Phys · general-medicine
Drug Allergy and Desensitisation
Also known as drug hypersensitivity · drug allergy · penicillin allergy · beta-lactam allergy · drug desensitisation · rapid drug desensitisation · drug provocation testing · aspirin-exacerbated respiratory disease · AERD · Samter triad · DRESS · drug reaction with eosinophilia and systemic symptoms · Stevens-Johnson syndrome · SJS · toxic epidermal necrolysis · TEN · SCORTEN
Consultant-physician-depth guide to drug allergy and desensitisation for FRACP DWE and DCE — the allergy-versus-intolerance distinction, the immediate IgE-mediated versus delayed T-cell mediated classification, beta-lactam allergy with penicillin skin testing and side-chain-based cross-reactivity and the modern delabeling strategy, non-beta-lactam allergies (sulfonamide, NSAID hypersensitivity and aspirin-exacerbated respiratory disease, local anaesthetics, radiocontrast media), the severe cutaneous adverse reactions DRESS and Stevens-Johnson syndrome or toxic epidermal necrolysis with the RegiSCAR and SCORTEN scores, and the principle and indications of drug desensitisation with the Brigham 12-step protocol and drug provocation testing as the diagnostic gold standard.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Drug Allergy and Desensitisation

The answer first
Drug allergy is an immunologically mediated, reproducible adverse reaction occurring at a dose normally tolerated. That single sentence separates it from drug intolerance, which is a non-immune, dose-related adverse effect (codeine nausea, aspirin tinnitus, statin myalgia). The distinction matters because an allergy label carries a lifelong contraindication weight that an intolerance does not, and because most allergy labels in medical records are false. [1]
Three rules that change outcome: [1]
- Most penicillin allergy labels are wrong or have been outgrown. Only 10 to 20 per cent of patients who carry the label have true allergy on formal testing. The label drives the use of broader, more toxic and more expensive antibiotics, higher rates of resistant infection and Clostridioides difficile, longer stays and higher mortality. Proactive delabeling is a patient-safety intervention, not a nicety [1].
- Beta-lactam cross-reactivity is side-chain-based, not core-ring-based. The historical 10 per cent penicillin-cephalosporin cross-reactivity is wrong; the modern figure is 1 to 2 per cent overall and near zero for cephalosporins with dissimilar R1 side chains (ceftriaxone, cefuroxime). Carbapenem cross-reactivity is under 1 per cent [4].
