Phys · general-medicine
Multi-morbidity and Complex Care — Managing the Patient with Multiple Chronic Diseases
Also known as multimorbidity · multi-morbidity · complex multimorbidity · multiple chronic conditions · complex care · comprehensive geriatric assessment · CGA · patient-centred care · shared decision making · advance care planning · goals of care · care coordination · medication reconciliation · STOPP/START · Beers criteria · deprescribing · prescribing cascade · frailty · Clinical Frailty Scale · single-disease paradigm · polypharmacy · triple whammy
Consultant-physician-depth guide to multi-morbidity (two or more chronic conditions): epidemiology (Barnett 2012), the failure of the single-disease paradigm (Boyd 2005), the comprehensive assessment (CGA, medication reconciliation and review with STOPP/START and Beers, function, cognition, frailty, social), the five management principles (patient-centred, holistic, prioritised, coordinated, evidence-informed), the key multi-morbidity scenarios (HF with CKD, diabetes with CVD, AF with CKD and falls, COPD with HF), deprescribing, advance care planning, and care coordination. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Multi-morbidity and Complex Care — Managing the Patient with Multiple Chronic Diseases

The answer first
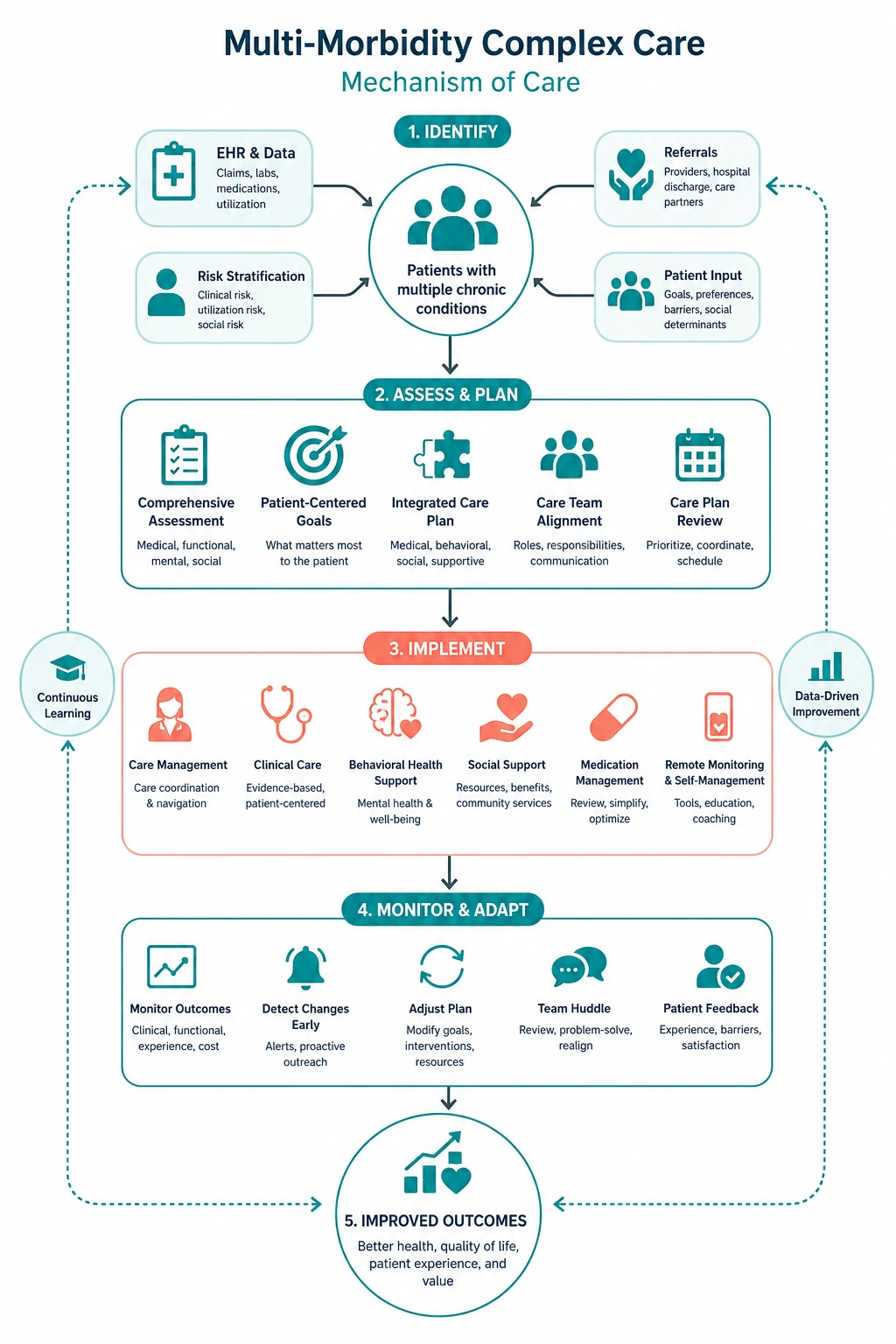
Multi-morbidity is the coexistence of two or more chronic conditions in the same individual. It is the rule, not the exception, in adult medicine — by age 65 most people have it, and by 80 almost everyone does [1]. The clinician's job is not to treat each disease by its own guideline, because those guidelines were written for patients with a single disease in isolation and they fail when stacked on top of each other [2]. The job is to treat the person, not the diseases: to find out what matters to the patient, to prioritise the problems that matter most, to reconcile and rationalise the medications, to coordinate the specialists under a single shared plan, and to adapt the evidence to this individual's goals, frailty and life expectancy.
