Phys · general-medicine
END OF Life Decision Making
Also known as END OF Life Decision Making · end of life decision making
Consultant-physician depth guide to END OF Life Decision Making for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
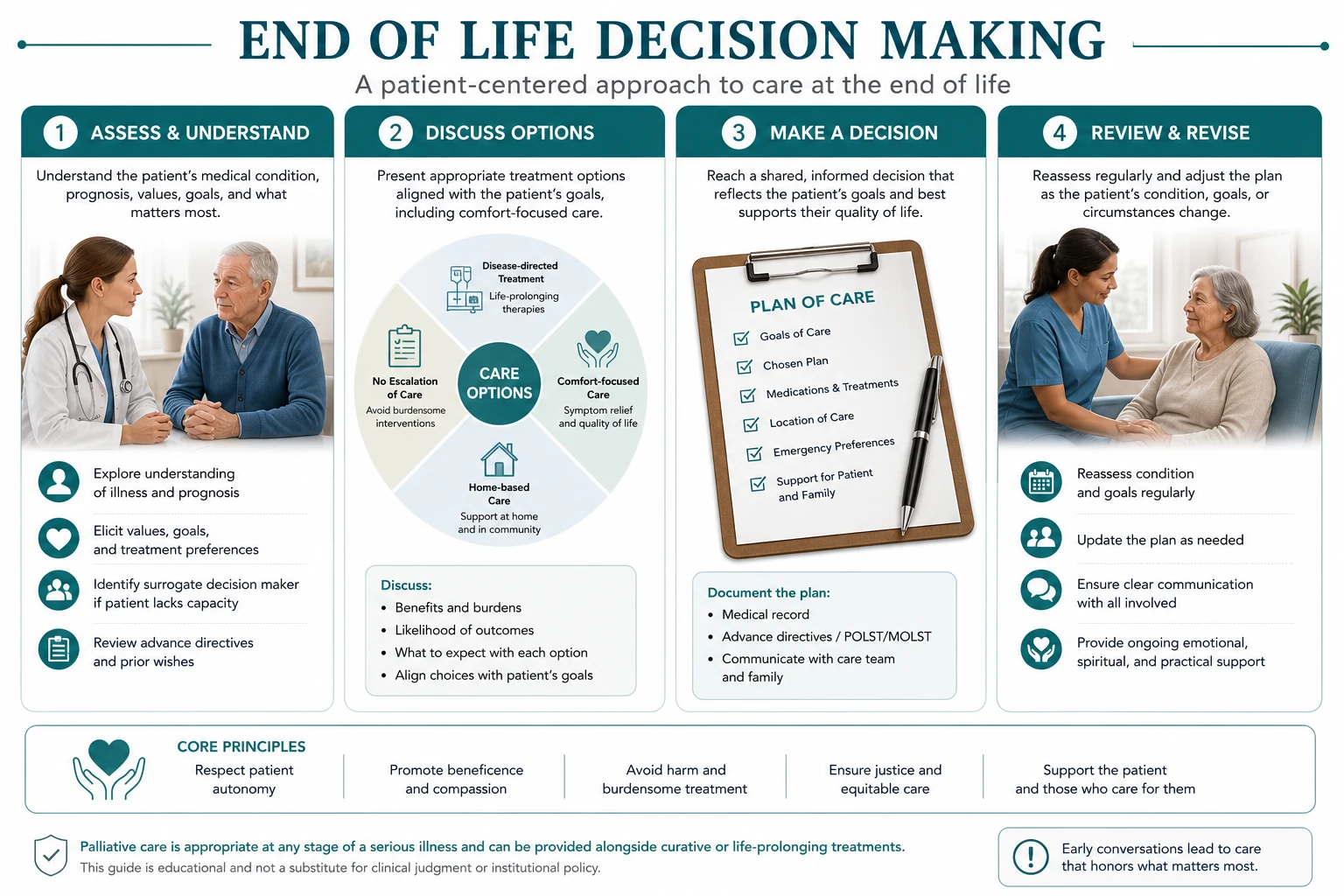
END OF Life Decision Making is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
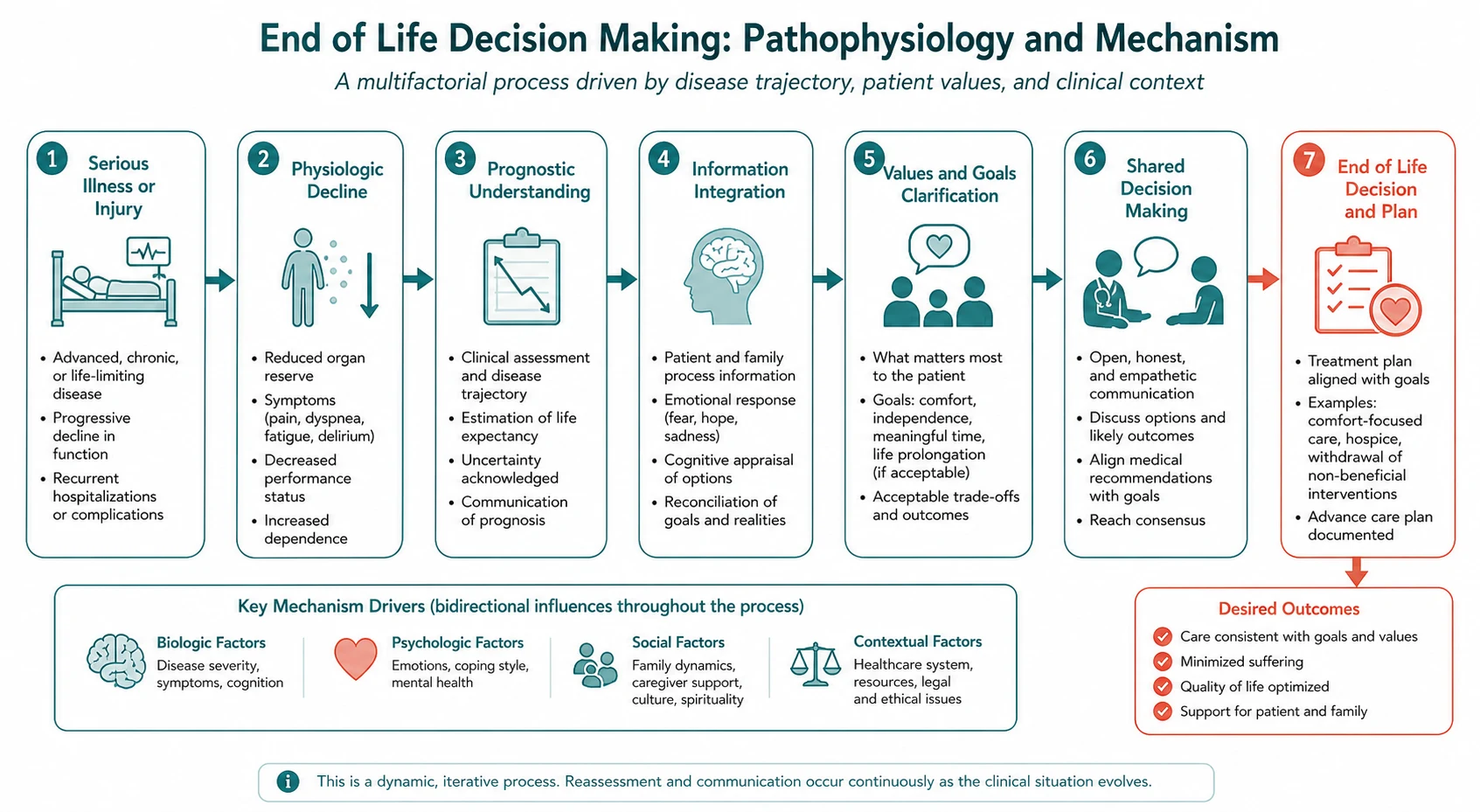
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
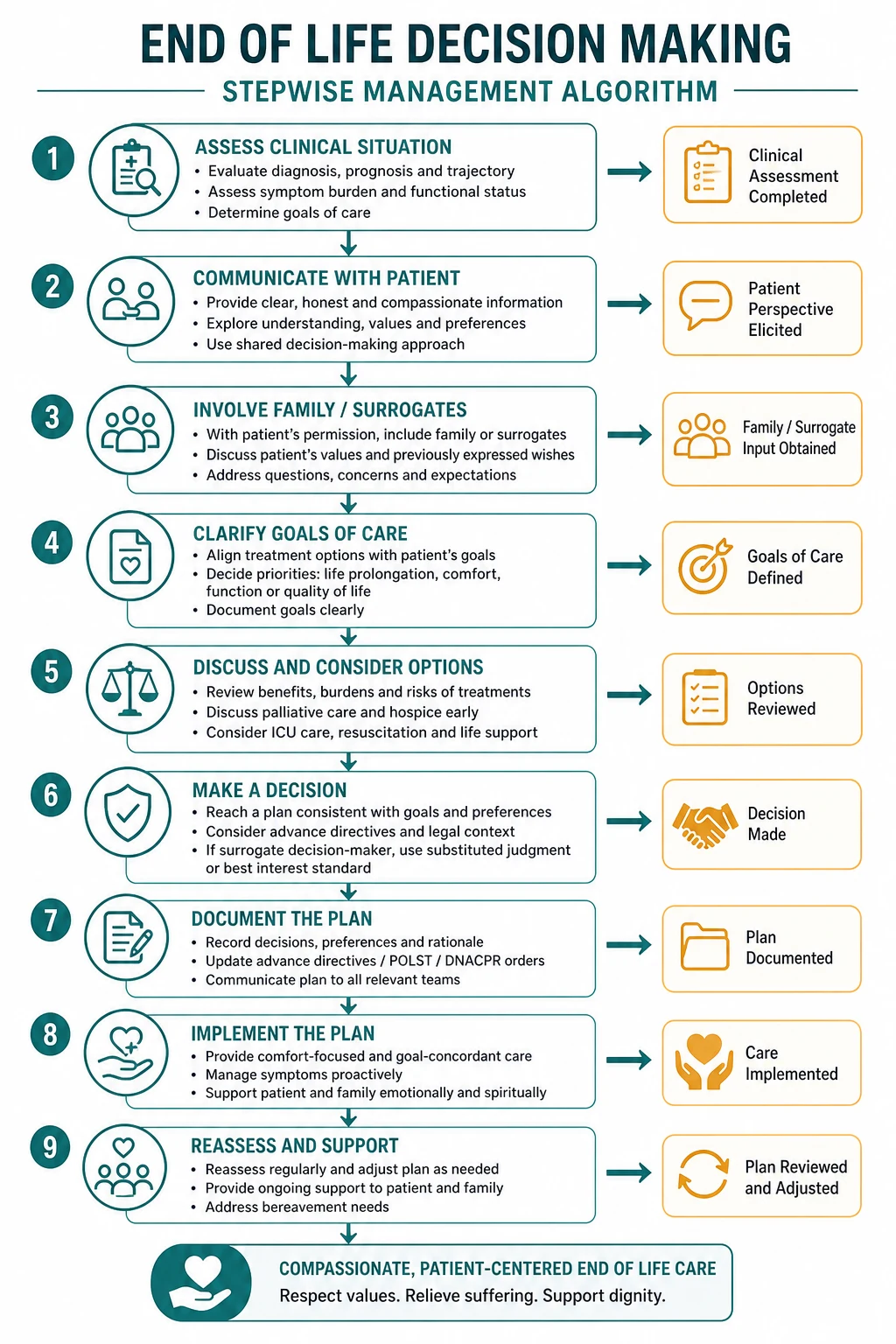
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]
Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link END OF Life Decision Making to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Bolton P, White BP, Huppert J, Dadich A Assisted Dying Makes Us Think Differently About Care Health Expect, 2026.PMID 42460812
- [2]Bergen K, Bouwmans P, van Oevelen M, Avesani CM, et al. Deciding between conservative kidney management and dialysis in older people with kidney failure: a narrative review Clin Kidney J, 2026.PMID 42459744