- Desensitisation induces temporary tolerance for an essential drug with no alternative — and the tolerance is lost if the drug is stopped for more than 48 hours. Desensitisation is never used after Stevens-Johnson syndrome, toxic epidermal necrolysis or DRESS [5].
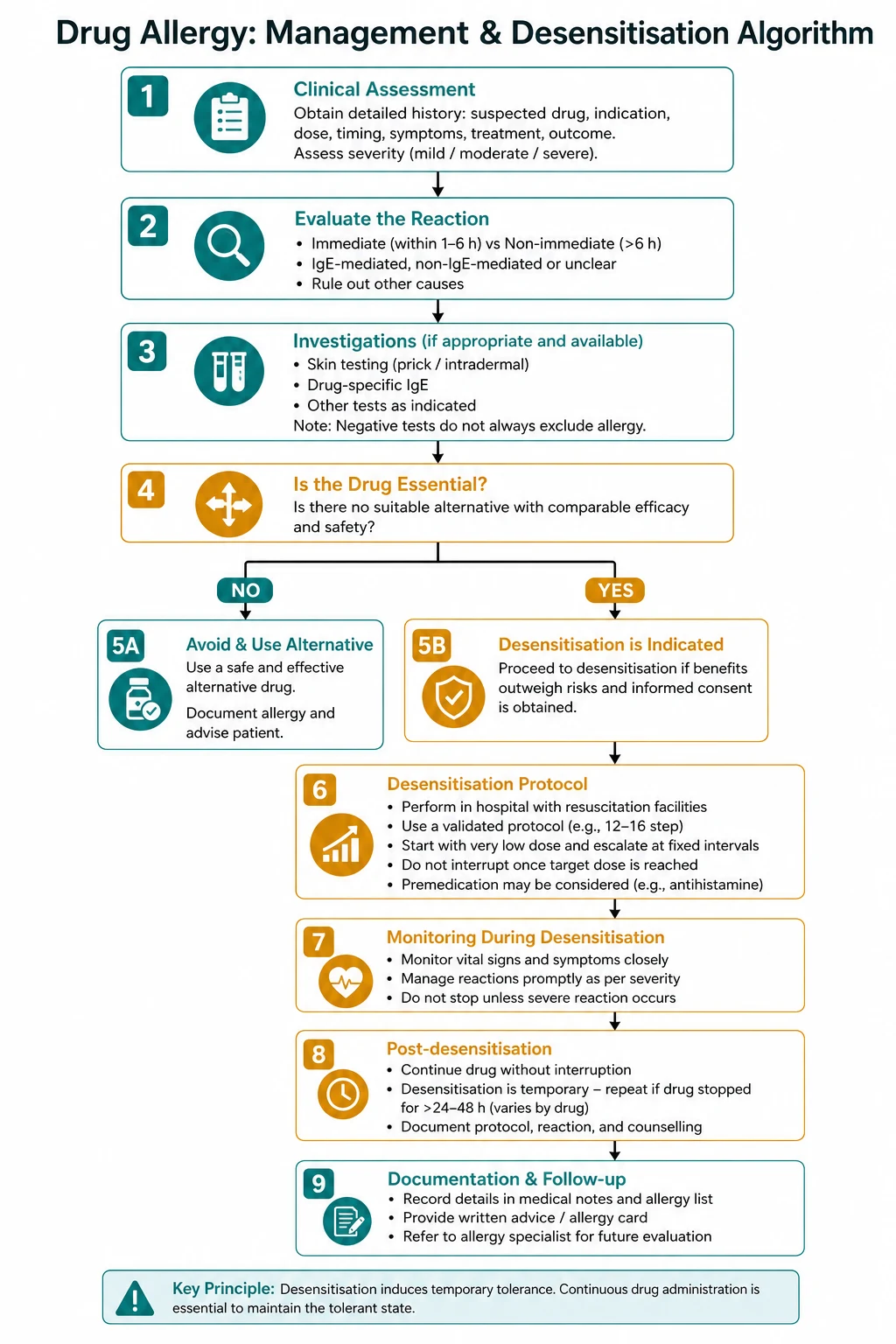
The clinical reasoning moves in three steps at the bedside. First, take a structured allergy history — the culprit drug, the timing relative to dosing, the clinical features, the time since the reaction and any co-administered drugs. Second, classify by timing — immediate (minutes to 1 hour, IgE) versus delayed (hours to weeks, T-cell) — because the mechanism dictates the testing strategy and the contraindication weight. Third, risk-stratify and decide — low risk warrants a direct oral challenge; higher risk warrants skin testing then challenge; a severe delayed reaction is an absolute lifelong contraindication; an essential drug with no alternative warrants desensitisation. [1]
Allergy versus intolerance — the conceptual framework
The first question with any reported drug reaction is whether it is immune-mediated. Drug allergy is an immunological response — IgE, T-cell, immune complex or cytotoxic — that is reproducible on re-exposure and occurs at doses normally tolerated by others. Drug intolerance is a non-immune, expected, dose-related pharmacological effect: opioid nausea and pruritus (histamine release), aspirin tinnitus (dose-dependent ototoxicity), metformin gastrointestinal upset, statin myalgia. [1]
The distinction is not semantic. An allergy label is entered into the electronic medication record, printed on the wristband, and drives lifelong avoidance of a drug class. An intolerance label rarely carries that weight — a patient who is nauseated by codeine can still receive morphine, and a patient with aspirin tinnitus can still receive low-dose aspirin for cardiovascular protection if the indication justifies it. The most common error is transcribing a childhood intolerance (a rash with a viral illness that coincided with an antibiotic) as a lifelong penicillin allergy — and then denying that patient beta-lactams for decades. [1]
DWE high-yield: The single most testable distinction is allergy (immune-mediated, reproducible at any dose) versus intolerance (non-immune, dose-related, expected pharmacological effect). Most penicillin allergy labels in medical records are false; only 10 to 20 per cent have true allergy on testing. [1]
Classification framework

