Phys · general-medicine
Neurological Examination of the Upper Limbs — The DCE Short-Case Routine
Also known as upper limb neurological examination · upper limb neurological exam · neurological examination upper limbs · examine this patient upper limbs neurologically · DCE short case upper limb neurology · PACES neurological station upper limb · motor examination upper limb · myotome examination · dermatome examination upper limb · tone power reflexes coordination sensory · UMN versus LMN · finger-nose test · pronator drift · Hoffman sign · MRC power grading · dysdiadochokinesia · cogwheel rigidity · lead-pipe rigidity · inverted supinator sign
Consultant-physician-depth guide to the systematic neurological examination of the upper limbs for the FRACP DCE short case and the MRCP PACES neurological station. Covers the eight-step routine — inspection, tone, power by myotome, reflexes, coordination, sensory, cortical sensory, and functional testing — the interpretation of each sign, the UMN versus LMN framework, the presentation template the candidate delivers aloud, and the examiner discussion questions by finding. Addresses muscle wasting patterns (dorsal interossei in MND, thenar eminence in median nerve, hypothenar in ulnar nerve), tremor classification, tone abnormalities (spastic, lead-pipe, cogwheel, hypotonic), the MRC power grading, reflex levels and the inverted supinator sign, the finger-nose test and dysdiadochokinesia, the spinothalamic and dorsal column sensory pathways, stereognosis and graphesthesia, and the common examination traps. Structured for FRACP DCE and MRCP PACES preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Neurological Examination of the Upper Limbs — The DCE Short-Case Routine

The answer first
The instruction "Please examine this patient's upper limbs neurologically" is the single most common DCE short-case instruction in the FRACP examination, and it is the classic neurological station in the MRCP PACES Station 3. The candidate who performs it fluently and presents a clear localisation demonstrates the core neurological competency the examiners are testing: the ability to translate physical signs into anatomical localisation, and from there into a differential diagnosis. [1]
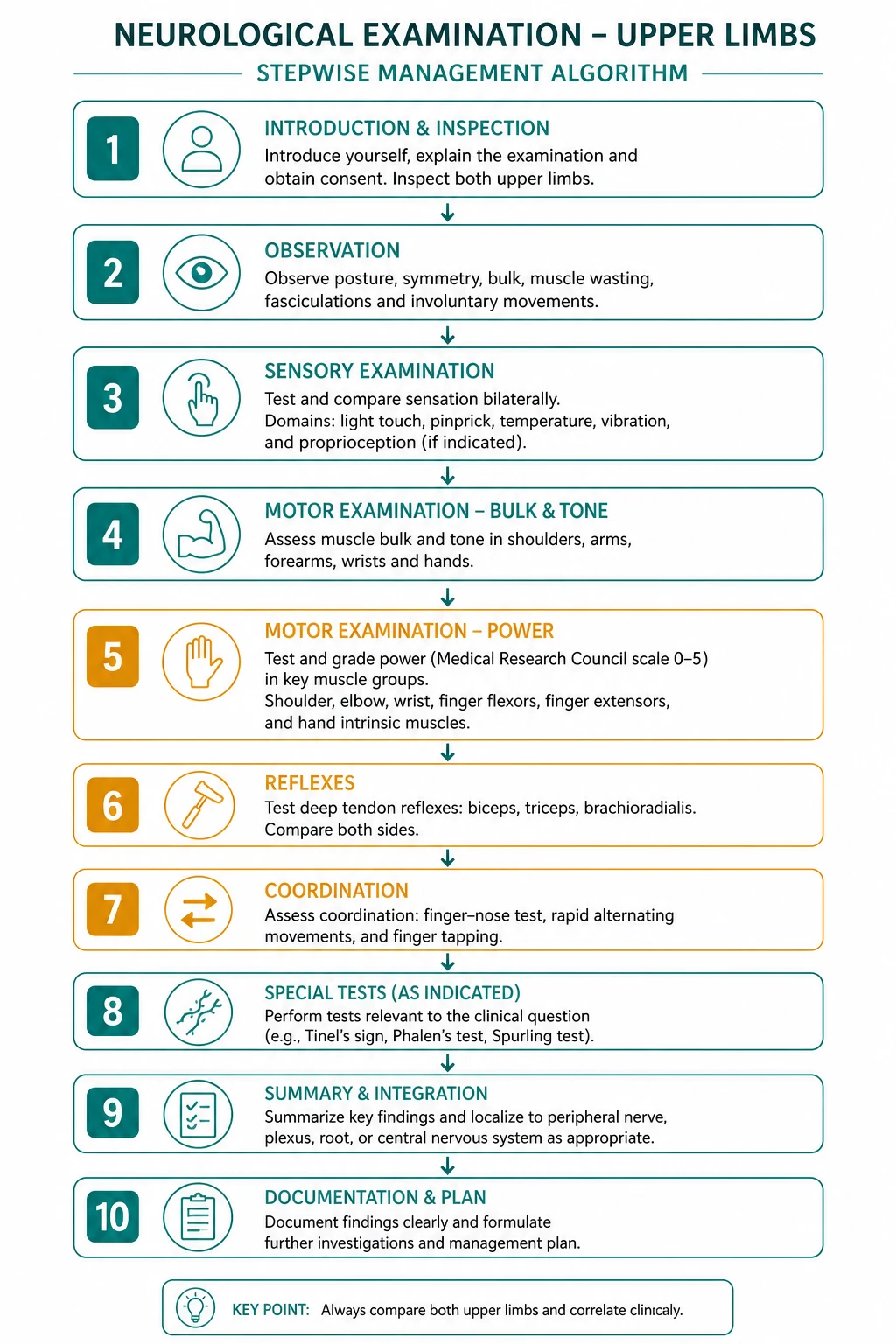
The routine is eight steps, performed in the same order every time: [1]
- Inspection — wasting, fasciculations, tremor, abnormal postures
- Tone — at the wrist and the elbow
- Power — by myotome, with MRC grading
- Reflexes — biceps, supinator, triceps, finger jerk, Hoffman
- Coordination — finger-nose, rapid alternating movements, pronator drift
- Sensory — light touch, pinprick (spinothalamic), vibration, joint position (dorsal column)
- Additional and cortical sensory — APR, stereognosis, graphesthesia
- Functional — button, pick up a small object [1]

The candidate who jumps to power before tone, or who forgets the sensory exam, has failed the sequence and has also failed to collect the data the localisation requires. The eight steps are not an arbitrary checklist — they are the order in which the lesion declares itself, and the order in which the examiner expects the findings. [1]
Viva trap: "What is the single most important observation in the first ten seconds of the upper limb neurological exam?" The honest answer is the look test. The candidate who spends thirty seconds inspecting before touching the patient — looking for wasting, for fasciculations, for tremor, for abnormal posture — has often generated the differential before a single reflex is struck. The candidate who rushes to reflexes and misses the wasted, fasciculating first dorsal interosseus has missed motor neuron disease. [1]
Step 1 — Inspection: the look test that frames the differential
The examination begins the moment the patient exposes their arms. The candidate sits or stands the patient comfortably, exposes both arms to above the elbow (and ideally to the shoulder), and inspects systematically from the shoulder girdle to the fingertips, comparing left with right. The four observations that frame the differential are: [1]
Muscle wasting — the pattern identifies the lesion
Generalised wasting of the upper limb with reduced muscle bulk throughout indicates a chronic lower motor neuron process — a severe peripheral neuropathy, a polio survivor, or advanced motor neuron disease with extensive LMN involvement. [1]
Focal wasting by muscle group is the high-yield observation because each pattern maps to a specific nerve or root: [1]
- Dorsal interossei wasting (the guttering between the metacarpals on the dorsum of the hand) is the classic sign of motor neuron disease and of ulnar nerve palsy. The discriminator: in MND the wasting is often asymmetric, accompanied by fasciculations and by UMN signs elsewhere; in ulnar nerve palsy the wasting is confined to the ulnar distribution (hypothenar, interossei, medial two lumbricals) with sparing of the thenar eminence (median nerve, supplied by C8/T1 but via the median nerve).
