Phys · general-medicine
Skin Examination for Systemic Disease — DCE Short-Case Routine
Also known as skin examination · examine the skin · cutaneous signs of systemic disease · skin short case · DCE skin examination · PACES skin examination · dermatological examination routine · skin signs of internal disease · skin manifestation examination · please examine this patient's skin
Consultant-physician guide to the systematic skin examination for the DCE short case: the six-step routine from general inspection through hands, face, trunk, legs and specific patterns, the morphology vocabulary (macule through purpura), the distribution and arrangement clues (photosensitive, acral, dermatomal, annular, livedoid), and the high-yield skin-to-system sign map — malar rash of SLE sparing nasolabial folds, heliotrope and Gottron papules of dermatomyositis, palmar erythema and spider naevi of cirrhosis, acanthosis nigricans of insulin resistance and GI malignancy, erythema nodosum and pyoderma gangrenosum, necrobiosis lipoidica, pretibial myxoedema, dermatitis herpetiformis of coeliac disease, and the purpura and livedo patterns of vasculitis and antiphospholipid syndrome — with the model presentation template, the examiner discussion questions, and the classic exam traps.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Skin Examination for Systemic Disease — DCE Short-Case Routine

The one-minute consultant answer
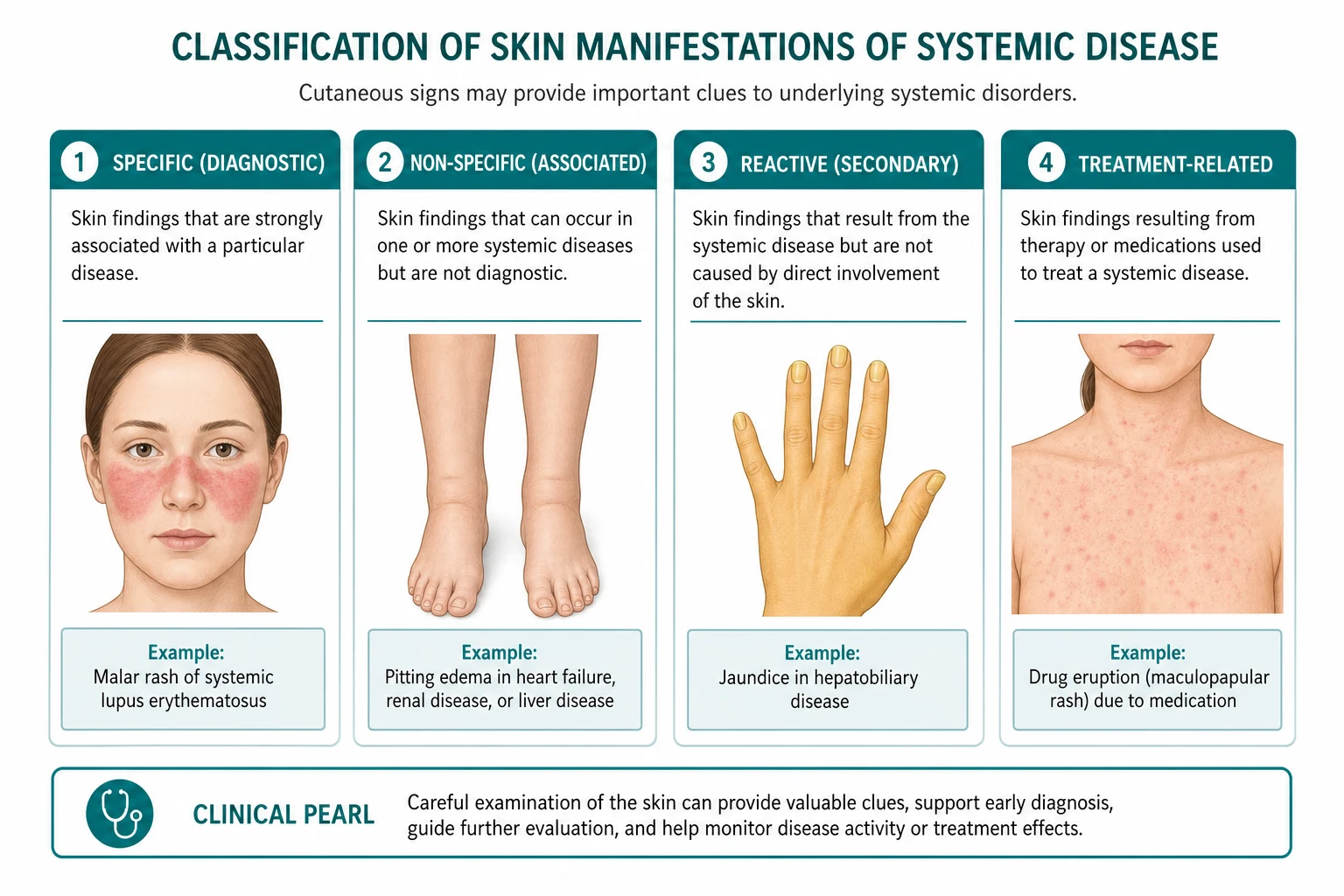
The skin short case is the instruction "Please examine this patient's skin," and the winning candidate runs the same six-step routine every time: general inspection, the hands, the face, the trunk, the legs, and the specific patterns. The routine is not a list of diseases — it is a systematic sweep of the body surface that guarantees you do not miss a finding. The examiner is watching for three things: do you use the correct morphology vocabulary, do you relate the distribution to an anatomical or pathophysiological mechanism, and do you connect each finding to a systemic diagnosis with the right discriminating detail. [1]
The single most important principle is describe before you diagnose. The candidate who looks at the shins and says "diabetes" has jumped past the finding. The candidate who says "bilateral, symmetric, yellow-brown, atrophic plaques with a waxy surface and telangiectatic border on the pretibial skin, consistent with necrobiosis lipoidica, a cutaneous marker of diabetes mellitus" has shown the morphology, the distribution, the named entity, and the systemic link in one sentence. The morphology is the data; the diagnosis is the synthesis. Always lead with the data. [1]
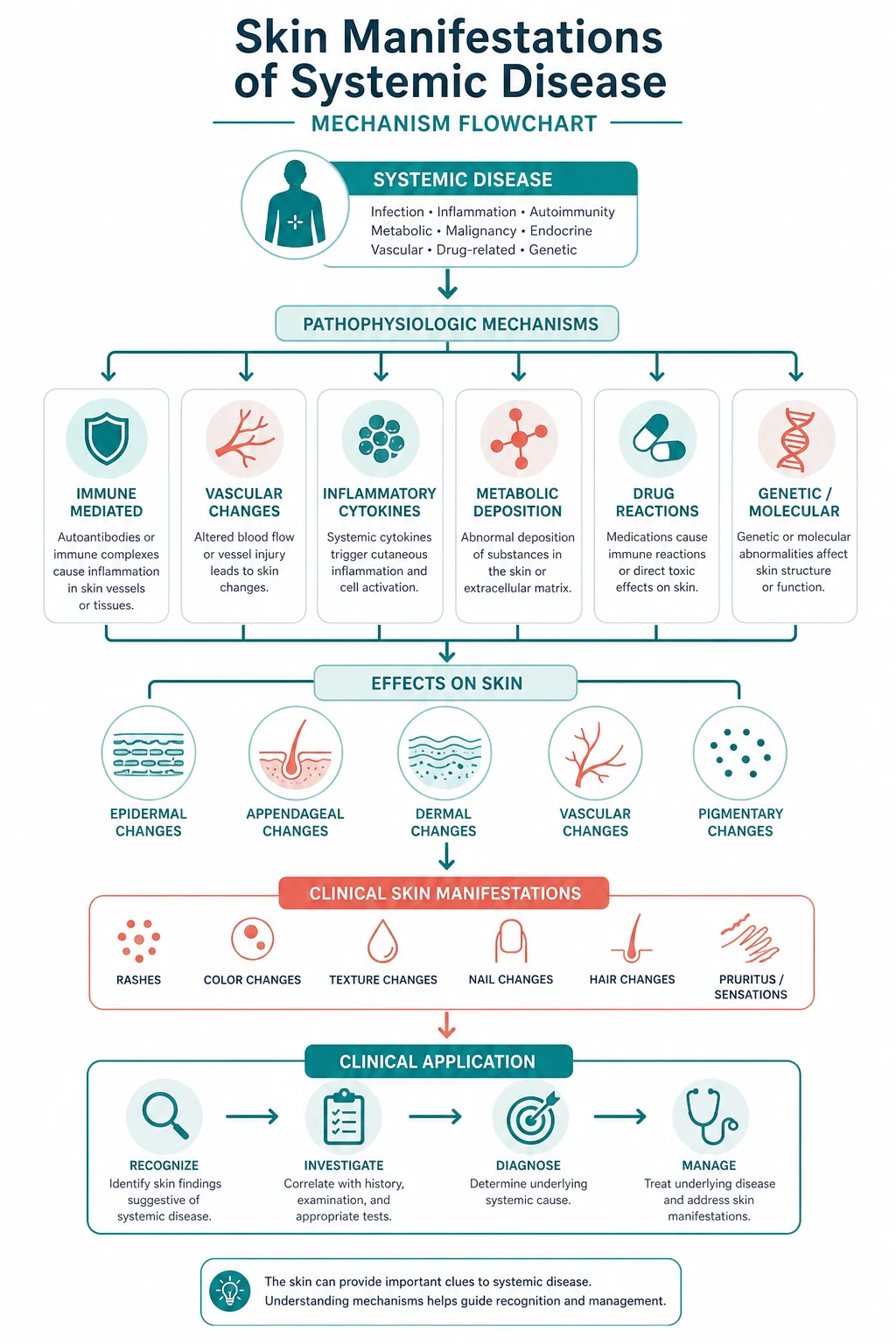