The classification that matters at the bedside is timing: immediate (within minutes to one hour) versus delayed (hours to days, sometimes weeks). The timing defines the mechanism and the testing strategy. [1]
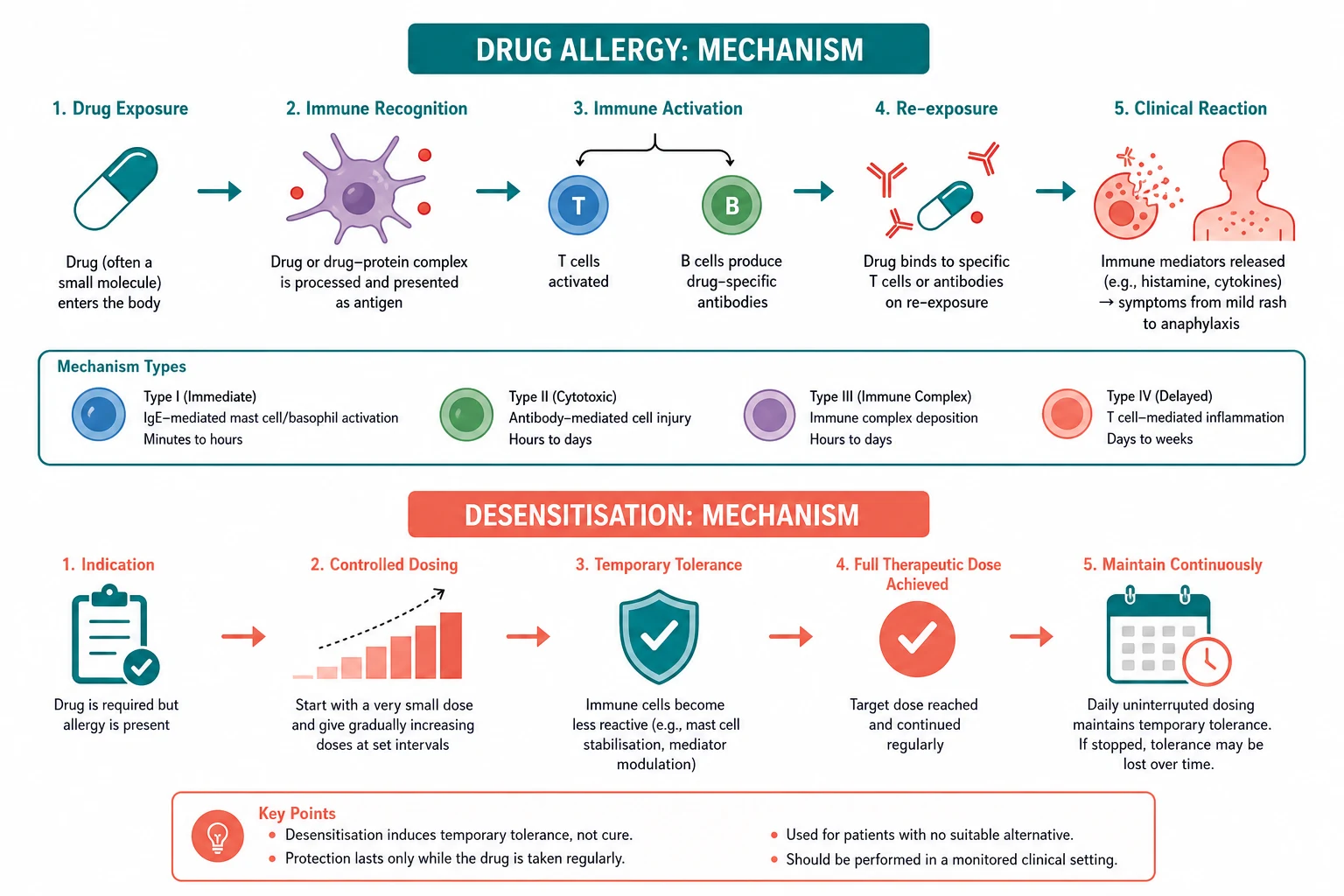
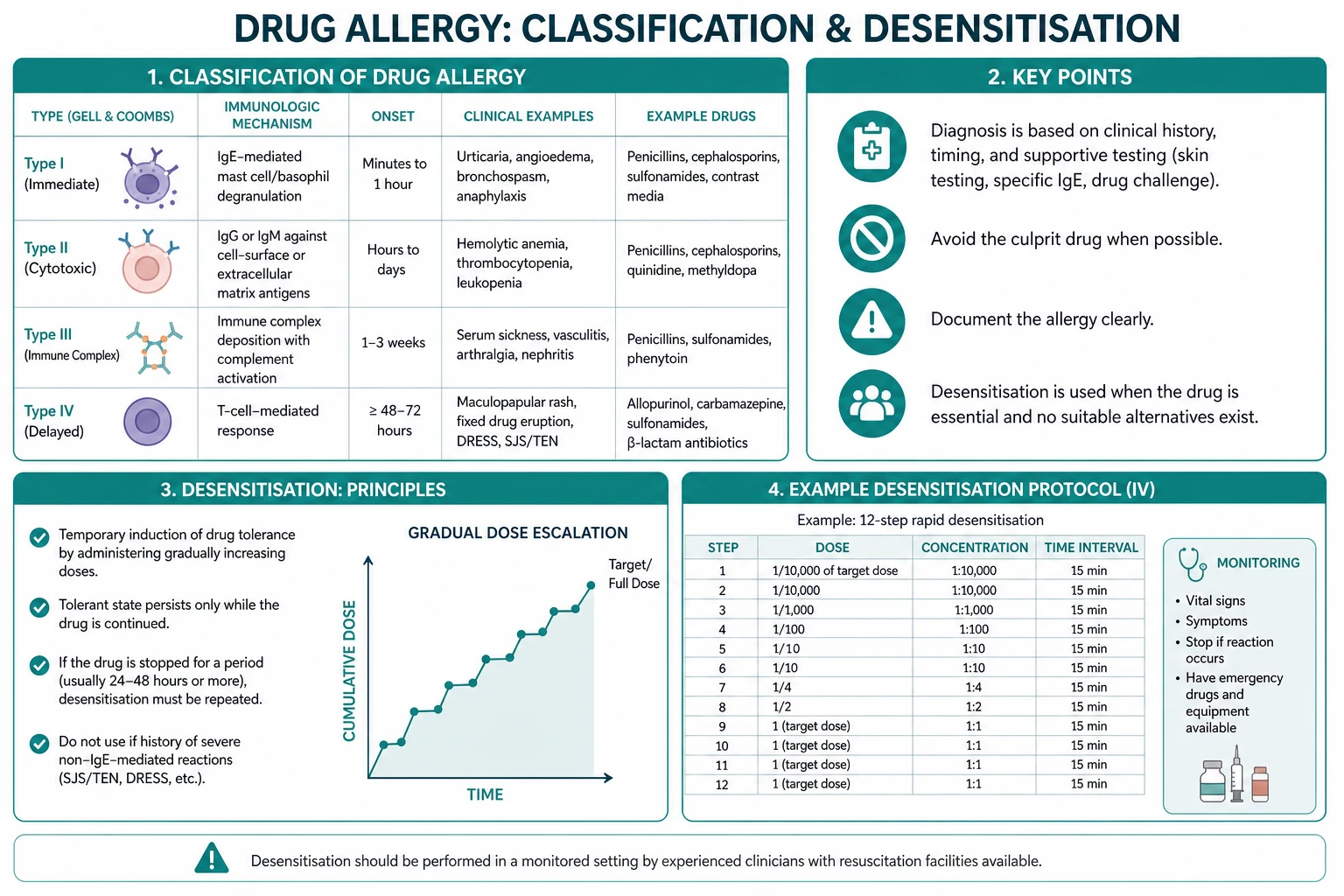
Immediate reactions (minutes to 1 hour) are IgE-mediated (type I). Drug-specific IgE binds the Fc-epsilon-RI receptor on mast cells and basophils; cross-linking by the drug triggers degranulation of preformed histamine and tryptase and synthesis of leukotrienes and prostaglandins. The clinical phenotype is urticaria, angioedema, conjunctivitis, rhinitis, bronchospasm, hypotension and anaphylaxis. The defining feature is onset within one hour — not severity. A patient who develops urticaria 30 minutes after a penicillin dose has an IgE reaction; a patient who develops a maculopapular rash on day 7 has a T-cell reaction. [1]
Delayed reactions (hours to weeks) are T-cell mediated (type IV). Drug-specific T cells recognise drug-modified peptides and mount a cytokine response whose phenotype depends on the T-cell profile and target tissue. The clinical phenotypes are: [1]
- Maculopapular exanthem — the commonest, appearing days 5 to 10 of treatment, often with pruritus and low-grade fever.
- Fixed drug eruption — a round, well-demarcated erythematous to violaceous plaque that reappears at the same anatomical site on each re-exposure, with residual hyperpigmentation.
- DRESS (drug reaction with eosinophilia and systemic symptoms) — 2 to 8 weeks after exposure, with fever, facial oedema, lymphadenopathy, eosinophilia, atypical lymphocytes and multi-organ involvement (hepatitis, interstitial nephritis, pneumonitis).
- Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) — full-thickness epidermal necrosis with mucosal involvement, occurring days to weeks after exposure; SJS involves under 10 per cent of body surface area, the SJS-TEN overlap 10 to 30 per cent, and TEN over 30 per cent.
- Acute generalised exanthematous pustulosis (AGEP) — sterile non-follicular pustules on an erythematous base within hours to days, usually self-limiting. [1]
Type II (cytotoxic) and type III (immune complex) reactions are less common — drug-induced immune haemolytic anaemia, heparin-induced thrombocytopenia, serum sickness-like reactions. [1]
Beta-lactam allergy
Penicillin allergy — the commonest label and the delabeling imperative