- Thenar eminence wasting (the fleshy pad at the base of the thumb, flattening of the APB and OP muscles) is the classic sign of a median nerve lesion — most commonly carpal tunnel syndrome at the wrist, or less commonly a proximal median nerve lesion. The key teaching point: the thenar muscles (APB, OP, superficial head of FPB) are supplied by the recurrent motor branch of the median nerve (C8/T1), which is vulnerable at the carpal tunnel. The hypothenar muscles are ulnar and are spared in carpal tunnel syndrome.
- Hypothenar wasting (the fleshy pad on the ulnar side of the palm) indicates an ulnar nerve lesion — at the wrist (Guyon canal) or at the elbow (cubital tunnel). In ulnar nerve palsy the hand shows the claw hand deformity: hyperextension of the metacarpophalangeal joints and flexion of the interphalangeal joints of the ring and little fingers (the "hand of benediction" when the patient is asked to extend the fingers).
- Wasting of the small muscles of the hand with sparing of the thenar eminence suggests a T1 radiculopathy or a lower brachial plexus lesion (Klumpke paralysis), because T1 supplies all the intrinsic hand muscles via both the median and the ulnar nerves — so a T1 root lesion wastes the thenar AND the hypothenar, while a combined median-plus-ulnar peripheral lesion is rare.
- Scapular winging (the medial border of the scapula lifting off the chest wall on pushing against a wall) indicates serratus anterior weakness (long thoracic nerve, C5/6/7) — a common incidental finding in the short case. [1]
Fasciculations — the sign of anterior horn cell disease
Fasciculations are involuntary, brief, visible muscle twitches under the skin — the clinical signature of anterior horn cell or motor axon irritability. They are best seen in the relaxed muscle, in good light, with the muscle at rest. The candidate should look specifically at the deltoid, the biceps, the triceps, the forearm muscles, the thenar eminence, and the first dorsal interosseus. [1]
The critical interpretation: fasciculations with weakness and wasting indicate a lower motor neuron lesion. The combination of widespread fasciculations with wasting and weakness, especially if accompanied by UMN signs (brisk reflexes, increased tone) in the same or other limbs, is the clinical signature of motor neuron disease (amyotrophic lateral sclerosis) — the combination of denervation (LMN signs) and corticospinal tract degeneration (UMN signs) is the disease's hallmark [1][2].
The trap: benign fasciculations — fasciculations without weakness, without wasting, and without reflex change — are common, especially in the calf of healthy young adults, and they do not indicate disease. The candidate who diagnoses MND on the basis of calf fasciculations in a neurologically normal patient has overcalled the sign. [1]
Tremor — the type localises the lesion
The tremor is classified by when it occurs: [1]
- Rest tremor — present when the limb is fully supported and at rest, suppressed by voluntary movement. The classic pill-rolling tremor at 4 to 6 Hz, prominent in the hands, is the signature of Parkinson disease and of other parkinsonian syndromes. The MDS clinical diagnostic criteria define parkinsonism as bradykinesia plus rest tremor or rigidity [4]. The candidate should observe the tremor with the hands resting in the lap, then with the arms outstretched (the rest tremor often suppresses with posture).
- Postural tremor — present when the limb is held against gravity (arms outstretched), absent at rest. The differential is essential tremor (a bilateral, slowly progressive, action tremor, often with a family history, improved by alcohol), thyrotoxicosis (a fine, fast tremor with tachycardia, weight loss, and lid lag), alcohol withdrawal, beta-agonist or lithium therapy, and physiological tremor exaggerated by anxiety or caffeine. The discriminator: essential tremor improves with alcohol and worsens with movement; the parkinsonian rest tremor is present at rest and often suppressed by movement.
- Intention tremor — a tremor that appears and worsens as the finger approaches a target (the nose in the finger-nose test), absent at rest and at the start of the movement. The intention tremor is a cerebellar sign and is accompanied by dysmetria (past-pointing). The candidate tests it during the coordination step, not at inspection, but the observation of a coarse, irregular tremor at the end of a movement during inspection may raise the cerebellar question early.
Abnormal postures
Dystonia — sustained, involuntary muscle contractions causing twisting, repetitive movements or abnormal postures (pronation of the forearm, flexion of the wrist, extension of the fingers, torticollis). Dystonia may be focal (writer's cramp, cervical dystonia), segmental, or generalised, and it may be idiopathic, drug-induced (neuroleptics, metoclopramide — the tardive dystonias), or secondary to a structural lesion (basal ganglia stroke, Wilson disease). [1]
A fixed flexion deformity of the wrist and fingers with pronation of the forearm is the classic hemiparetic posture of an established upper motor neuron lesion — the "pyramidal" distribution of weakness where the flexors are stronger than the extensors in the upper limb. This is the appearance of the chronic stroke patient's arm, and it tells the candidate, before any reflex is struck, that this is a UMN lesion. [1]
Step 2 — Tone: the gateway to UMN versus LMN
Tone is assessed by the candidate passively moving the patient's joints through their full range of motion, with the patient relaxed. The candidate holds the patient's hand as if shaking it, and moves the wrist through flexion, extension, abduction, and adduction; then moves the forearm through pronation and supination; then flexes and extends the elbow. The four abnormalities are: [1]
Spasticity — the clasp-knife and the UMN lesion
Spasticity is velocity-dependent increased tone — the resistance is greater with fast passive movement and less with slow movement. The classic description is the clasp-knife phenomenon: an initial strong resistance that suddenly gives way as the movement continues, like the blade of a clasp knife snapping shut. Spasticity preferentially affects the flexors and pronators of the upper limb (the pyramidal distribution). The localisation: a corticospinal tract (upper motor neuron) lesion anywhere from the motor cortex to the spinal cord segment above the level of the muscle. [1]
Rigidity — the lead-pipe and the cogwheel
Rigidity is velocity-independent increased tone — the resistance is constant throughout the range of movement, independent of speed. Two subtypes: [1]
- Lead-pipe rigidity — a smooth, uniform resistance throughout the range, like bending a lead pipe. This is a basal ganglia sign, seen in any cause of extrapyramidal rigidity.
