Phys · general-medicine
Lymph Node Examination and Organomegaly — The DCE Short-Case Systematic Approach
Also known as lymph node examination · examination of lymph nodes · examine this patient's lymph nodes · lymphadenopathy examination · cervical lymph node examination · axillary lymph node examination · inguinal lymph node examination · epitrochlear lymph node · Virchow node · Troisier sign · supraclavicular lymph node · splenomegaly examination · examine for organomegaly · hepatosplenomegaly examination · spleen versus kidney · massive splenomegaly · liver span · hepatomegaly examination · grading of splenomegaly · rubbery lymph node
Consultant-physician-depth guide to the systematic examination of lymph nodes and organomegaly (splenomegaly and hepatomegaly) for the DCE short case and MRCP PACES. Covers the reproducible head-to-toe lymph node routine (head and neck, axillary, epitrochlear, inguinal, popliteal), the five characteristics of every palpable node (size, consistency, mobility, tenderness, overlying skin), the interpretation of node consistency (soft reactive, firm lymphoma, rubbery Hodgkin, hard metastatic, matted TB or lymphoma), the significance of the Virchow node, the correct technique for splenomegaly (start in the right iliac fossa, move diagonally toward the left costal margin along the tenth rib, left hand behind the ribs to lift the spleen forward), the differentiation of spleen from kidney (cannot get above, dull to percussion, notch, moves with respiration), the grading of splenomegaly and the causes of massive splenomegaly (CML, myelofibrosis, chronic malaria, visceral leishmaniasis, Gaucher disease), the examination and description of hepatomegaly, the standard oral presentation template, and the discussion questions the examiner will ask. Structured for FRACP DCE and MRCP PACES. Every sign is referenced to the JAMA Rational Clinical Examination series and the foundational lymphadenopathy reviews.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Lymph Node Examination and Organomegaly — The DCE Short-Case Systematic Approach

The answer first
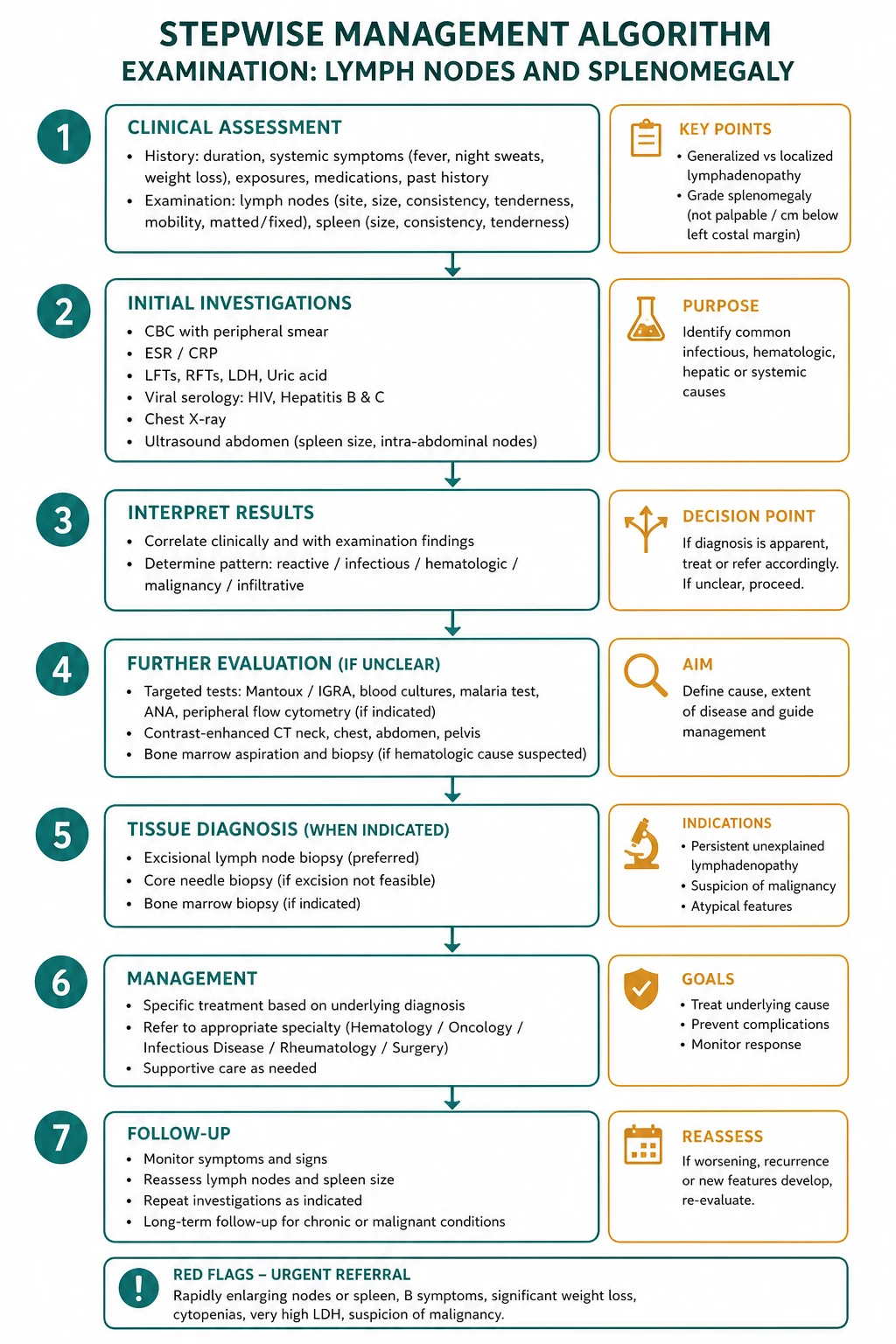
The instruction in the DCE short case is always one of two sentences: "Please examine this patient's lymph nodes," or "Examine this patient for organomegaly." Both are high-yield, frequently tested short cases, and they are inseparable — the candidate who finds a Virchow node is duty-bound to examine the abdomen, and the candidate who finds massive splenomegaly is duty-bound to examine the node fields. The candidate who performs a fluent, complete, reproducible routine across every node region, describes each node by its five characteristics, grades the splenomegaly, differentiates the spleen from the kidney at the bedside, and presents in a structured two-minute format passes. The candidate who omits node groups, who fails to describe consistency, or who cannot tell a spleen from a kidney has already failed regardless of what they find. [1]
The reproducible sequence has two halves. First, the lymph node examination, performed head to toe: head and neck nodes, then axillary, then epitrochlear, then inguinal, then popliteal. Second, the abdominal examination for organomegaly, focused on the spleen, the liver, and the kidneys. The hands and face are examined at the start of both halves, because the stigmata of haematological malignancy (pallor, bruising, petechiae), chronic liver disease (palmar erythema, spider naevi), and infection (clubbing, stigmata of infective endocarditis) frame the differential before a single node is touched. [1]

DCE high-yield: The three most commonly tested lymph node and organomegaly short-case scenarios are (1) generalised lymphadenopathy from lymphoma, where the candidate must find nodes in at least two regions and describe the rubbery consistency; (2) the Virchow node, where a single hard left supraclavicular node signals gastric cancer and the candidate must then examine the abdomen; and (3) massive splenomegaly, where the candidate must differentiate the spleen from the kidney, grade it as massive, and generate the narrow differential of CML, myelofibrosis, chronic malaria, visceral leishmaniasis, and Gaucher disease. [1]
