Phys · general-medicine
Medical Errors and Open Disclosure
Also known as medical error · adverse event · patient safety incident · near miss · never event · sentinel event · open disclosure · duty of candour · root cause analysis · RCA · Swiss cheese model · human factors · just culture · second victim · mandatory notification · notifiable conduct · coronial referral · incident report
Consultant-physician guide to medical errors and open disclosure: the four definitions that anchor the field (medical error, adverse event, near miss, never event), the Swiss cheese model of Reason (active failures and latent conditions, slips lapses and mistakes, errors of execution versus planning), the types of error by stage of care (diagnostic, treatment, preventive, other), the high-alert medicines that concentrate risk (insulin, anticoagulants, opioids), the Australian Open Disclosure Framework (the staged process and the four elements — apology, factual explanation, acknowledgement, prevention), the duty of candour, root cause analysis and the London Protocol, the just culture algorithm, and the reporting and medico-legal pathways (incident report, AHPRA mandatory notification, coronial referral, medical defence organisation).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Medical Errors and Open Disclosure

Medical errors are common, and the way a physician responds when one occurs is a defining act of professional practice. This page is built so a registrar who has just discovered a tenfold insulin overdose on the ward, a missed pulmonary nodule, or a patient given the wrong blood can act decisively: stabilise the patient, recognise the event, disclose it openly, report it, investigate the system, and support the clinician. The two examiner errors to avoid are treating the disclosure as an admission of liability (it is not) and blaming the individual at the sharp end while leaving the latent system defect in place. [1]
The four definitions that anchor the field
Every patient-safety discussion begins with four definitions. They are tested directly in the FRACP and MRCP professional practice papers, and they are the source of most examiner confusion. [1]
Medical error is the failure of a planned action to be completed as intended — an error of execution — or the use of a wrong plan to achieve an aim — an error of planning. An error does not require harm. It may be caught before reaching the patient (a near miss), or it may reach the patient without causing injury. The defining feature is intentionality: the action did not go as intended, or the plan itself was wrong. [1]
Adverse event is an injury caused by medical management rather than by the underlying disease, resulting in prolonged hospital stay, temporary or permanent disability, or death. An adverse event may be preventable (caused by error) or unpreventable (a recognised complication in which no error occurred — for example a true allergic reaction in a patient with no prior exposure). The Harvard Medical Practice Study established the methodology for detecting adverse events by structured record review and is the foundation of modern patient-safety epidemiology. [1]
Near miss is an incident that did not reach the patient, either by chance or because it was intercepted. The pharmacist who catches a tenfold overdose at the dispensing window, the nurse who questions a look-alike drug before administration, the clinical decision support alert that stops a contraindicated prescription — each is a near miss. Near misses are the richest source of latent-condition intelligence because the patient was not harmed and staff report them more freely. A high near-miss reporting rate is a marker of a healthy safety culture, not a marker of a dangerous unit. [1]
Never event (also termed sentinel event) is a serious, largely preventable patient safety incident that should not occur if the available preventions are in place. The canonical examples are wrong-site surgery, wrong-patient surgery, wrong-procedure surgery, retained foreign object (swab, instrument), incompatible blood transfusion, medication error leading to death or severe harm, and suicide of a patient in hospital or within 30 days of discharge. Never events trigger a mandatory organisational response including a full root cause analysis and external reporting to the ACSQHC. [1]
The discriminator the examiner wants
Do not conflate an adverse event with negligence. An adverse event is an injury caused by management. Negligence is a legal finding requiring breach of the standard of care, causation and damage. Many adverse events are unpreventable complications and many do not meet the legal threshold for negligence. Never equate harm with negligence in the disclosure or in the exam answer. [1]
The Swiss cheese model — why the system, not the person
The central model of modern patient safety is James Reason's Swiss cheese model [1]. Hazards in a healthcare system are held back by multiple successive layers of defence: organisational policy, supervision, preconditions (training, equipment, scheduling), and specific defences (allergy checks, independent double-checks, barcode administration). Each layer has holes created by active failures (the errors and violations committed by the sharp-end clinician) and by latent conditions (dormant weaknesses in system design, culture, rostering, equipment).
