Phys · general-medicine
Cardiovascular System Examination — The Classic DCE Short-Case Routine
Also known as cardiovascular examination · cardiovascular system examination · cardiac examination · praecordial examination · murmur examination · auscultation of the heart · JVP examination · apex beat examination · cardiovascular short case · PACES cardiovascular station · dynamic cardiac manoeuvres · valve examination · short case cardiovascular
Consultant-physician-depth guide to the systematic cardiovascular system examination as performed in the FRACP, MRCP PACES and ABIM clinical examinations. Covers the reproducible eleven-step routine from the end-of-bed survey through the hands, face, eyes, neck and jugular venous pressure, the praecordium (inspection, palpation of the apex beat and thrills), the systematic four-area auscultation with the diaphragm and bell, the dynamic manoeuvres (respiration, Valsalva, squat-to-stand, hand grip), the back, abdomen and legs, the timing-based murmur framework, the candidate's spoken presentation template, the examiner discussion by finding, and the common examination traps and pitfalls.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Cardiovascular System Examination — The Classic DCE Short-Case Routine

The answer first
The instruction "Please examine this patient's cardiovascular system" is the single commonest short case in the FRACP Divisional Clinical Examination, the MRCP PACES Station 3, and the ABIM clinical assessment. The examiner is not primarily testing