Setting up — before you touch the patient
Introduce yourself, confirm the patient's identity, explain what you are going to do, and request permission. Position the patient sitting upright at 45 degrees for the head and neck nodes, then lying supine with one pillow for the axillary, epitrochlear, inguinal, and abdominal examination. Expose the relevant regions with dignity — neck and supraclavicular fossae for the cervical chain, the upper limbs and axillae for the axillary nodes, and the abdomen from xiphisternum to symphysis pubis for the organomegaly examination. Ensure good lighting, warm your hands, and stand on the patient's right side for the abdominal examination. [1]
End-of-bed observations. Before you palpate a single node, observe the patient for thirty seconds. Look for cachexia (malignancy, chronic infection, advanced HIV), pallor (anaemia from marrow infiltration, haemolysis, or chronic disease), jaundice (haemolysis, hepatic infiltration), and the body habitus. Note the breathing pattern, and observe the bedside clues — the medication chart (chemotherapy, antiretrovirals, steroids), the IV pole, and the walking frame. [1]
DCE high-yield: The pallor–massive-splenomegaly combination is a near-pathognomonic short-case vignette. A pale patient with a spleen crossing the midline has a myeloproliferative neoplasm until proven otherwise — reach for the blood film and the BCR-ABL and JAK2 tests. Name this combination aloud when you present. [1]
Part one — the lymph node examination
Examine the nodes in a fixed, reproducible order so that you never omit a region. The sequence is: head and neck, then axillary, then epitrochlear, then inguinal, then popliteal. Examine the nodes from in front of the patient for the head and neck, from behind for the posterior neck and supraclavicular fossae, then return to the patient's right side for the axillary, epitrochlear, inguinal, and popliteal nodes. [1]
Step 1 — The head and neck nodes
Palpate the head and neck nodes systematically using the pads of your index and middle fingers, with the patient's neck slightly flexed and relaxed. Work in a fixed order so no group is missed: submental, submandibular, pre-auricular, post-auricular, occipital, tonsillar (jugulodigastric), anterior cervical chain, posterior cervical chain, supraclavicular, pre-tracheal. [1]
Submental and submandibular. Palpate under the chin in the submental triangle (between the two anterior bellies of the digastric), then the submandibular region along the body of the mandible. These drain the floor of the mouth, the tongue, the lips, and the teeth — enlargement points to infection or malignancy of the oral cavity. [1]
Pre-auricular and post-auricular. Palpate in front of the tragus (pre-auricular, draining the scalp, external ear, and conjunctiva) and behind the ear over the mastoid process (post-auricular, draining the scalp and ear). Pre-auricular adenopathy with conjunctivitis is the oculoglandular syndrome of cat-scratch disease (Parinaud syndrome). [1]
Occipital. Palpate at the base of the skull posteriorly, draining the posterior scalp. Occipital adenopathy is common in scalp infections (tinea capitis, pediculosis) and in rubella. [1]
Tonsillar (jugulodigastric). Palpate just below the angle of the mandible, beneath the anterior border of sternocleidomastoid. This is the largest node of the head and neck and is the most common site of reactive cervical adenopathy (tonsillitis, pharyngitis). A unilateral enlarged tonsillar node in an older adult with a smoking history raises head and neck squamous cell carcinoma. [1]
Anterior cervical chain. Palpate along the anterior border of sternocleidomastoid, from the mastoid down to the clavicle. Divide the chain into upper, middle, and lower. These nodes drain the throat, the thyroid, and the deep structures of the neck. [1]
Posterior cervical chain. Palpate along the posterior border of sternocleidomastoid, in the posterior triangle. Posterior cervical adenopathy is a feature of infectious mononucleosis, toxoplasmosis, and lymphoma. [1]
