Phys · general-medicine
Neurological Examination of the Lower Limbs — The DCE Short-Case Routine
Also known as lower limb neurological examination · lower limb neurological exam · neurological examination lower limbs · examine this patient lower limbs neurologically · DCE short case lower limb neurology · PACES neurological station lower limb · motor examination lower limb · heel-shin test · Romberg test · Babinski sign · plantar response · ankle clonus · MRC power grading · myotome examination lower limb · dermatome examination lower limb · tone power reflexes coordination sensory gait · UMN versus LMN · pes cavus · high-stepping gait · foot drop
Consultant-physician-depth guide to the systematic neurological examination of the lower limbs for the FRACP DCE short case and the MRCP PACES neurological station. Covers the eight-step routine — inspection including gait and stance, tone with ankle clonus, power by myotome, reflexes by root level, the plantar response, coordination with the heel-shin test, the spinothalamic and dorsal column sensory pathways, and the gait assessment — the interpretation of each sign, the UMN versus LMN framework, the presentation template the candidate delivers aloud, and the examiner discussion questions by finding. Addresses gait patterns (hemiplegic, parkinsonian, ataxic, high-stepping, waddling), the Romberg test, muscle wasting patterns, foot deformity (pes cavus in Friedreich ataxia and Charcot-Marie-Tooth), tone abnormalities (spasticity with clonus, lead-pipe rigidity), the MRC power grading with myotomes from L2 to S2, reflex levels (knee jerk L3/4, ankle jerk S1/2), the absent ankle jerk with preserved knee jerk of diabetic neuropathy and the delayed relaxation of hypothyroidism, the Babinski sign, the heel-shin test for cerebellar function, stocking-distribution sensory loss, and the common examination traps. Structured for FRACP DCE and MRCP PACES preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Neurological Examination of the Lower Limbs — The DCE Short-Case Routine

The answer first
The instruction "Please examine this patient's lower limbs neurologically" is one of the most frequently tested DCE short-case stations in the FRACP examination, and it is a classic neurological station in the MRCP PACES Station 3. The lower limb differs from the upper limb in one critical respect: the gait and the stance are observable before the candidate touches the patient, and they alone can deliver the diagnosis. The candidate who watches the patient walk to the examination couch has often generated the differential — hemiplegic, parkinsonian, ataxic, high-stepping, or waddling — before a single reflex is struck. [1]
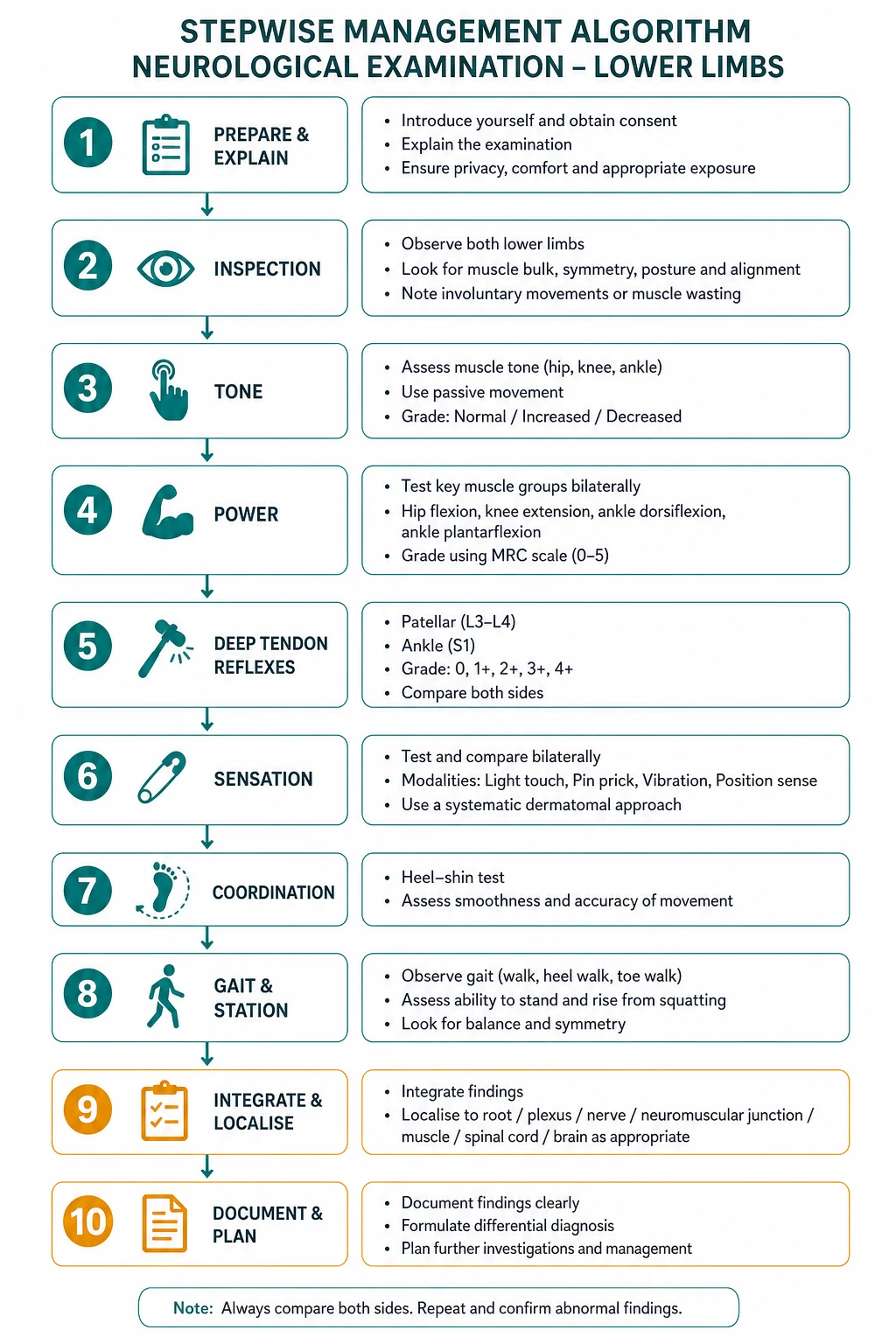
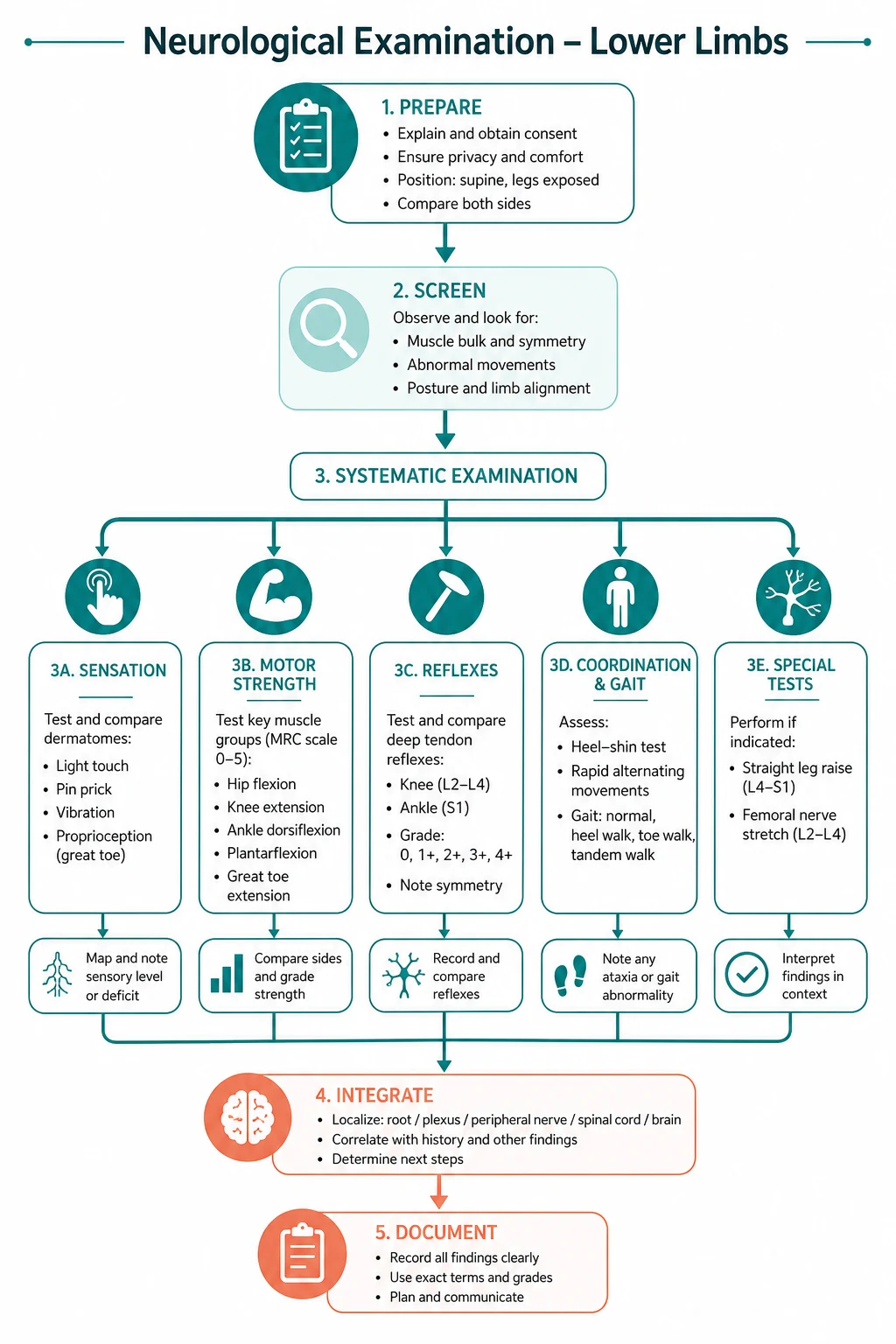
The routine is eight steps, performed in the same order every time: [1]
- Gait and inspection — gait pattern, stance including Romberg, muscle wasting, fasciculations, foot deformity, scars
- Tone — at the hip, the knee, and the ankle; ankle clonus
- Power — by myotome, with MRC grading
- Reflexes — knee jerk, ankle jerk; with reinforcement
- Plantar response — Babinski
- Coordination — heel-shin test, foot tapping
- Sensory — light touch, pinprick (spinothalamic), vibration, joint position (dorsal column); dermatomes
- Functional and completion — toes and heels walking, and the statement of the rest of the neurological exam [1]

The candidate who skips the gait, or who forgets the plantar response or the Romberg test, has failed the sequence and has also failed to collect the data the localisation requires. The eight steps are not an arbitrary checklist — they are the order in which the lesion declares itself, and the order in which the examiner expects the findings. [1]
Viva trap: "What is the single most important observation in the first thirty seconds of the lower limb neurological exam?" The honest answer is the gait. No other part of the neurological examination compresses so much diagnostic information into so short an observation. A hemiplegic gait with circumduction shouts cortical UMN lesion; a shuffling, festinating gait with reduced arm swing shouts Parkinson disease; a wide-based ataxic gait shouts cerebellum or dorsal column; a high-stepping foot-drop gait shouts a common peroneal nerve or L5 root lesion. The candidate who starts at the ankle reflexes without watching the patient walk has surrendered the single highest-yield observation of the entire station. [1]
Step 1 — Gait and inspection: the look test that frames the differential