An adverse event occurs only when the holes in every layer momentarily align, allowing the hazard to pass through. The clinical implication is profound: it is almost never the single act of a single clinician. The prescribing registrar's error was not caught by the pharmacist, was not caught by the nurse, was not caught by the monitoring, and reached the patient — the holes aligned. The durable fix is to build defences in depth rather than to try to make humans infallible. [1]
Active failures versus latent conditions
An active failure is the error or violation committed at the sharp end by the clinician in contact with the patient — the wrong dose prescribed, the site not marked, the result not checked. A latent condition is a dormant weakness in the system that creates the conditions for error — a confusing drug chart design, a fatigued roster, a culture that discourages questioning, a latent interaction not flagged by the decision support. Latent conditions are the higher-leverage target because a single fix prevents many future active failures. [1]
Slips, lapses and mistakes
Reason's taxonomy divides error by cognitive mechanism. A slip is an action-based failure — the plan was right but the execution failed (picking up the wrong syringe, a motor-programme error in a familiar task). A lapse is a memory-based failure (forgetting to check the allergy box, forgetting to give a dose, omitting to act on a result). A mistake is a planning failure — the plan itself was wrong (misdiagnosing and treating for the wrong condition, or applying a correct plan to the wrong patient). Slips and lapses are skill-based errors; mistakes divide into rule-based (the wrong rule applied to a recognised situation) and knowledge-based (the clinician lacked the knowledge to form the right plan). The taxonomy matters because the countermeasures differ: slips are reduced by forcing functions and standardisation, lapses by checklists and prompts, mistakes by decision support, cognitive aids and education. [1]
Error of execution versus error of planning
An error of execution is the failure of a planned action to be completed as intended — intending to give gentamicin but giving the wrong dose. An error of planning is the use of a wrong plan — choosing the wrong antibiotic for the infection. Execution errors are addressed by forcing functions and standardisation; planning errors are addressed by decision support, education and cognitive aids. This is the official definition used in the IOM taxonomy. [1]
Violation versus error
A violation is a deliberate (though usually well-intentioned) deviation from a rule or protocol — bypassing the two-patient-identifier check because "I know the patient", working beyond safe hours, overriding an alert out of habit. An error is unintentional. Routine violations are a warning sign of a poorly designed system (a rule that cannot realistically be followed) and are themselves a latent condition for future error. Reckless violations are a conduct issue managed separately from the systems analysis. The just culture algorithm (below) operationalises this distinction. [1]
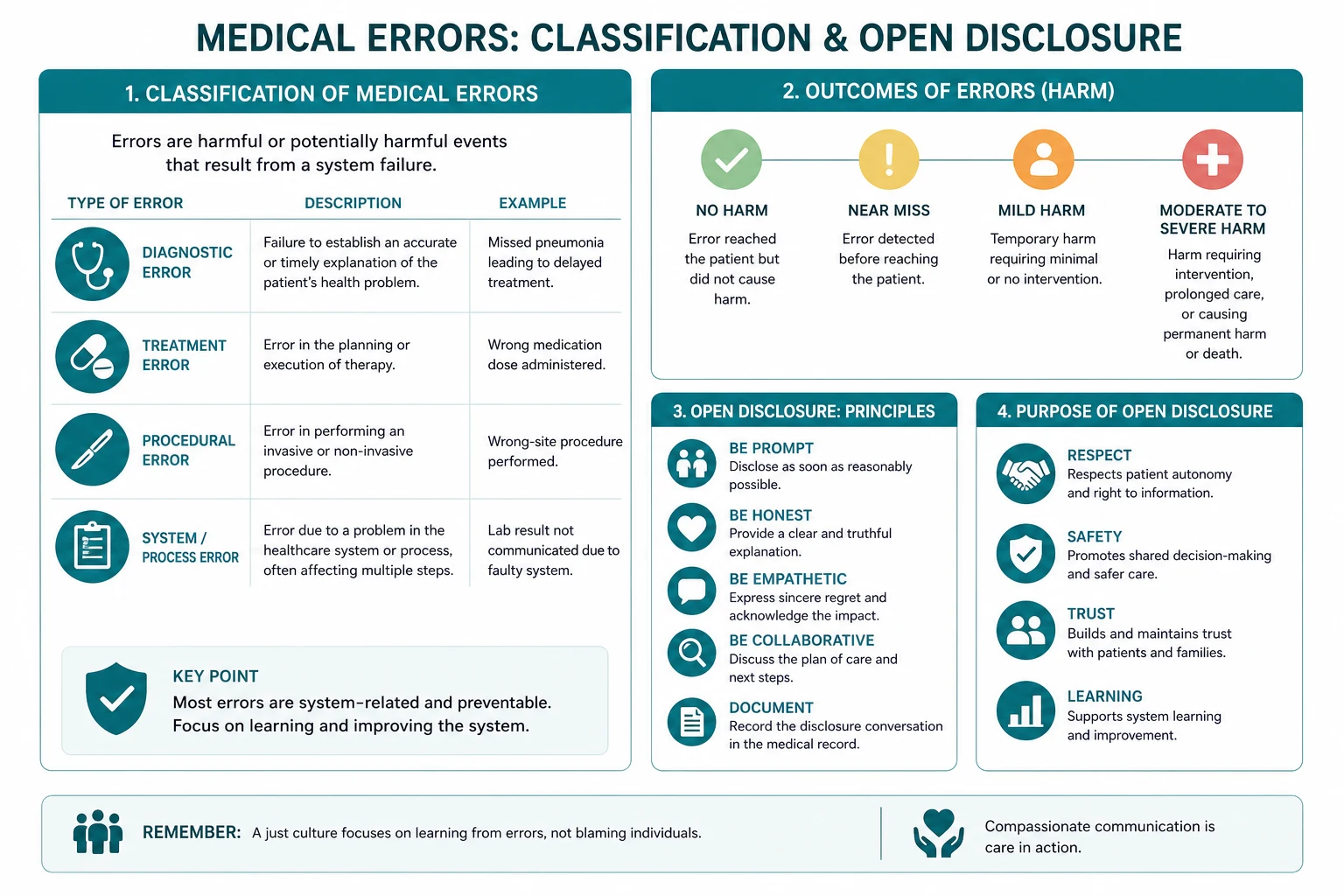
Types of error by stage of care
The standard classification of error by the stage of the patient encounter is the one tested in the FRACP professional practice paper. [1]
Diagnostic error
Diagnostic errors are the leading and most under-recognised category of preventable harm in internal medicine. They include the delayed diagnosis (the pulmonary embolism treated as a COPD exacerbation for 48 hours), the wrong diagnosis (the aortic dissection treated as gastro-oesophageal reflux), the missed diagnosis (the incidental pulmonary nodule on a CT done for another reason that becomes advanced lung cancer two years later), and the failure to order the indicated test (the troponin not sent in a patient with atypical chest pain). Diagnostic errors are dominated by cognitive biases — anchoring, premature closure, availability, confirmation bias — and by system failures in result handling (the critical result sent to no one, or lost in the inbox). [1]
Treatment error
Treatment errors include the wrong drug, the wrong dose, the wrong route, the wrong patient, and the wrong technique. The classic fatal never events sit here: intrathecal vincristine instead of intravenous (a wrong-route error that is uniformly fatal), the tenfold insulin overdose from a misplaced decimal, the look-alike drug (hydralazine versus hydroxyzine), the patient who receives the prescription intended for the same-surname patient in the next bed. Most harmful treatment errors involve failures at more than one stage of the medication use process — prescribing, transcribing, dispensing, administration, monitoring. [1]
Preventive error
Preventive errors are the failure to provide a proven preventive intervention: the failure to vaccinate (the elderly patient not offered the pneumococcal or influenza vaccine), the failure to screen (the patient with atrial fibrillation not assessed for anticoagulation, the patient with diabetes not screened for retinopathy), and the failure to prophylax against a known risk (the inpatient not given venous thromboembolism prophylaxis, the patient on a proton pump inhibitor not given stress ulcer prophylaxis in ICU). Preventive errors are silent — there is no event to recognise, only an omission — which is why audit and reminder systems are the defence. [1]
Other (communication, equipment, system failure)
