Phys · general-medicine
The Deteriorating Ward Patient — Recognition, Systematic Assessment and Escalation
Also known as deteriorating patient · acutely ill patient · NEWS2 · National Early Warning Score · track and trigger · early warning score · ABCDE approach · MET call · medical emergency team · rapid response team · rapid response system · ICU outreach · SBAR · failure to rescue · ceiling of care · ward cardiac arrest · clinical deterioration
Consultant-physician-depth guide to recognising and managing the acutely deteriorating ward patient. Covers the hours of warning before arrest, NEWS2 and track-and-trigger systems, the ABCDE structured assessment, the common causes of ward deterioration (sepsis, hypovolaemia, cardiac, respiratory, neurological, drug-related, metabolic), MET call criteria and escalation thresholds, SBAR structured handover, rapid response system evidence, and end-of-life decision-making including ceilings of care. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The Deteriorating Ward Patient — Recognition, Systematic Assessment and Escalation

The answer first
The acutely deteriorating ward patient is a failure of recognition before it is a failure of resuscitation. The patient who arrests on the ward has, in the great majority of cases, shown physiological warning signs for hours — and those signs have either not been measured, not been recorded, not been recognised as dangerous, or not been acted upon. Schein and colleagues established this in 1990: 84 per cent of in-hospital cardiac arrest patients had documented clinical deterioration in the eight hours before arrest, and the dominant antecedents were respiratory and mental-state changes, not cardiac [1]. The modern registrar's job at the bedside of a deteriorating patient is therefore twofold — recognise that the patient is deteriorating, then respond with a structured, escalating, communicated plan.
The reproducible sequence for any deteriorating ward patient is: [1]
- Recognise deterioration — measure the full vital sign set, calculate NEWS2, and weigh the trend over time.
- Respond with the ABCDE assessment — a systematic, do-it-now examination that treats life-threats as they are found.
- Resuscitate in parallel — oxygen, intravenous access, fluid, glucose, and the cause-specific therapy (antibiotics for sepsis, blood for haemorrhage, reversal for hyperkalaemia).
- Escalate — call for help at the threshold the score and the clinical picture mandate; never delay a MET call for a fuller workup.
- Communicate — use SBAR to hand over a structured picture to the person you escalated to.
- Make a plan for the ceiling of care — decide, with the patient and family where possible, what escalation is appropriate before you need it. [1]
The single most dangerous error is treating the abnormal observation but not the patient — chasing a number on the chart while the patient continues to fall through the gaps between the teams looking after them. The second is failing to escalate because the score is borderline or because calling for help feels like an admission of inadequacy. Calling for help early is a sign of competence, not the opposite. [1]
Viva trap: "What kills the deteriorating ward patient?" The honest answer is not the cardiac arrest — it is the hours of unrecognised respiratory deterioration that precede it. The respiratory rate is the most informative and the most neglected vital sign. A rising respiratory rate is the body's first measurable response to hypoxia, acidaemia, pain, sepsis, and metabolic upset. If you measure it, document it, and act on it, you have intercepted most preventable ward arrests at their origin. [1]
Why patients deteriorate on the ward — the warning window
The central insight of four decades of acute-medicine research is that in-hospital cardiac arrest and unanticipated ICU admission are rarely sudden events. They are the end-state of a period of physiological instability that is measurable, has a characteristic signature, and is — most of the time — present for hours before the crisis [1]. This is the empirical foundation for every track-and-trigger system, every early warning score, and every rapid response team in modern practice.
Schein's 1990 prospective study of 64 ward cardiac arrests found that 84 per cent of patients had documented deterioration in the eight hours before arrest, with a mean respiratory rate of 29 breaths per minute. The antecedents were predominantly respiratory (38 per cent) or a combination of respiratory and metabolic (27 per cent); pure cardiac events were a minority (9 per cent) [1]. Subsequent multi-centre data have confirmed that approximately 80 per cent of in-hospital arrest patients exhibit physiological instability in the hours before the event.
The physiological signature of deterioration follows a predictable cascade. The compensatory phase comes first: the respiratory rate rises to defend oxygenation and acid-base balance, the heart rate rises to maintain cardiac output, and the peripheries constrict to preserve central perfusion. Blood pressure and conscious level are held near-normal by these mechanisms — which is precisely why they are late markers of deterioration. The decompensatory phase follows when compensatory mechanisms fail: blood pressure falls, oxygen saturation drops, urine output falls, and mental state deteriorates. The patient who has reached this phase is already critically ill, and the window for prevention is closing fast. [1]
