Phys · general-medicine
Abdominal Examination Routine — The DCE Short-Case Systematic Approach
Also known as abdominal examination · abdominal exam · abdomen examination · examine the abdomen · abdominal physical examination · per abdominal examination · gastrointestinal examination · hepatomegaly examination · splenomegaly examination · organomegaly differentiation · ascites examination · shifting dullness · fluid thrill · spider naevi · palmar erythema · caput medusae · Kayser-Fleischer ring · Virchow node · Troisier sign · Dupuytren contracture · expansile pulsation
Consultant-physician-depth guide to the systematic abdominal examination for the DCE short case and MRCP PACES. Covers the reproducible head-to-toe twelve-step routine, the key physical signs and their interpretation (clubbing, palmar erythema, Dupuytren contracture, spider naevi, scleral icterus, Kayser-Fleischer rings, Virchow node, caput medusae), the differentiation of organomegaly (liver versus spleen versus kidney by direction, percussion, ballotability and surface), the evidence-based examination of ascites (shifting dullness, fluid thrill), the abdominal aortic aneurysm (expansile pulsation), the signs of peritonitis, the standard oral presentation template, and the discussion questions the examiner will ask. Structured for FRACP DCE and MRCP PACES. Every sign is referenced to the JAMA Rational Clinical Examination series.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Abdominal Examination Routine — The DCE Short-Case Systematic Approach
The answer first
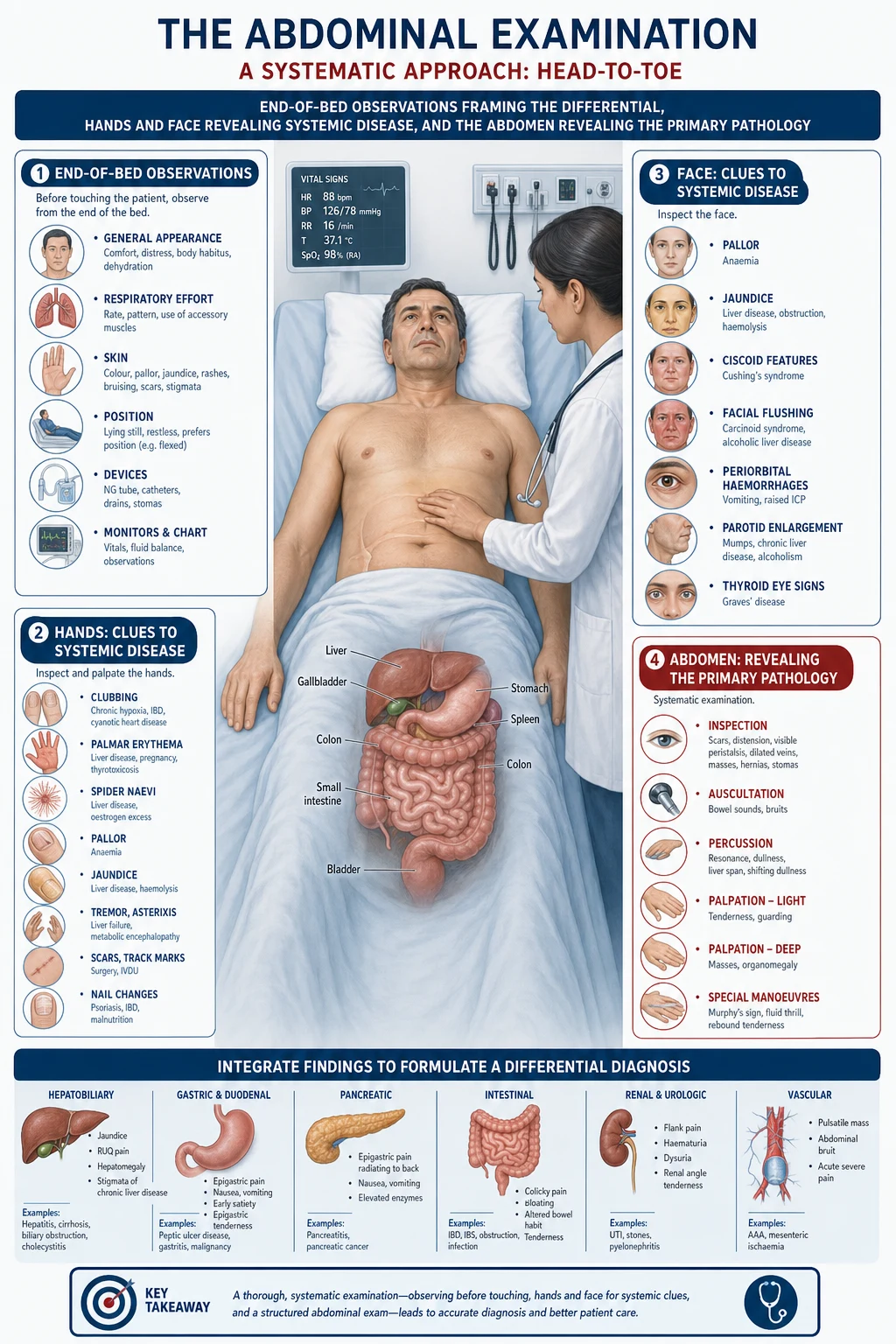
The abdominal examination is the classic DCE short case — it appears in every FRACP DCE cycle and is a mandatory station in MRCP PACES (Station 3). The instruction is always the same: "Please examine this patient's abdomen." The candidate who performs a fluent, complete, reproducible head-to-toe routine, presents the findings in a structured two-minute presentation, and discusses the interpretation of each sign with confidence will pass. The candidate who auscultates after palpation, who cannot differentiate a spleen from a kidney, or who omits the hands, face and neck has already failed, regardless of what they find in the abdomen itself. [1]
The reproducible sequence is a twelve-step head-to-toe routine that examines the abdomen in the context of the whole patient, because the abdomen is the target organ for systemic diseases — chronic liver disease, inflammatory bowel disease, malignancy, nephrotic syndrome, endocrine disease, and infection all leave signs in the hands, face, chest and legs long before they are palpable in the abdomen. The candidate who examines only the abdomen misses half the marks. [1]
The single most important departure from other system examinations is that you auscultate before you palpate. In the cardiovascular and respiratory examinations, you inspect, palpate, percuss then auscultate. In the abdominal examination, you inspect, auscultate, then palpate and percuss — because palpation and percussion can stimulate or alter bowel sounds, destroying the very information you are trying to collect. Every examiner watches for this, and the candidate who palpates first has demonstrated that they do not understand why the sequence differs. [1]
The second non-negotiable principle is start palpation away from the site of pain. If the patient reports right iliac fossa pain, you begin in the left iliac fossa and work systematically toward the painful area. This builds trust, allows the patient to relax, and gives you a baseline of what their non-tender abdomen feels like before you reach the tender region. [1]
DCE high-yield: The three most commonly tested abdominal short-case scenarios are (1) chronic liver disease with its constellation of stigmata — spider naevi, palmar erythema, Dupuytren contracture, gynaecomastia, ascites, and hepatosplenomegaly; (2) organomegaly — the candidate who can differentiate liver, spleen and kidney at the bedside passes; and (3) the acute abdomen — guarding, rigidity, rebound tenderness, and the differentiation of surgical from medical causes. [1]
Step 1 — The end of the bed
Before you touch the patient, stand at the end of the bed and observe for thirty seconds. The end-of-bed inspection is the highest-yield thirty seconds of the entire examination — it generates your differential before you have laid a hand on the patient. [1]
General appearance and body habitus. Look for cachexia (malignancy, chronic liver disease, malabsorption, inflammatory bowel disease, cardiac cachexia), obesity (metabolic syndrome, non-alcoholic fatty liver disease), and Cushingoid habitus (moon face, central obesity, purple striae — chronic steroid therapy, Cushing syndrome, or the alcohol-induced pseudo-Cushing state). [1]
Skin colour. Jaundice (yellow sclera and skin — hepatobiliary disease, haemolysis), pallor (anaemia), bronze pigmentation (haemochromatosis — iron deposition in skin), generalised hyperpigmentation (Addison disease — sun-exposed areas, palmar creases, oral mucosa), and erythema ab ignine (reticulated brown discolouration from chronic heat exposure — chronic back pain with a hot water bottle, a clue to chronic pancreatitis or malignancy). [1]
Breathing pattern and posture. Is the patient comfortable lying flat? A patient who lies rigidly still with knees drawn up has peritonism. A patient who is breathless lying flat may have massive ascites or an unrelated cardiopulmonary problem. A patient who is leaning forward and distressed may have acute pancreatitis. [1]
Bedside clues. Look for the vomit bowl, the nasogastric tube, the urinary catheter bag (haematuria, oliguria), the drain sites, the stoma bag, the walking frame, the oxygen, the IV pole with parenteral nutrition, the medication chart (lactulose, spironolactone, furosemide — cirrhosis with ascites; pancreatic enzyme replacements — chronic pancreatitis; immunosuppressants — IBD or transplant). [1]
