Phys · general-medicine
Medical Ethics, Capacity and Consent
Also known as medical ethics · bioethics · capacity assessment · decision-making capacity · competence · informed consent · advance care planning · advance directive · advance care directive · substitute decision-maker · best interests · confidentiality · mandatory reporting · Beauchamp and Childress · four principles · Mental Capacity Act 2005
Consultant-physician-depth guide to medical ethics, capacity and consent for FRACP DWE and DCE — the four principles of biomedical ethics (Beauchamp and Childress: autonomy, beneficence, non-maleficence, justice), the functional two-stage test of capacity (understanding, retaining, using and weighing, communicating — Appelbaum 2007), the presumption of capacity and its decision-specific and time-specific nature, valid consent (informed, voluntary, capacitous), treatment without consent (emergency doctrine of necessity, mental health legislation, court order), advance care planning (binding advance refusals, values statements, ceilings of treatment, not-for-resuscitation orders that do not abandon), confidentiality and its limits (mandatory reporting, imminent risk, court order), and professional regulation (AHPRA, GMC, revalidation) — with the SPIKES protocol, the Mental Capacity Act 2005 five principles, and the ANZ guardianship and substitute decision-maker framework.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Medical Ethics, Capacity and Consent

The answer first
Medical ethics is the structured reasoning a physician applies when there is a genuine tension between duties — to respect the patient's voice, to act in their interest, to avoid harm, and to be fair. The framework you use in every FRACP ethics question is the four principles of biomedical ethics published by Beauchamp and Childress in 1979: autonomy (respect the patient's informed, voluntary decisions, including refusals), beneficence (act for the patient's welfare), non-maleficence (avoid harm), and justice (treat like cases alike, distribute resources fairly). These principles do not give you the answer — they give you a disciplined way to name the conflict and reach a defensible decision. [1]
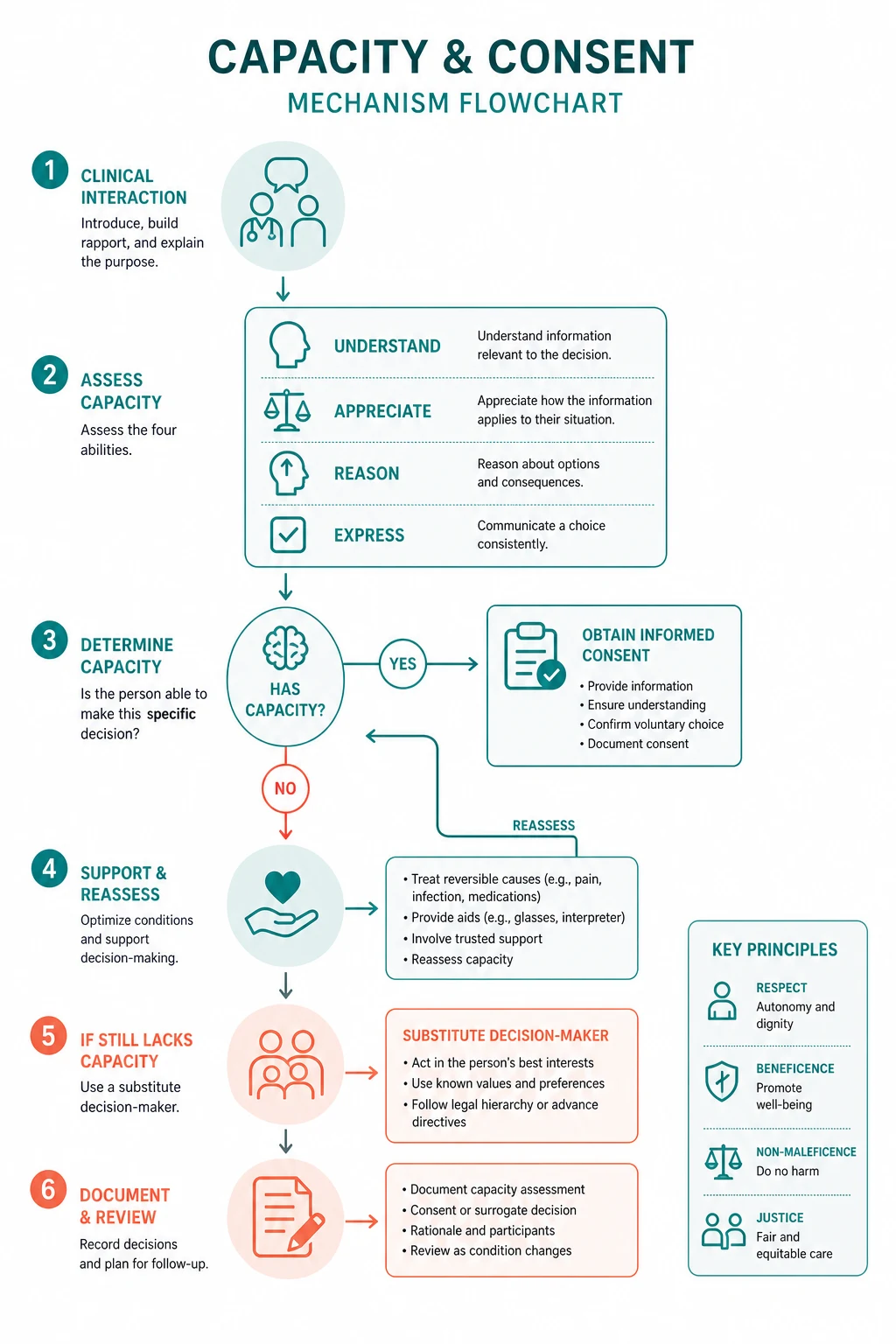
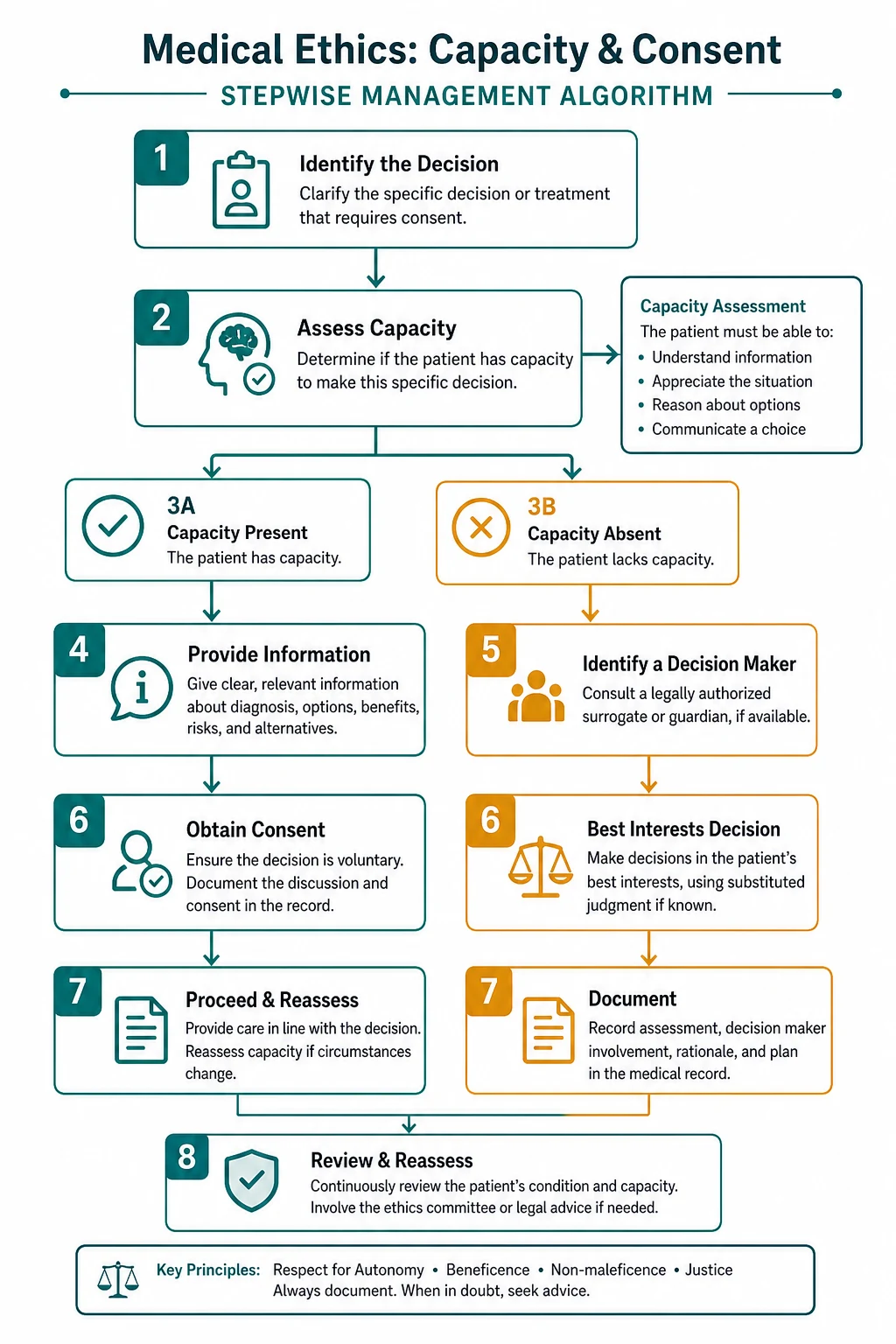
The two most examinable skills beneath the principles are capacity assessment and valid consent. Capacity is presumed in every adult, is decision-specific and time-specific, and is assessed by a two-stage functional test — first, is there an impairment or disturbance of mind or brain, and second, does that impairment make the person unable to make the specific decision [1]? Unable means failing one or more of the four functional abilities: understanding the information, retaining it long enough to decide, using or weighing it as part of the decision, and communicating the choice by any means. Valid consent requires three pillars: the patient has capacity for that decision, the consent is informed (nature, purpose, risks, benefits, alternatives, consequences of no treatment), and it is voluntary (free from coercion or undue influence).
The three situations where consent is not required are the doctrine of necessity (life-saving treatment for a patient who lacks capacity and where delay threatens death or serious harm, and no prior valid refusal exists), statutory authority (mental health legislation permitting involuntary treatment of the mental illness, and public health legislation for notifiable disease), and a court order. Everything else — every procedure, every blood transfusion, every medication — requires consent. [1]
DWE high-yield: The single most tested concept is that a capacitous adult can refuse any treatment, including life-saving treatment, and that refusal must be respected. The second is that capacity is decision-specific — a patient may have capacity to consent to a blood test but not to refuse a below-knee amputation. The third is the two-stage test (diagnostic then functional) and the four functional abilities (understand, retain, use or weigh, communicate). [1]
1. The four principles of biomedical ethics

