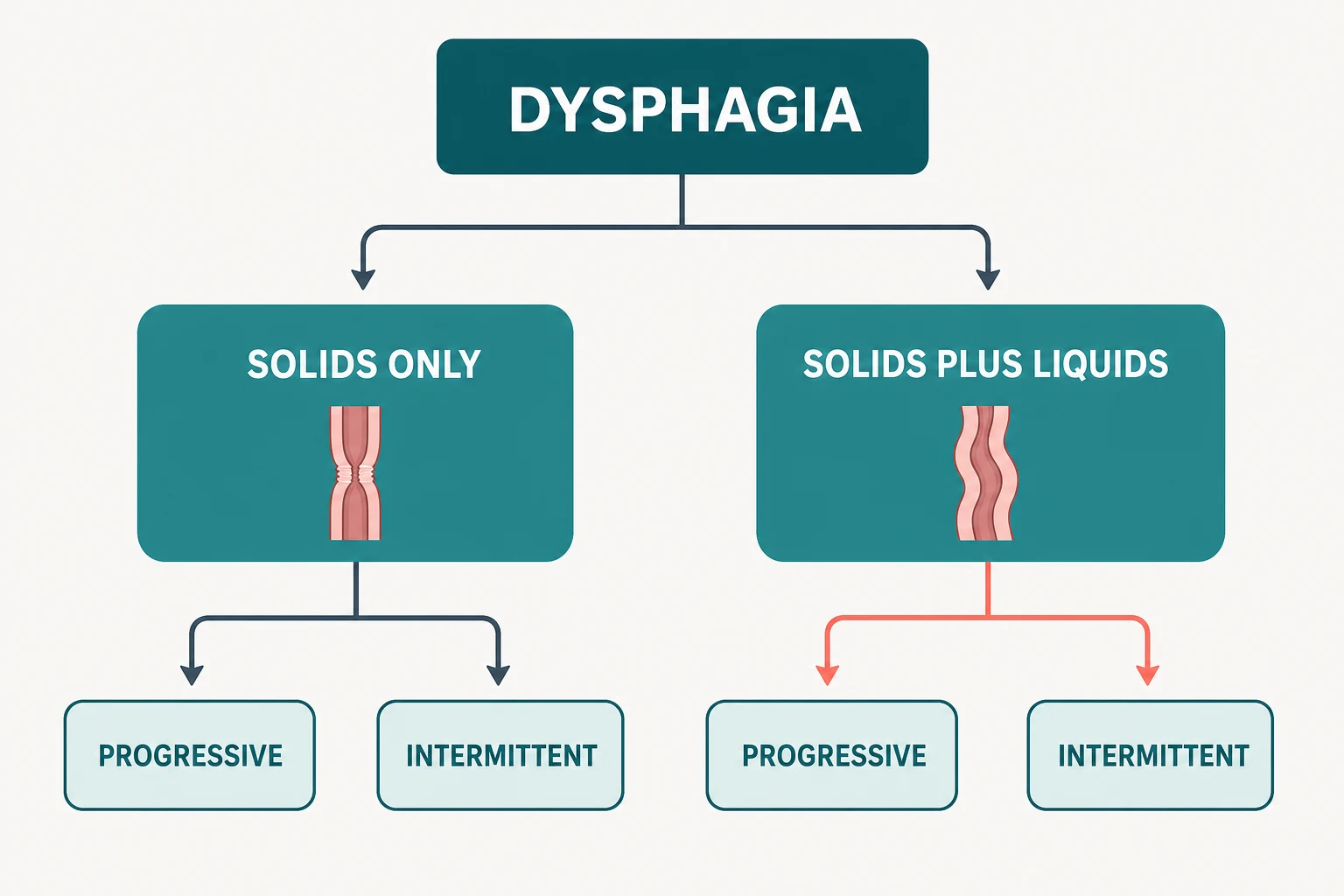
Dysphagia is a sensation of impaired bolus transit; odynophagia is pain on swallowing and points to mucosal ulceration (infection, pills, caustic injury) rather than narrowing. Confine the history to dysphagia and six questions classify it [1]:
- Solids, liquids, or both from the start? Solids first → mechanical. Liquids equal to solids from the beginning → motility.
- Progressive or intermittent? Progressive over weeks to months → peptic stricture or malignancy. Intermittent over years → ring, web, EoE or spasm.
