Phys · general-medicine
Perioperative Medicine — Physician Assessment and Optimisation Before Surgery
Also known as perioperative medicine · preoperative assessment · preoperative cardiac risk · Revised Cardiac Risk Index · Lee index · RCRI · metabolic equivalents · MET capacity · preoperative functional capacity · perioperative diabetes · variable rate intravenous insulin infusion · VRIII · GKI · warfarin bridging · DOAC perioperative management · VTE prophylaxis · Caprini score · Padua score · enhanced recovery after surgery · ERAS · prothrombin complex concentrate · PCC · idarucizumab · andexanet alfa
Consultant-physician-depth guide to perioperative medicine: preoperative cardiac risk stratification (Revised Cardiac Risk Index, MET capacity, stress testing), pulmonary optimisation, perioperative diabetes management (metformin, SGLT2 inhibitors, insulin, variable-rate IV insulin infusion), anticoagulation management and reversal (warfarin bridging, DOACs, PCC, idarucizumab, andexanet alfa), chronic medication management, VTE prophylaxis (Caprini, Padua), postoperative complications, and Enhanced Recovery After Surgery (ERAS). Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Perioperative Medicine — Physician Assessment and Optimisation

The answer first
Perioperative medicine is the physician's job of making a complex patient safe for surgery without over-investigating them. The five questions that decide everything are: [1]
- What is the cardiac risk? Use the Revised Cardiac Risk Index (Lee index) and the patient's functional capacity. Functional testing is reserved for patients with poor or unknown functional capacity who face elevated risk — it is not a routine pre-op test.
- Is the airway and the lung ready? Stop smoking, optimise COPD and asthma, and plan for lung-protective analgesia and early mobilisation.
- How is the diabetes managed? Stop SGLT2 inhibitors three days before; manage metformin, sulfonylureas and insulin by fasting status; use a variable-rate intravenous insulin infusion (VRIII) when the patient is fasting and at risk, and never use a sliding scale.
- What happens to the anticoagulant? Decide for each patient whether to stop, bridge or continue, based on the thrombotic risk of the underlying condition and the bleeding risk of the surgery. Know how to reverse each agent in an emergency.
- What is the venous thromboembolism (VTE) risk, and what prophylaxis? Use Caprini for surgical and Padua for medical patients. The single most preventable cause of perioperative death is a pulmonary embolism that was not prophylaxed. [1]
The recurring trap: treatments that seem protective — starting a beta-blocker, giving aspirin, revascularising a coronary artery purely to "clear" a patient — are harmful or useless when applied routinely. Perioperative medicine rewards restraint, risk stratification, and continuation of drugs that are working. [1]
Preoperative cardiac assessment
The Revised Cardiac Risk Index (Lee index)
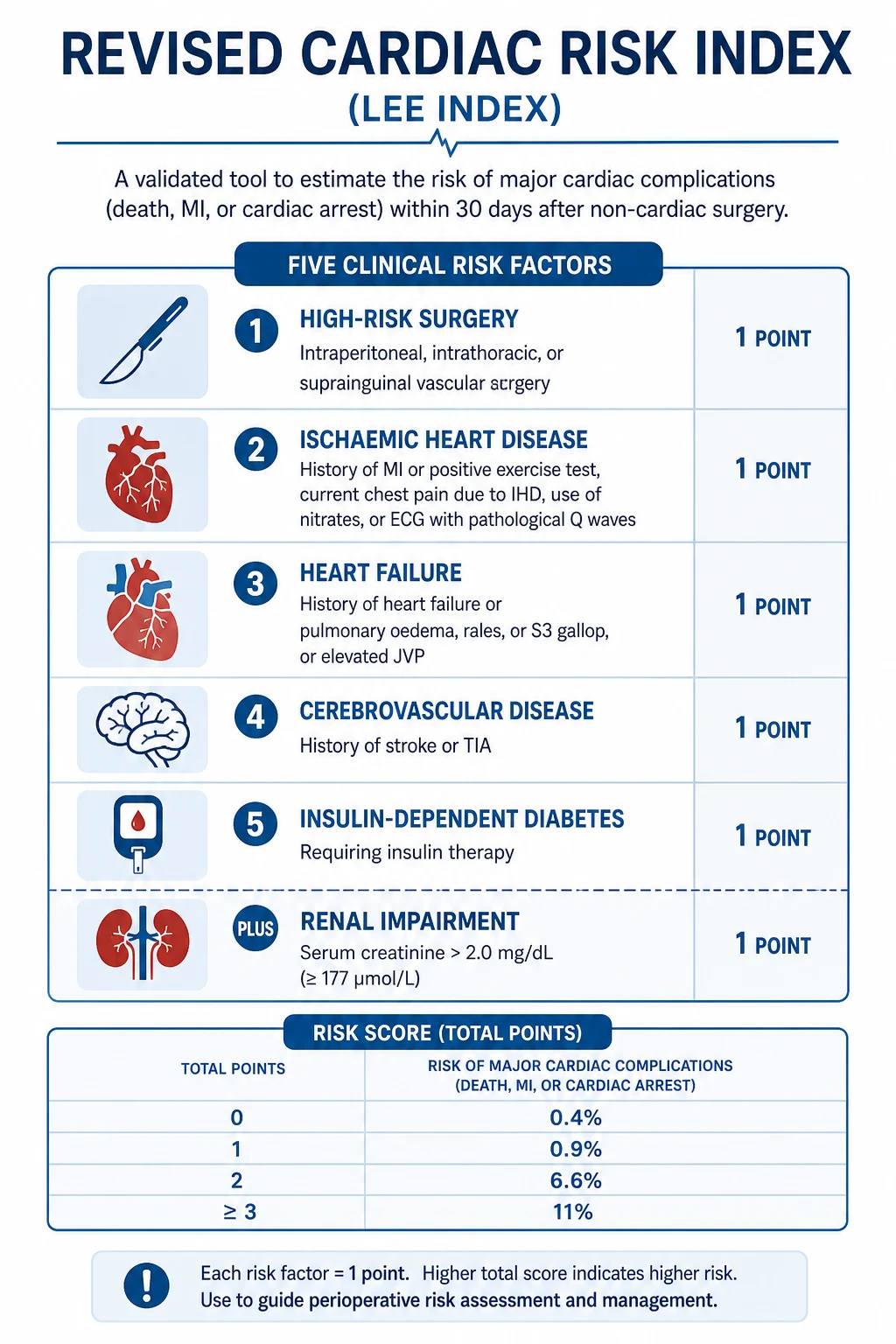
The Revised Cardiac Risk Index (RCRI), derived and validated by Lee and colleagues, is the workhorse of preoperative cardiac risk stratification. It estimates the probability of major cardiac complications — cardiac death, non-fatal myocardial infarction, and non-fatal cardiac arrest — after non-cardiac surgery. The six predictors, each worth one point, are: [1]
- High-risk surgery — intraperitoneal, intrathoracic, or suprainguinal vascular procedures.