The lower limb examination begins the moment the patient walks into the room. The candidate observes the gait first, then exposes both legs to the groin (preserving dignity with a gown or sheet) and inspects systematically from the hip to the toes, comparing left with right. [1]
The gait — five patterns that each name a lesion

-
Hemiplegic (spastic) gait — the affected leg is held stiff and extended, and the foot is plantarflexed and inverted; the patient swings the leg outward in a semicircle (circumduction) to clear the toes. This is the gait of an established upper motor neuron lesion — a chronic stroke, a residual from a hemispheric lesion. The circumduction, the equinus foot posture, and the associated flexed posture of the ipsilateral arm together form the classic hemiparetic picture. [1]
-
Parkinsonian gait — slow to start (start hesitation), shuffling with short steps, festination (the steps accelerate and shorten as if chasing the centre of gravity), reduced or absent arm swing, flexed posture of the trunk and limbs, and freezing at doorways or on turning. The MDS clinical diagnostic criteria define parkinsonism as bradykinesia plus rest tremor or rigidity, and the gait is a core manifestation [4]. The reduced arm swing is often the earliest and most asymmetric sign.
-
Cerebellar ataxic gait — a wide-based, unsteady, staggering gait with irregular foot placement, worse on turning or on tandem walking. The patient walks as if drunk. This localises to the midline cerebellar structures (the vermis) when the ataxia is symmetric, or to a cerebellar hemisphere when it is asymmetric and accompanied by ipsilateral limb dysmetria. The tandem (heel-to-toe) gait exaggerates and reveals the subtle cerebellar ataxia. [1]
-
Sensory ataxic gait (stamping gait) — a broad-based gait with high lifting of the legs and a stamping footfall, the patient watching the ground and their feet intently to compensate for the loss of joint position sense. This is the gait of a dorsal column lesion — tabes dorsalis classically, but more commonly today a peripheral neuropathy or a vitamin B12 deficiency. The discriminating test: the patient who walks steadily eyes open but loses balance eyes closed has a positive Romberg — sensory ataxia, not cerebellar. [1]
-
High-stepping (steppage) gait with foot drop — the patient lifts the affected leg excessively high to clear the dropped foot, and the forefoot slaps the ground on landing (a slapping foot drop). This is the gait of a foot drop — weakness of ankle dorsiflexion, most commonly a common peroneal (fibular) nerve palsy, an L4/5 radiculopathy, or a severe peripheral neuropathy. The candidate who hears the slap before they see the lift has the diagnosis. [1]
-
Waddling gait — a rolling, side-to-side gait with exaggerated lumbar lordosis, the shoulders lurching to compensate for weak hip abductors. This is the gait of a proximal myopathy (the pelvifemoral muscular dystrophies, polymyositis, statin myopathy, Cushing myopathy) or of hip disease. The patient cannot stabilise the pelvis in the stance phase (a positive Trendelenburg sign — the pelvis drops on the contralateral side when standing on the affected leg). [1]
Muscle wasting — the pattern identifies the lesion
Generalised wasting of the lower limb with reduced muscle bulk throughout indicates a chronic lower motor neuron process — a severe peripheral neuropathy, an old polio, or advanced motor neuron disease with extensive LMN involvement. [1]
Distal wasting (the "inverted champagne bottle" legs — slender calves and ankles with preserved thigh bulk) is the classic sign of a hereditary motor sensory neuropathy (Charcot-Marie-Tooth disease), in which the peroneal muscles and the tibialis anterior are preferentially denervated, producing wasting below the knee with a stork-leg appearance [7].
Proximal wasting (the thigh quadriceps and the hip girdle, with preserved distal bulk) points to a proximal myopathy — polymyositis, dermatomyositis, the muscular dystrophies, or a steroid myopathy. The candidate who tests the proximal muscles (hip flexion, hip abduction, knee extension) in a patient with proximal wasting has confirmed the distribution. [1]
Focal wasting of the tibialis anterior (the shiny, wasted anterior tibial compartment with the foot held in equinovarus) indicates a common peroneal nerve palsy or an L4/5 root lesion. The foot drop is the clinical correlate. [1]
Asymmetric focal wasting with fasciculations, especially of one calf or one thigh, in a patient with brisk reflexes and an upgoing plantar on the same side, is the signature of motor neuron disease affecting the lumbosacral segment [1][2].