The non-negotiable principles: start at the end of the bed and note the distribution pattern before you touch the patient, because the distribution (photosensitive, acral, dependent, dermatomal, flexural, extensor) is often the first clue to the mechanism; describe each lesion in morphology terms (macule, papule, plaque, nodule, vesicle, bulla, pustule, purpura, erythema, scale, crust, atrophy, ulcer) because the vocabulary is the exam currency; examine the hands, the nails and the nail folds first, because the hands carry more discriminating systemic signs per square centimetre than any other body region; look at the face for the pattern rashes (malar, heliotrope, oral ulcers, periorbital xanthelasma) because the face identifies the rheumatological and metabolic diseases; examine the trunk for the stigmata of liver disease, insulin resistance, Cushing syndrome and the phakomatoses because the trunk carries the general medical signs; examine the legs for the panniculitides, the neutrophilic dermatoses, the diabetic and thyroid dermopathies, the purpura and the livedo patterns because the legs carry the highest-yield individual signs; and close with the mucosae, the scalp and the nails, because the skin examination is incomplete without them. [1]
The examination routine — the six-step sequence

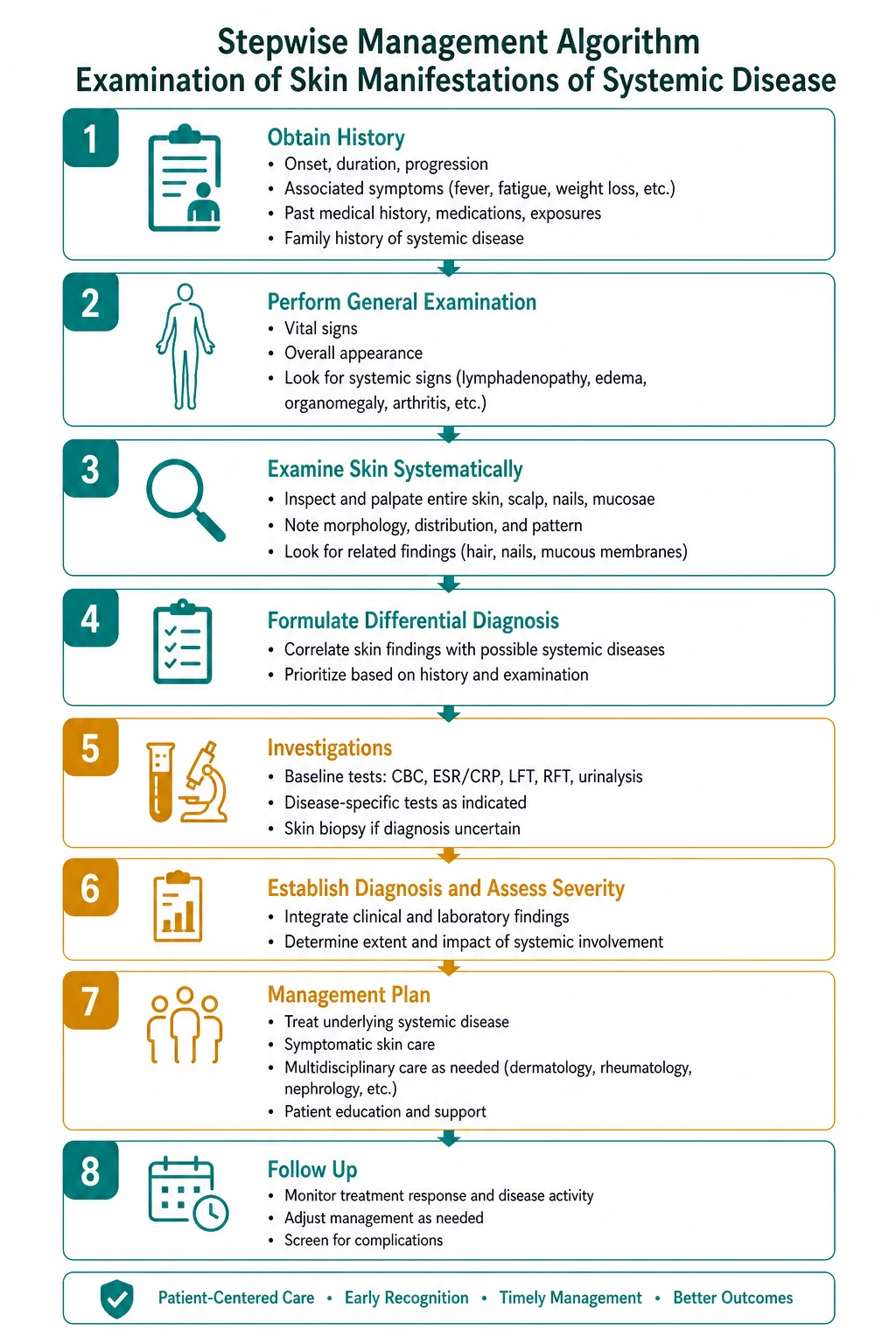
The skin short case has a fixed sequence: general inspection, hands, face, trunk, legs, specific patterns and closure. Every candidate must perform the steps in the same order every time, so that no region is omitted and the examiner can follow the logic. The time available in the DCE short case is approximately six minutes for the examination and two minutes for the presentation and discussion. The sequence below is designed for that constraint. [1]
Step 1 — General inspection (from the end of the bed)
Before you touch the patient, stand at the end of the bed and take ten seconds. You are looking for three things: the distribution pattern, the overall morphology class, and the arrangement of the lesions. [1]
Distribution is the first discriminator. A photosensitive distribution (face, the V of the neck, the dorsa of the forearms, sparing the areas protected by clothing or hair) points to lupus or dermatomyositis. An acral distribution (fingers, toes, nose, ears — the extremities) points to vasculitis, antiphospholipid syndrome, cryoglobulinaemia or pernio. A dependent distribution (the lower legs and the sacrum) points to venous stasis, oedema-associated dermatoses, or purpura from thrombocytopenia or amyloidosis. A dermatomal distribution (following a single dermatome, unilateral, stopping at the midline) points to herpes zoster. A flexural distribution (the antecubital fossae, the popliteal fossae, the axillae, the neck) points to atopic eczema or to acanthosis nigricans. An extensor distribution (the elbows, the knees, the shins) points to psoriasis, dermatitis herpetiformis, erythema nodosum or necrobiosis lipoidica. [1]
