Phys · general-medicine
Neurological Examination — Cranial Nerves
Also known as cranial nerve examination · CN I-XII examination · cranial nerves · neurological short case · cranial nerve palsies · third nerve palsy · oculomotor palsy · facial nerve palsy · Bell palsy · Horner syndrome · relative afferent pupillary defect · RAPD · Rinne and Weber · pupil-sparing third nerve palsy
Classic DCE short-case routine for cranial nerve examination (CN I to XII): the systematic sequence, the signs to elicit, their localising value, a say-aloud presentation template, examiner discussion questions and the pitfalls that fail candidates — for FRACP DCE, MRCP PACES and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Neurological Examination — Cranial Nerves

The answer first
The instruction "Please examine this patient's cranial nerves" is one of the most frequently set and most reliably failed short cases in the FRACP DCE and MRCP PACES. The examiners are not testing whether you can name all twelve nerves — they are testing whether you can perform a fluent, systematic, reproducible sequence, elicit and correctly interpret a small number of high-yield signs, and then present a localising diagnosis before you reach for a scanner. The candidate who walks to the foot of the bed, says "I will examine the cranial nerves systematically from one to twelve", and then does exactly that — in the same order every time — outperforms the candidate who hunts for the abnormality. [1]
The four ideas that govern every cranial-nerve station: [1]
- System over hunting. A rigid sequence from CN I to CN XII protects you from omission and projects competence. Never break sequence to chase a sign you have glimpsed — finish each nerve, note the abnormality, and return to it in your presentation.
- The pupil earns or fails the candidate. The swinging-flashlight test for a relative afferent pupillary defect, and the distinction between a pupil-sparing and a pupil-involving third nerve palsy, are the two highest-yield signs in the whole examination. Know them cold [5].
- UMN versus LMN is decided at the bedside. The facial nerve (CN VII) and the tongue (CN XII) both have an upper-motor-neuron and a lower-motor-neuron pattern, and the distinction changes the differential from stroke to Bell palsy or motor neuron disease. Forehead sparing is the single most examined discriminator.
- Direction of deviation localises the lesion. An eye that is down and out with ptosis is a third nerve palsy; an eye that will not abduct is a sixth nerve palsy; a tongue that deviates toward the lesion is hypoglossal; a uvula that deviates away from the lesion is vagal. These are mnemonics worth memorising because the examiner will ask you to explain them.
The organising principle is examine in order, interpret as you go, and present a localising diagnosis supported by the single most discriminating sign. [1]
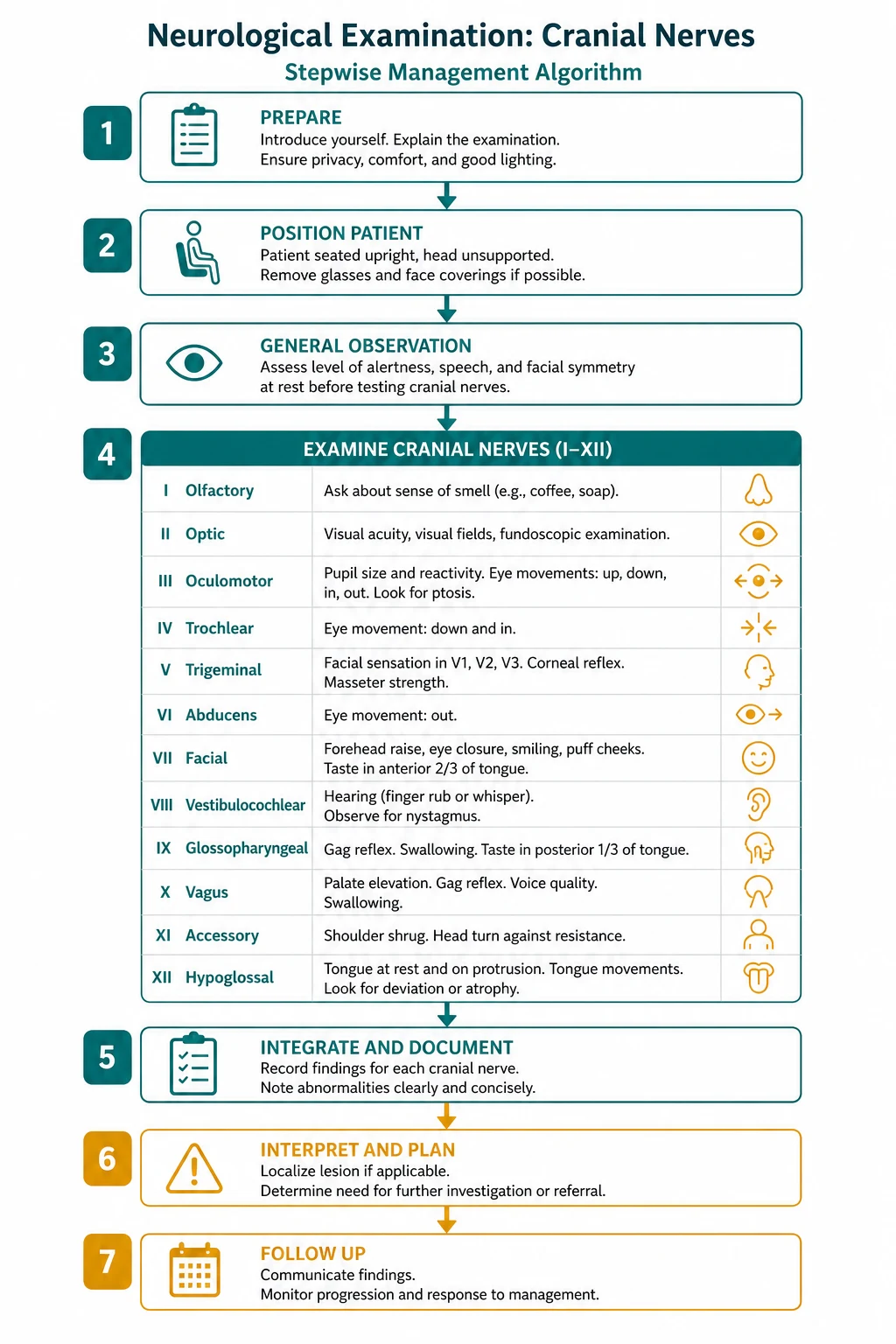
