Phys · general-medicine
Anaphylaxis
Also known as anaphylactic shock · allergic reaction · adrenaline · epinephrine · EpiPen · anaphylactoid reaction · mast cell degranulation · venom allergy · perioperative anaphylaxis · biphasic anaphylaxis · idiopathic anaphylaxis
Consultant-physician-depth guide to anaphylaxis — the NIAID/FAAN diagnostic criteria applied at the bedside, IgE-mediated and non-IgE mechanisms, the adrenaline-first acute algorithm with refractory management and the beta-blocker trap, biphasic reactions and observation, serum tryptase timing and interpretation, triggers and cofactors including ACE inhibitors and beta-blockers, perioperative anaphylaxis, venom immunotherapy and drug desensitisation, and the discharge bundle — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Anaphylaxis
The answer first
Anaphylaxis is a clinical diagnosis treated with intramuscular adrenaline — everything else, including the tests, is refinement. Three rules carry you through the DWE, the resus bay and the viva [2] [3]:
- Diagnose on pattern, not on tests or skin signs. The NIAID/FAAN criteria let you make the diagnosis on exposure-plus-multisystem-pattern alone; skin and mucosal signs are absent in up to one in five genuine reactions, and hypotension after a known trigger needs nothing else [1] [3].
- Adrenaline into the anterolateral thigh is the first and most important drug — antihistamines and corticosteroids never substitute for it. Delayed adrenaline, not absent steroids, is the recurring theme in fatality reviews; the Cochrane evidence for the second-line drugs is thin by comparison [11] [6] [7].
- The acute save is only half the job. Every patient gets a tryptase pair, an observation period calibrated to severity, and a discharge bundle — two adrenaline autoinjectors, device training, a written action plan, and specialist allergy referral [9] [13].
Recognition — making the diagnosis at the bedside
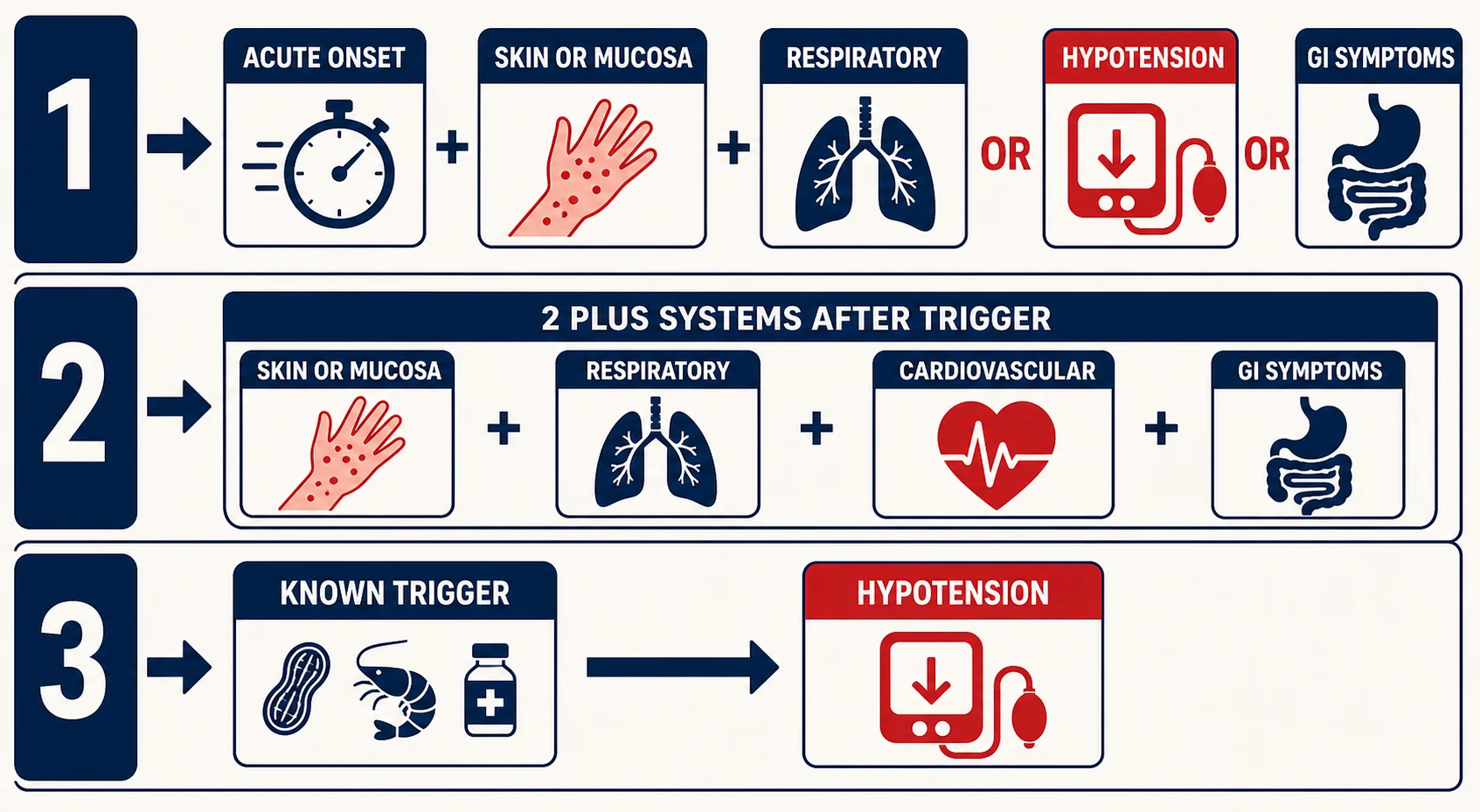
The NIAID/FAAN consensus criteria — reaffirmed in the 2020 World Allergy Organization guidance — exist to make anaphylaxis diagnosable within minutes, in three different clinical costumes. Any ONE of the three is sufficient [1] [3].
| Criterion | The pattern | Bedside translation |
|---|---|---|