diagnosis — the diagnosis is often deliberately straightforward. The examiner is testing whether the candidate can perform a complete, fluent, reproducible examination that follows a logical sequence, elicits every relevant sign, and then presents the findings in a structured, confident, hypothesis-driven way. The candidate who walks straight to the chest and listens has already failed the question. [1]
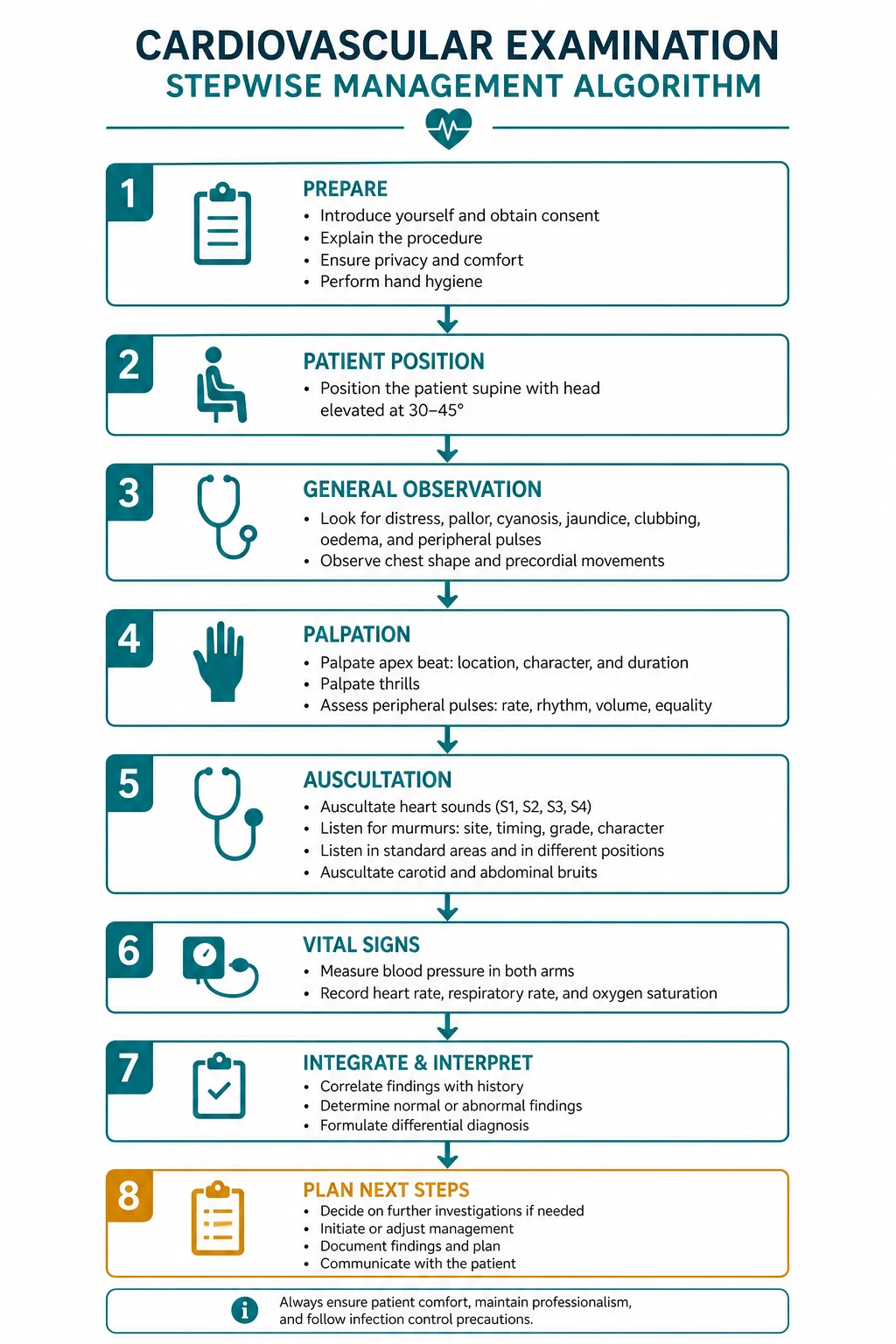
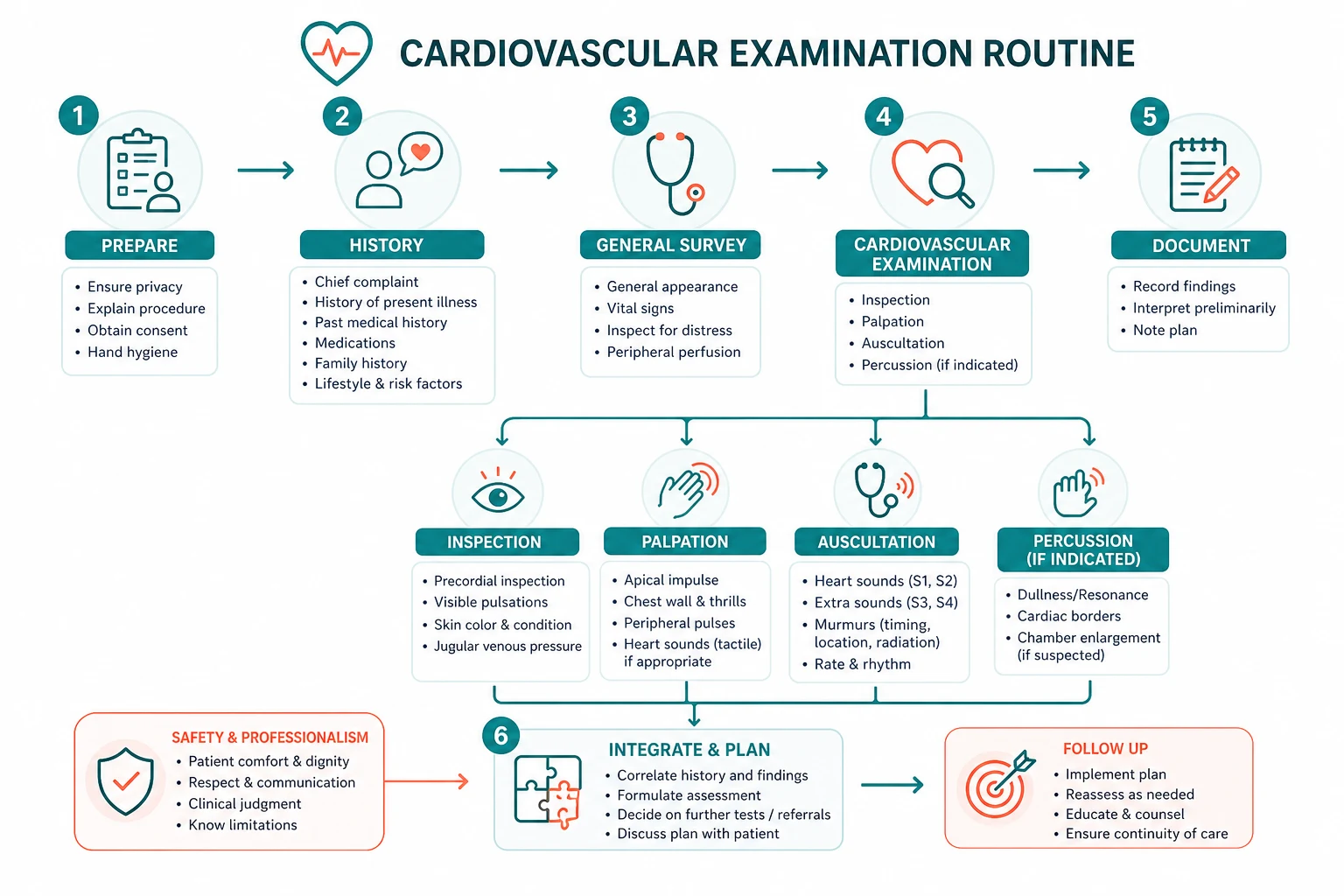
The reproducible routine, committed to muscle memory before the examination, is: [1]
- End of bed — breathless, cyanosed, cachectic, Cushingoid, skeletal abnormalities (Marfanoid habitus), obvious scars and devices.
- Hands — clubbing, peripheral stigmata of endocarditis, peripheral cyanosis, tendon xanthomata, the pulse (rate, rhythm, character).
- Face — malar flush, dysmorphic features, dental caries, high arched palate.
- Eyes — conjunctival pallor, xanthelasma, corneal arcus, hypertelorism, blue sclerae.
- Neck — the jugular venous pressure (height and waveform), the carotid pulse (character and volume).
- Praecordium — inspect (scars, visible impulses), palpate the apex beat (position and character), palpate for thrills and a right ventricular heave.
- Auscultation — the four valve areas, diaphragm and bell, timing and character of every sound.
- Dynamic manoeuvres — respiration, Valsalva, squat-to-stand, hand grip.
- Back — basal crackles, pleural effusion.
- Abdomen — hepatomegaly, pulsatile liver, ascites, splenomegaly.