Fasciculations — the sign of anterior horn cell disease
Fasciculations are involuntary, brief, visible muscle twitches under the skin — the clinical signature of anterior horn cell or motor axon irritability. In the lower limbs the candidate looks at the quadriceps, the calf (gastrocnemius), the tibialis anterior, and the small muscles of the foot. The interpretation is the same as in the upper limb: fasciculations with weakness and wasting indicate a lower motor neuron lesion. Widespread fasciculations with wasting, weakness, and brisk reflexes (UMN signs) in the same or other limbs is the signature of motor neuron disease (amyotrophic lateral sclerosis) [1][2]. Benign fasciculations (without weakness, without wasting, without reflex change) are common, especially in the calf of healthy young adults, and do not indicate disease.
Foot deformity — the hereditary neuropathies and the ataxias
Pes cavus (a high-arched foot with clawing of the toes and a rigid plantar-flexed first ray) is the single most important hereditary deformity in the neurological short case. Pes cavus is bilateral, long-standing (present since childhood, often noticed by the patient's mother), and points to a hereditary motor sensory neuropathy (Charcot-Marie-Tooth) or a hereditary cerebellar ataxia (Friedreich ataxia). The two are discriminated by the rest of the exam: in CMT the patient has a peripheral neuropathy (distal wasting, weakness, areflexia, distal sensory loss, and often a family history) [7]; in Friedreich ataxia the patient has absent lower limb reflexes with upgoing plantars (a pathognomonic combination), dysarthria, a cardiomyopathy, scoliosis, and often diabetes [5][6].
The teaching point: a patient with pes cavus and upgoing plantars has Friedreich ataxia until proven otherwise, and a patient with pes cavus and downgoing plantars with a peripheral neuropathy has Charcot-Marie-Tooth until proven otherwise. Pes cavus is the high-yield foot deformity that must be actively sought and presented. [1]
A clawed foot with equinovarus deformity (the foot plantarflexed and inverted, the toes hyperextended at the MTP and flexed at the IP joints) indicates a common peroneal nerve palsy or an L4/5 root lesion — the imbalance between the paralysed dorsiflexors and the intact plantarflexors and inverters. [1]
Scars — lumbar spine scars (laminectomy, spinal instrumentation), hip and knee replacement scars, varicose vein stripping scars, and amputation or arterial bypass scars — all carry diagnostic information and must be noted. A lumbar spine scar in a patient with a foot drop reframes the differential toward a structural L4/5 lesion or a postoperative cauda equina injury. [1]
Step 2 — Tone: the gateway to UMN versus LMN
Tone is assessed at three joints: the hip, the knee, and the ankle. The candidate rolls the leg on the bed (assessing hip adductor tone), then passively flexes and extends the knee, then briskly dorsiflexes the ankle with the knee flexed. The patient must be relaxed; the candidate compares left with right. The four abnormalities are: [1]
Spasticity — the clasp-knife and the UMN lesion
Spasticity is velocity-dependent increased tone — the resistance is greater with fast passive movement and less with slow movement. The classic description is the clasp-knife phenomenon: an initial strong resistance that suddenly gives way as the movement continues, like the blade of a clasp knife snapping shut. In the lower limb, spasticity preferentially affects the extensors (the quadriceps, the gastrocnemius) — the pyramidal distribution, which is the opposite of the upper limb (where the flexors are preferentially affected). The localisation: a corticospinal tract (upper motor neuron) lesion anywhere from the motor cortex to the spinal cord segment above the muscle. A hemispheric stroke produces contralateral leg spasticity; a spinal cord lesion produces bilateral leg spasticity (paraplegia) with sparing of the arms. [1]
Clonus — the sustained UMN sign
Clonus is tested at the ankle by rapidly dorsiflexing the relaxed foot (a single sharp upward push at the forefoot, with the knee flexed and the ankle supported). A sustained, rhythmic, repetitive beating of the foot — three or more beats, or indefinitely — is sustained clonus, a definitive sign of an upper motor neuron lesion. One or two beats may be physiological (especially in anxious or anxious-examined patients), but sustained clonus is always pathological. Clonus localises to the corticospinal tract and confirms the UMN pattern when combined with spastic tone and a brisk reflex. The candidate who elicits clonus and does not present it has missed a cardinal sign. [1]
Rigidity — the lead-pipe and the cogwheel
Rigidity is velocity-independent increased tone — the resistance is constant throughout the range of movement, independent of speed. In the lower limb, rigidity is best felt at the hip and knee by slow, continuous passive movement. Lead-pipe rigidity — a smooth, uniform resistance throughout the range — is a basal ganglia sign, seen in Parkinson disease and other parkinsonian syndromes. Cogwheel rigidity — a ratchety, jerky resistance that is the combination of lead-pipe rigidity with a superimposed tremor — is also a Parkinsonian sign, though in the lower limb it is less prominent than in the upper limb. The teaching point: spasticity and rigidity are both increased tone, but they localise differently — spasticity to the corticospinal tract (pyramidal), rigidity to the basal ganglia (extrapyramidal) [4].
Hypotonia — the LMN and cerebellar sign
Hypotonia — reduced or absent resistance to passive movement, a "floppy" leg — is seen in lower motor neuron lesions (where the denervated muscle offers no resistance), in cerebellar disease, in acute UMN lesions (spinal shock — the first 24 to 48 hours after an acute cord lesion, before spasticity develops), and in muscle disease (myopathy). The hypotonic leg may show pendular reflexes — the knee jerk, when struck, oscillates several times like a pendulum before settling, classically seen in cerebellar disease. [1]
Step 3 — Power: the myotome map and the MRC grade

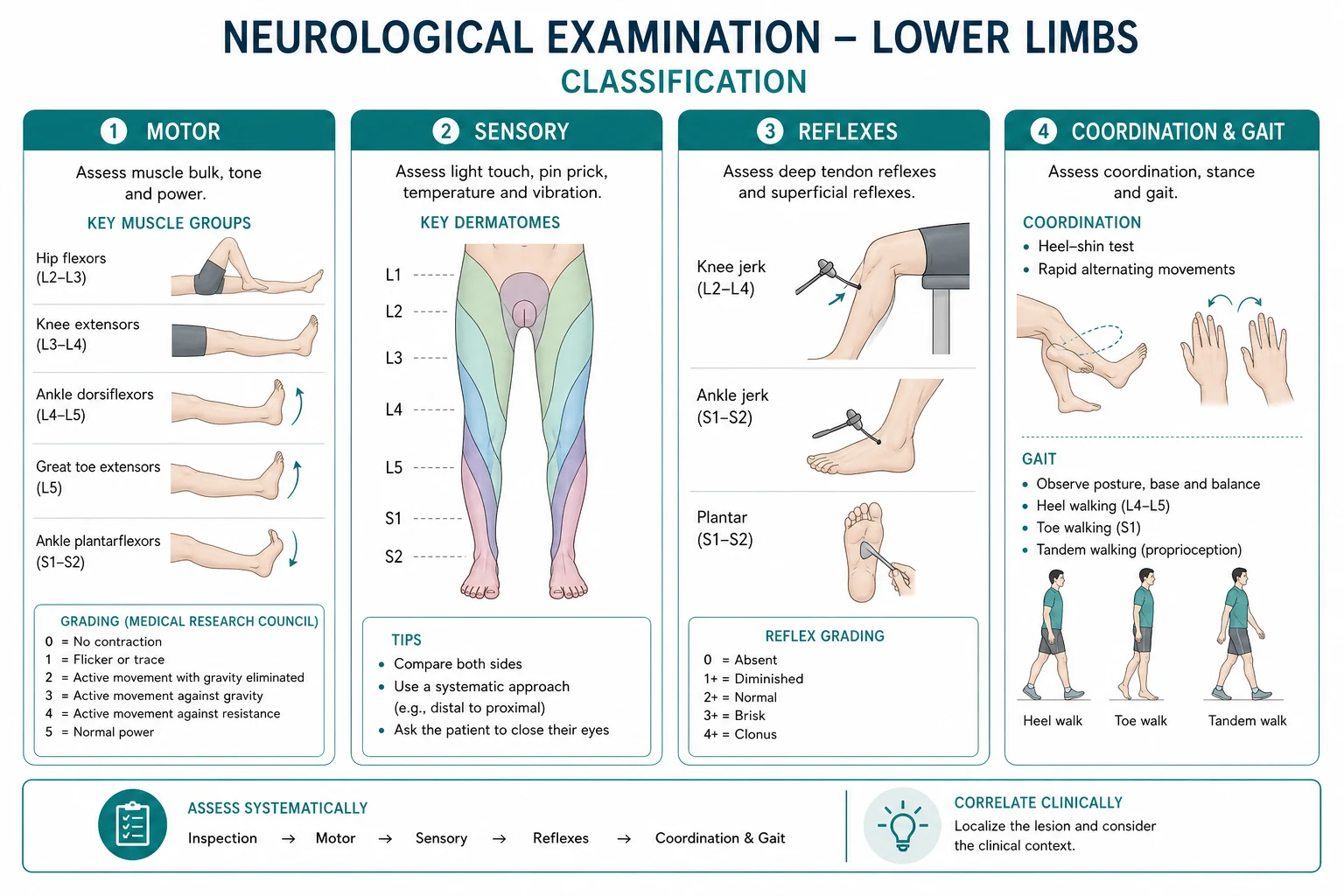
Power is tested by myotome, with the muscle group acting against the candidate's resistance. The candidate tests each movement, compares left with right, and grades with the Medical Research Council scale (0 to 5): [1]