Distribution of abdominal distension. If the abdomen is distended, the distribution tells you the cause before you palpate. Ascites distends the flanks preferentially and produces a protuberant umbilicus. Gaseous distension from obstruction is more central and tympanic. An ovarian mass or pregnancy produces a domed, central distension. A localised bulge may be a hernia, a mass, or a distended bladder. [1]
Step 2 — The hands
Examine both hands systematically. The hands are a window into chronic gastrointestinal, hepatic and systemic disease. [1]
Clubbing. Examine the nail from the side — the normal angle between the nail plate and the proximal nail fold (Lovibond angle) is approximately 160 degrees. In clubbing, the angle is lost (greater than 180 degrees), there is increased sponginess of the nail bed, and the distal phalanx is bulbous. Schamroth's window test: ask the patient to place the nails of the same finger of both hands together — in a normal person, a small diamond-shaped window is visible between the nail beds; in clubbing, this window is lost. [1]
Palmar erythema (liver palms). A diffuse, blanchable erythema affecting the thenar and hypothenar eminences and the fingertips, sparing the centre of the palm. It occurs in cirrhosis (from oestrogen excess due to impaired hepatic metabolism), pregnancy, rheumatoid arthritis, hyperthyroidism, and as a normal variant. It is non-specific but, combined with other signs, supports chronic liver disease. [1]
Dupuytren contracture. Palpable nodules and thickening of the palmar fascia with progressive flexion contracture of the digits (classically the ring and little fingers). Associated with cirrhosis (especially alcoholic), epilepsy, diabetes, manual labour, smoking, and increasing age. The association with liver disease is through the same fibrogenic pathway. [1]
Finger-prick marks and calluses. Multiple finger-prick marks on the fingertips indicate the insulin-dependent diabetic. Calluses on the dorsum of the fingers (from self-induced vomiting in eating disorders) or on the palmar aspect (from crutch use) may be relevant. [1]
Nail signs. Leuconychia (whitening of the nails — hypoalbuminaemia from cirrhosis or nephrotic syndrome), koilonychia (spoon nails — iron deficiency), half-and-half nails (Lindsay nails — chronic kidney disease), and splinter haemorrhages (infective endocarditis, though also trauma). [1]
Tremor and signs of withdrawal. A fine tremor may indicate alcohol withdrawal, hyperthyroidism, or beta-agonist therapy. A coarse tremor with ataxia is Wilson disease (copper deposition in the basal ganglia). A liver flap (asterixis) indicates hepatic encephalopathy — you check for this by asking the patient to hold their hands out with wrists dorsiflexed for 30 seconds. [1]
Step 3 — The arms
Continue up the arms, looking for: [1]
Bruising. Easy bruising and purpura indicate coagulopathy (impaired clotting factor synthesis in cirrhosis, vitamin K deficiency in cholestasis or malabsorption) or thrombocytopenia (hypersplenism from portal hypertension, bone marrow failure, or ITP). [1]
Needle-track marks. Track marks in the antecubital fossae indicate intravenous drug use — the gateway to viral hepatitis (B and C), which leads to chronic hepatitis, cirrhosis, and hepatocellular carcinoma. This single finding reframes the entire differential. [1]
Arteriovenous fistula. A palpable thrill and audible bruit over the radiocephalic or brachiocephalic fistula in the forearm indicates the patient is on haemodialysis for end-stage kidney disease — the abdomen may show polycystic kidneys, a transplant, or nephrotic syndrome. [1]
Excoriations and scratch marks. Linear excoriations on the extensor surfaces and the back indicate pruritus. In the context of abdominal examination, pruritus without a rash points to cholestasis (primary biliary cholangitis, primary sclerosing cholangitis, biliary obstruction) — the bilirubin is not yet high enough to cause visible jaundice, but the bile salts deposited in the skin are intensely pruritic. [1]
Tattoos. Tattoos are a risk factor for hepatitis B and C, particularly if acquired in an unregulated setting. Note but do not comment unnecessarily. [1]
Pulse and blood pressure. Check the radial pulse (rate, rhythm — atrial fibrillation is common in sepsis, thyrotoxicosis, and alcohol-related disease) and measure the blood pressure if not already done. [1]
Step 4 — The face
The face is examined systematically: eyes, mouth, then lips. [1]
Eyes
Scleral icterus (jaundice). Look at the sclera in natural light. Jaundice becomes clinically visible when the serum bilirubin exceeds approximately 40 to 50 micromoles per litre. The sclerae yellow before the skin because elastin in the sclera has a high affinity for bilirubin. Ask the patient to look down while you gently elevate the upper eyelid to expose the superior sclera, where jaundice first appears. [1]
Xanthelasma and xanthomata. Yellow, flat or raised lipid deposits on the eyelids (xanthelasma) or extensor tendons (xanthomata) indicate hyperlipidaemia. In the context of hepatobiliary disease, xanthelasma is a classic sign of primary biliary cholangitis, where the cholestasis causes disordered lipid metabolism. [1]
Kayser-Fleischer rings. A brownish-green ring at the periphery of the cornea, best seen with a slit lamp, caused by copper deposition in Descemet membrane. This is the cardinal ocular sign of Wilson disease. The ring is most dense at the superior and inferior poles initially. It is present in approximately 95 per cent of patients with neurological Wilson disease but in only about 65 per cent of those presenting with hepatic disease. [1]