- Legs — peripheral oedema, peripheral pulses, deep vein thrombosis signs. [1]
The three principles that govern the whole encounter: [1]
- Sequence before sophistication. A complete, fluent, well-organised examination with a simple correct interpretation beats a brilliant but incomplete one. The examiner marks the routine first.
- Characterise the murmur by timing first. Timing is the single most reliable bedside discriminator. Systolic, diastolic, or continuous — then site, radiation, character, pitch, and the effect of dynamic manoeuvres [5].
- Present with a hypothesis. The presentation names the dominant finding, offers the anatomical and pathological diagnosis, and states the single investigation that confirms it. A list of unconnected observations is a fail; a synthesis is a pass.
DCE short-case trap: The candidate who walks to the chest and listens has committed the cardinal error — the cardiovascular examination begins at the end of the bed and ends at the legs, and the stethoscope is one instrument among many. The examiner has already formed a judgement before the candidate picks up the stethoscope. [1]
The examination-sequence diagram

The sequence below is the routine every candidate should rehearse until it is automatic. Each step is described as the candidate performs it, with the key signs and their interpretation. [1]
Step 1 — The end-of-bed survey
Before touching the patient, stand at the foot of the bed and take five seconds. The observations gathered here frame the entire examination: [1]
- Breathlessness and distress — is the patient comfortable at rest, breathless on minimal exertion, or in respiratory distress? The patient in acute pulmonary oedema will be sitting upright, sweating, breathless and using accessory muscles.
- Cyanosis — central (blue tongue and lips, warm) indicates hypoxaemia or a right-to-left shunt; peripheral (blue cold fingers with normal tongue) indicates poor perfusion.
- Cachexia — cardiac cachexia in advanced heart failure is a poor prognostic sign.
- Cushingoid habitus — from chronic steroid therapy (post-transplant, vasculitis), relevant to hypertension and fluid overload.
- Skeletal and body-habitus clues — the tall, thin, long-limbed patient with an arm span exceeding height and a low upper-segment-to-lower-segment ratio suggests Marfan syndrome (aortic root aneurysm, aortic regurgitation, mitral valve prolapse); the short, web-necked patient with a shield chest suggests Noonan syndrome (pulmonary stenosis, hypertrophic cardiomyopathy); the markedly obese, plethoric, buffalo-hump patient suggests Cushing syndrome.
- Scars and devices — median sternotomy (prior cardiac surgery), left or right subclavicular device bump (pacemaker or defibrillator), a lateral thoracotomy (mitral valvotomy, coarctation repair). [1]
Step 2 — The hands
The hands carry more cardiovascular information per square centimetre than any other region. Take the patient's right hand and examine both the dorsal and palmar surfaces: [1]
Clubbing. Assess using Schamroth's sign — the patient opposes the dorsal surfaces of the terminal phalanges of the same finger on each hand; the normal diamond-shaped window disappears with clubbing, and the distal phalangeal profile becomes convex. The cardiovascular causes of clubbing are cyanotic congenital heart disease (tetralogy of Fallot, transposition, Eisenmenger syndrome) and infective endocarditis. Aortic regurgitation, by contrast, does not cause clubbing unless there is an associated patent ductus arteriosus with reversal. The distinction matters: clubbing with a central cyanotic lesion points to congenital disease; clubbing with a new murmur and fever points to endocarditis. [1]
Peripheral stigmata of infective endocarditis. Look for splinter haemorrhages (linear red-brown streaks in the nail bed, best seen with the fingertip held against a light), Osler nodes (tender nodules on the finger and toe pads, immunological in origin), and Janeway lesions (painless macular erythematous lesions on the palms and soles, septic emboli). Splinter haemorrhages are non-specific (also caused by trauma), but Osler nodes and Janeway lesions, when present with a murmur, are highly suggestive of endocarditis. [1]
Peripheral cyanosis and perfusion. Cold, blue, slow-recovering digits indicate poor peripheral perfusion (low cardiac output, vasoconstriction). [1]
Tendon xanthomata. Yellow-orange nodular swellings along the extensor tendons (dorsum of the hand, the Achilles tendon, the extensor tendons of the fingers) indicate familial hypercholesterolaemia — a major risk factor for premature atherosclerosis and aortic stenosis. [1]
The radial pulse. Assess rate, rhythm, and character. Rate and rhythm: count for at least 30 seconds; an irregularly irregular pulse is atrial fibrillation. Character is the high-yield, high-fail component: [1]
- Bounding (water-hammer, collapsing) pulse — a large-volume pulse that collapses sharply in diastole, characteristic of aortic regurgitation. Confirm by elevating the arm and grasping the wrist firmly with the palm — the slapping impact is unmistakable.
- Slow-rising (pulsus parvus et tardus) pulse — a small-volume pulse with a delayed peak, characteristic of aortic stenosis.
- Pulsus alternans — alternation of a strong and a weak beat at a regular interval, indicating severe left ventricular failure.
- Radiofemoral delay — feel the radial and femoral pulses simultaneously; a delay, with upper-limb hypertension, indicates coarctation of the aorta. This is a mandatory manoeuvre in the young hypertensive patient. [1]
All peripheral pulses. Examine the brachial, radial, and — later — the femoral, popliteal, posterior tibial and dorsalis pedis pulses. Absent or unequal pulses point to peripheral arterial disease, coarctation, or dissection. [1]
Step 3 — The face
- Malar flush — the plum-red discolouration over the cheeks, classically associated with mitral stenosis (and pulmonary hypertension).