- Where is it felt? Retrosternal localisation is accurate; suprasternal-notch localisation can come from anywhere in the oesophagus.
- What comes back up? Regurgitation of bland undigested food → achalasia or a pharyngeal pouch; acidic regurgitation → GORD.
- Is there pain, spasm or chest pain? Suggests spastic motility disorders; but cardiac ischaemia must be excluded first in anyone with risk factors.
- Who is the patient? Young, atopic, male, with previous food impactions → EoE. Older smoker with weight loss → cancer until scoped [1].
| Pattern | Mechanical or motility | Classic causes | First test |
|---|---|---|---|
| Solids only, progressive | Mechanical | Peptic stricture; oesophageal cancer (weeks–months, weight loss) | Endoscopy [1] |
| Solids only, intermittent | Mechanical | Schatzki ring, oesophageal web, EoE | Endoscopy with biopsies |
| Solids and liquids, progressive | Motility | Achalasia; scleroderma oesophagus | Barium swallow then manometry [15] |
| Solids and liquids, intermittent with chest pain | Motility | Diffuse oesophageal spasm; jackhammer oesophagus | Manometry after cardiac exclusion [15] |
Gastro-oesophageal reflux disease
GORD is symptoms or complications from reflux of gastric contents. The typical syndrome is heartburn and regurgitation; the atypical or extra-oesophageal presentations — chronic cough, laryngitis, asthma exacerbations, dental erosion, non-cardiac chest pain — are real but less specific, and attributing them to reflux requires more than a hunch [2].
Diagnosis is clinical first. Classic heartburn and regurgitation without alarm features earns an eight-week once-daily PPI trial; response supports the diagnosis, and no endoscopy is needed if symptoms resolve. Alarm features, persistent symptoms despite therapy, or dysphagia mean endoscopy [2].
Lifestyle advice — but only the advice with evidence. The systematic review of lifestyle measures found real support for weight loss in overweight patients and elevation of the head of the bed for nocturnal symptoms, plus avoiding meals within two to three hours of lying down. Blanket prohibitions on coffee, chocolate, alcohol and spicy food have no supporting evidence and should not be ritualistically recited [3].
GORD — the working numbers
Refractory GORD — prove it before you escalate
"Refractory heartburn" is one of the most mismanaged labels in gastroenterology. Before any escalation, work the sequence: adherence and timing (is the PPI taken 30–60 minutes before food?), dose optimisation, then objective testing — endoscopy (usually normal) and 24-hour pH-impedance monitoring off PPI. The pH-impedance study sorts refractory patients into three groups with completely different treatments [2]:
| pH-impedance result | Diagnosis | Treatment direction |
|---|---|---|
| Elevated acid exposure time | True ongoing acid reflux | Escalate anti-reflux therapy — including surgery if suitable [2] |
| Normal acid exposure, symptoms correlate with reflux events | Reflux hypersensitivity | Reflux-directed measures, neuromodulators, explanation |
| Normal acid exposure, no symptom correlation | Functional heartburn | Not reflux — stop escalating PPIs; treat as a functional disorder |
Anti-reflux surgery and LOTUS
For proven, PPI-responsive GORD where the patient prefers surgery or medication is not tolerated, laparoscopic fundoplication is the standard. The LOTUS trial randomised chronic GORD patients to esomeprazole or laparoscopic anti-reflux surgery: over five years both strategies maintained remission in the great majority, with a trade-off — more heartburn and regurgitation on drug therapy, more dysphagia, bloating and flatulence after surgery. The lesson is not that one wins; it is that both are legitimate in the correctly selected patient, and selection requires proven reflux and adequate oesophageal motility [4].