The five questions that decide everything are: [1]
- What are the patient's priorities? What do they want to achieve, what outcomes are unacceptable to them, and what trade-offs will they accept? This anchors every decision.
- What is the prioritised problem list? Number the problems, rank them by what matters most to the patient and by what is most modifiable, and address the highest-impact items first.
- What is the medication review? Reconcile the list, apply STOPP/START and Beers, dose-adjust for renal function, and deprescribe what now does more harm than good [12] [13].
- Who is coordinating the care? A single clinician (usually the GP or general physician) owns the integrated plan, with the specialists as advisers.
- What is the advance care plan? Document the ceiling of treatment, the resuscitation status, the surrogate decision-maker, and the goals for future admissions — early, while the patient can participate.
The recurring trap: treatments that seem protective — adding a drug for every disease, pursuing tight targets, deferring the goals conversation — cause net harm when applied to the whole multi-morbid patient. Multi-morbidity rewards restraint, integration, and anchoring every decision to what the patient actually wants. [1]

Why the single-disease paradigm fails
Modern medicine is organised around diseases. Each disease has its own specialty, its own guideline, its own trial programme, its own quality indicator, and its own clinic. This single-disease paradigm works well for the patient with one problem. It fails the patient with several, for three reasons [2] [3].
First, guidelines are built in isolation. A clinical practice guideline for heart failure assumes the patient has heart failure and nothing else. A guideline for COPD assumes the patient has COPD and nothing else. When a patient has both — plus diabetes, plus osteoporosis, plus osteoarthritis — applying every guideline in full produces a regimen that no human could tolerate. Boyd and colleagues demonstrated this in 2005 with a now-classic paper: they constructed a hypothetical 79-year-old woman with five common chronic conditions, aggregated the recommendations from the relevant guidelines, and found that strict adherence would prescribe 12 medications at a cost of 406 dollars per month, with multiple drug-drug interactions and a treatment burden that was frankly impossible [2]. The single-disease paradigm, applied faithfully to a multi-morbid patient, generates harm.
Second, trials exclude multi-morbid patients. The randomised trials that underpin guidelines enrol highly selected patients with a single disease and few comorbidities. The evidence on which the guideline rests does not represent the patient in front of you. When you apply that evidence to a frail 82-year-old with six conditions and ten medications, you are extrapolating — and the extrapolation often overstates benefit and understates harm. [1]
Third, guidelines do not prioritise. A guideline tells you what to do for one disease; it does not tell you how that disease ranks against the patient's other problems, or against the patient's own priorities. The heart failure guideline does not ask whether preventing a heart failure admission matters more to this patient than preserving her mobility, her cognition, or her independence. That judgement is the physician's job — and it cannot be delegated to a guideline. [1]
Epidemiology — who has multi-morbidity, and why it matters
The landmark epidemiological study is Barnett and colleagues' 2012 cross-sectional analysis of 1.75 million people registered with 314 general practices in Scotland [1]. The findings reshaped how we think about the problem:
- Prevalence rises steeply with age. Multi-morbidity (two or more of 40 conditions) was present in 23 per cent of the whole population and in most people aged 65 and over.
- But the absolute burden is in mid-life. Because there are far more younger people than older people, the absolute number of people with multi-morbidity was higher in those under 65 than in those over 65. Multi-morbidity is not exclusively a problem of old age.
- Deprivation brings it earlier. People in the most deprived areas developed multi-morbidity 10 to 15 years earlier than those in the most affluent areas, and their multi-morbidity was more likely to include mental health conditions.
- Mental and physical conditions cluster. Depression was strongly associated with physical multi-morbidity, and the combination carried a greater burden than either alone. [1]
The clinical implication is that every adult patient you see is likely to have more than one chronic condition, and the more deprived they are, the earlier this begins. Multi-morbidity is the modal patient, and the health system — organised around single diseases — is designed for the exception [4].
The comprehensive multi-morbidity assessment
The assessment of the multi-morbid patient is broader than the assessment of a single disease. It asks not only "what diseases does this patient have?" but "how do these diseases interact, what is the treatment burden, what is the functional impact, and what does the patient want?" The domains are those of comprehensive geriatric assessment (CGA), applied to the multi-morbid patient of any age (see the CGA and frailty topic for the full framework). [1]
Medication reconciliation and review
Obtain the best possible medication history (BPMH) from every available source: the patient, the family or carer, the general practitioner, the community pharmacist, the residential aged-care medication administration record, the dispensing records, the previous discharge summaries, and the explicit questioning about over-the-counter, complementary, "as needed", topical and inhaler medications. Reconcile this against the current chart, identify discrepancies (omissions, duplications, wrong doses, wrong drugs), and document the reconciled list in a single shared record. [1]
Then apply a structured medication review tool. The two most validated are the STOPP/START criteria (version 3, 2023) and the AGS Beers Criteria (2023). STOPP (Screening Tool of Older Persons' Prescriptions) identifies potentially inappropriate medications that should be stopped; START (Screening Tool to Alert to Right Treatment) identifies prescribing omissions — drugs the patient should be on but is not [13]. A review that only stops drugs is incomplete; always ask whether an indicated drug (anticoagulation in atrial fibrillation, an SGLT2 inhibitor in heart failure with CKD, a bisphosphonate after a fracture) is missing [12].