Supraclavicular (Virchow node — the most important node in the body). Examine the supraclavicular fossae from behind the patient, with the patient's neck flexed forward and the shoulders relaxed (ask the patient to shrug the shoulders and let them drop, or to take a deep breath in and let it out — this relaxes the sternocleidomastoid and the scalenes). Place your fingers deep into the angle between the clavicle and the sternocleidomastoid, on each side, and press firmly but gently downward and inward. [1]
Pre-tracheal and paratracheal. Palpate in the midline over the trachea and just lateral to it. These deep nodes drain the trachea, the thyroid, and the larynx, and are usually only felt when significantly enlarged. [1]
Step 2 — The axillary nodes
The axillary nodes are examined with the patient sitting or lying, and are best approached from the front. There are five groups, and the candidate who names all five demonstrates anatomical fluency. [1]
Support the patient's right arm with your left hand (for the right axilla) so that the axillary muscles are relaxed, and place your right hand high into the apex of the axilla, with the fingertips pointing toward the clavicle. Press the fingertips against the chest wall and draw them downward through the axilla, feeling for nodes against the ribs. Repeat for the left axilla with hands reversed. Examine each of the five groups: [1]
- Apical (infraclavicular). High in the axillary apex, near the clavicle. These receive lymph from all the other axillary groups.
- Anterior (pectoral). Along the lower border of pectoralis major, on the anterior axillary fold. These drain the anterior chest wall and the breast — the most common site of breast cancer metastasis.
- Posterior (subscapular). Along the posterior axillary fold, on the subscapularis. These drain the posterior chest wall and the upper back.
- Lateral (humeral). Along the upper humerus, in the groove between biceps and triceps. These drain the upper limb and are the nodes that drain into the apical group.
- Central. In the fat of the axillary floor, the most commonly palpable group. These receive lymph from the anterior, posterior, and lateral groups. [1]
Axillary adenopathy raises breast cancer (unilateral, hard), lymphoma (bilateral, rubbery), melanoma (from a upper limb or truncal primary), and infection of the hand or arm. Always examine the ipsilateral breast, the upper limb, and the back when you find an axillary node. [1]
Step 3 — The epitrochlear nodes
The epitrochlear node is examined by cupping the patient's elbow in your hand and palpating with the thumb or fingers in the groove above and 3 cm proximal to the medial epicondyle of the humerus, between the biceps and triceps. The patient's elbow should be flexed to about 90 degrees and slightly supinated. [1]
Step 4 — The inguinal nodes
Examine the inguinal nodes with the patient supine, the hip slightly flexed and externally rotated. Palpate along the inguinal ligament (the horizontal group) and along the saphenous vein in the upper medial thigh (the vertical group). The horizontal group drains the skin of the lower anterior abdominal wall, the external genitalia, the perineum, the gluteal region, and the lower anal canal. The vertical group drains the lower limb. [1]
Step 5 — The popliteal nodes
The popliteal node is the most commonly omitted node in the short case. With the patient's knee slightly flexed, palpate deeply in the popliteal fossa behind the knee. The popliteal node drains the lateral leg and foot. Enlargement is uncommon but points to infection or malignancy of the distal lower limb. [1]
Describing a lymph node — the five characteristics
When you palpate a node, describe it by five characteristics, every time. A node described only as "enlarged" earns no marks. The five characteristics are: [1]
- Site — name the anatomical group precisely (for example, "the left supraclavicular fossa," not just "the neck"). State the distribution: is the adenopathy localised (one region) or generalised (two or more non-contiguous regions)? This distinction changes the entire differential.