Barrett's oesophagus
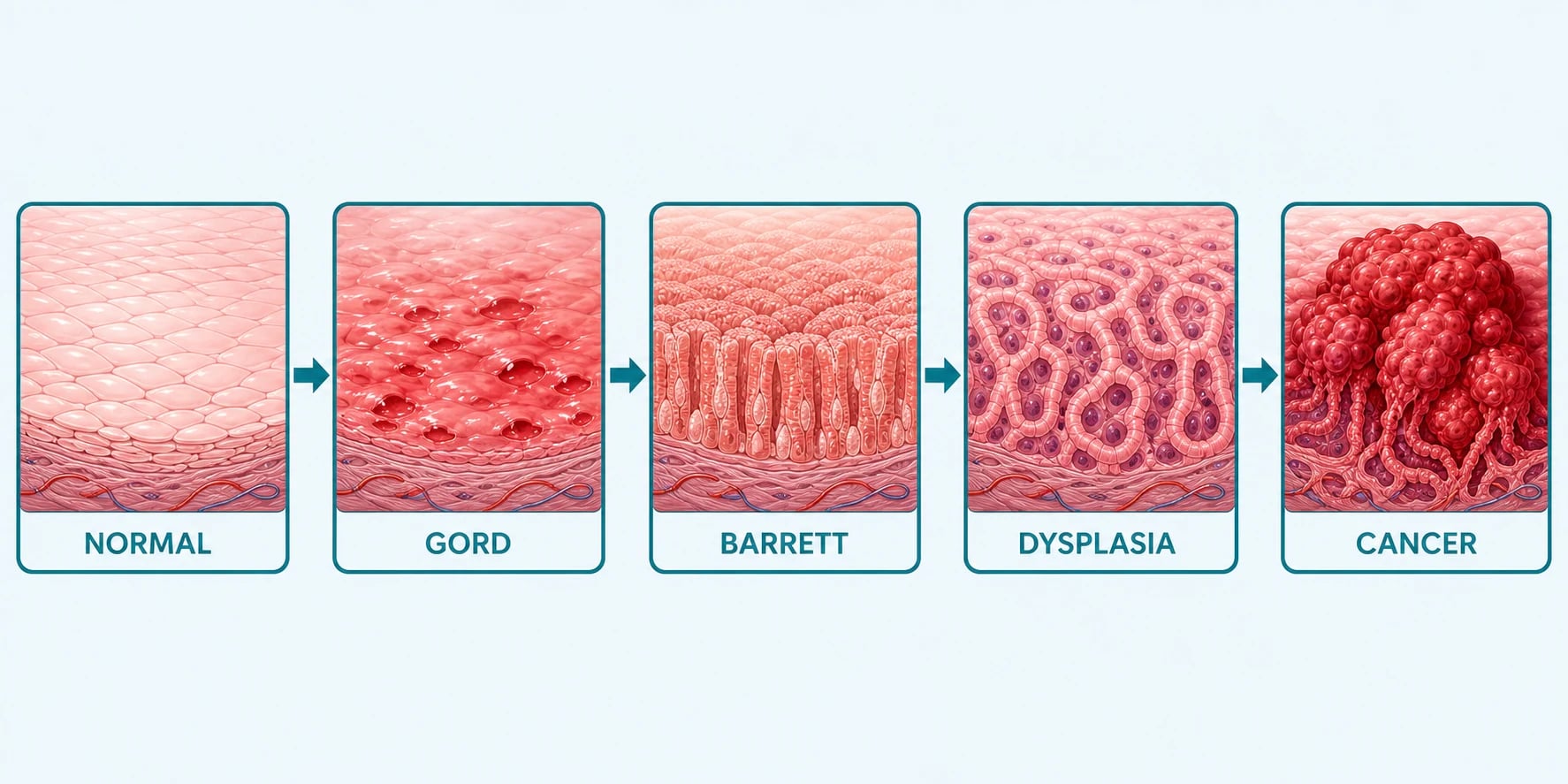
Barrett's is the replacement of distal oesophageal squamous mucosa by columnar mucosa with intestinal metaplasia — goblet cells on biopsy — extending at least 1 cm above the gastro-oesophageal junction. The ACG definition insists on the intestinal metaplasia; columnar lining without goblet cells does not carry the same malignant implication and does not make the diagnosis [5].
The endoscopic extent is reported with the Prague C&M criteria: C is the circumferential extent of columnar mucosa above the junction, M the maximal extent including tongues — so "C2M5" means 2 cm circumferential with tongues to 5 cm. It is the shared language of every surveillance report [6].
Screening. The ACG suggests a one-time screening endoscopy in patients with chronic GORD plus three or more risk factors: age over 50, male sex, white ethnicity, central obesity and smoking. This is a suggestion, not a mandate — but it is a favourite DWE stem [5].