The most reliable leading indicators of deterioration are therefore those that change first: [1]
- Respiratory rate — the earliest and most neglected; rises before any other vital sign in the majority of deteriorations.
- Oxygen saturation — falls when respiratory reserve is exhausted; a lagging marker relative to respiratory rate.
- Heart rate and rhythm — rises with compensatory demand; new arrhythmia is itself a cause of deterioration.
- Blood pressure — a late marker; normal blood pressure does not exclude significant shock, particularly in the chronically hypertensive patient.
- Conscious level (AVPU/GCS) — a late marker; new confusion or drowsiness is a red flag.
- Urine output — a marker of organ perfusion; falling output is a sign that the kidneys are no longer being perfused adequately.
- Temperature — high or low; a marker of infection but also of environmental exposure, drug effect, or hypothalamic dysfunction. [1]
DWE high-yield: The single most examinable fact about ward deterioration is that the respiratory rate is the most frequently abnormal and the most frequently omitted vital sign. A ward observation set without a recorded respiratory rate is a missed opportunity to recognise deterioration. The corollary is that the trend across consecutive observation sets is more informative than any single value — a respiratory rate that has risen from 18 to 24 to 30 over six hours is a deteriorating patient even if each value is not individually catastrophic. [1]
Track and trigger — the Early Warning Score systems
A track and trigger system assigns a weight to each physiological parameter, sums the weights into an aggregate score, and links the score to a predefined clinical response. The aim is to convert the subjective judgement "this patient looks unwell" into an objective, reproducible trigger that mandates escalation — removing the hesitation and the inter-observer variability that delay the response. [1]
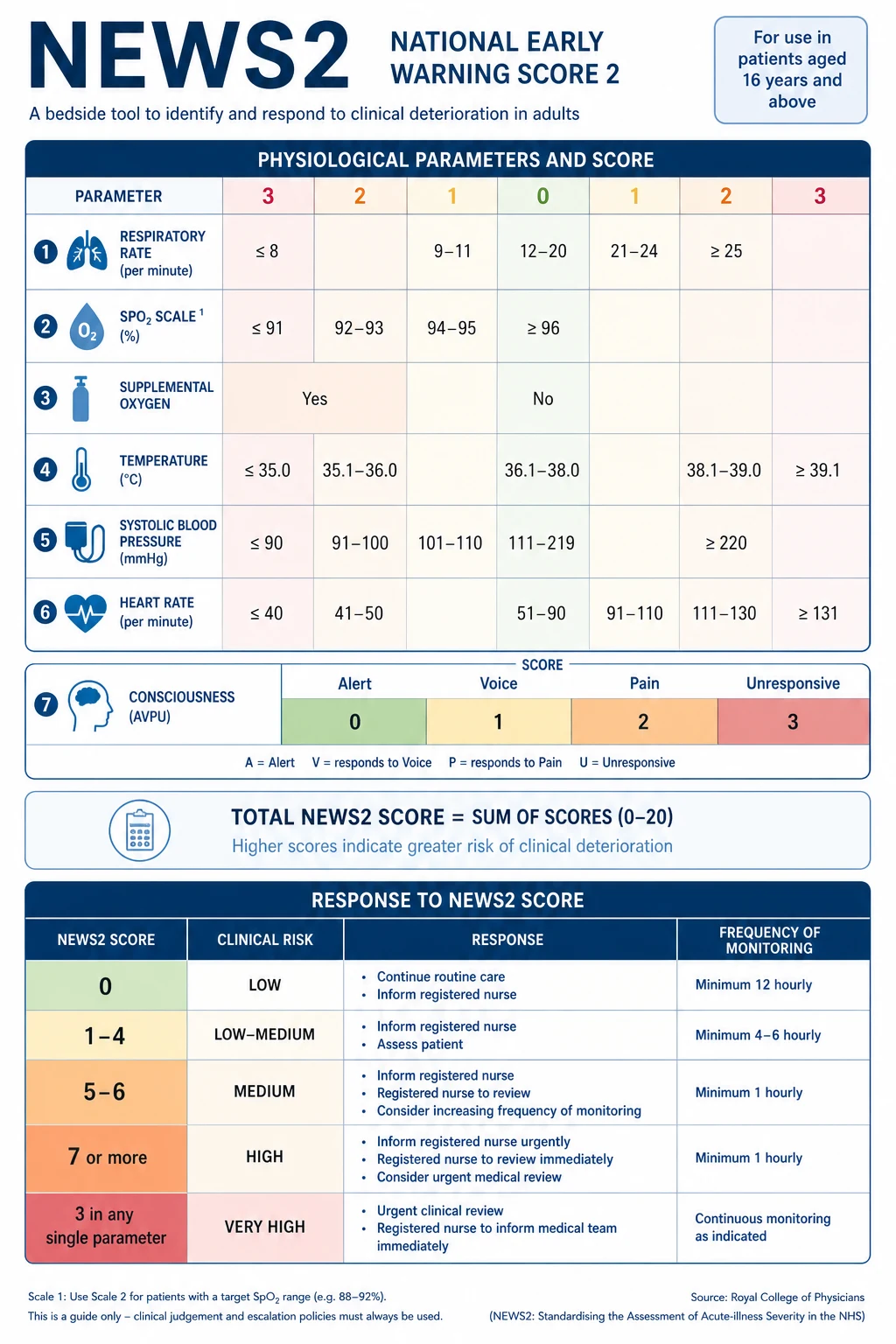
The dominant system in the English-speaking world is NEWS2, the second iteration of the National Early Warning Score, developed by the Royal College of Physicians (RCP) and published in 2017. NEWS2 standardises the assessment of acute illness severity across the NHS and is widely adopted in ANZ and elsewhere as the bedside track-and-trigger tool. [1]
The seven NEWS2 parameters
NEWS2 is built from six physiological measurements plus a conscious-level score: [1]
- Respiratory rate (breaths per minute)
- Oxygen saturation (SpO2) — with a modified scale for patients on supplemental oxygen
- Supplemental oxygen — air or oxygen (a binary "yes/no" that itself scores points)
- Temperature (degrees Celsius)
- Systolic blood pressure (mmHg)
- Heart rate (beats per minute)
- Conscious level — AVPU (Alert, Voice, Pain, Unresponsive), or the new ACVPU that adds New Confusion [1]
Each parameter is scored 0 to 3, with 0 representing the normal range and progressively higher scores for greater deviation in either direction. The aggregate (the sum) is the NEWS2 value, ranging from 0 to 20. [1]
The high-yield scoring bands to remember: [1]
| Parameter | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|
| Respiratory rate (/min) | 12 to 20 | 9 to 11, or 21 to 24 | — | 8 or less, or 25 or more |
| SpO2 (scale 1) (%) | 96 or more | 94 to 95 | 92 to 93 | 91 or less |
| Air or oxygen | Air | Oxygen | — | — |
| Systolic BP (mmHg) | 111 to 219 | 101 to 110 | — | 100 or less, or 220 or more |
| Heart rate (/min) | 51 to 90 | 41 to 50, or 91 to 110 | — | 40 or less, or 111 or more |
| Conscious level | Alert | — | — | Voice, Pain, Unresponsive, or New confusion |
| Temperature (deg C) | 36.1 to 38.0 | 35.1 to 36.0, or 38.1 to 39.0 | — | 35.0 or less, or 39.1 or more |
A second SpO2 scale (scale 2) exists for patients with hypercapnic respiratory failure who have a prescribed lower target range (typically 88 to 92 per cent) — the defining example is the COPD patient at risk of CO2 retention. The scale-2 modification prevents these patients from being over-scored and over-oxygenated. [1]
The three response thresholds
NEWS2 links the aggregate score to a graded clinical response, and this is the part the examiner will probe: [1]
- NEWS2 of 0 — a low-score, low-risk patient. Routine monitoring, at least 12-hourly, on a standard ward.
- NEWS2 of 1 to 4 — low-score. Registered nurse review. The minimum monitoring frequency increases to at least 4- to 6-hourly. A single score of 3 in any one parameter ("red score") prompts urgent ward-based review regardless of the aggregate, because a single markedly abnormal value may be missed by a low aggregate.
- NEWS2 of 5 to 6 — medium-score, the key threshold. Urgent review by a clinician (or team) with competencies in acute illness — usually a ward registrar within 30 minutes to an hour. Monitoring at least hourly. This is the threshold at which deterioration is real and the response must be prompt.
- NEWS2 of 7 or more — high-score, clinical emergency. Emergency assessment by a critical care team (ICU outreach or MET) within minutes. The patient is at high risk of deterioration, arrest, or death. Monitoring is continuous. [1]
Smith and colleagues validated NEWS against 33 other early warning scores and showed it discriminated patients at risk of cardiac arrest, unanticipated ICU admission, and death at least as well as any existing system [2]. The score is a tool, not a substitute for clinical judgement — but it is a tool that, used consistently, closes the gap between deterioration and response.
