Phys · general-medicine
Neurological Examination — Speech and Higher Mental Function
Also known as speech examination · higher mental function · higher cortical function · cognitive assessment · aphasia examination · dysphasia · dysarthria · dysphonia · Broca aphasia · Wernicke aphasia · conduction aphasia · global aphasia · MMSE · MoCA · ACE-III · clock drawing test · mini-mental state examination · Montreal Cognitive Assessment
Classic DCE short-case routine for speech and higher mental function: the systematic six-step speech sequence, the aphasia classification (fluency, comprehension, repetition), dysarthria and dysphonia, the cognitive domains and their bedside tests (orientation, attention, memory, language, visuospatial, executive), the MMSE, MoCA and ACE-III, a say-aloud presentation template, examiner discussion and the pitfalls that fail candidates — for FRACP DCE, MRCP PACES and ABIM preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Neurological Examination — Speech and Higher Mental Function

The answer first
The instruction "Please examine this patient's speech and higher mental function" is a classic DCE short case, and it is the station where a structured routine matters more than any single sign. The examiners are not testing whether you can recite the cranial nerves again — they are testing whether you can distinguish an aphasia (a language disorder) from a dysarthria (a motor speech disorder), classify the aphasia from three bedside axes — fluency, comprehension and repetition — and then assess the major cognitive domains in a sequence that looks competent from the foot of the bed. The candidate who says "I will first examine the speech, then the higher mental functions" and runs both halves in order passes; the candidate who launches into a disjointed battery of tests fails. [1]
The four ideas that govern this station: [1]
- Speech before cognition. Examine speech first — it is impossible to test comprehension or memory through a language the patient cannot use, and a severe aphasia will invalidate every cognitive score you record.
- Classify aphasia on three axes. Fluency, comprehension and repetition separate Broca, Wernicke, conduction, global and the transcortical aphasias. Never classify on one axis alone.
- Aphasia versus dysarthria is the first fork. Aphasia is a disorder of language (content and structure); dysarthria is a disorder of articulation (the mechanical production of sound). A dysarthric patient understands, formulates and writes normally; an aphasic patient does not.
- Map every cognitive test to a domain. Orientation, attention, memory, language, visuospatial and executive function — name the domain before you run the test, so the presentation reads as a system, not a list. [1]
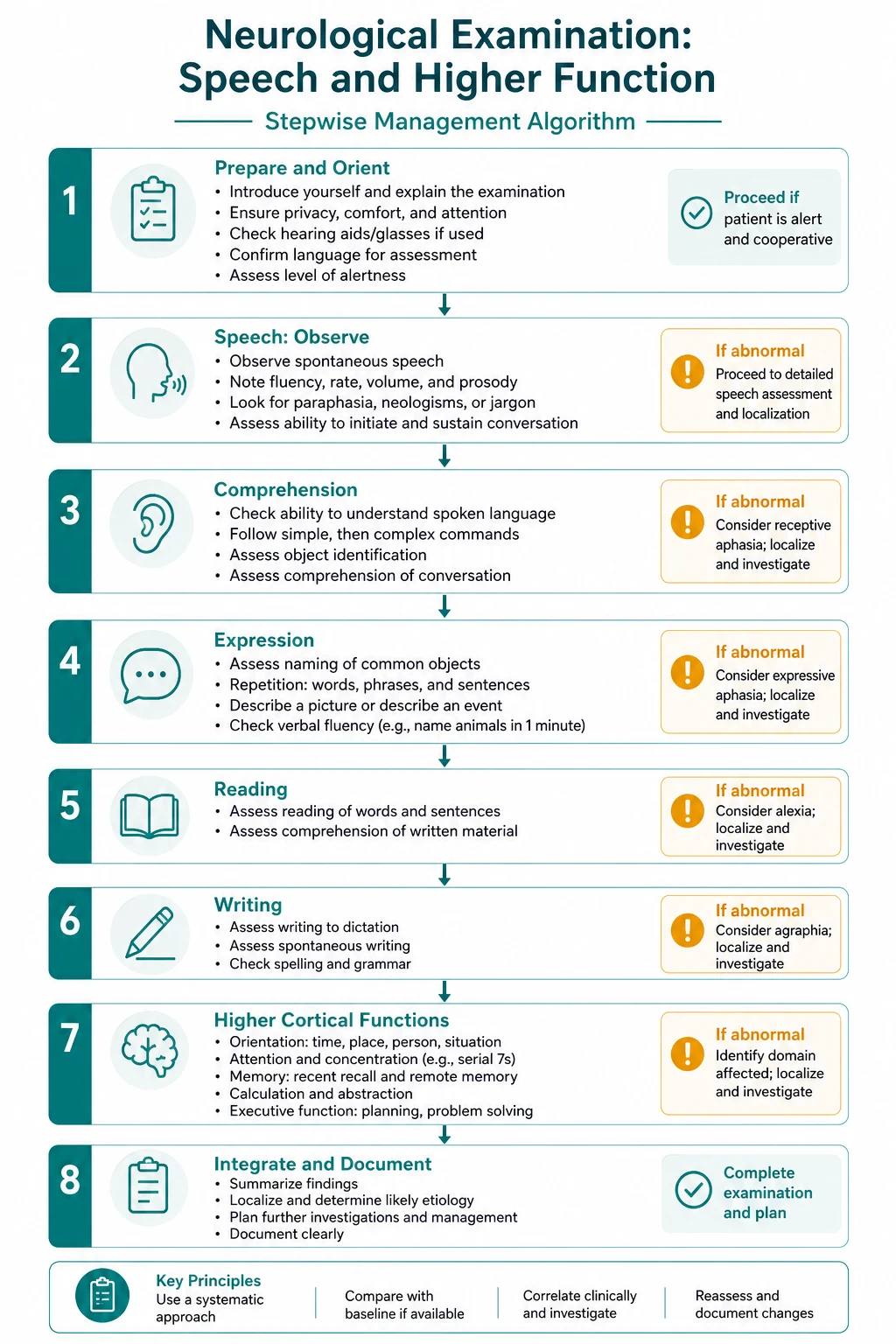
The organising principle is examine speech in a six-step sequence, classify any aphasia on fluency, comprehension and repetition, then assess the cognitive domains in a fixed order, and present a problem list with a localising and aetiological formulation. [1]
Setting up the examination
Before you touch the patient, set the stage. Stand at the foot of the bed. State your plan aloud: "I will first examine this patient's speech, then their higher mental functions. I will begin by introducing myself, confirming consent, and positioning the patient comfortably." Seat the patient upright at your eye level, ensure their hearing aids are in and working, and check they have their glasses — a patient who cannot hear or see will fail every test and confound your assessment. Exclude pain, fever, hypoxia or sedation first: a patient in distress or with an acute confusional state cannot be validly assessed for chronic cognitive function. Note the ambient environment — a noisy ward inflates inattention. [1]
Observe from the end of the bed before you speak. The things that betray a speech or cognitive disorder at a glance are a hemiparesis with a flaccid face (a stroke and its aphasia), a patient sitting silently and motionless (abulia or severe depression), a restless, picking, mumbled patient (delirium or Wernicke aphasia), and a tremulous, hypomimic, flexed patient (Parkinson disease and its hypophonic dysarthria). Spend thirty seconds here — it frames everything. [1]
Part A — The speech examination