Morphology is the vocabulary. Before you name a disease, classify what you see. A macule is a flat colour change you cannot feel. A papule is a raised solid lesion less than one centimetre. A plaque is a raised flat-topped lesion more than one centimetre (the surface area is greater than the elevation). A nodule is a solid lesion extending into the dermis or deeper, more than one centimetre. A vesicle is a fluid-filled blister less than one centimetre; a bulla is a fluid-filled blister more than one centimetre. A pustule is a pus-filled blister. Purpura is bleeding into the skin — non-blanching, because the red cells are extravascular. Erythema is redness that blanches on pressure, because it is vascular dilatation. Scale is compacted desquamating stratum corneum. Crust is dried serum, blood or pus on the surface. Atrophy is thinning of the skin — a loss of epidermis, dermis or subcutaneous tissue. An ulcer is a full-thickness loss of the epidermis and at least the papillary dermis. [1]

Arrangement is the spatial pattern. Annular (ring-shaped) lesions suggest granuloma annulare, tinea corporis, erythema migrans of Lyme disease, or the advancing edge of subacute cutaneous lupus. Linear lesions suggest a contact dermatitis, koebnerisation (psoriasis appearing in lines of trauma), or the linear immunoglobulin A bullous dermatosis. Grouped (herpetiform) lesions suggest dermatitis herpetiformis or herpes simplex. A reticular (net-like) arrangement suggests livedo reticularis or livedo racemosa. Target (iris) lesions are the hallmark of erythema multiforme. [1]
The teaching point: the five to ten seconds at the end of the bed frame the entire examination. State your impression of the distribution and the morphology class before you approach the patient: "On general inspection, this patient has an extensor-distribution eruption of symmetric, erythematous nodules on both shins, consistent with a panniculitis. The most likely diagnosis is erythema nodosum." Then confirm or refute that impression region by region. [1]
Step 2 — The hands
The hands are the highest-yield region in the skin short case, because they carry signs of rheumatological, endocrine, hepatic, haematological, infectious and genetic disease. Examine the hands systematically: the nails, the nail folds, the palms and the fingers. [1]

Nail changes: [1]
- Clubbing — loss of the nail-fold angle (Lovibond angle), the Schamroth window sign is positive (when the nails of the same finger are placed nail-to-nail, the normal diamond-shaped window disappears). Clubbing points to pulmonary (lung cancer, bronchiectasis, pulmonary fibrosis, mesothelioma), cardiac (cyanotic congenital heart disease, infective endocarditis), gastrointestinal (inflammatory bowel disease, cirrhosis, coeliac disease) and other (thyroid — thyroid acropachy is a variant) causes.
- Koilonychia — spooning of the nails (a concave nail plate that can hold a drop of water). The classic association is iron-deficiency anaemia, but koilonychia also occurs with haemochromatosis, Plummer-Vinson syndrome and thyroid disease.