- History of ischaemic heart disease — prior MI, positive exercise test, current chest pain due to ischaemia, nitrate therapy, or pathological Q waves on the ECG.
- History of heart failure — or physical examination findings of heart failure.
- History of cerebrovascular disease — prior transient ischaemic attack or stroke.
- Diabetes requiring insulin therapy.
- Preoperative serum creatinine greater than 177 micromoles per litre (2.0 mg/dL). [1]
The risk of a major cardiac event rises with the score: a score of zero carries roughly a 0.4 to 0.5 per cent risk; one or two points, around 1 to 2 per cent; and three or more points, approximately 5 to 6 per cent and sometimes higher in vascular surgery. The RCRI is simple, reproducible, and well calibrated — but it underestimates risk in patients undergoing open aortic and other major vascular surgery, where the NSQIP surgical risk calculator performs better. In practice, most perioperative physicians use the RCRI as the first screen and add functional capacity before deciding on further testing. [1]
Functional capacity — metabolic equivalents
Functional capacity is the patient's ability to perform physical activity, measured in metabolic equivalents (METs). One MET is resting oxygen consumption. Climbing a flight of stairs is roughly 4 METs; strenuous sport such as swimming or singles tennis is more than 10 METs. The discriminator is whether the patient can manage 4 METs — equivalent to walking briskly up two flights of stairs or walking on a slight incline without symptoms. [1]
A patient who can achieve at least 4 METs without chest pain, breathlessness or limiting fatigue has good functional capacity. Their perioperative cardiac risk is low regardless of the RCRI, and further cardiac testing is unlikely to change management. A patient with poor functional capacity — fewer than 4 METs, or unable to tell you (classically the patient who "cannot climb a flight of stairs") — has an independent marker of risk and may benefit from further assessment if the surgical risk is also elevated. [1]
When to order functional testing — and when not to
The cardinal rule of perioperative cardiac testing is restraint. Non-invasive cardiac testing — exercise ECG, dobutamine stress echocardiography, or myocardial perfusion scanning — is reserved for a specific group: patients with elevated clinical risk (RCRI two or more, or a high-risk procedure) AND poor or unknown functional capacity, in whom the result will change management. Order a stress echo or a myocardial perfusion scan in the patient who cannot climb a flight of stairs and is facing an intraperitoneal or vascular procedure. Do not order it for the asymptomatic patient who walks five kilometres daily, no matter what the surgery. [1]
The choice between dobutamine stress echocardiography and myocardial perfusion imaging is partly local availability and partly patient factors — stress echo gives structural and ischaemic information; perfusion scanning is preferred when the echo windows are poor. Both have good negative predictive value but only modest positive predictive value, which is why a positive test is a prompt for coronary angiography only if the patient has independent cardiac indications. [1]
Coronary revascularisation is rarely needed before surgery
The CARP trial (McFalls and colleagues) established that prophylactic coronary revascularisation before elective major vascular surgery does not improve long-term survival or reduce perioperative cardiac events in patients with stable coronary disease. Coronary artery bypass grafting or percutaneous coronary intervention should be performed for the same cardiac indications that would mandate them independent of surgery — an acute coronary syndrome, unstable or severe angina, or ischaemia producing significant left ventricular dysfunction — and not to "clear" a patient for an operation. [1]
There is one procedural caveat the examiner will probe: if a patient has had a coronary stent, the minimum antiplatelet period before elective non-cardiac surgery is two weeks for a bare-metal stent and six months for a drug-eluting stent (recent guidelines allow three to six months for drug-eluting stents in stable patients with low bleeding-risk surgery, but the conservative floor remains six months). Surgery within the minimum stent period carries a high risk of acute stent thrombosis — a frequently fatal event — because the exposed metal is thrombogenic. The pragmatic rule: defer elective surgery until the minimum period has elapsed, so that dual antiplatelet therapy can be safely reduced. [1]
Beta-blockers, statins, aspirin, alpha-2 agonists
Beta-blockers — continue, do not start acutely. A patient already on a beta-blocker for any indication should continue it through surgery. Abrupt perioperative cessation risks rebound tachycardia, hypertension and myocardial ischaemia. The POISE trial (Devereaux and colleagues) settled the question of starting beta-blockers de novo: initiating extended-release metoprolol just before surgery reduced perioperative myocardial infarction but increased all-cause mortality and stroke, driven by perioperative hypotension and bradycardia. The current consensus is that beta-blocker-naive patients should not be started on the morning of surgery; if initiation is considered for a high-risk patient, it should be titrated days to weeks ahead with careful haemodynamic monitoring. [1]
Statins — start or continue for vascular surgery. Statins stabilise coronary plaque and are associated with reduced perioperative cardiac events in vascular surgery, supported by a Cochrane review (Sanders and colleagues). Guidelines recommend starting a statin in all patients undergoing major vascular surgery who are not already on one, and continuing existing statins across all surgery. Atorvastatin 20 to 40 milligrams daily is a reasonable perioperative choice. [1]
Aspirin — continue for stents, otherwise individualise. The POISE-2 trial showed that initiating or continuing aspirin perioperatively in unselected patients did not reduce death or myocardial infarction but increased major bleeding. The exception carved out by guideline interpretation is the patient with a recent coronary stent, in whom aspirin should be continued through surgery unless the bleeding risk is extreme — the catastrophic risk is stent thrombosis. For primary prevention, aspirin is generally held. For secondary prevention without a recent stent, the decision balances thrombotic against bleeding risk and the procedure-specific bleeding profile. [1]