The speech examination runs in a fixed six-step sequence. The first and most important decision is whether the patient has an aphasia (a disorder of language — the selection and ordering of words) or a dysarthria (a disorder of articulation — the mechanical production of clear sound) or a dysphonia (a disorder of voice — the phonation itself). You resolve this by listening, then testing the language system. [1]
Step 1 — Listen to spontaneous speech
Start with open conversation. Ask the patient to describe what brought them to hospital, or to recount the news of the day. Listen for two things: is the speech fluent, and is it informative? [1]
Fluent speech flows effortlessly — normal phrase length, normal melody, normal rate, words strung together smoothly. Non-fluent speech is effortful, halting and sparse — short phrases, long pauses, and visible struggle to get words out. The patient may look frustrated. Then ask whether the content is meaningful: does the patient actually convey information, or do they speak in a torrent of sound that carries no sense? A fluent speaker whose words are meaningless has a posterior (Wernicke) aphasia; a non-fluent speaker whose few words are correct has an anterior (Broca) aphasia. [1]
Listen specifically for paraphasias — errors of word or sound. A phonemic (literal) paraphasia substitutes a sound ("spoot" for "spoon"); a verbal (semantic) paraphasia substitutes a related word ("fork" for "spoon"). A neologism is a newly invented non-word that follows phonological rules but means nothing. Copious fluent speech laced with paraphasias and neologisms, spoken without insight, is the hallmark of Wernicke aphasia — and patients are often unaware they are not making sense, a state called anosognosia for the language deficit. [1]
Step 2 — Assess fluency (formally)
If spontaneous speech has not settled the question, elicit a longer sample. Ask the patient to describe a picture or to tell you about their family. Decide fluency on these features: phrase length (short versus full sentences), effort (high versus low), articulatory agility (impaired versus preserved), melodic line (flat versus normal), and content (empty versus informative). The bedside judgement is binary — fluent or non-fluent — and it is the first axis of the aphasia classification. [1]
A small but critical point: do not confuse dysarthria with non-fluency. A dysarthric patient has intact language but mechanically garbled articulation. The discriminating test is that a dysarthric patient can write a perfectly formed sentence even if they cannot speak it — their language is intact. Always carry a pen and paper and, when fluency is in doubt, ask the patient to write a sentence. This single act separates aphasia (writing impaired) from dysarthria (writing preserved). [1]
Step 3 — Comprehension
Comprehension is the second axis of aphasia classification, and it is the one most poorly tested at the bedside. Test it in a graded hierarchy. [1]
Yes or no questions. Start with simple, concrete questions whose answer is obvious from the context: "Is it raining outside?", "Are we in a hospital?", "Are you sitting down?" The patient answers yes or no. Then progress to questions requiring stored knowledge: "Does a stone sink in water?", "Do dogs have four legs?" Avoid questions the patient can answer from social cueing alone — nodding at them as you ask "Do you want to go home?" invites agreement. [1]
One-step commands. Ask the patient to perform a single action: "Close your eyes", "Point to the ceiling", "Touch your nose." If they succeed, the basic comprehension pathway is intact. [1]
Two-step commands. Escalate: "Point to the door, then the window", "Pick up the pen, then hand it to me." A patient who manages one step but not two has impaired comprehension — and the failure localises to the posterior language area (Wernicke). [1]
Pointing to objects on command ("Point to the one you tell time with") tests comprehension without requiring the patient to name, which separates a comprehension deficit from a naming (anomic) deficit. A patient with pure anomia comprehends perfectly but cannot name; a patient with Wernicke aphasia fails both. [1]
The pitfall: a patient who is deaf, sedated, depressed, or simply not paying attention will appear to have impaired comprehension. Always confirm hearing and attention before declaring a comprehension deficit. If in doubt, test with written commands — hand the patient a card reading "Close your eyes" — which bypasses the auditory pathway. [1]
Step 4 — Repetition