Renal function must be estimated before prescribing renally-cleared drugs. Use the 2021 CKD-EPI creatinine equation (race-free); in the very frail with low muscle mass, consider cystatin C, because a "normal" serum creatinine can mask a severely reduced eGFR. Dose-adjust the DOACs, gabapentinoids, metformin, digoxin, allopurinol, atenolol and lithium accordingly. Cockcroft-Gault remains the basis for drug dosing in the product information of many older drugs. [1]
Functional assessment
Function predicts outcome better than any single diagnosis. Assess activities of daily living (ADLs) — bathing, dressing, toileting, transferring, continence and feeding — and instrumental activities of daily living (IADLs) — shopping, cooking, housework, managing finances, managing medications, using transport and using the telephone. A patient who has lost IADLs is struggling to live independently; a patient who has lost ADLs needs daily help. Functional decline on admission to hospital is a red flag for a poor trajectory and triggers a rehabilitation plan. [1]
Cognitive and mood assessment
Screen cognition with the Mini-Mental State Examination (MMSE) or the Montreal Cognitive Assessment (MoCA), and screen for delirium with the 4AT (which incorporates the months of the year backwards). Screen mood with the Patient Health Questionnaire-9 (PHQ-9) or the Geriatric Depression Scale (GDS). Depression is common, under-diagnosed and treatable in multi-morbidity, and it amplifies the burden of every physical condition. Dementia and delirium frequently coexist with physical illness and each requires its own management. [1]
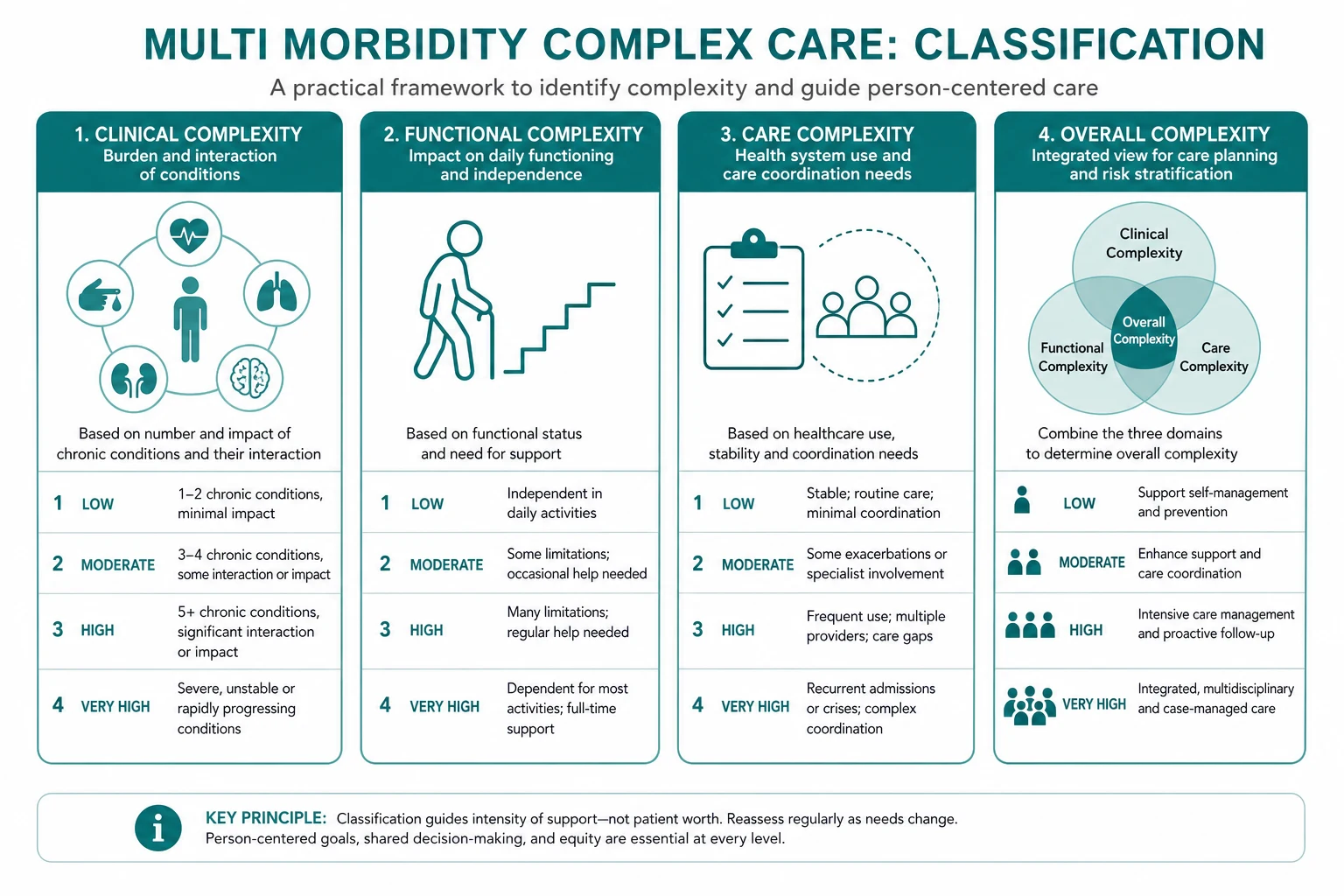
Frailty assessment
Estimate frailty with the Clinical Frailty Scale (CFS) — a 9-point judgement-based scale from 1 (very fit) to 9 (terminally ill), developed and validated by Rockwood and colleagues from the Canadian Study of Health and Aging [10]. A CFS of 5 or more (mildly frail or worse) flags a patient at elevated risk of adverse outcomes and modifies the benefit-harm balance of every treatment decision: intensive treatment brings less benefit and more harm to the frail patient than to the fit one. Frailty is not the same as multi-morbidity (a patient can have many diseases without being frail, or be frail with few), but the two usually travel together and each amplifies the other.