DWE exam trap: The single most testable NEWS2 fact is that a score of 7 or more is a clinical emergency requiring an emergency critical care assessment within minutes, and that a single score of 3 in any parameter (a "red score") mandates urgent review regardless of the aggregate. The candidate who says "I would wait and recheck in an hour" for a NEWS2 of 7 has failed the question. The corollary trap: NEWS2 does not replace clinical judgement — a patient with a NEWS2 of 2 who "looks unwell" to an experienced clinician still needs urgent assessment. The score is the floor of the response, not the ceiling. [1]
Other track-and-trigger systems and the regional delta
NEWS2 is not the only system. The Modified Early Warning Score (MEWS) predates NEWS and is still used in some institutions. The Paediatric Early Warning Score (PEWS) adapts the principle to age-specific physiology. The National Early Warning Score for children is the paediatric analogue. In ANZ, the Between the Flags system (NSW) uses a colour-banded ("red zone" and "yellow zone") single-parameter and aggregate approach with predefined escalation — functionally equivalent to NEWS2 but institutionally branded. In the United States, the Modified Early Warning Score and institution-specific "criticare" thresholds are common; the National Early Warning Score is less uniformly adopted. [1]
The regional delta the registrar must carry: the principle is universal (track physiological parameters, trigger a graded response), but the specific thresholds and the brand name differ by institution. Always confirm the local system on arrival at a new hospital, and use it as it is configured — the worst of both worlds is to carry a NEWS2 habit into a Between the Flags hospital and escalate at the wrong thresholds. [1]
The ABCDE structured assessment
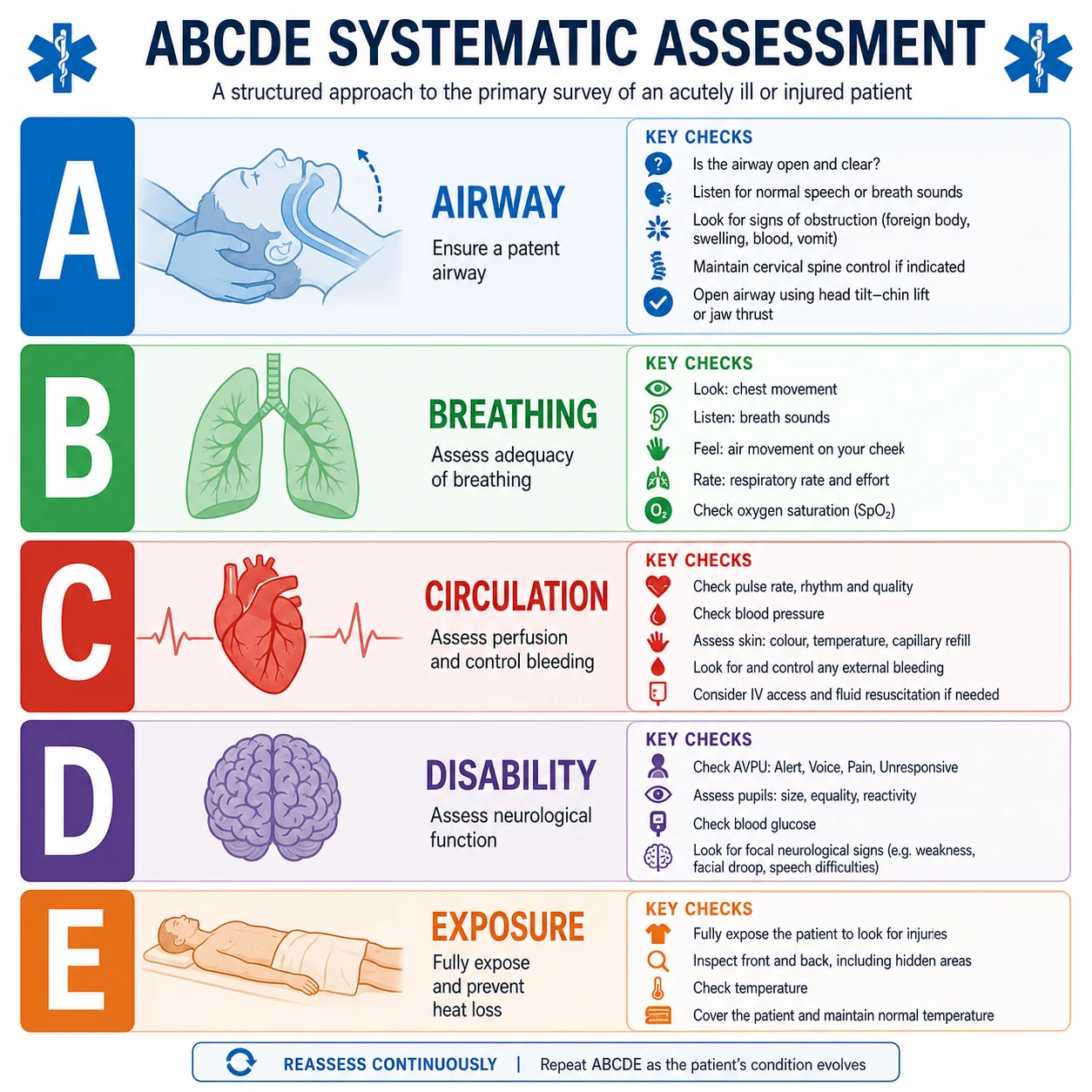
The ABCDE approach is the universal structured assessment for any acutely ill patient. Its power is that it imposes an order of priority — treat the life-threat in front of you before moving to the next system — and that it is reproducible under pressure. Every member of the team using the same sequence can hand over without ambiguity. [1]
The principle: assess and treat in order, and do not move past a compromised system until it is either resolved or supported. A patient with an obstructed airway is not helped by an intravenous fluid bolus; a patient in tension pneumothorax is not helped by a vasopressor. The order matters. [1]
A — Airway
The first question is always: is the airway patent? An obstructed airway kills in minutes and is the most immediately reversible cause of deterioration. [1]
- Assess: Look for chest movement, listen for breath sounds at the mouth, feel for expired air (the look-listen-feel technique). Signs of obstruction include paradoxical chest and abdominal movement (see-saw breathing), snoring (partial upper-airway obstruction by the tongue), gurgling (fluid or secretions in the airway), stridor (upper-airway obstruction, a surgical emergency), and wheeze (lower-airway narrowing).
- Manage: Basic manoeuvres first — head tilt and chin lift, or jaw thrust if cervical spine injury is suspected. Airway adjuncts — an oropharyngeal (Guedel) airway if the patient is unconscious with no gag reflex, or a nasopharyngeal airway if the gag is intact but the airway is at risk. Suction secretions and vomit. Sit the patient up if conscious and able. Position lateral if the conscious level is reduced and the airway is unprotected.
- Escalate: If basic manoeuvres and adjuncts fail, call for senior airway help immediately. The patient who cannot be oxygenated and ventilated with a bag-valve-mask needs an anaesthetist or intensivist at the bedside now. Do not wait. [1]
B — Breathing
Once the airway is patent or supported, assess the adequacy of breathing. [1]
- Assess: Respiratory rate, oxygen saturation, chest expansion (symmetry and depth), use of accessory muscles, tracheal position, percussion note, auscultation (air entry, added sounds — wheeze, crackles, rub), and the pattern of breathing. A high respiratory rate is the leading indicator of deterioration; a low rate suggests opioid, sedative, or neurological depression. Check a bedside SpO2, and send an arterial blood gas if there is any concern about oxygenation, ventilation, or acid-base status.
- Manage: Give oxygen to any acutely hypoxaemic patient. Start with high-flow oxygen via a reservoir mask at 15 L/min for the patient who is critically ill or whose saturation is below 85 per cent; titrate down to a target saturation (92 to 96 per cent for most patients; 88 to 92 per cent for those at risk of hypercapnic respiratory failure) as soon as the saturation recovers. Treat the cause — bronchodilators for bronchospasm, pleural aspiration or chest drain for tension pneumothorax, antibiotics and physiotherapy for pneumonia.
- Investigate: A chest X-ray, an arterial blood gas, and a focused bedside assessment. Remember that a normal SpO2 does not exclude a rising CO2 — the patient breathing inadequately (small tidal volumes, opioid-induced hypoventilation, neuromuscular weakness) can have a normal saturation and a dangerously high PaCO2. The blood gas is the test that catches this. [1]
DCE high-yield: "How much oxygen would you give?" The safe answer for the critically ill, hypoxaemic patient is high-flow oxygen via a reservoir mask at 15 L/min, then titrate down once the saturation is in a safe range. The common error is to under-oxygenate a critically ill patient for fear of CO2 retention — a risk that is real in a small subset of COPD patients but is not a reason to withhold oxygen from a hypoxaemic, acutely deteriorating patient. For the known hypercapnic COPD patient, use a Venturi mask at 28 to 31 per cent (target SpO2 88 to 92 per cent) and check a blood gas within 30 to 60 minutes. [1]
C — Circulation
- Assess: Heart rate and rhythm (a 12-lead ECG plus continuous monitoring), blood pressure, capillary refill time (press on the nail bed or sternum for 5 seconds; refill over 2 seconds is prolonged), peripheral and central pulses (bounding, thready, or absent), jugular venous pressure, skin temperature and mottling, and urine output (the integrated marker of renal perfusion). A urine output of less than 0.5 mL/kg/hour is oliguria and suggests inadequate perfusion.
- Manage: Two large-bore intravenous cannulae. Give an intravenous fluid challenge — 500 mL of balanced crystalloid (Hartmann's or Plasma-Lyte) over 15 minutes in the adult without severe cardiac or renal failure, repeated to clinical effect while watching for fluid overload. Identify and treat the cause — blood for haemorrhage, antibiotics and fluid for sepsis, antiarrhythmic or rate control for a tachyarrhythmia, inotrope for cardiogenic shock. Control external bleeding with direct pressure.