Surveillance intervals depend entirely on dysplasia grade, and dysplasia must be confirmed by an expert gastrointestinal pathologist before it drives any decision [5]:
| Histology | Action | Interval |
|---|---|---|
| No dysplasia | Surveillance endoscopy | Every 3–5 years [5] |
| Indefinite for dysplasia | Optimise PPI, re-biopsy | Repeat in about 6–12 months |
| Low-grade dysplasia (confirmed) | Offer endoscopic eradication | — (treatment, not surveillance) |
| High-grade dysplasia / intramucosal cancer | Endoscopic eradication | — |
Endoscopic eradication — EMR then RFA
The modern standard for dysplastic Barrett's is endoscopic eradication therapy: endoscopic mucosal resection (EMR) of any visible lesion (nodule, ulcer, irregularity — both treatment and T-staging), followed by radiofrequency ablation (RFA) of the remaining flat Barrett's segment [5].
The trial evidence is exactly what an examiner wants quoted. In the AIM Dysplasia trial, RFA achieved complete eradication of high-grade dysplasia in about 90 per cent and of low-grade dysplasia in about 81 per cent of patients, with fewer cancers than sham ablation. In SURF, patients with confirmed low-grade dysplasia randomised to RFA progressed to high-grade dysplasia or cancer in 1.5 per cent versus 26.5 per cent under surveillance over three years — the trial that converted low-grade dysplasia from "watch" to "treat" [8] [9].
Eosinophilic oesophagitis
EoE is a chronic, food-antigen-driven, Th2-mediated inflammation of the oesophagus. Think of it as asthma of the oesophagus: young atopic men, often with asthma, eczema, allergic rhinitis or IgE-mediated food allergy, presenting with intermittent dysphagia to solids and food bolus impactions — the classic ED presentation is a twenty-something who has bolted a steak. Children present with feeding dysfunction and failure to thrive [10].
Diagnosis requires symptoms of oesophageal dysfunction plus at least 15 eosinophils per high-power field on oesophageal biopsy, with the process isolated to the oesophagus. Two discriminating points for exams: endoscopic signs (rings, linear furrows, white exudates, strictures, mucosal fragility) can be subtle or absent, so biopsy even a normal-looking oesophagus when the story fits; and take biopsies from multiple levels because disease is patchy [10].
EoE treatment ladder
PPI first
A PPI trial induces clinical and histological remission in roughly half of patients — cheap, safe, and the accepted first step, not a diagnostic confounder to apologise for
Dietary elimination
Six-food elimination (milk, wheat, egg, soy, nuts, seafood) or step-up empiric elimination with re-endoscopy to identify triggers
Topical steroids
Swallowed fluticasone or budesonide orodispersible/viscous preparation — first-line pharmacology alongside PPIs
Biologic for refractory disease
Dupilumab, blocking IL-4/IL-13 signalling, for steroid-refractory or steroid-dependent EoE
Dilation for strictures
Careful bougie or balloon dilation for fixed fibrotic narrowing — treats the stricture, not the inflammation
The evidence base, in the order examiners quote it. PPIs induce remission in roughly half of patients in the meta-analysis by Lucendo — which is why PPI-first is legitimate initial therapy rather than a failed paradigm. The six-food elimination diet achieved histological remission in about 72 per cent in Kagalwalla's landmark cohort, establishing diet as therapy, though step-up two- or four-food strategies are kinder in practice. Budesonide orodispersible tablets produced histological remission in 58 per cent versus none on placebo in the EOS-1 induction trial. And dupilumab — the LIBERTY trial — delivered histological remission in about 60 per cent of adolescents and adults versus 5–6 per cent on placebo at 24 weeks, giving refractory EoE its first approved biologic [11] [12] [13] [14].
Achalasia and the spastic motility disorders
Achalasia is the loss of inhibitory myenteric neurons (VIP- and nitric-oxide-mediated), producing failure of lower oesophageal sphincter relaxation plus absent peristalsis. The clinical triad is dysphagia to liquids and solids from the onset, regurgitation of bland undigested food, and weight loss — often with years of diagnostic delay labelled as "reflux" [19].