Social assessment
Understand who is at home with the patient, who provides care, what the home environment is (stairs, bathroom access, falls hazards), what financial and community supports exist, and what the patient's cultural and personal values are. The social context determines whether a discharge plan will succeed, whether a medication regimen can be adhered to, and whether the goals of care are realistic. [1]

The five principles of multi-morbidity management
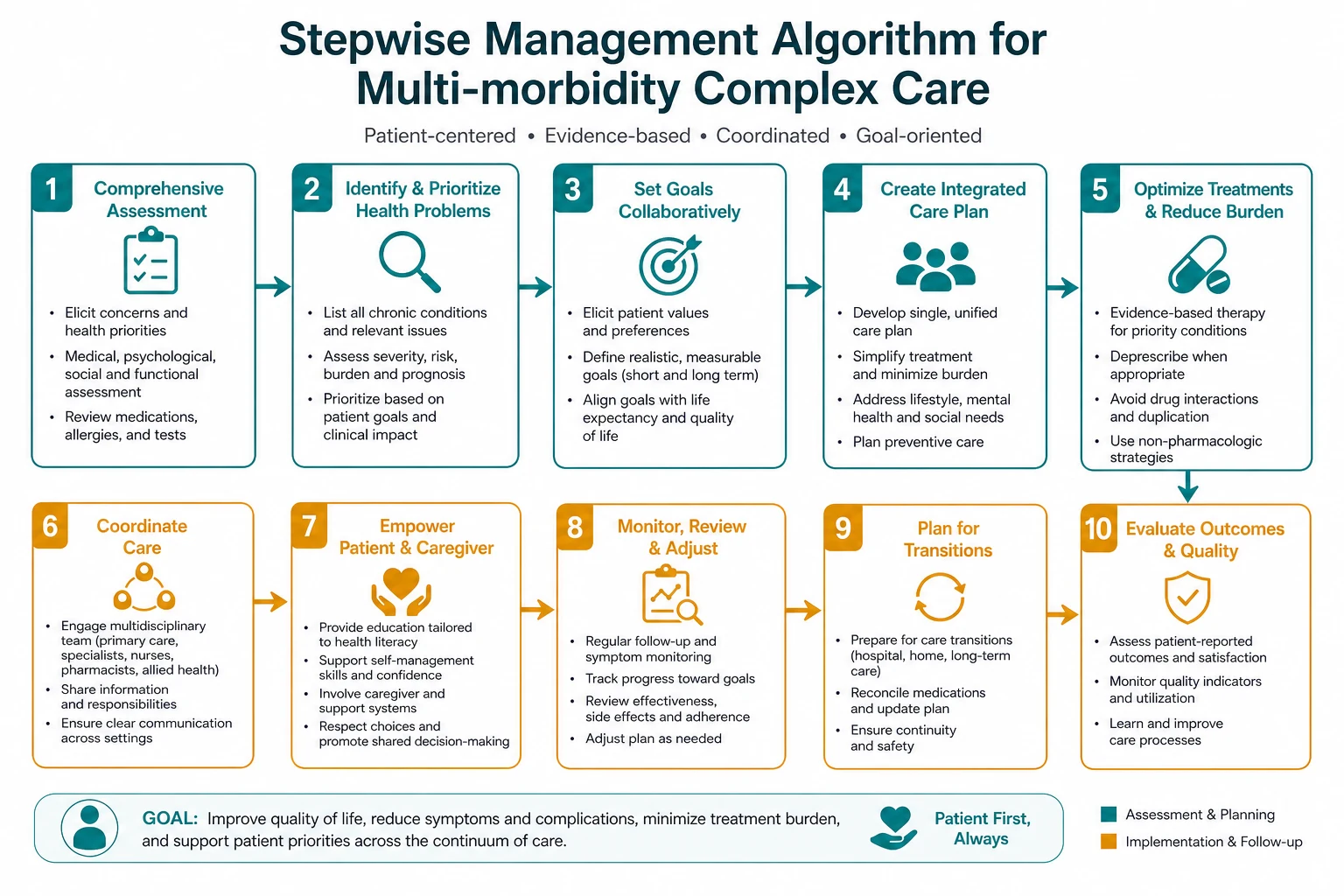
The NICE guideline NG56 (Multimorbidity: clinical assessment and management) and the AGS guidance on the care of older adults with multimorbidity converge on five principles that frame the integrated plan. Internalise these and you will not go far wrong. [1]
1. Patient-centred — align with the patient's goals
The first question is not "what does the guideline say?" but "what matters to this patient?" Use a structured goals-of-care conversation: ask what they value, what they hope to achieve, what outcomes they would find unacceptable, and what trade-offs they are willing to accept. A patient whose overriding goal is to remain independent at home will prioritise falls prevention, mobility and a tolerable medication regimen over a small absolute reduction in cardiovascular events at five years. A patient whose overriding goal is to live as long as possible will accept a more intensive regimen. There is no right answer that is right for everyone — the right answer is the one that fits this patient's priorities, and it is the physician's job to elicit and document them. [1]
2. Holistic — treat the person, not the disease
Treat the whole patient, not a collection of diseases. This means looking for treatments that benefit several conditions at once (the SGLT2 inhibitor that helps heart failure, CKD and diabetes simultaneously), avoiding treatments that help one disease but harm another (the NSAID that eases arthritis but precipitates AKI in the cardio-renal patient), and recognising that the cumulative treatment burden is itself a harm that must be weighed against the benefits. [1]
3. Prioritised — focus on what matters most
A multi-morbid patient may have eight or ten active problems. You cannot address them all at once, and neither can the patient. Prioritise: identify the two or three problems that matter most to the patient and that are most modifiable, address those first, and defer or deprioritise the rest. Explicit prioritisation — communicated to the patient and documented in the record — is the antidote to the chaos of fragmented care. [1]
4. Coordinated — a single care plan and a care coordinator
Fragmented care — the cardiology clinic, the renal clinic, the diabetes clinic, the respiratory clinic, each with its own letter and its own recommendation — is a major source of harm in multi-morbidity. The fix is coordination. Nominate a single coordinating clinician, usually the general practitioner or the general physician, who owns the integrated care plan. Maintain a shared care plan with the reconciled medication list, the problem list, the goals of care and the advance care plan, accessible to every clinician involved. Hold case conferences — including the patient and family — when the plan changes. The coordinating clinician is the one who asks, before any new drug is added: "How does this fit with everything else this patient is on?" [1]
5. Evidence-informed — adapt guidelines for the multi-morbidity context