Repetition is the third and most discriminating axis, because it tests the integrity of the arcuate fasciculus — the white-matter bundle that carries the auditory word from Wernicke area to Broca area for re-articulation. Ask the patient to repeat after you, using a sentence of graded complexity: a single word, a short phrase, then a high-load sentence. [1]
The standard test sentence is "No ifs, ands, or buts." It is chosen because it is loaded with small, grammatical function words that patients with conduction aphasia and the transcortical aphasias handle differently. Have the patient repeat "hospital", then "It is a sunny day today", then "No ifs, ands, or buts." [1]
The decisive finding: a patient who speaks fluently, comprehends well, but cannot repeat has a conduction aphasia — a lesion of the arcuate fasciculus, classically from a left superior temporal or supramarginal gyrus infarct. Repetition is worse than spontaneous speech, which is the paradox that defines the syndrome. By contrast, a patient who can repeat everything — even long sentences — but cannot generate spontaneous speech or comprehend it has a transcortical aphasia, because the perisylvian language area is preserved as an isolated circuit that can echo but not create or decode. Preserved repetition is the signature of a watershed-territory lesion. [1]
Step 5 — Naming
Naming is tested because anomia — the inability to retrieve a word — is present in every aphasia, so it does not by itself classify the type. But the pattern of naming failure adds localising colour. Show the patient common objects and ask "What is this?" Use a watch, a pen and a key. Then ask for components: the watch face, the hand, the winder (the stem). Ask for colours, and ask the patient to name their fingers (index, ring, thumb). Ask the patient to name what you do with the object if they fail the noun — this tests whether the semantic network is intact and only the phonological retrieval is impaired (anomia) versus a deeper loss of meaning. [1]
A patient who can describe the function but not name the object ("it's the thing you tell time with") has a pure anomia or a transcortical sensory component; a patient who cannot even gesture its use has a deeper semantic breakdown. Anomia with preserved fluency and comprehension is the hallmark of anomic aphasia, which is common in recovery and in neurodegenerative disease, and is also the presenting feature of primary progressive aphasia when it progresses insidiously. [1]
Step 6 — Reading and writing
Reading and writing close the language examination because they localise within the dominant hemisphere. Ask the patient to read a short sentence aloud and to follow a written command ("Close your eyes" written on a card). Then ask them to write a spontaneous sentence. [1]
The classical teaching is the alexia with agraphia syndrome — the patient can neither read nor write — which follows a dominant-hemisphere inferior parietal (angular gyrus) lesion. Alexia without agraphia, by contrast, is the disconnection syndrome of a left posterior cerebral artery infarct: the patient cannot read (the visual input from the intact right hemisphere cannot reach the left language area because the left occipital lobe is infarcted and the splenium is damaged), but they can write spontaneously because the language output area is intact. The curiosity is that the patient can write a sentence and then, moments later, cannot read back what they have just written. Writing also distinguishes aphasia from dysarthria definitively: the dysarthric patient writes normally; the aphasic patient does not. [1]
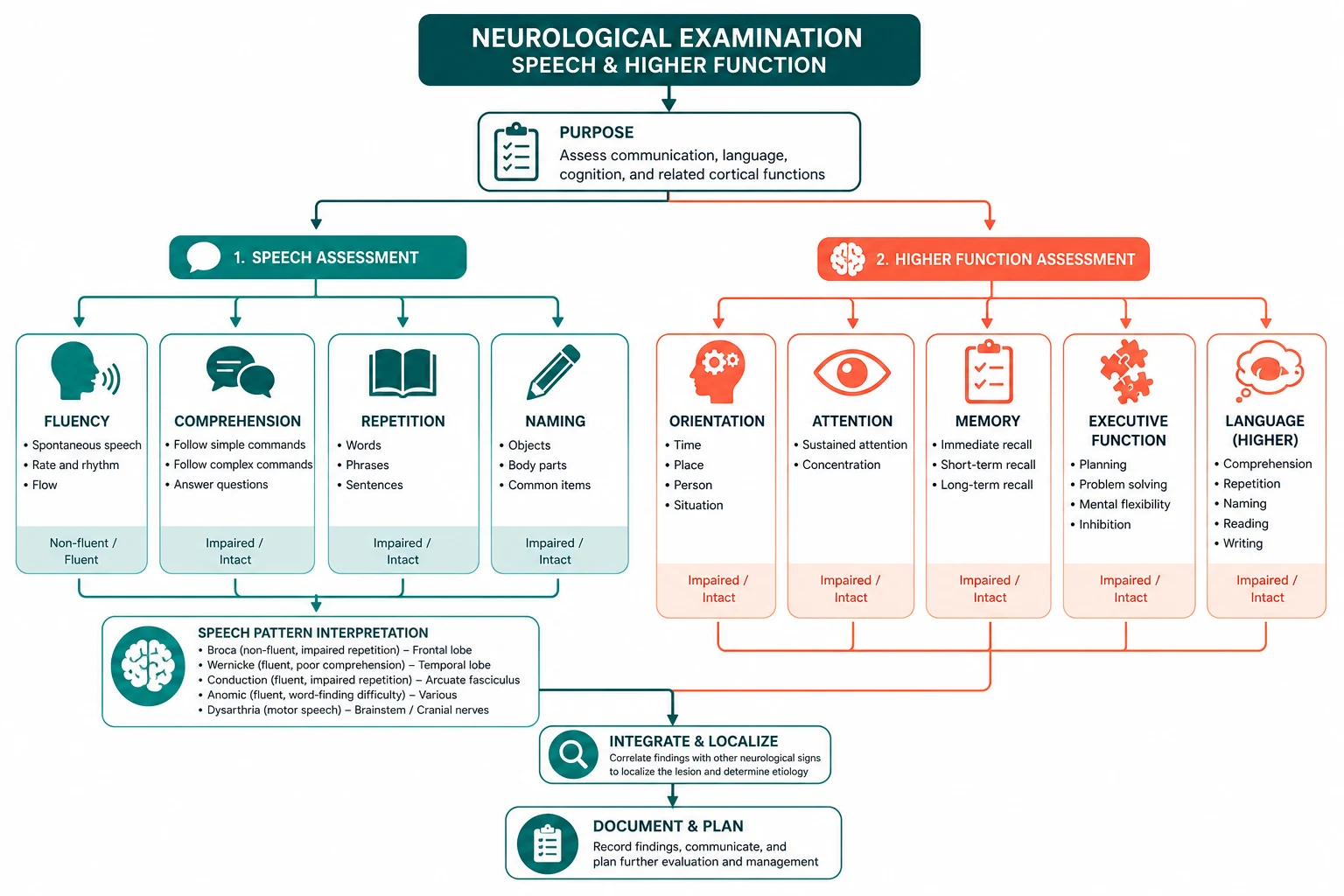
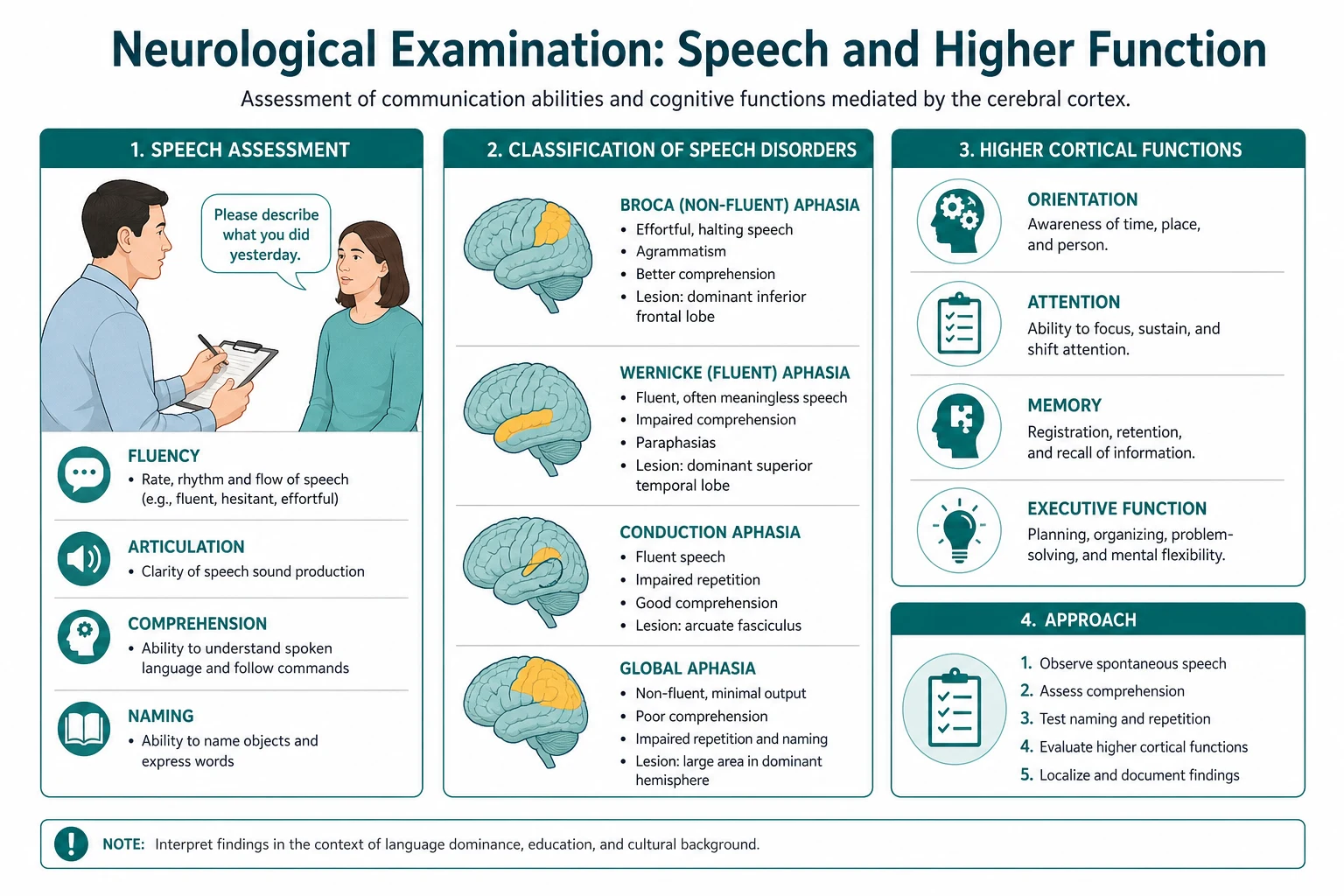
Aphasia classification — the three-axis system

Once you have the three axes — fluency, comprehension and repetition — you classify the aphasia. The classification is not an academic exercise; it localises the lesion within the dominant (usually left) hemisphere and frames the differential (stroke, tumour, degeneration) and the prognosis. [1]
| Aphasia type | Fluency | Comprehension | Repetition | Lesion |
|---|---|---|---|---|
| Broca (expressive) | Non-fluent, effortful, telegraphic | Preserved | Impaired | Inferior frontal gyrus (Broca area), MCA superior division |
| Wernicke (receptive) | Fluent, empty, paraphasic | Impaired | Impaired | Superior temporal gyrus (Wernicke area), MCA inferior division |
| Conduction | Fluent | Preserved | Severely impaired | Arcuate fasciculus / supramarginal gyrus |
| Global | Non-fluent | Impaired | Impaired | Large dominant MCA territory |