- Beau lines — transverse grooves across all the nails at the same level, representing a transient arrest of nail growth during a severe systemic illness, a high fever, chemotherapy, or a major surgical event. You can date the insult by measuring the distance from the line to the proximal nail fold and dividing by the nail growth rate (approximately three millimetres per month for fingernails).
- Splinter haemorrhages — linear, reddish-brown streaks under the nail plate, aligned with the long axis of the nail. The classic association is infective endocarditis (two or more, with a fever and a murmur), but they also occur with trauma, psoriasis and as a normal finding in manual workers. Do not call every splinter haemorrhage endocarditis in isolation.
- Nail-fold capillary changes — the single most discriminating rheumatological sign in the hands. Examine the proximal nail fold with good lighting, ideally with an ophthalmoscope or a dermatoscope at 10 to 20 dioptres. Dilated, tortuous capillary loops with dropout (avascular areas) indicate systemic sclerosis or dermatomyositis. Normal, fine, evenly spaced hairpin loops argue against a connective tissue disease. The presence of periungual erythema and ragged, hypertrophic cuticles (Samitz sign) supports dermatomyositis.
- Onycholysis — separation of the nail plate from the nail bed, beginning distally. Occurs with psoriasis, thyrotoxicosis (Plummer nails), trauma and fungal infection.
- Pitting and onychorrhexis — nail pitting (small depressions in the nail plate) is a sign of psoriasis and alopecia areata; onychorrhexis (longitudinal ridging) is non-specific but common in lichen planus and ageing. [1]
Palmar changes: [1]
- Palmar erythema — a diffuse, warm, pink-to-red discolouration of the palms, especially the thenar and hypothenar eminences, sparing the central palm. It occurs in cirrhosis, pregnancy, thyrotoxicosis, rheumatoid arthritis and as a normal variant. It blanches and is not a rash — it is a vascular phenomenon.
- Gottron papules — violaceous (iliac-coloured), flattish-topped papules over the dorsal surfaces of the metacarpophalangeal and interphalangeal joints. Gottron papules are pathognomonic for dermatomyositis. Do not confuse them with the rheumatoid nodule (firm, subcutaneous, over the extensor surface but not the skin surface) or with Heberden or Bouchard nodes (bony, hard, osteoarthritic) [2][3].
- Thenar atrophy — wasting of the thenar eminence from median nerve compression (carpal tunnel syndrome), not a skin sign per se, but it is part of the hand inspection and may point to a systemic cause (hypothyroidism, pregnancy, amyloidosis, rheumatoid arthritis).
- Mechanic hands — hyperkeratotic, fissured, dirty-appearing skin on the radial and palmar aspects of the fingers and the palms. A characteristic sign of dermatomyositis (especially the antisynthetase syndrome), it mimics the hands of a manual worker [3].
Finger changes: [1]
- Sclerodactyly — thickening, tightening and tethering of the skin of the fingers distal to the metacarpophalangeal joints, with loss of skin creases and a shiny, waxy appearance. A hallmark of systemic sclerosis. Digital pitting scars (small, depressed scars on the fingertips from ischaemic microinfarcts) and calcinosis cutis (firm, white subcutaneous deposits) are the other scleroderma-specific hand findings.
- Calcinosis — hard, white, subcutaneous nodules on the fingertips or over the joints, representing calcium deposition. The C in the CREST syndrome (calcinosis, Raynaud, oesophageal dysmotility, sclerodactyly, telangiectasia).
- Telangiectasia — visible, dilated small vessels on the fingers, the palms or the face. Matted telangiectasia of systemic sclerosis distinguishes it from the simple fine telangiectasia of rosacea or chronic sun damage. [1]
Step 3 — The face
The face identifies the rheumatological, metabolic, infectious and genetic diseases. Examine the face systematically: the forehead and hairline, the eyes and periorbital skin, the cheeks, the nose, the lips and the oral mucosa. [1]
Malar rash (butterfly rash) of SLE — an erythematous, flat or slightly raised rash over the cheeks and the bridge of the nose, sparing the nasolabial folds. The nasolabial fold sparing is the discriminating detail, because the malar rash of SLE is a photosensitive reaction and the nasolabial folds are shielded from ultraviolet light by the overlying tissue. The malar rash must be distinguished from rosacea (which involves the nasolabial folds, has papules and pustules, and is associated with flushing and telangiectasia) and from the photosensitive rash of dermatomyositis (which may involve the face but is more violaceous and is accompanied by the heliotrope rash and the Gottron papules) [1].
Heliotrope rash of dermatomyositis — a violaceous (dusky lilac) discolouration of the upper eyelids, sometimes with periorbital oedema. The heliotrope rash is the most specific cutaneous sign of dermatomyositis. It is the colour of the heliotrope flower — a dusky purple. It may be subtle, so examine the upper eyelids carefully, asking the patient to close the eyes. The heliotrope rash, with the Gottron papules, makes the diagnosis of dermatomyositis from the skin alone [2][3].
Oral ulcers — painless ulcers on the hard palate (the preferred site in SLE) or painful aphthous ulcers on the buccal mucosa, the tongue or the lips (Behcet disease, inflammatory bowel disease, coeliac disease, reactive arthritis). Painless oral ulcers on the hard palate, in a patient with a malar rash and positive antinuclear antibodies, support SLE [1].
Periorbital xanthelasma — yellowish, flat or slightly raised plaques on the eyelids, especially the medial canthus. A sign of dyslipidaemia (primary hypercholesterolaemia, familial hypercholesterolaemia) or of chronic cholestasis (primary biliary cholangitis). Examine for arcus senilis (a grey-white ring at the corneal margin) and tendon xanthomata (in the Achilles, the extensor tendons of the hands and the patellar tendons) to complete the hyperlipidaemia screen. [1]
Spider naevi (spider telangiectasia) — a central arteriole with radiating fine vessels, found in the distribution of the superior vena cava (above the nipple line — the face, the neck, the upper chest, the arms). Blanch on pressure (the central arteriole is the feeder) and refill from the centre outward. More than three to five spider naevi, in a man or a non-pregnant woman, suggests chronic liver disease (cirrhosis) with oestrogen excess from impaired hepatic metabolism. Spider naevi also occur in pregnancy (a benign, oestrogen-driven state). [1]
Facial signs of endocrine disease — the moon face, the plethora and the buffalo hump of Cushing syndrome; the exophthalmos, the lid retraction and the lid lag of Graves disease (cross-link to the thyroid examination topic); the coarse facial features, the prognathism and the enlarged hands and feet of acromegaly. [1]
Step 4 — The trunk
The trunk carries the general medical signs — the stigmata of liver disease, insulin resistance, glucocorticoid excess and the inherited tumour syndromes. Examine the anterior chest, the abdomen, the back and the axillae. [1]
Acanthosis nigricans — velvety, thickened, hyperpigmented skin in the flexures (the axillae, the back of the neck, the inguinal folds, the antecubital fossae). The common association is insulin resistance (type 2 diabetes, obesity, metabolic syndrome). The mechanism is the hyperinsulinaemia stimulating the insulin-like growth factor 1 receptors on the keratinocytes and the fibroblasts. Acanthosis nigricans that is rapidly progressive, extensive, involves the oral mucosa or the palms (tripe palms), or occurs in a non-obese patient without metabolic risk factors is malignant acanthosis nigricans — a paraneoplastic phenomenon, most commonly from a gastric or other gastrointestinal adenocarcinoma [8][10].