- 0 — no contraction
- 1 — flicker of contraction, no movement
- 2 — movement with gravity eliminated (horizontal plane)
- 3 — movement against gravity
- 4 — movement against resistance (with the subdivisions 4-minus, 4, 4-plus)
- 5 — normal power [1]
The myotome sequence for the lower limb, with the root, the muscle, and the action: [1]
| Movement | Root level | Key muscle | Action |
|---|---|---|---|
| Hip flexion | L1/L2 (also L3) | Iliopsoas | Lift the thigh off the bed against resistance |
| Hip extension | L4/L5/S1 | Gluteus maximus | Push the leg down into the bed |
| Hip abduction | L4/L5/S1 | Gluteus medius | Push the leg out against the hand on the lateral knee |
| Hip adduction | L2/L3 | Adductor group | Squeeze the legs together against the candidate's fist |
| Knee extension | L3/L4 | Quadriceps | Straighten the knee against resistance |
| Knee flexion | L5/S1/S2 | Hamstrings | Bend the knee against resistance |
| Ankle dorsiflexion | L4/L5 | Tibialis anterior | Pull the foot up against the hand on the dorsum |
| Ankle plantarflexion | S1/S2 | Gastrocnemius/soleus | Push down (stand on toes — the most sensitive test) |
| Great toe extension | L5 | Extensor hallucis longus | Pull the big toe up against resistance |
| Toe flexion | S1/S2 | Flexor digitorum/hallucis longus | Curl the toes down |
The high-yield teaching points: [1]
The pattern of weakness localises the lesion. A pyramidal (UMN) weakness of the lower limb preferentially affects the flexors (hip flexion, knee flexion, ankle dorsiflexion) — the opposite of the upper limb, where the extensors are preferentially affected. The foot drop and the equinus posture of the chronic stroke leg are the clinical correlate. A lower motor neuron weakness preferentially affects the muscles supplied by the damaged nerve or root — an L5 root lesion weakens great toe extension (EHL) and ankle dorsiflexion; a common peroneal nerve lesion weakens ankle dorsiflexion and eversion with sparing of inversion (tibialis posterior, tibial nerve) and of great toe extension. [1]
Great toe extension (extensor hallucis longus, L5) is the single most important myotome in the lower limb because it isolates the L5 root, which is the root most commonly compressed by an L4/L5 disc. The candidate who tests EHL has screened for the commonest radiculopathy. The discriminating point: in an L5 root lesion the inversion (tibialis posterior, L4/L5) is variably weak but eversion (peroneal muscles, L5/S1, superficial peroneal nerve) is also weak; in a common peroneal nerve palsy the eversion is weak and the inversion is spared (the tibial nerve and its branches are intact). This inversion-sparing is the bedside discriminator between an L5 root lesion and a common peroneal nerve palsy. [1]
The ankle plantarflexion (S1/S2) is best tested functionally by asking the patient to stand on their toes. A patient who can generate a normal plantarflexion against the hand but cannot stand on their toes has subtle S1 weakness that the resisted test misses. Plantarflexion is the last to be lost in a neuropathy because the gastrocnemius is the most powerful muscle in the body, and only the functional test (standing on toes) is sensitive enough to detect early weakness. [1]
Step 4 — Reflexes: the root level and the UMN sign
The deep tendon reflexes are tested with a tendon hammer, comparing left with right, and graded as 0 (absent), plus-minus (present with reinforcement), plus (normal), plus-plus (brisk), plus-plus-plus (very brisk with clonus). The candidate should use the Jendrassik manoeuvre for reinforcement: in the lower limb, the patient hooks the hands together and pulls apart hard (or clenches the fists and grits the teeth) while the candidate strikes the tendon — the reinforcement activates the gamma loop and brings out an absent reflex. [1]
The reflex arc and the root level: [1]
| Reflex | Root level | Nerve | Technique |
|---|---|---|---|
| Knee jerk (patellar) | L2/L3/L4 (mainly L4) | Femoral | Strike the patellar tendon just below the patella |
| Ankle jerk (Achilles) | S1/S2 (mainly S1) | Tibial | Dorsiflex the foot, strike the Achilles tendon |
The absent ankle jerk with preserved knee jerk — the diabetic neuropathy
The dissociated reflex pattern of absent ankle jerks with preserved (or even brisk) knee jerks is the classic bedside sign of a length-dependent peripheral neuropathy, most commonly diabetic neuropathy. The longest nerve in the body is the sensory and motor supply to the gastrocnemius (S1, via the tibial nerve), and it is the first to fail in an axonal neuropathy — hence the absent ankle jerk precedes the loss of the knee jerk as the neuropathy advances. The candidate who finds absent ankle jerks in an elderly patient with preserved knee jerks has the clinical sign of diabetic (or alcoholic, or nutritional) peripheral neuropathy, and the next step is a fasting glucose and an HbA1c. The teaching point: the ankle jerk is the first reflex lost in a peripheral neuropathy, and its isolated absence with preserved knee jerks is a high-yield finding. [1]
The delayed relaxation of the ankle jerk — the hypothyroid sign
Delayed relaxation of the ankle jerk — the foot, after the jerk, returns to its resting position slowly, with a visible "hang" — is the classic bedside sign of hypothyroidism. The mechanism is the slowed contraction and relaxation of the muscle in the hypothyroid state (a change in the calcium re-uptake kinetics of the sarcoplasmic reticulum). The sign is best elicited by kneeling the patient on a chair (the Wile reflex hammer test) and striking the Achilles tendon, watching the slow relaxation. A delayed-relaxation ankle jerk with a clinical picture of hypothyroidism (cold intolerance, bradycardia, weight gain, dry skin, delayed relaxation of other reflexes) is a high-yield bedside clue and prompts a serum TSH. [1]
The reflex interpretation framework
- Absent reflexes with weakness and wasting — lower motor neuron lesion (anterior horn cell, root, nerve). The combination of absent ankle jerks, distal wasting, distal weakness, and a stocking sensory loss is the classic peripheral neuropathy.
- Brisk reflexes with spastic tone and an upgoing plantar — upper motor neuron lesion (corticospinal tract). The combination of brisk reflexes, clonus, spastic tone, an extensor plantar, and pyramidal-pattern weakness is the classic hemiparesis or paraparesis.