Alpha-2 agonists — do not use for cardiac protection. Clonidine and the related alpha-2 agonists do not reduce perioperative cardiac events and increase clinically important hypotension and bradycardia; they have no routine role in perioperative cardiac risk reduction. [1]
Preoperative pulmonary assessment
Postoperative pulmonary complications — atelectasis, pneumonia, respiratory failure and exacerbation of chronic lung disease — are as common as, and carry similar mortality to, cardiac complications, yet are systematically under-assessed. The physician's contribution is to optimise the lungs before surgery and reduce risk factors after. [1]
Smoking cessation. Stopping smoking reduces postoperative complications, and the earlier the better. Cessation for at least four to eight weeks before elective surgery yields the greatest reduction in pulmonary and wound complications; even a few days improves carbon monoxide clearance and ciliary function. The old teaching that recent cessation paradoxically increases sputum and risk is not supported by modern evidence — encourage every smoker to stop, regardless of the interval to surgery, and offer nicotine replacement therapy and behavioural support. [1]
Optimise chronic airways disease. For COPD and asthma, ensure the patient is on maximal inhaled therapy for their disease severity, check inhaler technique, give a written action plan, and treat any active exacerbation before elective surgery. Optimise COPD to GOLD (Global Initiative for Chronic Obstructive Lung Disease) Group A to D therapy; escalate inhaled corticosteroid, long-acting muscarinic antagonist and long-acting beta-agonist therapy as appropriate; and consider a short course of oral corticosteroids and antibiotics if there is an infective exacerbation. Continue inhaled bronchodilators on the morning of surgery. Measure baseline spirometry only if it will change management — routine preoperative spirometry in asymptomatic patients is not recommended. [1]
Incentive spirometry and chest physiotherapy. Teach deep-breathing exercises, directed coughing, and incentive spirometry before surgery, and continue them postoperatively. Early mobilisation and upright positioning are at least as effective as formal physiotherapy in preventing atelectasis. High-risk patients — those with COPD, obesity, upper abdominal or thoracic surgery, or a long anticipated immobilisation — benefit most. [1]
Reduce risk factors. Aim for a nasogastric tube only when necessary (it predisposes to pneumonia), use lung-protective ventilation intra-operatively, prefer regional or spinal anaesthesia where appropriate, and avoid prolonged sedation postoperatively. [1]
Diabetes management in the perioperative period
The goals are to avoid hypoglycaemia (which is dangerous under anaesthesia because the patient cannot report symptoms), to avoid marked hyperglycaemia (which impairs wound healing and immunity and raises infection risk), and to return the patient to their usual regimen as soon as they are eating. The Joint British Diabetes Societies and the Australian Diabetes Society frame this around the fasting state and the procedure length. [1]
The general framework
- Place the patient first on the morning operating list to minimise fasting.
- Target capillary glucose 6 to 10 mmol/L, accepting 4 to 12 mmol/L as the wider acceptable range.
- Switch to a variable-rate intravenous insulin infusion (VRIII) when the patient is fasting for more than one missed meal or has poorly controlled diabetes (HbA1c above 69 mmol/mol, or 8.5 per cent), or is undergoing major surgery.
- Resume the usual oral therapy or subcutaneous insulin once the patient is eating and drinking normally. [1]
Drug-by-drug management
Metformin. Continue metformin up to and including the morning of surgery if the patient is having minor surgery with a short fasting period and has normal or near-normal renal function (eGFR above 60). If the eGFR is reduced or the procedure involves contrast or carries a renal-impairment risk, hold metformin at the time of surgery and restart when renal function is stable and the patient is eating — typically 24 to 48 hours. The historical fear of metformin-associated lactic acidosis is largely overstated in stable patients, but it is real during acute kidney injury, sepsis or hypoperfusion, so the conservative rule in any acutely unwell or renally stressed patient is to hold it. [1]
SGLT2 inhibitors (dapagliflozin, empagliflozin). Stop these three days before elective surgery (the conservative recommendation, reflecting drug pharmacokinetics and fasting). The danger is euglycaemic diabetic ketoacidosis, which is precipitated by the combination of SGLT2 inhibitor, fasting, surgical stress, dehydration and relative insulin deficiency — and which is frequently missed because the glucose may be only mildly elevated. The patient can resume the SGLT2 inhibitor once they are eating and drinking normally and clinically stable. [1]
Sulfonylureas. Hold gliclazide and most sulfonylureas on the morning of surgery because of hypoglycaemia risk during fasting. Glibenclamide (glyburide) carries a particularly high hypoglycaemia risk in older patients and in renal impairment — avoid it perioperatively and consider an alternative. [1]
Insulin — basal-bolus regimens. The standard approach for a patient on a once-daily long-acting (basal) insulin plus rapid-acting meal-time boluses: continue the basal insulin at 75 to 100 per cent of the usual dose on the night before and the morning of surgery (a small reduction prevents hypoglycaemia during fasting), and omit the meal-time bolus while fasting. For a twice-daily biphasic (premixed) insulin, give one-third to one-half of the usual morning dose on the day of surgery. [1]
The variable-rate intravenous insulin infusion (VRIII). The VRIII — formerly and still colloquially called the GKI (glucose–potassium–insulin) infusion — is the standard method for glycaemic control in fasting surgical patients with diabetes who need insulin. It is a separate insulin infusion run alongside a glucose-containing substrate fluid (for example 10 per cent glucose with added potassium and a fixed rate), titrated against hourly capillary glucose using a standard sliding-scale table. It is NOT a "sliding-scale" in the obsolete sense (see below). The VRIII is continued until the patient is eating and their usual subcutaneous insulin has been re-established, with an overlap of the subcutaneous dose and the infusion to prevent rebound hyperglycaemia. [1]