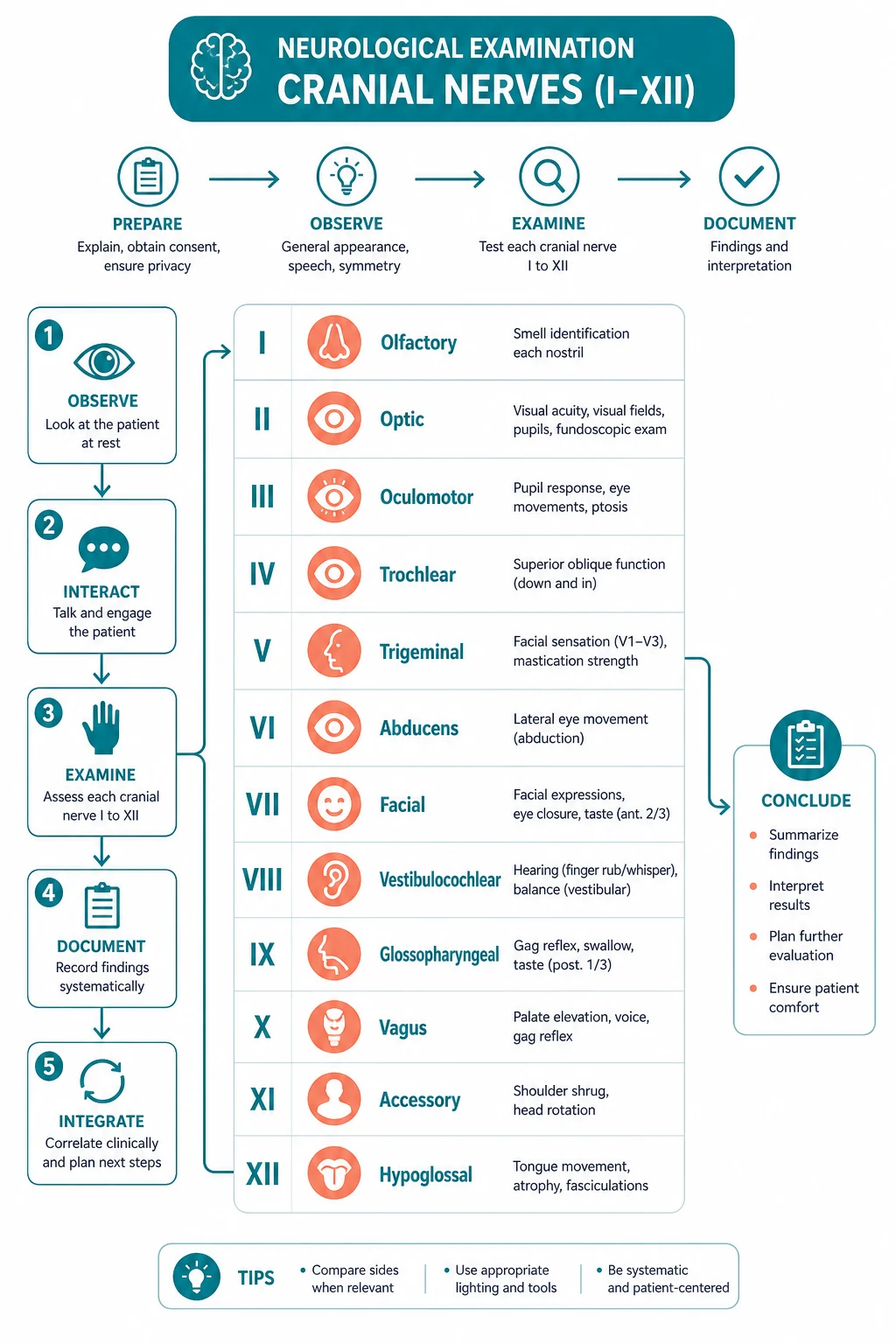
The examination sequence

Before you touch the patient, set the stage. Stand at the foot of the bed. State your plan aloud: "I will examine this patient's cranial nerves systematically from the first to the twelfth. I will begin by introducing myself, confirming consent, and positioning the patient." Ask the patient to sit up at the edge of the bed or in a chair at your eye level — examining cranial nerves with the patient supine hides facial asymmetry and makes the eye and palate inaccessible. Have a Snellen chart or a near-vision card, a pin, a cotton wisp, a tuning fork (512 Hz), an ophthalmoscope, and a reflex hammer within reach. [1]
Observe from the end of the bed before you examine. The five things that betray a cranial-nerve lesion at a glance are ptosis (CN III or sympathetic), a facial droop with a flattened nasolabial fold (CN VII), a head tilt to compensate for diplopia (CN IV or III), a wasting of the temporalis fossa or tongue (CN V or XII), and scars — a craniotomy, a parotidectomy, or a carotid endarterectomy scar that explains a Horner syndrome. [1]
Then proceed nerve by nerve. [1]
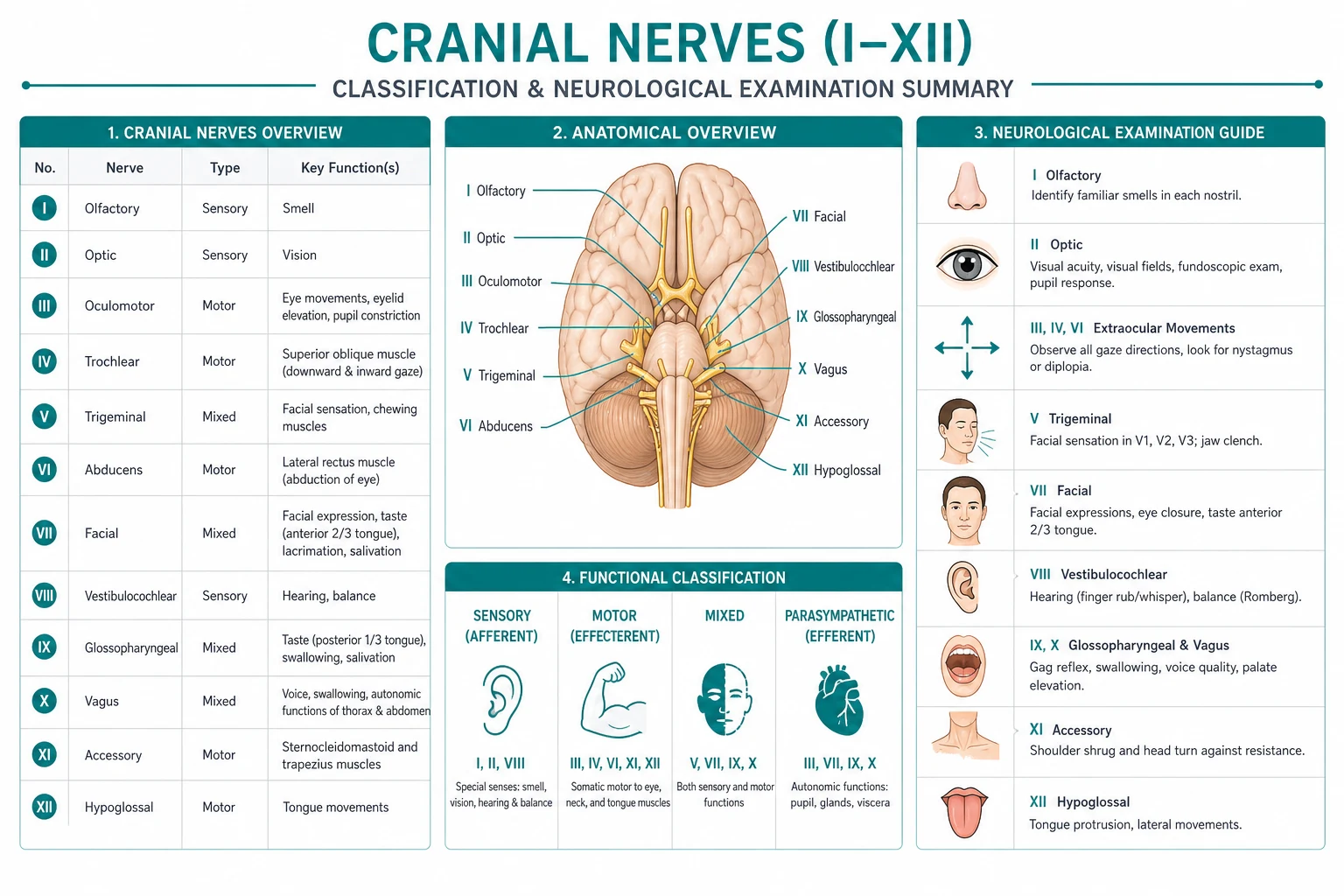
CN I — Olfactory
Olfaction is rarely tested in the routine short case because it is logistically awkward and the finding is usually incidental. If the examiner asks, or if the history suggests frontal-lobe pathology (a meningioma, a head injury, Parkinson disease), test each nostril separately: occlude one nostril with a finger and ask the patient to close their eyes and identify a non-irritant odour — coffee, vanilla or soap held at the nostril. Repeat for the other side. [1]
Avoid ammonia and other irritants. Ammonia stimulates the trigeminal nerve (CN V), not the olfactory nerve (CN I), so a patient with anosmia will still perceive it and give you a false negative. Unilateral anosmia, with the contralateral nostril intact, localises to the olfactory pathway on that side — most commonly head trauma severing the olfactory filaments, or a subfrontal mass such as an olfactory groove meningioma. Bilateral loss is common and usually attributable to upper-respiratory infection, chronic sinus disease, smoking, or age; it is rarely a focal neurosurgical problem. [1]
CN II — Optic
The optic nerve is examined in four parts: acuity, fields, reflexes, and the fundus. [1]
Visual acuity. Use a Snellen chart at six metres if available, or a near-vision card. Test each eye separately with the patient's usual distance correction; if none is available, use a pinhole to correct refractive error. Record the smallest line read — for example, 6/6 or 6/12. If acuity is too poor for the chart, progress down the hierarchy: counting fingers, hand movements, perception of light only, or no light perception. A patient who cannot read the top line but has a normal fundus and normal pupils has a refractive or retinal problem until proven otherwise; a patient with reduced acuity, a relative afferent pupillary defect and a swollen disc has an optic neuropathy. [1]