Arcus senilis. A white or grey ring at the corneal periphery — associated with hypercholesterolaemia in the young patient (arcus juvenilis) but a normal age-related finding in the older patient. [1]
Anaemia. Conjunctival pallor indicates anaemia. The lower eyelid conjunctiva should be pink. [1]
Mouth
Oral candidiasis (thrush). White, curd-like plaques on the buccal mucosa, palate or tongue that can be scraped off, leaving an erythematous base. In the context of abdominal examination, oral candidiasis indicates immunosuppression — HIV, chemotherapy, chronic steroid therapy (IBD, autoimmune hepatitis), or broad-spectrum antibiotic use. [1]
Aphthous ulcers. Painful, shallow ulcers on the oral mucosa. Multiple recurrent aphthous ulcers are a feature of inflammatory bowel disease (especially Crohn disease), coeliac disease, Behcet syndrome, and nutritional deficiency (iron, B12, folate). [1]
Angular cheilitis. Cracking and inflammation at the corners of the mouth — iron deficiency, B12 deficiency, folate deficiency, or candidal infection. [1]
Telangiectasia. Small, dilated blood vessels on the lips, tongue and oral mucosa indicate hereditary haemorrhagic telangiectasia (Osler-Weber-Rendu syndrome), which causes GI bleeding from arteriovenous malformations in the gut, and is also associated with pulmonary, hepatic and cerebral AVMs. [1]
Mucosal pigmentation. Dark brown pigmentation on the buccal mucosa and gums (not the teeth) is Addison disease. Blue-grey macules on the buccal mucosa are the Peutz-Jeghers sign. [1]
Glossitis and angular stomatitis. A smooth, beefy-red, atrophic tongue (glossitis) indicates B12, folate or iron deficiency. [1]
Lips
Pigmented spots on the lips. Multiple small (1 to 5 mm), dark brown to blue-black macules on the lips, especially the lower lip, and on the buccal mucosa and fingers, are pathognomonic of Peutz-Jeghers syndrome — an autosomal dominant condition with mucocutaneous pigmentation and hamartomatous gastrointestinal polyps (predominantly small bowel) carrying a significantly increased risk of GI and other cancers. [1]
Central cyanosis. A blue discoloration of the lips indicates central cyanosis (or methaemoglobinaemia). [1]
Step 5 — The neck
Examine the cervical and supraclavicular lymph nodes. [1]
Virchow node (Troisier sign). A hard, enlarged left supraclavicular lymph node (in the region where the thoracic duct drains into the left subclavian vein) is a sentinel node for intra-abdominal malignancy — classically gastric cancer, but also pancreatic, hepatobiliary, testicular, ovarian, and renal malignancy. The node receives lymphatic drainage from the entire abdomen via the cisterna chyli and thoracic duct. Finding this node in a patient with abdominal symptoms mandates urgent upper GI endoscopy and cross-sectional imaging. A Virchow node is one of the highest-yield single findings in clinical medicine — every candidate must examine for it. [1]
Other lymph nodes. Examine the cervical chain, the axillary nodes (axillary adenopathy with abdominal symptoms may indicate lymphoma), and the epitrochlear nodes. [1]
Step 6 — The chest
The chest wall carries the cutaneous and hormonal stigmata of chronic liver disease. Examine from the clavicles to the umbilicus, because the signs of chronic liver disease are distributed above the level of the umbilicus (the territory of the superior vena cava). [1]
Spider naevi (spider telangiectasia). These are small (up to 1 cm), bright red, radiating vascular lesions with a central arteriole (the body) and radiating capillary branches (the legs). They are found in the distribution of the superior vena cava — face, neck, upper chest, shoulders, arms, and hands. The diagnostic test is blanching: press the centre with a pinhead or glass slide, and the entire lesion blanches, then refills from the centre outward when released. [1]
Gynaecomastia. Enlargement of the glandular breast tissue in the male, palpable as a disc of firm tissue beneath the areola. In cirrhosis, gynaecomastia results from oestrogen excess (impaired metabolism) and testosterone reduction (impaired synthesis from the diseased liver and increased conversion of androgens to oestrogens in peripheral tissue). Spironolactone (used for ascites) also causes gynaecomastia by inhibiting testosterone action. Distinguish gynaecomastia from lipomastia (fat deposition, no glandular tissue). [1]
Loss of axillary and pubic hair. In advanced cirrhosis and in hypogonadism, the loss of body hair reflects the hormonal disruption (low testosterone, high oestrogen). [1]
Superior vena cava obstruction. Distended veins over the upper chest wall without caudal flow may indicate SVC obstruction (malignancy — lung cancer, mediastinal mass). [1]
Step 7 — Inspection of the abdomen
Now turn to the abdomen. Position the patient supine with the head supported by one pillow and the arms at the sides — this relaxes the abdominal musculature. Expose the abdomen from the xiphisternum to the symphysis pubis (with appropriate dignity and a chaperone if needed). Ask the patient to let you know if any area is tender before you touch them. [1]
Contour
Flat abdomen. Normal or cachexia. [1]
Scaphoid abdomen. Cachexia — advanced malignancy, chronic malnutrition, anorexia nervosa, Addison disease. [1]
Distended abdomen. Use the distribution to identify the cause before you palpate: [1]
- Generalised, flanks filled, everted umbilicus — ascites. The fluid pools in the flanks by gravity when supine.
- Central, tympanic, drum-like — gaseous distension from bowel obstruction or paralytic ileus.
- Dome-shaped, central, arising from the pelvis — pregnancy, ovarian mass (large ovarian cyst), distended bladder.