Sliding-scale insulin is obsolete. The traditional "sliding scale" — reactive boluses of short-acting insulin prescribed against a capillary glucose reading, with no basal insulin — is obsolete and dangerous. It produces erratic control, swings between hyper- and hypoglycaemia, and no background basal cover. Modern perioperative diabetes care uses the VRIII with a substrate infusion and a titrated algorithm, or continuation of the patient's own basal insulin. The phrase to avoid in the exam and at the bedside is "sliding scale"; the phrase to use is "variable-rate intravenous insulin infusion." [1]
Why glycaemic targets matter
Perioperative hyperglycaemia impairs neutrophil function, increases surgical-site infection, and slows wound healing. Hypoglycaemia under general anaesthesia or sedation is silent and can cause neurological harm or cardiac ischaemia. The 6 to 10 mmol/L target reflects a pragmatic balance — tight control (4 to 6 mmol/L) increases hypoglycaemia and has not improved outcomes in the perioperative setting, while permitting uncontrolled hyperglycaemia raises infection rates. [1]
Anticoagulation management
The physician's perioperative anticoagulation task is a balance between two opposing risks: thrombosis if the anticoagulant is stopped, and bleeding if it is continued. The decision is driven by the thrombotic risk of the underlying condition, the bleeding risk of the procedure, and the pharmacokinetics of the agent. The aim is to minimise the time off anticoagulation without exposing the patient to uncontrolled bleeding. [1]
Warfarin
Warfarin is stopped approximately five days before surgery to allow the INR to normalise (its half-life is 36 to 42 hours). Whether to bridge with a fast-acting agent such as low-molecular-weight heparin (LMWH) depends on the annual thrombotic risk of the indication: [1]
- High thrombotic risk — bridge. A mechanical mitral valve, a recent (within three months) venous thromboembolism, a bileaflet mechanical aortic valve with additional risk factors, atrial fibrillation with rheumatic heart disease or a prior stroke, or severe thrombophilia. Stop warfarin five days before, start therapeutic-dose LMWH three days before, give the last LMWH dose 24 hours before surgery, and restart LMWH 24 to 48 hours after surgery once haemostasis is secure. Warfarin is restarted on the evening of surgery or the next day, and LMWH is continued until the INR is again therapeutic.
- Low or moderate thrombotic risk — do not bridge. Bileaflet mechanical aortic valve without other risk factors, atrial fibrillation without high-risk features, or a remote (more than three months ago) VTE. The BRIDGE trial showed that for atrial fibrillation, withholding bridging was non-inferior to bridging for arterial thromboembolism and caused significantly less major bleeding. Most atrial fibrillation patients having minor or low-bleeding-risk surgery do not need bridging. [1]
The high-yield exam trap is the mechanical mitral valve — this is the patient who must always be bridged, because the annual thrombotic risk of an untreated mechanical mitral valve is the highest of any indication and a valve thrombosis is usually fatal. [1]
Direct oral anticoagulants (DOACs)
DOACs (dabigatran — a direct thrombin inhibitor; apixaban and rivaroxaban — anti-Xa inhibitors) have a shorter offset and onset than warfarin and do not require bridging, because they reach full anticoagulant effect within hours of a dose. The standard approach is to stop the DOAC 24 to 48 hours before surgery. The exact interval depends on the drug, the renal function (renal impairment prolongs DOAC clearance, especially for dabigatran which is largely renally cleared), and the bleeding risk of the procedure: [1]
- Standard bleeding-risk surgery (most surgery): stop apixaban or rivaroxaban 48 hours before (two missed doses), and dabigatran 48 hours before if the creatinine clearance is at least 80, extending to 72 to 96 hours if the CrCl is below 50.
- Minimal bleeding-risk surgery (cataract surgery, some endoscopy without biopsy): the DOAC may be continued or held for one dose.
- Major bleeding-risk surgery (cardiac, neurosurgery, major cancer): extend the stop to 48 hours for apixaban and rivaroxaban and to 48 to 96 hours for dabigatran depending on renal function. [1]
Restart the DOAC once haemostasis is secure, typically 24 hours after minor surgery and 48 to 72 hours after major surgery. No routine DOAC-level testing is needed before surgery; if there is uncertainty about residual anticoagulant effect, a normal thrombin time effectively excludes clinically significant dabigatran, and a normal anti-Xa level effectively excludes apixaban or rivaroxaban — but in practice most decisions are made on timing and renal function alone. [1]
Antiplatelet agents and coronary stents
Aspirin is continued in patients with coronary stents unless the bleeding risk is extreme (intracranial surgery, posterior-chamber eye surgery, prostate surgery). Dual antiplatelet therapy — aspirin plus a P2Y12 inhibitor (clopidogrel, ticagrelor) — must not be stopped within the minimum stent period (two weeks bare-metal, three to six months drug-eluting) without cardiology advice, because stent thrombosis carries a mortality approaching 30 to 50 per cent. If surgery cannot be deferred, continue aspirin and stop the P2Y12 inhibitor for the shortest possible period. [1]

Anticoagulation reversal
When a patient on an anticoagulant presents with life-threatening bleeding, reversal must be agent-specific and immediate. The general principle is to stop the anticoagulant, give the specific antidote or non-specific factor replacement, and treat the source of bleeding surgically or endoscopically. [1]
Warfarin. For life-threatening bleeding, give 4-factor prothrombin complex concentrate (4F-PCC) plus intravenous vitamin K 5 to 10 milligrams. The PCC reverses the INR within minutes by replacing factors II, VII, IX and X; the vitamin K takes 6 to 12 hours to enable hepatic synthesis of new factors and so sustains the reversal. PCC is preferred over fresh frozen plasma because it is faster, requires a smaller volume (avoiding transfusion-related circulatory overload), and was shown by Sarode and colleagues to be non-inferior to plasma for haemostasis and superior for rapid INR correction. For a non-bleeding patient with a high INR before a procedure, oral low-dose vitamin K (1 to 2.5 milligrams) is sufficient. [1]