- Cogwheel rigidity — a ratchety, jerky resistance, as if a cogwheel were engaging at intervals. This is the combination of rigidity with a superimposed tremor, and it is the classic tone abnormality of Parkinson disease [4]. The cogwheel is best felt at the wrist with a slow, continuous pronation-supination movement.
The teaching point: spasticity and rigidity are both increased tone, but they localise differently — spasticity to the corticospinal tract (pyramidal), rigidity to the basal ganglia (extrapyramidal). The candidate who feels increased tone and calls it all "hypertonia" has lost the localisation. [1]
Hypotonia — the LMN and cerebellar sign
Hypotonia — reduced or absent resistance to passive movement, a "floppy" limb — is seen in lower motor neuron lesions (where the denervated muscle offers no resistance), in cerebellar disease (where the cerebellar influence on tone is lost), in acute UMN lesions (spinal shock — the first 24 to 48 hours after an acute cord lesion, before spasticity develops), and in muscle disease (myopathy). The hypotonic limb may also show pendular reflexes — a reflex swing that oscillates several times before settling, classically seen in cerebellar disease. [1]
Step 3 — Power: the myotome map and the MRC grade

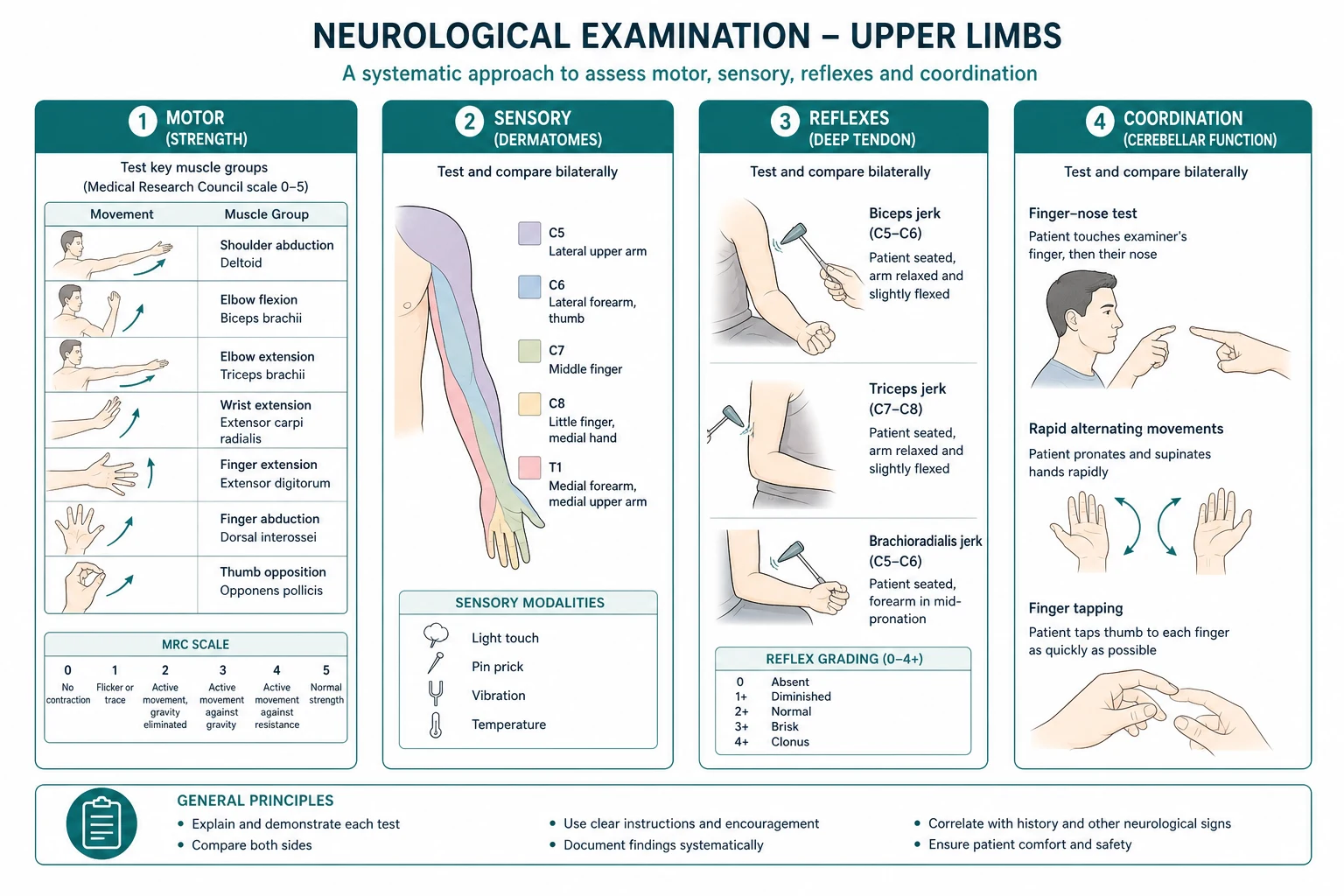
Power is tested by myotome, with the muscle group acting against the candidate's resistance. The candidate tests each movement, compares left with right, and grades with the Medical Research Council scale (0 to 5): [1]
- 0 — no contraction
- 1 — flicker or trace of contraction
- 2 — active movement with gravity eliminated
- 3 — active movement against gravity
- 4 — active movement against gravity and some resistance (subdivided as 4-minus, 4, 4-plus for finer grading)
- 5 — normal power [1]
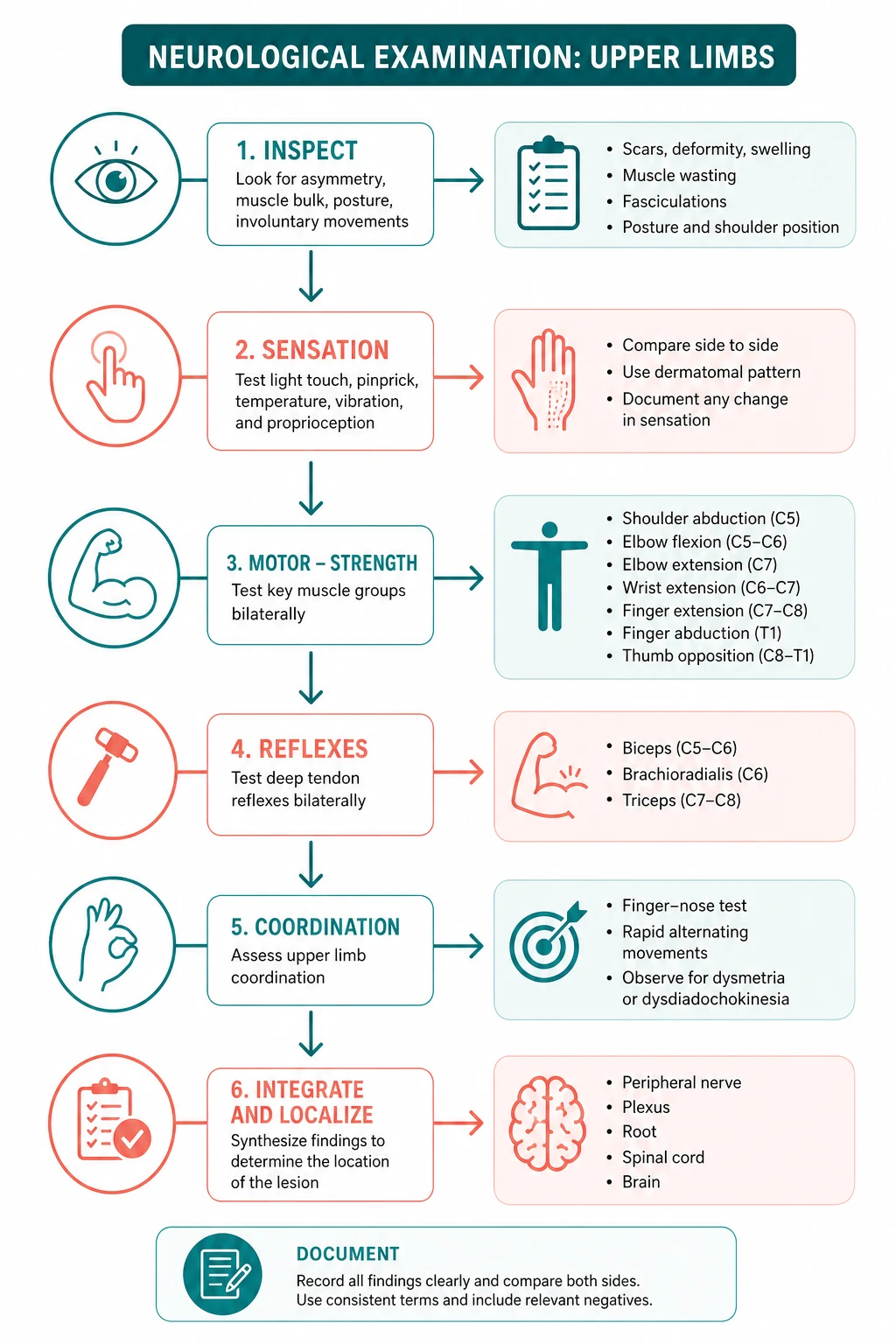
The myotome sequence for the upper limb, with the root, the muscle, and the action: [1]
| Movement | Root level | Key muscle | Action |
|---|---|---|---|
| Shoulder abduction | C5 (axillary nerve) | Deltoid | Abduct the arm to 90 degrees against resistance at the elbow |
| Elbow flexion | C5/C6 (musculocutaneous nerve) | Biceps, brachialis | Flex the elbow against resistance at the forearm |
| Elbow extension | C7 (radial nerve) | Triceps | Extend the elbow against resistance at the forearm |
| Wrist extension | C7 (radial nerve) | Extensor carpi radialis, ulnaris | Cock up the wrist against resistance at the dorsum of the hand |
| Finger flexion | C8 (median and ulnar nerves) | Flexor digitorum superficialis and profundus | Squeeze the candidate's two fingers |
| Finger abduction | T1 (ulnar nerve) | Dorsal interossei | Spread the fingers apart against resistance |
| Thumb opposition | T1 (median nerve) | Abductor pollicis brevis, opponens pollicis | Touch the thumb to the little finger against resistance |
The high-yield teaching points: [1]
The pattern of weakness localises the lesion. A pyramidal (UMN) weakness preferentially affects the extensors of the upper limb (triceps, wrist extensors, finger extensors) and the flexors of the lower limb — this is the "pyramidal distribution" that gives the hemiparetic arm its flexed posture. A lower motor neuron weakness preferentially affects the muscles supplied by the damaged nerve or root — a C7 root lesion weakens triceps and wrist extensors; an ulnar nerve lesion weakens finger abduction and the hypothenar muscles; a median nerve lesion weakens thumb opposition and the thenar muscles. [1]