The "other" category captures the failures that cross stages: the communication failure (the critical handover not given, the discharge summary omitting a new diagnosis), the equipment failure (the infusion pump that free-flows, the monitor that alarms and is silenced), and the system failure (the result-handling system with no recall mechanism, the scheduling system that books two patients into the same slot). Communication failures underlie the majority of serious adverse events and are the single most addressable category by structured handover tools (ISBAR, SBAR). [1]
High-alert medicines — where error concentrates
A small number of drug classes cause a disproportionate share of fatal and serious medication errors because the therapeutic index is narrow and the consequences of error are severe. These are the high-alert medicines, and they concentrate risk that must be defended in depth. [1]
Insulin is the classic. The use of "U" for units (4U read as 44), the trailing zero (5.0 versus 5), and the missing leading zero (.5 versus 0.5) are documented causes of tenfold and greater insulin overdose and of fatal hypoglycaemia. The defence is non-negotiable: write units in full, never use a trailing zero, and always use a leading zero. [1]
Anticoagulants — heparin, warfarin, the direct oral anticoagulants — exemplify the error chain. The prescription is wrong for renal function or weight. The monitoring is not done or the supratherapeutic INR is not acted on. A new antibiotic potentiates the warfarin. A tenfold heparin overdose is given. The evening team is not informed of the rising INR. The patient duplicates the dose at home. The defence is independent double-checks, dose adjustment to renal function, interaction checking in decision support, and patient education at every contact. [1]
Opioids cause respiratory depression and death, especially in the opioid-naive, the elderly, and the patient with hepatic or renal impairment or co-prescribed sedatives. The defence is standardised equianalgesic conversion tables, dose rounding, the use of smart pumps with hard rate limits, naloxone availability, and sedation-and-respiratory-rate monitoring (not sedation alone) on the ward. [1]
Concentrated electrolytes — potassium chloride, hypertonic saline — were historically a leading cause of fatal error when concentrated potassium chloride was stocked on wards and mistaken for normal saline or furosemide. The defence is the removal of concentrated potassium chloride from ward stock entirely, storage in the pharmacy, and the use of premixed standard concentrations. [1]
Chemotherapy, neuromuscular blockers, and sedatives complete the high-alert list. The cross-cutting system defences are independent double-checks (two clinicians independently verifying the drug, dose, route, patient and rate), standardised concentrations, tall-man lettering for look-alike names (DOPamine versus DOBUTamine), and smart pumps with drug libraries and hard dose limits. Computerised physician order entry (CPOE) with clinical decision support — allergy, interaction, dose-range and duplicate-therapy checking — intercepts the error at the prescribing step, though the alerts must be calibrated to avoid alert fatigue that leads clinicians to override them. [1]
Recognising that an adverse event has occurred
The first step is recognition. Many adverse events are missed because the clinical deterioration is attributed to the disease ("the septic patient got worse") rather than to the treatment ("the septic patient was given the wrong antibiotic and the wrong fluid and became overloaded"). [1]
Use a low threshold triggered by:
- unexpected clinical deterioration (the patient on warfarin with a supratherapeutic INR and an intracranial bleed);
- a complaint from the patient or family;
- an incident report from a staff member;
- a discrepancy between the expected and the actual clinical course;
- an unexpected return to theatre or readmission;
- the global trigger tool — a structured record review that identifies signs of harm such as a new fall, a new pressure injury, an unplanned transfer to ICU, an unexpected halt in sedation, or a new unplanned drug to treat a side effect. [1]
Classifying severity
Severity is classified on a validated scale. The NCC MERP index for medication errors grades events A through I — from circumstances that could cause harm (A) through an error that reached the patient but caused no harm (E) to an error that contributed to or caused the patient's death (I). The WHO International Classification for Patient Safety grades harm as none, mild, moderate, severe, or death. The severity classification determines the disclosure intensity, the reporting pathway, and the level of investigation (from local review through to a full root cause analysis). [1]
The immediate response — clinical priority first
When an adverse event is recognised, the clinical priority always precedes the disclosure and the investigation. [1]
- Stabilise and treat the patient. Apply the ABC of the harm caused — oxygen, fluids, reversal agents (naloxone for opioid overdose, 50 per cent dextrose for insulin overdose, protamine for heparin overdose, vitamin K and prothrombin complex concentrate for warfarin reversal), resuscitation, and escalation to a higher level of care. The harm caused by the error is treated exactly as if the same clinical state had arisen from any other cause.
- Preserve the evidence. Do not discard the equipment or the drugs. Secure the relevant medication chart and chart entries. Retain any implicated device (the infusion pump, the syringe, the blood bag). The investigation will need them.