- Investigate: Blood tests — full blood count, urea and electrolytes, liver function, coagulation, lactate (the marker of tissue hypoperfusion), troponin if cardiac is suspected, and blood cultures before antibiotics if infection is the cause. A venous or arterial blood gas gives rapid pH, lactate, and electrolyte information at the bedside. [1]
The discriminator in the hypotensive patient is the cause of the shock: hypovolaemic (bleeding, dehydration — respond to fluid), distributive (sepsis, anaphylaxis — need fluid and vasopressors), cardiogenic (infarction, failure — worsened by excessive fluid, need inotropes and cause-specific therapy), or obstructive (tension pneumothorax, massive PE, tamponade — need decompression or specific therapy, not fluid). The ABCDE assessment, the fluid challenge, and the focused examination together discriminate these, and the wrong treatment for the wrong cause worsens the patient. [1]
D — Disability
- Assess: Conscious level using AVPU (Alert, Voice, Pain, Unresponsive) or the Glasgow Coma Scale (GCS — eye, verbal, motor, out of 15). Examine pupil size and reactivity (small, large, asymmetric — a unilateral fixed dilated pupil suggests herniation until proven otherwise). Check a bedside blood glucose in every patient with an altered conscious level — hypoglycaemia is a rapidly reversible cause of coma and is missed catastrophically if not measured. Assess limb power, tone, and reflexes if focal neurology is suspected.
- Manage: Treat hypoglycaemia immediately — 50 to 100 mL of 50 per cent dextrose intravenously, or 200 mL of 10 per cent dextrose if central access is unavailable. Protect the airway of the unconscious patient (position lateral, consider intubation if GCS is 8 or less). Treat seizures with a benzodiazepine (lorazepam 4 mg intravenously, repeated). Give thiamine before glucose to the malnourished or chronic alcoholic patient to avoid precipitating Wernicke encephalopathy. Give naloxone titrated to respiratory effort if opioid toxicity is the cause.
- Investigate: A CT brain if there is any suspicion of a structural lesion (new focal signs, head trauma, anticoagulation, or a deteriorating conscious level without metabolic explanation). [1]
E — Exposure
- Assess: Fully expose the patient and examine systematically — temperature, skin (rash, mottling, bruising, surgical wounds, lines and drains, pressure areas), the abdomen (distension, tenderness, rigidity), and the peripheries (oedema, perfusion, DVT signs). Check for hidden sources of sepsis (a retained urinary catheter, an infected line, a diabetic foot ulcer).
- Manage: Keep the patient warm — hypothermia worsens coagulopathy and acidosis. Take the opportunity to take a focused history and to review the drug chart, the observation trend, and the recent results — the cause of the deterioration is often found in the chart rather than the bedside. [1]
Common causes of deterioration on the ward
The differential for the deteriorating ward patient is broad but clusters into a manageable set of categories. Sepsis is the single commonest cause of ward deterioration, and in any deteriorating patient without an immediately obvious cause, infection must be assumed and actively sought [4]. The other major categories are hypovolaemia, cardiac, respiratory, neurological, drug-related, and metabolic.
Sepsis — assume it until excluded
Sepsis is the leading cause of deterioration because it is common, it presents non-specifically, and it progresses rapidly. The clinical signs — fever or hypothermia, tachycardia, tachypnoea, altered mental state, falling urine output, rising lactate — overlap with every other cause of deterioration, which is why the first question in any deteriorating patient is "where is the infection?" and the first intervention bundle is the Sepsis Six (three tests, three treatments within one hour): [1]
- Give oxygen to target saturation.
- Take blood cultures (and cultures from any suspected source — urine, sputum, line) before antibiotics.
- Give intravenous antibiotics — broad-spectrum, within one hour, at the right dose for the suspected source and the local resistance pattern.
- Give intravenous fluid resuscitation — 30 mL/kg of balanced crystalloid in the first three hours for sepsis with hypoperfusion or septic shock [4].
- Measure lactate — a marker of tissue hypoperfusion and a key prognostic indicator.
- Measure urine output — catheterise and monitor hourly.
The Surviving Sepsis Campaign 2021 guidelines frame the hour-1 bundle: the recognition of sepsis (infection plus organ dysfunction) triggers the simultaneous measurement of lactate, blood cultures, broad-spectrum antibiotics, fluid resuscitation, and vasopressors if the patient is in septic shock [4]. Delayed antibiotics increase mortality hour by hour; the first dose is the most important intervention in septic deterioration.
Hypovolaemia — bleeding and dehydration
The second commonest cause of ward deterioration is loss of circulating volume: haemorrhage (overt — GI bleed, surgical site, retroperitoneal; or concealed — occult postoperative, aortic aneurysm leak, anticoagulant-related) and dehydration (inadequate intake in the acutely or chronically unwell, persistent vomiting or diarrhoea, polyuria from uncontrolled diabetes or diuretics). The signs are tachycardia, postural hypotension, dry mucous membranes, reduced skin turgor, oliguria, and a rising urea. The history (recent surgery, anticoagulation, melena, vomiting) and the examination (abdominal tenderness, melaena on rectal examination, surgical wound) usually point to the source. [1]
Management is fluid and blood. For haemorrhagic shock, give balanced crystalloid as a bridge to transfusion; activate the massive transfusion protocol for major bleeding; control the source (endoscopic for GI bleed, surgical for surgical bleed, reversal for anticoagulant-related). For dehydration, give balanced crystalloid — Hartmann's or Plasma-Lyte preferred over normal saline for large volumes, because normal saline causes hyperchloraemic metabolic acidosis. [1]
Cardiac — arrhythmia, infarction, failure
A new cardiac problem is a frequent precipitant of ward deterioration, particularly in the older patient with established cardiac disease. Atrial fibrillation with rapid ventricular response is the classic new arrhythmia on the ward — precipitated by sepsis, electrolyte disturbance, hypoxia, pain, or thyrotoxicosis. Acute coronary syndrome may present atypically in the postoperative or diabetic patient (silent, with breathlessness or confusion rather than chest pain). Acute decompensated heart failure presents with breathlessness, orthopnoea, bilateral crackles, raised JVP, and oedema. A 12-lead ECG is mandatory in any deteriorating patient and is the highest-yield single investigation for the cardiac causes. [1]