Evidence is necessary but not sufficient. Take the evidence for each treatment, and adapt it to this patient by asking: does the benefit seen in the trial population apply to this patient (who was probably excluded from the trial)? What is the time to benefit (will the patient live long enough to benefit)? What is the harm (drug interactions, treatment burden, frailty)? The result is an evidence-informed, patient-specific judgement — not a guideline-driven reflex. [1]

The key multi-morbidity scenarios
The scenarios below recur in the long case and in the clinic. For each, the answer is an integrated treatment that serves more than one condition, avoids the treatments that help one disease while harming another, and is anchored to the patient's goals. [1]
Heart failure with chronic kidney disease
This is the archetype of overlapping cardio-renal disease. The heart failure guideline recommends an ACE inhibitor or ARB, a beta-blocker, an MRA, an SGLT2 inhibitor and a diuretic. The CKD guideline cautions about ACEi-induced hyperkalaemia and the rise in creatinine, and forbids NSAIDs. The integrated answer: [1]
- The SGLT2 inhibitor is the prototype multi-morbidity drug. Dapagliflozin reduced the composite of sustained eGFR decline, kidney failure and renal or cardiovascular death in patients with CKD with or without diabetes in DAPA-CKD [7], and empagliflozin reduced cardiovascular death and heart failure hospitalisation while slowing eGFR decline in HFrEF in EMPEROR-Reduced [8]. A single once-daily oral dose benefits the heart, the kidney and (if present) the diabetes — simplifying rather than complicating the regimen.
- Use the ACE inhibitor or ARB with monitoring. A creatinine rise of up to 30 per cent and a potassium rise are expected and acceptable; stop only if the rise exceeds 30 per cent or hyperkalaemia is severe and persistent. Monitor renal function and potassium at initiation, at dose changes, and with intercurrent illness.
- Avoid NSAIDs. The combination of ACEi (afferent arteriolar vasodilation) and NSAID (efferent arteriolar vasoconstriction) in a patient with reduced renal perfusion is the classic "double whammy"; add a diuretic and you have the triple whammy that precipitates acute kidney injury.
- Manage potassium actively. Dietary advice, potassium binders (patiromer, sodium zirconium cyclosilicate) when persistent hyperkalaemia would otherwise force you to stop a beneficial ACEi or MRA, and a low threshold to review contributing drugs.
Diabetes with cardiovascular disease
Type 2 diabetes and cardiovascular disease travel together, and modern glucose-lowering therapy is cardioprotective and renoprotective. The integrated approach: [1]
- Prioritise cardiovascular and renal risk reduction over tight glycaemic control. Empagliflozin reduced cardiovascular death by 38 per cent in EMPA-REG OUTCOME [6], and semaglutide reduced major kidney events in FLOW [9]. An SGLT2 inhibitor and a GLP-1 receptor agonist are first-line add-ons to metformin in the patient with established or high-risk CVD or CKD, regardless of the HbA1c.
- Individualise the HbA1c target. A target of 53 mmol/mol (7 per cent) is reasonable for most, but relax it to 64 to 70 mmol/mol (8 to 8.5 per cent) in the frail older patient, in those with limited life expectancy, and in anyone in whom hypoglycaemia or the treatment burden of intensive control would cause net harm. Hypoglycaemia is dangerous — it causes falls, confusion, arrhythmia and death — and is entirely iatrogenic.