Penicillin is the most commonly reported drug allergy. Approximately 10 per cent of patients carry the label, but only 10 to 20 per cent of those — that is, 1 to 2 per cent of the population — have true allergy on formal testing [1]. The rest have either a non-allergic rash (viral exanthem, intolerance), a reaction that has resolved with time (IgE allergy wanes over years in most patients), or a label transcribed from a childhood history that was never allergic.
The harm of a false label is substantial and measurable. Penicillin-allergic patients receive more fluoroquinolones, clindamycin, aztreonam and vancomycin; they have higher rates of methicillin-resistant Staphylococcus aureus (MRSA) colonisation, Clostridioides difficile infection, longer hospital stays, surgical site infections and higher mortality. Delabeling is therefore a patient-safety intervention. [1]
The risk-stratified delabeling strategy from the 2022 practice parameter [1]:
- Low risk — remote (more than 10 years ago), non-severe, vague childhood rash, or a reaction without immediate features. These patients can be delabeled by a direct oral amoxicillin challenge (250 mg with 1 hour observation) without prior skin testing. Over 95 per cent tolerate the challenge.
- Moderate risk — a more recent (within 10 years) or more convincing immediate history. These patients undergo penicillin skin testing with major and minor determinants, followed by an oral amoxicillin challenge if the skin test is negative.
- High risk — recent anaphylaxis, severe immediate features, or a history of SJS, TEN or DRESS. These patients are not challenged. If a beta-lactam is essential, proceed to skin testing in a specialist setting or desensitisation. SJS, TEN and DRESS are absolute lifelong contraindications to re-exposure. [1]
Penicillin skin testing uses the major determinant (penicilloyl-polylysine, Pre-Pen), which accounts for 95 per cent of metabolites, and the minor determinant mixture (penilloate, penicilloate), which accounts for most IgE anaphylaxis. A negative skin test has a negative predictive value above 95 per cent for IgE allergy — but a positive skin test requires confirmation with an oral challenge, because skin-test sensitivity exceeds clinical reactivity [1].
Cross-reactivity — the side-chain principle

The beta-lactam ring is the core allergenic determinant of penicillin, but cross-reactivity between penicillin and other beta-lactams is determined by the R1 side chain, not the core ring. The historical 10 per cent figure came from early studies that included contaminated cephalosporins and did not account for side-chain specificity [4].