The management is cause-specific: rate control or rhythm control for atrial fibrillation (the choice depends on haemodynamic stability — if unstable, the patient is for synchronised DC cardioversion); antiplatelet, anticoagulant, and reperfusion for acute coronary syndrome; diuresis, vasodilator, and inotrope for acute heart failure. The common error is treating the arrhythmia without identifying and treating the precipitant — the AF that comes with sepsis will not stay controlled until the sepsis is treated. [1]
Respiratory — PE, pneumonia, atelectasis, aspiration
Respiratory deterioration on the ward is commonly pneumonia (hospital-acquired, aspiration in the dysphagic or postoperative patient), atelectasis (postoperative splinting or mucus plugging), pulmonary embolism (the feared and under-recognised cause of sudden deterioration in the immobilised, postoperative, or malignant patient), and aspiration in the patient with reduced conscious level or impaired swallow. The clinical signs are tachypnoea, hypoxaemia, increased work of breathing, and focal findings on auscultation. The chest X-ray, the blood gas, and (for PE) the D-dimer and CTPA are the key investigations. [1]
PE is the diagnosis most likely to be missed. The deteriorating patient with unexplained tachycardia, tachypnoea, hypoxia, and a normal or near-normal chest X-ray, particularly with a risk factor (immobilisation, recent surgery, active cancer, pregnancy), has a PE until proven otherwise. [1]
Neurological — stroke, seizure, encephalopathy
Neurological deterioration presents as a change in conscious level, a new focal deficit, or a seizure. Stroke (ischaemic or haemorrhagic) is the time-critical diagnosis — the FAST test (Face, Arm, Speech, Time) screens for it, and the CT brain is the discriminator. Seizure may be the presentation (a first seizure in a metabolic or structural context) or the consequence (post-ictal deterioration). Metabolic encephalopathy — from sepsis, electrolyte disturbance, hypoxia, drug effect, or hepatic or renal failure — is the commonest cause of a deteriorating conscious level on the ward, and is a diagnosis of exclusion after structural and infectious causes are ruled out. A bedside glucose, a CT brain, and (if indicated) a lumbar puncture are the core investigations. [1]
Drug-related — adverse effect, overdose, withdrawal
Drugs are a frequent and frequently missed cause of ward deterioration. Opioid-induced respiratory depression (postoperative or palliative), sedative accumulation (benzodiazepines in the elderly or renally impaired), adverse drug reactions (antibiotic-related colitis, ACE-inhibitor angioedema, amiodarone pulmonary toxicity), drug withdrawal (alcohol, benzodiazepine, opioid), and overdose (deliberate or accidental — see the dedicated poisoning topic) are all common. The drug chart is the single highest-yield document in the deteriorating patient without an obvious cause — review every drug, every dose, and every recent change. [1]
The specific antidotes are part of the D-step of ABCDE: naloxone for opioid, flumazenil (selectively) for benzodiazepine, glucose for hypoglycaemia, thiamine for Wernicke risk. [1]
Metabolic — DKA, hypoglycaemia, electrolyte disturbance, acid-base disorder
The metabolic causes of deterioration are the most easily missed and the most easily treated. Diabetic ketoacidosis (DKA) presents with vomiting, abdominal pain, tachypnoea (Kussmaul breathing), and a falling conscious level; the bedside glucose is high, the blood gas shows a high anion-gap metabolic acidosis, and the urine or blood ketones are positive. Hypoglycaemia presents with any neurological picture from confusion to seizure to coma; the bedside glucose is low, and the treatment is immediate dextrose. Hyperkalaemia causes weakness, palpitation, and (ultimately) ventricular fibrillation; the ECG shows peaked T waves, loss of P waves, and widening of the QRS, and the treatment is calcium chloride for membrane stabilisation, insulin-dextrose and salbutamol to shift potassium into cells, and removal (renal replacement therapy) if refractory. Hyponatraemia causes confusion, seizure, and coma; the rate of correction is critical to avoid osmotic demyelination. [1]
A venous blood gas, a urea and electrolytes, and a glucose together catch the metabolic causes of deterioration in minutes. The registrar who does not check these in a deteriorating patient has missed a treatable cause. [1]
Escalation — when to call for help
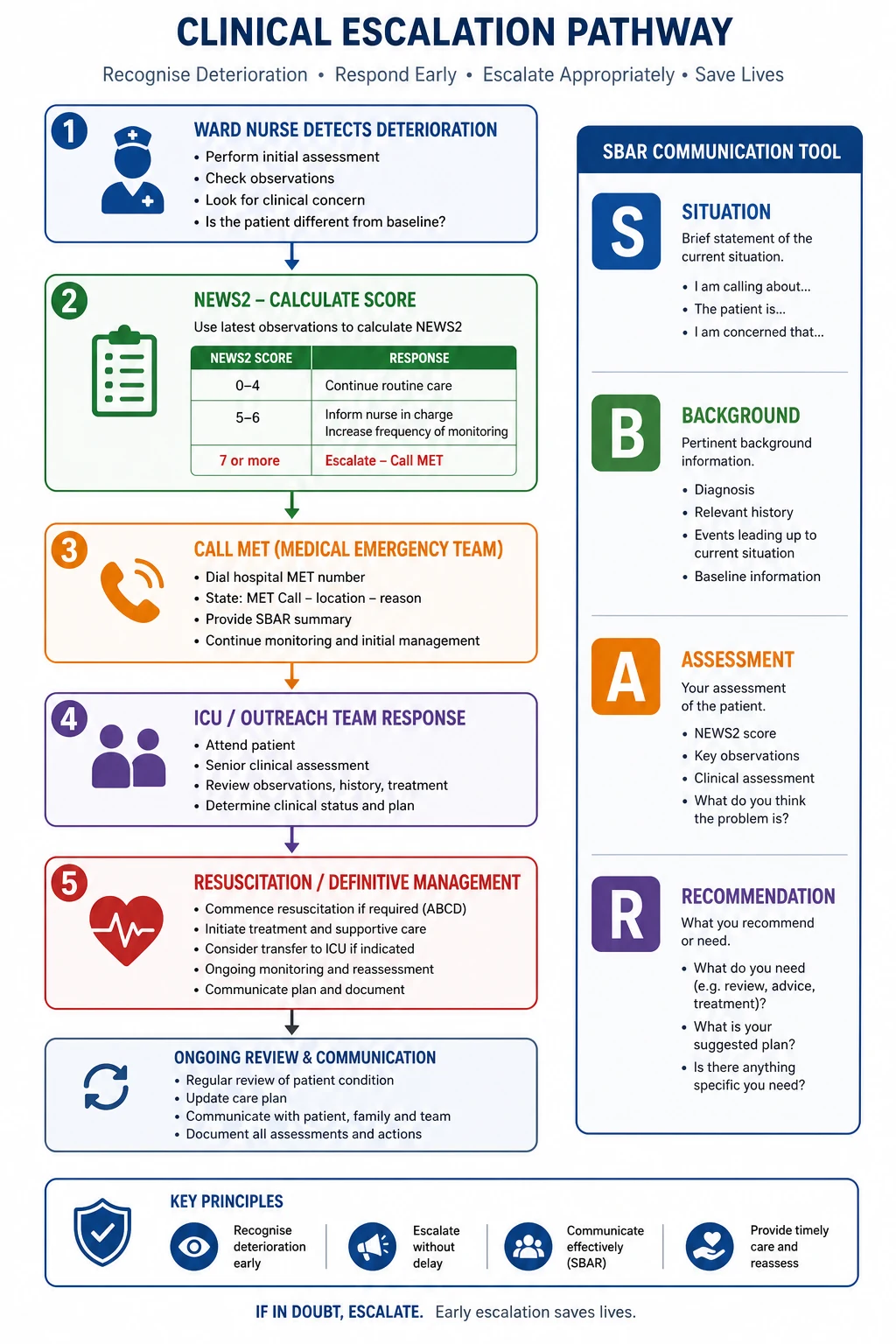
The escalation pathway is the second half of the rapid response system: the recognition tool (NEWS2) identifies the deteriorating patient, and the response arm delivers the right clinician to the bedside at the right time. The principle is that the threshold for calling for help is set lower than the threshold for arrest — the system is designed to intervene before the patient crashes. [1]
MET call criteria
Most institutions operate a Medical Emergency Team (MET) call system with a defined set of calling criteria that any staff member — nurse, junior doctor, allied health — can activate. The criteria combine single-parameter physiological derangements with subjective concern. A representative set (the specifics vary by institution): [1]
- Airway threat — any concern that the airway is or may become compromised.
- Respiratory rate — less than 8 or more than 30 per minute.
- Oxygen saturation — below 90 per cent despite supplemental oxygen.
- Heart rate — less than 40 or more than 130 per minute.
- Systolic blood pressure — less than 90 mmHg despite a fluid challenge.
- Conscious level — a sudden fall in GCS of 2 points or more, new agitation or confusion, or a new seizure.
- Any patient you are worried about — the "worried" criterion, deliberately included because clinical concern precedes measurable derangement. [1]
The "worried" criterion is the most important and the most underused. Staff who are worried about a patient but whose observations do not yet cross a threshold often hesitate to call — and the system is designed to support, not penalise, that call. The MERIT study, while its primary composite outcome was negative, demonstrated that the MET system was activated far more frequently in intervention hospitals (8.7 versus 3.1 calls per 1000 admissions) — the culture of calling was the intervention's measurable effect [3].
When to call ICU and ICU outreach
The MET call brings a critical-care-trained team to the ward; the question that follows is whether the patient needs ICU admission. The decision is based on the failure to respond to ward-level therapy or the need for organ support that the ward cannot provide: [1]
- Airway support — a patient who needs intubation or sustained airway adjuncts.
- Respiratory support — a patient who needs continuous positive airway pressure (CPAP), bi-level non-invasive ventilation, or mechanical ventilation.