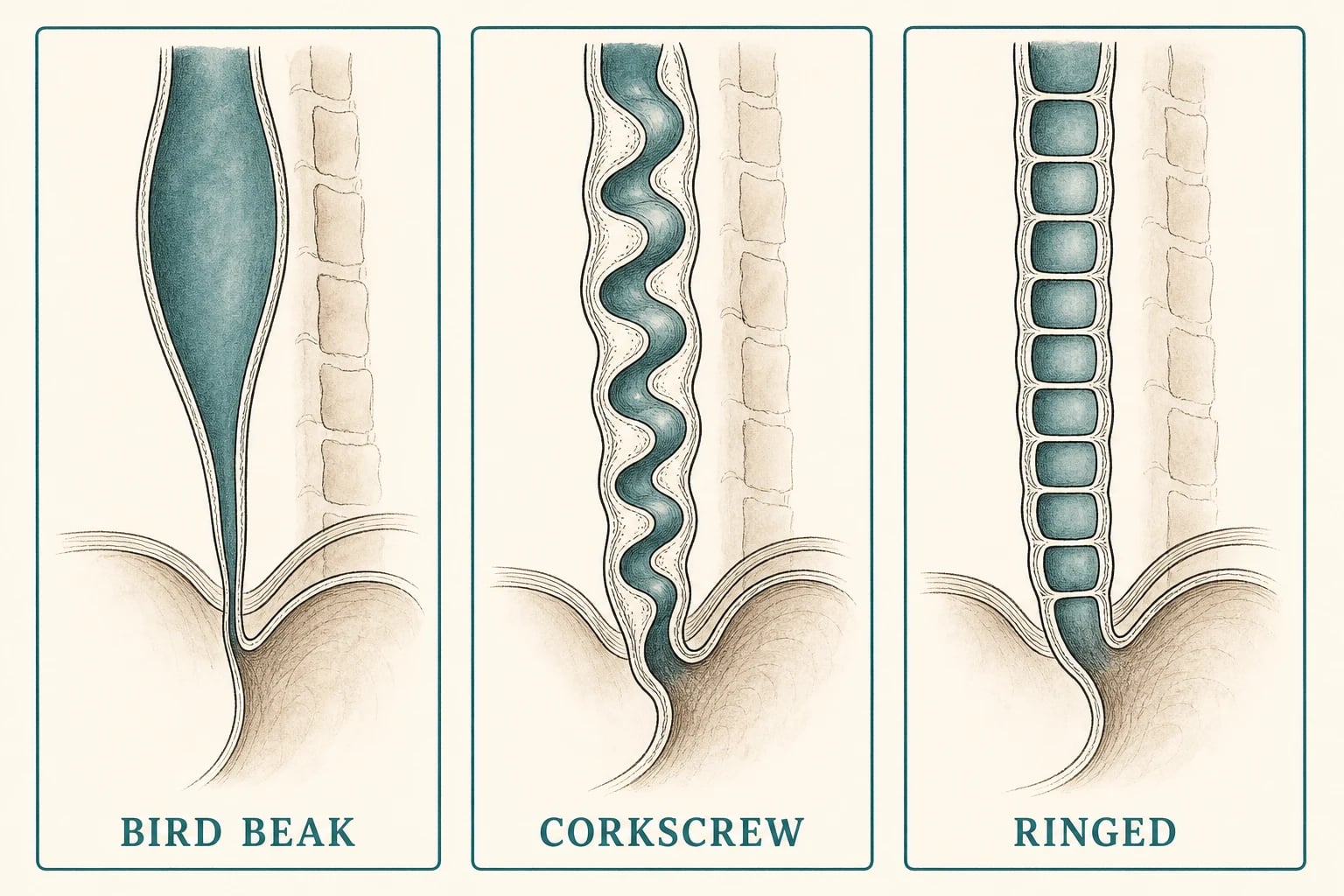
Diagnosis is a sequence. The barium swallow shows the smooth tapered bird-beak narrowing at the cardia with a dilated oesophagus above; a timed barium study quantifies emptying (column height at 1, 2 and 5 minutes) and gives a baseline for post-treatment comparison. Endoscopy is performed to exclude pseudoachalasia — a cardia or junctional tumour mimicking achalasia, suggested by age over about 55, a short history and marked weight loss. High-resolution manometry is mandatory and delivers the Chicago v4.0 subtype [15] [19].
| Chicago v4.0 type | Manometric signature | Clinical behaviour |
|---|---|---|
| Type I — classic | Aperistalsis with no oesophageal pressurisation | Intermediate response to treatment [15] |
| Type II — with compression | Pan-oesophageal pressurisation | Best response to any LES-disrupting treatment |
| Type III — spastic | Premature (spastic) distal contractions | Poorest response to dilation/Heller; needs long myotomy — POEM preferred |
Severity is tracked with the Eckardt score — dysphagia, regurgitation, chest pain and weight loss each graded 0–3 (maximum 12), with a score of 3 or less defining remission. Eckardt's own outcome work after pneumatic dilation identified younger patients as doing less well with dilation — a nuance that still flavours the dilation-versus-myotomy choice in the young man [20].