The modern figures: [1]
- Penicillin to cephalosporin — approximately 1 to 2 per cent overall. Cross-reactivity is concentrated in cephalosporins that share the aminopenicillin (amoxicillin/ampicillin) R1 side chain: cefalexin, cefaclor, cefadroxil, cefprozil, cefatrizine. These should be avoided in amoxicillin-allergic patients. Cephalosporins with dissimilar side chains (ceftriaxone, cefuroxime, cefepime, ceftazidime) can be given safely to most penicillin-allergic patients.
- Penicillin to carbapenem — less than 1 per cent. The trans-hydroxyethyl side chain of carbapenems differs from the penicillin side chain. Meropenem, imipenem and ertapenem can be given to most penicillin-allergic patients without skin testing.
- Penicillin to aztreonam (monobactam) — negligible cross-reactivity, except in patients specifically sensitised to ceftazidime (which shares the same side chain). [1]
The practical rule: when a cephalosporin is needed in a penicillin-allergic patient, choose one with a dissimilar R1 side chain. Ceftriaxone and cefuroxime are safe choices for most penicillin-allergic patients; cefalexin is not, if the allergy is to amoxicillin. [1]
Examiner trap: Never quote 10 per cent penicillin-cephalosporin cross-reactivity in a modern exam. The figure is 1 to 2 per cent overall and near zero for dissimilar side chains. The 10 per cent figure is a historical artefact from contaminated early cephalosporins. [1]
Non-beta-lactam drug allergies
Sulfonamide antibiotics
Sulfonamide antibiotics (trimethoprim-sulfamethoxazole, TMP-SMX) are a leading cause of drug allergy, especially in HIV-positive patients on Pneumocystis jirovecii prophylaxis. The reaction is usually a delayed maculopapular rash; severe reactions (SJS, TEN, DRESS) occur and are more common in HIV. [1]
Two facts to carry: [1]
- Cross-reactivity between sulfonamide antibiotics and non-antibiotic sulfonamides (frusemide, thiazides, sulfasalazine, celecoxib) is negligible. The structures differ enough that a sulfonamide antibiotic allergy is not a contraindication to frusemide or a thiazide unless there is a specific reaction to that drug. The common myth of "sulfa allergy" lumping all sulfonamides together is wrong.
- TMP-SMX desensitisation is established for HIV patients with non-severe prior reactions who need prophylaxis or treatment, with success in the majority; it is absolutely contraindicated after SJS or TEN. [1]
NSAID hypersensitivity
NSAID hypersensitivity has several distinct phenotypes, and the phenotype determines management: [1]
- Cross-reactive NSAID hypersensitivity (the commonest) — urticaria or angioedema within hours of any COX-1 inhibitor (aspirin, ibuprofen, naproxen, diclofenac). The mechanism is COX-1 inhibition diverting arachidonic acid to leukotriene synthesis. Selective COX-2 inhibitors (celecoxib) are usually tolerated because they spare COX-1.
- Aspirin-exacerbated respiratory disease (AERD, Samter triad) — adult-onset asthma, nasal polyps and bronchospasm or nasal congestion within 30 to 120 minutes of aspirin or a non-selective NSAID. The mechanism is the same COX-1 inhibition-driven leukotriene excess. Management is leukotriene receptor antagonists (montelukast), intranasal steroids, endoscopic sinus surgery, and aspirin desensitisation (graded oral aspirin to 650 mg twice daily maintenance) in selected patients.
- Single-NSAID IgE reaction — urticaria or anaphylaxis to one NSAID with tolerance of others. This is a true IgE allergy to a specific drug, and cross-reactivity with other NSAIDs does not apply.
- Delayed NSAID reactions — contact dermatitis, SJS/TEN (rare), nephritis. [1]
DWE high-yield: Aspirin-exacerbated respiratory disease is the triad of asthma, nasal polyps and aspirin sensitivity. The mechanism is COX-1 inhibition driving leukotriene excess. Selective COX-2 inhibitors (celecoxib) are usually tolerated. Aspirin desensitisation reduces polyp regrowth and asthma exacerbations after sinus surgery. [1]
Local anaesthetics
True IgE allergy to local anaesthetics is vanishingly rare. Most reactions attributed to local anaesthetic allergy are: [1]
- Vasovagal syncope — bradycardia, pallor, hypotension, rapid recovery with recumbency; common with dental injection.
- Local anaesthetic systemic toxicity — circumoral tingling, tinnitus, agitation, seizures, then cardiac depression from sodium channel blockade; a dose-dependent effect of amide anaesthetics (lignocaine, bupivacaine), not allergy.
- Epinephrine effect — palpitations, tremor, tachycardia from the added vasoconstrictor.
- Allergy to the ester class — procaine and other esters are metabolised to para-aminobenzoate (PABA), a known allergen; the amide class (lignocaine, bupivacaine, ropivacaine) is far less allergenic. [1]
When a patient reports local anaesthetic allergy, the strategy is to use an amide local anaesthetic from a different class (lignocaine if the reaction was to procaine), with or without a graded challenge. Skin testing is rarely needed. [1]
Radiocontrast media
Radiocontrast reactions are immediate (within minutes), non-IgE and mast-cell mediated — direct histamine release from the hyperosmolar contrast. The key points: [1]
- Risk is higher with high-osmolar ionic contrast and in patients with prior reactions. Use low-osmolar non-ionic contrast in all patients with a prior reaction.