Striae — purple (if recent) or white (if old) linear atrophic bands, perpendicular to the line of skin tension, on the abdomen, the flanks, the thighs and the breasts. The classic association is Cushing syndrome (exogenous or endogenous glucocorticoid excess), where the striae are purple, broad (more than one centimetre) and on the abdomen. Striae also occur in pregnancy, rapid weight gain, adolescence and Marfan syndrome. The discriminating detail is the colour (purple striae suggest active glucocorticoid excess) and the distribution (the abdomen and the flanks, not the thighs alone). [1]
Gynaecomastia — bilateral (or asymmetric) enlargement of the male breast glandular tissue, from an altered oestrogen-to-testosterone ratio. The hepatic association is cirrhosis (impaired metabolism of oestrogens). Drug causes include spironolactone, digoxin, ketoconazole and anabolic steroids. Distinguish true gynaecomastia (glandular tissue, felt as a firm disc beneath the areola) from pseudogynaecomastia (adipose tissue, soft and diffuse, in the obese male). [1]
Spider naevi on the trunk — as above, spider naevi above the umbilicus (in the distribution of the superior vena cava) suggest portal hypertension and chronic liver disease. The combination of spider naevi, palmar erythema, gynaecomastia, caput medusae (dilated periumbilical veins from recanalised umbilical veins) and jaundice makes the bedside diagnosis of cirrhosis. [1]
Caput medusae — dilated, tortuous veins radiating from the umbilicus, representing recanalised paraumbilical veins in portal hypertension. Distinguish from the inferior vena cava obstruction pattern (dilated veins on the abdominal wall with upward blood flow toward the superior vena cava) by determining the direction of venous flow — in portal hypertension, the flow is away from the umbilicus (the recanalised umbilical vein drains toward the systemic veins). [1]
Shagreen patches and ash-leaf macules (tuberous sclerosis) — shagreen patches are firm, flesh-coloured to yellowish-brown, cobblestone-textured plaques in the lumbosacral region (the lower back). Ash-leaf macules are hypopigmented (whiter than the surrounding skin, best seen with a Wood lamp), oval or ash-leaf-shaped macules on the trunk or the limbs. Both are cutaneous markers of tuberous sclerosis (an autosomal dominant neurocutaneous syndrome with epilepsy, intellectual disability, renal angiomyolipomata and cardiac rhabdomyomata). Also look for angiofibromata (small, red, telangiectatic papules on the cheeks and the nasolabial folds, formerly called adenoma sebaceum) and periungual and subungual fibromata (Koenen tumours) on the nails. [1]
Cafe-au-lait macules (neurofibromatosis type 1) — flat, uniformly light-brown (coffee-with-milk) macules, more than five millimetres in diameter before puberty or more than fifteen millimetres after puberty. Six or more cafe-au-lait macules meet a diagnostic criterion for NF1. Also look for axillary and inguinal freckling (Crowe sign), cutaneous neurofibromata (soft, flesh-coloured, buttonhole-sign-positive nodules) and Lisch nodules (iris hamartomata, seen with a slit lamp). [1]
Step 5 — The legs
The legs carry the highest-yield individual signs in the skin short case — the panniculitides, the neutrophilic dermatoses, the diabetic and thyroid dermopathies, the purpura and the livedo patterns. Examine both legs from the groin to the toes, comparing left and right. [1]
Erythema nodosum — bilateral, symmetric, tender, erythematous, subcutaneous nodules on the anterior (pretibial) shins. The lesions are deep (in the subcutaneous fat, the panniculus) and do not ulcerate. The differential of the causes is the exam question: streptococcal infection (the commonest infectious cause in children), sarcoidosis (the commonest cause in young adults in many series, look for bilateral hilar lymphadenopathy on the chest X-ray and uveitis), inflammatory bowel disease (Crohn disease, ulcerative colitis), drugs (the oral contraceptive pill, sulfonamides, penicillins), tuberculosis, yersinia, chlamydia, histoplasmosis, coccidioidomycosis, Behcet disease, Hodgkin lymphoma and pregnancy. Approximately 30 to 55 per cent of cases are idiopathic. The workup is a throat swab, an antistreptolysin O titre, a chest X-ray (for sarcoidosis and tuberculosis) and inflammatory markers [5].
Pyoderma gangrenosum — a painful, rapidly enlarging ulcer with an undermined, violaceous, boggy border, often preceded by a pustule or a nodule. The hallmark is pathergy (the ulcer worsens with trauma — debridement makes it worse). Pyoderma gangrenosum is a diagnosis of exclusion, because there is no confirmatory test. Approximately 50 to 70 per cent of cases are associated with a systemic disease — inflammatory bowel disease (ulcerative colitis more than Crohn disease), inflammatory arthritis (rheumatoid arthritis, seronegative spondyloarthropathy), and haematological disease (myelodysplasia, acute myeloid leukaemia, monoclonal gammopathy, especially IgA). Do not debride a suspected pyoderma gangrenosum ulcer — the pathergy response will worsen it [6].
Necrobiosis lipoidica — bilateral, symmetric, yellow-brown, atrophic plaques with a waxy surface, telangiectatic borders and a central pallor, on the pretibial shins. The yellow colour (from lipid deposition) and the atrophy (the thinning of the skin so that the underlying vasculature is visible) are the discriminating features. The classic association is diabetes mellitus (previously called necrobiosis lipoidica diabeticorum), but only approximately 15 to 20 per cent of patients with necrobiosis lipoidica have diabetes, and not all diabetics develop the condition. The plaques can ulcerate (approximately one-third of cases) and rarely transform to squamous cell carcinoma [7][9].