Visual fields. Test by confrontation. Sit opposite the patient at arm's length, ask them to cover their left eye with their left hand, and to look at your right eye — your eyes are the fixation targets. Bring a red pinhead or a wiggling finger in from the periphery along the four diagonals and the vertical meridians, and ask the patient to say "now" when they first see it. Your field and the patient's field should coincide. Then test the other eye. [1]
The field defects that localise a lesion are worth knowing precisely. A homonymous hemianopia (loss of the same half of the field in both eyes) is a lesion of the retrochiasmal pathway — occipital, parietal or temporal — and in a stroke patient points to the posterior cerebral artery. A bitemporal hemianopia (loss of the outer half of each field) compresses the central chiasm from below or in front — a pituitary macroadenoma or a craniopharyngioma. A superior quadrantanopia localises to the temporal lobe (Meyer's loop); an inferior quadrantanopia to the parietal lobe. A monocular field defect or a central scotoma is optic nerve or retinal. [1]
Pupillary reflexes. Examine the pupils in a dim room with a bright penlight. First inspect: size, shape, and symmetry at rest. A normal pupil is round, between 2 and 5 millimetres, and equal to its fellow (anisocoria up to 0.4 millimetres is physiological). An irregular or notched pupil suggests trauma, surgery, or inflammation. Then test the direct and consensual reflex: shine the light into the right eye and watch the right pupil constrict (direct); shine it into the right eye and watch the left pupil constrict (consensual). Both should be brisk. [1]
The decisive bedside test is the swinging-flashlight test for a relative afferent pupillary defect (RAPD). Swing the light briskly from one eye to the other, holding it on each for two to three seconds. In a normal patient both pupils constrict each time the light lands. In a patient with an optic nerve lesion on one side, when the light swings into the affected eye, both pupils paradoxically dilate — because the brain perceives less light input from that eye. This is a Marcus Gunn pupil, and a positive RAPD is the most sensitive clinical sign of an optic neuropathy, more reliable than acuity or the fundus in early disease [5]. The lesion is afferent (CN II), so the defect is present in both eyes when the bad eye is illuminated, and both pupils move together — an isolated efferent (CN III) defect would affect only one pupil.