Dabigatran. Reverse with idarucizumab 5 grams intravenously (two 2.5-gram boluses). Idarucizumab is a humanised monoclonal antibody fragment that binds dabigatran with very high affinity and neutralises its activity within minutes, as demonstrated by Pollack and colleagues. It is the treatment of choice for life-threatening dabigatran-related bleeding or before emergency surgery. [1]
Apixaban and rivaroxaban (anti-Xa inhibitors). Reverse with andexanet alfa — a recombinant modified factor Xa decoy protein that binds and sequesters the inhibitor — given as a bolus then an infusion, as studied in the ANNEXA-4 trial by Connolly and colleagues. Where andexanet is unavailable, 4F-PCC at a dose of 25 to 50 units per kilogram is a reasonable alternative that restores haemostasis without fully reversing the anti-Xa activity. [1]
Heparins. Unfractionated heparin is reversed with protamine sulphate (1 milligram per 100 units of heparin, given in the preceding two hours). LMWH is partially reversed by protamine (about 60 per cent neutralisation). Fondaparinux is not reversed by protamine; recombinant factor VIIa has been used in life-threatening bleeding. [1]
The single most dangerous error is reversing warfarin with vitamin K alone in a patient who is actively bleeding — it is too slow, and the patient continues to haemorrhage while waiting for hepatic synthesis. Always give PCC plus vitamin K for major bleeding, and vitamin K alone only for non-urgent reversal. [1]
Chronic medications in the perioperative period
A practical rule for the patient's regular medications: continue almost everything, with a small number of specific exceptions. Stopping long-term drugs abruptly causes more harm than continuation in the great majority of cases. [1]
ACE inhibitors and angiotensin receptor blockers. This is the one genuinely contested area. ACEi and ARBs are associated with intra-operative and early postoperative hypotension, because they block the renin–angiotensin vasoconstrictor response to anaesthesia-induced vasodilation. Many units stop the ACEi or ARB on the morning of surgery to reduce this risk; others continue it, particularly for heart failure, arguing that the evidence is inconsistent and that stopping risks a hypertensive rebound. The pragmatic position for the exam: stop the morning dose for major surgery where significant haemodynamic shifts are expected, and continue it for minor surgery and in heart failure; restart as soon as the patient is haemodynamically stable. Never stop an ACEi or ARB permanently — resume it on day one or two postoperatively once blood pressure and renal function are stable. [1]
Diuretics. Hold loop diuretics on the morning of surgery if the patient is fasting, to avoid intra-operative hypovolaemia and electrolyte disturbance; restart once the patient is stable and taking oral fluids. [1]
Beta-blockers. Continue — as discussed above, do not stop abruptly. [1]
Statins. Continue — and start for vascular surgery. [1]
Corticosteroids. Continue, and give a stress dose to patients on long-term steroids (the equivalent of prednisolone 5 milligrams or more daily for more than three weeks) who face major surgery, because their hypothalamic–pituitary–adrenal axis is suppressed and cannot mount the cortisol response to surgical stress. A typical regimen is intravenous hydrocortisone 100 milligrams at induction, then 50 milligrams every eight hours for 24 to 48 hours, tapering to the patient's usual oral dose. Patients taking less than 5 milligrams of prednisolone, or who have stopped steroids more than three months previously, do not need stress-dose cover. [1]
Thyroxine. Continue — it has a long half-life (about seven days) and a missed dose is irrelevant, but continuation maintains euthyroidism. For a patient who is nil by mouth and hypothyroid, intravenous levothyroxine (about 70 to 80 per cent of the oral dose) is substituted. [1]
Anti-epileptic drugs. Continue — seizures in the perioperative period are dangerous and the patient may be fasting. Give the usual doses, using intravenous formulations (intravenous levetiracetam, valproate, phenytoin) if the patient cannot take oral medications. [1]
Parkinson medications (levodopa). Continue — levodopa has a short half-life and withdrawal risks neuroleptic-malignant-syndrome-like parkinsonism hyperpyrexia and severe rigidity that can compromise the airway. Time the surgery for first on the list, give the morning dose, and use a nasogastric tube for missed doses if needed. [1]
Opioids and chronic pain medications. Continue to avoid withdrawal and uncontrolled pain; convert oral to intravenous or transdermal equivalents if the patient is fasting. [1]
Contraceptive pill and hormone replacement. Combined oral contraceptives carry a small VTE risk and many units stop them four weeks before major surgery; the absolute risk is low and the decision is individualised, particularly as unintended pregnancy carries its own risks. [1]
Venous thromboembolism prophylaxis
VTE — deep vein thrombosis and pulmonary embolism — remains the commonest preventable cause of perioperative death. Every surgical and immobilised medical patient should have a formal VTE risk assessment and a documented prophylaxis plan, recorded against a validated risk score. [1]
Risk stratification — Caprini and Padua
The Caprini score stratifies VTE risk in surgical patients, summing weighted risk factors (age, body mass index, cancer, prior VTE, major surgery, and many others) into low, moderate, high and very high risk categories, each guiding the intensity of prophylaxis. The Padua Prediction Score (Barbar and colleagues), developed and validated in hospitalised medical patients, uses 11 weighted factors — active cancer, previous VTE, reduced mobility, known thrombophilia, and others — with a score of 4 or more defining a high-risk patient for whom pharmacological prophylaxis is recommended. [1]
| Risk tool | Population | High-risk threshold | Action |
|---|---|---|---|
| Caprini | Surgical | Score greater than 5 (or 3 to 4 with additional factors) | Pharmacological prophylaxis; add mechanical if bleeding risk high |
| Padua | Medical inpatient | Score 4 or more | Pharmacological prophylaxis (LMWH or fondaparinux) |
| Rogers (Venous Thromboembolism Outcome Study) | Surgical alternative | Score-dependent | Use where Caprini not preferred |
Pharmacological prophylaxis
Low-molecular-weight heparin (LMWH). The standard pharmacological agent — enoxaparin 40 milligrams subcutaneously daily (or 20 milligrams daily in renal impairment) for most surgical and medical patients. LMWH is preferred over unfractionated heparin for once-daily dosing, lower rates of heparin-induced thrombocytopenia, and more predictable pharmacokinetics, and is the basis of most modern prophylaxis guidelines (Gould and colleagues, ACCP 9th edition). [1]