- Dysmorphic features — downslanting palpebral fissures, low-set ears, a webbed neck and a shield chest suggest Noonan syndrome (pulmonary stenosis, hypertrophic cardiomyopathy). The coarse facies of myxoedema or acromegaly point to their respective cardiac associations.
- Dental caries and halitosis — poor dentition is a risk factor for infective endocarditis; mention it as a relevant positive that informs prevention.
- High arched palate — ask the patient to open wide; a high arched palate with dental crowding is a feature of Marfan syndrome.
- Facies of hyperlipidaemia — corneal arcus in the young (under 40), or tuberous xanthomata on the elbows. [1]
Step 4 — The eyes
- Conjunctival pallor — anaemia, which may worsen a flow murmur or a high-output state.
- Xanthelasma — yellow lipid deposits on the eyelids, indicating hyperlipidaemia.
- Corneal arcus — a grey-white ring at the corneal margin; significant only in the young (under 40) as a marker of hyperlipidaemia; in the elderly it is an age-related finding (arcus senilis).
- Hypertelorism — widely spaced eyes, a feature of Noonan syndrome.
- Blue sclerae — the thin, translucent sclerae of osteogenesis imperfecta, associated with aortic root dilatation and aortic regurgitation.
- Ectopia lentis (on fundoscopy or noted from the history) — upward lens dislocation, pathognomonic of Marfan syndrome. [1]
Step 5 — The neck — the jugular venous pressure and the carotid pulse
The jugular venous pressure (JVP). Position the patient at 45 degrees, with the head turned slightly away and the neck muscles relaxed. Use the right internal jugular vein (deep, medial to sternocleidomastoid) as the reference. Identify the height — the vertical distance from the sternal angle to the top of the pulsation, measured in centimetres; the normal is less than 3 cm, and a value above 4 cm is elevated. Then identify the waveform: [1]
- a wave — atrial contraction. Cannon a waves (regular, large intermittent waves) indicate complete heart block or ventricular tachycardia with atrioventricular dissociation. Absent a waves occur in atrial fibrillation.
- v wave — venous filling against a closed tricuspid valve. Large systolic (cv, or prominent v) waves indicate tricuspid regurgitation — the regurgitant jet fills the venous system in systole.
- x and y descents — a slow y descent suggests tricuspid stenosis; a rapid y descent suggests constrictive pericarditis or severe tricuspid regurgitation. [1]
The JVP is distinguished from the carotid pulse by four features: it is not palpable, it changes with position (lowering the patient raises it), it rises with abdominal pressure (hepatojugular reflux), and it has a complex waveform (two peaks per cycle, unlike the single carotid upstroke). [1]
The carotid pulse. Palpate the carotid to confirm the pulse character and volume that you inferred from the radial — the slow-rising pulse of aortic stenosis and the collapsing pulse of aortic regurgitation are best appreciated at the carotid. Do not palpate both carotids simultaneously (risk of cerebral ischaemia). [1]
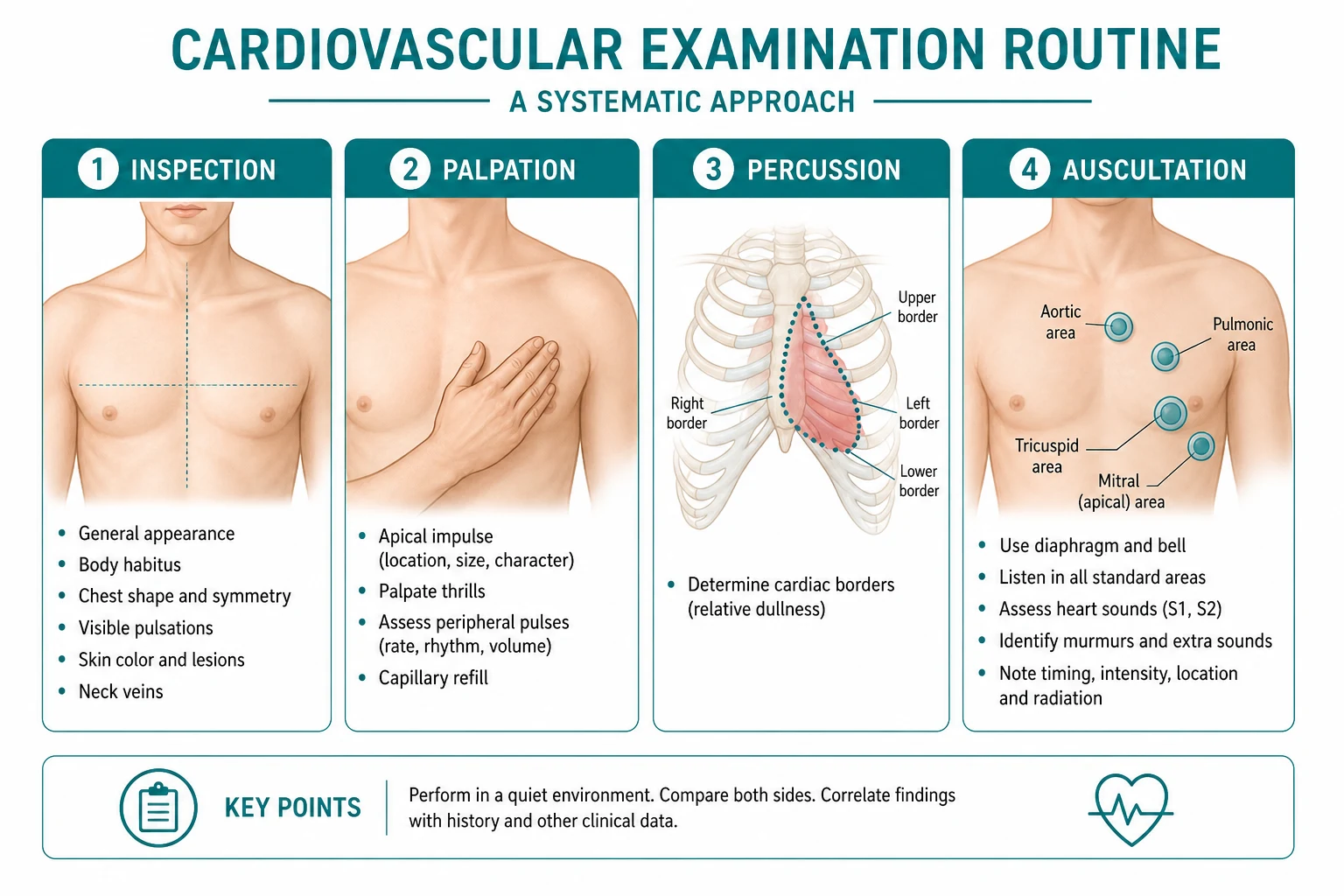
Step 6 — The praecordium — inspection and palpation
Inspection. Look for median sternotomy and thoracotomy scars, visible impulses (a hyperdynamic apex, a parasternal heave), chest-wall deformities (pectus excavatum in Marfan syndrome), and device bumps. [1]
Palpation of the apex beat. With the flat of the right hand, localise the most lateral point of maximal cardiac impulse. The normal position is the fifth intercostal space in the midclavicular line. Three features matter: [1]