Fundoscopy. Examine the optic disc, the vessels, and the macula, after dilating the pupil if the examiner permits. Two disc appearances define the short case. Papilloedema — bilateral disc swelling from raised intracranial pressure — shows blurred disc margins, elevation, venous engorgement, and eventually haemorrhages and cotton-wool spots; the patient may have headache, a sixth nerve palsy, and visual obscurations. Optic atrophy — a pale, sharply defined disc — is the end stage of any optic neuropathy: chronic papilloedema, a compressive lesion, demyelination, ischaemia, or hereditary disease. A swollen disc with reduced acuity and a RAPD is optic neuritis; a swollen disc without reduced acuity or a RAPD is early papilloedema from raised pressure. [1]
CN III, IV and VI — Oculomotor, Trochlear and Abducens
These three nerves move the eye and (for CN III) the lid and the pupil, so they are examined together. The order is: the pupils, the lids, then the movements. [1]
The pupils (continued from CN II)
Beyond the RAPD, the pupil examination answers two further questions: is there a third nerve palsy, and is there a Horner syndrome? Test the accommodation reflex by asking the patient to look at a distant target and then at your finger held thirty centimetres away — the pupils constrict and the eyes converge. [1]
A fixed dilated pupil with ptosis and an eye that is down and out is a complete CN III (oculomotor) palsy. The direction of deviation tells the story: the unopposed lateral rectus (CN VI) abducts the eye, and the unopposed superior oblique (CN IV) depresses it. The critical subdivision is whether the pupil is involved. The parasympathetic fibres to the pupil run on the surface of the third nerve, so a compressive lesion — classically a posterior communicating artery aneurysm, but also a tumour or a herniating temporal lobe — picks them off first and produces a pupil-involving palsy with a dilated, unresponsive pupil. The motor fibres run in the centre of the nerve, so a microvascular (ischaemic) palsy — in a patient with diabetes or hypertension — spares the pupil, producing a pupil-sparing palsy. This is the rule of the pupil, and it is the single most examined concept in neuro-ophthalmology. A painful, pupil-involving third nerve palsy is an aneurysm until proven otherwise and demands urgent CT angiography, never observation. [1]
A constricted pupil (miosis) with a partial ptosis and anhidrosis on the same side is Horner syndrome — interruption of the sympathetic chain anywhere from the hypothalamus to the eye. The ptosis is partial (Mueller's muscle is weak, not the levator), the pupil is small but reactive (the parasympathetic pathway is intact), and there may be facial anhidrosis depending on the level of the lesion. Look for the associated clues: a brachial plexus tumour (Pancoast) causing arm pain, a carotid dissection causing neck pain and an ischaemic stroke, or a brainstem stroke with the lateral medullary (Wallenberg) syndrome. The pharmacologic confirmation (cocaine or apraclonidine drops) and the imaging strategy depend on whether the lesion is central, preganglionic, or postganglionic; modern practice leans toward MRI of the sympathetic pathway rather than stepwise drop testing [4].