- Inform the senior clinician in charge and the treating team. The consultant, the nurse unit manager, and (for serious events) the executive on call must be informed. For a serious adverse event, notify the medical defence organisation before any formal statement is made. [1]
The Australian Open Disclosure Framework
The Australian Open Disclosure Framework (ACSQHC, 2013) is the national standard for open and honest communication with patients when things go wrong. It is operationalised through the National Safety and Quality Health Service Standards — Standard 1 (Clinical Governance) requires incident management and open disclosure systems, and Standard 2 (Partnering with Consumers) requires patient and family involvement. The Standards are mandatory for accreditation of all Australian hospitals and day procedure services, which makes open disclosure a requirement of doing business, not an optional courtesy. [1]
The four elements of disclosure
Whatever the jurisdiction, the four elements are constant. Disclosure must include: [1]
- an apology — an expression of regret for what happened and for its impact on the patient; it is explicitly NOT an admission of legal liability;
- a factual explanation — a plain-language account of what is known, what is not yet known, and what is being done to find out;
- an acknowledgement — a recognition of the impact on the patient and their family, and a genuine engagement with their experience;
- a plan to prevent recurrence — what is being done and what will be done differently. [1]
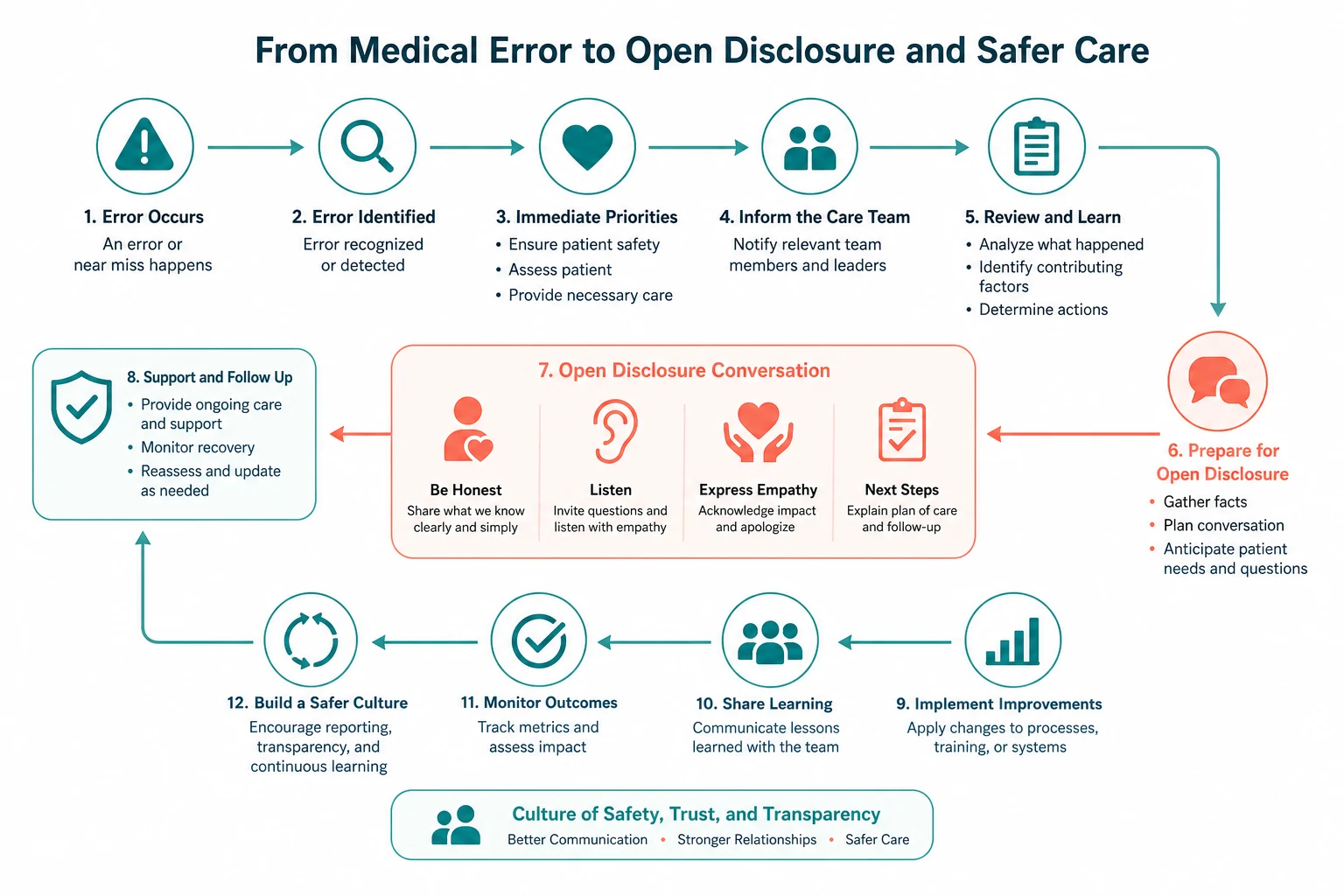
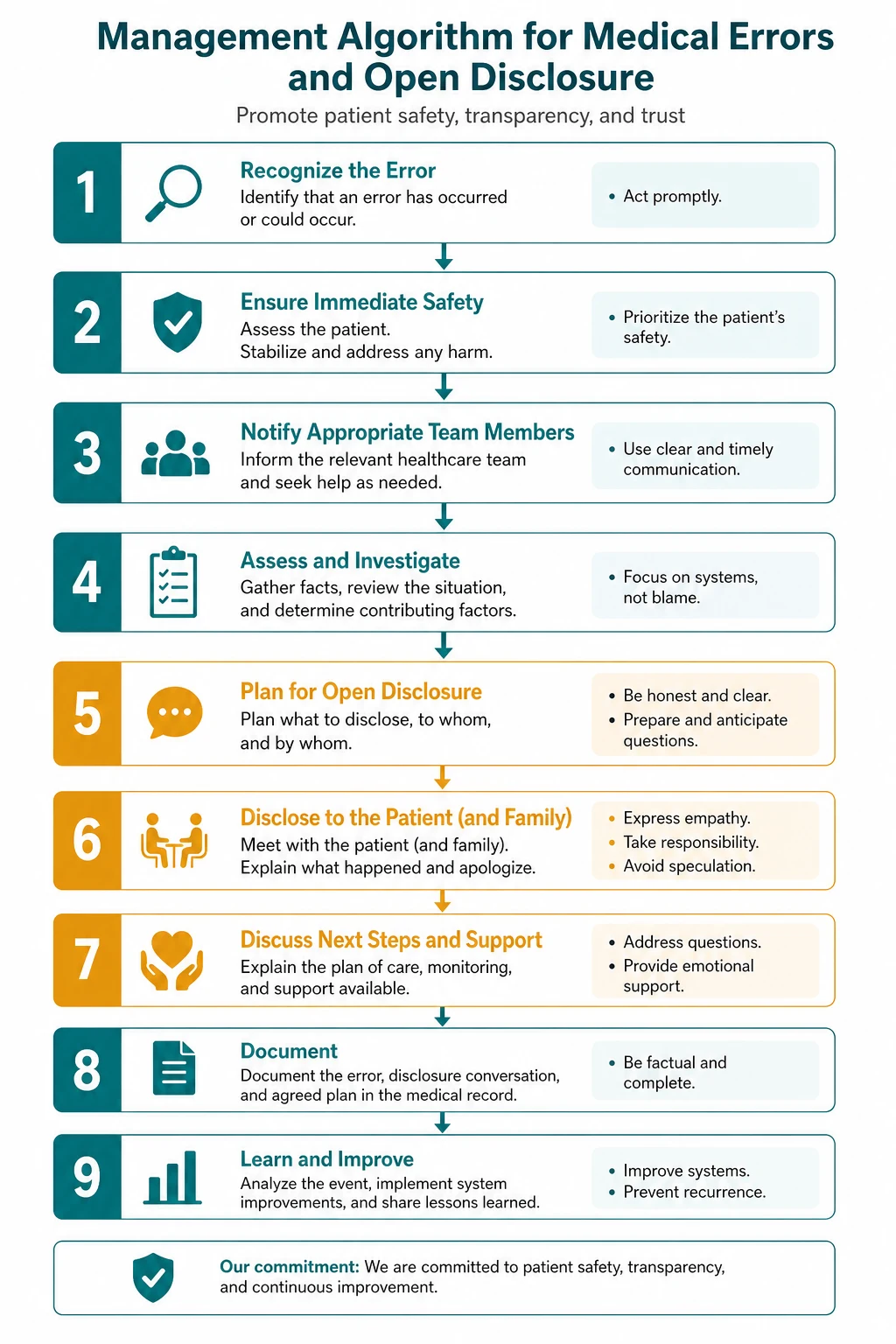
The staged process
The framework is staged, recognising that the facts evolve. [1]