- The mixed pattern — absent or reduced reflexes at one level with brisk reflexes at another, or a wasted fasciculating muscle with a brisk reflex — is the signature of motor neuron disease [1][2].
Step 5 — The plantar response: the Babinski sign
The plantar response is tested by stroking the lateral aspect of the sole of the foot, from the heel forward to the base of the little toe (avoiding the ball of the foot, which can produce a withdrawal response), with a reasonably sharp but painless stimulus — an orange stick, the handle of the tendon hammer, or a key. The candidate observes the movement of the great toe. [1]
- Downgoing (flexor) plantar — the normal adult response: the great toe flexes (moves downward) and the other toes curl.
- Upgoing (extensor) plantar — the Babinski sign — the great toe extends (dorsiflexes), often with fanning of the other toes and dorsiflexion of the ankle. This is a pathological reflex indicating an upper motor neuron (corticospinal tract) lesion — it is the lower-limb equivalent of the Hoffman sign in the upper limb. The Babinski sign is present in infants (the corticospinal tract is not yet myelinated) and reappears in adults with any lesion of the corticospinal tract: a stroke, a spinal cord lesion, multiple sclerosis, motor neuron disease, a structural brain lesion. [1]
The interpretation: an upgoing plantar is a UMN sign, and it must be interpreted with the tone and the reflexes. A spastic leg with a brisk knee jerk, sustained clonus, and an upgoing plantar is the complete UMN syndrome of the lower limb. The candidate who tests the plantar and does not present it has omitted a cardinal sign. [1]
The variants: the Chaddock sign (stroking the lateral border of the foot, below the lateral malleolus) is an alternative elicitation for the same reflex, useful when the standard Babinski is ambiguous or when the patient is too ticklish or too withdrawal-prone. The Oppenheim sign (running the knuckles down the anterior tibial crest) and the Gordon sign (squeezing the calf) are other alternatives, all testing the same corticospinal tract pathway. [1]
Step 6 — Coordination: the cerebellar and the UMN screen
Coordination testing of the lower limb assesses the cerebellum and the corticospinal tract. Two tests: [1]
The heel-shin test
The patient lies supine (or sits), and the candidate asks them to place the heel of one foot on the opposite knee, then run the heel down the shin (the anterior tibial crest) to the ankle, then back up to the knee — smoothly and accurately. The candidate watches for: [1]
- Dysmetria — the heel overshoots the knee or lands off-target. This is a cerebellar sign, localising to the ipsilateral cerebellar hemisphere (the anterior lobe for the lower limb).
- Intention tremor — a tremor that appears and worsens as the heel approaches the target (the ankle). This is a cerebellar sign.
- Ataxia — irregular, clumsy, broken movement that does not follow the line of the shin. Cerebellar.
- Pendular movement — the heel wobbles side to side as it descends, characteristic of cerebellar disease. [1]
The teaching point: the heel-shin test requires intact power. A patient with severe pyramidal weakness cannot lift the heel to the knee, and the candidate who interprets this inability as cerebellar dysmetria has confused weakness with incoordination. The candidate tests coordination only in a limb with adequate power, and explicitly notes "coordination is limited by weakness." [1]
Rapid foot tapping
The patient is asked to tap the foot (the forefoot, keeping the heel on the ground) as rapidly and regularly as possible against the candidate's hand or the floor. Dysrhythmia and slowness of the foot tapping is a cerebellar sign (the lower-limb equivalent of dysdiadochokinesia), and slowness without dysrhythmia may be a bradykinetic (parkinsonian) sign. The candidate compares left and right; the side with the worse foot tapping points to the ipsilateral cerebellar hemisphere. [1]
Step 7 — Sensory: the two-pathway framework
The sensory exam tests the two ascending pathways of the spinal cord: [1]
The spinothalamic pathway — pain and temperature
The candidate tests pinprick (using a disposable neurotip or the sharp end of a safety pin, disposed of in a sharps bin after single use) and, if indicated, temperature (a cold tuning fork or test tube). The patient closes their eyes and reports "sharp" or "dull" as the candidate alternates the sharp and blunt ends on the skin. [1]
The candidate tests the dermatomes of the lower limb: L1 (the inguinal region and the superior anterior thigh), L2 (the anterior thigh), L3 (the medial knee), L4 (the medial calf and the medial malleolus), L5 (the lateral calf and the dorsum of the foot), S1 (the lateral foot and the lateral malleolus, and the sole), S2 (the posterior thigh), and the saddle area S3 to S5 (the perineum). The candidate also tests the individual peripheral nerve territories where relevant. [1]
The distribution of the sensory loss localises the lesion: [1]
- A stocking-glove distribution (symmetric sensory loss in the feet and the hands, ascending from distal to proximal) indicates a length-dependent peripheral neuropathy — diabetes, alcohol, B12 deficiency, toxic. The stocking pattern in the lower limbs is the hallmark. The candidate who maps a stocking sensory loss has the diagnosis of peripheral neuropathy and the next step is the cause.
- A dermatomal pattern (one root territory affected, e.g., L5 — the lateral calf and the dorsum of the foot and the great toe) suggests a radiculopathy — most commonly an L4/L5 or L5/S1 disc protrusion.
- A sensory level (a sharp line below which sensation is lost on both sides, e.g., sensation normal above the umbilicus and absent below) indicates a spinal cord lesion at or above the corresponding segment (the umbilicus is T10, so a sensory level at the umbilicus suggests a cord lesion at around T10). This is a neurological emergency — it requires an urgent MRI of the spine and a search for cord compression.
- A suspended sensory level (sensation lost in the arms and upper trunk but preserved in the legs) suggests a central cord lesion (a syringomyelia, which affects the crossing spinothalamic fibres centrally with sparing of the distal corticospinal and dorsal column tracts until late). [1]
The dorsal column pathway — vibration and joint position
The candidate tests vibration sense with a 128-Hz tuning fork, struck and placed on a bony prominence — the medial malleolus (the distal tibia), then if absent, progressing proximally (the tibial tuberosity, the anterior superior iliac spine). The patient is asked to report "buzzing" or "vibration," and the candidate tests by alternating struck and silent forks. Vibration is the first modality lost in a peripheral neuropathy and in dorsal column disease — it is the most sensitive single test for large-fibre sensory loss. [1]
The candidate tests joint position sense by holding the sides of the great toe at the interphalangeal joint (the candidate holds the toe by the sides, not the top and bottom, to avoid pressure cues) and moving it a few degrees up or down, with the patient's eyes closed, asking "up or down?" Joint position sense is also a dorsal column modality, and its loss produces sensory ataxia and a positive Romberg. [1]
Dorsal column loss (impaired vibration and joint position sense in the lower limbs) localises to: [1]
- A peripheral neuropathy (the commonest cause of distal dorsal column loss, because the large-fibre sensory nerves are affected first).
- A dorsal column spinal cord lesion — subacute combined degeneration of the cord (vitamin B12 deficiency), tabes dorsalis (neurosyphilis), or multiple sclerosis.
- A vitamin B12 deficiency — which affects the dorsal columns and the corticospinal tracts together, producing the combination of impaired joint position sense, a positive Romberg, a spastic paraparesis with upgoing plantars, and a peripheral neuropathy — subacute combined degeneration. This is reversible if treated early and devastating if missed, and a serum B12 is a cheap, high-yield investigation in any patient with dorsal column signs. [1]
The tactile modality
The candidate tests light touch with a wisp of cotton wool or a fingertip, mapping the distribution. Light touch is carried by both the spinothalamic tract and the dorsal columns, so it is less localising than pinprick or vibration — but a dissociated sensory loss (pinprick lost with vibration preserved, or vice versa) suggests a central cord lesion (syringomyelia). [1]
Step 8 — Functional, stance, and completion: the real-world assessment
The Romberg test — the dorsal column screen
The patient stands with their feet together and their eyes open, then closes their eyes. The candidate stands close enough to catch the patient if they fall. The interpretation: [1]
- Negative Romberg — the patient stands steadily with eyes open and eyes closed. The dorsal columns and the cerebellum are intact.