| 1. Classic multi-system | Acute onset (minutes to hours) of skin/mucosal involvement — urticaria, flushing, angioedema — PLUS at least one of: respiratory compromise, hypotension or end-organ hypoperfusion, or severe gastrointestinal symptoms | Urticaria or a swollen tongue WITH wheeze, stridor, collapse, or crampy pain and vomiting [1] |
| 2. Likely trigger, two systems | Two or more of: skin/mucosal, respiratory, cardiovascular, gastrointestinal — occurring rapidly after exposure to a likely allergen for that patient | No hypotension required. Urticaria plus wheeze after the first dose of penicillin qualifies [1] |
| 3. Hypotension after a known trigger | Blood pressure fall after exposure to a known allergen for that patient: systolic below 90 mmHg in adults, or a drop of more than 30% from baseline | The criterion that diagnoses anaphylaxis without any skin signs at all — the perioperative and venom-collapse presentation [1] [3] |
Severity grading. Brown's grading system, derived from over a thousand reactions, is the one Australian examiners know: grade 1 is skin and subcutaneous tissue only; grade 2 adds moderate multi-system features (gastrointestinal symptoms, dyspnoea, throat tightness); grade 3 is severe — hypoxia, hypotension, collapse or confusion. Two of Brown's observations earn marks: severe reactions can begin with gastrointestinal symptoms, particularly after insect stings, and early dizziness or collapse in a sting reaction predicts a severe course [10].
What fatal reactions look like. Fatal anaphylaxis is rare and the rate is stable even as admissions rise; iatrogenic triggers — drugs, contrast, perioperative agents — carry the highest case fatality, while fatal food reactions cluster in adolescents and young adults with asthma and delayed adrenaline [11]. Australian data show fatalities rose over 1997–2013, driven by medication-induced deaths [12]. The recurring, preventable themes in fatality reviews are delayed or absent adrenaline, and patients being stood up or walked during the reaction [11].
Pathophysiology — why it looks like this
The IgE-mediated pathway. Sensitisation loads mast-cell and basophil FcεRI receptors with allergen-specific IgE. On re-exposure, the allergen cross-links adjacent IgE molecules and triggers explosive degranulation: preformed mediators (histamine, tryptase) within minutes, then newly synthesised lipid mediators (prostaglandin D₂, leukotrienes) and platelet-activating factor over the following minutes to hours — the biochemical basis of the biphasic reaction [2] [8].