The small muscles of the hand (T1) are the commonest site of clinically significant weakness. The candidate who tests finger abduction (dorsal interossei, ulnar nerve, T1) and thumb opposition (APB, median nerve, T1) has screened for ulnar nerve palsy, median nerve palsy, T1 radiculopathy, and brachial plexopathy in two movements. A patient who cannot abduct the fingers but can oppose the thumb has an ulnar nerve lesion; a patient who cannot oppose the thumb but can abduct the fingers has a median nerve lesion; a patient who can do neither has a T1 root or lower plexus lesion. [1]
Step 4 — Reflexes: the root level and the UMN sign
The deep tendon reflexes are tested with a tendon hammer, comparing left with right, and graded as 0 (absent), plus-minus (present with reinforcement), plus (normal), plus-plus (brisk), plus-plus-plus (very brisk with clonus). The candidate should use the Jendrassik manoeuvre (the patient hooks the fingers of both hands together and pulls) to reinforce an absent reflex. [1]
The reflex arc and the root level: [1]
| Reflex | Root level | Nerve | Technique |
|---|---|---|---|
| Biceps jerk | C5/C6 | Musculocutaneous | Thumb on the biceps tendon, strike the thumb |
| Supinator (brachioradialis) jerk | C5/C6 | Radial | Strike the radius just above the wrist, watch for elbow flexion |
| Triceps jerk | C7 | Radial | Strike the triceps tendon just above the olecranon |
| Finger jerk (Wartenberg) | C8 | Median and ulnar | Strike the candidate's fingers placed on the patient's palmar surface, watch for finger flexion |
The inverted supinator sign — the classic cervical localisation
The inverted supinator sign is pathognomonic of a C5/C6 cervical cord lesion (most commonly cervical spondylotic myelopathy at C5/C6). When the supinator reflex is struck, instead of the normal elbow flexion, the response is paradoxical finger flexion (a C8 response) with absent or diminished elbow flexion (the C5/C6 reflex arc is interrupted at the cord). The mechanism: the lesion at C5/C6 interrupts the afferent limb of the supinator reflex (so the expected response is absent), but the descending corticospinal tract is also interrupted at that level, removing the inhibitory influence on the reflex arcs below the lesion (so the C8 finger jerk becomes exaggerated). The inverted supinator with a brisk finger jerk and Hoffman sign is the classic bedside triad of cervical myelopathy at C5/C6. [1]
Hoffman sign — the UMN screen
The Hoffman sign is tested by flicking the patient's middle fingernail downward (the candidate holds the patient's middle finger at the proximal interterphalangeal joint and flicks the distal phalanx). A positive response is flexion and adduction of the thumb and flexion of the index finger — a pathological reflex indicating upper motor neuron involvement (loss of cortical inhibition on the flexor reflex). The Hoffman sign is the upper-limb equivalent of the Babinski sign in the lower limb. [1]
The evidence: a systematic review of physical examination maneuvers in cervical myelopathy found that the Hoffman sign, while a useful screening test, has variable sensitivity (approximately 20 to 60 per cent across studies) and should not be used in isolation to confirm or refute the diagnosis [3]. A bilateral or markedly asymmetric Hoffman sign is more clinically significant than a weakly positive unilateral finding, which may be present in up to 3 per cent of healthy asymptomatic individuals. The candidate interprets the Hoffman sign in the context of the other UMN signs (tone, reflexes, pronator drift) and confirms with MRI.