- Localised bulge — mass (hepatomegaly causing right upper quadrant fullness, splenomegaly in the left upper quadrant, epigastric mass from gastric or pancreatic cancer), hernia, or abdominal aortic aneurysm. [1]
Skin and surface
Scars. Identify each scar — they are a map of the surgical history. A midline laparotomy scar (vertical, from xiphisternum to pubis), a Kocher incision (right subcostal, for open cholecystectomy or liver surgery), a Lanz or appendix incision (right iliac fossa), a Pfannenstiel incision (transverse suprapubic, for gynaecological or urological surgery), laparoscopic port sites (typically four small scars — umbilical, and three in the upper abdomen), and drain sites (small scars in the flank or suprapubic region). [1]
Stoma. Identify whether it is a colostomy (usually in the left iliac fossa, flush to the skin, formed stool) or an ileostomy (usually in the right iliac fossa, spouted, liquid effluent). A urostomy (ileal conduit) is also in the right iliac fossa with a stoma appliance collecting urine. Assess the mucosa (pink and healthy versus ischaemic or dusky), the surrounding skin (irritation from effluent leak), and the output. [1]
Visible peristalsis. Ripples of bowel wall contraction visible through the abdominal wall — pathognomonic of chronic intestinal obstruction (the bowel hypertrophies over time and its contractions become visible). This is not seen in acute obstruction because the bowel has not had time to hypertrophy. Visible peristalsis accompanied by visible distension and colicky pain is a high-yield sign. [1]
Caput medusae. A cluster of dilated, radiating veins around the umbilicus, reminiscent of the head of Medusa. This indicates portal hypertension — the portal venous system decompresses through the recanalised umbilical vein into the systemic circulation via the periumbilical veins. To confirm, determine the direction of venous blood flow: place two index fingers on a segment of vein, occlude it, then lift one finger and observe the direction of refill. In caput medusae, the flow is away from the umbilicus in all directions (above the umbilicus the flow is upward, below it flows downward). This distinguishes it from inferior vena cava obstruction, where all superficial abdominal veins drain upward toward the SVC. [1]
Striae. Purple striae (recent) or white/silvery striae (old) — Cushing syndrome, pregnancy, rapid weight gain or loss. [1]
Hernial orifices. Inspect the inguinal and femoral regions, especially when the patient coughs or strains — a cough impulse confirms a hernia. Note any visible bulge at rest. [1]
Dilated superficial veins. As above — caput medusae (portal hypertension), or pattern suggesting SVC or IVC obstruction. [1]
Step 8 — Auscultation BEFORE palpation
This is the step that distinguishes the competent candidate from the rest. In the abdominal examination, you auscultate before you palpate. The rationale is that palpation and percussion can alter or stimulate bowel sounds, giving a false impression. Listen for a full minute in each quadrant, starting in the right iliac fossa (near the caecum, where bowel sounds are normally most active). [1]
Bowel sounds
Normal. Intermittent gurgling and clicking sounds, occurring approximately every 5 to 15 seconds. [1]
Hyperactive (tinkling, rushing). High-pitched, frequent, tinkling sounds that occur in early mechanical bowel obstruction — the hyperactive bowel is attempting to overcome the obstruction. As the obstruction progresses and the bowel fatigues, the sounds may become absent. [1]
Absent (silent abdomen). No bowel sounds heard for two or more minutes of continuous listening. This indicates paralytic ileus (postoperative, electrolyte disturbance, peritonitis, retroperitoneal haemorrhage) or generalised peritonitis (the bowel is paralysed by the inflammatory process). A truly silent abdomen with rigidity and guarding is a surgical emergency. [1]
Bruits
Listen for vascular bruits over the aorta (epigastrium), the renal arteries (mid-abdomen, just lateral to the midline on each side), and the iliac arteries (lower abdomen). [1]
Epigastric bruit. May indicate an abdominal aortic aneurysm or mesenteric artery stenosis. However, epigastric bruits are also heard in normal, thin individuals (especially under age 40). [1]
Renal artery bruit. A systolic bruit in the flank or mid-abdomen, especially if it extends into diastole, suggests renal artery stenosis. This is a moderate-specificity, low-sensitivity finding. [1]
Hepatic bruit. A bruit over the liver suggests hepatocellular carcinoma or alcoholic hepatitis. [1]
Succession splash. Place the stethoscope over the epigastrium and shake the patient's abdomen from side to side. A splashing sound (like shaking a half-full bottle) indicates gastric outlet obstruction or gastroparesis — the stomach is distended with fluid and air. A positive succession splash in the fasting patient is pathological. [1]
Step 9 — Palpation
Palpate in the correct order: superficial (light) palpation first, then deep palpation. Start in the quadrant farthest from the pain and work systematically around the abdomen (typically clockwise from the left iliac fossa through the left upper quadrant, epigastrium, right upper quadrant, right iliac fossa, suprapubic, and back to the left iliac fossa). Kneel or sit beside the patient so that your examining hand is at the level of the abdomen. Keep your hand flat (do not prod with fingertips), use the pads of the fingers, and watch the patient's face throughout for signs of discomfort. [1]
Light (superficial) palpation
Palpate gently, approximately 1 cm deep, across all nine regions of the abdomen. You are assessing: [1]
Tenderness. Where is it? Is it localised or generalised? [1]
Guarding. Voluntary contraction of the abdominal muscles in response to pain or apprehension. Guarding is voluntary if the muscles relax when the patient is distracted and the hand is warmed, and the rigidity is not sustained. Voluntary guarding is common with anxiety and mild pain. [1]