Stage 1 — Identify the incident. Recognise the adverse event, provide immediate clinical care, notify the team and the senior clinician, and make the decision to disclose. The recognition step is the responsibility of every clinician, not just the consultant. [1]
Stage 2 — Initial disclosure. Conduct an initial conversation as soon as practicable after the event (ideally within hours, certainly within 24 hours). State the facts as they are currently known, apologise, explain what is being done to investigate and to prevent recurrence, and arrange the follow-up. Do not speculate about the cause. Do not blame a colleague. [1]
Stage 3 — Ongoing communication. Keep the patient and family informed as the investigation proceeds. Provide a single point of contact. Answer questions honestly. [1]
Stage 4 — Formal open disclosure meeting. Once the facts are established, conduct the formal discussion. Present the full factual account, acknowledge the impact, explain the root causes, describe the actions taken to prevent recurrence, and offer ongoing support. This meeting is the one the patient will remember. [1]
Stage 5 — Follow-up. Provide the written outcome of the investigation, confirm the actions taken, offer continued support (a second opinion, counselling, advocacy), and document the entire process in the medical record. [1]
The apology — not an admission of liability
The most-tested fact in this area is that an apology is NOT an admission of legal liability. The civil liability legislation of the Australian states expressly provides that an expression of regret or apology is not an admission of liability and is not admissible as evidence of liability. The Australian Open Disclosure Framework restates this. The ethical duty of candour requires the apology; the law protects it; and the evidence shows that open disclosure with a genuine apology reduces the number and value of civil claims [3].
