Phys · general-medicine
Rapid Response Systems and MET Calls — The System That Catches the Deteriorating Patient
Also known as rapid response system · RRS · medical emergency team · MET call · MET · rapid response team · RRT · critical care outreach · CCO · track and trigger · early warning score · NEWS2 · between the flags · failure to rescue · SBAR · afferent limb · efferent limb · ceiling of care · goals of care · clinical deterioration · deteriorating patient
Consultant-physician-depth guide to the Rapid Response System as a patient-safety structure, not a resuscitation technique. Covers the four limbs of the RRS (afferent detection, efferent response, governance, quality improvement), track-and-trigger systems (NEWS2, Between the Flags, COMPASS), single-parameter MET calling criteria, the MET versus RRT versus critical care outreach models, the three failure-to-rescue modes (recognise, communicate, respond), SBAR escalation, the clinical response to a MET call, the post-MET plan and ceiling of care, governance and audit, and the evidence base (MERIT, Chan, Maharaj). Structured for FRACP DWE and DCE preparation, with ANZ primary anchoring.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Rapid Response Systems and MET Calls — The System That Catches the Deteriorating Patient

The answer first
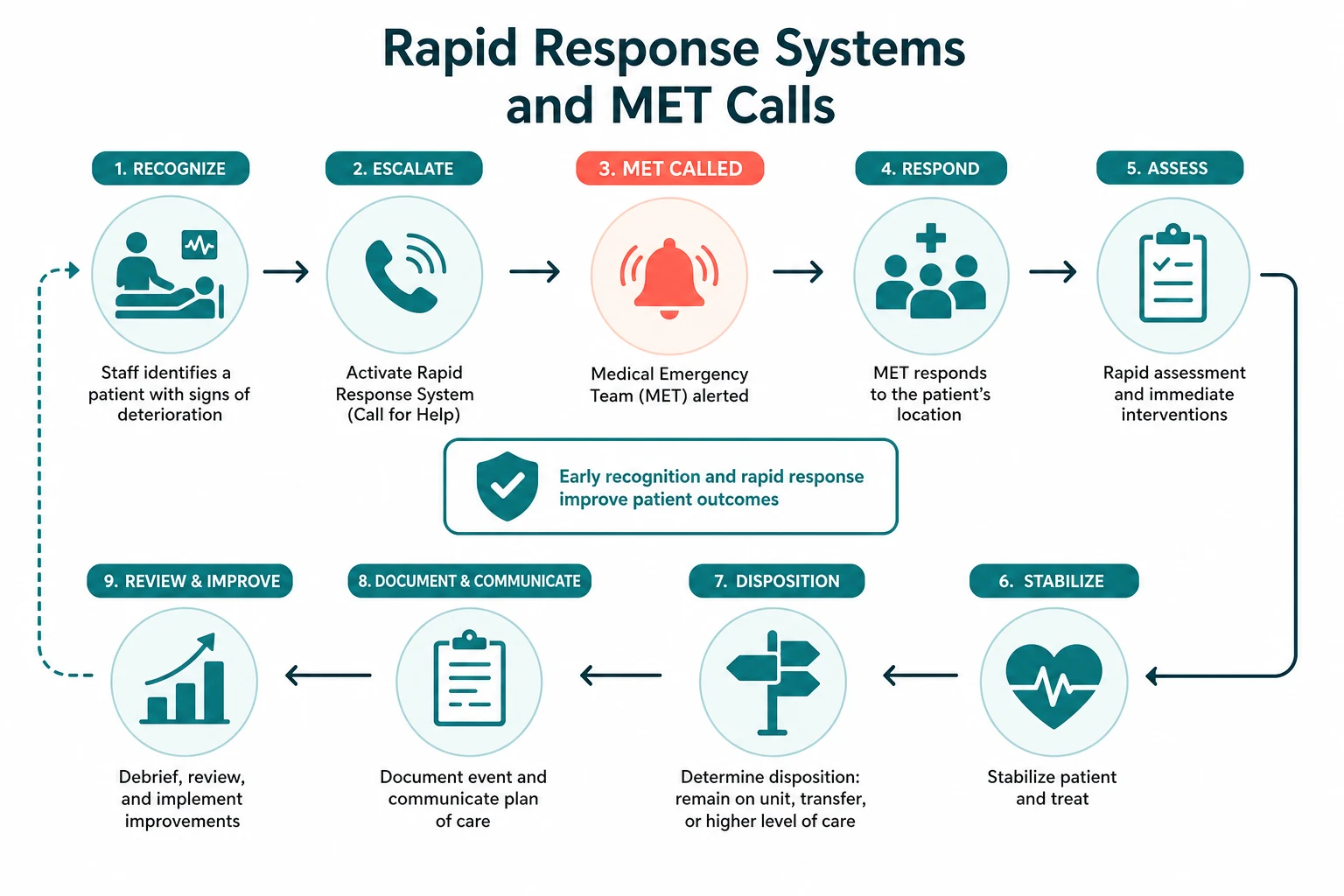
A Rapid Response System (RRS) is not a resuscitation technique and not a team. It is an organisational structure designed to identify and respond to the deteriorating ward patient before they suffer a cardiac arrest or other major adverse event. The empirical foundation is four decades of acute-medicine research showing that in-hospital cardiac arrest and unexpected ICU admission are rarely sudden — they are the end-state of hours of measurable, characteristic physiological deterioration that, in the majority of cases, is present but not recognised, not communicated, or not acted upon [1]. The RRS is the hospital's organised answer to that failure.