Pretibial myxoedema (thyroid dermopathy) — bilateral, symmetric, firm, non-pitting, waxy plaques or nodules on the pretibial skin, with a peau d'orange (orange-peel) surface texture. The classic association is Graves disease — pretibial myxoedema is part of the triad of exophthalmos, dermopathy and thyroid acropachy that defines severe Graves autoimmune disease. The mechanism is the thyroid-stimulating hormone receptor antibodies stimulating the skin fibroblasts to produce glycosaminoglycans (hyaluronic acid), which draw in water and produce the waxy induration. Cross-link to the thyroid examination topic for the full Graves orbitopathy assessment. [1]
Livedo reticularis and livedo racemosa — a net-like (reticular), cyanotic, reddish-blue discolouration of the skin, caused by the deoxygenation of the blood in the slow-flowing superficial venous plexus. Physiological livedo reticularis (cutis marmorata) is a normal response to cold and disappears on rewarming. Persistent livedo — especially livedo racemosa (a coarser, irregular, broken, non-resolution-on-rewarming pattern) — is pathological and points to antiphospholipid syndrome (the Sneddon syndrome variant with livedo and cerebrovascular events), systemic vasculitis (polyarteritis nodosa), cryoglobulinaemia, cholesterol emboli, or a myeloproliferative disorder with hyperviscosity. Livedo racemosa on the buttocks, the thighs and the lower back is a classic sign of polyarteritis nodosa. [1]
Purpura and petechiae — purpura is bleeding into the skin that does not blanch on pressure (the red cells are extravascular). Petechiae are pinhead-sized (less than three millimetres) purpuric lesions. Ecchymoses are larger areas (more than one centimetre) of purpura. The distribution and the morphology distinguish the mechanism. Non-palpable purpura (flat, macular) suggests a platelet or coagulation disorder — thrombocytopenia (immune thrombocytopenic purpura, leukaemia, aplastic anaemia, drug-induced), platelet dysfunction, or a coagulopathy (liver disease, disseminated intravascular coagulation, warfarin excess). Palpable purpura (raised, you can feel it) suggests small-vessel vasculitis (leucocytoclastic vasculitis from immune complex deposition) or an infectious embolus (meningococcaemia, gonococcaemia, Rocky Mountain spotted fever, infective endocarditis). Palpable purpura is the skin sign that mandates a vasculitis and infection workup — check the urine for blood and protein (renal vasculitis), the blood for ANCA, cryoglobulins, hepatitis B and C, complement levels, and blood cultures [1].
Digital infarcts and splinter haemorrhages (the microvascular occlusion signs) — small, dark, wedge-shaped infarcts at the fingertips, the toes, or the earlobes. The differential is vasculitis, antiphospholipid syndrome, cholesterol emboli (from a ruptured atheromatous plaque, often after a vascular procedure, with a livedo pattern and blue toes), cryoglobulinaemia, and infective endocarditis (Osler nodes are tender, pink papules on the pulps from immune complex deposition; Janeway lesions are painless, erythematous macules on the palms and the soles from septic microemboli). [1]
Step 6 — Specific patterns and the mucosae
The final step is to recognise the pattern rashes — the morphological entities whose appearance alone names the diagnosis — and to close the examination by checking the mucosae, the scalp and the genitalia. [1]
Dermatomal pattern — herpes zoster (shingles) — a painful, vesicular eruption in a single dermatome, unilateral and stopping at the midline. The vesicles evolve to pustules and then to crusts. The thoracic dermatomes are the most commonly involved, followed by the trigeminal (especially the ophthalmic division, where the Hutchinson sign — a vesicle on the tip of the nose, innervated by the nasociliary nerve — predicts ocular involvement and mandates urgent ophthalmology referral). Post-herpetic neuralgia is the most common complication. [1]
Dermatitis herpetiformis — intensely itchy (the patient scratches more than the lesions show), grouped (herpetiform), small vesicles on the extensor surfaces (the elbows, the knees, the buttocks, the shoulders, the scalp). The vesicles are often excoriated or crusted by the time of presentation, because the itch precedes the visible lesion. Dermatitis herpetiformis is the specific cutaneous manifestation of coeliac disease — nearly all patients have a gluten-sensitive enteropathy, though many are asymptomatic from the gut. The diagnosis is confirmed by a skin biopsy with direct immunofluorescence showing granular immunoglobulin A deposition in the dermal papillae. The autoantigen is epidermal transglutaminase (transglutaminase 3), and the shared autoimmunity with the tissue transglutaminase of coeliac disease links the skin and the gut. The treatment is a lifelong gluten-free diet, with dapsone for the skin until the diet takes effect [4].