| Mediator | Dominant actions | Clinical correlate |
|---|---|---|
| Histamine | Vasodilatation, increased permeability, bronchospasm, pruritus | Urticaria, flushing, angioedema, wheeze, hypotension [2] |
| Tryptase | Protease released in proportion to mast-cell activation; activates complement and matrix proteases | The measurable fingerprint — the basis of the acute serum test [13] |
| Prostaglandin D₂ / leukotrienes | Sustained bronchospasm, mucus secretion, further vasodilatation | Refractory wheeze; why NSAID-sensitive patients flare through the COX-1 shunt [23] |
| Platelet-activating factor | Potent vasodilatation and permeability; correlates with severity | The mediator most linked to fatal cardiovascular collapse [11] |
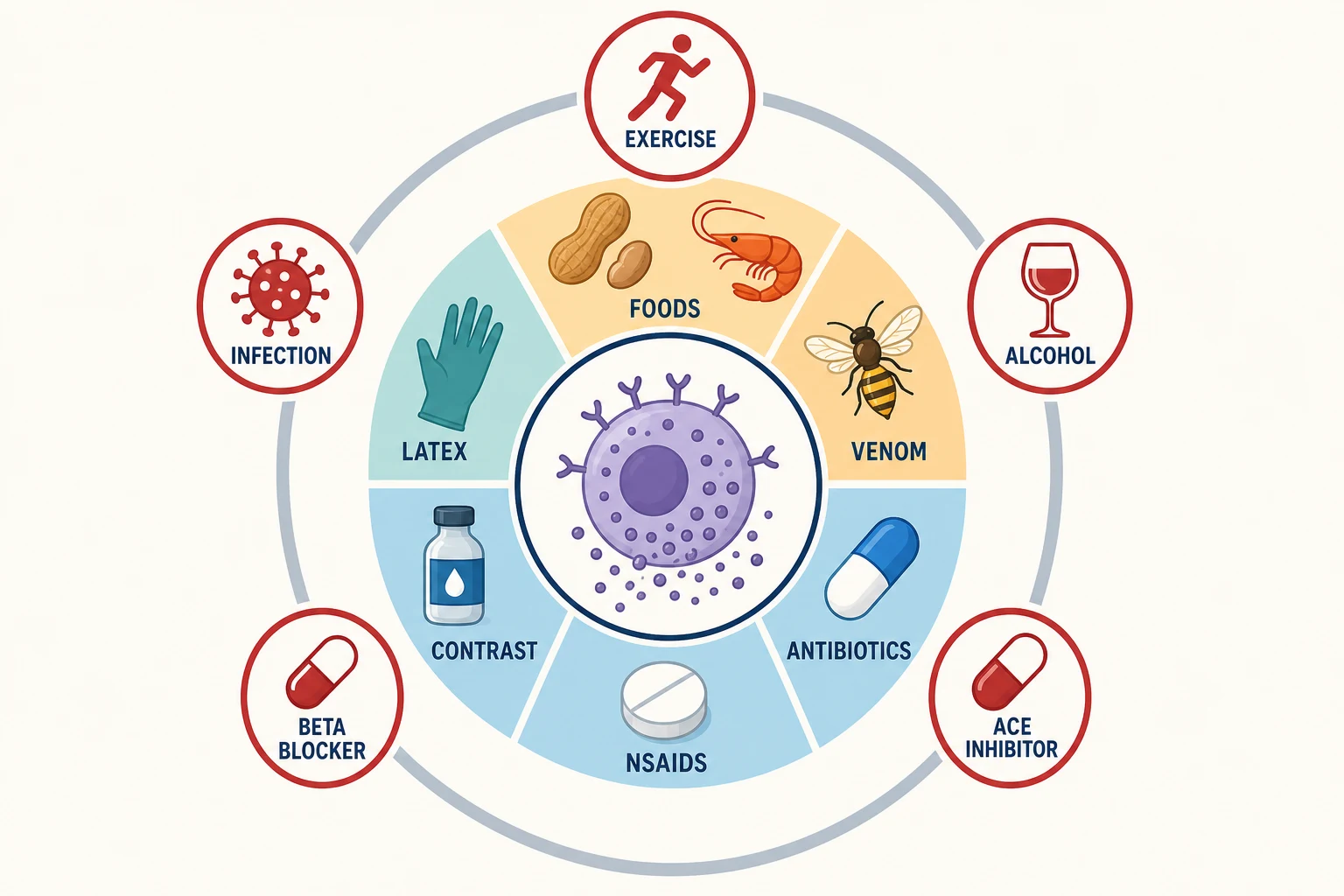
The non-IgE pathways matter because the exam loves them and because they explain reactions on first known exposure: complement-derived anaphylatoxins (C3a, C5a) — the historical “anaphylactoid” reactions to contrast; direct mast-cell activation through MRGPRX2 by drugs such as neuromuscular blockers, vancomycin, opioids and fluoroquinolones; and cyclo-oxygenase-1 inhibition by NSAIDs shunting arachidonic acid toward leukotrienes — the mechanism behind cross-reactive, multi-NSAID hypersensitivity [16] [23]. The classification that matters for NSAIDs is Kowalski's: cross-reactive reactions (any COX-1-inhibiting NSAID triggers; includes NSAID-exacerbated respiratory and cutaneous disease) versus selective single-drug reactions, which are usually IgE-mediated [23].