- Circulatory support — a patient who needs ongoing vasopressor or inotrope infusion, or who is in refractory shock.
- Neurological support — a patient who is comatose with an unprotected airway, or who needs intracranial pressure monitoring.
- Renal support — a patient who needs renal replacement therapy for hyperkalaemia, acidosis, fluid overload, or uraemia. [1]
ICU outreach (also called critical care outreach or the medical emergency team, depending on the institution) is the service that spans the gap between the ward and the ICU. Outreach teams — typically senior nursing and medical staff with critical care competencies — review deteriorating patients, support ward staff in the early phases of resuscitation, and triage ICU admissions. The early call to outreach is the call that prevents the late call to the cardiac arrest team. [1]
When to initiate resuscitation (and when not to)
For the patient who has arrested, the decision to initiate cardiopulmonary resuscitation (CPR) follows the standard advanced life support algorithm: confirm arrest, call for help, commence chest compressions and ventilation, defibrillate if the rhythm is shockable (VF/pVT), and identify and treat reversible causes (the 4 Hs and 4 Ts). The detail that belongs to this topic — and that the examiner will probe — is the decision NOT to resuscitate. This is addressed below under end-of-life decision-making. [1]
Communication — the SBAR handover
A deterioration is not well managed if it is not well communicated. The standardised handover tool is SBAR — Situation, Background, Assessment, Recommendation — a structure that delivers a complete clinical picture in under a minute and that is now embedded in acute-care communication across the English-speaking world. [1]
The four components, with the registrar's task at each: [1]
- Situation — who you are, who the patient is, where they are, and what has happened in one sentence. "This is Dr Smith, the ward registrar. I am calling about Mr Jones in bed 7, a 72-year-old man who has acutely deteriorated in the last hour with a NEWS2 of 9."
- Background — the relevant history: the admission diagnosis, the comorbidities, the recent course. "He was admitted three days ago with community-acquired pneumonia, treated with IV benzylpenicillin and clarithromycin. He has ischaemic heart disease and chronic kidney disease stage 3."
- Assessment — the current findings: the vital signs, the examination, the key investigations, and your working diagnosis. "His observations are: respiratory rate 30, SpO2 88 per cent on 15 L via reservoir mask, heart rate 128, blood pressure 84 over 50, GCS 13, temperature 38.9. His lactate is 4.2. He is oliguric. My assessment is septic shock with worsening pneumonia."
- Recommendation — what you want the person you are calling to do, and the timeframe. "I would like you to come and review him on the ward now. I have given the Sepsis Six and a 500 mL fluid bolus. I think he needs ICU assessment for inotropic support and possibly non-invasive ventilation." [1]
The common SBAR failure is to under-call the Recommendation — to deliver a thorough Assessment and then trail off with "I just thought I would let you know." The Recommendation must be specific, timed, and must name the action you want. "I would like you to come now" is the recommendation that the deteriorating patient needs. [1]
Viva trap: The examiner will ask, "What is the single most common reason a MET call is delayed?" The evidence-based answer is the caller's uncertainty about whether the call is justified — the so-called "failures to escalate." The fix is twofold: the objective trigger (the NEWS2 or single-parameter criterion) that removes the subjective hesitation, and the cultural message (from the top of the organisation down) that it is always acceptable to call, and never acceptable to delay a call for a patient you are worried about. A "false positive" MET call costs a few minutes of a team's time; a delayed call costs a life. [1]
Rapid response systems — do they work?
The evidence base for rapid response systems is the question every acute physician must answer with nuance, because the data are mixed and the examiners know it. [1]
The MERIT study (Hillman and colleagues, 2005) was the landmark cluster-randomised controlled trial of the MET system across 23 Australian hospitals. It found that introducing the MET system increased the rate of emergency team calls (from 3.1 to 8.7 per 1000 admissions) but did not significantly reduce the composite primary outcome of cardiac arrest, unexpected death, or unplanned ICU admission (5.31 versus 5.86 per 1000 admissions) [3]. The trial was criticised for inadequate statistical power, contamination (control hospitals increased their own MET-like calls during the study), and a short implementation period — but it remains the only randomised evidence and the result must be carried honestly.
The meta-analytic evidence is more favourable. Chan and colleagues' 2010 systematic review and meta-analysis of 18 studies found that rapid response teams were associated with a 33.8 per cent reduction in non-ICU cardiopulmonary arrests (relative risk 0.66) but no significant reduction in overall hospital mortality (RR 0.96) [5]. Maharaj and colleagues' 2015 Cochrane-style review suggested reductions in both cardiac arrest and mortality in adults but assessed the evidence as low quality due to heterogeneity and before-and-after design [6].
The synthesis the registrar should carry: [1]
- Rapid response systems reduce non-ICU cardiac arrests — this is the consistent finding across studies and meta-analyses.
- The effect on overall hospital mortality is less certain — the trials are underpowered, the designs are observational, and the effect may be diluted by deaths in patients for whom escalation is inappropriate.
- The mechanism of benefit is broader than the arrest count — rapid response systems change the safety culture of a hospital, surface the deteriorating patient earlier, support ward staff, and facilitate appropriate (not just more) escalation.
- The negative MERIT result does not invalidate the system — it is the starting point for understanding why culture, implementation, and the afferent (recognition) limb matter as much as the efferent (response) limb. [1]
End-of-life decision-making in the deteriorating patient
Not every deterioration should be met with escalation. The deteriorating patient with advanced chronic disease, a terminal illness, or an acute event from which recovery is not realistic deserves a considered decision about the ceiling of care — and that decision must be made before the crisis, with the patient and family where possible, and communicated clearly to the team. [1]
The frameworks and concepts: [1]
- Ceiling of treatment — the most intensive level of treatment that is appropriate for this patient at this time. The ceiling might be ward-based supportive care (no escalation to ICU, no CPR), ward-based active treatment (fluid, antibiotics, oxygen, but not ventilation), high-dependency (single-organ support, but not multi-organ ICU), or full ICU and resuscitation. The ceiling is a clinical decision, made with the patient's informed preferences and the realistic prognosis.
- Not for cardiopulmonary resuscitation (DNACPR / NFR) — a specific decision that CPR will not be attempted in the event of arrest. The decision is based on the clinical judgement that CPR will not succeed (the patient with advanced metastatic cancer, end-stage heart failure, or frailty with aRockwood score indicating very poor baseline function) or that the burdens (rib fractures, ICU, prolonged coma) outweigh the benefits. The decision is documented, communicated to the patient (if they wish to know) and the family, and recorded in a recognised form that travels with the patient.
- Advance care directives and advance care planning — the patient's own statement of the treatments they would or would not want, made in advance of incapacity. In Australia, an Advance Care Directive is a legally binding document; in the UK, advance decisions to refuse treatment have legal force under the Mental Capacity Act. The clinician's job is to ask for and respect the directive, and where none exists, to facilitate the conversation.
- Goals of care — the broader framing that aligns the treatment plan with what the patient wants to achieve (cure, prolongation of life, comfort, or a dignified death). The goals-of-care conversation is the conversation that surfaces the ceiling of care; it should happen early in the admission for any patient with advanced disease, not in the middle of a crisis.