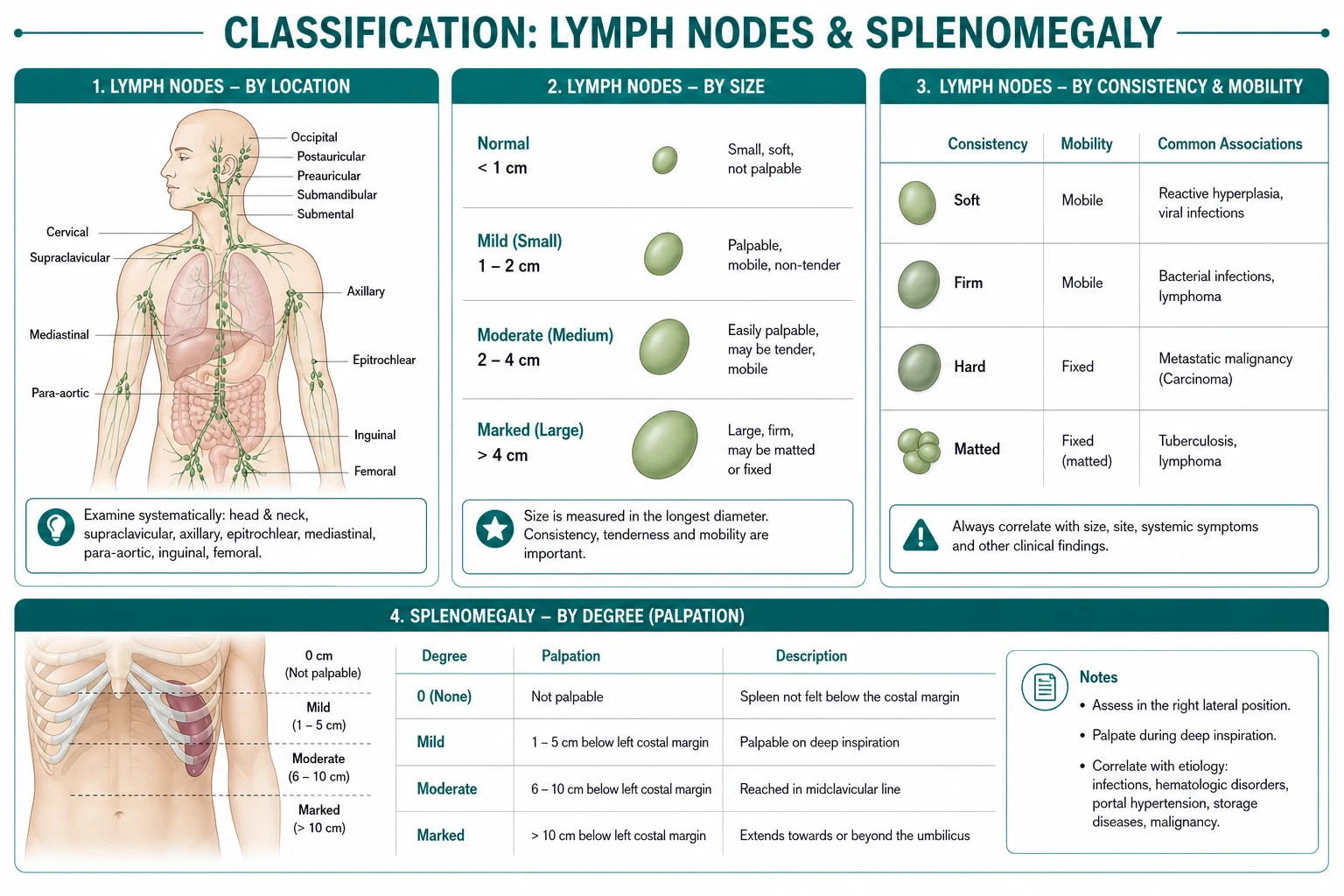
- Size — measure in centimetres. Nodes over 1 cm in diameter are generally considered abnormal, except for the inguinal nodes (where up to 1 to 2 cm may be normal). A node over 2 cm in any region, or any supraclavicular node, warrants investigation.
- Consistency — the single most discriminating characteristic. Describe it precisely:
- Soft — like a lip or a well-filled water balloon. Reactive or infective.
- Firm — like the tip of the nose. Lymphoma (non-Hodgkin), chronic lymphocytic leukaemia, granulomatous disease.
- Rubbery — like a piece of india rubber, dense but slightly bouncy. The classic consistency of Hodgkin lymphoma.
- Hard — like bone or stone. Metastatic malignancy (squamous cell carcinoma, adenocarcinoma).
- Matted — nodes fused together into a confluent mass. Tuberculosis (caseating nodes) or advanced lymphoma.