The conceptual model, formalised at the first international consensus conference in 2005 and published by DeVita and colleagues in 2006, frames the RRS as four interdependent limbs [4]:
- The afferent limb (detection) — the ward staff, the track-and-trigger system, and the calling criteria that recognise deterioration and trigger the response.
- The efferent limb (response) — the Medical Emergency Team, the Rapid Response Team, or the critical care outreach team that arrives at the bedside.
- The administrative or governance limb — the resources, the staffing, the policy, and the organisational culture that embed the system.
- The quality improvement limb — the audit, the outcome review, the education, and the feedback loop that refine the system over time. [1]
The cardinal teaching point for the registrar — and the one the examiner will probe — is that the afferent limb is the weakest link in almost every system. A perfectly constituted MET team is useless if the ward staff do not measure the observations, do not calculate the score, do not recognise the trend, or do not call. The MERIT study, the only cluster-randomised trial of a MET system, found that the team was called to only about 30 per cent of patients who met the calling criteria and were subsequently admitted to ICU [3]. The intervention that failed was not the team — it was the detection.
Viva trap: "What is the difference between a Rapid Response System and a Medical Emergency Team?" The honest answer is that the MET is one limb of the RRS — the efferent limb — and the common error is to fund the team, brand the team, and audit the team while neglecting the afferent limb that determines whether the team is ever called. A system is only as strong as its weakest link, and in the RRS the weakest link is almost always the ward nurse who is worried but unsure whether to call, and the junior doctor who is unsure whether the score justifies the escalation. [1]
The empirical foundation — hours of warning before arrest
Every track-and-trigger system, every calling criterion, every early warning score, and every rapid response team traces its justification to a single empirical insight: in-hospital cardiac arrest is a late event in a sequence of measurable deterioration that has been unfolding for hours. [1]
Schein and colleagues established this in 1990 with their prospective study of 64 ward cardiac arrests. They found that 84 per cent of patients had documented clinical deterioration in the eight hours before arrest, with a mean respiratory rate of 29 breaths per minute. The antecedents were predominantly respiratory (38 per cent) or a combination of respiratory and metabolic (27 per cent); pure cardiac events were a minority (9 per cent) [1]. Subsequent multi-centre data have confirmed that approximately 80 per cent of in-hospital arrest patients exhibit physiological instability in the hours before the event.
The implication is decisive. If the deterioration is measurable, then it is detectable. If it is detectable, then it is actionable. If it is actionable, then the arrest is preventable in a meaningful proportion of cases — and the system that delivers the detection and the action is the Rapid Response System. The cardiac arrest team, by contrast, arrives after the event and rescues a small minority; the RRS arrives before the event and prevents the majority. This is the conceptual shift the registrar must carry: the RRS is a prevention system, and the cardiac arrest team is a rescue service. [1]
The physiological signature of deterioration follows a predictable cascade. The compensatory phase comes first: the respiratory rate rises, the heart rate rises, the peripheries constrict. Blood pressure and conscious level are held near-normal by these mechanisms, which is precisely why they are late markers. The decompensatory phase follows when compensation fails: blood pressure falls, saturation drops, urine output falls, and mental state deteriorates. The patient who has reached this phase is already critically ill. The RRS is designed to intercept the patient in the compensatory phase — when the score is rising, the trend is adverse, and the call is still early. [1]
The four limbs of the Rapid Response System
The afferent limb — detection
The afferent limb is the detection mechanism: the ward staff who measure the vital signs, the track-and-trigger system that scores them, the calling criteria that mandate escalation, and the cultural permission to call. It is the limb that converts the subjective judgement "this patient looks unwell" into an objective, reproducible trigger that mandates a response — removing the hesitation and the inter-observer variability that delay the response. [1]

The afferent limb has two functional designs: [1]
- Single-parameter or calling-criteria systems — a defined list of physiological derangements, any one of which triggers the call. The MET calling criteria (below) are the canonical example. The strength is simplicity: a single markedly abnormal value is an unambiguous trigger. The weakness is that a patient with several mildly abnormal values — each individually below the single-parameter threshold — may be missed.