Treatment — matched to subtype and patient
All definitive achalasia treatment works the same way: disrupt the lower oesophageal sphincter — by balloon, by knife, or from inside. There is no therapy that restores peristalsis [19].
| Treatment | Evidence | Best for | Main drawback |
|---|---|---|---|
| Graded pneumatic dilation (30 → 35 → 40 mm) | European Achalasia Trial: equivalent to Heller at 2 years; at 5 years success around 80 per cent in both arms, with about a quarter of dilation patients needing redilation | Type I/II; older patients; surgical-risk patients | Perforation risk of a few per cent; repeat sessions [16] [17] |
| Laparoscopic Heller myotomy + partial fundoplication | Same European trial; durable, single-session | Type I/II in fit surgical candidates | Surgical morbidity; reflux if fundoplication omitted [16] [17] |
| POEM (per-oral endoscopic myotomy) | Randomised against pneumatic dilation: clinical success about 83 per cent versus 42 per cent at 24 months | Type III (myotomy can be extended proximally); failed prior therapy | High rates of post-procedure reflux — erosive oesophagitis in up to half; commits many to long-term PPI [18] |
| Botulinum toxin injection | Short-lived (months) | Frail, unfit, bridging | Wears off; repeated use scars the plane |
The other motility disorders, briefly. Diffuse oesophageal spasm requires premature contractions on manometry with normal LES relaxation — intermittent dysphagia and chest pain, the corkscrew oesophagus on barium; jackhammer oesophagus is hypercontractile rather than uncoordinated. First-line management is a PPI trial (GORD is a common driver) and smooth-muscle relaxants, with POEM reserved for refractory cases. And after any myotomy — surgical or endoscopic — reflux becomes the new disease: say so, and say that partial fundoplication accompanies Heller and that post-POEM patients need reflux surveillance [15] [18].
Oesophageal cancer
Oesophageal cancer is two different diseases sharing an organ [5]:
| Adenocarcinoma | Squamous cell carcinoma | |
|---|---|---|
| Location | Distal oesophagus and gastro-oesophageal junction | Mid and upper oesophagus |
| Precursor | Barrett's metaplasia → dysplasia | Chronic mucosal injury |
| Risk profile | Chronic GORD, central obesity, white, male, smoking | Smoking, alcohol, achalasia, caustic strictures, Plummer-Vinson, prior head/neck SCC |
| Western trend | Rising steeply over decades | Declining [5] |
Presentation is the mechanical pattern from the framework: progressive dysphagia from solids to liquids over weeks to months, weight loss, iron-deficiency anaemia — the alarm triad that sends the patient straight to endoscopy and biopsy [1].
Staging is layered: CT of neck/chest/abdomen first for gross spread; PET-CT to hunt occult distant metastases that upstage a third of apparently resectable patients; and endoscopic ultrasound for T-depth and regional nodes when the patient remains potentially curable. Junctional tumours may need laparoscopy to exclude peritoneal disease. The stage — and the patient's fitness — decides between endoscopic, surgical and palliative paths [21].
| Stage group | Treatment backbone | Trial anchor |
|---|---|---|
| Intramucosal (T1a), especially in Barrett's | Endoscopic resection + ablation of the remaining segment | EMR/RFA evidence base [5] [8] |
| Locally advanced oesophageal/junctional, fit for surgery | CROSS neoadjuvant chemoradiotherapy (weekly carboplatin + paclitaxel with 41.4 Gy) then oesophagectomy | Median survival roughly doubled (49 vs 24 months) in CROSS; benefit durable at ten years [21] [22] |
| Junctional/gastric-type adenocarcinoma, fit | FLOT perioperative chemotherapy (4 pre- and 4 post-operative cycles of 5-FU/leucovorin, oxaliplatin, docetaxel) | FLOT4 improved median survival over ECF/ECX (50 vs 35 months) [23] |
| Unresectable/metastatic with dysphagia | Palliation: stenting, radiotherapy/brachytherapy, systemic therapy; nutrition first | — |
The short list — other oesophageal disorders you must not fumble
Zenker diverticulum is a posterior pharyngoesophageal pouch herniating through Killian's dehiscence in the elderly — halitosis, regurgitation of undigested food eaten hours earlier, gurgling, and aspiration pneumonia. Diagnose with a barium swallow (endoscopy risks perforating the pouch), and treat symptomatic pouches with endoscopic septotomy or surgical diverticulectomy [24].