Why reactions escalate — cofactors. The same allergen dose produces a mild reaction one day and a fatal one the next. The amplifiers examiners test are exercise, alcohol, acute infection, NSAIDs, ACE inhibitors and beta-blockers, and uncontrolled asthma [11] [3]. Beta-blockers deserve their own sentence: they both increase reaction severity and blunt the response to adrenaline, producing the refractory hypotension that answers to glucagon [11] [20]. Food-dependent exercise-induced anaphylaxis — the classic is wheat followed by exertion — is the purest demonstration that the cofactor can be the difference between tolerance and collapse [3].
Acute management — the adrenaline-first algorithm
Whatever the trigger, the first five minutes look the same. This sequence, delivered cleanly, is a complete written answer by itself [2] [3].
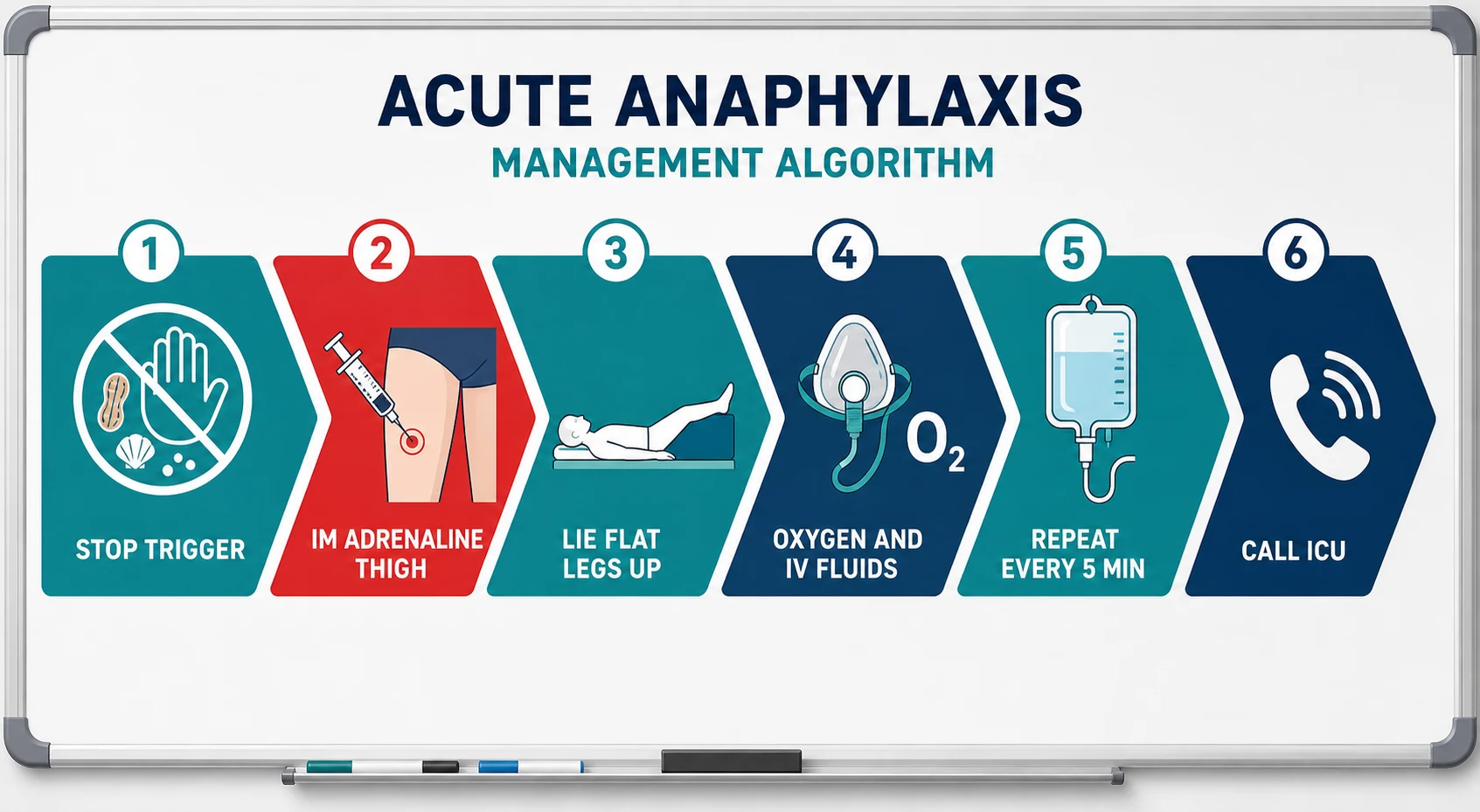
The first five minutes
Stop the trigger and call for help
Stop the infusion, remove the sting, keep the suspected drug vial. Call the MET or anaesthetic help early — do not manage alone
IM adrenaline into the anterolateral thigh
Adult 0.5 mg (0.5 mL of 1:1000). Do not delay for IV access, antihistamines or steroids
Position
Lie flat with legs elevated; left lateral if pregnant; never allow standing or walking
Airway, breathing, circulation
High-flow oxygen; wide-bore IV access; continuous monitoring; prepare for early intubation if the tongue or larynx is swelling
IV crystalloid for hypotension
1–2 litres rapidly in the adult (20 mL/kg aliquots in children) — the circulation is vasodilated and leaking
Repeat adrenaline every 5 minutes
While airway, breathing or circulation features persist; more than one or two doses means call ICU and prepare an adrenaline infusion
Second-line drugs only after resuscitation is underway
Antihistamines for itch and urticaria; corticosteroids on the biphasic rationale; nebulised bronchodilator for persistent wheeze
Adrenaline — get the drug, route and dose exactly right. This is the single most examined prescribing fact in the topic [2].
Adrenaline in anaphylaxis — the numbers that must be reflex