The reflex interpretation framework
- Absent reflexes with weakness and wasting — lower motor neuron lesion (anterior horn cell, root, nerve).
- Brisk reflexes with increased tone and weakness — upper motor neuron lesion (corticospinal tract).
- Mixed UMN and LMN signs in the same patient across body regions — motor neuron disease [1][2]. The combination of a brisk reflex in a wasted, fasciculating limb is the classic "ALS reflex" and should be sought specifically.
- Diffusely brisk reflexes with normal power and tone in a young, anxious patient — anxiety-driven hyperreflexia; the candidate does not overcall this as neurological disease.
Step 5 — Coordination: the cerebellar and the UMN screen
Coordination testing assesses the cerebellum and the corticospinal tract. Three tests: [1]
The finger-nose test
The candidate holds a finger at arm's length from the patient and asks the patient to touch their own nose, then the candidate's finger, then their nose again, moving the target finger to different positions. The candidate watches for: [1]
- Intention tremor — a tremor that appears and worsens as the finger approaches the target. This is a cerebellar sign, localising to the ipsilateral cerebellar hemisphere.
- Dysmetria (past-pointing) — the finger overshoots or undershoots the target. Dysmetria is also a cerebellar sign. The candidate tests for past-pointing by asking the patient to touch the target with their eyes open, then with their eyes closed — past-pointing that is consistent in one direction suggests a cerebellar lesion; past-pointing that is random and worsens with the eyes closed suggests a proprioceptive (dorsal column) deficit.
- Decomposition of movement — the smooth arc of the movement breaks into a series of jerky, segmented steps. Another cerebellar sign. [1]
Rapid alternating movements — dysdiadochokinesia
The patient is asked to rapidly pronate and supinate one hand on the other (the "patting" test) or to tap the fingers rapidly on the thigh or the dorsum of the other hand. Dysdiadochokinesia — slowness, irregularity, and clumsiness of the rapid alternating movement — is the classic cerebellar sign, indicating an ipsilateral cerebellar hemisphere lesion. The candidate compares the two sides; the side with the worse dysdiadochokinesia points to the ipsilateral cerebellum. [1]
Pronator drift (Barré sign) — the sensitive UMN screen
The patient holds both arms outstretched with the palms supinated and the eyes closed for 20 to 30 seconds. The candidate watches for: [1]
- Pronator drift — the affected arm slowly drifts downward and pronates (the palm turns inward and downward). This is the classic UMN sign — the supinator muscles (which hold the palm up) are weaker than the pronator muscles in a pyramidal lesion, so with the eyes closed and the visual compensation removed, the arm drifts and pronates. Pronator drift is often more sensitive than power testing for detecting subtle UMN weakness.
- Upward drift with writhing fingers — the arm drifts upward and laterally with involuntary writhing movements of the fingers (pseudoathetosis). This is proprioceptive (dorsal column) loss, not UMN weakness — the patient cannot maintain the arm position without visual input because they have lost the position sense.
- Downward drift without pronation — the arm slowly sinks but does not pronate; this may be seen with proximal weakness or with non-organic weakness. [1]
The candidate who tests pronator drift with eyes open has missed the sign — the eyes-closed component is what makes the test sensitive, because it removes the visual compensation. [1]
Step 6 — Sensory: the two-pathway framework

The sensory exam tests the two ascending pathways of the spinal cord: [1]
The spinothalamic pathway — pain and temperature
The candidate tests pinprick (using a disposable neurotip or the sharp end of a safety pin) and, if indicated, temperature (a cold tuning fork or test tube). The patient is asked to report "sharp" or "dull" as the candidate alternates the sharp and blunt ends on the skin. [1]
The candidate tests the dermatomes of the upper limb: C5 (lateral upper arm), C6 (lateral forearm and thumb), C7 (middle finger), C8 (medial forearm and little finger), T1 (medial upper arm). The candidate also tests the individual nerve territories: the median nerve (the palmar surfaces of the thumb, index, and middle fingers), the ulnar nerve (the palmar surfaces of the ring and little fingers), and the radial nerve (the dorsum of the hand, the web space). [1]
The distribution of the sensory loss localises the lesion: [1]
- A dermatomal pattern (one root territory affected) suggests a radiculopathy.
- A glove distribution (all fingers and the palm, symmetric, bilateral) suggests a peripheral neuropathy (the classic "glove and stocking" distribution of a length-dependent axonal neuropathy).
- A single nerve territory (median, ulnar, radial) suggests a mononeuropathy.
- A sensory level on the trunk (loss of pinprick below a line on the chest or abdomen) suggests a spinal cord lesion (the level of the sensory loss is typically one to two segments below the cord lesion). [1]
The dorsal column pathway — vibration and joint position
The candidate tests vibration sense with a 128-Hz tuning fork, struck and placed on a bony prominence — the distal interphalangeal joint of the index finger or the little finger, the radial styloid, the ulnar styloid, and if absent distally, progressing proximally. The patient is asked to report "buzzing" or "vibration," and the candidate tests by alternating struck and silent forks. [1]
The candidate tests joint position sense by holding the sides of the distal interphalangeal joint of a finger (the candidate holds the finger by the sides, not the top and bottom, to avoid pressure cues) and moving it a few degrees up or down, with the patient's eyes closed, asking "up or down?" [1]
Dorsal column loss (impaired vibration and joint position sense) localises to:
- A peripheral neuropathy (the commonest cause of distal dorsal column loss, because the large-fibre sensory nerves are affected).
- A posterior column lesion in the spinal cord — vitamin B12 deficiency (subacute combined degeneration), tabes dorsalis (neurosyphilis), multiple sclerosis.