The eyelids
Inspect for ptosis. Decide the mechanism: a CN III ptosis is complete (the levator palpebrae is paralysed), a Horner ptosis is partial (a few millimetres), a myasthenic ptosis is variable and fatigable (worsens on sustained upgaze and improves with ice), and a senile or aponeurotic ptosis is chronic and fixed with a high lid crease. [1]
Eye movements
Ask the patient to keep their head still and follow your finger with their eyes. Draw an H-pattern — six cardinal directions — testing each muscle in its vertical action: right and left (medial and lateral rectus), up and right, down and right, up and left, down and left. At each extreme, ask the patient whether they see one finger or two (diplopia), and watch for nystagmus. The diplopia is always worst in the direction of action of the weak muscle — a simple rule that identifies the palsied nerve. [1]
The three eye-movement palsies and their directions: [1]
- CN III palsy — the eye is down and out at rest, with ptosis and a pupil that may be dilated. Diplopia is relieved by the ptosis (the lid covers the eye). The patient may adopt a head turn away from the affected side.
- CN IV (trochlear) palsy — the superior oblique is weak, so the eye elevates (the action of the inferior oblique is unopposed) and intorts. Diplopia is worst on looking down and in — classically when reading or descending stairs — and the patient tilts their head away from the affected side to reduce the torsion. This head tilt is the giveaway.
- CN VI (abducens) palsy — the lateral rectus is weak, so the eye will not abduct and rests adducted. Diplopia is worst on looking toward the affected side. The sixth nerve has the longest intracranial course and is vulnerable to raised intracranial pressure, where a bilateral palsy is a false localising sign pointing to a distant mass. [1]


CN V — Trigeminal
The trigeminal nerve has three sensory divisions and a motor component. Examine sensation, the corneal reflex, motor bulk, and the jaw jerk. [1]
Sensation. Test light touch (cotton wisp) and pinprick (pin) in each of the three divisions on both sides — the ophthalmic (V1) on the forehead, the maxillary (V2) on the cheek, and the mandibular (V3) on the jaw. Ask the patient to close their eyes and say "sharp" or "soft" and compare sides. A dissociated loss — pinprick gone but touch preserved — points to a brainstem lesion (the spinal trigeminal tract); a complete loss in all three divisions points to a peripheral nerve or Gasserian ganglion lesion; a loss confined to one division localises to a branch injury (V1 after orbital trauma, V2 or V3 after a maxillary or mandibular fracture or a basal skull tumour). [1]
Corneal reflex. This is the most discriminating test of the ophthalmic division. Ask the patient to look up and away. Gently touch the lateral cornea (not the conjunctiva, and never the centre) with a wisp of cotton wound to a point. Both eyes should blink. The afferent limb is V1 and the efferent limb is CN VII (facial). A loss of the direct blink (same eye) but preservation of the consensual blink (opposite eye) means the afferent V1 is intact and the efferent VII is out on the touched side — a Bell palsy. A loss of both blinks when touching the affected side, with preservation when touching the other side, means the afferent V1 is out on the affected side. Test both sides and reason through the circuit at viva. [1]
Motor. Inspect the temporalis and masseter for wasting — best seen in the temporalis fossa. Ask the patient to clench their teeth and palpate the masseter and temporalis — they should contract firmly and symmetrically. Unilateral weakness causes the jaw to deviate toward the affected side on opening (the intact pterygoids push the jaw across). [1]
Jaw jerk. Ask the patient to let their jaw hang open. Place your finger on the chin and tap it with the reflex hammer. A brisk jaw jerk indicates a bilateral upper motor neuron lesion above the mid-pons — most commonly motor neuron disease or diffuse cerebrovascular disease. A normal jaw jerk is a single, gentle movement. Never call a present jaw jerk abnormal in isolation; it must be pathologically brisk to signify anything. [1]
CN VII — Facial
The facial nerve is the most frequently examined cranial nerve in the short case because the UMN-versus-LMN distinction is visible from the door. Examine by inspection, then four active movements. [1]
Inspect. Look at the face at rest: are the forehead wrinkles symmetric, is there a nasolabial fold on both sides, does the mouth angle sit level? Unilateral flattening of the nasolabial fold and drooping of the mouth angle are visible before you test. [1]
Raise the eyebrows (frontalis). Ask the patient to wrinkle their forehead and look up. This is the decisive test. Because the upper face receives bilateral cortical innervation, an upper motor neuron (UMN) lesion (a stroke) spares the forehead — the patient can still wrinkle it. A lower motor neuron (LMN) lesion (Bell palsy) abolishes forehead wrinkling on the affected side. Forehead sparing equals UMN; forehead loss equals LMN. [1]
Close the eyes tightly (orbicularis oculi). Ask the patient to screw their eyes shut and resist your attempt to open them. In an LMN lesion the eye cannot be closed and the Bell phenomenon is seen — the eyeball rolls upwards and outwards as the patient tries to close the lid. In a UMN lesion the eye closes with reduced force but the patient can usually keep it shut. [1]
Show the teeth (orbicularis oris). Ask the patient to show their teeth or blow out their cheeks. The mouth fails to elevate on the weak side, and in a severe LMN lesion the cheek cannot be puffed out (air escapes). Show teeth yourself to demonstrate. [1]
Puff out the cheeks. Air escapes on the weak side. This also screens for a palatal or facial weakness pattern. [1]
The clinical reasoning: a UMN facial weakness is a stroke or a hemisphere tumour — the forehead is spared and the limb weakness on the same side tells you it is a cortex lesion. An LMN facial weakness is Bell palsy (idiopathic, by far the commonest), Ramsey Hunt syndrome (herpes zoster oticus, with vesicles in the ear and a worse prognosis), otitis media, a parotid tumour or surgery, or a skull base fracture. The treatment of Bell palsy is oral corticosteroids started within 72 hours of onset, which significantly improves the chance of complete recovery; the addition of antivirals adds little or no benefit over steroids alone [1][2][3]. Always examine the ear (for vesicles and discharge) and the parotid (for a mass or a scar) in an LMN palsy — the facial nerve exits the stylomastoid foramen and runs through the parotid, so a parotidectomy commonly injures it.