Why intramuscular and why the thigh. Simons' pharmacokinetic work settled this: intramuscular injection into the vastus lateralis produces faster and higher peak plasma adrenaline concentrations than subcutaneous injection, whose absorption is delayed by local vasoconstriction — precisely the wrong pharmacology in a distributive shock [5]. Conversely, undiluted intravenous bolus adrenaline in a perfusing patient is dangerous: arrhythmia, myocardial ischaemia and hypertensive catastrophe are well described, and IV adrenaline is reserved for cardiac arrest dosing or a carefully titrated infusion under monitoring [2] [17].
Fluids and oxygen. High-flow oxygen for everyone with respiratory or circulatory features. Hypotension means the vascular tree has dilated and is leaking — fill it: 1–2 litres of crystalloid rapidly in the adult, reassessing between aliquots; large cumulative volumes are common in refractory cases [2].
The second-line drugs — know exactly what they can and cannot do. Antihistamines (an oral or IV H1-blocker, with or without an H2-blocker) settle itch and urticaria and nothing else; the Cochrane review found no randomised trials of adequate quality establishing their benefit in anaphylaxis, and they do not reverse airway oedema or shock [6]. Corticosteroids are given on the theoretical rationale of preventing protracted or biphasic reactions — the Cochrane review again found no adequate trial evidence, and their onset is far too slow to treat the acute phase [7]. Nebulised salbutamol or adrenaline is a reasonable adjunct for bronchospasm that persists after IM adrenaline [2].
Refractory anaphylaxis — when two doses are not enough
Refractory anaphylaxis — ongoing airway, breathing or circulatory compromise despite at least two appropriately timed IM adrenaline doses — is uncommon but disproportionately lethal. European registry data put multi-dose requirement at roughly one in twenty reactions, with drug-induced reactions and cardiovascular comorbidity over-represented [22]. The management pivot is conceptual: stop repeating isolated boluses and start a titrated adrenaline infusion, with continuous haemodynamic monitoring and intensive-care involvement — this is no longer a ward problem [2] [22].