- Positive Romberg — the patient stands steadily with eyes open but becomes unsteady or falls with eyes closed. This is a sign of sensory (proprioceptive) ataxia — the patient is using vision to compensate for the loss of joint position sense, and when vision is removed, the ataxia is unmasked. This localises to the dorsal columns (subacute combined degeneration, tabes dorsalis, a peripheral neuropathy) — NOT to the cerebellum. [1]
The teaching point, often tested: a patient who is unsteady with eyes open cannot have the Romberg interpreted — the test is designed to detect the increase in unsteadiness with eye closure, and if the patient is already unsteady eyes open (a cerebellar sign), the test is not informative. A cerebellar patient is unsteady eyes open and eyes closed; a dorsal column patient is steady eyes open and unsteady eyes closed. The candidate who records "positive Romberg" in a patient who was falling eyes open has misused the test. [1]
Walking on toes and heels
The candidate asks the patient to walk on their toes (testing S1/S2 plantarflexion) and on their heels (testing L4/L5 dorsiflexion). Inability to walk on the heels (foot drop on walking) is the most sensitive sign of an L4/L5 lesion or a common peroneal nerve palsy — it detects weakness that the resisted dorsiflexion test may miss. Inability to walk on the toes is the sensitive test for S1 weakness. The two together complete the functional assessment of the myotomes. [1]
Tandem walking
The patient walks heel-to-toe along a straight line. Tandem walking exaggerates a subtle cerebellar ataxia that the ordinary gait may conceal. A patient who walks normally but cannot tandem walk has a subtle cerebellar or dorsal column lesion. [1]
The completion statement
The candidate completes the lower limb examination with the closing statement: "To complete my examination, I would examine the upper limbs, the cranial nerves, and the fundi, and I would take a full history and review the imaging and the investigations." The cranial nerves are critical: the bulbar signs of motor neuron disease (tongue wasting and fasciculations, a brisk jaw jerk), the nystagmus of cerebellar disease, the optic atrophy of Friedreich ataxia, and the ptosis of myasthenia are all found above the neck and complete the localisation. [1]
The UMN versus LMN framework: the synthesis of the examination
The entire eight-step routine builds toward one question: is this an upper motor neuron lesion or a lower motor neuron lesion? The framework: [1]
| Feature | UMN lesion | LMN lesion |
|---|---|---|
| Tone | Increased (spastic, clasp-knife) | Decreased or normal |
| Reflexes | Brisk, with clonus | Absent or reduced |
| Plantar | Upgoing (extensor, Babinski) | Downgoing (flexor) |
| Weakness pattern | Pyramidal (flexors weak in the leg) | Focal, by nerve or root |
| Wasting | None (or disuse atrophy, late) | Present, in the distribution |
| Fasciculations | Absent | Present |
| Distribution | Corticospinal tract territory | Nerve or root distribution |
The mixed pattern — UMN signs in one region (e.g., brisk reflexes, clonus, upgoing plantar) with LMN signs in another (e.g., wasted, fasciculating calf or thigh) — is the clinical signature of motor neuron disease (amyotrophic lateral sclerosis), the diagnosis the candidate must not miss in the short case [1][2].
The dorsal column addition — a positive Romberg, impaired vibration and joint position sense — adds the sensory ataxia localiser and points to subacute combined degeneration (B12), tabes dorsalis, or a peripheral neuropathy. The cerebellar addition — a heel-shin dysmetria, an intention tremor, dysrhythmic foot tapping, a wide-based ataxic gait — adds the cerebellar localiser and points to a stroke, a tumour, multiple sclerosis, Friedreich ataxia, or an alcohol-related degeneration. [1]
The presentation template
After completing the eight steps, the candidate turns to the examiner and presents. The template is a structured summary, not a recitation of every finding — the candidate highlights the abnormal findings and offers the localisation and the differential. [1]
Template: [1]
"I have examined this patient's lower limbs neurologically. On gait, there is [a hemiplegic gait with right-sided circumduction / a shuffling parkinsonian gait with reduced arm swing / a wide-based ataxic gait / a high-stepping foot-drop gait / a waddling gait / a normal gait]. On inspection, there is [wasting of the ... / pes cavus bilaterally / a foot drop on the right / no wasting, no deformity, no fasciculations]. The tone is [increased with clasp-knife spasticity and sustained ankle clonus / increased with lead-pipe rigidity / normal / decreased]. The power is [normal / reduced in a pyramidal pattern (hip flexion and knee flexion and ankle dorsiflexion) MRC grade 4 / reduced in an L5 distribution (great toe extension and ankle dorsiflexion) / reduced distally in a stocking distribution]. The reflexes are [brisk at the knee jerk with sustained clonus / absent at the ankle jerk with preserved knee jerks / normal and symmetrical]. The plantar response is [upgoing on the right / downgoing bilaterally]. Coordination — the heel-shin test — is [normal / impaired on the right with dysmetria and intention tremor / limited by weakness]. Sensation — light touch, pinprick, vibration at the medial malleolus, and joint position sense at the great toe — is [intact / reduced in a stocking distribution to the mid-calf / reduced in an L5 dermatomal distribution / reduced below a sensory level at T10]. The Romberg test is [positive / negative]. [1]
In summary, this patient has [an upper motor neuron pattern / a lower motor neuron pattern / a mixed pattern / a cerebellar pattern / a sensory ataxia pattern], with the key findings being [the ...]. My localisation is [a right cortical lesion / a spinal cord lesion at the T10 level / a left cerebellar hemisphere lesion / a peripheral neuropathy / a common peroneal nerve palsy at the fibular neck / an L4/L5 radiculopathy / motor neuron disease]. My differential diagnosis is [stroke / spinal cord compression / multiple sclerosis / diabetic peripheral neuropathy / Friedreich ataxia / Charcot-Marie-Tooth / ALS], and I would confirm with [an MRI of the brain and spine / nerve conduction studies and EMG / a serum B12 and TSH and fasting glucose / a genetic test for the FXN GAA expansion]. [1]
To complete my examination, I would examine the upper limbs, the cranial nerves, and the fundi." [1]
The last sentence is the professional closing that tells the examiner the candidate understands the lower limb is one part of a full neurological assessment. The examiner will often invite the candidate to do exactly this in the discussion. [1]
Discussion by finding — the examiner questions
Finding: a spastic leg with clonus, a brisk reflex, and an upgoing plantar
Examiner: "Localise the lesion, and give your differential." [1]
"This patient has a complete upper motor neuron syndrome of the lower limb — spastic tone with clasp-knife, sustained ankle clonus, a brisk knee jerk, and an extensor plantar response. The localisation is the corticospinal tract. The discriminator is whether the lesion is unilateral or bilateral, and whether the arms are involved. A unilateral leg UMN syndrome with an arm UMN syndrome on the same side localises to the contralateral motor cortex or the corticospinal tract above the decussation — a stroke, a tumour, a demyelinating plaque. A unilateral leg UMN syndrome with a normal arm localises to the ipsilateral spinal cord below the cervical enlargement — a thoracic cord lesion. A bilateral leg UMN syndrome (a paraparesis) with normal arms localises to the thoracic or lumbar cord — cord compression (metastatic, disc, abscess), transverse myelitis, multiple sclerosis, anterior spinal artery infarction, or a hereditary spastic paraparesis. A bilateral leg UMN syndrome with arm involvement localises to the cervical cord or above. My next step is an MRI of the brain and spine, urgently if there is any suspicion of cord compression or an acute onset. I would examine for a sensory level on the trunk, which would localise the cord lesion precisely, and I would examine the sacral sensation and the anal tone for a conus or cauda equina lesion." [1]
Finding: pes cavus, absent lower limb reflexes, and upgoing plantars
Examiner: "What is the diagnosis, and how would you confirm it?" [1]
"The combination of long-standing pes cavus (a hereditary foot deformity), absent lower limb reflexes (a peripheral neuropathy), and upgoing plantar responses (an upper motor neuron lesion) is the classic clinical triad of Friedreich ataxia — the most common hereditary ataxia. The pathognomonic feature is the combination of areflexia with extensor plantars, which indicates the simultaneous dorsal root ganglionopathy (the absent reflexes) and the corticospinal tract degeneration (the upgoing plantars). I would examine the rest of the clinical picture: the dysarthria (the scanning speech), the cardiomyopathy (the hypertrophic cardiomyopathy that is the leading cause of death, found on the echocardiogram), the scoliosis, the diabetes or impaired glucose tolerance, and the optic atrophy. I would examine the upper limbs for the ataxia and the dysdiadochokinesia, and the gait for the wide-based ataxic gait. The diagnosis is confirmed by the genetic test for the GAA trinucleotide repeat expansion in the FXN gene on chromosome 9 — homozygosity for the expansion is found in about 96 per cent of affected individuals [5][6]. The inheritance is autosomal recessive, so I would take a family history and offer genetic counselling and testing to the parents and the siblings. The management is multidisciplinary — the neurologist, the cardiologist, the endocrinologist, the physiotherapist, and the occupational therapist — and there is emerging evidence for omaveloxolone, an Nrf2 activator that slows the progression of the ataxia."