Beauchamp and Childress proposed four prima facie principles — duties that bind unless they conflict, in which case the clinician must balance them and justify the balance. The principles are a common-morality framework: they reflect values that most moral traditions accept, which is why they travel across cultures and jurisdictions. [1]
Autonomy — respect for the patient's self-determination
Autonomy is the duty to respect a competent patient's informed, voluntary choices about their own body and life. In clinical practice it generates the requirements of informed consent, of truth-telling (honest prognostic information), of confidentiality (the patient controls their information), and of respecting refusals — even refusals of life-sustaining treatment that the clinician considers unwise. The crucial caveat is that autonomy is not a blank cheque: it attaches to a patient who has capacity for the decision. A confused, coerced or panicked patient is not exercising autonomy when they assent or refuse; they need protection. [1]
Registrar teaching point: Autonomy does not mean "the patient gets whatever they ask for". A patient may autonomously refuse a treatment you recommend; they may not autonomously demand a treatment that is not clinically indicated, because that is not a decision about their own body but a request that you act against your professional judgement. The principle that bounds autonomy here is non-maleficence and the integrity of the profession. [1]
Beneficence — act for the patient's welfare
Beneficence is the positive duty to act in the patient's best interest — to relieve suffering, to cure disease, to prevent deterioration, to comfort. It is what draws doctors to medicine. It frequently runs alongside autonomy (the patient consents to the treatment that benefits them), but when they conflict — a patient who would benefit from a treatment they refuse — autonomy prevails for a capacitous adult. Beneficence alone (acting for the patient's good) never justifies overriding a capacitous refusal. [1]
Non-maleficence — do no harm
Non-maleficence (primum non nocere) is the duty to avoid causing harm. It is distinct from beneficence because the obligation to not harm is more stringent than the obligation to do good. Every intervention with a risk of harm (surgery with mortality, chemotherapy with toxicity, a blood transfusion with a small risk of reaction) must be justified by a proportionate expected benefit — the risk-benefit balance that you explain in the consent conversation. Non-maleficence is also the principle behind the doctrine of double effect (touched on in the palliative care topic): an action with a foreseen but unintended harmful consequence (sedation, a shorter survival) is permissible when the intended consequence (relief of refractory suffering) is good and proportionate. [1]
Justice — fairness in distribution and process
Justice in medical ethics is principally distributive justice — the fair allocation of scarce healthcare resources (ICU beds, transplant organs, expensive biologics) — but it also includes procedural justice (like cases treated alike, access without discrimination) and the social determinants of health. Triage decisions, fair innings arguments, and prioritisation frameworks all invoke justice. A justice dilemma every physician faces is whether a scarce or costly intervention should be offered equally to all who might benefit or preferentially to those most likely to benefit. [1]
DWE discriminator: When a stem describes a conflict, name the principles in tension before choosing the answer. A patient refusing dialysis is autonomy-versus-beneficence — for a capacitous adult, autonomy wins. A request to withhold a ventilator from one patient because another patient needs it is justice — it must follow a transparent triage protocol, not an ad hoc judgement. [1]
2. Capacity — the functional two-stage test
Capacity is the gateway to autonomy: a patient can only make a binding decision if they have capacity for that decision. The law presumes capacity in every adult, and the burden is on the clinician asserting incapacity to demonstrate it [1][2].
The presumption of capacity