Escalation, in the order a viva examiner wants it: early ICU call and senior airway help (angioedema can make late intubation impossible); an adrenaline infusion titrated to response under arterial-line or close non-invasive monitoring; ongoing aggressive crystalloid with reassessment for leak and overload; a second vasopressor such as noradrenaline or vasopressin when vasoplegia dominates; and early consideration of extracorporeal support in truly refractory arrest-level cases through ECMO-capable centres [2] [22].
Biphasic reactions and the observation period
A biphasic reaction is recurrence of anaphylaxis features after apparent resolution, without re-exposure. Pooled data put the incidence in the low single figures per cent, with most recurrences within the first several hours but occasional late events; the predictors that matter are a severe index reaction, hypotension, and delayed initial adrenaline [8]. This is why the observation period is calibrated to severity rather than fixed for everyone: observe a minimum of several hours — at least four — after complete resolution, and admit overnight those with severe, hypotensive, refractory or respiratory-dominant reactions, poorly controlled asthma, or late-night presentations where a recurrence would go unnoticed [9] [8].
Investigation — tryptase done properly, then trigger hunting
Serum tryptase is a timing-dependent test, and botched timing is a favourite exam trap. Mast-cell tryptase peaks at one to two hours after symptom onset and falls with a half-life of about two hours [13].
| Sample | When | What it tells you |
|---|---|---|
| Acute sample | As soon as feasible, ideally within 1–2 hours of onset (a second sample at 3–4 hours is used in perioperative protocols) | The peak — elevation supports mast-cell activation; correlates roughly with severity [13] [14] |
| Baseline sample | After 24 hours, or at follow-up | The comparator — and, if persistently elevated, a clue to mastocytosis or hereditary alpha-tryptasaemia [13] [15] |
Interpretation is a delta, not a single number: the consensus criterion for significant acute release is a peak of at least 1.2 × baseline + 2 micrograms/L [15]. Two warnings: a normal acute tryptase does not exclude anaphylaxis — food-triggered reactions in particular often show no rise — and an elevated baseline reframes the whole case toward a clonal mast-cell disorder, which needs KIT D816V testing and haematology input [13] [15].
Trigger testing waits. Allergen-specific IgE and skin-prick testing are performed at least 4–6 weeks after the reaction, because the acute period produces false negatives from mediator depletion and test suppression; the clinical history remains the highest-yield investigation, and testing without a compatible history generates false positives that mislabel patients for life [9] [19]. Basophil activation testing and supervised challenge have defined but specialist-level roles [9].
Triggers and cofactors — the landscape
Trigger patterns shift with age and setting, and the DWE expects you to know the distribution, not just the list [3] [16].
| Setting | Dominant triggers | Physician-level notes |
|---|---|---|
| Community — foods | Peanut, tree nuts, shellfish, fish, wheat, egg and milk (children) | Adolescents and young adults with asthma dominate fatal food reactions; cofactor-loaded reactions (exercise, alcohol, NSAIDs) are the adult pattern [11] |
| Community — venom | Bee and wasp stings; jack jumper ants in parts of Australia | Cardiovascular collapse without skin signs is classic; early GI symptoms predict severity; immunotherapy is disease-modifying [10] [19] |
| Hospital — drugs | Antibiotics (beta-lactams), NSAIDs, chemotherapy and monoclonal antibodies | The highest case-fatality category; check the anaesthetic chart and the drug chart before blaming the antibiotic [11] [21] |
| Perioperative | Neuromuscular blockers, antibiotics, chlorhexidine, patent blue dye, latex | Cardiovascular-first presentation under drapes; NAP6 reshaped both recognition and dosing [16] [17] |
| Radiology — contrast | Iodinated contrast (non-IgE, complement-mediated) | Premedication and agent change for future imaging; the history is usually mislabelled as “allergy” [23] |
| Physical | Exercise (with or without a food cofactor), cold, sunlight | Food-dependent exercise-induced anaphylaxis — classically wheat — is the DWE favourite [3] |
The medication cofactors deserve consultant-level precision. ACE inhibitors increase reaction severity — plausibly through bradykinin — and beta-blockers both worsen reactions and impair adrenaline response; both associations appear in fatal-reaction series [11]. This drives a real discharge decision: after a serious venom or idiopathic reaction, review the ACE inhibitor and beta-blocker, weigh the cardiovascular indication against the allergy risk, and document the shared decision — particularly when venom immunotherapy is planned [19].