CN VIII — Vestibulocochlear
Test the cochlear (hearing) and vestibular divisions. [1]
Bedside hearing. Mask the opposite ear by rubbing the tragus or occluding the meatus, then whisper a number into the test ear from sixty centimetres. Compare sides. If hearing is reduced, perform the tuning fork tests with a 512 Hz fork (never 128 Hz — too low, vibrates rather than rings; never 1024 Hz — too high, fades too fast). [1]
Rinne test. Strike the fork and hold the base on the mastoid process (bone conduction) until the patient can no longer hear it, then immediately move the vibrating tines beside the ear canal (air conduction). In a normal ear or a sensorineural loss, air conduction is heard longer than bone — Rinne positive. In a conductive loss (otosclerosis, otitis media, wax), bone conduction is heard longer than air — Rinne negative. A severe sensorineural loss on the tested side can give a false negative Rinne because the sound crosses to the good cochlea via the skull — the patient hears it via the opposite ear's bone conduction; the Weber test resolves the ambiguity. [1]
Weber test. Strike the fork and place the base on the vertex or forehead midline. Ask the patient where they hear the sound. In a conductive loss the sound lateralises to the worse ear (it is not masked by ambient air conduction, so bone conduction relatively dominates). In a sensorineural loss the sound lateralises to the better ear. So: conductive — heard in the bad ear; sensorineural — heard in the good ear. [1]
If hearing loss is confirmed, refer for formal pure-tone audiometry. A unilateral progressive sensorineural loss raises the possibility of a vestibular schwannoma and warrants an MRI internal auditory meatus. [1]
Vestibular function. In a routine cranial-nerve examination, test Romberg's sign (the patient stands with feet together, eyes open then closed; a marked worsening on eye closure suggests a proprioceptive or vestibular deficit, though a cerebellar lesion causes unsteadiness with eyes open too) and, if relevant, the Unterberger/Fukuda stepping test (marching on the spot for one minute; rotation toward one side suggests a unilateral vestibular paresis). The full vestibular battery — the head impulse test, the Dix-Hallpike manoeuvre, caloric testing — belongs to the dedicated balance examination. [1]
CN IX and X — Glossopharyngeal and Vagus
These two nerves are examined together because they share the palate and the gag reflex. [1]
Inspect the palate and the voice. Listen to the voice first: a hoarse (dysphonic) voice suggests a recurrent laryngeal nerve palsy (a branch of the vagus); nasal speech or nasal regurgitation of fluids suggests palatal weakness. Ask the patient to say "ah" and watch the palate and uvula. The palate elevates symmetrically and the uvula stays midline in health. In a unilateral vagal (LMN) lesion, the intact side elevates and pulls the uvula away from the lesion — the uvula deviates toward the good side. In a bilateral UMN lesion (pseudobulbar palsy), the palate elevates poorly and the gag reflex is brisk. [1]
Gag reflex. Gently touch each posterior pharyngeal wall with a tongue depressor or a swab. The patient gags. The afferent limb is CN IX (glossopharyngeal) and the efferent limb is CN X (vagus). An absent gag on touching one side but present on the other localises the afferent (IX) lesion to the side that does not gag; an absent gag on both sides with a normal palate is usually a normal variant in the elderly and is not, by itself, a lesion. The gag reflex is uncomfortable and not always necessary — many examiners accept a visible palatal elevation as adequate. [1]
CN XI — Accessory
The spinal accessory nerve supplies the sternocleidomastoid (SCM) and the trapezius. [1]
Trapezius. Ask the patient to shrug their shoulders against your resistance. Unilateral weakness causes a drooping shoulder and a scapula displaced downward and laterally. [1]
Sternocleidomastoid. Ask the patient to turn their head to one side against your hand, and palpate the opposite SCM. The SCM turns the head to the opposite side — so to test the right SCM, ask the patient to turn the head to the left. An LMN lesion (after neck surgery or a jugular foramen tumour) wastes and weakens the muscle. A UMN lesion is harder to detect because the SCM receives substantial bilateral cortical input, but in a hemispheric stroke the head may be turned toward the side of the lesion (the intact hemisphere drives the contralateral SCM, rotating the head toward the weak limbs). [1]
CN XII — Hypoglossal
The hypoglossal nerve moves the tongue. [1]
Inspect the tongue in the mouth. Look for wasting and fasciculations on the surface — these indicate an LMN lesion or motor neuron disease. A normal tongue lies in a gentle curve within the mouth; a wasted tongue is wrinkled and reduced in bulk, and fasciculations are brief, irregular flickers across the surface, best seen with the tongue relaxed in the floor of the mouth (asking the patient to protrude it induces normal tremor, which is not fasciculation). [1]