Every adult patient is presumed to have capacity unless the contrary is shown. Three operational consequences follow. First, unwise decisions do not equal incapacity — a patient may make a decision the clinician considers foolish, irrational or self-harming, and capacity is intact unless a functional impairment of mind or brain explains the decision. Second, capacity is not lost by diagnosis — a diagnosis of dementia, schizophrenia, bipolar disorder, intoxication or delirium raises a flag to assess, but does not by itself establish incapacity. Third, the patient must be given practicable help to decide — explain in plain language, use an interpreter, support communication (hearing aids, glasses, a speech-and-language therapist, pictures), and treat reversible barriers (pain, hypoxia, sepsis, sedation) before concluding the patient lacks capacity. [1]
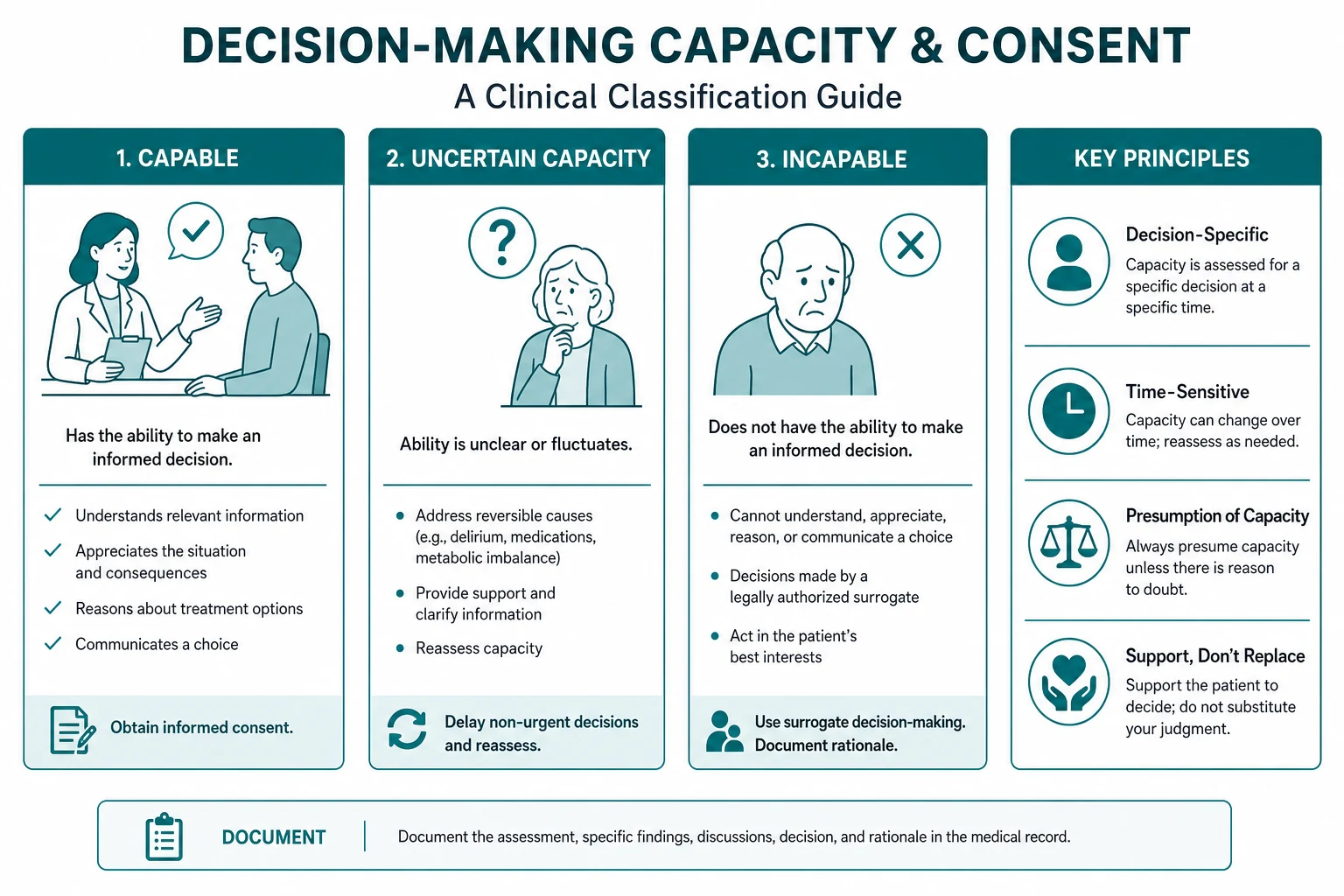
Capacity is decision-specific
A patient may have capacity for one decision and not another. The threshold of understanding scales with the stakes and the complexity of the decision. A patient with mild cognitive impairment may have capacity to consent to a venepuncture (low stakes, simple information) but lack capacity to consent to a below-knee amputation for critical limb ischaemia (high stakes, complex trade-offs of risk against benefit, irreversible). The corollary is that you assess capacity for the specific decision in front of you, not "capacity in general". A common exam trap is a question implying a patient lacks capacity for everything because they lack it for one decision. [1]
Capacity is time-specific
Capacity fluctuates. Delirium, intoxication, sedation, the post-ictal state, a manic episode, a depressive crash, and even the immediate aftermath of receiving bad news can transiently impair capacity. The rule is to defer non-urgent decisions until capacity is restored, and to treat the reversible cause (the sepsis, the opioids, the metabolic derangement). For urgent decisions that cannot wait, treat under the doctrine of necessity (below) and reassess. For decisions that must be made in a window of lucidity (a dementia patient with fluctuating capacity), arrange the conversation for the patient's best time of day and document carefully. [1]
The two-stage test
The Mental Capacity Act 2005 (England and Wales) crystallised the test into two stages, and this structure is now used in UK and increasingly in ANZ and North American practice. [1]
Stage 1 — the diagnostic stage. Is there an impairment of, or disturbance in the functioning of, the mind or brain? This covers delirium, dementia, intoxication, psychosis, depression, learning disability, acquired brain injury, the effect of sedatives or opioids, and the acute confusion of severe illness. If there is no impairment, the patient has capacity — the test stops. If there is an impairment, you proceed to the functional stage. [1]
Stage 2 — the functional stage. Does the impairment make the person unable to make the specific decision? "Unable" means the patient fails one or more of the four functional abilities described below. If any one ability is absent because of the impairment, the patient lacks capacity for that decision at that time. [1]
The four functional abilities
The four abilities — established by Appelbaum and Grisso and codified in the MacArthur Competence Assessment Tool (MacCAT-T) [2][3] — are the clinical content of capacity assessment. Each must be tested directly.
- Understanding — can the patient paraphrase the relevant information in their own words? This includes the nature of the condition, the proposed treatment, the principal risks and benefits, the reasonable alternatives, and the consequences of declining. You must explain the information in plain language, free of jargon, in small chunks, and then ask the patient to tell you back what they have understood. A nod is not understanding.
- Retaining — can the patient hold the information long enough to weigh it and decide? The information need not be retained indefinitely, but must be held for the decision. A patient with severe short-term memory impairment who cannot keep the relevant facts in mind for even a few minutes may fail this ability. (Where retention is impaired but the patient is consistent over time when the information is re-presented, some jurisdictions accept that capacity may be intact — a nuance the examiner may probe.)