- The deteriorating patient as a trigger for the conversation — a rise in NEWS2, an unplanned ICU admission, a second escalation in 24 hours, or a failure to respond to appropriate therapy are all triggers to ask: "Is this deterioration expected? Is escalation appropriate? What would the patient want?" The registrar who treats every deterioration as a resuscitation problem without this question has missed a major part of acute medicine. [1]
The communication skill is to reframe the conversation from "we are giving up" to "we are focusing on what will help." The patient or family who hears "we will not resuscitate" may hear abandonment; the patient or family who hears "we will focus on comfort, on symptom control, and on being with your family, and we will not pursue treatments that will cause suffering without benefit" hears care. The clinician who can hold both frames — the active treatment of reversible pathology alongside the honest prognosis and the comfort-focused plan — is the clinician who manages the deteriorating patient well. [1]
DCE long-case approach
Patient scenario
Mrs Margaret O'Sullivan, 78, retired teacher, was admitted four days ago with community-acquired pneumonia. She has a background of ischaemic heart disease (prior NSTEMI three years ago), chronic kidney disease stage 3 (baseline creatinine 140 micromol/L), type 2 diabetes (on metformin and empagliflozin), hypertension, and moderate aortic stenosis. She lives independently with her husband. The nurse calls you at 02:00 because her NEWS2 has risen from 3 to 9 over the last six hours. [1]
On assessment: respiratory rate 30, SpO2 88 per cent on room air (92 per cent on 15 L via reservoir mask), temperature 38.7, heart rate 128 in new atrial fibrillation, blood pressure 84/52, GCS 14 (new mild confusion), capillary refill 4 seconds, mottled peripheries, urine output 15 mL/hour via catheter. Lactate 4.6. Creatinine 210 (up from 140). Potassium 5.8. Chest X-ray shows progressive right lower lobe consolidation. [1]
Candidate's opening statement (SASPOP)
"Mrs O'Sullivan is a 78-year-old retired teacher who was admitted four days ago with community-acquired pneumonia and has acutely deteriorated overnight with a rising NEWS2 from 3 to 9. She has ischaemic heart disease, chronic kidney disease, type 2 diabetes, and moderate aortic stenosis. Her main problems are septic shock from progressive pneumonia with new-onset atrial fibrillation, acute kidney injury with hyperkalaemia, and a rising lactate indicating tissue hypoperfusion. My immediate priorities are the ABCDE assessment with high-flow oxygen, intravenous fluid resuscitation, the Sespis Six bundle with broad-spectrum antibiotics, treatment of her hyperkalaemia, and an urgent MET call for ICU outreach review given her refractory hypotension, multi-organ involvement, and the need to consider the ceiling of care in the context of her comorbidities." [1]
Problem list
- Septic shock — progressive pneumonia, refractory hypotension, lactate 4.6, mottled peripheries.
- New atrial fibrillation with rapid ventricular response — heart rate 128, likely a complication of the sepsis and the acute illness.
- Acute kidney injury with hyperkalaemia — creatinine risen from 140 to 210, potassium 5.8, oliguric; on a background of CKD 3 and potential nephrotoxic contribution from empagliflozin (which should be withheld).
- Respiratory failure — type 1, with SpO2 88 per cent on room air; at risk of type 2 given the hyperkalaemia and the reduced conscious level.
- Delirium — new mild confusion; a marker of severity and a management priority (identify and treat the cause, avoid sedatives, orient and reassure).
- Underlying comorbidities and the ceiling-of-care question — ischaemic heart disease, aortic stenosis, CKD, diabetes; the question of whether ICU escalation is appropriate. [1]
Integrated management plan
- ABCDE resuscitation in parallel with the diagnostic workup: high-flow oxygen to target SpO2 92 to 96 per cent; two large-bore cannulae; 500 mL balanced crystalloid bolus repeated to clinical effect while watching for fluid overload (she has aortic stenosis and is at risk of pulmonary oedema); continuous cardiac monitoring. [1]2. Sepsis Six within one hour: blood cultures, broad-spectrum IV antibiotics (the pneumonia has progressed on first-line therapy — escalate to a broader regimen per local guideline, e.g. piperacillin-tazobactam, and reconsider the organism, including atypical and resistant pathogens), 30 mL/kg crystalloid, lactate, urine output, oxygen.
- Treat the hyperkalaemia (potassium 5.8 with ECG changes if present): calcium gluconate 10 mL of 10 per cent IV for membrane stabilisation, insulin-dextrose (10 units Actrapid in 50 mL of 50 per cent dextrose), salbutamol nebuliser; recheck potassium and ECG.
- Manage the atrial fibrillation: the AF is almost certainly secondary to the sepsis and the acute illness. Rate control with a beta-blocker or digoxin is problematic given the hypotension; the priority is to treat the sepsis and the shock. If the AF is causing haemodynamic compromise beyond the shock, consider amiodarone 300 mg IV over one hour, or synchronised DC cardioversion if she is peri-arrest. Avoid calcium-channel blockers in hypotension.
- Withhold the nephrotoxic and harmful drugs: metformin (lactic acidosis risk in AKI and shock), empagliflozin (euglycaemic DKA risk, nephrotoxic in volume depletion), ACE inhibitor or ARB if she is on one (hypotension and AKI), NSAIDs. Manage her glucose with a sliding-scale insulin protocol.
- Escalate and consider the ceiling of care: call ICU outreach now. She has multi-organ failure (shock, AKI, respiratory failure, delirium) and is likely to need vasopressor support and possibly non-invasive ventilation. The decision about ICU admission must weigh her comorbidities (CKD, aortic stenosis, ischaemic heart disease), her baseline function (independent, living with her husband), and her expressed wishes (ask the family about advance care directives). A patient with this comorbidity profile who is independent at baseline is, in most institutions, a candidate for a trial of ICU-level care with a defined review point. [1]
Examiner probing questions
- "Her NEWS2 rose from 3 to 9 over six hours. What does that trajectory tell you, and what should have happened at each stage?" → "The trajectory tells me she was deteriorating throughout, and the responses at each stage should have been: NEWS2 of 5 to 6 should have triggered an urgent ward-registrar review and an increase in monitoring to hourly; the failure to arrest the rise indicates the ward-level therapy was inadequate and the escalation to ICU outreach should have been earlier. The lesson is that the trend is the signal, and a single 'acceptable' value in a rising trend is not reassuring." [1]- "How would you decide whether she is for ICU?" → "I would weigh three things: the reversibility of the acute problem (the pneumonia is potentially reversible with antibiotics and support), her baseline function (she is independent, which favours escalation), and her expressed wishes (I would ask her family about an advance care directive and about what she would want). On balance, a previously independent 78-year-old with reversible sepsis is, in most institutions, a candidate for a time-limited trial of ICU care, with a clear review point at 48 to 72 hours and an honest conversation with the family throughout."
- "Why has she developed atrial fibrillation?" → "New AF in the acutely ill is multifactorial — the sepsis drives sympathetic surge and atrial stretch, the fever and the reduced conscious level increase catecholamine release, the electrolyte disturbance (she is hyperkalaemic and likely hypomagnesaemic) lowers the threshold, and her underlying ischaemic heart disease and aortic stenosis provide the substrate. The treatment is to treat the sepsis and correct the electrolytes; the AF will usually revert as the acute illness resolves. Specific antiarrhythmic therapy is reserved for haemodynamically compromising AF that persists after the sepsis is treated."
- "What is her prognostic risk, and how would you communicate it?" → "She has septic shock with multi-organ failure on a background of significant comorbidity. Her in-hospital mortality risk is high — perhaps 30 to 50 per cent on the worst day. I would communicate this to her family with honesty and hope: that the sepsis is treatable, that she is in the best place for the supportive care she needs, that the next 48 hours will tell us whether the treatment is working, and that we will keep them informed at every step. I would also ask, gently, what she would want if the treatment were not working — to surface the ceiling-of-care conversation early, not in a crisis." [1]
DCE short-case discussion: the bedside assessment
Instruction: "You are called to review a ward patient the nursing staff are concerned about. Describe your systematic approach to the assessment." [1]
Systematic assessment routine
- End of the bed — the "look" test. Is the patient in distress? Are they breathing comfortably, using accessory muscles, or see-saw breathing? Is the colour normal, pale, cyanosed, mottled, flushed? Is the conscious level appropriate — are they rousable, agitated, drowsy? The experienced clinician forms a gestalt of "sick or not sick" in the first five seconds, and that gestalt is rarely wrong.