Rigidity (involuntary guarding). Sustained, involuntary contraction of the abdominal muscles that the patient cannot relax. This is a sign of peritonitis — the inflamed parietal peritoneum reflexively causes the overlying muscles to guard to prevent movement. A board-like, rigid abdomen with absent bowel sounds is generalised peritonitis — a surgical emergency. [1]
Rebound tenderness. Pain that is worse on the sudden release of the palpating hand than on the initial pressure. This indicates peritoneal inflammation — the release of pressure allows the inflamed paritoneum to spring back, producing pain. Rebound tenderness is uncomfortable for the patient; many examiners now prefer testing for percussion tenderness (a gentle tap on the abdominal wall is painful) or the Rovsing sign (palpation of the left iliac fossa producing pain in the right iliac fossa in appendicitis) as gentler surrogates. [1]
Deep palpation
After light palpation, palpate more deeply (4 to 5 cm) to assess masses, organomegaly and deeper tenderness. In the obese or muscular patient, use the two-hand technique (one hand on top of the other for reinforcement). [1]
Liver
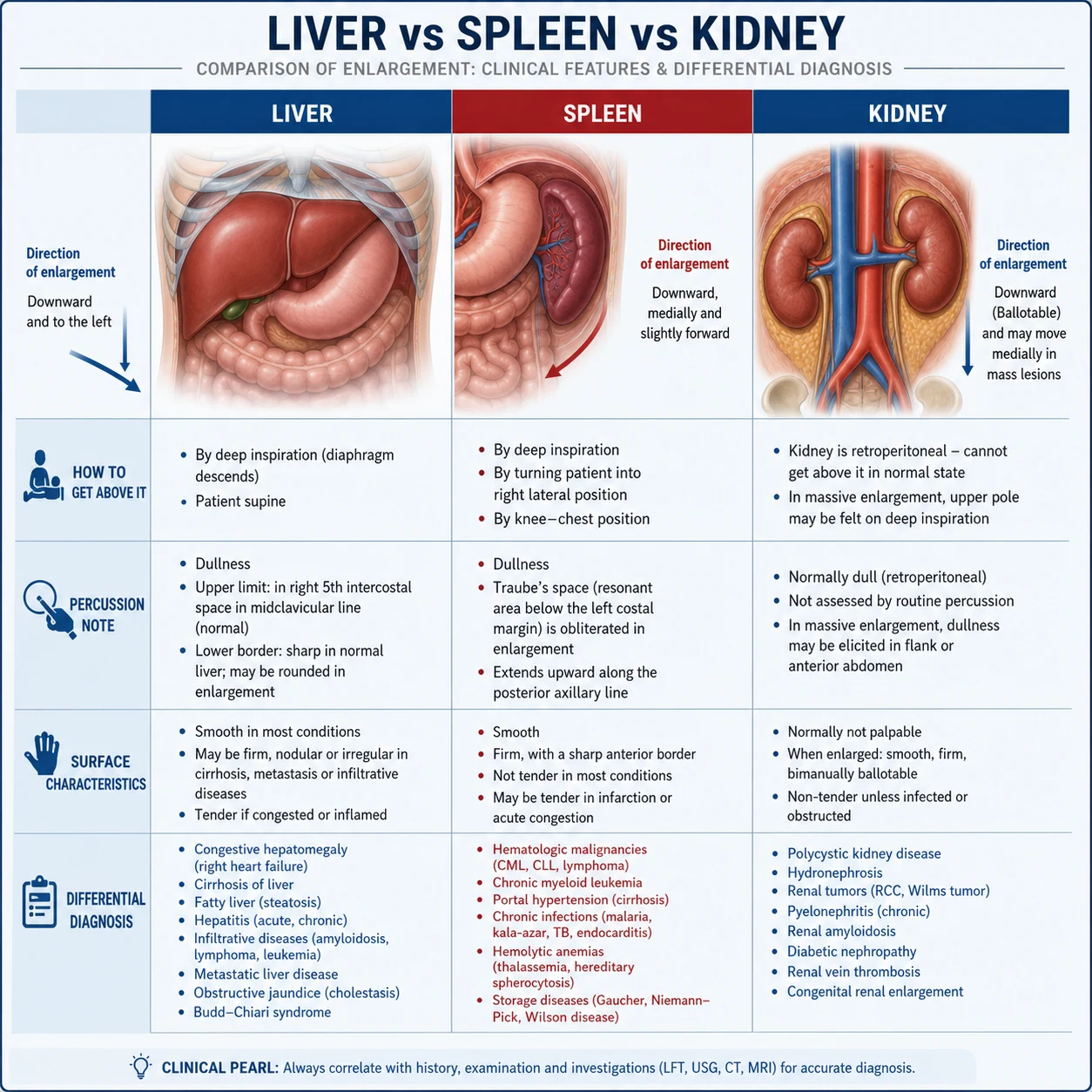
The liver is examined with the patient breathing deeply in and out through the mouth. Place your examining hand flat in the right iliac fossa, lateral to the rectus muscle, with the fingers pointing toward the right costal margin. Ask the patient to breathe in deeply and slowly. As the diaphragm descends on inspiration, the liver edge is pushed downward toward your waiting hand. Move your hand progressively upward — one centimetre per inspiration — toward the costal margin, until you feel the liver edge slip under your fingertips. [1]
Spleen
The spleen is examined from the right side of the patient, using the same inspiratory technique but starting in the right iliac fossa and moving diagonally toward the left costal margin (the direction of splenic enlargement). Alternatively, start in the left iliac fossa and move toward the left costal margin. Ask the patient to roll slightly toward you (right lateral decubitus position) to bring the spleen closer to the abdominal wall. [1]
Causes of splenomegaly to know: [1]
- Massive splenomegaly (extends into the right iliac fossa): chronic myeloid leukaemia, myelofibrosis, chronic malaria (hyperreactive malarial splenomegaly), visceral leishmaniasis (kala-azar), Gaucher disease.
- Moderate splenomegaly: portal hypertension (any cause of cirrhosis), lymphoma, leukaemia, haemolytic anaemia, infection (infectious mononucleosis, bacterial endocarditis), storage diseases, connective tissue disease (SLE, rheumatoid arthritis — Felty syndrome). [1]
Kidneys
The kidneys are examined by ballottement. Place one hand in the renal angle (the costovertebral angle, posteriorly) and one hand anteriorly in the upper quadrant. Ask the patient to breathe out, then push the posterior hand upward (or forward) to flick the kidney between your two hands. A ballotable kidney feels like a firm mass that moves between the hands. You can get above a ballotable kidney (unlike the spleen), and it is resonant to percussion (because of overlying bowel gas). A palpable right kidney may be normal in thin individuals. A palpable left kidney is always abnormal and suggests polycystic kidney disease, hydronephrosis, renal cell carcinoma, or a renal transplant. [1]
Renal angle tenderness (Murphy punch sign). Gentle percussion or palpation in the costovertebral angle produces pain in pyelonephritis, renal colic, or perinephric abscess. [1]
Bladder
Palpate in the suprapubic region for a distended bladder — a smooth, round, tense mass arising from the pelvis, dull to percussion, which cannot be got above. If the bladder is distended, it may extend to or above the umbilicus. [1]
Aorta
Palpate in the epigastrium for the aorta. Place the hands on either side of the midline, with the fingers pointing toward the spine, and feel for the aortic pulsation. [1]
Masses
If you palpate a mass, describe its: location (which quadrant), size (in centimetres), shape, surface (smooth, irregular, nodular), consistency (soft, firm, hard, cystic), mobility (mobile, fixed, moves with respiration), tenderness, and whether it is pulsatile or expansile. [1]
Step 10 — Percussion
Percuss all four quadrants systematically. You are assessing: [1]
Liver span. Percuss downward from the right third intercostal space in the midclavicular line until the note changes from resonant (lung) to dull (liver) — this is the upper border. Then percuss upward from below the right costal margin until the note changes from tympanic (bowel) to dull (liver) — this is the lower border. The distance between the upper and lower borders is the liver span. A normal span is 10 to 12 cm in the midclavicular line. A span over 12 to 14 cm suggests hepatomegaly. A span under 8 cm suggests a small liver (cirrhosis). [1]
Splenomegaly. Percuss in the left upper quadrant. Castell sign: percuss in the lowest intercostal space in the left anterior axillary line (normally tympanic from the splenic flexure of the colon). With the patient supine and then in the right lateral decubitus position, if the note becomes dull, the spleen is enlarged. Traube space: the triangular space of tympany over the left lower anterior chest (bounded by the sixth rib, the midaxillary line, and the costal margin). Dullness in Traube space in a fasting patient suggests splenomegaly (but may be unreliable if the patient has eaten or has a pleural effusion). [1]
Ascites — shifting dullness. This is the most reliable bedside sign for ascites. Percuss from the midline outward to the flank in a supine patient. In the midline, the bowel floats on the ascitic fluid and the note is tympanic. In the dependent flanks, the ascitic fluid pools and the note is dull. Mark the transition point from tympanic to dull. Now ask the patient to roll onto their side (away from the side you are percussing) and wait 30 seconds for the fluid to redistribute. Re-percuss: the previously dull flank should now be tympanic (the fluid has shifted with gravity). This shift of the dullness confirms free fluid. Shifting dullness detects approximately 1000 mL or more of ascites [1].