- Using or weighing — can the patient use the information as part of the process of deciding? This is the most often missed ability at the bedside. A patient who can parrot the risks but then reasons in a way that shows they have not integrated the information into the decision (for example, refusing surgery because they believe the surgeons are trying to poison them, or because a depressive illness makes them believe they deserve to die) fails to use or weigh. Beliefs arising from the mental illness itself — delusions about the treatment, nihilism in severe depression — indicate failure of this ability.
- Communicating — can the patient communicate the decision by any means (speech, writing, sign, gesture, communication aid)? A patient who is intubated, has expressive aphasia, or is too weak to speak may still be able to communicate a choice by blinking, nodding or using a letter board. Failure to communicate because the patient cannot be understood, not because they have no view, is failure of this ability. [1]
DWE discriminator: The single highest-yield capacity fact is the four abilities. A stem will give you a patient who can repeat the information but then bases their refusal on a delusional belief, and the answer is that they lack capacity because they cannot use or weigh the information. Another classic is the patient with severe short-term memory loss who cannot retain the information long enough to decide — they fail retention. [1]

How to conduct a capacity assessment at the bedside
A structured capacity interview is a clinical skill that the DCE communication station (and the MRCP PACES Station 4) will test. The method: [1]
- Set the scene — private, quiet, unhurried, with a family member or support person if the patient wishes, and an interpreter if English is not the patient's first language.
- Establish the decision — name the specific decision to be made (for example, "We are discussing whether to have the operation to bypass the blocked artery in your leg").
- Explain the information in plain language — the condition, the proposed treatment, the principal risks and benefits, the reasonable alternatives, and the consequences of not having the treatment. Chunk the information; check for understanding at each step.
- Test understanding — ask the patient to paraphrase: "Tell me in your own words what the operation involves and what could go wrong." A paraphrase tests understanding; a yes-or-no answer does not.
- Test retention — ask the patient to recall the key points after a short interval, or observe whether they hold the information throughout the discussion.
- Test use or weighing — ask the patient to explain their reasoning: "How did you weigh up the risks and benefits in reaching your decision?" Listen for whether they have integrated the information or are reasoning from delusion, compulsion, or an inability to conceive of the consequences.
- Test communication — ensure the patient can express a decision by whatever means.
- Document the decision, the specific question assessed, the information given, the patient's responses for each of the four abilities, your clinical judgement with reasoning, and the outcome. [1]
Exam trap: The most common capacity error is to equate "the patient agrees with me" with "the patient has capacity". Capacity is not about the decision's content — it is about the process of deciding. A patient who agrees with a sensible recommendation may still lack capacity (they may agree because they cannot understand or weigh). Conversely, a patient who refuses may have full capacity. Test the process, not the outcome. [1]
3. When a patient lacks capacity — best interests and least restrictive option
When the patient lacks capacity for the specific decision, the clinician cannot simply proceed — they must act in the patient's best interests using a defined process, and they must use the least restrictive option that achieves the purpose. The framework is the Mental Capacity Act 2005 in the UK and the state and territory guardianship legislation in Australia (the Guardianship and Administration Acts and the Substitute Decision-Maker provisions), which share the same five principles. [1]
The five principles (Mental Capacity Act 2005)
- A person must be assumed to have capacity unless it is established that they lack it.