- Review the observation chart (NEWS2 trend) — the full vital sign set and the trajectory over the last 12 to 24 hours. Identify the parameter that is driving the score, the rate of change, and any "red score" single-parameter derangements. The chart tells the story that the bedside confirms.
- ABCDE in order — airway (patency, adjuncts), breathing (rate, effort, SpO2, auscultation), circulation (heart rate, blood pressure, capillary refill, JVP, mottling, urine output), disability (GCS/AVPU, pupils, glucose), exposure (temperature, full examination including the abdomen, the skin, the lines, the wound).
- Focused history and chart review — the admission diagnosis, the comorbidities, the drug chart (every drug, every dose, every recent change), the recent results (bloods, imaging, microbiology), and the collateral from the nursing staff and the family. [1]
Presentation template
"I have assessed Mrs O'Sullivan, a 78-year-old woman admitted with pneumonia. She is critically unwell. Her NEWS2 is 9, driven by a respiratory rate of 30, SpO2 of 88 per cent on room air, heart rate of 128 in new atrial fibrillation, blood pressure of 84 over 52, GCS of 14 with new confusion, and a temperature of 38.7. On ABCDE: her airway is patent; she is tachypnoeic with accessory muscle use and bilateral basal crackles; she is tachycardic in AF, hypotensive with a capillary refill of 4 seconds and mottled peripheries, and oliguric at 15 mL/hour; she is mildly confused with a GCS of 14 and a normal bedside glucose; she is febrile with a rigid abdomen not examined in detail. My working diagnosis is septic shock with multi-organ failure. My immediate plan is high-flow oxygen, intravenous fluid resuscitation, the Sepsis Six bundle, treatment of her hyperkalaemia, and an urgent MET call for ICU outreach. I am worried about her aortic stenosis and the risk of fluid overload, and I will reassess her response to the first bolus before giving more." [1]
Discussion questions
Examiner: "What is your threshold for calling ICU outreach?" [1]
"My threshold is set by the NEWS2 and by my clinical concern. A NEWS2 of 7 or more is an automatic emergency call; a single red-score parameter (any score of 3) is an urgent review; a NEWS2 of 5 or 6 with a rising trend or a failure to respond to ward therapy is an urgent call. But the threshold I weight most heavily is the subjective one — if I am worried, or if the nursing staff are worried, I call. The 'worried' criterion is deliberately built into the MET criteria because it precedes the measurable derangement, and a call that turns out to be unnecessary costs minutes; a call that should have been made and was not, costs a life." [1]
Examiner: "How do you decide whether a patient is 'not for escalation'?" [1]
"The decision is made by a senior clinician, ideally the treating consultant, in discussion with the patient (if they have capacity) or their family and the multidisciplinary team. The factors are the reversibility of the acute illness, the patient's baseline function and quality of life, the burden of the proposed treatment relative to the likely benefit, and the patient's expressed wishes (an advance care directive, a prior conversation, or the family's report of what the patient would want). The decision is documented, communicated to the team and the family, and revisited if the clinical situation changes. The decision is not 'giving up' — it is focusing the care on what will help, which may be comfort, symptom control, and the presence of family, alongside the active treatment of reversible elements." [1]
Examiner: "What is the evidence that rapid response systems save lives?" [1]
"The evidence is nuanced. The MERIT study, the only cluster-randomised trial, did not show a significant reduction in the composite of cardiac arrest, unexpected death, or unplanned ICU admission, though it was underpowered and had methodological issues. The meta-analytic evidence, including Chan's 2010 systematic review, shows a consistent reduction in non-ICU cardiopulmonary arrests of about a third, but a less consistent effect on overall hospital mortality [5]. My reading of the evidence is that rapid response systems work by changing the culture of the hospital — surfacing deterioration earlier, supporting ward staff, and facilitating appropriate escalation — and that the benefit is real even if the mortality signal is diluted by the patients for whom escalation is appropriately withheld."
Key DWE MCQ patterns
- Recognise deterioration from the vital sign trend. A patient whose respiratory rate has risen from 18 to 24 to 30 over six hours is deteriorating — the trend is the answer even if each value is not catastrophic, and the response is urgent review, not "recheck in an hour."
- NEWS2 response thresholds. A NEWS2 of 7 or more is a clinical emergency requiring an emergency critical care assessment within minutes; 5 to 6 requires urgent ward-registrar review; a single red score (3 in any parameter) mandates urgent review regardless of the aggregate.
- The first investigation in the deteriorating patient with an altered conscious level. Bedside blood glucose — hypoglycaemia is rapidly reversible and is missed catastrophically if not measured.
- The order of ABCDE. Airway before breathing, breathing before circulation — treat the life-threat in front of you before moving on. The patient with an obstructed airway is not helped by a fluid bolus.
- The cause of shock determines the treatment. Hypovolaemic responds to fluid, cardiogenic is worsened by excessive fluid, obstructive needs decompression, distributive needs fluid and vasopressors. The wrong treatment for the wrong cause worsens the patient.
- The ceiling of care and the DNACPR decision. The decision is clinical, made with the patient and family, documented and communicated — and a deterioration is a trigger to revisit it, not an automatic trigger for escalation.
- The SBAR recommendation must be specific. "I would like you to come and review this patient now" is the recommendation; "I just thought I would let you know" is a failure to escalate.
- The MERIT study result. The introduction of the MET system increased calls but did not significantly reduce the composite primary outcome — the honest answer the examiner wants. [1]
References
[1] Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest 1990;98(6):1388–92. The foundational prospective study showing that 84 per cent of in-hospital arrest patients had documented deterioration in the preceding eight hours, with respiratory and mental-state changes dominating — the empirical basis for every track-and-trigger system.
[2] Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013;84(4):465–70. The validation of NEWS against 33 other early warning scores, demonstrating discrimination of cardiac arrest, unanticipated ICU admission, and death.
[3] Hillman K, Chen J, Cretikos M, et al.; MERIT study investigators. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet 2005;365:2091–7. The landmark — and only — randomised trial of the MET system, showing increased MET calls but no significant reduction in the composite primary outcome.
[4] Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021;47(11):1181–1247. The international consensus on the recognition and management of sepsis, including the hour-1 bundle, fluid resuscitation, vasopressors, and the source-control principles that frame the management of the commonest cause of ward deterioration.
[5] Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid Response Teams: a systematic review and meta-analysis. Arch Intern Med 2010;170(1):18–25. The meta-analysis of 18 studies showing a 33.8 per cent reduction in non-ICU cardiopulmonary arrests with rapid response teams, but no significant reduction in overall hospital mortality.
[6] Maharaj R, Raffaele I, Wendon J. Rapid response systems: a systematic review and meta-analysis. Cochrane Database Syst Rev 2015. The Cochrane-style review suggesting reductions in both cardiac arrest and mortality in adults but assessing the evidence as low quality due to heterogeneity and before-and-after design.
Schein et al., Chest 1990; Smith et al., Resuscitation 2013; Hillman et al. (MERIT), Lancet 2005; Evans et al. (Surviving Sepsis 2021), Intensive Care Med 2021; Chan et al., Arch Intern Med 2010; Maharaj et al., Cochrane 2015; Royal College of Physicians NEWS2 2017; NICE CG50; Australian Commission on Safety and Quality in Health Care Standard 9. [1]
References
- [1]Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL Clinical antecedents to in-hospital cardiopulmonary arrest Chest, 1990.PMID 2245680
- [2]Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death Resuscitation, 2013.PMID 23295778
- [3]Hillman K, Chen J, Cretikos M, et al.; MERIT study investigators Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial Lancet, 2005.PMID 15964445
- [4]Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021 Intensive Care Med, 2021.PMID 34599691
- [5]Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C Rapid Response Teams: A Systematic Review and Meta-analysis Arch Intern Med, 2010.PMID 20065195
- [6]Maharaj R, Raffaele I, Wendon J Rapid response systems: a systematic review and meta-analysis Crit Care, 2015.PMID 26070457