The largest single driver of complaints and litigation is not the harm itself but the perception of a cover-up — the patient who was not told, who felt dismissed, who had to discover the error by chance. Open disclosure addresses that driver directly. [1]
The duty of candour
The duty of candour is the ethical and, in many jurisdictions, the legal obligation on the clinician and the organisation to be open and honest with a patient when something has gone wrong. [1]
The ethical duty derives from the four principles of biomedical ethics. Autonomy holds that the patient has a right to know what has happened to them, to make informed decisions about ongoing care and about whether to seek redress. Beneficence holds that the duty to act for the patient's welfare includes restoring trust and supporting recovery after harm. Non-maleficence holds that concealment is a harm — it compounds the original injury with deception and prevents the patient from seeking appropriate further care. Justice holds that honesty in the health system requires that those harmed are identified and that the system is improved for others. [1]
The legal duty varies by jurisdiction. In England the statutory duty of candour (Regulation 20 of the Health and Social Care Act 2008 Regulated Activities Regulations 2014) imposes a legal requirement on registered providers to notify and apologise for notifiable safety incidents, with penalties for breach. In Australia the duty is given effect through the National Safety and Quality Health Service Standards and the Australian Open Disclosure Framework, which are conditions of accreditation. The ethical duty is universal and predates the legal duty. [1]
Root cause analysis — investigating the system
A root cause analysis (RCA) is the structured investigation of a serious adverse event. The aim is to find out what happened, why it happened, and how to prevent it happening again — at the level of the system, not the individual. [1]
The RCA process follows a defined sequence. First, define the event and its impact — a clear statement of what happened and the harm caused. Second, gather and timeline the data — chronologically reconstruct the event from the record, the device logs, the interviews with all involved staff. Third, identify the contributory factors using a structured framework. The London Protocol (Vincent and colleagues) provides seven contributory factor domains: patient factors, task factors, individual factors, team factors, environment, organisation, and institutional context. Fourth, distinguish active failures from latent conditions — the active failure is the last hole to align; the latent conditions are the deeper system defects. Fifth, ask why iteratively (the "five whys") until the root causes are reached. Sixth, generate and prioritise recommendations that address the root causes. Seventh, assign owners and timelines for implementation and audit the implementation. [1]
The London Protocol contributory factors
When you present a contributory-factor analysis in a viva, use the seven domains. Patient factors: the patient's complexity, comorbidities, communication, language. Task factors: the design of the task, the availability of protocols, the use of checklists. Individual factors: the clinician's knowledge, skill, experience, fatigue, stress. Team factors: communication, leadership, role clarity, handover. Environment: the physical environment, the equipment, the staffing, the workload. Organisation: the culture, the policy, the training, the incentive structures. Institutional context: the regulatory, economic, and political environment. The exam discriminator is the ability to move beyond blame of the individual to the system. [1]
Human Factors Analysis and Classification System (HFACS)
For the most serious events, the Human Factors Analysis and Classification System (HFACS) structures the investigation in four tiers, moving up from the sharp end to the blunt end. The first tier is unsafe acts (errors and violations). The second is preconditions for unsafe acts (the condition of operators — fatigue, stress — and the practices and environment). The third is unsafe supervision (inadequate supervision, planned inappropriate operations, failure to correct known problems). The fourth is organisational influences (resource management, organisational climate, organisational process). HFACS forces the investigation to the organisational level where the most durable fixes live. [1]
The just culture and the second victim
The just culture algorithm
A just culture is the precondition for a reporting culture and for any sustainable patient-safety improvement. It distinguishes three kinds of behaviour and matches each to a distinct response. [1]
- Human error (an inadvertent slip, lapse, or mistake) is consoled — the clinician is supported, and the system that allowed the error is fixed.
- At-risk behaviour (a shortcut the clinician did not realise was risky) is coached — the clinician is counselled, and the inducement to the shortcut is removed.
- Reckless behaviour (a conscious disregard of a substantial and unjustifiable risk) is managed — remedial action, a performance plan, or discipline. [1]
The algorithm prevents both the blame culture (which scapegoats a clinician for a system failure, drives concealment, and guarantees recurrence) and the no-blame culture (which excuses a clinician who needs individual management and fails to protect patients from reckless conduct). The just culture is the answer the examiner wants when the probing question is "what do you do about the individual." [1]
The second victim
The second victim is the clinician involved in the adverse event. The first victim is the patient. The second victim is the clinician. The phenomenon is common — a majority of involved clinicians report acute distress in surveys — and is under-recognised. The course is predictable: an acute distress reaction in the days after, intrusive thoughts and self-doubt, loss of clinical confidence, defensive practice, burnout, depression, and, in documented series, an increased risk of suicidal ideation. [1]
Management is a professional obligation. Immediate peer support. Timely access to debriefing. Removal of blame within a just culture. Access to an employee assistance programme and to the medical defence organisation. A structured re-entry to practice. Failing to support the second victim is itself a patient-safety risk, because the distressed clinician is more error-prone — and it drives concealment, burnout, and attrition. [1]
Reporting and medico-legal pathways
The internal incident report
Every adverse event, near miss, and never event is reported to the organisation's incident management system, regardless of perceived severity. The report triggers the local severity assessment, which determines the level of investigation (from local review through to a full RCA). The aggregate of reports is analysed for patterns and trends that single-event review cannot detect. Under-reporting is the norm and is itself a safety risk; a unit with a low reporting rate is not a safe unit but a unit that is not surfacing its errors. [1]
AHPRA mandatory notification
The AHPRA mandatory notification framework requires a treating practitioner to notify AHPRA when they form a reasonable belief that a registered health practitioner has engaged in notifiable conduct. The four categories of notifiable conduct are: [1]
- Practising while intoxicated by alcohol or drugs.
- Sexual misconduct in connection with the practice of the profession.
- Placing the public at risk of substantial harm because of an impairment (physical or mental).