- A sensory ataxia — the patient with dorsal column loss will have a positive Romberg (falls with eyes closed) and pseudoathetosis (writhing fingers with arms outstretched and eyes closed). [1]
The teaching point: vibration is the first modality lost in a peripheral neuropathy and in dorsal column disease. The candidate who tests vibration at the distal interphalangeal joint has the most sensitive single test for large-fibre sensory loss. [1]
The tactile modality
The candidate tests light touch with a wisp of cotton wool or a fingertip, mapping the distribution. Light touch is carried by both the spinothalamic tract and the dorsal columns, so it is less localising than pinprick or vibration — but a dissociated sensory loss (pinprick lost with light touch preserved, or vice versa) suggests a central cord lesion (syringomyelia, where the crossing spinothalamic fibres are selectively damaged with sparing of the dorsal columns and the light touch fibres). [1]
Step 7 — Additional and cortical sensory: the higher-order testing
The APR (abnormal puppet reflex)
The APR is a variant of the pronator drift test: the patient holds the arms outstretched with eyes closed, palms up, and the candidate taps the forearms downward briskly. The affected arm pronates and drifts more than the normal arm — a sensitive UMN sign. The APR is not universally taught but is a useful adjunct when the standard pronator drift is equivocal. [1]
Stereognosis
The patient is asked, with eyes closed, to identify a common object placed in the hand — a coin, a key, a button, a paperclip. The candidate tests each hand separately. Astereognosis — the inability to identify objects despite intact primary sensory modalities (touch, pain, vibration, joint position) — indicates a lesion in the contralateral sensory cortex (parietal lobe). The teaching point: before concluding astereognosis, the candidate must confirm that the primary sensory modalities are intact in that hand — a patient who cannot feel the coin because of a peripheral neuropathy is not astereognosic. [1]
Graphesthesia
The candidate traces a number or letter on the patient's palm with the eyes closed. Agraphesthesia — the inability to identify the figure with intact primary sensation — also indicates a contralateral parietal lobe lesion. Like stereognosis, graphesthesia requires intact primary sensation to be interpretable. [1]
Two-point discrimination
The candidate uses callipers or a bent paperclip to test the minimum distance at which the patient can distinguish one point from two on the fingertip. The normal threshold on the fingertip is 2 to 5 mm. An elevated threshold (with intact primary sensation) indicates a cortical sensory deficit. Two-point discrimination is less commonly tested in the DCE short case but may be asked in the PACES neurological station. [1]
Step 8 — Functional testing: the real-world assessment
The candidate asks the patient to perform a functional task: fasten and unfasten a button, pick up a small object (a coin or a pen) from the table, or pour water from a jug. The observation is not just whether the task is accomplished, but how — with which fingers, with what dexterity, with what compensatory movements. Functional testing reveals the impact of the neurological deficit on the patient's daily life, and it is a test of integration: a patient with a normal power grade and normal reflexes who cannot button a shirt may have a cerebellar deficit, a proprioceptive loss, a cortical sensory deficit, or an apraxia — each of which is missed by the segmental testing and revealed by the functional task. [1]
The UMN versus LMN framework: the synthesis of the examination
The entire eight-step routine builds toward one question: is this an upper motor neuron lesion or a lower motor neuron lesion? The framework: [1]
| Feature | UMN lesion | LMN lesion |
|---|---|---|
| Tone | Increased (spastic, clasp-knife) | Decreased (flaccid) |
| Power | Decreased, pyramidal pattern (extensors weaker in the arm) | Decreased, in the distribution of the nerve or root |
| Reflexes | Brisk (hyperreflexia), clonus | Absent or reduced (hyporeflexia) |
| Plantar | Upgoing (extensor, Babinski) | Normal (downgoing, flexor) |
| Wasting | Absent (or late, from disuse) | Present, in the distribution of the nerve or root |
| Fasciculations | Absent | Present |
| Sensory | May have a sensory level (cord lesion) or a hemisensory loss (cortex) | May have a dermatomal or nerve-territory sensory loss |
The mixed pattern — UMN signs in one region (e.g., brisk reflexes, increased tone) with LMN signs in another (e.g., wasted, fasciculating muscles) — is the clinical signature of motor neuron disease (amyotrophic lateral sclerosis), the diagnosis the candidate must not miss in the short case [1][2].
The presentation template
After completing the eight steps, the candidate turns to the examiner and presents. The template is a structured summary, not a recitation of every finding — the candidate highlights the abnormal findings and offers the localisation and the differential. [1]
Template: [1]
"I have examined this patient's upper limbs neurologically. On inspection, there is [wasting of the ... / no wasting] and [fasciculations in the ... / no fasciculations]. There is [a rest tremor / a postural tremor / no tremor]. The tone is [increased with cogwheeling / increased with clasp-knife spasticity / normal / decreased]. The power is [normal / reduced, with weakness of ... (MRC grade ...)]. The reflexes are [brisk / normal / absent] at the [biceps / supinator / triceps / finger jerk], with [a positive Hoffman sign / no Hoffman sign]. Coordination is [normal / impaired, with intention tremor and past-pointing / impaired, with dysdiadochokinesia]. Pronator drift is [present on the right / absent]. Sensation is [intact / reduced in a ... distribution]. Cortical sensory testing is [normal / abnormal, with astereognosis]. [1]
In summary, this patient has [an upper motor neuron pattern / a lower motor neuron pattern / a mixed pattern / a cerebellar pattern], with the key findings being [the ...]. My localisation is [a right cortical lesion / a cervical cord lesion at the C5/C6 level / a left cerebellar hemisphere lesion / a peripheral neuropathy / a median nerve lesion at the wrist / motor neuron disease]. My differential diagnosis is [stroke / cervical spondylotic myelopathy / Parkinson disease / carpal tunnel syndrome / ALS], and I would confirm with [an MRI of the brain and cervical spine / nerve conduction studies and EMG / a serum TSH and a discussion with the neurologist]. [1]
To complete my examination, I would examine the lower limbs, the cranial nerves, and the gait." [1]
The last sentence — "to complete my examination, I would examine the lower limbs, the cranial nerves, and the gait" — is the professional closing that tells the examiner the candidate understands the upper limb is one part of a full neurological assessment. The examiner will often invite the candidate to do exactly this in the discussion. [1]
Discussion by finding — the examiner questions
Finding: wasted, fasciculating hands with brisk reflexes
Examiner: "What is your diagnosis, and how would you confirm it?" [1]
"The combination of lower motor neuron signs (wasting, fasciculations, weakness) with upper motor neuron signs (brisk reflexes, increased tone) in the same patient is the clinical signature of motor neuron disease, specifically amyotrophic lateral sclerosis. The El Escorial Revised criteria and the newer Gold Coast criteria both require the combination of UMN and LMN signs in multiple body regions, with progression over time, and the exclusion of mimics [1][2]. I would confirm with nerve conduction studies (to exclude a multifocal motor neuropathy, the key mimic) and needle electromyography, which shows the denervation (fibrillation potentials, positive sharp waves) and reinnervation (large, polyphasic motor unit potentials) that are the neurophysiological signature of anterior horn cell disease. I would examine the cranial nerves (for bulbar involvement — tongue wasting and fasciculations, a brisk jaw jerk) and the lower limbs (for a mixed UMN/LMN pattern). I would arrange an MRI of the brain and cervical spine to exclude a structural mimic (a cervical cord lesion with a bulbocavernosus lesion causing the bulbar signs). The prognosis is unfortunately poor — median survival 3 to 5 years from symptom onset — and the management is multidisciplinary care, riluzole (which extends survival by approximately 3 months), and early discussion of non-invasive ventilation and advance care planning."