- A person is not to be treated as unable to make a decision unless all practicable steps to help them do so have been taken without success.
- A person is not to be treated as unable to make a decision merely because they make an unwise decision.
- An act done, or decision made, for or on behalf of a person who lacks capacity must be done, or made, in their best interests.
- Before the act is done, regard must be had to whether the purpose can be as effectively achieved in a way that is less restrictive of the person's rights and freedom of action. [1]
These principles are examinable verbatim in the MRCP and are the conceptual backbone of the ANZ guardianship statutes. [1]
Best interests — the substituted judgement standard
Best interests is not a purely objective medical judgement of what is "best" in the abstract; it is a person-centred judgement that asks what this patient would have wanted and what would promote their welfare in their specific circumstances. The clinician must: [1]
- Consider all relevant circumstances, not just the medical — past and present wishes and feelings, beliefs and values, cultural and religious background, and the views of anyone engaged in caring for the person or interested in their welfare.
- Consult the substitute decision-maker — the person legally authorised to make the decision on the patient's behalf. In the UK, this is the attorney under a Lasting Power of Attorney (health and welfare), a court-appointed deputy, or (in their absence) the treating clinician acting in best interests, consulting family and carers. In ANZ, the legislation names a hierarchy of "person responsible" — a guardian (an enduring guardian or a tribunal-appointed guardian) first, then a spouse or de facto partner, then an adult child, then a parent, then a sibling, then a carer (with state-by-state variation).
- Apply the substituted judgement — what would the patient have decided if they had capacity? This is distinct from what the family would decide for themselves.
- Consider any valid advance directive or values statement that bears on the decision (below).
- Not be motivated by age, disability or the desire to bring about death. [1]
The least restrictive option
Where two options achieve the purpose, choose the one that interferes least with the patient's rights and freedom. This is the principle behind, for example, treating a patient with oral antibiotics at home rather than intravenous antibiotics in hospital if both are equally effective; or using a supervised community treatment order rather than an inpatient admission if the patient can be safely managed in the community. [1]
Disputes and the guardianship tribunal
Where there is genuine dispute between the clinician, the family and the substitute decision-maker, or where the decision is so serious or irreversible that it requires independent authority (for example, the non-therapeutic sterilisation of an incapacitous adult, the withdrawal of clinically assisted nutrition and hydration from a patient in a permanent vegetative state, or a major amputation), the matter is referred to the guardianship tribunal or board (in the UK, the Court of Protection). The court makes the decision on best interests, applying the substituted judgement standard. [1]
4. Consent — the three pillars

Consent is the agreement of a patient to a proposed investigation or treatment after the relevant information has been disclosed and understood. Valid consent requires three pillars, all of which must be present. [1]
Capacity
The patient must have capacity for the specific decision (see above). This is the threshold pillar: without capacity, the patient cannot give valid consent, and the clinician must either invoke an exception (emergency, statute, court) or act in best interests with the substitute decision-maker. [1]
Informed
The patient must understand, in broad terms, the nature of the proposed treatment (what will be done), its purpose (why it is being proposed), the principal risks (the material or significant risks, including the common and the serious), the benefits (the realistic expected benefit, not a guarantee), the reasonable alternatives (including the option of no treatment), and the consequences of declining. The standard is the reasonable patient standard (Montgomery v Lanarkshire, UK, 2015): the clinician must disclose any risk that a reasonable patient in the patient's position would attach significance to, taking into account the individual patient's circumstances. This replaced the older "professional" standard (Bolam) which asked what a reasonable body of doctors would disclose. The reasonable patient standard is now broadly adopted across common-law jurisdictions. [1]
Consent is a process, not a signature on a form. The form documents the conversation; it does not constitute consent. The conversation must allow the patient to ask questions, and the patient must be given enough time to consider (where the decision is not urgent). [1]
Voluntary
The decision must be the patient's own, free from coercion, undue influence or pressure. Coercion includes threats from family members, pressure from clinicians (subtle or overt), the panic of an acute illness or bad news, and the disorientation of an unfamiliar environment. A patient who consents because they are frightened of the consequences of refusing, or because a family member has insisted, is not giving voluntary consent. The clinician's role is to offer a recommendation (patients want and expect a professional opinion) and to create the conditions for a free decision. [1]
DWE discriminator: A stem describing a patient pressured by family to accept a treatment they do not want tests voluntariness — the answer is to see the patient alone, explore their own wishes, and ensure the decision is theirs. A stem describing a clinician who failed to disclose a significant risk tests the informed pillar (the reasonable patient standard). [1]
5. When consent is not required — the three exceptions
Consent is the default, but there are three situations where treatment may proceed without the patient's consent. [1]
The doctrine of necessity (emergency)
When a patient lacks capacity for a decision, and treatment is immediately necessary to save life or prevent serious deterioration, and it is not reasonably practicable to wait for capacity to be restored or for a substitute decision-maker to be consulted, and no prior valid refusal (an advance directive) is known to exist, the clinician may treat under the doctrine of necessity. The treatment given must be the minimum reasonably required to address the emergency, and the patient must be reassessed as soon as possible. This is the legal basis for emergency surgery on an unconscious trauma patient, for thrombolysis of a stroke patient who cannot consent, and for a blood transfusion in a haemorrhaging patient who is delirious. The doctrine does not extend to non-urgent treatment that can wait, nor to treatment the patient has previously refused by valid advance directive. [1]
Statutory authority
Certain statutes authorise treatment without consent. Mental health legislation permits the involuntary detention and treatment of a patient with a mental illness that meets defined criteria (a risk to self or others, or a serious deterioration in health), with review by a mental health tribunal — but the legislation authorises treatment of the mental illness, not unrelated medical conditions (a patient detained under the Mental Health Act for schizophrenia retains the right to refuse an appendicectomy on capacity grounds). Public health legislation authorises the treatment, isolation or detention of a patient with a notifiable disease that poses a risk to public health (for example, infectious tuberculosis). These statutes vary by jurisdiction but share the principle that the public health or mental health need can, in defined circumstances, override individual autonomy. [1]
Court order
A court (in the UK, the Court of Protection; in ANZ, the guardianship tribunal or the Supreme Court in its inherent jurisdiction) can authorise treatment that is in the best interests of a patient who lacks capacity, particularly for serious, irreversible or ethically contested decisions — non-therapeutic sterilisation, withdrawal of artificial nutrition and hydration from a patient in a permanent vegetative state, organ donation by an incapacitous person, or termination of pregnancy. [1]
Exam trap: The most common error is to invoke the emergency doctrine for treatment that could wait. The doctrine is for immediate, life-or-limb-saving treatment where delay is harmful and no substitute can be reached — not for "it is more convenient to operate now than to wait for the family". [1]
6. Advance care planning and ceilings of treatment
Advance care planning is the structured conversation and documentation that allows a patient, while they have capacity, to record their preferences for treatment at a future time when they may lack capacity. The SUPPORT trial (1995) — a landmark negative trial — showed that simply providing more information and documentation to physicians did not, by itself, improve end-of-life care, and taught the field that advance care planning is a conversation that must be integrated, repeated and communicated, not a one-off form [4]. The Brinkman-Stoppelenburg systematic review (2014) confirmed that advance care planning is associated with reduced use of life-sustaining treatment at the end of life, increased hospice use, and improved concordance between patient preferences and the care delivered [5].