- [3]Hoftiezer L, Hof MHP, van Lingen RA, Hukkelhoven CWPM, et al. Beyond cut-offs: gestational age-specific perinatal mortality across the birthweight-for-gestational-age continuum-a population-based cross-sectional study Eur J Pediatr, 2026.PMID 42458127
- [4]Aljohar A, Williamson MD, Mitchell RA, Roston TM, et al. Arrhythmogenic Right Ventricular Cardiomyopathy in Athletes: The Importance of Shared Decision-Making and an Individualized Approach JACC Case Rep, 2026.PMID 42460947
- [5]Genoud A, Portugal I, Murith N, Deux JF, et al. Coronary Artery Anomalies Revisited: Description of the Types, Pathophysiology and Treatment Options Based on Latest Guidelines J Clin Med, 2026.PMID 42452422
- [6]Shah V, Constantin K, Taddio A, McMurtry CM, et al. A Systematic Review and Meta-Analysis of the Effectiveness of Physical Interventions Administered Orally for Infants for Reducing Distress During Vaccine Injections Clin J Pain, 2026.PMID 42444178
- [7]Doan HN, Chang MC Comparative Effectiveness of Unstable Versus Stable Resistance Training on Lower Limb Strength, Mobility, and Fear of Falling in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials Am J Phys Med Rehabil, 2026.PMID 42468010
- [8]Liu HW, Tsai TL Virtual Reality-assisted Physiotherapeutic Training for Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis Am J Phys Med Rehabil, 2026.PMID 42468005
- [9]Osborne AK, Brown RD, Sillence E Effects of Social Media Narratives on Affective and Behavioral Responses to Menopause Content: Randomized Online Experimental Study JMIR Form Res, 2026.PMID 42467962
- [10]Diaz SD, Picart JK, Dualeh S, Aubry ST, et al. Impact of vehicular data on trauma outcomes after motor vehicle crashes Trauma Surg Acute Care Open, 2026.PMID 42465198
- [11]Tayon KG, Vardar U, Dineen EH, Shapiro BP, et al. Multimodality Risk Stratification in Athletes With Long QT Syndrome JACC Case Rep, 2026.PMID 42460964
- [12]Fischer SM, Fink RM, Alasmar AY, Campbell EG, et al. Palliative Care Physicians' Perceptions about Using Artificial Intelligence for Prognostication J Pain Symptom Manage, 2026.PMID 42463061