- Mobility and matting — mobile (freely movable against the skin and deep structures — benign or early malignancy), matted (fixed to each other — TB or lymphoma), or fixed (tethered to skin or deep structures — advanced malignancy with invasion). Fixity to the skin suggests breast or head and neck SCC; fixity to deep structures suggests advanced malignancy.
- Tenderness and the overlying skin — tender nodes indicate rapid capsular stretching, almost always from infection or inflammation (but also from rapid haemorrhage into a node, as in lymphoma). Non-tender nodes suggest chronic or malignant disease. Examine the overlying skin for erythema, warmth, sinus tract (scrofuloderma of TB), ulceration, and fixation. [1]
Part two — the abdominal examination for organomegaly
After the lymph node examination, examine the abdomen for organomegaly — the spleen, the liver, and the kidneys. The instruction "examine for organomegaly" is itself a complete short case. Position the patient supine with one pillow, arms at the sides, exposed from xiphisternum to symphysis pubis, and kneel or sit so your examining hand is at the level of the abdomen. [1]

Examination of the spleen
The spleen is examined from the right side of the patient. The key principles are: start in the right iliac fossa, move diagonally toward the left costal margin along the line of the tenth rib, use your left hand behind the lower ribs to lift the spleen forward, and ask the patient to breathe in deeply. [1]
The technique. Place your right hand flat in the right iliac fossa, lateral to the rectus, with the fingers pointing diagonally toward the left costal margin. Place your left hand behind the lower left ribs, over the lower costal margin and the renal angle, and pull forward gently — this splints the lower ribs and lifts the spleen toward your examining right hand. Ask the patient to breathe in slowly and deeply through the mouth. As the diaphragm descends on inspiration, the spleen is pushed downward and medially toward your right hand. Move your right hand progressively — one or two centimetres per inspiration — diagonally toward the left costal margin along the line of the tenth rib (the long axis of the spleen, which lies along ribs 9 to 11). When the spleen is enlarged, you feel the splenic edge descend and tap your fingertips on inspiration, then retreat on expiration. [1]
Why diagonally, and why from the right? The spleen enlarges along its long axis, which runs diagonally from the left upper quadrant toward the right iliac fossa, parallel to the tenth rib. Starting in the right iliac fossa and moving diagonally ensures you meet the descending splenic edge as it crosses your hand. Examining from the right side allows you to use the bimanual technique with the left hand splinting the ribs. [1]
The right lateral decubitus position. If the spleen is not palpable supine, roll the patient onto their right side (right lateral decubitus), support the lower ribs with your left hand, and palpate again. This brings the spleen closer to the abdominal wall by gravity and is the position that maximises sensitivity — a spleen just below the costal margin may be felt only in this position. [1]
Percussion aids. Two percussion signs increase the sensitivity for splenomegaly when the spleen is not palpable. Castell sign: percuss in the lowest intercostal space in the left anterior axillary line (normally tympanic from the splenic flexure of the colon); dullness on inspiration or in the right lateral decubitus position suggests splenomegaly. Traube space: the triangular area of tympany over the left lower anterior chest (bounded by the sixth rib superiorly, the midaxillary line laterally, and the costal margin inferiorly); dullness in a fasting patient suggests splenomegaly. Both are imperfect — Traube space is unreliable if the patient has eaten or has a left pleural effusion. The Grover systematic review of splenomegaly examination found that clinical palpation has moderate sensitivity and that a non-palpable spleen does not exclude splenomegaly, particularly in obese patients; imaging is required when splenomegaly is clinically suspected but not palpable [1].
Spleen versus kidney — the three differentiators
This is one of the most commonly tested distinctions in the DCE. The spleen and the left kidney both present as a left upper quadrant mass, but they are differentiated by three features, each of which you must be able to state aloud: [1]
Grading of splenomegaly
Once you confirm a mass is the spleen, grade the splenomegaly — the grade changes the differential: [1]
- Mild splenomegaly (just palpable, up to a few centimetres below the costal margin). Causes: portal hypertension from any chronic liver disease, acute and chronic infection (infectious mononucleosis, viral hepatitis, bacterial endocarditis, malaria, typhoid), haemolytic anaemia (hereditary spherocytosis, autoimmune haemolytic anaemia), congestive (right heart failure, Budd-Chiari), and early lymphoma or leukaemia.
- Moderate splenomegaly (palpable well below the costal margin, extending toward the umbilicus). Causes: the above plus lymphoma, chronic myeloid leukaemia, chronic lymphocytic leukaemia, myelofibrosis, thalassaemia major, and chronic infection (malaria, brucellosis, kala-azar).