Ascites — fluid thrill (fluid wave). This detects tense ascites (typically over 2000 mL). Place the edge of one hand firmly on the midline of the abdomen (to dampen transmission through the fat). With the other hand, tap one flank sharply. If you feel a distinct impulse or thrill on the opposite flank (place the other hand on the opposite flank to receive it), the test is positive — the wave has been transmitted through the fluid. This is less sensitive than shifting dullness but more specific for large-volume ascites. [1]
Bladder. Percuss the suprapubic region — a distended bladder is dull to percussion. [1]
Percussion of a mass
A mass that is dull to percussion is solid or fluid-filled (liver, spleen, bladder, tumour, cyst). A mass that is tympanic is gas-filled (distended bowel). [1]
Additional examination
After the systematic abdominal examination, complete the assessment with: [1]
Hernial orifices. Examine the inguinal and femoral canals, with the patient standing if possible (hernias are more prominent standing). Ask the patient to cough — a cough impulse confirms a hernia. Identify: inguinal hernia (above and medial to the pubic tubercle — indirect passes through the deep inguinal ring, direct through Hesselbach triangle), femoral hernia (below and lateral to the pubic tubercle — higher risk of strangulation). [1]
Digital rectal examination (PR). Indicated if there is a history of altered bowel habit, rectal bleeding, tenesmus, or suspected prostate pathology. Examine for masses (rectal tumour, faecal impaction), prostate size and consistency (smooth and enlarged — benign prostatic hyperplasia; hard, irregular, nodular — prostate cancer), tenderness (prostatitis, abscess), and the character of the stool (melena — upper GI bleed; hard impacted stool — constipation; empty rectum with obstruction — proximal obstruction). Always offer PR examination — it is a core part of the complete abdominal examination and candidates lose marks for omitting it. [1]
Genitalia. Examine if indicated — testicular masses, hydrocele, varicocele (especially left-sided, which may indicate renal cell carcinoma if the varicocele does not decompress on lying down — the "bag of worms"). [1]
Stoma assessment. If a stoma is present, assess the type (colostomy vs ileostomy vs urostomy), the mucosa (pink vs ischaemic), the height (spouted for ileostomy), the aperture, and the surrounding skin. [1]
Step 12 — The legs
Complete with a brief leg examination: [1]
Oedema. Peripheral oedema (sacral in the bed-bound patient, ankle in the ambulatory) indicates fluid overload from cirrhosis (hypoalbuminaemia, the hepatorenal syndrome), nephrotic syndrome (hypoalbuminaemia), right heart failure, or malnutrition. The distribution and severity (pitting versus non-pitting, the extent up the leg) should be documented. [1]
Deep vein thrombosis. Calf swelling and tenderness — a risk in any immobile patient, and in the hypercoagulable states (malignancy, IBD, nephrotic syndrome, pregnancy, cirrhosis with reduced antithrombin III). [1]
Signs of chronic liver disease on the legs. Peripheral oedema, ecchymoses (coagulopathy), and sparse hair (hormonal). [1]
The presentation template
After completing the examination, present your findings in a structured two-minute summary. The examiner is assessing not only what you found but how you organise and present it — a disorganised presentation loses marks even when the findings are correct. [1]
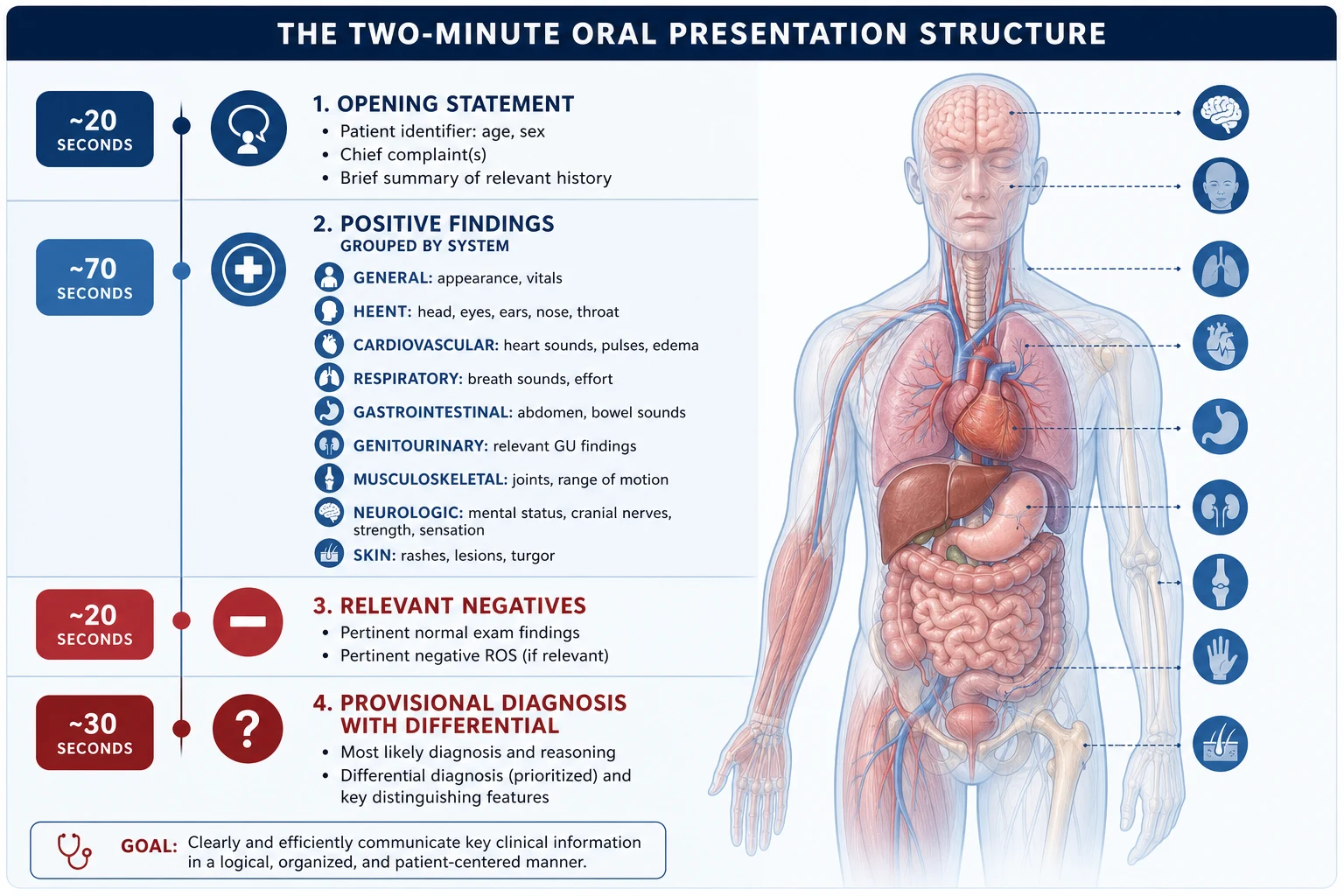
The structure is: [1]
- Opening statement — who, what, and the overall impression
- Positive findings — grouped and prioritised
- Relevant negatives — what you looked for and did not find
- Provisional diagnosis — the most likely diagnosis
- Differential diagnosis — the alternatives ranked by likelihood
- Investigation and management plan — the next steps [1]
Model presentation — chronic liver disease: "I examined this patient's abdomen. At the end of the bed, the patient is cachectic with obvious scleral icterus. In the hands, there is finger clubbing, palmar erythema, and a Dupuytren contracture of the right ring finger. There are excoriations on the forearms consistent with pruritus. On the face, there is scleral icterus, periorbital xanthelasma, and multiple spider naevi on the face and neck. There is no Virchow node. On the chest, there are more than ten spider naevi in the SVC distribution, gynaecomastia, and loss of axillary hair. The abdomen is distended with the flanks filled and an everted umbilicus. There is a caput medusae. Bowel sounds are present and normal. On palpation, the liver edge is palpable 3 cm below the costal margin, firm, with an irregular nodular surface and a hard edge. The spleen is palpable 4 cm below the left costal margin, smooth, with a notch — I can confirm this is the spleen as I cannot get above it. There is shifting dullness confirming ascites, and a fluid thrill indicating large-volume ascites. There is no expansile pulsation to suggest an abdominal aortic aneurysm. There is bilateral pitting oedema to the mid-shin. My findings are consistent with chronic liver disease with portal hypertension and cirrhosis. The likely aetiology, given the xanthelasma and the pruritus, is primary biliary cholangitis, though I would also consider alcohol-related liver disease, viral hepatitis, and metabolic liver disease. I would like to complete my examination with a digital rectal examination and a full set of bloods including liver function tests, synthetic liver function, viral serology, autoantibodies including antimitochondrial antibodies, an abdominal ultrasound with Doppler, and a FibroScan." [1]