- A significant departure from accepted professional standards of practice. [1]
The threshold is public protection, not peer disapproval. The report is to AHPRA, not to the police. Mandatory notification is distinct from the internal incident report — the incident report is an internal organisational learning tool; the AHPRA notification is a report to the regulator about a practitioner's fitness to practise. The two pathways run in parallel and have different thresholds and different purposes. [1]
Coronial referral
A death is reportable to the coroner if it is:
- unexpected — not reasonably expected by the treating team;
- unnatural or violent;
- the identity of the deceased is unknown;
- it occurred during a medical procedure or as a result of an anaesthetic (and is not due to natural causes in a patient with a known condition for which the procedure or anaesthetic was a recognised treatment);
- it occurred in custody or care. [1]
A death attributable to an adverse event or medical error is reportable. The duty is to report — not to investigate or to conclude. The medical record and any equipment must be preserved. The body must not be cremated. The ordinary death certificate must not be issued until the coronial process has run. The treating clinician notifies the coroner, who decides whether to accept jurisdiction and whether to request an autopsy, a statement, or an inquest. [1]
The medical defence organisation
Notify the medical defence organisation (MDO) as soon as a serious adverse event, a complaint, or a potential claim arises, and before any formal statement. The MDO provides medico-legal advice, may appoint a solicitor, supports the clinician through the disclosure and the investigation, and indemnifies covered claims. Early notification protects the clinician and does not prejudice the patient, because the disclosure and clinical care continue independently. The MDO is your ally, not your adversary. [1]
Complaint, claim, and mandatory notification — three distinct pathways
These three are distinct and often confused. A complaint is an expression of dissatisfaction (to the health service, to the complaints commissioner, to AHPRA) about care. A claim is a formal demand for compensation, usually pleaded in negligence (requiring duty of care, breach of the standard of care, causation and damage). A mandatory notification is a report to the regulator about a practitioner's conduct, performance or health that meets the notifiable threshold. The three pathways are distinct, run in parallel, and require different documentation and different responses. [1]
Clinical governance — the system that holds it together
Clinical governance is the framework through which a healthcare organisation is accountable for the quality and safety of the care it provides. Its components are the machinery that makes patient safety real. Incident reporting surfaces the events. Morbidity and mortality (M and M) meetings review the deaths and the serious complications for learning across the team. Audit measures practice against a standard and feeds back for improvement. Peer review exposes individual practice to constructive challenge. Accreditation (against the NSQHS Standards in Australia) holds the organisation to account externally. A physician who understands clinical governance knows not only how to manage the single event but how to change the system that produced it. [1]
Communication
The disclosure conversation, step by step
Structure the disclosure conversation deliberately. Choose a private setting. Ensure the right people are present — the patient, a support person, the treating clinician, and (for formal disclosure) an open disclosure facilitator. Open with an acknowledgement and an apology. Give a factual, plain-language account of what is known and what is not yet known. Acknowledge the impact on the patient. State what is being done to investigate and to prevent recurrence. Offer support — a second opinion, counselling, independent advocacy. Invite questions. Agree on the next contact. Document the conversation in the medical record. [1]
Delivering the apology without admitting liability
The apology is an expression of regret for what happened and for the impact on the patient. It is not an admission of fault or of legal liability. The civil liability legislation of the Australian states expressly provides that an apology is not an admission of liability and is not admissible as evidence of liability. The apology is ethically required, psychologically healing for the patient, and legally protected. [1]
Communicating with the family when the patient has died
Identify the legal substitute decision-maker. Conduct the disclosure with them and their support person. Maintain the same principles — apology, facts, acknowledgement, support, plan. Be alert to the heightened grief and anger that a death causes. Do not attribute blame to an individual clinician in the family's presence. The second-victim clinician should generally be supported by a senior colleague rather than facing the family alone. [1]
The colleague whose error you have witnessed
Address it directly but privately, without blame — the "cup of coffee" conversation. Focus on the system that allowed the error and on the shared duty to the patient. Support the colleague as a second victim. Escalate through the clinical governance pathway if the error caused harm. The just culture principle is that human error is consoled, at-risk behaviour is coached, and reckless behaviour is managed. [1]
A complaint after an adverse event
Acknowledge it promptly. Meet with the patient and family. Listen for the underlying driver — harm, not being told, dismissiveness. Apologise where the service fell short. Explain what happened. Offer a remedy where appropriate. Report through the complaints and incident systems. Feed back the outcome. The majority of complaints are resolved by honest communication and a genuine apology, and the minority that proceed to formal claims are reduced in number and value by early open disclosure. [1]
Regional guideline anchoring
The ANZ primary framework is the Australian Commission on Safety and Quality in Health Care (ACSQHC), which publishes the Australian Open Disclosure Framework and the National Safety and Quality Health Service Standards. The AHPRA mandatory notification framework governs reporting of practitioner conduct, performance and health. The coronial framework is state-based but concordant across Australian jurisdictions. The UK secondary framework is the NHS England statutory duty of candour (Regulation 20 of the 2014 Regulations), the General Medical Council's Good Medical Practice (2024) duty of candour, and the Care Quality Commission's enforcement of the duty. The US tertiary framework is the AHRQ Communication and Optimal Resolution (CANDOR) toolkit, which operationalises disclosure with immediate response, fact-finding, explanation and offer. The global framework is the WHO Patient Safety programme and the Global Patient Safety Action Plan 2021 to 2030. The principles are concordant across regions: honest, timely, supported disclosure; an apology that is not an admission of liability; a factual account; a prevention plan; and a just culture that supports the second victim. [1]
The high-yield exam traps
- The most common error is to treat the disclosure as an admission of legal liability. An apology (an expression of regret) is explicitly NOT an admission of liability under Australian civil liability legislation and under the open disclosure framework. Candidates who withhold an apology for fear of liability breach the ethical and (in many jurisdictions) legal duty of candour and paradoxically increase the likelihood of a claim.
- The most common classification error is to conflate an adverse event with negligence. An adverse event is an injury caused by management. Negligence is a legal finding requiring breach of the standard of care, causation and damage. Never equate harm with negligence in the disclosure or the exam answer.