Protrude the tongue. Ask the patient to stick out their tongue. In a unilateral LMN lesion the tongue deviates toward the side of the lesion (the intact genioglossus pushes the tongue forward and across). In a unilateral UMN lesion the tongue deviates away from the cortical lesion (toward the weak side of the body), without wasting. Bilateral wasting with fasciculations and a spastic palate is bulbar motor neuron disease. The direction rule — the tongue points to the lesion in an LMN palsy — is the rule examiners test. [1]
The say-aloud presentation template
When you finish, stand back and present a structured, localising summary. Lead with the patient, state the abnormal system, give the localising sign, offer the differential, and propose the next investigation. A model presentation for a candidate with a pupil-sparing third nerve palsy: [1]
"I examined Mr Shah, a 68-year-old man with diabetes and hypertension. He is alert and cooperative. On examination of the cranial nerves, the pupils are equal and reactive and there is no relative afferent pupillary defect. There is a complete ptosis of the right eye, and the right eye is deviated down and out. The right eye fails to adduct, elevate or depress, and abduction is preserved. There is a fatigable diplopia in the directions of the weak muscles. The remaining cranial nerves, including the facial nerve and the tongue, are intact. [1]
In summary, this patient has a complete right third nerve palsy with the pupil spared. A pupil-sparing, complete third nerve palsy in a vasculopathic patient is consistent with a microvascular (ischaemic) oculomotor palsy. I would confirm the vascular risk factors, check the blood glucose and lipids, and expect spontaneous recovery over three months. Because the rule of the pupil is a guide and not absolute, I would arrange urgent CT angiography of the intracranial circulation to exclude a posterior communicating artery aneurysm, and refer to neurology." [1]
Three habits that separate a passing from a failing presentation: say the diagnosis before the differential; state the single sign that localises it (here, the spared pupil); and always propose the next investigation — never leave the examiner to ask "and what would you do?". [1]
Examiner discussion questions
The discussion after a cranial-nerve short case tests reasoning, not memory. The following questions recur; prepare a one-paragraph answer to each. [1]
"Why does a pupil-involving third nerve palsy demand urgent imaging?" Because the parasympathetic pupillary fibres run on the surface of the third nerve, and a lesion that involves the pupil is compressive until proven otherwise. The classic cause is a posterior communicating artery aneurysm at its junction with the internal carotid, which lies beside the third nerve; as it expands it compresses the surface fibres first, dilating the pupil before it paralyses the eye. An expanding aneurysm may rupture into a subarachnoid haemorrhage, which carries a high mortality. A painful third nerve palsy with a dilated pupil is therefore a neurosurgical emergency requiring urgent CT angiography and, if confirmed, endovascular or surgical securing of the aneurysm. The rule is not absolute — a pupil-involving palsy can rarely be microvascular, and a pupil-sparing palsy can rarely be compressive, especially if incomplete and evolving — so most neuro-ophthalmologists image any new third nerve palsy that does not fit the textbook microvascular pattern. [1]
"How do you distinguish an upper from a lower motor neuron facial palsy, and why does it matter?" By the forehead. The upper facial muscles (frontalis, orbicularis oculi) receive bilateral cortical input, so a UMN lesion in the motor cortex spares the forehead — the patient can still wrinkle it and close the eye, though with reduced force. The lower face (orbicularis oris) receives only contralateral input, so a UMN lesion paralyses the lower face on the opposite side. An LMN lesion, by contrast, abolishes movement of the entire hemiface — forehead, eye and mouth — because the facial nerve itself is out. The distinction matters because a UMN facial palsy is a stroke (look for ipsilateral limb weakness and aphasia) while an LMN facial palsy is Bell palsy or a peripheral lesion (examine the ear and the parotid, and start steroids within 72 hours) [1][2].
"What is the significance of a relative afferent pupillary defect, and how do you test for it?" The swinging-flashlight test compares the two optic nerves. A normal pupil constricts each time the light enters either eye. When the light swings into an eye with an optic nerve lesion, the brain perceives less light, the stimulus to constriction falls, and both pupils dilate — a paradoxical dilation that signals a relative afferent pupillary defect (a Marcus Gunn pupil). The defect is relative because it compares the two eyes; bilateral symmetric optic nerve disease produces no RAPD. The RAPD localises to the afferent pathway (the retina or optic nerve, not the chiasm or behind it), and it is the most sensitive clinical sign of an optic neuropathy — present before acuity falls or the disc looks abnormal [5].