| Transcortical motor | Non-fluent | Preserved | Preserved | Watershed, anterior to Broca |
| Transcortical sensory | Fluent | Impaired | Preserved | Watershed, posterior to Wernicke |
| Mixed transcortical | Non-fluent | Impaired | Preserved | Watershead, sparing perisylvian |
| Anomic | Fluent | Preserved | Preserved | Various, often temporo-parietal or thalamic |
The two rules that make the table usable under exam pressure: repetition is preserved only in the transcortical aphasias (watershed lesions that spare the perisylvian language loop), and both fluency and comprehension are impaired only in global aphasia (a large MCA territory infarct). Everything else sits on a spectrum: if fluent but comprehends, it is conduction or anomic; if fluent and does not comprehend, it is Wernicke; if non-fluent but comprehends, it is Broca. Practise this table until the classification is instant. [1]
A note on terminology: aphasia and dysphasia are used interchangeably in different regions — the RACP and most modern texts prefer aphasia for any acquired language disorder, while some UK sources retain dysphasia for a partial deficit and aphasia for a total one. At viva, state your convention and use aphasia consistently. [1]
Dysarthria — the motor speech disorder
Dysarthria is a disorder of articulation — the mechanical clarity of speech — caused by weakness, incoordination, rigidity or fatigability of the muscles of speech production. The language itself is intact: the patient understands, formulates and writes normally, but the spoken words are slurred, distorted or too quiet. The cause is a lesion anywhere along the motor pathway from cortex to muscle, and the character of the dysarthria localises the lesion. [1]
Listen for the pattern, then examine the relevant system: [1]
- Spastic (pseudobulbar) dysarthria — a strained, strangled, effortful voice with poor articulation, from bilateral upper motor neuron lesions of the corticobulbar tracts. The tongue is slow and spastic, the jaw jerk and gag are brisk, and there may be emotional lability. Causes include motor neuron disease, multiple sclerosis and bilateral hemisphere strokes.
- Flaccid (bulbar) dysarthria — a breathy, nasal, weak voice with visible muscle wasting and fasciculation, from lower motor neuron lesions of the brainstem nuclei or the cranial nerves. The tongue is wasted and fasciculating. Causes include motor neuron disease (bulbar onset), Guillain-Barre syndrome and brainstem stroke.
- Ataxic (cerebellar) dysarthria — a slow, scanning, drunk-sounding speech with irregular emphasis and broken-up words, from a cerebellar lesion. Test for cerebellar signs (nystagmus, dysmetria, gait ataxia). Causes include stroke, multiple sclerosis, alcohol-related cerebellar degeneration and inherited ataxias.
- Hypokinetic (extrapyramidal) dysarthria — a soft, rapid, monotonous, mumbled voice (hypophonia) with reduced facial expression, from Parkinson disease and other parkinsonian syndromes. The speech fades as the sentence progresses. The patient is hypomimic, rigid and tremulous.
- Hyperkinetic dysarthria — a voice interrupted by involuntary movements (chorea, dystonia, tics), seen in Huntington disease, tardive dyskinesia and dystonia.
- Myasthenic dysarthria — a voice and articulation that fatigue as the patient keeps speaking, then recover after rest, from myasthenia gravis. The speech may deteriorate markedly within a single long sentence. Always consider myasthenia when speech (or ptosis) worsens with use. [1]
The discriminating bedside test that separates dysarthria from aphasia is writing: the dysarthric patient writes a flawless sentence; the aphasic patient writes a garbled one. If you are unsure which you are dealing with, hand over the pen. [1]
Dysphonia — the voice disorder
Dysphonia is a disorder of phonation — the production of sound at the vocal cords — and it manifests as a hoarse, breathy or whispered voice. The language and the articulation are intact; only the sound source is impaired. The commonest cause is unilateral vocal cord palsy from injury to the recurrent laryngeal nerve (a branch of the vagus, CN X), which loops under the aortic arch on the left and the subclavian artery on the right. A left vocal cord palsy raises the question of a mediastinal or apical lesion — a bronchial carcinoma, an enlarged left atrium in mitral stenosis, or a post-thoracic-surgery injury. Ask about neck or chest surgery, intubation and any neck mass. [1]