- Massive splenomegaly (extending beyond the umbilicus into the right iliac fossa, crossing the midline). The differential narrows dramatically: [1]

Examination of the liver
The liver is examined from the patient's right side. The technique mirrors the spleen but on the right. [1]
Palpation. Place your right hand flat in the right iliac fossa, lateral to the rectus, with the fingers pointing toward the right costal margin. Ask the patient to breathe in slowly and deeply. As the diaphragm descends, the liver edge is pushed downward toward your hand. Move your hand progressively upward — one centimetre per inspiration — toward the costal margin until you feel the liver edge slip under your fingertips. With your left hand, you may splint the lower right ribs from behind to bring the liver forward (the bimanual technique). [1]
Describing the liver — four characteristics. When you palpate the liver, describe four things: [1]
- Size. State the number of centimetres the liver edge is palpable below the right costal margin in the midclavicular line on inspiration. Then estimate the liver span by percussion — percuss downward from the right third intercostal space in the midclavicular line until the note changes from resonant (lung) to dull (the upper liver border), and percuss upward from below the costal margin until the note changes from tympanic (bowel) to dull (the lower liver border). The distance between the two is the liver span; a normal span is 12 to 15 cm in the midclavicular line. A span greater than 15 cm suggests hepatomegaly; a span less than 10 cm suggests a small liver (cirrhosis).
- Surface. Smooth (normal, or acute hepatitis, or congestion), hard and nodular (cirrhosis or metastases), or irregular and rock-hard (metastatic malignancy).
- Edge. Sharp and smooth (normal), rounded (fatty liver, congestion), or hard and irregular (cirrhosis, metastases).
- Tenderness. A tender liver indicates capsular stretching — acute hepatitis, hepatic congestion from right heart failure, or a rapidly enlarging liver from malignancy. [1]
Examination of the kidneys
The kidneys are examined by ballottement. Place your left hand in the right renal angle (the costovertebral angle, posteriorly) and your right hand anteriorly in the right upper quadrant. Ask the patient to breathe out, then push the posterior hand sharply upward — the right kidney, if enlarged, flicks between your two hands. Repeat on the left with hands reversed. A ballotable kidney feels like a firm mass that moves between the hands. [1]
The differentiators from the spleen (for the left kidney) are as above: you can get above a kidney, it is resonant to percussion, it has no notch, and it can be ballotted. A palpable right kidney may be normal in thin individuals; a palpable left kidney is always abnormal and suggests polycystic kidney disease, hydronephrosis, or renal cell carcinoma. [1]
The presentation template
After completing the examination, present your findings in a structured two-minute summary. The examiner is assessing not only what you found but how you organise and present it. [1]

The structure is: [1]
- Opening statement — who, what, the overall impression, and whether the adenopathy is localised or generalised.
- The lymph node findings — state the distribution (localised or generalised), then each positive region with the five characteristics (site, size, consistency, mobility, tenderness and overlying skin). State the relevant negatives (for example, "no Virchow node," "no hepatosplenomegaly" if relevant).
- The organomegaly findings — if the spleen is enlarged, name the grade (mild, moderate, massive) and state that you cannot get above it and it is dull to percussion with a notch. If the liver is enlarged, state the span, surface, and edge.
- Relevant negatives — the nodes you examined and found normal, the absence of stigmata of chronic liver disease, the absence of B symptoms.
- Provisional diagnosis with differential — lead with the most likely diagnosis, then the alternatives, and the investigation you would do next. [1]
Model presentation — generalised lymphadenopathy (lymphoma): "I examined Mr David K's lymph nodes. At the end of the bed, the patient is pale but not cachectic or jaundiced. There is generalised lymphadenopathy. In the neck, there are bilateral, rubbery, mobile, non-tender nodes in the anterior and posterior cervical chains, the largest 2 by 2 centimetres, with a similar node in the left supraclavicular fossa that is rubbery rather than hard and therefore more likely lymphoma than a Virchow node from carcinoma. In both axillae, there are matted, firm, mobile masses up to 3 centimetres. The epitrochlear nodes are palpable bilaterally. The inguinal nodes are small, mobile, and shotty — consistent with reactive change. In the abdomen, the spleen is palpable 6 centimetres below the left costal margin, smooth, with a notch — I cannot get above it, and it is dull to percussion, confirming it is the spleen; this is moderate splenomegaly. The liver is not enlarged, with a percussion span of 13 centimetres. There is no pallor-dependent stigmata of chronic liver disease. My findings are of generalised lymphadenopathy with moderate splenomegaly. The most likely diagnosis is lymphoma — the rubbery consistency, the generalised distribution, the epitrochlear involvement, and the splenomegaly all support this. I would also consider chronic lymphocytic leukaemia, HIV-related lymphadenopathy, and infectious mononucleosis. I would investigate with a full blood count and film, a lactate dehydrogenase, an HIV test, EBV serology, and an excisional biopsy of the most abnormal node for histology, flow cytometry, and immunohistochemistry, followed by a staging CT and a PET scan." [1]