Advance refusals of treatment — legally binding
An advance decision to refuse treatment (in the UK, an Advance Decision under the Mental Capacity Act 2005; in ANZ, a refusal within a binding advance care directive) is a statement, made by a capacitous adult, specifying treatment they refuse in specified future circumstances. If the refusal is valid (the patient had capacity, was not coerced, and intended the refusal to apply) and applicable (the circumstances have arisen, and the refusal clearly covers the treatment now proposed), it is binding — the clinician must respect it as if the now-incapacitous patient were refusing in real time. A valid advance refusal of life-sustaining treatment must be specific, and in some jurisdictions must be in writing, signed and witnessed, with an express statement that it applies even if life is at risk. Ignoring a valid advance refusal is unlawful. [1]
Advance statements of values and preferences — persuasive, not binding
An advance statement (values statement, statement of preferences) records what matters to the patient — their beliefs, values, what they would consider an acceptable outcome, what they would want their family to know. It is not legally binding, but it is persuasive: the clinician and the substitute decision-maker must consider it when determining the patient's best interests. Most advance care plans combine binding refusals (where the patient is clear) with persuasive values statements (where the patient expresses preferences). [1]
Goals of care conversations
The goals-of-care conversation is the active, ongoing discussion between the patient (where possible), the family and the clinician about the overall aim of treatment — cure, prolongation of life, symptom control, or comfort — and the treatments that are appropriate to that aim. The structure is: explore understanding, explore values and priorities, share honest prognostic information, align recommendations with values, and document and review. This is covered in detail in the palliative care topic. [1]
Ceilings of treatment and not-for-resuscitation orders
A ceiling of treatment agreement documents the level of intervention appropriate in the event of deterioration — for example, ward-based care with intravenous fluids and antibiotics, but not ICU admission or mechanical ventilation. A not-for-resuscitation (or not-for-cardiopulmonary resuscitation) order documents the decision not to attempt CPR in the event of cardiac arrest. [1]
The single most important communication principle is that a not-for-resuscitation order is not a decision to withdraw treatment — the patient continues to receive all appropriate active treatment within the agreed ceiling, including treatment of the precipitating illness, symptom relief, and escalation to a higher level of care up to the agreed ceiling. The phrase the examiner listens for is "we will not resuscitate, but we will not abandon". The conversation should frame CPR in the context of the patient's overall illness (in advanced chronic disease, frailty and end-stage organ failure, CPR rarely succeeds and may cause harm), should pair the limitation with a clear statement of what will be done, should be documented with the rationale, and should be communicated to the team and the family. [1]
DCE long-case insight: When asked about a patient with advanced disease who is deteriorating, the consultant answer pairs the ceiling of treatment with the goals of care: "We have agreed a ceiling of ward-based active treatment, focused on symptom control and the treatment of reversible precipitants, and we will not attempt CPR. We will continue to treat the pneumonia, manage the pain, and support the family. This is not withdrawal of care — it is care proportionate to the goals." The registrar answer is "we made him not for resus" without the proportionality and the continuation. [1]
7. Confidentiality and its limits
The duty of confidentiality is a core medical obligation: information shared by a patient with a clinician, in the context of the clinical relationship, must not be disclosed to third parties without the patient's consent. The duty is ethical (rooted in autonomy and trust), professional (codified in the codes of conduct of the Medical Board of Australia, the GMC, and the ABIM), and legal (the common law and, in many jurisdictions, statutory privacy law). Confidentiality is what makes the clinical relationship possible — a patient who feared disclosure would not disclose the substance of their problem. [1]
When confidentiality may be breached
Confidentiality is a strong duty but not absolute. It may be breached, without the patient's consent, in defined circumstances, and the decision and its justification must always be documented. [1]
- Mandatory reporting — certain conditions must, by law, be reported to the relevant authority. In Australia, child abuse and neglect are mandatory to report in all states and territories; in the UK, the duty is similarly strong under safeguarding guidance. Notifiable diseases (tuberculosis, HIV in some jurisdictions, and a defined list under public health legislation) must be reported to public health authorities. Certain impairments (in Australia, any health condition that may affect a doctor's ability to practise safely, and any driver with a condition that impairs safe driving above a threshold) carry reporting obligations.
- Serious imminent risk to an identifiable third party — where a patient presents a serious and imminent risk of death or serious harm to an identifiable person or persons, and the clinician judges that disclosure is necessary to avert the risk, the duty to protect can override confidentiality. The classic case is the patient who confides an intent to kill an identifiable person; the clinician may need to warn the person and the police. The principle (Tarasoff duty, originating in a US case) is recognised, with jurisdictional variation, across common-law countries.