Model presentation — organomegaly of unknown cause: "I examined this patient's abdomen. At the end of the bed, the patient is comfortable and not cachectic or icteric. The hands and face are unremarkable, with no clubbing, palmar erythema or stigmata of chronic liver disease. There is no Virchow node. The abdomen is not distended. Bowel sounds are normal. On palpation, there is a large mass in the left upper quadrant extending to the umbilicus and crossing the midline toward the right iliac fossa. It has a smooth surface, a palpable notch on its medial border, and I cannot get above it. It is dull to percussion. This is the spleen — the findings are of massive splenomegaly. There is no hepatomegaly, no ascites, and no expansile pulsation. The most likely cause of massive splenomegaly to this degree is a myeloproliferative neoplasm — chronic myeloid leukaemia or myelofibrosis. I would also consider chronic malaria, visceral leishmaniasis, lymphoma, and a storage disorder such as Gaucher disease. I would like to investigate with a full blood count and film, a bone marrow biopsy, and an abdominal CT." [1]
Discussion by finding — examiner questions
The examiner will ask you to interpret your findings. Below are the high-yield discussion topics for each key finding, with model answers. [1]
Finding: spider naevi
Q: How do you confirm a spider naevus, and what is the distribution? [1]
A spider naevus has a central arteriole with radiating capillary branches. To confirm: press the centre with a glass slide or pinhead — the entire lesion blanches, and on release it refills from the centre outward. The distribution is in the territory of the superior vena cava — face, neck, upper chest, upper arms, and hands. More than five is significant. The pathophysiology is oestrogen excess from impaired hepatic oestrogen metabolism [5].
Finding: hepatomegaly
Q: What are the causes of a large, smooth, tender liver? [1]
Acute viral hepatitis, right heart failure causing hepatic congestion (nutmeg liver), alcoholic hepatitis, Budd-Chiari syndrome (hepatic vein thrombosis), and amoebic liver abscess. The tenderness is from capsular stretching. [1]
Q: What are the causes of a hard, nodular, irregular liver? [1]
Cirrhosis (micronodular in alcohol, macronodular in viral hepatitis) and metastatic malignancy (primary in the colon, stomach, pancreas, breast, lung, or melanoma). A hard, nodular liver in a patient with weight loss is metastatic disease until proven otherwise. [1]
Finding: splenomegaly with hepatomegaly
Q: The patient has both hepatosplenomegaly. What is your differential? [1]
The differential for combined hepatosplenomegaly includes: chronic liver disease with portal hypertension (the spleen enlarges from congestion), haematological malignancy (lymphoma, leukaemia), chronic infection (infectious mononucleosis, malaria, brucellosis, schistosomiasis), storage diseases (Gaucher, Niemann-Pick), and myeloproliferative neoplasms (CML, myelofibrosis, polycythaemia vera). [1]
Finding: ascites
Q: How do you differentiate ascites from other causes of abdominal distension? [1]
The key bedside test is shifting dullness — percussion reveals tympany in the centre (floating bowel) and dullness in the flanks (pooled fluid), and the dullness shifts when the patient rolls onto their side. This distinguishes free fluid from a mass, a cyst, or gas. Obesity produces a uniformly dull abdomen without shifting. An ovarian mass produces central dullness that does not shift. A fluid wave confirms tense, large-volume ascites [1].
Q: What are the causes of ascites with a high serum-ascites albumin gradient (over 11 g/L)? [1]
Portal hypertension — cirrhosis (90 per cent of all ascites), heart failure, Budd-Chiari syndrome, hepatic veno-occlusive disease. A low gradient (under 11 g/L) indicates peritoneal disease — peritoneal carcinomatosis, tuberculous peritonitis, pancreatic ascites, or nephrotic syndrome. [1]
Finding: caput medusae
Q: What does caput medusae indicate and how do you confirm the direction of flow? [1]
Caput medusae (dilated periumbilical veins) indicates portal hypertension with recanalisation of the umbilical vein. To confirm: occlude a segment of vein between two fingers, release one finger, and observe the direction of refill. In portal hypertension, blood flows away from the umbilicus in all directions (upward above the umbilicus, downward below). In IVC obstruction, blood flows upward in all veins. [1]
Finding: expansile pulsation
Q: How do you differentiate an AAA from a normal aorta in a thin patient? [1]
Place your hands on either side of the aorta in the epigastrium. An expansile pulsation pushes the hands apart and outward (the aorta expands in all directions). A transmitted pulsation pushes the hands upward and forward only (the mass is being moved by the aorta but does not itself expand). If there is any doubt, measure the aortic diameter by ultrasound — physical examination alone is not reliable enough to exclude or confirm an AAA [4].