Other causes include laryngitis (infectious or from voice overuse), laryngeal cancer, hypothyroidism (a deep, hoarse voice from myxoedematous cord infiltration), and functional (psychogenic) dysphonia. A fatigable dysphonia that worsens with sustained speech is again myasthenia gravis until excluded. Confirm with flexible laryngoscopy if the cause is not apparent clinically. [1]
Part B — Higher mental function
Once the speech is characterised, assess the cognitive domains. The aim is a domain-by-domain map, not a single score. The bedside assessment covers six domains: orientation, attention, memory, language, visuospatial function and executive function. Name the domain as you test it, so the routine looks structured. [1]
1. Orientation
Ask for the time, place and person. Time: the day, date, month and year, and the season. Place: the building, the floor, the city. Person: their own name and, where appropriate, the names of those around them. Disorientation for time is the earliest and most sensitive to go, followed by place; disorientation for person (not knowing who one is) is rare and usually psychogenic or part of a profound acute confusional state. The Abbreviated Mental Test Score (AMTS) — ten questions including time, place and the monarch's name — is a rapid orientation screen used in many ANZ hospitals; a score of 7 or fewer suggests cognitive impairment and warrants fuller assessment. [1]
2. Attention and concentration
Attention is the gateway domain: if attention is impaired, every subsequent test is contaminated. Test it with tasks that require sustained, effortful processing. [1]
Serial 7s. Ask the patient to subtract 7 from 100 and keep subtracting 7: 100, 93, 86, 79... Record the sequence. Five correct subtractions is a pass. Serial 7s is sensitive to inattention but also penalises the poorly educated and the dyscalculic, so have a backup. [1]
Spelling WORLD backwards. Ask the patient to spell the word "world" — D-L-R-O-W. This is the MMSE attention test and is less dependent on numeracy than serial 7s. [1]
Months of the year backwards. Ask the patient to recite the months from December back to January. This is the easiest and most sensitive attention test in patients with limited education. [1]
Digit span. Give a string of numbers at one per second and ask the patient to repeat them forward (normal 6 or more) and backward (normal 4 or more). A reduced digit span indicates impaired attention and is characteristic of an acute confusional state or a working-memory (frontal) deficit. [1]
If attention is impaired, do not interpret the remaining cognitive scores as reliable — declare at presentation that attention was impaired, so memory and executive scores are provisional. The most common reason a cognitive screen is uninterpretable is unrecognised inattention from delirium. [1]
3. Memory
Memory is not one faculty; test each store separately. [1]
Immediate memory (registration). Name three unrelated objects — for example, apple, table, penny — and ask the patient to repeat them. This is registration, the input step; failure here is an attentional problem, not an amnesia. [1]
Short-term (episodic) recall. After three minutes filled with other testing, ask the patient to recall the three objects. Loss of recall with preserved registration is the hallmark of an amnestic syndrome — the episodic memory deficit of Alzheimer disease, Korsakoff syndrome or temporal lobe pathology. [1]
Long-term memory. Test personal memory (their address, their children's names, their wedding day), semantic memory (the names of past prime ministers, the capital of Australia, what a hammer is for) and procedural memory (demonstrating how to use a key or brush teeth). Procedural memory is preserved early in Alzheimer disease because it relies on the basal ganglia and cerebellum, not the hippocampus — which is why a patient may still play the piano but not remember learning it. [1]
Remote memory. Ask about well-established autobiographical and historical events. Remote memory is relatively preserved in early Alzheimer disease (Ribot's law — recent memories decay before old ones) but impaired in semantic dementia. [1]
4. Language
Language has been covered in Part A, but in the cognitive examination state it as a domain: note the fluency, comprehension, repetition and naming you have already assessed, and record whether the patient can read and write. Aphasia inflates the apparent severity of every other cognitive domain because the tests depend on language, so always state the language status before quoting a cognitive score. [1]