Fondaparinux. A synthetic pentasaccharide anti-Xa inhibitor given as 2.5 milligrams subcutaneously daily. It has a lower risk of heparin-induced thrombocytopenia than LMWH and is an alternative in patients with HIT or at high HIT risk. It is renally cleared and contraindicated in severe renal impairment (CrCl below 30). [1]
Direct oral anticoconagulants. Low-dose apixaban, rivaroxaban or dabigatran are approved for VTE prophylaxis after hip and knee replacement; their role in general surgical and medical prophylaxis is narrower than LMWH. [1]
Mechanical prophylaxis
Graduated compression stockings and intermittent pneumatic compression reduce VTE by enhancing venous return and fibrinolysis. Mechanical prophylaxis is the choice when pharmacological prophylaxis is contraindicated by active or very high bleeding risk (neurosurgery, active haemorrhage, severe thrombocytopenia), and is added to pharmacological prophylaxis in the highest-risk patients. Contraindications to mechanical prophylaxis include severe peripheral arterial disease and acute leg ischaemia — apply stockings only after assessing the arterial circulation. [1]
Timing of the first dose
The first prophylactic dose is timed against the bleeding risk. For general surgery, LMWH is given 6 to 12 hours postoperatively once haemostasis is secure, rather than pre-operatively, balancing efficacy against bleeding. For hip and knee replacement surgery, by contrast, the dose may be given before or immediately after surgery as per the specific drug protocol. Continuation of prophylaxis for the full hospital stay, and for up to four weeks after major orthopaedic or cancer surgery, reduces late VTE. [1]
Postoperative complications
The physician reviewing a patient after surgery should screen systematically for the common and dangerous complications: [1]
Atelectasis. The commonest pulmonary complication — collapse of dependent lung segments from hypoventilation, splinting from pain, and supine positioning. Presents with basal crackles, reduced air entry, and mild hypoxia within 24 to 48 hours of surgery. Treat with incentive spirometry, deep breathing, early mobilisation, and adequate analgesia to permit coughing. Prevent with the same measures plus avoidance of prolonged sedation. [1]
Pneumonia. Suspect with new or worsening fever, purulent sputum, focal consolidation, and rising inflammatory markers, typically two to five days postoperatively. Aspiration risk is high after impaired swallowing, prolonged intubation, or ileus. Treat with physiotherapy, oxygen, and antibiotics guided by local protocols and culture; the at-risk organisms include Streptococcus pneumoniae and Haemophilus in the early period, and enteric gram-negatives and Staphylococcus aureus in nosocomial or aspiration pneumonia. [1]
Venous thromboembolism — DVT and PE. Presents with unilateral leg swelling, pain and tenderness (DVT) or pleuritic chest pain, dyspnoea, tachycardia, syncope or hypotension (PE). The diagnosis is confirmed by compression ultrasonography for DVT and CT pulmonary angiography for PE, with a D-dimer of limited use in the high-risk postoperative setting because it is almost always elevated. Prevent with prophylaxis as above; treat confirmed VTE with therapeutic anticoagulation, respecting the timing after surgery. [1]
Delirium. Acute fluctuating disturbance of attention and cognition, commonest in older patients and after major surgery, hip fracture, and cardiac surgery. Screen with the Confusion Assessment Method (CAM) or 4AT. The cause is almost always multifactorial — infection, hypoxia, metabolic disturbance, drugs (especially anticholinergics and opioids), pain, urinary catheterisation, constipation, sleep deprivation, and environmental disruption. Manage by treating the precipitant, stopping deliriogenic drugs, reorientation, sensory re-enablement (glasses, hearing aids), early mobilisation, and family involvement. Reserve low-dose antipsychotics for severe distress or danger. [1]
Acute kidney injury. Common after major surgery, with causes that fall into pre-renal (hypovolaemia, hypotension, the triple-whammy of ACEi + diuretic + NSAID), intrinsic (nephrotoxins — contrast, aminoglycosides, NSAIDs), and post-renal (urinary retention, especially after pelvic surgery in older men). Screen with daily creatinine and urine output; stage by KDIGO criteria; manage by correcting volume status, stopping nephrotoxins, treating the cause, and supporting renal function — with renal replacement therapy reserved for the standard indications. [1]
Surgical-site infection. Presents with increasing pain, erythema, purulent discharge, and systemic signs at the wound, typically five days or more after surgery. Risk factors include diabetes with poor glycaemic control, obesity, smoking, immunosuppression, prolonged surgery, and inadequate antibiotic prophylaxis. Prevent with appropriate surgical antibiotic prophylaxis within 60 minutes of incision, glycaemic control, normothermia, and meticulous technique; treat with antibiotics guided by culture and source control. [1]
Enhanced Recovery After Surgery (ERAS)
Enhanced Recovery After Surgery, or ERAS, is a multimodal, evidence-based perioperative care pathway that reduces complications, shortens hospital stay, and accelerates recovery by counteracting the surgical stress response. The ERAS Society has codified protocols for colorectal, hepatic, pancreatic, urologic, gynaecologic and many other surgical domains; the shared principles apply broadly (Ljungqvist and colleagues). [1]
The core ERAS elements are: [1]
- Preoperative counselling and optimisation — set expectations, optimise nutrition, stop smoking, and manage comorbidities before admission.
- Avoidance of prolonged fasting — allow clear fluids up to two hours and a light meal up to six hours before surgery, and give a carbohydrate drink pre-operatively to reduce insulin resistance and the catabolic response.
- No routine bowel preparation for colonic surgery (or a minimal preparation), because traditional full bowel preparation dehydrates the patient and harms the gut.
- Goal-directed fluid management — neither restrict fluid to dehydration nor overload; use cardiac output monitoring where appropriate to titrate fluid and maintain perfusion.
- Minimally invasive surgery where feasible — laparoscopic or robotic approaches reduce the stress response and pain.