Model presentation — Virchow node (gastric cancer): "I examined Mrs Anne L's lymph nodes. At the end of the bed, the patient is cachectic and pale. The cervical, axillary, epitrochlear, and inguinal nodes are unremarkable. In the left supraclavicular fossa, there is a single hard, fixed, non-tender node, 2 by 2 centimetres — this is a Virchow node, Troisier sign. The right supraclavicular fossa is clear. Proceeding to the abdomen, there is a hard, irregular liver edge palpable 3 centimetres below the costal margin with a nodular surface — consistent with metastatic disease. There is no splenomegaly and no ascites. My findings are of a Virchow node with hepatomegaly and a nodular liver surface. The most likely diagnosis is metastatic intra-abdominal malignancy, classically gastric cancer, with hepatic metastases and a sentinel supraclavicular node via the thoracic duct. I would investigate with an upper GI endoscopy with biopsy, a CT of the chest, abdomen and pelvis, and tumour markers." [1]
Model presentation — massive splenomegaly (CML): "I examined this patient for organomegaly. At the end of the bed, the patient is pale but not cachectic or jaundiced, and not in distress. The hands show pallor of the palmar creases and the conjunctivae. There is no generalized lymphadenopathy — the cervical, axillary, epitrochlear, and inguinal nodes are unremarkable. In the abdomen, there is a large mass in the left upper quadrant extending from the left costal margin to the level of the umbilicus and crossing the midline toward the right iliac fossa. It has a smooth surface, a firm consistency, and a palpable notch on its medial border. I cannot get above it. It is dull to percussion. This is the spleen — the findings are of massive splenomegaly. There is no hepatomegaly, no ascites, and no other abdominal mass. The most likely cause of splenomegaly of this magnitude is a myeloproliferative neoplasm — chronic myeloid leukaemia or myelofibrosis. I would also consider chronic malaria, visceral leishmaniasis or kala-azar, and a storage disorder such as Gaucher disease. I would investigate with a full blood count and peripheral blood film, a lactate dehydrogenase, a bone marrow biopsy with cytogenetics for the BCR-ABL translocation of CML and the JAK2 mutation of myelofibrosis, and an abdominal CT." [1]
Discussion by finding — examiner questions
The examiner will ask you to interpret your findings. Below are the high-yield discussion topics for each key finding, with model answers. [1]
Finding: a single hard left supraclavicular node
Q: What is the significance of a Virchow node and what is the mechanism? [1]
A Virchow node (Troisier sign) is a sentinel left supraclavicular node for intra-abdominal malignancy. The mechanism is lymphatic drainage — the thoracic duct drains lymph from the entire abdomen via the cisterna chyli and empties into the left venous angle (the junction of the left subclavian and left internal jugular veins). Malignant cells from the abdomen are trapped in the node at this lymphatic bottleneck. The classic primary is gastric cancer, but pancreatic, hepatobiliary, colorectal, testicular, ovarian, and renal malignancy also metastasise here. A right supraclavicular node more often signals lung cancer or a mediastinal lymphoma, because the right lymphatic duct drains the right hemithorax and right upper limb. [1]
Finding: rubbery generalised lymphadenopathy
Q: What consistency of node suggests Hodgkin lymphoma, and why? [1]
Hodgkin lymphoma classically produces rubbery nodes — dense, firm but slightly bouncy, like a piece of india rubber. This differs from the hard, stony node of metastatic carcinoma and the soft, tender node of acute infection. The rubbery texture reflects the orderly proliferation of the Reed-Sternberg cells within a background of reactive inflammatory cells, which preserves some of the normal node architecture while expanding it. Hodgkin lymphoma also characteristically spreads in a contiguous fashion from one node group to the next (unlike the non-contiguous spread of non-Hodgkin lymphoma), and the nodes are typically painless — though alcohol-induced pain in Hodgkin-involved nodes is a classic (if rare) exam vignette. [1]
Finding: massive splenomegaly
Q: Name the causes of massive splenomegaly. [1]
The high-yield list is: chronic myeloid leukaemia, myelofibrosis, chronic malaria (hyperreactive malarial splenomegaly), visceral leishmaniasis (kala-azar), Gaucher disease, and primary hypersplenism. Massive splenomegaly narrows the differential immediately — you do not list the dozens of causes of mild splenomegaly when the spleen crosses the midline. The bedside clue of pallor alongside massive splenomegaly points to the myeloproliferative neoplasms (CML and myelofibrosis), which cause anaemia by marrow infiltration or fibrosis. A travel history to an endemic region points to malaria or kala-azar. A patient of Ashkenazi Jewish ancestry with bone pain and pancytopenia raises Gaucher disease. [1]
Q: How do you differentiate the spleen from the left kidney? [1]
Three features. First, I cannot get above the spleen — its upper border is continuous with the diaphragm under the costal margin; I can palpate above a ballotable kidney because it descends from the retroperitoneum. Second, the spleen is dull to percussion (it lies behind the stomach, which is displaced); the kidney is resonant because of the overlying stomach and splenic flexure gas. Third, the spleen has a notch on its medial border; the kidney does not. Additionally, the spleen moves with respiration, enlarges diagonally toward the right iliac fossa, and cannot be ballotted. The Grover systematic review found these manoeuvres have moderate sensitivity and that a non-palpable spleen does not exclude splenomegaly, particularly in obese patients [1].