5. Visuospatial function
Visuospatial function tests the non-dominant (usually right) parietal lobe, and it is the domain most often skipped in a hurried examination. Two bedside tests cover it. [1]
Clock drawing. Give the patient a blank circle and ask them to "draw a clock, put in all the numbers, and set the hands to ten past eleven." This single task tests attention, planning, visuospatial organisation and executive function. Score it on a recognised system (Shulman or Sunderland). The error patterns localise: neglect of one side (numbers crammed onto the right half) is a non-dominant parietal lesion; perseveration (repeated numbers, hands drawn as loops) is a frontal executive deficit; a conceptual breakdown (the numbers do not go to twelve, the hands are wrong) suggests a more generalised dementia. A systematic review of the clock drawing test reports a pooled sensitivity of about 80 per cent and specificity of about 75 per cent for dementia under the Shulman system, though it is less sensitive for very mild impairment [5].

Intersecting pentagons. Show the patient a card with two overlapping pentagons and ask them to copy it. The MMSE pentagon copy is scored all-or-nothing: two pentagons must intersect to form a four-sided figure. Failure suggests a parietal or generalised deficit. [1]
6. Executive function and frontal lobes
Executive function — planning, set-shifting, inhibition and abstraction — is the domain of the frontal lobes, and it is the hardest to test at the bedside. Use several complementary tests. [1]
Verbal fluency. Ask the patient to name as many animals as they can in one minute (normal is roughly 18 or more, adjusted for education). Then ask for words beginning with a letter — classically F, A, S — in one minute. Reduced verbal fluency is one of the earliest signs of a frontal (including frontotemporal dementia) or subcortical deficit. Category fluency (animals) is relatively preserved in pure frontal disease but impaired in semantic dementia; letter fluency (FAS) is impaired early in frontal executive dysfunction. [1]
The Luria three-step test (fist-edge-palm). Demonstrate the sequence — make a fist, place the hand edge-on, then flat palm — and ask the patient to copy and repeat it. Perseveration (inability to shift between positions) indicates a frontal lesion. [1]
Trail-making. Trail Making Test A (connect numbers 1 to 25) tests processing speed; Trail Making Test B (alternate between numbers and letters: 1-A-2-B-3-C) tests set-shifting. Part B is exquisitely sensitive to frontal executive dysfunction. These are usually done as a paper test with a stopwatch. [1]
Abstract thinking — similarities. Ask "How are an apple and a banana alike?" (both fruit), then "How are a watch and a ruler alike?" (both measure). A concrete answer ("you eat one, you measure with the other") without the abstract superordinate category suggests a frontal or generalised deficit. [1]
Frontal release signs. Elicit the grasp reflex (the patient involuntarily grips your fingers placed in their palm), the palmar-mental reflex (stroking the palm causes a twitch of the ipsilateral mentalis muscle), and the pout or snout reflex (tapping the lips causes a pout). These primitive reflexes are normal in infancy, suppressed in adulthood, and re-emerge with frontal lobe disease — but they are also common in normal ageing, so they support rather than establish a diagnosis. Utilisation behaviour — the patient picks up and uses objects in reach (a comb, a pen) without being asked — is a striking sign of frontal lobe damage. [1]
Cognitive screening instruments
Three instruments dominate bedside cognitive screening, and the candidate should know what each measures and where each falls short. [1]
The Mini-Mental State Examination (MMSE) is the Folstein 30-point screen, sampling orientation, registration, attention and calculation, recall, language and the pentagon copy [1]. It is brief (5 to 10 minutes) and well known, but it is insensitive to mild cognitive impairment, weighted heavily toward language (it was designed in a literate, English-speaking population), influenced by education and age, and now restricted by copyright. A score of 24 or below is the traditional cut-off for dementia, but a well-educated patient may score 27 and still have early Alzheimer disease.