Erythema multiforme — target (iris) lesions: concentric rings of colour with a dark or bullous centre, a pale oedematous ring and an outer erythematous ring, distributed symmetrically on the extensor surfaces, the palms, the soles and the mucous membranes. The classic triggers are herpes simplex virus (the commonest cause of recurrent erythema multiforme), mycoplasma pneumoniae, and drugs (sulfonamides, penicillins, anticonvulsants, non-steroidal anti-inflammatory drugs). Erythema multiforme with minimal or no mucosal involvement is erythema multiforme minor; with two or more mucosal sites and skin detachment less than 10 per cent of the body surface area it is erythema multiforme major. [1]
Stevens-Johnson syndrome and toxic epidermal necrolysis — the severe end of the spectrum. Stevens-Johnson syndrome is defined by skin detachment of less than 10 per cent of the body surface area, with two or more mucosal sites involved and target lesions or atypical target lesions. Toxic epidermal necrolysis is skin detachment of more than 30 per cent of the body surface area, with full-thickness epidermal necrosis and a positive Nikolsky sign (the epidermis shears off with lateral pressure). The commonest triggers are drugs (allopurinol, anticonvulsants — lamotrigine, carbamazepine, phenytoin — sulfonamide antibiotics, nevirapine, and non-steroidal anti-inflammatory drugs, especially oxicams). The condition is a dermatological emergency requiring immediate drug cessation, transfer to a burns or intensive care unit, and supportive care. [1]
Morbilliform drug eruption — the commonest drug rash. A symmetric, confluent, measles-like (morbilliform) maculopapular eruption beginning on the trunk and the proximal extremities, spreading centrifugally, often with low-grade fever and pruritus. It typically appears 7 to 14 days after the first exposure to the drug (or 1 to 3 days after re-exposure). The commonest causative drugs are penicillins, cephalosporins, sulfonamides and allopurinol. The rash usually resolves on drug cessation, but it can progress to more severe cutaneous adverse reactions. [1]
The presentation template
The presentation takes under two minutes. The examiner can interrupt at any point. The structure is: the one-sentence synthesis, the positive findings grouped by body region, the relevant negatives, the systemic differential, and the proposed investigations. [1]
The model opening for a skin short case with a malar rash: [1]
"I introduced myself to the patient, explained the examination, and obtained consent. I examined the patient in good natural light, exposing the relevant areas while maintaining dignity. [1]
On general inspection, this young woman has an erythematous rash over the cheeks and the bridge of the nose, sparing the nasolabial folds, in a photosensitive distribution. [1]
In the hands, the nails are normal with no clubbing, no nail-fold capillary changes, and no Gottron papules. There is no sclerodactyly. [1]
On the face, the malar rash is flat, confluent, and spares the nasolabial folds. There are small, painless ulcers on the hard palate. There is no heliotrope rash, no periorbital oedema, and no xanthelasma. There are two spider naevi on the neck. [1]
On the trunk, there is no acanthosis nigricans in the axillae or the neck, no striae, and no cafe-au-lait macules. [1]
On the legs, there is no erythema nodosum, no purpura, and no livedo. [1]
In summary, this patient has a photosensitive malar rash sparing the nasolabial folds, with painless oral ulcers, consistent with systemic lupus erythematosus. I would like to take a full history including sun exposure, joint symptoms, and a drug history, and I would check the full blood count, the renal and liver function, the urinalysis, the antinuclear antibodies, the extractable nuclear antigens (anti-dsDNA, anti-Smith), and the complement levels [1]."
Discussion questions
Q1: "You described a malar rash sparing the nasolabial folds as consistent with SLE. What else is in the facial rash differential, and how do you distinguish them?" [1]
"The three facial rashes to distinguish are the malar rash of SLE, the photosensitive rash of dermatomyositis, and rosacea. The malar rash of SLE is erythematous, flat or slightly raised, spares the nasolabial folds, and is photosensitive — it appears on sun-exposed skin. The dermatomyositis rash is more violaceous (ilac-coloured), is accompanied by the heliotrope rash on the upper eyelids and the Gottron papules on the knuckles, and may involve the scalp, the V of the neck and the shawl area. Rosacea involves the nasolabial folds (it does not spare them), has papules and pustules, and is associated with flushing, telangiectasia and rhinophyma. The laboratory confirmation is the ANA, the anti-dsDNA and the anti-Smith for SLE, and the creatine kinase and the myositis-specific antibodies for dermatomyositis [1]."
Q2: "What does a palpable purpura on the lower legs signify, and what is your investigation approach?" [1]
"Palpable purpura signifies small-vessel (leucocytoclastic) vasculitis — the immune complex deposition in the postcapillary venules produces inflammation and extravasation of red cells, so the lesion is raised (palpable) and non-blanching. The investigation approach is to identify the cause and to assess for systemic involvement. For the cause, I check the ANCA (for microscopic polyangiitis, granulomatosis with polyangiitis, eosinophilic granulomatosis with polyangiitis), the cryoglobulins and the complement (for cryoglobulinaemia, usually from hepatitis C), the hepatitis B and C serology, the antinuclear antibodies (for lupus vasculitis), the rheumatoid factor, and the serum protein electrophoresis. For the systemic involvement, I check the urinalysis for blood and protein (renal vasculitis is the most important complication), the renal function, the full blood count, and I examine for abdominal pain and gastrointestinal bleeding (mesenteric vasculitis) and for neuropathy (mononeuritis multiplex). A skin biopsy with direct immunofluorescence confirms the vasculitis and the immune complex type." [1]
Q3: "A patient has bilateral, tender, erythematous nodules on the shins. What is the diagnosis, and what is your approach to the cause?" [1]
"The diagnosis is erythema nodosum — the commonest form of panniculitis, presenting as bilateral, symmetric, tender, subcutaneous nodules on the anterior shins that do not ulcerate. The approach to the cause is a systematic screen: a throat swab and an antistreptolysin O titre (streptococcal infection, the commonest infectious cause), a chest X-ray (for sarcoidosis with bilateral hilar lymphadenopathy — Lofgren syndrome is erythema nodosum with bilateral hilar lymphadenopathy and ankle arthritis, a self-limiting form of sarcoidosis — and for tuberculosis), a drug history (the oral contraceptive pill, sulfonamides, penicillins, bromides), a history of gastrointestinal symptoms (inflammatory bowel disease — Crohn disease and ulcerative colitis), and a travel and exposure history (tuberculosis, yersinia, chlamydia, histoplasmosis, coccidioidomycosis). In approximately 30 to 55 per cent of cases, no cause is found. Erythema nodosum is usually self-limiting over two to eight weeks, with symptomatic treatment with bed rest, leg elevation and non-steroidal anti-inflammatory drugs [5]."
Q4: "How do you distinguish pyoderma gangrenosum from a venous ulcer, and why does the distinction matter?" [1]
"Pyoderma gangrenosum is a painful, rapidly enlarging ulcer with an undermined, violaceous, boggy border, often preceded by a pustule, and characterised by pathergy — it worsens with debridement. A venous ulcer is a shallower, irregular ulcer, typically over the medial malleolus, with the surrounding signs of venous hypertension (haemosiderin staining, lipodermatosclerosis, varicose eczema, oedema). The distinction matters because the management is opposite: a venous ulcer benefits from compression bandaging and debridement, while a pyoderma gangrenosum ulcer is worsened by debridement (pathergy) and requires systemic immunosuppression (corticosteroids, ciclosporin, or biologic agents such as infliximab). Approximately 50 to 70 per cent of pyoderma gangrenosum cases are associated with a systemic disease — inflammatory bowel disease, inflammatory arthritis, or a haematological disorder — so I screen for these associations [6]."