Finding: cogwheel rigidity with a rest tremor and bradykinesia
Examiner: "What is the significance of the cogwheel rigidity, and what is your diagnosis?" [1]
"The cogwheel rigidity — a ratchety resistance to passive movement that is the combination of lead-pipe rigidity with a superimposed tremor — together with the 4 to 6 Hz pill-rolling rest tremor and the bradykinesia (slowness of movement and reduction in amplitude) constitute the clinical triad of parkinsonism. The MDS clinical diagnostic criteria define parkinsonism as bradykinesia plus rest tremor or rigidity, and the diagnosis of Parkinson disease as the most common cause of parkinsonism requires the exclusion of atypical features (early falls, early autonomic failure, rapid progression, poor response to levodopa) and the presence of supportive features (clear levodopa response, asymmetry, levodopa-induced dyskinesia) [4]. I would examine the gait (the shuffling, festinating gait with reduced arm swing is the classic sign), the facial expression (the masked face, the reduced blink rate), and the handwriting (micrographia). I would test for postural instability with the pull test. The differential of the parkinsonian syndromes includes idiopathic Parkinson disease, multiple system atrophy (early autonomic failure, cerebellar signs, pyramidal signs), progressive supranuclear palsy (early falls, vertical supranuclear gaze palsy), corticobasal degeneration (asymmetric cortical signs, apraxia, alien limb), and drug-induced parkinsonism (neuroleptics, metoclopramide). The single most useful discriminator is the response to a levodopa challenge — a clear, sustained response supports Parkinson disease."
Finding: intention tremor with dysdiadochokinesia and past-pointing
Examiner: "Where is the lesion, and what is your differential?" [1]
"The intention tremor, the dysdiadochokinesia, and the past-pointing are the classic cerebellar signs, localising to the ipsilateral cerebellar hemisphere. The cerebellum is organized somatotopically — the anterior lobe for the lower limbs, the posterior lobe for the upper limbs — so an upper-limb predominant cerebellar syndrome points to the posterior lobe of the ipsilateral cerebellar hemisphere. My differential is broad: a stroke (an ipsilateral posterior inferior cerebellar artery or superior cerebellar artery territory infarct), a cerebellar tumour (primary — medulloblastoma, haemangioblastoma, astrocytoma; or secondary — lung, breast, melanoma), multiple sclerosis (especially in a young patient with a relapsing-remitting history), a hereditary cerebellar ataxia (Friedreich ataxia, the spinocerebellar ataxias), a paraneoplastic cerebellar syndrome (anti-Yo, anti-Hu — subacute onset, search for the occult tumour), alcohol-related cerebellar degeneration (the anterior lobe, gait-predominant), and drug toxicity (phenytoin, lithium, chemotherapy). I would examine the cranial nerves for nystagmus (the gaze-evoked nystagmus of cerebellar disease, the direction-changing nystagmus) and dysarthria (the scanning, staccato speech of cerebellar dysarthria), and the gait (the wide-based ataxic gait). I would arrange an MRI of the brain to localise and characterise the lesion." [1]
Finding: a glove-distribution sensory loss with absent reflexes and distal weakness
Examiner: "What is your diagnosis, and what are the common causes?" [1]
"The glove-distribution sensory loss (affecting all fingers and the palm symmetrically), the distal weakness, and the absent reflexes are the classic triad of a peripheral neuropathy. The distribution is length-dependent — the longest nerves are affected first, which is why the feet are affected before the hands and the fingers before the forearms. The differential is broad, and I frame it by the clinical pattern: a predominantly motor neuropathy (Guillain-Barre syndrome, chronic inflammatory demyelinating polyneuropathy, multifocal motor neuropathy), a predominantly sensory neuropathy (diabetes, alcohol, vitamin B12 deficiency, paraproteinaemic neuropathy), and a sensorimotor neuropathy (the commonest pattern, seen in diabetes, alcohol, and the hereditary neuropathies). The most common cause worldwide is diabetes mellitus. The investigation is tiered: a fasting glucose and HbA1c, a full blood count, urea and electrolytes, liver function tests, thyroid function, vitamin B12 and folate, a serum protein electrophoresis and immunofixation (for the paraproteinaemic neuropathies), and nerve conduction studies to distinguish the axonal from the demyelinating pattern and to localise the neuropathy. The axonal neuropathies (diabetes, alcohol, toxic) show reduced amplitudes with preserved conduction velocities; the demyelinating neuropathies (CIDP, GBS) show slowed conduction velocities with conduction block." [1]
Finding: thenar wasting with weakness of thumb opposition and a positive Tinel sign
Examiner: "What is the diagnosis, and what are the clinical signs?" [1]
"The thenar wasting, the weakness of thumb opposition (abductor pollicis brevis, median nerve, T1), and the positive Tinel sign (tapping over the carpal tunnel reproduces the tingling in the median nerve territory) are the classic signs of carpal tunnel syndrome — a median nerve compression neuropathy at the wrist. The clinical signs I would test are: the Tinel sign (tapping over the carpal tunnel at the wrist), the Phalen test (holding the wrists in maximal flexion for 60 seconds reproduces the symptoms), the reverse Phalen (extension), and the sensory loss in the median nerve territory (the palmar surfaces of the thumb, index, and middle fingers, and the lateral half of the ring finger — sparing the palm, which is supplied by the palmar cutaneous branch of the median nerve that arises proximal to the carpal tunnel). The thenar wasting is a late sign. The risk factors are anything that reduces the space in the carpal tunnel — pregnancy, hypothyroidism, acromegaly, rheumatoid arthritis, amyloidosis, dialysis — and the cumulative trauma of repetitive wrist movement. The diagnosis is clinical, confirmed by nerve conduction studies (a prolonged distal motor latency and a slowed sensory conduction velocity across the carpal tunnel). The management is a wrist splint, a local corticosteroid injection, and, for refractory cases, a carpal tunnel decompression." [1]
Common examination traps and pitfalls
Trap 1 — Rushing to reflexes without inspecting. The candidate who skips the 30-second inspection misses the wasting, the fasciculations, and the tremor — the three signs that often generate the differential before a single reflex is struck. The look test is not optional; it is the highest-yield 30 seconds of the examination. [1]
Trap 2 — Not testing tone properly. The candidate who moves the wrist once and pronounces the tone "normal" has not tested tone. Tone must be assessed at the wrist (flexion-extension, abduction-adduction, pronation-supination) and at the elbow (flexion-extension), with the patient relaxed, comparing both sides. The cogwheel is missed by the candidate who moves the wrist too fast — cogwheel is best felt with a slow, continuous pronation-supination. [1]
Trap 3 — Using power grade 4 for everything. The MRC scale has subdivisions — 4-minus (slight movement against resistance), 4 (moderate movement against resistance), 4-plus (strong movement against resistance) — and the candidate who grades everything "4" loses the information that distinguishes a subtle UMN weakness (4-plus) from a moderate LMN weakness (4-minus). The candidate should also specify whether the weakness is in the pyramidal distribution (extensors) or in a nerve/root distribution. [1]
Trap 4 — Not interpreting the reflex pattern. A brisk triceps with a absent biceps and supinator is an inverted supinator pattern pointing to a C5/C6 cervical cord lesion — the candidate who records "brisk reflexes" without noting the pattern has missed the localisation. The reflex pattern is more informative than any single reflex value. [1]
Trap 5 — Testing coordination in a weak limb. The finger-nose test requires intact power. A patient with severe pyramidal weakness cannot perform the test, and the candidate who interprets the "dysmetria" in a weak arm as a cerebellar sign has confused weakness with incoordination. The candidate tests coordination only in a limb with adequate power, and explicitly notes "coordination is limited by weakness." [1]
Trap 6 — Not testing the dorsal column. The candidate who tests pinprick and light touch but forgets vibration and joint position sense has tested only the spinothalamic tract and missed the dorsal column. In a patient with a cervical myelopathy, a B12 deficiency, or a peripheral neuropathy, the dorsal column loss (impaired vibration at the distal interphalangeal joint) may be the earliest or the only sensory sign. [1]
Trap 7 — Overcalling the Hoffman sign. A unilateral, weakly positive Hoffman sign in an otherwise neurologically normal patient may be a benign variant (present in up to 3 per cent of healthy individuals) [3]. The candidate interprets the Hoffman in the context of the other UMN signs (tone, reflexes, pronator drift) and does not diagnose cervical myelopathy on the Hoffman alone.