- Position — displacement laterally indicates ventricular dilatation (dilated cardiomyopathy, volume overload, severe mitral or aortic regurgitation, heart failure).
- Character — thrusting (heaving) — a forceful, sustained impulse indicating pressure overload (aortic stenosis, hypertension, hypertrophic cardiomyopathy).
- Character — tapping — a localized, low-volume, non-displaced tapping impulse indicating mitral stenosis (the palpable, loud first heart sound).
- Character — diffuse and hyperdynamic — a widespread, poorly localised impulse indicating left ventricular failure or a high-output state. [1]
The right ventricular heave. Place the heel of the hand on the left parasternal edge; a sustained lifting impulse, felt best on full expiration, indicates right ventricular hypertrophy or dilatation (pulmonary hypertension, pulmonary stenosis, cor pulmonale, atrial septal defect). [1]
Thrills. A palpable murmur — a vibration like a purring cat. A systolic thrill at the upper right sternal edge suggests severe aortic stenosis (a murmur grade 4 of 6 or above); a diastolic thrill at the left sternal edge suggests severe aortic regurgitation; a continuous thrill under the left clavicle suggests a patent ductus arteriosus. [1]
Step 7 — Auscultation — the systematic four-area approach
Listen with both the diaphragm (high-pitched sounds — aortic regurgitation, the first and second heart sounds, most systolic murmurs) and the bell (low-pitched sounds — the mitral stenosis rumble, the third and fourth heart sounds). Use the four traditional areas, remembering that they are areas of maximal radiation, not valve locations: [1]
- Apex (mitral area) — the fifth intercostal space, midclavicular line. Roll the patient onto the left side and listen with the bell for the low-pitched mid-diastolic rumble and opening snap of mitral stenosis, and the pansystolic murmur of mitral regurgitation.
- Lower left sternal edge (tricuspid area) — the fourth intercostal space at the left sternal edge. Listen for the pansystolic murmur of tricuspid regurgitation (louder on inspiration — Carvallo's sign).
- Left upper sternal edge (pulmonary area) — the second intercostal space at the left sternal edge. Listen for the ejection systolic murmur of pulmonary stenosis and the pulmonary component of the second heart sound (a loud P2 indicates pulmonary hypertension).
- Right upper sternal edge (aortic area) — the second intercostal space at the right sternal edge. Listen for the ejection systolic murmur of aortic stenosis radiating to the carotids, and the early diastolic murmur of aortic regurgitation. [1]
For aortic regurgitation, sit the patient forward, ask them to hold their breath in expiration, and listen with the diaphragm at the left sternal edge (the third intercostal space — Erb's point) pressed firmly. [1]
At each area, identify, in order: the first heart sound (S1), the second heart sound (S2) and its splitting (normal, wide, fixed, paradoxical), added sounds (the third heart sound S3, the fourth heart sound S4, an ejection click, an opening snap, a pericardial knock), and murmurs. Characterise every murmur by timing, location, radiation, grade (1 to 6), pitch, and the effect of respiration and the dynamic manoeuvres. [1]
Heart sounds:
- S1 (mitral and tricuspid closure) — loud in mitral stenosis (the taut, stenotic valve snaps shut); soft in mitral regurgitation and first-degree heart block.