- Premedicate with a glucocorticoid (oral prednisolone 50 mg at 13 hours, 7 hours and 1 hour before, or intravenous hydrocortisone 200 mg at 1 hour before if urgent) plus an H1 antihistamine (oral chlorphenamine or intravenous equivalent).
- Radiocontrast reactions have no relationship to iodine or seafood allergy. The mechanism is mast cell histamine release, not IgE to iodine. Patients with seafood or iodine allergy do not require premedication unless they have had a prior contrast reaction. [1]
Severe cutaneous adverse reactions
DRESS — drug reaction with eosinophilia and systemic symptoms
DRESS (also called drug-induced hypersensitivity syndrome, DIHS) is a delayed multi-organ T-cell reaction occurring 2 to 8 weeks after drug exposure. The classic culprits are anticonvulsants (carbamazepine, phenytoin, lamotrigine), sulfonamide antibiotics, allopurinol, minocycline, dapsone and vancomycin. [1]
Clinical features: fever, a diffuse maculopapular rash that may become exfoliative, facial oedema, lymphadenopathy, eosinophilia (often above 1.5 times 10 to the ninth per litre), atypical lymphocytes, and systemic involvement — hepatitis (the leading cause of death), interstitial nephritis, interstitial pneumonitis, myocarditis and reactivation of human herpesvirus 6. [1]
Diagnosis is by the RegiSCAR scoring system, which classifies cases as no, possible, probable or definite based on fever, rash, lymphadenopathy, organ involvement, eosinophilia and atypical lymphocytes [2].
Management: stop the culprit drug immediately. Systemic glucocorticoids (prednisolone 1 mg per kg daily, or intravenous methylprednisolone 0.5 to 1 mg per kg daily in severe disease) for any organ involvement, tapered slowly over weeks to months because relapse is common. Ciclosporin is used for severe or steroid-refractory cases. Monitor for viral reactivation (HHV-6, cytomegalovirus, Epstein-Barr virus). Re-exposure to the culprit drug causes a more rapid and severe recurrence — it is an absolute lifelong contraindication. [1]
Stevens-Johnson syndrome and toxic epidermal necrolysis
SJS and TEN are severe delayed T-cell reactions causing keratinocyte apoptosis and full-thickness epidermal necrosis with mucosal involvement. The classic culprits are allopurinol, anticonvulsants (carbamazepine, lamotrigine, phenytoin), sulfonamide antibiotics, nevirapine and NSAIDs (particularly oxicams). The HLA-B1502 allele confers high risk of carbamazepine-induced SJS in Han Chinese and Southeast Asian populations; HLA-B5801 confers high risk of allopurinol-induced SJS. [1]
Classification by body surface area (BSA) of detachment: SJS (under 10 per cent), SJS-TEN overlap (10 to 30 per cent), TEN (over 30 per cent). Mucosal involvement (oral, conjunctival, genital, tracheobronchial, urethral) is characteristic. [1]
SCORTEN is the prognostic score, calculated within 24 hours of admission. Each of the following scores one point: age over 40, malignancy, heart rate over 120 beats per minute, detached BSA over 10 per cent, serum urea over 10 mmol per litre, serum bicarbonate under 20 mmol per litre, serum glucose over 14 mmol per litre. Mortality rises from 3 per cent (score 0 to 1) to over 90 per cent (score 5 or more) [3].
Management: stop the culprit drug immediately. Admit to a burns unit or intensive care for detachment over 10 per cent. Supportive care — fluid and electrolyte management (the skin loss behaves like a burn), nutritional support, wound care, ophthalmology assessment (ocular adhesions and corneal ulceration are the leading long-term sequelae), and infection surveillance. The role of systemic glucocorticoids, intravenous immunoglobulin and ciclosporin is debated; no agent has proven mortality benefit in randomised trials. Re-exposure to the culprit drug is an absolute lifelong contraindication. [1]
Desensitisation — graded administration of an essential drug
When to desensitise

Desensitisation is the graded administration of escalating doses of a drug to induce a temporary state of clinical unresponsiveness. It is indicated when an essential drug has no satisfactory alternative and the prior reaction was immediate (IgE) or non-life-threatening. The classic indications: [1]
- Penicillin for syphilis in pregnancy — penicillin is the only recommended treatment and prevents congenital syphilis; desensitisation is justified because the disease is worse than the procedure.
- TMP-SMX for Pneumocystis prophylaxis in HIV — when alternatives (dapsone, atovaquone, aerosolised pentamidine) are inadequate or not tolerated.
- Aspirin in cardiovascular disease — when antiplatelet therapy is mandatory and no alternative (clopidogrel) is acceptable or sufficient.
- Platinum chemotherapy (carboplatin, cisplatin, oxaliplatin) — for ovarian and other cancers where the platinum is the most effective agent and hypersensitivity develops with repeated cycles.