"How do you interpret Rinne and Weber, and what are the pitfalls?" Rinne compares air and bone conduction on one side: air longer than bone (positive) is normal or sensorineural; bone longer than air (negative) is conductive. Weber lateralises to the worse ear in a conductive loss and to the better ear in a sensorineural loss. The pitfall is the severe unilateral sensorineural loss: when you test that ear by bone, the sound crosses the skull and is heard by the good cochlea, giving a false negative Rinne. The Weber test resolves it — in a true conductive loss the Weber lateralises to that ear, whereas in a sensorineural loss it lateralises away. If the two tests disagree, trust the Weber and request audiometry. [1]
"What causes a Horner syndrome and how do you localise it?" Horner syndrome is interruption of the three-neuron sympathetic chain to the eye: the central first-order neuron from the hypothalamus to the ciliospinal centre (a brainstem or cervical cord stroke, classically lateral medullary), the preganglionic second-order neuron that exits at T1 and climbs over the lung apex (a Pancoast tumour, a brachial plexus injury) and the postganglionic third-order neuron travelling with the carotid into the cavernous sinus (a carotid dissection, a cluster headache, a cavernous sinus lesion). Anhidrosis helps localise: central and preganglionic lesions cause hemifacial anhidrosis, whereas postganglionic lesions cause anhidrosis confined to the forehead (the sweat fibres to the face travel with the external carotid). Pharmacologic confirmation with apraclonidine (a Horner pupil dilates, a normal pupil constricts) is now preferred over cocaine, and MRI of the sympathetic pathway is the imaging strategy in the modern era [4]. Because a carotid dissection is a treatable cause of stroke, a painful Horner syndrome warrants urgent imaging.
Common traps and pitfalls
The candidates who fail the cranial-nerve station do so for predictable reasons. Avoid these: [1]
- Breaking sequence to chase a sign. A candidate sees a facial droop, abandons the eye examination, tests the face, and never returns to the pupils. Finish each nerve in order; the abnormality goes into the presentation, not the sequence. Examiners mark the routine as heavily as the findings.
- Failing to test the swinging flashlight. Many candidates test direct and consensual reflexes and stop. The RAPD is the single most sensitive sign of optic nerve disease and the test most often omitted. Practise it until it is automatic [5].
- Misclassifying the pupil in a third nerve palsy. The temptation is to call every third nerve palsy compressive. A complete palsy with the pupil spared in a vasculopathic patient is microvascular and managed conservatively; a pupil-involving palsy is compressive and imaged urgently. Partial and evolving palsies are imaged regardless — the rule of the pupil is a heuristic, not a law.
- Confusing UMN and LMN facial weakness. Test the forehead. If you do not explicitly raise the eyebrows, you cannot make the distinction, and you will fail the discussion. The same applies to the tongue — a wasted, fasciculating tongue that deviates to the lesion is LMN; a non-wasted tongue that deviates away from a cortical lesion is UMN.
- Forgetting the ear and the parotid in an LMN facial palsy. Ramsey Hunt vesicles, otitis media, and a parotid mass or surgical scar change the diagnosis and the management. Examine them; state that you have.
- Misreading the corneal reflex. Reason through the circuit: V1 afferent, VII efferent. A loss of both blinks when touching the bad side is an afferent (V1) lesion; a loss of the direct but not the consensual blink is an efferent (VII) lesion. State the circuit aloud at viva.
- Calling a brisk jaw jerk in isolation. The jaw jerk signifies a bilateral UMN lesion only when pathologically brisk. A present jaw jerk is normal; over-calling it is a common error.
- Not asking about diplopia in each direction of gaze. The diplopia is worst in the direction of action of the weak muscle. If you do not ask, you cannot localise the palsy, and the eye movements become guesswork.
- Neglecting the fundus. Papilloedema and optic atrophy are high-yield findings that change the entire case. If the pupils permit, dilate and look; if not, look anyway. A candidate who presents a cranial-nerve case without having looked at the discs has not completed the examination.
Integration with the long case
Cranial-nerve findings appear in the DCE long case as one problem among several, and the skill is to integrate them. A patient with a stroke may have a facial palsy (CN VII), a hemianopia (CN II) and dysphagia (CN IX, X) alongside limb weakness — the cranial nerves localise the lesion to the brainstem or the cortex and frame the rehabilitation plan. A patient with motor neuron disease may show tongue wasting and fasciculation (CN XII), a brisk jaw jerk (CN V), and pseudobulbar palatal weakness — a pattern that, with limb signs, secures the diagnosis. A patient with a thymoma and myasthenia gravis may have fatigable ptosis and ophthalmoplegia that mimic a cranial-nerve palsy — the variability and the pupil sparing distinguish it. Always set the cranial-nerve findings into the problem list and the management plan, never as an isolated observation. [1]
The cranial-nerve short case rewards the candidate who is systematic, fluent and localising. Practise the sequence until it is a reflex; learn the signs until their interpretation is instant; rehearse the presentation until it leads with the diagnosis. That is the standard the examiner expects, and the standard that passes. [1]
References
- [1]Sullivan FM, Swan IR, Donnan PT, et al. Early treatment with prednisolone or acyclovir in Bell's palsy N Engl J Med, 2007.PMID 17942873
- [2]Madhok VB, Gagyor I, Daly F, et al. Corticosteroids for Bell's palsy (idiopathic facial paralysis) Cochrane Database Syst Rev, 2016.PMID 27428352
- [3]Gagyor I, Madhok VB, Daly F, Sullivan F Antiviral treatment for Bell's palsy (idiopathic facial paralysis) Cochrane Database Syst Rev, 2019.PMID 31486071
- [4]Sadaka A, Schockman SL, Golnik KC Evaluation of Horner Syndrome in the MRI Era J Neuroophthalmol, 2017.PMID 28445191
- [5]Chang DS, Xu L, Boland MV, Friedman DS Accuracy of pupil assessment for the detection of glaucoma: a systematic review and meta-analysis Ophthalmology, 2013.PMID 23809274