- S2 (aortic and pulmonary closure) — the aortic component (A2) is normally louder and precedes the pulmonary component (P2). Wide fixed splitting indicates an atrial septal defect. Paradoxical (reversed) splitting (P2 before A2, splitting widening on expiration) indicates severe aortic stenosis or left bundle branch block. A loud P2 indicates pulmonary hypertension.
- S3 (the third heart sound, the ventricular gallop) — a low-pitched sound just after S2, best heard with the bell at the apex; indicates heart failure with elevated filling pressures or a high-output state. In the patient over 40 it is pathological.
- S4 — a low-pitched sound just before S1, from atrial contraction into a stiff ventricle; indicates a hypertrophied, non-compliant ventricle (hypertension, aortic stenosis, hypertrophic cardiomyopathy).
- Ejection click — an early systolic sound from a stenotic but still mobile aortic or pulmonary valve (bicuspid aortic valve, pulmonary stenosis).
- Opening snap — an early diastolic sound from a stenotic mitral valve opening, followed by the mid-diastolic rumble of mitral stenosis. [1]
The murmur framework — timing first

Classify every murmur by timing first, then site, then character. This is the single most reliable bedside discriminator and the approach a PACES examiner expects [5].
| Timing | Murmur | Site | Radiation | Character | Key modifiers |
|---|---|---|---|---|---|
| Ejection systolic | Aortic stenosis | Upper right sternal edge | To the carotids | Crescendo-decrescendo | Slow-rising pulse; soft A2; later-peaking as severity increases |
| Ejection systolic | Pulmonary stenosis | Upper left sternal edge | To the left lung field | Crescendo-decrescendo | Loud P2 if mild; soft P2 if severe; ejection click |
| Ejection systolic | Hypertrophic cardiomyopathy | Lower left sternal edge | Variable | Crescendo-decrescendo | Louder on Valsalva and on standing; softer on squatting and hand grip |
| Pansystolic | Mitral regurgitation | Apex | To the axilla | Blowing | Louder on expiration; soft S1; thrusting apex |
| Pansystolic | Tricuspid regurgitation | Lower left sternal edge | To the right sternal edge and liver | Blowing | Louder on inspiration (Carvallo); prominent v waves; pulsatile liver |
| Pansystolic | Ventricular septal defect | Lower left sternal edge | Localised (no radiation) | Harsh | Often with a thrill |
| Early diastolic | Aortic regurgitation | Left sternal edge (3rd ICS, Erb's point) | None | High-pitched, decrescendo | Heard best sitting forward, breath held in expiration; wide pulse pressure |
| Mid-diastolic | Mitral stenosis | Apex | Localised | Low-pitched rumble | Loud S1; opening snap; bell of stethoscope, left lateral position |
| Continuous | Patent ductus arteriosus | Under the left clavicle | None | Machinery | Thrill; bounding pulses |
Murmur grade (Levine scale)
- Very faint, heard only after tuning in. 2. Faint, heard immediately. 3. Loud, no thrill. 4. Loud with a thrill. 5. Very loud, heard with the stethoscope partly off the chest. 6. Heard with the stethoscope off the chest. A grade 4 or above always has a thrill — if you feel a thrill, the murmur is at least grade 4. [1]
Austin Flint murmur
In severe aortic regurgitation, the regurgitant jet impinges on the anterior mitral leaflet, producing a low-pitched mid-diastolic rumble at the apex that mimics mitral stenosis. The discriminator is the absence of an opening snap and a soft (not loud) S1 — and, of course, the presence of the obvious early diastolic murmur and the wide pulse pressure of aortic regurgitation. [1]
Dynamic manoeuvres — the manoeuvres that separate candidates
The examiner distinguishes the prepared candidate by whether they use the dynamic manoeuvres. These change preload, afterload, or heart rate and shift the murmur in a predictable, diagnosis-specific way. Perform them when you have identified a murmur and need to characterise it. [1]
| Manoeuvre | Effect | Murmurs that get louder | Murmurs that get softer |
|---|---|---|---|
| Inspiration | Increased venous return to the right heart | Right-sided murmurs (tricuspid and pulmonary) | Left-sided murmurs |
| Expiration | Increased venous return to the left heart | Left-sided murmurs (mitral, aortic) | Right-sided murmurs |
| Valsalva (strain phase) | Reduced preload, reduced afterload | Hypertrophic cardiomyopathy | Aortic stenosis; mitral regurgitation |
| Squat-to-stand (standing up) | Reduced preload, reduced afterload | Hypertrophic cardiomyopathy; mitral valve prolapse click moves earlier | Aortic stenosis |
| Stand-to-squat (squatting down) | Increased preload, increased afterload | Aortic stenosis; mitral regurgitation | Hypertrophic cardiomyopathy |
| Hand grip | Increased afterload | Mitral regurgitation; aortic regurgitation; VSD | Aortic stenosis; hypertrophic cardiomyopathy |
| Passive leg raise | Increased preload | Aortic stenosis | Hypertrophic cardiomyopathy |
Hypertrophic cardiomyopathy is the classic manoeuvre-dependent murmur: it is the only left-sided systolic murmur that gets louder on Valsalva and on standing (less ventricular filling brings the septum and mitral leaflet closer, increasing the obstruction) and softer on squatting and hand grip (more filling and more afterload reduce the obstruction). [1]
Mitral valve prolapse is the classic that moves: the click and the murmur move earlier and longer on standing (less preload brings prolapse earlier in systole) and later and shorter on squatting. [1]