- Avoid the drugs that harm. Sulfonylureas (especially glibenclamide) and sliding-scale insulin cause hypoglycaemia in the older multi-morbid patient; thiazolidinediones cause fluid retention in heart failure; and metformin is contraindicated in severe CKD, sepsis or haemodynamic compromise (lactic acidosis).
Atrial fibrillation with CKD and falls risk
The three-way tension here is stroke prevention (anticoagulation) versus bleeding versus falls. The integrated approach: [1]
- Anticoagulate, adjusting the DOAC dose to the eGFR. The annual stroke risk in AF with risk factors (CHA2DS2-VASc 2 or more in men, 3 or more in women) is high — 4 to 10 per cent or more — and dwarfs the incremental bleeding risk from anticoagulation in most patients. Use a DOAC over warfarin (lower intracranial bleeding, no monitoring). Dose-adjust by the eGFR: apixaban 5 mg twice daily (reduce to 2.5 mg twice daily if two of age 80 or more, weight 60 kg or less, or creatinine 133 micromol/L or more); rivaroxaban dose-adjusted by indication and eGFR; dabigatran avoided in severe CKD as it is largely renally cleared.
- Assess the falls risk, but do not let it stop you from anticoagulating. The fall itself must be serious and recurrent (a head strike with a traumatic brain bleed) to tip the balance against anticoagulation in a patient with a high CHA2DS2-VASc score. The much-cited "falls mean no anticoagulation" is a myth for most patients; do the arithmetic, correct the reversible falls risk factors, and anticoagulate.
- Address the modifiable bleeding risk. Stop the NSAID, reduce or stop the antiplatelet that is no longer indicated (aspirin is rarely indicated alongside a DOAC for AF alone), treat the iron deficiency, and control the blood pressure. [1]
COPD with heart failure
This combination causes diagnostic and therapeutic confusion. The integrated approach: [1]
- Differentiate breathlessness. Pulmonary congestion (orthopnoea, bibasal crackles, elevated BNP or NT-proBNP, pulmonary oedema on chest X-ray) points to heart failure; exacerbation of COPD (sputum, wheeze, prolonged expiratory phase, response to bronchodilators) points to the lungs. The two coexist and each may worsen the other; treat both.
- Use cardioselective beta-blockers and do not withhold them. The myth that beta-blockers are contraindicated in COPD is outdated and harmful. Cardioselective beta-1 blockers (bisoprolol, metoprolol, nebivolol) are safe in the great majority of patients with COPD, including moderate reversible airways disease, and they reduce mortality in heart failure. A minority with severe or highly reversible COPD may bronchospasm, but the cardiovascular benefit usually outweighs the small respiratory risk. Non-selective beta-blockers (propranolol, carvedilol at high dose) should be used with more caution.
- Diurese carefully. Over-diuresis causes dehydration, hypotension, electrolyte disturbance and acute kidney injury; under-diuresis leaves the patient congested. Aim for euvolaemia, guided by clinical examination, daily weights, renal function and the jugular venous pressure.
- Address the shared risk factors. Smoking, physical deconditioning and osteoporosis are common to both; address each as part of the integrated plan. [1]
Deprescribing in the multi-morbid patient
Deprescribing is the planned, supervised process of withdrawing an inappropriate medication, supervised by a clinician, with the goal of managing polypharmacy and improving outcomes [14]. It is not "stopping everything"; it is the active, positive counterpart of prescribing. The Scott five-step process provides the framework:
- Ascertain all drugs in use — the reconciled BPMH, including over-the-counter and complementary medicines.
- Identify potentially inappropriate medications — apply STOPP/START and Beers; flag drugs with no current indication, with cumulative harm, with a poor benefit-to-harm ratio in this patient's context, or from a prescribing cascade [12] [13].
- Assess each drug against current benefit versus harm in the context of the patient's goals, frailty and life expectancy. A statin started 20 years ago for primary prevention in a patient now frail with limited life expectancy is a different decision from a statin after a recent myocardial infarction.
- Plan the taper or cessation with the patient. Abrupt cessation causes withdrawal syndromes for benzodiazepines, beta-blockers, clonidine, SSRIs, corticosteroids and opioids; plan a supervised taper (for example, a benzodiazepine taper of 10 to 25 per cent every 1 to 2 weeks, with diazepam substitution for short-acting agents). Agree the monitoring plan and the plan if the original symptom returns.
- Monitor for withdrawal, rebound and return of the original condition. Review at an agreed interval (often 2 to 4 weeks), document the outcome, and communicate the deprescribed list to the GP, the pharmacist and the patient.