Finding: Virchow node
Q: What is the significance of a left supraclavicular lymph node and what is the mechanism? [1]
A hard, enlarged left supraclavicular node (Virchow node, Troisier sign) is a sentinel node for intra-abdominal malignancy. The mechanism is lymphatic drainage — the thoracic duct drains lymph from the entire abdomen (via the cisterna chyli) into the left venous angle (the junction of the left subclavian vein and the left internal jugular vein). Malignant cells from the abdomen are trapped in the node where the lymph enters the venous system. The classic primary is gastric cancer, but pancreatic, hepatobiliary, testicular, ovarian, and renal malignancy also metastasise here. [1]
Common examination traps and pitfalls
One-line exam answer
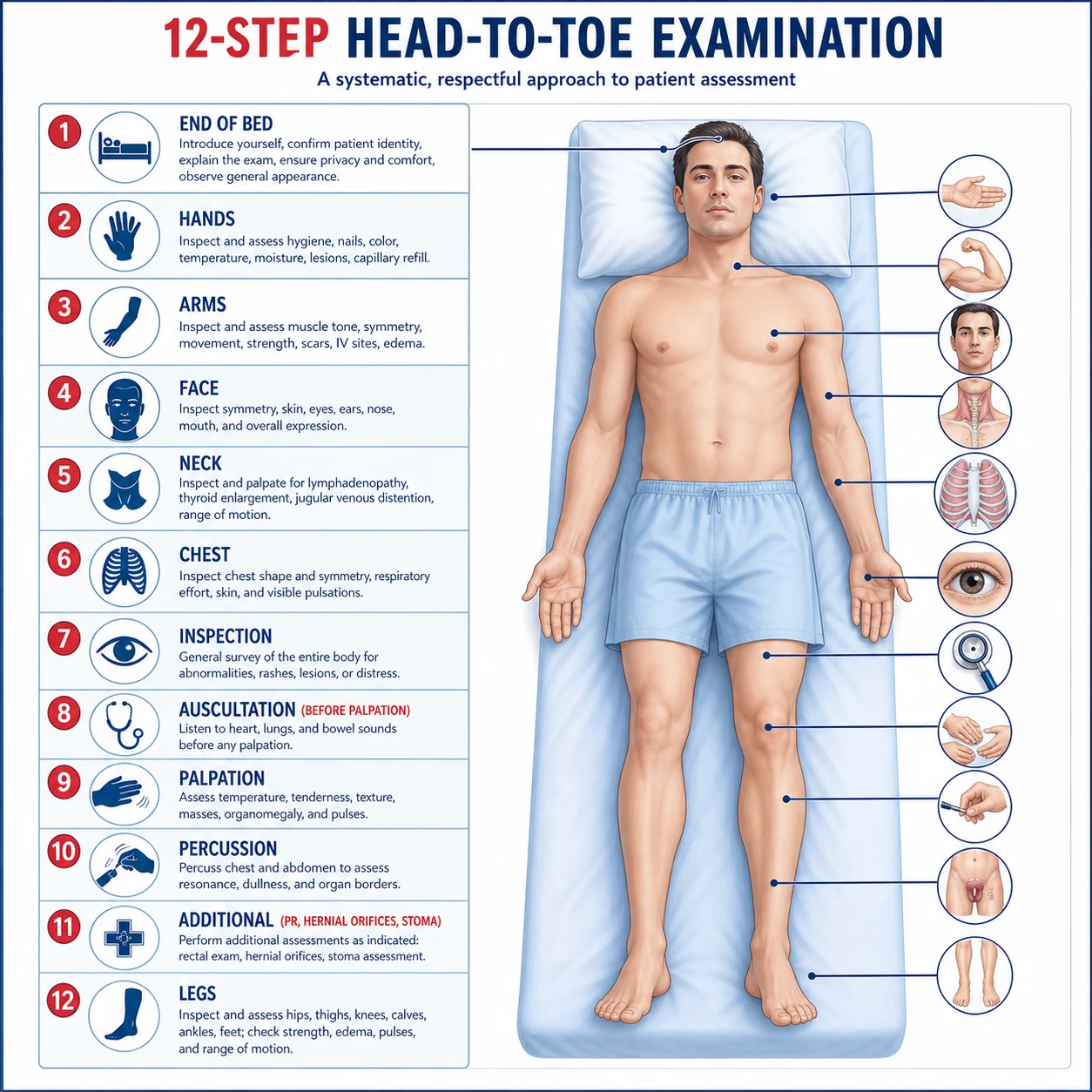
The abdominal examination is a reproducible twelve-step head-to-toe routine: end of bed, hands, arms, face, neck, chest, inspection, auscultation (before palpation), palpation (light then deep, start away from pain), percussion (shifting dullness for ascites), additional (hernial orifices, PR, genitalia, stoma), and legs. The candidate who performs this fluently, differentiates liver from spleen from kidney, identifies the stigmata of chronic liver disease, and presents in a structured format passes the short case. [1]
References and further reading
Williams JW, Simel DL. Does this patient have ascites? JAMA 1992 [1]; Grover SA, Barkun AN, Sackett DL. Does this patient have splenomegaly? JAMA 1993 [2]; Naylor CD. Physical examination of the liver. JAMA 1994 [3]; Lederle FA, Simel DL. Does this patient have abdominal aortic aneurysm? JAMA 1999 [4]; Udell JA, et al. Does this patient with liver disease have cirrhosis? JAMA 2012 [5]. Bates' Guide to Physical Examination and History Taking; Macleod's Clinical Examination; Douglas, Nicol and Robertson, Macleod's Clinical Examination; Hutchison's Clinical Methods. NICE NG12; BSG Guidelines; AASLD Practice Guidelines; GESA.
References
- [1]Williams JW Jr, Simel DL The rational clinical examination. Does this patient have ascites? How to divine fluid in the abdomen JAMA, 1992.PMID 1573754
- [2]Grover SA, Barkun AN, Sackett DL The rational clinical examination. Does this patient have splenomegaly? JAMA, 1993.PMID 8411607
- [3]Naylor CD The rational clinical examination. Physical examination of the liver JAMA, 1994.PMID 8196144
- [4]Lederle FA, Simel DL The rational clinical examination. Does this patient have abdominal aortic aneurysm? JAMA, 1999.PMID 9892455
- [5]Udell JA, Wang CS, Tinmouth J, et al. Does this patient with liver disease have cirrhosis? JAMA, 2012.PMID 22357834