DWE high-yield: If you remember one sentence for the dynamic manoeuvres, remember this — the murmur that gets louder on Valsalva and on standing, when every other left-sided murmur gets softer, is hypertrophic cardiomyopathy. The examiner who hears you say this knows you understand the physiology. [1]
Completing the examination — back, abdomen and legs
Step 9 — The back
Sit the patient forward. Auscultate the lung bases: fine basal crackles indicate pulmonary oedema; stony dullness to percussion with reduced breath sounds indicates a pleural effusion (a transudative effusion is common in heart failure). Check for sacral oedema in the bed-bound patient. [1]
Step 10 — The abdomen
Assess the liver — hepatomegaly from venous congestion (right heart failure, constrictive pericarditis, tricuspid regurgitation). A pulsatile liver — a liver that expands and fills in systole — is characteristic of tricuspid regurgitation (place the hand on the right upper quadrant and feel the expansile pulsation). Look for ascites (a shifting dullness or a fluid thrill) in advanced right heart failure or constrictive pericarditis. Palpate for splenomegaly, which in a patient with a murmur and fever points to infective endocarditis (and in heart failure may reflect congestion). [1]
Step 11 — The legs
Check for peripheral (pitting) oedema — grade the severity (ankle, mid-shin, knee, sacrum). Examine the peripheral pulses — femoral, popliteal, posterior tibial and dorsalis pedis — and look for signs of deep vein thrombosis (calf swelling, tenderness, warmth, superficial venous dilatation), the source of the pulmonary embolism that may present as apparent right heart failure. [1]
Complete the examination
State that you would complete the examination by measuring the blood pressure (in both arms, and the leg if coarctation is suspected), taking the temperature, checking the oxygen saturation, performing fundoscopy (Roth spots in endocarditis, hypertensive retinopathy), dipsticking the urine (proteinuria, haematuria in endocarditis), and reviewing the ECG and chest X-ray and, definitively, requesting an echocardiogram. [1]
The presentation template

The presentation is structured, spoken aloud, and hypothesis-driven. The template: [1]
Opening sentence: "I have examined this patient's cardiovascular system." [1]
End of bed: "At the end of the bed the patient is comfortable at rest, with no breathlessness, no cyanosis and no obvious distress. There is a median sternotomy scar." [1]
Hands: "The hands show no clubbing, no stigmata of infective endocarditis, no tendon xanthomata. The pulse is regular at 72 beats per minute, of normal character, with no radiofemoral delay." [1]
Face and eyes: "The face shows no malar flush and no dysmorphic features. The eyes show arcus senilis but no xanthelasma." [1]
Neck: "The jugular venous pressure is not elevated. The carotid pulse is of normal volume and character." [1]
Praecordium: "The apex beat is in the fifth intercostal space in the midclavicular line and is thrusting in character. There is a systolic thrill at the upper right sternal edge." [1]
Auscultation: "On auscultation the first heart sound is normal and the second heart sound is soft. There is an ejection systolic murmur, grade 4 of 6, at the upper right sternal edge, radiating to the carotids." [1]
Rest of examination: "The lung bases are clear. There is no hepatomegaly and no peripheral oedema. The peripheral pulses are all present and symmetrical." [1]
Synthesis: "In summary, this patient has a slow-rising pulse, a thrusting non-displaced apex, a systolic thrill, and an ejection systolic murmur radiating to the carotids with a soft second heart sound. These findings are consistent with severe aortic stenosis. I would confirm this with an echocardiogram and, given the likely severity, assess for symptoms with a careful history and an exercise test." [1]
The synthesis is what earns the pass: a dominant finding, a diagnosis, and a confirmatory investigation. The candidate who lists findings without synthesising them has performed the examination but not passed the case. [1]
Examiner discussion — by finding
After the presentation, the examiner probes the interpretation. The high-yield questions and the model answers: [1]
"What is the significance of a slow-rising pulse?" A slow-rising (pulsus parvus et tardus) pulse indicates aortic stenosis — the narrowed valve delays and reduces the systolic upstroke. It correlates with severity and, combined with a soft second heart sound and a late-peaking murmur, points to severe disease. [1]
"What causes a bounding pulse and a wide pulse pressure?" Aortic regurgitation — the diastolic run-off through the incompetent valve produces a large stroke volume (high systolic pressure) and a low diastolic pressure. The eponymous signs (Corrigan's visible carotid pulsation, de Musset's head bobbing, Quincke's nailbed pulsation, Duroziez's femoral bruit, Traube's pistol-shot) all reflect this exaggerated pulse. [1]
"What does a third heart sound mean?" A third heart sound is a low-pitched sound just after S2, from rapid ventricular filling into a stiff, overfilled ventricle. In the patient over 40 it indicates heart failure with elevated filling pressures; in the young, the pregnant and the athlete it may be physiological [1][2].