Special contexts
Perioperative anaphylaxis. Under anaesthesia, the first sign is usually cardiovascular — refractory hypotension or a rising airway pressure — and skin signs are hidden under drapes or absent entirely; NAP6, the UK national audit, found an incidence around one in ten thousand anaesthetics with antibiotics and neuromuscular blockers leading the culprits and chlorhexidine and patent blue dye prominent [16]. Management follows the same adrenaline-first logic but with anaesthesia-specific dosing discipline — early adrenaline in small titrated IV increments by the anaesthetist in a monitored, arrested-or-arresting patient, alongside stopping all suspect agents, calling for help, and maintaining the airway [17]. Every case gets three tryptase samples (immediate, 1–2 hours, and baseline after 24 hours) and mandatory referral to a specialist drug-allergy service before any future anaesthetic — patients have died from unlabelled re-exposure [14] [17].
Venom allergy and immunotherapy. A systemic reaction to a sting — anything beyond large local swelling — earns specific IgE and skin testing plus an immunology referral. Venom immunotherapy is the only disease-modifying treatment in allergy practice: the Cochrane review confirms it substantially reduces the risk of subsequent systemic reactions, and the practice parameter recommends it for patients with systemic reactions, typically continued for three to five years, with the autoinjector carried until protection is established [18] [19]. Immunotherapy itself provokes reactions, so it belongs in specialist hands — and the beta-blocker conversation happens before it starts [19].
Drug desensitisation. When the triggering drug is irreplaceable — first-line chemotherapy or a monoclonal antibody, aspirin after coronary stenting in an NSAID-sensitive patient, penicillin for syphilis in pregnancy — rapid desensitisation induces temporary tolerance through escalating micro-doses delivered over hours under resuscitation capability. It works for the duration of that course only, must be repeated for every subsequent course, and changes neither the underlying allergy nor the need for the discharge bundle [21].
Idiopathic anaphylaxis and the mast-cell question. Recurrent reactions without an identified trigger are a diagnosis of exclusion and a DCE long-case staple. The physician's sequence: reconstruct every episode minutely (foods in the preceding six hours, exercise, alcohol, NSAIDs, intercurrent illness, menstruation), check a baseline tryptase, and if elevated — or if episodes are severe and unexplained — pursue clonal disease with KIT D816V testing and haematology referral, because systemic mastocytosis and mast-cell activation syndromes hide inside this label [15] [13]. Management while hunting: twice-daily non-sedating antihistamine cover, meticulous cofactor control, autoinjectors, and a written plan — and specialist escalation for prophylactic options [15].
Discharge and prevention — where physicians earn their fee
The emergency department treats; the physician prevents the next one. The discharge bundle is fixed and auditable [9]:
- Two adrenaline autoinjectors (300 micrograms for adults and children over 30 kg; 150 micrograms for 15–30 kg), prescribed before the patient leaves, with hands-on device training and teach-back — carrying is not the same as being able to use [9].
- A written anaphylaxis action plan — the ASCIA plan in Australia — naming the trigger, the early features, the device steps, and the ambulance call [9].
- Specialist allergy/immunology referral for trigger confirmation, immunotherapy or desensitisation decisions, and cofactor review [9] [19].
- Medication and comorbidity review — ACE inhibitors and beta-blockers reconsidered, asthma brought under control, and a medical-alert record [11].
The DCE long-case angle is the patient with recurrent or idiopathic anaphylaxis: examiners want to see you move from the acute event to the system — episode reconstruction, trigger and cofactor audit, baseline tryptase and mast-cell screening, autoinjector technique observed in the room, action plans embedded at school or work, and the psychological weight of unpredictable reactions addressed openly [15] [9].
The short-case and counselling angles. There is no classical anaphylaxis short case, so it appears in two costumes: the examination of the recovered patient — skin for urticaria pigmentosa and a Darier sign, dermatographism, ENT for residual angioedema, chest for asthma control, and “show me your autoinjector” — and the counselling station, where you must discharge a first-reaction patient in eight minutes with device, plan and referral, and answer “will the next one be worse?” honestly: severity is not reliably progressive, but every reaction warrants the full safety net [9] [3].