The Montreal Cognitive Assessment (MoCA) was designed to detect mild cognitive impairment that the MMSE misses [2]. It is also a 30-point test, taking 10 to 15 minutes, and it samples a broader spread of domains — notably trail-making, cube copying, clock drawing, a five-word recall, attention, letter-fluency, abstraction and orientation. The MoCA is more sensitive than the MMSE to early and subcortical (vascular and Parkinson-related) cognitive impairment. A score of 26 or below is the cut-off for impairment; one point is added for 12 years or fewer of education.
The Addenbrooke's Cognitive Examination III (ACE-III) is a 100-point test taking 15 to 20 minutes, divided into five domains — attention, memory, fluency, language and visuospatial — each scored out of 20 [3]. It was developed to replace the ACE-R without the copyrighted MMSE sub-items, and it gives a richer domain profile than the MMSE or MoCA. A score of 82 or below suggests dementia; the domain profile helps differentiate Alzheimer disease (memory-dominant) from frontotemporal dementia (fluency and language-dominant) and vascular cognitive impairment. The ACE-III is the preferred extended screen in many ANZ and UK memory clinics.
Choose the tool to the question: the MMSE for a quick ward orientation screen, the MoCA to detect mild cognitive impairment or to screen in a stroke or Parkinson clinic, and the ACE-III for a structured domain assessment in a memory clinic. No screen is a diagnosis — all are triggers for fuller neuropsychological assessment when abnormal. [1]
The say-aloud presentation template
When you finish, stand back and present a structured summary. Lead with the patient and the setting, state whether the speech is aphasic or dysarthric (or both), classify any aphasia on the three axes, give the cognitive domain profile, offer a localising and aetiological formulation, and propose the next step. A model presentation for a patient with Wernicke aphasia: [1]
"I examined Mrs Kaur, a 72-year-old woman, brought in two hours after the sudden onset of confused speech. She is alert and afebrile. On examination of the speech, spontaneous speech is fluent but empty, with frequent phonemic and verbal paraphasias and several neologisms; she does not appear frustrated by this. Comprehension is impaired — she cannot follow two-step commands, though she manages simple one-step commands and yes or no questions intermittently. Repetition is impaired — she cannot repeat 'no ifs, ands, or buts.' Naming is impaired for both objects and their components. She can hear a whispered number in each ear, so hearing is intact. [1]
'On examination of higher mental function, attention and orientation are difficult to assess fully because of the language barrier, but she is alert and attending. Immediate registration is intact. The remaining domains are limited by the aphasia.' [1]
'In summary, this patient has a fluent aphasia with impaired comprehension and impaired repetition — a Wernicke aphasia. The sudden onset in a vasculopathic patient localises to the dominant superior temporal gyrus and is an acute middle cerebral artery inferior-division territory stroke. My immediate priority is to activate the stroke pathway for urgent imaging and thrombolysis assessment, and to exclude a confusional state and a seizure.'" [1]
Three habits that separate a passing from a failing presentation: state aphasia versus dysarthria up front; classify the aphasia on fluency, comprehension and repetition in one sentence; and always declare the language status before quoting cognitive scores, because aphasia contaminates every other domain. [1]
Examiner discussion questions
The discussion after this short case tests reasoning, not memory. The following questions recur; prepare a one-paragraph answer to each. [1]
"How do you distinguish aphasia from dysarthria, and why does it matter?" Aphasia is a disorder of language — the content and structure of speech, including word choice, grammar and meaning. Dysarthria is a disorder of articulation — the mechanical clarity of the spoken sound. The language of a dysarthric patient is intact: they understand, formulate and write normally, but the words come out slurred. The decisive test is writing — a dysarthric patient writes a perfect sentence; an aphasic patient writes a garbled one. It matters because the two localise differently: aphasia localises to the dominant hemisphere language network (Broca, Wernicke, the arcuate fasciculus), while dysarthria localises anywhere along the motor pathway from cortex to muscle (bulbar, pseudobulbar, cerebellar, extrapyramidal, neuromuscular). Misclassifying a dysarthria as an aphasia sends you to the wrong lobe and the wrong differential. [1]
"What is conduction aphasia, and what does it teach about language?" Conduction aphasia is fluent speech with preserved comprehension but severely impaired repetition, from a lesion of the arcuate fasciculus — the white-matter bundle connecting Wernicke area (comprehension) to Broca area (production). The paradox is that the patient understands and can speak, yet cannot echo what they have just heard, because the bridge between input and output is severed. The classical model — Wernicke area decodes, the arcuate fasciculus transmits, Broca area produces — was built to explain exactly this syndrome. The lesion is usually a left superior temporal or supramarginal gyrus infarct. It teaches that repetition is the most localising of the language axes, because it tests a single white-matter tract. [1]
"How do the transcortical aphasias differ, and what is their mechanism?" The transcortical aphasias — motor, sensory and mixed — share one feature: repetition is preserved, because the perisylvian language cortex is intact and connected as a self-contained circuit that can echo but not create or decode. The lesion is in the watershed territory around the perisylvian language area, which is disconnected from the rest of the brain but internally preserved. Transcortical motor aphasia (non-fluent, good comprehension, preserved repetition) is a lesion anterior and superior to Broca area; transcortical sensory (fluent, poor comprehension, preserved repetition) is posterior and superior to Wernicke; mixed transcortical (non-fluent, poor comprehension, preserved repetition) isolates the whole language area. They are most often caused by hypoperfusion — watershed infarction from cardiac arrest, profound hypotension or carotid occlusion — and the preserved repetition is the giveaway. [1]
"When does an acute confusional state mimic an aphasia, and how do you tell them apart?" A delirious patient may produce fluent, incoherent speech that sounds like Wernicke aphasia, and their comprehension may appear impaired. The distinguishing features of delirium are fluctuating attention, altered consciousness (not fully alert), disorganised thinking (rambling, off the point, tangential) and a recent, acute onset with a precipitating cause (infection, drug withdrawal, metabolic derangement). A Wernicke aphasia, by contrast, has preserved alertness and attention — the patient is awake and attending, but their language is empty. Test attention formally (digit span, months backwards): it is impaired in delirium and preserved in a pure aphasia. The error that fails candidates is labelling an acute, fluctuating, inattentive patient as having a focal Wernicke aphasia and sending them to the stroke unit when they have sepsis or hyponatraemia. [1]
"Which cognitive screening tool would you use, and what are its limits?" For a quick ward orientation screen, the MMSE [1] is familiar and brief, but it is insensitive to mild cognitive impairment and weighted toward language. For detecting mild cognitive impairment — in a stroke, Parkinson or memory clinic — the MoCA [2] is the better choice because it samples visuospatial and executive function. For a structured domain profile in a memory clinic, the ACE-III [3] gives five domain subscores and helps differentiate the dementia subtypes. No screen is diagnostic; all are triggers for formal neuropsychological assessment, and all are confounded by education, language, sensory impairment and mood. Always state the limits of the screen you quote.