- Monoclonal antibodies (rituximab, trastuzumab, cetuximab, infliximab) — for essential cancer or autoimmune therapy. [1]
The Brigham 12-step protocol
The standard protocol, developed by Castells at Brigham and Women's Hospital, uses three solutions of escalating concentration (solution 1 at a hundredth of the target, solution 2 at a tenth, solution 3 at the full target), each given in four doubling intravenous doses over approximately 15 minutes per step, reaching the target dose over approximately 6 hours [5][6]. The procedure is performed in a monitored setting with intravenous access, resuscitation equipment and a physician present. In the original series of 413 cases, 94 per cent of reactions during desensitisation were mild or absent, and the procedure was completed successfully in the vast majority [5].
If a reaction occurs, the infusion is stopped, the reaction treated (adrenaline if anaphylaxis, antihistamine and bronchodilator for milder reactions), and once symptoms resolve, the protocol resumes at the last tolerated dose or one step lower. Abandonment of the procedure is rare. [1]
The 48-hour rule — the critical pitfall
The tolerance induced by desensitisation is temporary. It is maintained only as long as the drug continues to be administered. If the drug is withheld for more than approximately 48 hours, tolerance is lost and a repeat full desensitisation is required before the next dose. This is the critical pitfall for chemotherapy patients on cyclical regimens — every cycle requires a repeat full desensitisation, because the gap between cycles exceeds 48 hours. Resuming the full dose after a gap without re-desensitisation can precipitate anaphylaxis. [1]
The mechanism of desensitisation is partly understood: it involves transient unresponsiveness of mast cells and basophils (mediator depletion, reduced IgE-Fc receptor signalling) and induction of regulatory T cells. The clinical correlate is that the state is dose-dependent, temporary, and re-inducible. [1]
Absolute contraindications to desensitisation
Desensitisation is never performed after: [1]
- Stevens-Johnson syndrome or toxic epidermal necrolysis — re-exposure causes a more severe recurrence and is potentially fatal.
- DRESS — re-exposure causes a rapid and severe recurrence.
- Drug-induced immune haemolytic anaemia or other severe cytotoxic (type II) reactions.
- Severe serum sickness. [1]
These are absolute lifelong contraindications to the culprit drug and to structurally related drugs. [1]
Drug provocation testing — the diagnostic gold standard
Drug provocation testing (DPT) — a graded oral or parenteral challenge with the suspected drug under supervised monitoring — is the gold standard for diagnosing drug allergy. The 2022 practice parameter positions DPT as the preferred confirmatory test for most non-severe, non-immediate reactions, increasingly over skin testing [1]. A negative DPT allows delabeling; a positive DPT confirms the diagnosis and the contraindication.
DPT is performed in a monitored setting with resuscitation equipment available. It is contraindicated in patients with a history of SJS, TEN, DRESS, severe serum sickness or severe immediate anaphylaxis — for these patients, the history alone establishes the contraindication. [1]
Immediate management — anaphylaxis
Anaphylaxis is the acute life-threatening complication of an IgE drug reaction. The management is: [1]
- Stop the drug and remove the trigger.
- Intramuscular adrenaline 0.5 mg (0.5 mL of 1:1000, which is 1 mg per mL) into the anterolateral thigh — repeat every 3 to 5 minutes as needed. Never give intravenous adrenaline 1:1000 undiluted; intravenous adrenaline is reserved for cardiac arrest using the dilute 1:10 000 preparation. [1]3. Supine positioning with legs raised — do not sit or stand the patient up suddenly, as this causes empty-vena-cava arrest.
- High-flow oxygen and intravenous crystalloid (1 to 2 litres rapidly) for hypotension.
- Adjuncts — H1 antihistamine (chlorphenamine), H2 antihistamine, intravenous hydrocortisone 200 mg — these do not treat the airway or circulation and are not substitutes for adrenaline.
- Observe for a biphasic reaction for at least 6 to 12 hours, because a second wave of anaphylaxis can occur without re-exposure.
- On discharge — provide an adrenaline autoinjector (EpiPen), a written anaphylaxis action plan, referral to an allergy specialist, and clear documentation of the culprit drug. [1]
Examiner trap: Intramuscular adrenaline into the anterolateral thigh is first-line for anaphylaxis. Intravenous adrenaline 1:1000 undiluted is dangerous and is reserved for cardiac arrest using the dilute 1:10 000 preparation. Do not delay adrenaline for antihistamines or hydrocortisone. [1]
The long-case synthesis
A classic long case for this topic is a patient with a long-standing penicillin allergy label admitted with an infection for which a beta-lactam is first-line — endocarditis (penicillin or ceftriaxone), meningitis (ceftriaxone), pyelonephritis in pregnancy (cephalexin or ceftriaxone), or syphilis in pregnancy (penicillin). The task is to refine the label, assess the risk, and decide among a non-cross-reactive beta-lactam, skin testing, drug provocation challenge and desensitisation. [1]
The opening statement (SASPOP): "Mrs AB is a 32-year-old primigravida at 24 weeks gestation presenting with secondary syphilis (rash and positive syphilis serology), with a penicillin allergy label from a childhood rash of uncertain nature. Her problem list is: (1) secondary syphilis in pregnancy requiring benzathine penicillin, the only recommended treatment to prevent congenital syphilis; (2) a penicillin allergy label of low certainty, requiring risk stratification and delabeling or desensitisation; (3) the pregnancy, which raises the stakes of both untreated syphilis and of desensitisation; (4) the risk of congenital syphilis; (5) the communication and documentation needs across obstetrics, microbiology and allergy." [1]
The management plan: take a structured allergy history. If the childhood reaction was non-severe and remote, risk-stratify as low-moderate and proceed to penicillin skin testing followed by an oral amoxicillin challenge to delabel — if negative, give benzathine penicillin. If the reaction history is more concerning or testing is positive, desensitise with graded penicillin in a monitored setting, because untreated syphilis in pregnancy causes congenital syphilis and penicillin is the only effective treatment [1].