Deprescribing is itself a form of shared decision-making. Frame it to the patient as optimisation — the medication was right when it was started, and stopping it now is also right, because the patient's circumstances have changed. This framing builds trust and counters the common fear that stopping a drug means "giving up". [1]
Advance care planning and goals of care
Advance care planning is the process of discussing and documenting the patient's preferences for future care, including the ceiling of treatment, the resuscitation status, the surrogate decision-maker, and the goals for future admissions. It is good practice for every adult, not only those near the end of life — but it is especially important in multi-morbidity, where the trajectory is one of gradual decline punctuated by acute deteriorations, and where the default (full escalation) may not match the patient's wishes. [1]
Introduce the conversation early, in a stable outpatient or ward setting, not in an emergency. Ask: what do you understand about your illnesses and their trajectory? What matters most to you? What outcomes would be unacceptable (for example, prolonged unconsciousness, dependence on a ventilator, admission to a nursing home)? Who would you want to make decisions for you if you could not? Document the answers in a shared record (an advance care directive, a goals-of-care form, an electronic patient record), communicate them to the GP and the family, and review them as circumstances change. [1]
The ceiling of treatment is a statement of the maximum intensity of treatment the patient would want — for example, "ward-based care only, not for ICU or cardiorespiratory resuscitation". It is not a withdrawal of care; all care continues (symptom control, dignity, treating reversible precipitants), only the ceiling is set. The resuscitation status (whether CPR would be attempted in the event of cardiac arrest) is a separate decision, made on the basis of the likelihood of survival to discharge with a meaningful quality of life, the patient's wishes, and the futility of CPR in advanced frailty or terminal illness. [1]
Care coordination and the care plan
The integrated care plan is the single document that holds the reconciled medication list, the prioritised problem list, the goals of care, the advance care plan and the follow-up arrangements. It is owned by the coordinating clinician (usually the GP or general physician), shared with every specialist involved, accessible to the patient, and reviewed at each transition of care. [1]
The coordination tasks that prevent the chaos of fragmented care: [1]
- Nominate a single coordinating clinician. This is usually the GP, supported by the general physician during an admission. The cardiologist, nephrologist, endocrinologist and respiratory physician advise; they do not each own a separate plan.
- Maintain a shared, reconciled medication list. At every transition (admission, discharge, clinic visit), reconcile the list, flag the changes, and communicate them to the patient, the GP and the pharmacist.
- Hold case conferences. When the plan changes, or when the patient is deteriorating, bring the key people together — the GP, the relevant specialists, the community nurse, the pharmacist, the patient and the family. A case conference is reimbursed under Medicare in Australia and is worth the time.
- Arrange a Home Medicines Review. The community pharmacist visits the patient at home, reviews all the medications (including those in the bathroom cabinet), and reports back to the GP with recommendations. This is one of the highest-yield interventions in multi-morbidity.
- Plan the follow-up proactively. Book the clinic review, the blood tests, the investigations, and the allied health referrals before the patient leaves — do not leave it to the patient to negotiate a fragmented system. [1]
Communication, consent and shared decision-making
Multi-morbidity care is as much a conversation as a prescription. The physician should make sure the patient understands: [1]
- What each condition is and what it means — in plain language, without jargon, and with realistic framing of the trajectory.
- What each medication is for, and what the alternatives are — including the alternative of stopping it, with the benefit and harm of each option.
- What the trade-offs are — the extra drug that might prevent an admission but causes side effects; the intensive target that might add months of life but causes hypoglycaemia today.
- What the patient's priorities are and how they shape the plan — "you told me that staying independent at home matters most; I have therefore prioritised your falls risk and simplified your medications, and we will not pursue the intensive blood pressure target that was making you dizzy". [1]
Use a shared decision-making model: present the options, explain the benefits and harms, elicit the patient's values and preferences, and agree the plan together. Document the conversation. A patient who understands their plan and the reasoning behind it is more likely to adhere to it, to recover faster, and to cope with the inevitable setbacks of multi-morbidity. [1]
Common exam traps and high-yield discriminators
- The prescribing cascade. The most common DWE error is adding a new drug to treat a symptom that is actually an adverse effect of an existing drug (metoclopramide causing parkinsonism, then levodopa added; an NSAID raising blood pressure, then another antihypertensive added). The correct answer is to review and stop the causative drug, not to add another.
- The beta-blocker in COPD. The most common pharmacology error is assuming beta-blockers are contraindicated in COPD. Cardioselective beta-1 blockers (bisoprolol, metoprolol, nebivolol) are safe and beneficial in the majority of patients with COPD and should be used when there is a cardiovascular indication.
- The SGLT2 inhibitor as the integrated answer. The most common missed concept in a multi-morbidity stem is that an SGLT2 inhibitor benefits HF, CKD and diabetes simultaneously. If a stem describes a patient with two or three of these, the SGLT2 inhibitor is very likely the single-best-answer.
- The integrated plan, not the disease-by-disease plan. The most common DCE long-case error is to present a list of diseases each with its own plan, without integration or prioritisation. The examiner wants an integrated plan anchored to what matters to the patient.
- The goals-of-care conversation is not optional. The most common advance-care-planning error is deferring the conversation until the patient is too unwell to participate. Introduce it early, document the priorities, and anchor every treatment decision to them.
- Renal function in the frail. A "normal" serum creatinine in a frail older patient masks a low eGFR because muscle mass is reduced. Always estimate the GFR and dose-adjust renally-cleared drugs.
- Tight targets harm the frail. Intensive blood pressure and glycaemic targets cause falls, hypoglycaemia and acute kidney injury in frail multi-morbid patients; individualise the target to the patient's frailty, life expectancy and priorities. [1]
Long-case integration
The multi-morbid patient is the classic DCE long case. A realistic archetype: an 82-year-old woman with heart failure with reduced ejection fraction, atrial fibrillation, type 2 diabetes, stage 3b CKD, osteoporosis, and mild cognitive impairment, on 14 medications, recently admitted with a fall, and now ready for discharge. The structured approach: [1]
- Opening statement (SASPOP) — present the patient, the presenting problem, the comorbidities, the medications, and the key issue for today.