- The most common system error is to treat the event as the fault of the individual at the sharp end. The Swiss cheese model teaches that the active failure is the last hole to align. The durable fixes are the latent conditions. Candidates who name only the individual and not the system have failed to understand the modern patient-safety paradigm [1].
- The most common medico-legal error is to complete the death certificate and release the body after a death attributable to an adverse event. Such a death is reportable to the coroner. The duty is to report, the record and any equipment must be preserved, and the ordinary death certificate must not be issued until the coronial process has run.
- The most common reporting error is to confuse the internal incident report with the AHPRA mandatory notification. The incident report is an internal organisational learning tool. The AHPRA notification is a report to the regulator about a practitioner's notifiable conduct. The two are distinct and the thresholds are different.
- The most common investigation error is to conduct a blame-finding inquiry rather than a root cause analysis. The RCA asks why iteratively until the system root causes are reached. An RCA that stops at "the nurse made a mistake" has failed and will not prevent recurrence.
- The most common communication error in disclosure is to speculate about the cause or to blame a colleague before the investigation is complete. The disclosure states what is known factually, what is not yet known, and what is being done. Speculation and blame are prohibited, they inflame the patient and family, they damage colleagues, and they are medico-legally hazardous.
- The most common prescribing error is the insulin abbreviation, the trailing zero, and the missing leading zero. Write units in full, never use a trailing zero, always use a leading zero. These are non-negotiable prescribing standards, not optional conventions.
Why this matters — the scale of the problem
The modern patient-safety movement was launched by the IOM report To Err is Human (1999), which estimated 44,000 to 98,000 US deaths annually from medical error. Makary and Daniel [2] re-estimated the figure at more than 250,000 US deaths per year — if correct, medical error is the third leading cause of death in the United States, behind only heart disease and cancer. The estimate is contested (the methodology extrapolates from heterogeneous studies and the preventability of any individual death is hard to determine), but the direction is clear: medical error is a leading cause of preventable death, and most of those deaths are preventable by system change, not by exhorting clinicians to be more careful. The Studdert analysis of US malpractice claims [4] confirmed that the claims and the compensation are concentrated in a small number of high-severity injuries, and that disclosure and early resolution reduce both. The reviews of open disclosure [5][6] converge on the same finding: while open disclosure is universally endorsed in policy, the gap between policy and practice is wide, the barriers are fear of litigation and a blame culture, and the patient needs are a sincere apology, timely information, and assurance that recurrence will be prevented. Closing that gap is the professional obligation of every physician.
References
- Reason J. Human error: models and management. BMJ 2000;320:768-770. PMID 10720363.
- Makary MA, Daniel M. Medical error — the third leading cause of death in the US. BMJ 2016;353:i2139. PMID 27143499.
- Studdert DM, Mello MM, Gawande AA, Brennan TA, Wang YC. Disclosure of medical injury to patients: an improbable risk management strategy. Health Aff (Millwood) 2007;26:215-226. PMID 17211031.
- Studdert DM, Mello MM, Gawande AA, Gandhi TK, Kachalia A, Yoon C, Puopolo AL, Brennan TA. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med 2006;354:2024-2033. PMID 16687715.
- Gallagher TH, Studdert D, Levinson W. Disclosing harmful medical errors to patients. N Engl J Med 2007;356:2713-2719. PMID 17596606.
- Rathnayake D, Sasame A, Radomska A, She EN, McAuliffe E, De Brun A. What can we learn from patient and family experiences of open disclosure and how they have been evaluated? A systematic review. BMC Health Serv Res 2025;25:238. PMID 39939873. [1]
Framework references (not PMID-indexed): Australian Commission on Safety and Quality in Health Care, Australian Open Disclosure Framework (2013). ACSQHC, National Safety and Quality Health Service Standards, 2nd edition (2017). AHPRA, Mandatory notifications: When to make a mandatory notification about a health practitioner. AHRQ, Communication and Optimal Resolution (CANDOR) toolkit. WHO, Global Patient Safety Action Plan 2021-2030. IOM (Kohn LT, Corrigan JM, Donaldson MS, eds.), To Err is Human: Building a Safer Health System (Washington DC: National Academy Press, 1999). Vincent C, Amalberti R, Safer Healthcare (Springer, 2016). Reason J, The Human Contribution (Ashgate, 2008). Marx D, Patient Safety and the Just Culture (2001). Vincent C et al, The London Protocol (contributory factors for RCA). WHO, International Classification for Patient Safety. NCC MERP, Index for Categorizing Medication Errors. UK Health and Social Care Act 2008 (Regulated Activities) Regulations 2014, Regulation 20 (statutory duty of candour). [1]
References
- [1]Reason J Human error: models and management BMJ, 2000.PMID 10720363
- [2]Makary MA, Daniel M Medical error-the third leading cause of death in the US BMJ, 2016.PMID 27143499
- [3]Studdert DM, Mello MM, Gawande AA, Brennan TA, Wang YC Disclosure of medical injury to patients: an improbable risk management strategy Health Aff (Millwood), 2007.PMID 17211031
- [4]Studdert DM, Mello MM, Gawande AA, Gandhi TK, Kachalia A, Yoon C, Puopolo AL, Brennan TA Claims, errors, and compensation payments in medical malpractice litigation N Engl J Med, 2006.PMID 16687715
- [5]Gallagher TH, Studdert D, Levinson W Disclosing harmful medical errors to patients N Engl J Med, 2007.PMID 17596606
- [6]Rathnayake D, Sasame A, Radomska A, She EN, McAuliffe E, De Brun A What can we learn from patient and family experiences of open disclosure and how they have been evaluated? A systematic review BMC Health Serv Res, 2025.PMID 39939873