Webs and rings. An oesophageal web — classically with iron-deficiency anaemia as the Plummer-Vinson/Paterson-Brown-Kelly syndrome — causes intermittent dysphagia and carries a squamous cancer association; treat the iron deficiency and dilate. A Schatzki ring at the squamocolumnar junction is the commonest benign cause of intermittent solids-only dysphagia in adults — the "steakhouse syndrome" bolus — and is treated by dilation and acid suppression [1].
Pill oesophagitis is localised ulceration from a lodged tablet — doxycycline and other tetracyclines, bisphosphonates, NSAIDs, iron and potassium chloride are the usual offenders. It produces sudden retrosternal pain and odynophagia in a patient with no swallowing history, and is prevented (and managed) by taking pills with a full glass of water and remaining upright for at least 30 minutes [25].
Management by diagnosis — the one-glance summary
| Diagnosis | First line | Escalation | The trap |
|---|---|---|---|
| GORD | PPI trial + weight loss/head-of-bed elevation [2] [3] | pH-impedance off PPI → fundoplication if proven | Escalating unproven "reflux" [2] |
| Barrett's, no dysplasia | PPI + surveillance 3–5 yearly [5] | — | Surveying dysplasia instead of treating it |
| Barrett's with dysplasia | EMR of visible lesions + RFA of flat segment [8] [9] | Post-eradication surveillance | Missing the visible lesion that needs EMR first |
| EoE | PPI first, then diet or topical steroid [11] [12] [13] | Dupilumab; gentle dilation for strictures [14] | Dilation without anti-inflammatory control |
| Achalasia I/II | Pneumatic dilation or Heller myotomy [16] [17] | POEM; botox if frail | Missing pseudoachalasia [19] |
| Achalasia III | POEM (long myotomy) [15] [18] | — | Treating type III like type I/II |
| Oesophageal cancer | Stage with CT → PET → EUS [21] | CROSS or FLOT then surgery; endoscopic for T1a | Offering surgery without PET/EUS staging [22] [23] |
DCE angles
The long case is Barrett's with dysplasia in multimorbidity: a 70-year-old with ischaemic heart disease, chronic kidney disease and a C3M6 Barrett's segment now showing low-grade dysplasia. The examiner wants to watch you weigh competing risks — the annual progression risk against procedural risk, anticoagulation, frailty and life expectancy — and to hear that confirmed dysplasia shifts the default to endoscopic eradication (EMR of visible lesions, then RFA) provided the patient will benefit from and tolerate the program, including the post-ablation surveillance that follows. A consultant answer names the SURF data, acknowledges the patient's cardiac comorbidity shaping anaesthesia and antiplatelet management, and closes with a shared decision rather than a guideline reflex [5] [9].
The short case has no oesophageal findings to feel — and that is the point. The dysphagia history station rewards a disciplined six-question framework (solids versus liquids, progressive versus intermittent, localisation, regurgitation character, pain, and who the patient is). The epigastric examination is about the sequelae: weight loss and cachexia, cervical nodes (a left supraclavicular Virchow node), chest signs of aspiration, epigastric tenderness or mass, and the stigmata of treatment — sternotomy or thoracotomy scars, a PEG or feeding jejunostomy [1].