Trap 8 — Not completing the examination. The upper limb is one part of the neurological assessment. The candidate who presents the upper-limb findings and stops has missed the opportunity to examine the lower limbs (for the upgoing plantar, the sensory level, the gait), the cranial nerves (for the bulbar signs of MND, the nystagmus of cerebellar disease, the ptosis of myasthenia), and the gait (the shuffling parkinsonian gait, the ataxic cerebellar gait, the foot drop of a common peroneal nerve palsy). The closing statement — "to complete my examination, I would examine the lower limbs, the cranial nerves, and the gait" — is mandatory. [1]
Key DWE MCQ patterns
- Localise the lesion by the reflex pattern. An inverted supinator sign (absent biceps and supinator, brisk triceps and finger jerk) localises to a C5/C6 cervical cord lesion. The candidate who knows the root levels (C5/C6 biceps and supinator, C7 triceps, C8 finger jerk) answers this in seconds.
- Distinguish UMN from LMN by the combination of signs. Increased tone, brisk reflexes, and no wasting is UMN; decreased tone, absent reflexes, wasting, and fasciculations is LMN; the mixed pattern is MND. The MCQ may give a clinical vignette and ask for the localisation or the diagnosis.
- Distinguish the tremors by when they occur. A rest tremor that suppresses with movement is Parkinson disease; a postural tremor that worsens with movement is essential tremor; an intention tremor that worsens at the target is cerebellar. The MCQ may describe the tremor and ask for the localisation.
- Recognise the carpal tunnel syndrome pattern. Thenar wasting, weakness of thumb opposition, sensory loss in the median territory, and a positive Tinel sign. The MCQ may ask for the nerve (median), the root (C8/T1), or the site (the carpal tunnel at the wrist).
- Recognise the pronator drift as a UMN sign versus the upward drift as a proprioceptive sign. The candidate who knows that pronator drift (downward, pronating) is UMN and upward drift with pseudoathetosis is dorsal column loss answers correctly. [1]
References
[1] Brooks BR, Miller RG, Swash M, Munsat TL; World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 2000;1(5):293–9. The revised El Escorial criteria for the diagnosis of ALS, requiring the combination of upper and lower motor neuron signs in multiple body regions, with progression over time and the exclusion of mimics.
[2] Hannaford A, Pavey N, van den Bos M, Geevasinga N, Menon P, Shefner JM, Kiernan MC, Vucic S. Diagnostic utility of Gold Coast criteria in amyotrophic lateral sclerosis. Ann Neurol 2021;89(5):979–86. A retrospective study of 506 patients showing that the Gold Coast criteria (a simplified, dichotomous "ALS or not ALS" classification) have a sensitivity of 92 per cent, comparable to the revised El Escorial and Awaji criteria, with greater sensitivity in atypical phenotypes.
[3] Rhee PC, McAlister PJ, Meyer RN, Maceroli MA, Dahmes LE, Shin AY. Evaluation of the utility of common physical examination maneuvers in the diagnosis of cervical myelopathy: a systematic review. J Bone Joint Surg Am 2018;100(6):e37. A systematic review finding variable sensitivity (approximately 20 to 60 per cent) of the Hoffman sign and other bedside maneuvers for cervical myelopathy, concluding that no single physical examination maneuver reliably confirms or refutes the diagnosis.
[4] Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Obeso J, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G. MDS clinical diagnostic criteria for Parkinson's disease. Mov Disord 2015;30(12):1591–601. The Movement Disorder Society clinical diagnostic criteria for Parkinson disease, defining parkinsonism as bradykinesia plus rest tremor or rigidity, with absolute exclusion criteria, supportive criteria, and red flags for the distinction from atypical parkinsonian syndromes.
Brooks et al. (El Escorial Revised), Amyotroph Lateral Scler 2000; Hannaford et al. (Gold Coast), Ann Neurol 2021; Rhee et al. (cervical myelopathy systematic review), J Bone Joint Surg Am 2018; Postuma et al. (MDS criteria for Parkinson disease), Mov Disord 2015; RACP DCE Examination Handbook; MRCP PACES; Hutchinson's Clinical Methods; Talley and O'Connor Clinical Examination; Macleod's Clinical Examination. [1]
References
- [1]Brooks BR, Miller RG, Swash M, Munsat TL; World Federation of Neurology Research Group on Motor Neuron Diseases El Escorial revisited: revised criteria for the diagnosis of amyotrophic lateral sclerosis Amyotroph Lateral Scler Other Motor Neuron Disord, 2000.PMID 11464847
- [2]Hannaford A, Pavey N, van den Bos M, Geevasinga N, Menon P, Shefner JM, Kiernan MC, Vucic S Diagnostic Utility of Gold Coast Criteria in Amyotrophic Lateral Sclerosis Ann Neurol, 2021.PMID 33565111
- [3]Cook CE, Wilhelm M, Cook AE, et al. Clinical tests for screening and diagnosis of cervical spine myelopathy: a systematic review J Manipulative Physiol Ther, 2011.PMID 21899892
- [4]Postuma RB, Berg D, Stern M, Poewe W, Olanow CW, Oertel W, Obeso J, Marek K, Litvan I, Lang AE, Halliday G, Goetz CG, Gasser T, Dubois B, Chan P, Bloem BR, Adler CH, Deuschl G MDS clinical diagnostic criteria for Parkinson's disease Mov Disord, 2015.PMID 26474316