- Multimodal, opioid-sparing analgesia — regional techniques (epidural, transversus abdominis plane block, local infiltration), paracetamol, and non-steroidals or their alternatives, minimising opioid use to reduce nausea, ileus, sedation and delirium.
- Early mobilisation — get the patient out of bed and walking on day zero or one, to prevent DVT, pneumonia, deconditioning and delirium.
- Early enteral nutrition — feed within 24 hours, ideally the same day, to maintain gut integrity and reduce infection.
- Avoidance of drains and tubes — minimise nasogastric tubes (which predispose to pneumonia) and drains (which impede mobilisation) unless specifically indicated.
- Audit of compliance and outcomes — ERAS works only when the bundle is delivered reliably, and outcomes improve with adherence. [1]
The physician's role in ERAS is to ensure medical comorbidities are optimised before admission, to support fluid and glycaemic management, to manage postoperative medical complications early, and to champion the culture of early mobilisation and feeding. [1]

Perioperative anaemia and iron optimisation
Preoperative anaemia is one of the few modifiable risk factors that the physician can correct before elective surgery, and it is common — present in up to a third of patients undergoing major surgery, and higher still in cancer and inflammatory bowel disease. Untreated anaemia increases the need for perioperative transfusion, and transfusion itself is associated with infection, longer hospital stay and, in some populations, mortality. The two-step approach is to find the cause and to treat it with time to work. [1]
Identify the cause. Send a full blood count, ferritin, transferrin saturation, B12, folate, and a reticulocyte count. The common patterns are iron deficiency (low ferritin, low transferrin saturation) — almost always due to blood loss or malabsorption in the surgical population, and frequently the presenting clue to the gastrointestinal cancer that the surgery is treating; anaemia of chronic disease (normal or raised ferritin, low transferrin saturation); and megaloblastic anaemia from B12 or folate deficiency. [1]
Iron therapy. For iron-deficiency anaemia, oral ferrous sulphate or ferrous fumarate is first-line, but it works slowly (weeks) and is poorly tolerated. Where surgery is within four to six weeks, or where oral iron is not tolerated or not absorbed (as in inflammatory bowel disease or after bariatric surgery), intravenous iron (ferric carboxymaltose or iron polymaltose) is preferred — it reconstitutes iron stores within days to two weeks and is now standard in many preadmission clinics. The exam point: do not rely on transfusion to "top up" a stable iron-deficient patient before elective surgery — transfusion carries risks that iron does not, and should be reserved for symptomatic anaemia or haemodynamic compromise. [1]
Erythropoiesis-stimulating agents. In selected patients — those with chronic kidney disease, or those declining transfusion (for example Jehovah's Witnesses) — erythropoietin with concomitant iron may be used, with care to avoid thrombocytosis and hypertension. [1]
The practical rule: screen every patient facing major elective surgery for anaemia early enough in the pathway (ideally at the surgical decision-to-treat) that there is time for iron therapy to work before the operation. [1]
Frailty and the older surgical patient
Older patients are over-represented in perioperative morbidity and mortality, and frailty — the loss of physiological reserve that makes a patient vulnerable to stress — is a stronger predictor of outcome than chronological age alone. A frail patient is more likely to suffer delirium, falls, infection, prolonged length of stay, institutional discharge and death after surgery, and the frailty is modifiable if identified early. [1]
Screen for frailty. Use a validated tool in the preadmission clinic — the Clinical Frailty Scale, the Edmonton Frail Scale, or the PRISMA-7. A score of 5 or more on the Clinical Frailty Scale (mildly frail or worse) flags a patient at elevated risk. Do not rely on age alone: a fit 80-year-old may tolerate major surgery better than a frail 65-year-old. [1]
Comprehensive geriatric assessment. For the frail older patient, a multi-domain assessment — cognition, mood, nutrition, function, comorbidity, polypharmacy, and social support — identifies the modifiable targets. Prehabilitation (structured exercise, nutritional support, and optimisation of comorbidities) in the weeks before surgery improves functional outcomes and reduces complications in trials of older surgical patients. [1]
Delirium prevention is perioperative care. The same measures that prevent delirium — avoiding deliriogenic drugs (anticholinergics, benzodiazepines), managing pain without excess opioids, maintaining orientation and sleep, ensuring vision and hearing aids are available, early mobilisation, and treating infection and metabolic disturbance — are the measures that protect the older brain through the surgical stress. [1]
Advance care planning and goals of care. For the frail older patient, document the patient's preferences, the ceiling of care, and the surrogate decision-maker before surgery. A perioperative discussion about resuscitation status and the realistic outcomes — including the possibility of a reduced trajectory of function or new institutional care — is part of informed consent in this group, not an afterthought. [1]
Communication, consent and shared decision-making
Perioperative medicine is as much a conversation as a prescription. The physician should make sure the patient understands: [1]
- What the surgery and the perioperative period involve — the procedure, the anaesthetic, the expected recovery, and the realistic risks.
- The patient-specific risks — quantified using the RCRI and the NSQIP calculator where helpful, so the patient hears "your chance of a heart complication is about 1 in 20" rather than a generic list.
- The medication changes — which drugs to stop, which to continue, when to stop them, and when to restart. Give a written perioperative medication plan.
- The diabetes and anticoagulation plan — written down, with dates, because these are the highest-risk medication decisions.
- The role of advance care planning — particularly in older and high-risk patients, including goals of care and surrogate decision-makers.
- The recovery expectations — mobilisation on day one, the length of stay, return to function, and the warning signs to report. [1]
Document the conversation and the shared decisions. A patient who understands their perioperative plan and the reasoning behind it is more likely to adhere to it and to recover faster. [1]
Common exam traps and high-yield discriminators
- The mechanical mitral valve patient. Always bridge — it is the highest annual thrombotic risk and a valve thrombosis is usually fatal. The bileaflet mechanical aortic valve usually does not need bridging.
- "Clearing" the asymptomatic patient. Do not revascularise, stress-test, or start a beta-blocker routinely to "clear" for surgery. Risk-stratify with the RCRI and functional capacity, and test or intervene only when the result will change management.