Exam traps, collected
References
- [1]Liu LWC, Andrews CN, Armstrong D, et al. Clinical Practice Guidelines for the Assessment of Uninvestigated Esophageal Dysphagia J Can Assoc Gastroenterol, 2018.PMID 31294391
- [2]Katz PO, Dunbar KB, Schnoll-Sussman FH, et al. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease Am J Gastroenterol, 2022.PMID 34807007
- [3]Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures effective in patients with gastroesophageal reflux disease? An evidence-based approach Arch Intern Med, 2006.PMID 16682569
- [4]Galmiche JP, Hatlebakk J, Attwood S, et al. Laparoscopic antireflux surgery vs esomeprazole treatment for chronic GERD: the LOTUS randomized clinical trial JAMA, 2011.PMID 21586712
- [5]Shaheen NJ, Falk GW, Iyer PG, et al. Diagnosis and Management of Barrett's Esophagus: An Updated ACG Guideline Am J Gastroenterol, 2022.PMID 35354777
- [6]Sharma P, Dent J, Armstrong D, et al. The development and validation of an endoscopic grading system for Barrett's esophagus: the Prague C & M criteria Gastroenterology, 2006.PMID 17101315
- [7]Hvid-Jensen F, Pedersen L, Drewes AM, et al. Incidence of adenocarcinoma among patients with Barrett's esophagus N Engl J Med, 2011.PMID 21995385
- [8]Shaheen NJ, Sharma P, Overholt BF, et al. Radiofrequency ablation in Barrett's esophagus with dysplasia N Engl J Med, 2009.PMID 19474425
- [9]Phoa KN, van Vilsteren FG, Weusten BL, et al. Radiofrequency ablation vs endoscopic surveillance for patients with Barrett esophagus and low-grade dysplasia: a randomized clinical trial JAMA, 2014.PMID 24668102
- [10]Liacouras CA, Furuta GT, Hirano I, et al. Eosinophilic esophagitis: updated consensus recommendations for children and adults J Allergy Clin Immunol, 2011.PMID 21477849
- [11]Lucendo AJ, Arias Á, Molina-Infante J. Efficacy of Proton Pump Inhibitor Drugs for Inducing Clinical and Histologic Remission in Patients With Symptomatic Esophageal Eosinophilia: A Systematic Review and Meta-Analysis Clin Gastroenterol Hepatol, 2016.PMID 26247167
- [12]Kagalwalla AF, Sentongo TA, Ritz S, et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis Clin Gastroenterol Hepatol, 2006.PMID 16860614
- [13]Lucendo AJ, Miehlke S, Schlag C, et al. Efficacy of Budesonide Orodispersible Tablets as Induction Therapy for Eosinophilic Esophagitis in a Randomized Placebo-Controlled Trial Gastroenterology, 2019.PMID 30922997
- [14]Dellon ES, Rothenberg ME, Collins MH, et al. Dupilumab in Adults and Adolescents with Eosinophilic Esophagitis N Engl J Med, 2022.PMID 36546624
- [15]Yadlapati R, Kahrilas PJ, Fox MR, et al. Esophageal motility disorders on high-resolution manometry: Chicago classification version 4.0(©) Neurogastroenterol Motil, 2021.PMID 33373111
- [16]Boeckxstaens GE, Annese V, des Varannes SB, et al. Pneumatic dilation versus laparoscopic Heller's myotomy for idiopathic achalasia N Engl J Med, 2011.PMID 21561346
- [17]Moonen A, Annese V, Belmans A, et al. Long-term results of the European achalasia trial: a multicentre randomised controlled trial comparing pneumatic dilation versus laparoscopic Heller myotomy Gut, 2016.PMID 26614104
- [18]Werner YB, Hakanson B, Martinek J, et al. Endoscopic or Surgical Myotomy in Patients with Idiopathic Achalasia N Engl J Med, 2019.PMID 31800987
- [19]Vaezi MF, Pandolfino JE, Yadlapati RH, et al. ACG Clinical Guidelines: Diagnosis and Management of Achalasia Am J Gastroenterol, 2020.PMID 32773454
- [20]Eckardt VF, Aignherr C, Bernhard G. Predictors of outcome in patients with achalasia treated by pneumatic dilation Gastroenterology, 1992.PMID 1451966
- [21]van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer N Engl J Med, 2012.PMID 22646630
- [22]Shapiro J, van Lanschot JJB, Hulshof MCCM, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial Lancet Oncol, 2015.PMID 26254683
- [23]Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial Lancet, 2019.PMID 30982686
- [24]Chirica M, Kelly MD, Siboni S, et al. Esophageal emergencies: WSES guidelines World J Emerg Surg, 2019.PMID 31164915
- [25]Kikendall JW. Pill esophagitis J Clin Gastroenterol, 1999.PMID 10372925