Finding: a hard nodular liver
Q: What does a hard, nodular, irregular liver indicate? [1]
Cirrhosis (micronodular in alcohol, macronodular in viral hepatitis) and metastatic malignancy (primary in the colon, stomach, pancreas, breast, lung, or melanoma). A hard, nodular liver in a patient with weight loss is metastatic disease until proven otherwise. The distinction from cirrhosis is made on the history (known chronic liver disease, alcohol, viral hepatitis), the stigmata of chronic liver disease (spider naevi, palmar erythema, Dupuytren contracture), and the imaging and biopsy. [1]
Q: What does a pulsatile liver indicate? [1]
Tricuspid regurgitation — the regurgitant systolic wave is transmitted through the vena cava to the hepatic veins and the liver. If I felt a pulsatile liver, I would examine the JVP for giant v-waves and listen for the pansystolic murmur of tricuspid regurgitation. [1]
Finding: hepatosplenomegaly
Q: The patient has both hepatomegaly and splenomegaly. What is your differential? [1]
The differential for combined hepatosplenomegaly includes: chronic liver disease with portal hypertension (the spleen enlarges from congestion in the portal venous system), haematological malignancy (lymphoma, leukaemia, especially chronic lymphocytic leukaemia), chronic infection (infectious mononucleosis, malaria, brucellosis, schistosomiasis), storage diseases (Gaucher, Niemann-Pick), and myeloproliferative neoplasms (CML, myelofibrosis, polycythaemia vera). The presence of stigmata of chronic liver disease points to portal hypertension; the presence of lymphadenopathy points to lymphoma; a marked leucocytosis on the blood film points to a leukaemia; and massive splenomegaly out of proportion to the hepatomegaly points to a myeloproliferative neoplasm. [1]
Finding: inguinal lymphadenopathy
Q: When is an inguinal node pathological? [1]
Small, mobile, discrete inguinal nodes under 1 to 2 cm are extremely common in adults, the result of repeated minor lower limb infection and trauma. They are pathological and warrant investigation when they are over 2 cm, hard or matted, fixed, progressive, associated with overlying cellulitis, or part of generalised lymphadenopathy. The inguinal nodes also have the lowest diagnostic yield on biopsy because of chronic reactive stimulation, so when a biopsy is needed and no node is dominant, the supraclavicular or cervical nodes are preferred [3][4].
Common examination traps and pitfalls
One-line exam answer
The lymph node and organomegaly examination is a reproducible head-to-toe routine: head and neck nodes (submental, submandibular, pre and post-auricular, occipital, tonsillar, anterior and posterior cervical chains, supraclavicular Virchow, pre-tracheal), then axillary (apical, anterior, posterior, lateral, central), epitrochlear, inguinal (horizontal and vertical groups), and popliteal — describe each node by site, size, consistency, mobility, and tenderness — then the abdomen for the spleen (start in the right iliac fossa, move diagonally toward the left costal margin, cannot get above it, dull, notch, grade the splenomegaly), the liver (span 12 to 15 cm, surface, edge), and the kidneys (ballot, can get above, resonant). The candidate who performs this fluently, finds and names the Virchow node, differentiates the spleen from the kidney, grades the splenomegaly, and presents in a structured format passes the short case. [1]
References and further reading
Grover SA, Barkun AN, Sackett DL. Does this patient have splenomegaly? JAMA 1993 [1]; Naylor CD. Physical examination of the liver. JAMA 1994 [2]; Ferrer R. Lymphadenopathy: differential diagnosis and evaluation. American Family Physician 1998 [3]; Habermann TM, Steensma DP. Lymphadenopathy. Mayo Clinic Proceedings 2000 [4]. Bates' Guide to Physical Examination and History Taking; Macleod's Clinical Examination; Douglas, Nicol and Robertson, Macleod's Clinical Examination; Hutchison's Clinical Methods. NICE NG12; British Society for Haematology Guidelines; HSANZ; American Society of Hematology.
References
- [1]Grover SA, Barkun AN, Sackett DL The rational clinical examination. Does this patient have splenomegaly? JAMA, 1993.PMID 8411607
- [2]Naylor CD The rational clinical examination. Physical examination of the liver JAMA, 1994.PMID 8196144
- [3]Ferrer R Lymphadenopathy: differential diagnosis and evaluation Am Fam Physician, 1998.PMID 9803196
- [4]Habermann TM, Steensma DP Lymphadenopathy Mayo Clin Proc, 2000.PMID 10907389