- Sliding-scale insulin. The phrase is a red flag. Use the variable-rate intravenous insulin infusion (VRIII) with a substrate fluid and a titrated algorithm. [1]- SGLT2 inhibitors and the fasted surgical patient. Stop three days before elective surgery because of the risk of euglycaemic diabetic ketoacidosis. The clue is a metabolic acidosis with only mildly elevated glucose.
- Aspirin and the coronary stent. Continue aspirin unless the bleeding risk is extreme. The catastrophic risk is stent thrombosis.
- Warfarin reversal for major bleeding. PCC plus intravenous vitamin K — not vitamin K alone, which is too slow.
- The patient "who cannot climb a flight of stairs." Poor functional capacity — fewer than 4 METs — is the trigger for further risk assessment if the surgical risk is elevated, not an automatic stress test.
- POISE. The trial that ended routine perioperative beta-blocker initiation. Know its findings: reduced MI, increased mortality and stroke, driven by hypotension and bradycardia.
- The first anticoagulant dose after surgery. Time it against bleeding risk — typically 6 to 12 hours postoperatively for LMWH in general surgery, after haemostasis is secure.
- Parkinson medications. Continue — withdrawal can cause life-threatening rigidity and airway compromise. [1]
Long-case integration
In a DCE long case, the perioperative patient is the multi-morbidity archetype: the 74-year-old with atrial fibrillation on warfarin, type 2 diabetes on insulin and an SGLT2 inhibitor, COPD, a mechanical mitral valve or a recent coronary stent, on an ACE inhibitor and a beta-blocker, facing a major intra-abdominal operation. The structured approach is: [1]
- Opening statement (SASPOP) — present the patient, the planned surgery, and the key problems.
- Problem list — number the active problems: the cardiac risk, the anticoagulation decision, the diabetes plan, the pulmonary optimisation, the chronic medication adjustments, the VTE prophylaxis, and the social and functional context.
- Cardiac risk stratification — calculate the RCRI, assess functional capacity, decide on testing (usually none, if capacity is good), and confirm the beta-blocker is continued and a statin is on board.
- Anticoagulation plan — state the thrombotic risk, the bridging decision (bridge the mechanical mitral valve), the stop and restart dates, and the reversal plan if bleeding occurs.
- Diabetes plan — stop the SGLT2 inhibitor three days before, manage the insulin with a VRIII during fasting, target 6 to 10 mmol/L, resume the usual regimen when eating. [1]6. Pulmonary optimisation — stop smoking, optimise COPD therapy, plan for incentive spirometry and early mobilisation.
- Chronic medications — list each drug and the plan (continue, hold the morning dose, or stress-dose).
- VTE prophylaxis — calculate the Caprini score, prescribe LMWH and mechanical prophylaxis, state the timing.
- ERAS elements — confirm the patient is on an ERAS pathway: carbohydrate drink, goal-directed fluid, opioid-sparing analgesia, early mobilisation, early feeding.
- Communication — explain the plan to the patient, give a written medication schedule, document the consent and the goals of care. [1]
References and guidelines
Lee RCRI derivation and validation (Lee 1999, Circulation); POISE trial on perioperative metoprolol (Devereaux 2008, Lancet); POISE-2 on aspirin and clonidine (Devereaux 2014, NEJM); CARP trial on coronary revascularisation before vascular surgery (McFalls 2004, NEJM); Padua Prediction Score for medical VTE risk (Barbar 2010, J Thromb Haemost); ACCP 9th edition VTE prophylaxis in surgical patients (Gould 2012, Chest); idarucizumab for dabigatran reversal (Pollack 2015, NEJM); andexanet alfa for factor Xa inhibitor reversal (Connolly 2016, NEJM); 4-factor PCC for warfarin reversal (Sarode 2013, Circulation); perioperative statins for vascular surgery (Sanders 2013, Cochrane); ERAS review (Ljungqvist 2017, JAMA Surg). ESC/ESA guidelines on cardiovascular assessment for non-cardiac surgery (Kristensen 2014); ACC/AHA perioperative guideline; Joint British Diabetes Societies perioperative diabetes guideline; Australian Diabetes Society; ANZCA perioperative medicine guidance. [1]
References
- [1]Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for prediction of cardiac risk of major noncardiac surgery Circulation, 1999.PMID 10477528
- [2]Devereaux PJ, Yang H, Yusuf S, et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial Lancet, 2008.PMID 18479744
- [3]Devereaux PJ, Mrkobrada M, Sessler DI, et al. Aspirin in patients undergoing noncardiac surgery N Engl J Med, 2014.PMID 24679062
- [4]McFalls EO, Ward HB, Moritz TE, et al. Coronary-artery revascularization before elective major vascular surgery N Engl J Med, 2004.PMID 15625331
- [5]Ljungqvist O, Scott M, Fearon KC Enhanced Recovery After Surgery: A Review JAMA Surg, 2017.PMID 28097305
- [6]Barbar S, Noventa F, Rossetto V, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score J Thromb Haemost, 2010.PMID 20738765
- [7]Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest, 2012.PMID 22315263
- [8]Pollack CV Jr, Reilly PA, Eikelboom J, et al. Idarucizumab for Dabigatran Reversal N Engl J Med, 2015.PMID 26095746
- [9]Connolly SJ, Milling TJ Jr, Eikelboom JW, et al. Andexanet Alfa for Acute Major Bleeding Associated with Factor Xa Inhibitors N Engl J Med, 2016.PMID 27573206
- [10]Sarode R, Milling TJ Jr, Refaai MA, et al. Efficacy and safety of a 4-factor prothrombin complex concentrate in patients on vitamin K antagonists presenting with major bleeding: a randomized, plasma-controlled, phase IIIb study Circulation, 2013.PMID 23935011
- [11]Sanders RD, Nicholson A, Lewis SR, Smith AF, Alderson P Perioperative statin therapy for improving outcomes during and after noncardiac vascular surgery Cochrane Database Syst Rev, 2013.PMID 23824754