- Imminent risk to self — where a patient is at imminent risk of suicide or serious self-harm and lacks capacity or is detained under mental health legislation, the duty to protect can override confidentiality, allowing disclosure to the mental health team, the family and emergency services to prevent the harm.
- Court order — a court can compel disclosure of confidential information, although the clinician should where possible seek to limit the disclosure to what is legally required and should notify the patient.
- Public interest — in rare cases, a serious threat to public health or safety (an epidemic, a serious crime) may justify disclosure, weighing the public interest against the patient's interest in confidentiality. [1]
DWE discriminator: A stem describing a patient who confides an intention to harm an identifiable person tests the Tarasoff duty — the answer is that the clinician may breach confidentiality to warn the identifiable victim and notify the authorities, and must document the reasoning. The duty is to the identifiable person, not a vague fear. [1]
8. Professional regulation and the doctor-patient relationship
The professional framework within which ethics, capacity and consent operate is set by the medical regulator — the Medical Board of Australia and AHPRA in Australia, the Medical Council of New Zealand, the General Medical Council (GMC) in the UK, and the state medical boards and the American Board of Internal Medicine in the US. Each publishes a code of conduct (Good Medical Practice) that defines the professional duties — patient-centred care, collegiality, teaching, research integrity, health of the practitioner, and the maintenance of professional boundaries. [1]
Revalidation and continuing professional development
Physicians must maintain competence through continuing professional development and, in many jurisdictions, revalidation — a periodic formal demonstration that the doctor remains fit to practise. In the UK, the GMC requires revalidation every five years, supported by annual appraisals. In Australia, the Medical Board requires participation in a continuing professional development program approved by a specialist college (the RACP for physicians). The principle is that the public has a right to assurance that the doctor is up to date and fit to practise. [1]
Professional boundaries and conflicts of interest
The physician must maintain professional boundaries — no personal, sexual or financial relationship with a patient that could exploit the trust of the clinical relationship. Conflicts of interest (financial relationships with industry, gifts, hospitality) must be declared and managed so that they do not influence clinical judgement. [1]
The doctor in difficulty
A doctor who is unwell — physically or mentally, or impaired by substances — has a professional duty to seek help and to limit or stop practice where the condition affects safe practice. Colleagues have a duty to support and, where patient safety is at risk, to report to the regulator. The duty to patients always overrides the loyalty to a colleague. [1]
9. Breaking bad news — the SPIKES protocol
The SPIKES protocol (Baile 2000) is the standard six-step framework for delivering bad news, and is examinable in the DCE communication station and the MRCP PACES [6].
- S — Setting. A private, quiet space, seated, with enough time, a senior clinician and a nurse present, and a family member or support person if the patient wishes. Interruptions minimised; tissues available; phones off.
- P — Perception. Ask what the patient already understands: "What have the doctors told you so far about your illness?" This avoids both information overload and the jarring mismatch of assuming the patient knows more or less than they do.
- I — Invitation. Ask how much information the patient wants: "Would you like me to go through the results in detail, or would you prefer a summary?" Respect a wish not to know in detail (some patients prefer the family to be told), but ensure the patient is offered the information.
- K — Knowledge. Give a warning shot ("I am afraid the news is not what we hoped for"), then deliver the information in plain language, in small chunks, with pauses to check understanding. Avoid jargon; avoid false reassurance; avoid the brutal truth delivered without preparation.
- E — Emotions. Acknowledge and name the emotion, validate it, and allow silence: "This is clearly a great shock. I can see how hard this is. Take a moment." This is the step most often skipped and the most important. Do not fill the silence; do not move to the plan before the emotion has been heard.
- S — Strategy and Summary. Agree a clear plan, give a written summary, name a single point of contact, and arrange follow-up. Check the patient's understanding of the plan before they leave. [1]
DCE long-case insight: The most common communication error in breaking bad news is information overload — a monologue of detail that the patient cannot absorb, delivered without checking perception or responding to emotion. The SPIKES protocol emphasises assessing perception and invitation before delivering knowledge, and the most important step is responding to the emotion with empathy and silence. [1]
10. Specific ethical scenarios in the physician setting
The patient who refuses life-sustaining treatment
A 68-year-old man with severe aortic stenosis and heart failure refuses a valve replacement that would prolong his life and improve his symptoms. He says he has "had enough" and does not want surgery. The ethical reasoning: assess his capacity for this specific decision (the stakes are high — understand, retain, weigh and communicate the nature of the valve, the principal risks and benefits, the alternative of medical management, and the expected outcome of declining). If he has capacity, his refusal is autonomous and must be respected, however unwise it seems. If he lacks capacity, the decision is made in his best interests using the substituted judgement standard, consulting the substitute decision-maker and considering any advance directive. The clinician's role is not to coerce or to abandon — it is to ensure the decision is capacitous and informed, to continue the doctor-patient relationship, to optimise medical therapy, and to plan for symptom control and the trajectory of the disease. [1]
The patient with fluctuating capacity from delirium
A 78-year-old woman with hospital-acquired delirium refuses antibiotics for a pneumonia. She is orientated in the morning and confused by evening. The reasoning: capacity is time-specific. Defer the decision where possible; treat the reversible precipitants of the delirium; reassess at her best time of day; if capacity is restored, consent or refuse on the basis of her capacitous decision. If the decision cannot wait (she is deteriorating from the pneumonia), treat under the doctrine of necessity and reassess. Document the assessment at each stage. [1]
The Jehovah's Witness who refuses blood
A 55-year-old man with a major upper gastrointestinal bleed refuses blood transfusion on the grounds of his faith. He has capacity, he understands that he may die without the transfusion, and his refusal is voluntary and informed. The reasoning: a capacitous refusal of life-saving treatment must be respected. The clinician's role is to use blood-conserving strategies (cell salvage if acceptable, tranexamic acid, erythropoietin, iron), to treat the cause of the bleed urgently, to document the refusal and the discussion, and to continue to care. A valid advance refusal of blood by a Jehovah's Witness who now lacks capacity is equally binding. [1]
The family who demand everything
The family of an 82-year-old woman with end-stage dementia and a pneumonia demand that she be admitted to ICU and intubated. The patient has no advance directive. The reasoning: the decision is the patient's, made in her best interests by the substitute decision-maker in consultation with the clinician, using the substituted judgement standard — what would she have wanted? The family's grief-driven wish for "everything" is not, of itself, the best-interests decision, and the clinician's role is to lead a goals-of-care conversation, to explain the likely outcome of ICU in her condition (low chance of survival to discharge, high chance of a prolonged and distressing death in ICU), and to propose a plan that is proportionate — active treatment of the pneumonia within a ceiling of ward-based care, with symptom control and family support. If the family and the clinician cannot agree, the matter is referred to the guardianship tribunal. [1]
The young man who threatens to kill his ex-partner
A 28-year-old man with a psychotic illness, detained under mental health legislation, confides to his psychiatrist that he intends to kill his ex-partner when he is discharged, and names her. The reasoning: there is a serious and imminent risk to an identifiable person. The duty to protect overrides confidentiality. The clinician should warn the ex-partner (directly or through the police), notify the authorities, ensure the patient's mental health treatment addresses the risk, and document the reasoning. The Tarasoff principle. [1]
Exam traps and high-yield discriminators
- Capacity is presumed in every adult, and is not lost by diagnosis, by an unwise decision, or by a refusal of life-saving treatment. The burden is on the clinician asserting incapacity to demonstrate it.