"What is the evidence for speech and language therapy in post-stroke aphasia?" The Cochrane review of speech and language therapy for aphasia following stroke found that therapy improves functional communication, receptive language and expressive language compared with no therapy, with a suggestion that higher intensity and dose are more effective [4]. There is insufficient evidence to favour one therapeutic approach over another, or to settle group versus individual therapy. So the practical position is: refer early to a speech and language therapist, deliver therapy at a clinically meaningful intensity, and set functional communication goals rather than expecting a single "best" technique.
Common traps and pitfalls
The candidates who fail this station do so for predictable reasons. Avoid these: [1]
- Testing cognition before speech. You cannot validly test comprehension, memory or executive function through a language the patient cannot use. Always examine speech first; if there is a significant aphasia, declare it and treat all subsequent cognitive scores as provisional.
- Classifying aphasia on fluency alone. Fluency separates anterior from posterior, but comprehension and repetition are needed to separate Wernicke from conduction, and the transcortical aphasias from their non-transcortical counterparts. Always complete the three axes.
- Confusing dysarthria with non-fluent aphasia. Both sound garbled, but the dysarthric patient writes normally and the aphasic patient does not. When in doubt, hand over the pen.
- Skipping the visuospatial and executive domains. The clock-drawing test and verbal fluency are quick, high-yield and frequently omitted. Their omission loses both the findings and the appearance of a complete system.
- Labelling delirium as a focal aphasia. An acute, fluctuating, inattentive patient is delirious until proven otherwise; do not anchor on a fluent, incoherent speech sample and miss the sepsis or the metabolic cause.
- Failing to exclude hearing and visual impairment. A patient without their hearing aids or glasses will fail comprehension and visuospatial tests for reasons unrelated to cognition. Confirm sensory aids before you start.
- Quoting a single MMSE or MoCA score without its domain breakdown. A score without the domain profile is uninterpretable; the pattern (memory-dominant versus fluency-dominant versus visuospatial-dominant) is what frames the differential. [1]
Integration with the long case
Speech and cognitive findings appear in the DCE long case as one problem among several, and the skill is to integrate them. A patient with a left middle cerebral artery stroke may have a global aphasia, a right hemiparesis and visual neglect — the aphasia frames the rehabilitation plan (early speech therapy, alternative communication) and the prognosis. A patient with Alzheimer disease may have an anomic aphasia, impaired episodic memory and a preserved procedural memory — the domain profile confirms the syndrome and guides the cholinesterase inhibitor discussion. A patient with frontotemporal dementia may present with a progressive non-fluent aphasia or semantic dementia, and the language profile (rather than the memory) is the key to the diagnosis. A patient with motor neuron disease may develop a dysarthria that is bulbar or pseudobulbar, and the distinction — flaccid versus spastic tongue, absent versus brisk gag — frames the prognosis and the airway plan. [1]
The speech and higher-function short case rewards the candidate who is systematic, domain-mapped and localising. Practise the six-step speech sequence and the six-domain cognitive map until they are reflexes; learn the aphasia table until the classification is instant; rehearse the presentation until it leads with the aphasia-versus-dysarthria fork and the three-axis classification. That is the standard the examiner expects, and the standard that passes. [1]
References
- [1]Folstein MF, Folstein SE, McHugh PR Mini-mental state. A practical method for grading the cognitive state of patients for the clinician J Psychiatr Res, 1975.PMID 1202204
- [2]Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [3]Hsieh S, Schubert S, Hoon C, Mioshi E, Hodges JR Validation of the Addenbrooke's Cognitive Examination III in frontotemporal dementia and Alzheimer's disease Dement Geriatr Cogn Disord, 2013.PMID 23949210
- [4]Brady MC, Kelly H, Godwin J, Enderby P, Campbell P Speech and language therapy for aphasia following stroke Cochrane Database Syst Rev, 2016.PMID 27245310
- [5]DeDeyn PP, Seripa D, Panza F, et al. The clock drawing test: A systematic review and meta-analysis of diagnostic accuracy J Adv Nurs, 2018.PMID 30047147