Exam traps, collected
References
- [1]Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second symposium on the definition and management of anaphylaxis: summary report--Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium J Allergy Clin Immunol, 2006.PMID 16461139
- [2]Muraro A, Roberts G, Worm M, et al. Anaphylaxis: guidelines from the European Academy of Allergy and Clinical Immunology Allergy, 2014.PMID 24909803
- [3]Cardona V, Ansotegui IJ, Ebisawa M, et al. World allergy organization anaphylaxis guidance 2020 World Allergy Organ J, 2020.PMID 33204386
- [4]Simons FE, Ardusso LR, Bilò MB, et al. World allergy organization guidelines for the assessment and management of anaphylaxis World Allergy Organ J, 2011.PMID 23268454
- [5]Simons FE, Gu X, Simons KJ Epinephrine absorption in adults: intramuscular versus subcutaneous injection J Allergy Clin Immunol, 2001.PMID 11692118
- [6]Sheikh A, Ten Broek V, Brown SG, et al. H1-antihistamines for the treatment of anaphylaxis: Cochrane systematic review Allergy, 2007.PMID 17620060
- [7]Choo KJ, Simons E, Sheikh A Glucocorticoids for the treatment of anaphylaxis: Cochrane systematic review Allergy, 2010.PMID 20584003
- [8]Lee S, Bellolio MF, Hess EP, et al. Time of Onset and Predictors of Biphasic Anaphylactic Reactions: A Systematic Review and Meta-analysis J Allergy Clin Immunol Pract, 2015.PMID 25680923
- [9]Campbell RL, Li JT, Nicklas RA, et al. Emergency department diagnosis and treatment of anaphylaxis: a practice parameter Ann Allergy Asthma Immunol, 2014.PMID 25466802
- [10]Brown SG Clinical features and severity grading of anaphylaxis J Allergy Clin Immunol, 2004.PMID 15316518
- [11]Turner PJ, Jerschow E, Umasunthar T, et al. Fatal Anaphylaxis: Mortality Rate and Risk Factors J Allergy Clin Immunol Pract, 2017.PMID 28888247
- [12]Mullins RJ, Wainstein BK, Barnes EH, et al. Increases in anaphylaxis fatalities in Australia from 1997 to 2013 Clin Exp Allergy, 2016.PMID 27144664
- [13]Schwartz LB Diagnostic value of tryptase in anaphylaxis and mastocytosis Immunol Allergy Clin North Am, 2006.PMID 16931288
- [14]Vitte J, Sabato V, Tacquard C, et al. Use and Interpretation of Acute and Baseline Tryptase in Perioperative Hypersensitivity and Anaphylaxis J Allergy Clin Immunol Pract, 2021.PMID 33746087
- [15]Valent P, Akin C, Arock M, et al. Definitions, criteria and global classification of mast cell disorders with special reference to mast cell activation syndromes: a consensus proposal Int Arch Allergy Immunol, 2012.PMID 22041891
- [16]Harper NJN, Cook TM, Garcez T, et al. Anaesthesia, surgery, and life-threatening allergic reactions: epidemiology and clinical features of perioperative anaphylaxis in the 6th National Audit Project (NAP6) Br J Anaesth, 2018.PMID 29935567
- [17]Harper NJN, Cook TM, Garcez T, et al. Anaesthesia, surgery, and life-threatening allergic reactions: management and outcomes in the 6th National Audit Project (NAP6) Br J Anaesth, 2018.PMID 29935569
- [18]Boyle RJ, Elremeli M, Hockenhull J, et al. Venom immunotherapy for preventing allergic reactions to insect stings Cochrane Database Syst Rev, 2012.PMID 23076950
- [19]Golden DB, Demain J, Freeman T, et al. Stinging insect hypersensitivity: A practice parameter update 2016 Ann Allergy Asthma Immunol, 2017.PMID 28007086
- [20]Zaloga GP, DeLacey W, Holmboe E, et al. Glucagon reversal of hypotension in a case of anaphylactoid shock Ann Intern Med, 1986.PMID 3717811
- [21]Castells MC Anaphylaxis to chemotherapy and monoclonal antibodies Immunol Allergy Clin North Am, 2015.PMID 25841555
- [22]Francuzik W, Dölle-Bierke S, Knop M, et al. Refractory Anaphylaxis: Data From the European Anaphylaxis Registry Front Immunol, 2019.PMID 31749797
- [23]Kowalski ML, Stevenson DD Classification of reactions to nonsteroidal antiinflammatory drugs Immunol Allergy Clin North Am, 2013.PMID 23639704