- Aggregate-weighted scoring systems — an Early Warning Score that assigns a weight to each physiological parameter, sums them, and links the total to a graded response. NEWS2 is the dominant example. The strength is that the aggregate catches the patient with several mildly abnormal values. The weakness is that a single markedly abnormal value may be diluted into an apparently acceptable total — which is why NEWS2 includes the "single red score" rule. [1]
The mature afferent limb uses both — an aggregate score for the graded response, and single-parameter criteria for the immediate emergency response. This is the structure of the NSW Between the Flags system and of most modern NEWS2 implementations. [1]
The efferent limb — the response
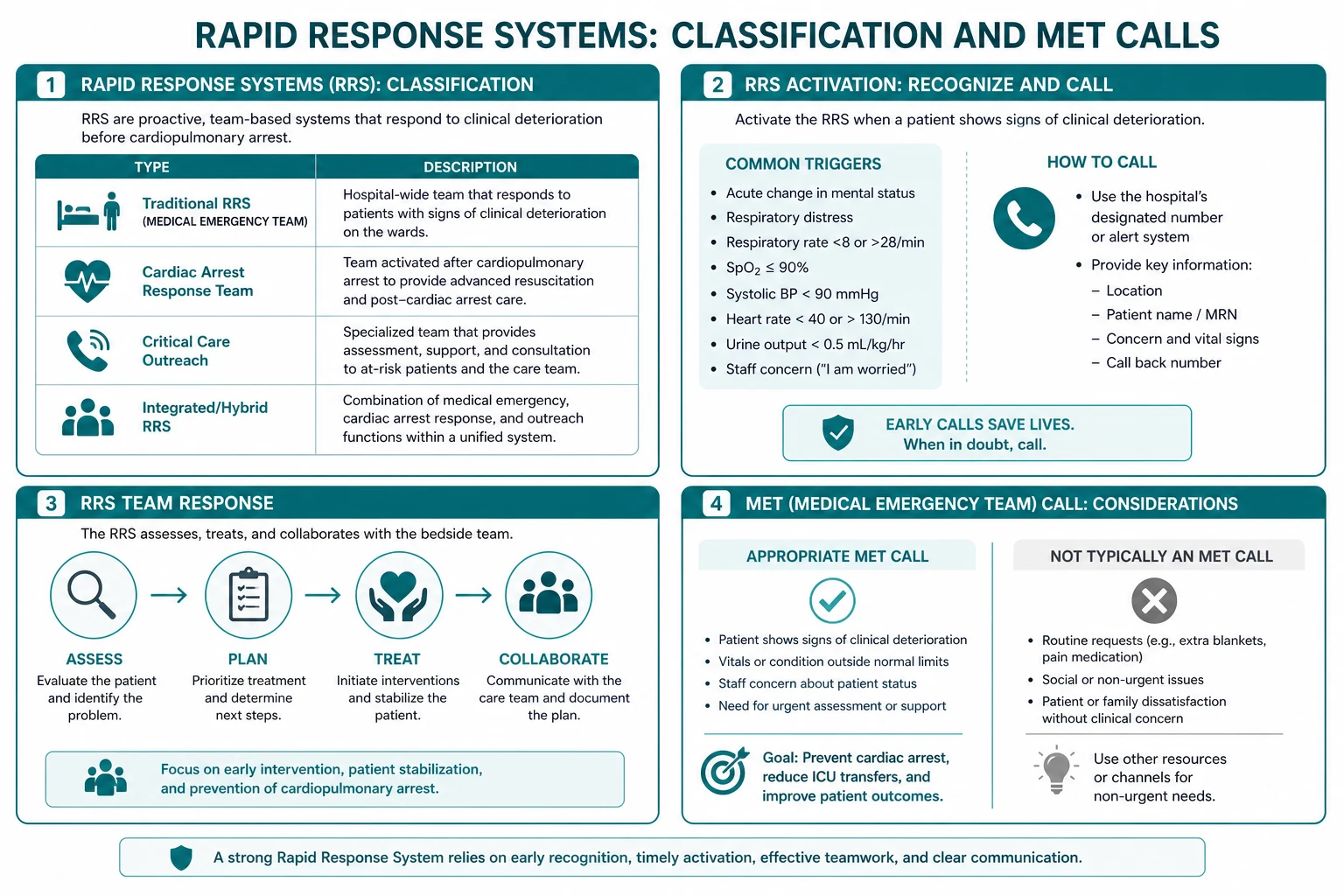
The efferent limb is the team that responds to the trigger. The three models in modern practice differ in composition and philosophy but share the function of bringing critical care competencies to the ward bedside: [1]
- The Medical Emergency Team (MET) — the ANZ model, physician-led, typically an ICU registrar and an ICU nurse, often joined by the covering medical registrar and a medical officer. The MET is reactive: it is called when the trigger fires.