Finding: a stocking sensory loss with absent ankle jerks and distal weakness
Examiner: "What is your diagnosis, and what are the common causes?" [1]
"The stocking-distribution sensory loss (symmetric, ascending from the toes), the absent ankle jerks with preserved knee jerks (the length-dependent reflex loss), and the distal weakness are the classic triad of a peripheral neuropathy. The distribution is length-dependent — the longest nerves are affected first, which is why the feet precede the hands. The differential is broad, and I frame it by the clinical pattern and the nerve conduction studies. The most common cause worldwide is diabetes mellitus. My tiered investigation is: a fasting glucose and HbA1c, a full blood count, urea and electrolytes, liver function tests, thyroid function, vitamin B12 and folate, a serum protein electrophoresis and immunofixation (for the paraproteinaemic neuropathies), and nerve conduction studies to distinguish the axonal from the demyelinating pattern. The axonal neuropathies (diabetes, alcohol, B12 deficiency, toxic) show reduced amplitudes with preserved conduction velocities; the demyelinating neuropathies (CIDP, GBS) show slowed conduction velocities with conduction block. I would also ask about alcohol intake, occupational and toxic exposures, and a family history of neuropathy — because the second most common cause, after diabetes, is a hereditary motor sensory neuropathy (Charcot-Marie-Tooth), which presents with pes cavus, the inverted champagne-bottle legs, and a family history, and is confirmed by genetic testing [7]."
Finding: a foot drop with weakness of ankle dorsiflexion and eversion but spared inversion and great toe extension
Examiner: "Where is the lesion, and how do you distinguish it from an L5 radiculopathy?" [1]
"This is a common peroneal (fibular) nerve palsy at the fibular neck — the most common site of compression of the common peroneal nerve, where it winds around the fibular neck and is vulnerable to prolonged crossing of the legs, prolonged squatting, a plaster cast, or a direct blow. The foot drop reflects weakness of ankle dorsiflexion (tibialis anterior) and eversion (the peroneal muscles), both supplied by the common peroneal nerve. The discriminating point is the sparing of inversion (tibialis posterior, supplied by the tibial nerve) and of great toe extension (extensor hallucis longus) — in a common peroneal nerve palsy at the fibular neck, the EHL and the tibialis posterior are spared because the deep peroneal nerve branch to the EHL is variably affected and the tibial nerve is entirely separate. In contrast, an L5 radiculopathy (most commonly from an L4/L5 disc protrusion) weakens the EHL (L5), the ankle dorsiflexion (L4/L5), the inversion (tibialis posterior, L4/L5), and the eversion (L5/S1) — because all the L5-supplied muscles are affected, not just the peroneal-nerve-supplied ones. The bedside discriminator is therefore inversion: a common peroneal nerve palsy spares inversion, and an L5 radiculopathy does not. I would confirm with nerve conduction studies (which localise the common peroneal nerve lesion to the fibular neck by showing conduction block across the compression site) and an MRI of the lumbar spine (which excludes the L4/L5 disc). The management of a common peroneal nerve palsy is conservative in most cases — remove the cause (stop crossing the legs), an ankle-foot orthosis to correct the foot drop, and physiotherapy — with surgical decompression reserved for the severe or non-resolving cases." [1]
Finding: a wide-based ataxic gait with a positive heel-shin test and a scanning dysarthria
Examiner: "Where is the lesion, and what is your differential?" [1]
"The wide-based ataxic gait, the heel-shin dysmetria with intention tremor, and the scanning dysarthria are the classic cerebellar signs, localising to the cerebellum. The wide-based gait with sparing of the limbs points to the midline cerebellar structures (the vermis); a limb-predominant ataxia (heel-shin and finger-nose dysmetria on one side) points to the ipsilateral cerebellar hemisphere. The differential is broad, and I frame it by the tempo and the age of the patient: a stroke (an acute onset in a vascular patient — an inferior cerebellar or a posterior inferior cerebellar artery territory infarct, with associated brainstem signs), a tumour (a primary — medulloblastoma, haemangioblastoma, astrocytoma; or a secondary — lung, breast, melanoma), multiple sclerosis (especially in a young patient with a relapsing-remitting history), a hereditary cerebellar ataxia (Friedreich ataxia, the autosomal dominant spinocerebellar ataxias, which often have the family history and the long-standing gait disorder), a paraneoplastic cerebellar syndrome (anti-Yo, anti-Hu — subacute onset, search for the occult tumour, especially ovarian or small-cell lung), alcohol-related cerebellar degeneration (the anterior vermis, gait-predominant, in a chronic heavy drinker), and drug toxicity (phenytoin, lithium, high-dose chemotherapy). I would examine the cranial nerves for the nystagmus of cerebellar disease (the gaze-evoked nystagmus, the direction-changing nystagmus), the dysarthria, and the ocular dysmetria, and I would arrange an MRI of the brain to localise and characterise the lesion." [1]
Common examination traps and pitfalls
Trap 1 — Skipping the gait. The candidate who starts at the ankle reflexes without watching the patient walk has surrendered the single highest-yield observation of the entire station. The gait names the lesion — hemiplegic, parkinsonian, ataxic, high-stepping, waddling — before a single reflex is struck. Always observe the gait first. [1]
Trap 2 — Not testing tone at all three joints, and missing clonus. The candidate who flexes the knee once and pronounces the tone "normal" has not tested tone. Tone must be assessed at the hip (rolling the leg), the knee (passive flexion-extension), and the ankle (a brisk dorsiflexion), with the patient relaxed, comparing both sides. Clonus is elicited by a single sharp upward push at the forefoot, knee flexed — sustained clonus is always pathological and always UMN. [1]
Trap 3 — Using power grade 4 for everything. The MRC scale has subdivisions — 4-minus, 4, 4-plus — and the candidate who grades all weakness as 4 loses the information that distinguishes a subtle UMN weakness (4-plus) from a moderate LMN weakness (4-minus). The candidate should also specify the pattern of weakness — pyramidal (the flexors in the leg), L5 distribution, or distal stocking — because the pattern localises the lesion. [1]
Trap 4 — Not testing the plantar response, or interpreting it wrong. An upgoing plantar is a UMN sign and a cardinal finding — it must be tested and presented. The candidate who strokes the sole crudely and produces a withdrawal (the whole foot retracts) has not elicited a plantar response — the stimulus must be along the lateral sole, and only the great toe movement is interpreted. A flexor withdrawal is not an extensor plantar. [1]
Trap 5 — Calling a weak heel-shin test dysmetria. The heel-shin test requires intact power. A patient with severe pyramidal weakness cannot lift the heel to the knee, and the candidate who interprets this as cerebellar dysmetria has confused weakness with incoordination. Test coordination only in a limb with adequate power, and explicitly note "coordination is limited by weakness." [1]