Q5: "You described necrobiosis lipoidica on the shins. How does this relate to diabetes, and what is the management?" [1]
"Necrobiosis lipoidica is a chronic granulomatous skin condition presenting as bilateral, symmetric, yellow-brown, atrophic plaques with telangiectatic borders on the pretibial shins. The association with diabetes is real but not absolute — approximately 15 to 20 per cent of patients with necrobiosis lipoidica have diabetes, and patients with necrobiosis lipoidica should be screened for diabetes, but the majority of diabetics never develop the condition. The mechanism is thought to involve microangiopathy and collagen degeneration. The management is challenging — there is no standardised, universally effective treatment. Topical and intralesional corticosteroids are first-line for early lesions, but they may worsen the atrophy. Other options include calcineurin inhibitors (tacrolimus), phototherapy (PUVA or narrowband UVB), and systemic agents (aspirin, pentoxifylline, or intravenous immunoglobulin) for severe cases. The most important complication is ulceration (approximately one-third of cases), and rarely, long-standing lesions can transform to squamous cell carcinoma [7][9]."
Exam traps
The jump-to-diagnosis trap: the candidate who looks at the shins and says "diabetes" before describing the lesion has failed the morphology test. Always describe the lesion first — the distribution, the morphology, the arrangement — then offer the diagnosis. The morphology is the data; the diagnosis is the synthesis. [1]
The nasolabial fold trap: the malar rash of SLE spares the nasolabial folds. Rosacea involves the nasolabial folds. This single discriminating detail separates the two most common causes of a red face in a young woman. The candidate who does not check the nasolabial folds has not completed the examination of the face. [1]
The palmar erythema trap: palmar erythema blanches (it is vascular dilatation), while a palmar purpura does not (the blood is extravascular). The candidate who squeezes a palmar lesion and does not check for blanching has not classified it. Blanching = erythema (vascular), non-blanching = purpura (haemorrhage). [1]
The splinter haemorrhage trap: a single splinter haemorrhage in a manual worker or a gardener is not infective endocarditis. Splinter haemorrhages are a sign of infective endocarditis only in the context of a fever, a murmur and the other features (Osler nodes, Janeway lesions, Roth spots, a vasculitic urine). The candidate who calls every splinter haemorrhage endocarditis has overcalled the sign. [1]
The palpable versus non-palpable purpura trap: non-palpable (macular) purpura is a platelet or coagulation problem (thrombocytopenia, coagulopathy). Palpable purpura is small-vessel vasculitis or an infectious embolus. The candidate who does not palpate a purpuric lesion has not classified it, and has missed the most important discriminator in purpura. [1]
The acanthosis nigricans trap: acanthosis nigricans in an obese patient with insulin resistance is benign and common. Acanthosis nigricans that is rapidly progressive, involves the oral mucosa or the palms (tripe palms), or occurs in a non-obese patient without metabolic risk factors is malignant acanthosis nigricans — a paraneoplastic phenomenon from a gastrointestinal adenocarcinoma (most often gastric). The candidate who labels all acanthosis nigricans as insulin resistance has missed the paraneoplastic possibility [8][10].
The livedo trap: physiological livedo reticularis (cutis marmorata) is a normal cold response that disappears on rewarming. Pathological livedo — especially livedo racemosa, the coarse, irregular, broken pattern that does not resolve — is associated with antiphospholipid syndrome, polyarteritis nodosa, cryoglobulinaemia and cholesterol emboli. The candidate who does not rewarm the patient before calling the livedo pathological has not distinguished the physiological from the pathological. [1]
The closure trap: the candidate who examines the skin and stops has not closed the examination. The closure must include the mucosae (the mouth for oral ulcers, the eyes for conjunctival signs), the scalp (for psoriasis, discoid lupus, scarring alopecia), the nails (a second look from the front and the side), and the genitalia if the history or the distribution warrants. The closure also includes stating the investigations — the full blood count, the urinalysis, the autoimmune screen and the imaging — and the specialist referral. [1]
Long-case integration and cross-links
In the DCE long case, the skin examination is one of the systems in the full systemic review. The skin findings are integrated into the problem list and the management plan. The patient with a malar rash, oral ulcers, proteinuria and arthritis has SLE with lupus nephritis — the skin is one of the systems, and the management (hydroxychloroquine, immunosuppression, sun protection) addresses the skin and the systemic disease together. The patient with acanthosis nigricans, central obesity and hyperglycaemia has metabolic syndrome with type 2 diabetes — the acanthosis is the cutaneous marker of the insulin resistance that is the core metabolic problem. [1]
Cross-link the management of SLE, dermatomyositis, systemic sclerosis, vasculitis and the endocrine and metabolic conditions to the dedicated disease-specific topics. Cross-link the thyroid and the hand examination to the thyroid examination and the rheumatological examination of the hands topics, where the technique and the discriminating signs are taught in detail. Cross-link the paraneoplastic dermatoses (dermatomyositis, malignant acanthosis nigricans, the sign of Leser-Trelat, erythema gyratum repens) to the oncologic emergencies and the immunotherapy topics. [1]
References
- [1]Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus Arthritis Rheumatol, 2019.PMID 31385462
- [2]Muro Y, Sugiura K, Akiyama M Cutaneous Manifestations in Dermatomyositis: Key Clinical and Serological Features-a Comprehensive Review Clin Rev Allergy Immunol, 2016.PMID 26100618
- [3]DeWane ME, Waldman R, Lu J Dermatomyositis: Clinical features and pathogenesis J Am Acad Dermatol, 2020.PMID 31279808
- [4]Reunala T, Salmi TT, Hervonen K Dermatitis herpetiformis: a cutaneous manifestation of coeliac disease Ann Med, 2017.PMID 27499257
- [5]Chowaniec M, Starba A, Wiland P Erythema nodosum - review of the literature Reumatologia, 2016.PMID 27407284
- [6]Boyatzis R, Shalabi M, Goshtasbi M, et al. Pyoderma Gangrenosum 2026.PMID 29489279
- [7]Lepe K, Zito PM. Necrobiosis Lipoidica 2026.PMID 29083569
- [8]Al-Uqaili NM, Tahir MQ, Al-Uqaili RMJ, Farhan SA Acanthosis Nigricans 2026.PMID 28613711
- [9]Reid SD, Ladizinski B, Lee K, Baibergenova A, Alavi A Update on necrobiosis lipoidica: a review of etiology, diagnosis, and treatment options J Am Acad Dermatol, 2013.PMID 23969033
- [10]Das A, Bhattacharya S, Lakshmi TV, et al. Acanthosis nigricans: A review J Cosmet Dermatol, 2020.PMID 32516476