"How do you distinguish the JVP from the carotid pulse?" The JVP is non-palpable, varies with position and respiration, rises with abdominal pressure, and has a biphasic waveform; the carotid pulse is palpable, does not vary with position, and has a single upstroke. [1]
"What is the significance of cannon a waves?" Regular cannon a waves indicate complete heart block or AV dissociation (the atrium contracting against a closed tricuspid valve). Irregular cannon a waves occur in ventricular tachycardia with AV dissociation. [1]
"What does a fixed wide split of the second heart sound mean?" Atrial septal defect — the right ventricle is volume-loaded, delaying pulmonary closure equally in inspiration and expiration. [1]
"Why does the tricuspid regurgitation murmur get louder on inspiration?" Inspiration increases venous return to the right heart (Carvallo's sign), increasing the regurgitant volume and the murmur intensity. [1]
"What does clubbing with a central cyanotic lesion mean?" Cyanotic congenital heart disease — tetralogy of Fallot, transposition of the great arteries, or Eisenmenger syndrome. Clubbing with a new murmur and fever means infective endocarditis. [1]
Common examination traps and pitfalls
Trap 1 — Walking to the chest first. The candidate who listens before observing the hands, face and neck has missed the stigmata of endocarditis, the dysmorphic features, the JVP and the pulse character — the findings that frame the auscultation. The examination is head-to-toe; the stethoscope comes in the middle, not at the start. [1]
Trap 2 — Not timing the murmur. The candidate who says "there is a murmur" without saying systolic or diastolic has given no useful information. Timing is the first descriptor and the most reliable discriminator. If unsure, time the murmur against the carotid pulse — a murmur that coincides with the upstroke is systolic; one that follows it is diastolic. [1]
Trap 3 — Not using the dynamic manoeuvres. The candidate who hears a systolic murmur and does not perform Valsalva or squat-to-stand cannot distinguish aortic stenosis from hypertrophic cardiomyopathy, and has failed to demonstrate the physiology that the examiner is testing. [1]
Trap 4 — Calling an innocent flow murmur pathological. A soft, short, vibratory ejection systolic murmur at the left sternal edge in a young, well patient with no radiation, no thrill and normal heart sounds is an innocent flow murmur. Overcalling it as aortic stenosis is a common and embarrassing error. [1]
Trap 5 — Missing the displaced apex. The character of the apex beat is the bridge between the periphery and the auscultation. A thrusting non-displaced apex with a slow-rising pulse points to aortic stenosis; a thrusting displaced apex with a collapsing pulse points to aortic regurgitation; a tapping non-displaced apex with a loud S1 points to mitral stenosis. The candidate who does not palpate the apex character has lost a pivotal discriminator. [1]
Trap 6 — Not completing the examination. The candidate who stops at the chest has missed the pulmonary oedema, the hepatomegaly, the peripheral oedema and the peripheral pulses. Always state the completion — blood pressure, temperature, oxygen saturation, fundoscopy, urinalysis, ECG, chest X-ray and echocardiogram. [1]
Trap 7 — Presenting findings without a synthesis. A list of unconnected observations is the mark of a candidate who has not integrated the examination. Always end with a dominant finding, a diagnosis, and a confirmatory investigation. The synthesis is what earns the pass [3][4].
Trap 8 — Forgetting the systemic and syndromic associations. The tall, thin patient with a high arched palate and an aortic regurgitation murmur has Marfan syndrome until proven otherwise — and the diagnosis changes the management (serial aortic imaging, family screening) [6]. The cardiovascular examination is never just about the heart; it is about the patient.
Key references
McDonagh et al. (ESC Heart Failure), Eur Heart J 2021 [1]; Bozkurt et al. (Universal Definition of HF), Eur J Heart Fail 2021 [2]; Otto et al. (ACC/AHA Valvular Heart Disease), Circulation 2021 [3]; Vahanian et al. (ESC/EACTS Valvular Heart Disease), Eur Heart J 2022 [4]; Etchells et al. (Rational Clinical Examination — systolic murmur), JAMA 1997 [5]; Loeys et al. (Revised Ghent nosology for Marfan syndrome), J Med Genet 2010 [6]; NICE NG106; ESC Guidelines; ACC/AHA Guidelines; Heart Foundation of Australia.
References
- [1]McDonagh TA, Metra M, Adamo M, et al.; ESC Scientific Document Group 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure Eur Heart J, 2021.PMID 34447992
- [2]Bozkurt B, Coats AJS, Tsutsui H, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association Eur J Heart Fail, 2021.PMID 33605000
- [3]Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation, 2021.PMID 33332150
- [4]Vahanian A, Beyersdorf F, Praz F, et al.; ESC/EACTS Scientific Document Group 2021 ESC/EACTS Guidelines for the management of valvular heart disease Eur Heart J, 2022.PMID 34453165
- [5]Etchells E, Bell C, Robb K Does this patient have an abnormal systolic murmur? JAMA, 1997.PMID 9032164
- [6]Loeys BL, Dietz HC, Braverman AC, et al. The revised Ghent nosology for the Marfan syndrome J Med Genet, 2010.PMID 20591885