- Capacity is decision-specific and time-specific. Assess for the specific decision in front of you, at the time the decision must be made. A patient may have capacity to consent to a blood test but not to refuse a life-saving operation; a delirious patient may have capacity in the morning and not in the evening.
- The two-stage test — diagnostic (is there an impairment of mind or brain?) then functional (does it make the patient unable to decide?). The four functional abilities are understand, retain, use or weigh, communicate. Failure of any one, because of the impairment, means the patient lacks capacity for that decision.
- A capacitous adult can refuse any treatment, including life-saving treatment. The refusal must be respected, however unwise. Over-riding it is assault.
- Valid consent needs capacity, informed and voluntary. The informed standard is the reasonable patient (Montgomery), not what doctors would disclose. Voluntary means free from coercion and undue influence.
- When a patient lacks capacity, act in best interests using the substituted judgement standard, with the substitute decision-maker, considering the advance directive, and using the least restrictive option.
- The three exceptions to consent are the doctrine of necessity (emergency), statutory authority (mental health, public health), and court order. The emergency doctrine is for immediate, life-or-limb-saving treatment where delay is harmful and no substitute can be reached.
- An advance refusal that is valid and applicable is binding. An advance statement of values is persuasive but not binding.
- A not-for-resuscitation order is not a decision to withdraw care. The patient continues to receive active treatment within the agreed ceiling — do not resuscitate but do not abandon.
- Confidentiality may be breached for mandatory reporting (child abuse, notifiable disease), serious imminent risk to an identifiable person (Tarasoff), and court order. Document the reasoning.
- The SPIKES protocol — Setting, Perception, Invitation, Knowledge, Emotions, Strategy. The most-skipped and most important step is responding to the emotion. [1]
Cross-links
- Delirium — the assessment and management of the confused patient, including the implications for capacity, are detailed in the delirium topic.
- Dementia — capacity assessment, advance care planning and substitute decision-making in the cognitively impaired patient are covered in the dementia topic.
- Palliative care and symptom management — goals-of-care conversations, ceilings of treatment, anticipatory prescribing and the doctrine of double effect are detailed in the palliative care topic.
- Comprehensive geriatric assessment and frailty — the multi-dimensional assessment that informs best-interests decisions and ceilings of treatment in the frail older patient.
- The deteriorating ward patient — recognising and responding to deterioration, and the goals-of-care and ceiling-of-treatment conversations that follow, are covered in the deteriorating ward patient topic.
- Polypharmacy and deprescribing — the principles of shared decision-making and the ethical basis of deprescribing in the patient with limited life expectancy. [1]
References and guidelines
Appelbaum — Clinical Practice: Assessment of Patients' Competence to Consent to Treatment (NEJM 2007) [1]; Appelbaum and Grisso — Assessing Patients' Capacities to Consent to Treatment (NEJM 1988) [2]; Grisso, Appelbaum and Hill-Fotouhi — The MacCAT-T (Psychiatr Serv 1997) [3]; The SUPPORT Principal Investigators — A controlled trial to improve care for seriously ill hospitalized patients (JAMA 1995) [4]; Brinkman-Stoppelenburg, Rietjens and van der Heide — The effects of advance care planning on end-of-life care: a systematic review (Palliat Med 2014) [5]; Baile and colleagues — SPIKES protocol for delivering bad news (The Oncologist 2000) [6]. UK Mental Capacity Act 2005 and its Code of Practice; GMC Good Medical Practice (2024) and Consent: patients and doctors making decisions together (2008); Medical Board of Australia / AHPRA Good Medical Practice: A Code of Conduct for Doctors in Australia; Australian Commission on Safety and Quality in Health Care national framework for advance care planning; Beauchamp and Childress, Principles of Biomedical Ethics (Oxford University Press, first edition 1979).
References
- [1]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [2]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [3]Grisso T, Appelbaum PS, Hill-Fotouhi C The MacCAT-T: a clinical tool to assess patients' capacities to make treatment decisions Psychiatr Serv, 1997.PMID 9355168
- [4]The SUPPORT Principal Investigators A controlled trial to improve care for seriously ill hospitalized patients. The study to understand prognoses and preferences for outcomes and risks of treatments (SUPPORT). The SUPPORT Principal Investigators JAMA, 1995.PMID 7474243
- [5]Brinkman-Stoppelenburg A, Rietjens JA, van der Heide A The effects of advance care planning on end-of-life care: a systematic review Palliat Med, 2014.PMID 24651708
- [6]Baile WF, Buckman R, Lenzi R, Glober G, Beale EA, Kudelka AP SPIKES-A six-step protocol for delivering bad news: application to the patient with cancer Oncologist, 2000.PMID 10964998