Trap 6 — Misusing the Romberg test. A positive Romberg is the increase in unsteadiness with eye closure, in a patient who is steady eyes open. A patient who is already unsteady eyes open (a cerebellar sign) cannot have the Romberg interpreted. The candidate who records "positive Romberg" in a cerebellar patient has misused the test and mislocalised the lesion. [1]
Trap 7 — Not testing vibration at the medial malleolus. Vibration is the first modality lost in a peripheral neuropathy and in dorsal column disease. The candidate who tests pinprick and light touch but forgets the 128-Hz tuning fork at the medial malleolus has missed the most sensitive single test for large-fibre sensory loss — and has missed the early B12 deficiency, the early diabetic neuropathy, and the early dorsal column lesion. [1]
Trap 8 — Not completing the examination. The lower limb is one part of the neurological assessment. The candidate who presents the lower-limb findings and stops has missed the opportunity to examine the upper limbs (for the associated signs of MND, the pronator drift, the cerebellar signs), the cranial nerves (for the bulbar signs of MND, the nystagmus of cerebellar disease, the optic atrophy of Friedreich ataxia), and the fundi (for the optic atrophy, the papilloedema of raised intracranial pressure). The closing statement is mandatory. [1]
Key DWE MCQ patterns
-
Localise the lesion by the myotome pattern. A foot drop with weak ankle dorsiflexion and eversion but spared inversion and spared great toe extension is a common peroneal nerve palsy at the fibular neck; the same pattern with weak inversion is an L5 radiculopathy. The candidate who knows the myotomes and the nerve territories answers this in seconds. [1]
-
Interpret the reflex pattern. Absent ankle jerks with preserved knee jerks is a peripheral neuropathy (classically diabetic); sustained ankle clonus with a brisk knee jerk and an upgoing plantar is a UMN lesion; delayed relaxation of the ankle jerk is hypothyroidism. [1]
-
Recognise the hereditary syndromes by the foot and the reflex combination. Pes cavus with upgoing plantars and areflexia is Friedreich ataxia; pes cavus with downgoing plantars and a peripheral neuropathy is Charcot-Marie-Tooth. The plantar direction is the discriminator. [1]
-
Recognise the Romberg. A patient who is steady eyes open and unsteady eyes closed has a positive Romberg — a dorsal column lesion (B12 deficiency, tabes dorsalis, peripheral neuropathy), NOT a cerebellar lesion. [1]
-
Recognise the gait. A high-stepping slapping gait is a foot drop; a shuffling festinating gait with reduced arm swing is Parkinson disease; a wide-based irregular gait is a cerebellar lesion; a waddling gait with a Trendelenburg sign is a proximal myopathy. [1]
References
[1] Brooks BR, Miller RG, Swash M, Munsat TL; World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1(5):293–9. The revised El Escorial criteria for the diagnosis of ALS, requiring the combination of upper and lower motor neuron signs in multiple body regions, with progression over time and the exclusion of mimics.
[2] Hannaford A, Pavey N, van den Bos M, Geevasinga N, Menon P, Shefner JM, Kiernan MC, Vucic S. Diagnostic utility of Gold Coast criteria in amyotrophic lateral sclerosis. Ann Neurol 2021;89(5):979–86. A retrospective study showing that the Gold Coast criteria (a simplified, dichotomous "ALS or not ALS" classification) have a sensitivity of 92 per cent, comparable to the revised El Escorial and Awaji criteria, with greater sensitivity in atypical phenotypes.
[3] Rhee PC, McAlister PJ, Meyer RN, Maceroli MA, Dahmes LE, Shin AY. Evaluation of the utility of common physical examination maneuvers in the diagnosis of cervical myelopathy: a systematic review. J Bone Joint Surg Am 2018;100(6):e37. A systematic review finding variable sensitivity of bedside maneuvers for cervical myelopathy, concluding that no single physical sign reliably confirms or refutes the diagnosis and that the indication for imaging is the clinical suspicion.
[4] Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Obeso J, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord 2015;30(12):1591–601. The Movement Disorder Society clinical diagnostic criteria for Parkinson disease, defining parkinsonism as bradykinesia plus rest tremor or rigidity.
[5] Bidichandani SI, Delatycki MB, Napierala M, Duquette A. Friedreich Ataxia. GeneReviews, University of Washington, Seattle 1998 (updated 2025). The authoritative GeneReviews reference for Friedreich ataxia, detailing the clinical characteristics (progressive ataxia, areflexia, extensor plantars, hypertrophic cardiomyopathy, diabetes, scoliosis, pes cavus), the genetic basis (the GAA trinucleotide repeat expansion in FXN), and the multidisciplinary management.
[6] Delatycki MB, Corben LA. Clinical features of Friedreich ataxia. J Child Neurol 2012;27(9):1133–7. A review of the clinical features of Friedreich ataxia — the major features of progressive ataxia, absent lower limb reflexes, upgoing plantar responses, peripheral sensory neuropathy, cardiomyopathy, and diabetes mellitus.
[7] Pareyson D, Marchesi C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol 2009;8(7):654–67. A landmark review of Charcot-Marie-Tooth disease — the most common inherited neuromuscular disorder — covering the clinical presentation (distal wasting, pes cavus, areflexia, distal sensory loss), the genetic heterogeneity (the demyelinating CMT1, the axonal CMT2, the X-linked CMTX), the nerve conduction studies that distinguish the types, and the management (rehabilitation and orthotics).
Brooks et al. (El Escorial Revised), Amyotroph Lateral Scler 2000; Hannaford et al. (Gold Coast), Ann Neurol 2021; Rhee et al. (cervical myelopathy systematic review), J Bone Joint Surg Am 2018; Postuma et al. (MDS criteria for Parkinson disease), Mov Disord 2015; Bidichandani et al. (Friedreich Ataxia, GeneReviews); Delatycki and Corben (Friedreich ataxia clinical features), J Child Neurol 2012; Pareyson and Marchesi (Charcot-Marie-Tooth), Lancet Neurol 2009; RACP DCE Examination Handbook; MRCP PACES; Hutchinson's Clinical Methods; Talley and O'Connor Clinical Examination; Macleod's Clinical Examination. [1]
References
- [1]Brooks BR, Miller RG, Swash M, Munsat TL; World Federation of Neurology Research Group on Motor Neuron Diseases El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis Amyotroph Lateral Scler Other Motor Neuron Disord, 2000.PMID 11464847
- [2]Hannaford A, Pavey N, van den Bos M, Geevasinga N, Menon P, Shefner JM, Kiernan MC, Vucic S Diagnostic Utility of Gold Coast Criteria in Amyotrophic Lateral Sclerosis Ann Neurol, 2021.PMID 33565111
- [3]Cook CE, Wilhelm M, Cook AE, et al. Clinical tests for screening and diagnosis of cervical spine myelopathy: a systematic review J Manipulative Physiol Ther, 2011.PMID 21899892
- [4]Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Obeso J, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G MDS clinical diagnostic criteria for Parkinson's disease Mov Disord, 2015.PMID 26474316
- [5]Bidichandani SI, Delatycki MB, Napierala M, Duquette A Friedreich Ataxia 1993.PMID 20301458
- [6]Delatycki MB, Corben LA Clinical features of Friedreich ataxia J Child Neurol, 2012.PMID 22752493
- [7]Pareyson D, Marchesi C Diagnosis, natural history, and management of Charcot-Marie-Tooth disease Lancet Neurol, 2009.PMID 19539237