- Structured problem list — number and prioritise the problems. Lead with the fall (the acute presentation), then the cardiovascular risk (HFrEF, AF, diabetes), then the CKD, then the osteoporosis, then the cognitive impairment, then the medication review, then the advance care plan.
- Integrated management plan — for each problem, the integrated treatment that serves more than one condition where possible (SGLT2i for HF, CKD and diabetes; DOAC dose-adjusted for eGFR for the AF; deprescribe the benzodiazepine and the anticholinergic with a supervised taper; bisphosphonate or denosumab for the osteoporosis; falls risk assessment; cognitive reassessment).
- Goals of care and advance care plan — document her priorities (independence at home), the ceiling of treatment, the resuscitation status, the surrogate decision-maker.
- Coordination and follow-up — GP as coordinating clinician, shared care plan, Home Medicines Review, case conference, clinic review, functional and cognitive reassessment. [1]
Short-case integration
The DCE short case in multi-morbidity is typically a bedside medication review and care coordination discussion. Walk through the structured routine: [1]
- Obtain and verify the BPMH — patient, family, GP, drug chart, the explicit questioning about over-the-counter, complementary, "as needed", topical and inhaler medications.
- Apply STOPP/START and Beers — name the tool, identify the potentially inappropriate medications and the prescribing omissions.
- Check the renal function and dose-adjust — estimate the eGFR with the 2021 CKD-EPI equation, dose-adjust the DOAC, and flag the renally-cleared drugs.
- Assess the falls risk and the anticholinergic burden — these are the highest-yield modifiable risks in the multi-morbid older patient.
- Present the integrated plan — the prioritised list of changes, the tapers and their timelines, the monitoring, the communication to the GP and pharmacist, and the plan if a symptom returns. [1]
References and guidelines
Barnett multimorbidity epidemiology (2012, Lancet, PMID 22579043); Boyd clinical practice guidelines and multi-morbidity (2005, JAMA, PMID 16091574); Sinnott GPs' perspectives on multi-morbidity (2013, BMJ Open, PMID 24038011); Fortin prevalence methodology (2012, Ann Fam Med, PMID 22412006); SPRINT intensive blood pressure (2015, NEJM, PMID 26551272); EMPA-REG OUTCOME empagliflozin (2015, NEJM, PMID 26378978); DAPA-CKD dapagliflozin (2020, NEJM, PMID 32970396); EMPEROR-Reduced empagliflozin in HF (2020, NEJM, PMID 32865377); FLOW semaglutide in CKD (2024, NEJM, PMID 38785209); Rockwood Clinical Frailty Scale (2005, CMAJ, PMID 16129869); AFFIRM-AHF ferric carboxymaltose (2020, Lancet, PMID 33197395); AGS Beers Criteria (2023, JAGS, PMID 37139824); STOPP/START version 3 (2023, Eur Geriatr Med, PMID 37256475); Scott deprescribing process (2015, JAMA Intern Med, PMID 25798731). NICE NG56 (Multimorbidity); AGS Guidance on the Care of Older Adults with Multimorbidity; ACSQHC Comprehensive Care Framework; WHO Multimorbidity Technical Series. [1]
References
- [1]Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study Lancet, 2012.PMID 22579043
- [2]Boyd CM, Darer J, Boult C, Fried LP, Boult L, Wu AW Clinical practice guidelines and quality of care for older patients with multiple comorbid diseases: implications for pay for performance JAMA, 2005.PMID 16091574
- [3]Sinnott C, McHugh S, Browne J, Bradley C GPs' perspectives on the management of patients with multimorbidity: systematic review and synthesis of qualitative research BMJ Open, 2013.PMID 24038011
- [4]Fortin M, Stewart M, Poitras ME, Almirall J, Maddocks H A systematic review of prevalence studies on multimorbidity: toward a more uniform methodology Ann Fam Med, 2012.PMID 22412006
- [5]Wright JT Jr, Williamson JD, Whelton PK, et al. (SPRINT Research Group) A Randomized Trial of Intensive versus Standard Blood-Pressure Control N Engl J Med, 2015.PMID 26551272
- [6]Zinman B, Wanner C, Lachin JM, et al. (EMPA-REG OUTCOME) Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes N Engl J Med, 2015.PMID 26378978
- [7]Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. (DAPA-CKD) Dapagliflozin in Patients with Chronic Kidney Disease N Engl J Med, 2020.PMID 32970396
- [8]Packer M, Anker SD, Butler J, et al. (EMPEROR-Reduced) Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure N Engl J Med, 2020.PMID 32865377
- [9]Perkovic V, Tuttle KR, Rossing P, et al. (FLOW) Effects of Semaglutide on Chronic Kidney Disease in Patients with Type 2 Diabetes N Engl J Med, 2024.PMID 38785209
- [10]Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people CMAJ, 2005.PMID 16129869
- [11]Ponikowski P, Kirwan BO, Anker SD, et al. (AFFIRM-AHF) Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: a multicentre, double-blind, randomised, controlled trial Lancet, 2020.PMID 33197395
- [12]Panel AGS 2023 Beers Criteria Update American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [13]O'Mahony D, O'Connor MN, Eustace J, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3 Eur Geriatr Med, 2023.PMID 37256475
- [14]Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing JAMA Intern Med, 2015.PMID 25798731