Show insight into the patient perspective: the anxiety of a supervised challenge in pregnancy, the relief of a removed label, the implications for future antibiotic choices, and the importance of accurate documentation to prevent re-application of an obsolete label by another clinician. [1]
Key exam traps
- Never treat a penicillin allergy label as a permanent contraindication. Most labels are false or have been outgrown. Risk-stratify and delabel proactively.
- The 10 per cent penicillin-cephalosporin cross-reactivity figure is wrong. The modern figure is 1 to 2 per cent overall and near zero for dissimilar R1 side chains.
- Never desensitise after SJS, TEN or DRESS. These are absolute lifelong contraindications.
- Desensitisation tolerance is temporary. It is lost if the drug is withheld for more than 48 hours; every chemotherapy cycle requires a repeat full desensitisation.
- Vancomycin red man syndrome is not allergy. It is rate-dependent histamine release managed by slow infusion, not vancomycin avoidance. [1]- Sulfonamide antibiotics do not cross-react with non-antibiotic sulfonamides. Frusemide and thiazides are safe unless there is a specific reaction.
- Radiocontrast reactions are not related to iodine or seafood allergy. The mechanism is mast cell histamine release.
- Intramuscular adrenaline into the anterolateral thigh is first-line for anaphylaxis, not intravenous adrenaline 1:1000, and not antihistamines or hydrocortisone. [1]
Regional and guideline notes
ANZ primary: Therapeutic Guidelines Australia (eTG) Antibiotic and Allergy sections provide the antibiotic selection framework for penicillin-allergic patients and the referral pathway to drug allergy clinics. The Australasian Society of Clinical Immunology and Allergy (ASCIA) publishes the ANZ guidance on drug allergy, anaphylaxis and adrenaline autoinjectors. [1]
UK secondary: NICE Clinical Guideline CG183 (Drug allergy: diagnosis and management) provides the UK framework, emphasising structured history, referral for specialist testing and structured documentation. [1]
US tertiary: The 2022 Drug Allergy Practice Parameter Update (Joint Task Force on Practice Parameters, AAAAI and ACAAI) is the authoritative US guideline for risk-stratified delabeling, drug provocation testing, cross-reactivity and desensitisation [1].
Global: The International Consensus (ICON) on drug allergy provides the global framework for classification, diagnosis and management [7].
References and further reading
Khan 2022 Drug Allergy Practice Parameter Update (J Allergy Clin Immunol, 36122788) [1]; Kardaun 2013 RegiSCAR diagnostic scoring for DRESS (Br J Dermatol, 23855313) [2]; Bastuji-Garin 2000 SCORTEN for toxic epidermal necrolysis (J Invest Dermatol, 10951229) [3]; Miranda da Cruz and Rieder 2018 Cross-reactivity in beta-lactam allergy (J Allergy Clin Immunol Pract, 29017833) [4]; Castells 2008 outcomes and safety of rapid desensitisation in 413 cases (J Allergy Clin Immunol, 18502492) [5]; Castells 2014 rapid drug desensitisation review (J Investig Allergol Clin Immunol, 24834769) [6]; Demoly 2014 International Consensus on drug allergy (Allergy, 24697291) [7].
References
- [1]Khan DA, Banerji A, Blumenthal KG, et al. Drug allergy: A 2022 practice parameter update J Allergy Clin Immunol, 2022.PMID 36122788
- [2]Kardaun SH, Sekula P, Valeyrie-Allanore L, et al. Drug reaction with eosinophilia and systemic symptoms (DRESS): an original multisystem adverse drug reaction. Results from the prospective RegiSCAR study Br J Dermatol, 2013.PMID 23855313
- [3]Bastuji-Garin S, Fouchard N, Bertocchi M, et al. SCORTEN: a severity-of-illness score for toxic epidermal necrolysis J Invest Dermatol, 2000.PMID 10951229
- [4]Miranda da Cruz BN, Rieder MJ Cross-reactivity in β-Lactam Allergy J Allergy Clin Immunol Pract, 2018.PMID 29017833
- [5]Castells MC, Tennant NM, Sloane DE, et al. Hypersensitivity reactions to chemotherapy: outcomes and safety of rapid desensitization in 413 cases J Allergy Clin Immunol, 2008.PMID 18502492
- [6]Castells MC Rapid drug desensitization for hypersensitivity reactions to chemotherapy and monoclonal antibodies in the 21st century J Investig Allergol Clin Immunol, 2014.PMID 24834769
- [7]Demoly P, Adkinson NF, Brockow K, et al. International Consensus on drug allergy Allergy, 2014.PMID 24697291