- The Rapid Response Team (RRT) — the North American term, often nurse-led or nurse-and-respiratory-therapist-led, with physician backup. Functionally equivalent to the MET.
- Critical Care Outreach (CCO) — the UK model of senior critical-care-trained nurses who proactively review at-risk ward patients, support ward staff in early resuscitation, and bridge the ward-ICU interface. [1]
The distinction the registrar must carry is the reactive-versus-proactive axis. The MET and RRT are reactive — they respond to a call. Outreach is proactive — it seeks out the at-risk patient and supports the ward before the trigger fires. The most mature systems combine both: outreach for the proactive review of rising-risk patients, and a MET for the emergency response. The question of whether physician-led teams outperform nurse-led teams is settled by the Maharaj 2015 meta-regression, which did not identify physician presence as a significant factor in mortality reduction [6]. The model should fit the institution's staffing and culture, not an assumption about seniority.
The governance and quality improvement limbs
The administrative limb provides the resources — the team, the staffing roster, the education budget, the policy, the escalation protocol — and embeds the system in the hospital's culture. The governance committee oversees the calling criteria, the team composition, the response times, and the audit. The quality improvement limb closes the loop: it audits the MET calls, reviews the outcomes, feeds back to the ward staff, debriefs after each call, and refines the system through successive cycles. A RRS without these limbs is a team without a system — and a team without a system is the MERIT control hospital. [1]
The afferent limb in depth — track and trigger
A track-and-trigger system measures the vital signs at intervals, assigns a weight to each, and links the result to a predefined clinical response. The aim is to standardise the recognition of deterioration so that it does not depend on the experience, the confidence, or the presence of a particular clinician at the bedside. [1]
NEWS2 — the dominant aggregate system
NEWS2, the second iteration of the National Early Warning Score, was developed by the Royal College of Physicians and published in 2017. It is built from six physiological measurements plus a conscious-level score: [1]
- Respiratory rate (breaths per minute)
- Oxygen saturation (SpO2, per cent)
- Supplemental oxygen (air or oxygen — yes or no)
- Temperature (degrees Celsius)
- Systolic blood pressure (mmHg)
- Heart rate (beats per minute)
- Conscious level (ACVPU — Alert, new Confusion, Voice, Pain, Unresponsive) [1]
Each parameter is scored 0 to 3, with 0 the normal range and higher scores for greater deviation. The sum is the NEWS2, ranging from 0 to 20. A second SpO2 scale (scale 2) exists for patients with hypercapnic respiratory failure who have a prescribed lower target range (typically 88 to 92 per cent) — the defining example is the COPD patient at risk of CO2 retention. [1]
The three response thresholds are the part the examiner will probe: [1]
- NEWS2 of 0 to 4 — low risk. Routine ward management. Monitoring at least every 4 to 6 hours, by a registered nurse.
- NEWS2 of 5 to 6 — medium risk (the key threshold). Urgent review by a registered medical practitioner or acute team — typically the ward registrar — within 30 minutes. Increase monitoring to hourly.
- NEWS2 of 7 or more — high risk (clinical emergency). Emergency assessment by a clinician with critical care competencies within minutes. Continuous monitoring. This is the MET call threshold. [1]
The single most testable NEWS2 rule is the red score: a single score of 3 in any one parameter mandates urgent review regardless of the aggregate, because a single markedly abnormal value may be diluted into an apparently acceptable total. A respiratory rate of 8, a systolic of 80, a heart rate of 140, or an SpO2 of 85 per cent cannot wait for the sum to be added. [1]
Smith and colleagues validated NEWS against 33 other early warning scores and showed it discriminated patients at risk of cardiac arrest, unanticipated ICU admission, and death at least as well as any existing system [2]. NEWS2 is the score; clinical judgement is the floor of the response, not the ceiling.
Between the Flags — the ANZ state-wide system
The Between the Flags program, developed by the NSW Clinical Excellence Commission and rolled out state-wide in January 2010, operationalises Standard 9 of the Australian Commission on Safety and Quality in Health Care across the whole NSW public hospital system. It uses a colour-banded observation chart with a red zone (single-parameter physiological derangement mandating an immediate clinical review by senior staff) and a yellow zone (mild derangement mandating a registered-nurse or registrar review). Any observation in the red zone, or two or more in the yellow zone, triggers a predefined escalation. The program also mandates a clinical review by a senior clinician and a rapid response escalation if the ward staff are worried, regardless of the zone. [1]
Between the Flags is functionally equivalent to NEWS2 with single-parameter calling criteria overlaid — but it is institutionally branded, embedded in a state-wide chart and escalation protocol, and backed by mandated education. The registrar arriving at a NSW hospital uses the Between the Flags chart as configured; the registrar arriving at a hospital that uses NEWS2 uses NEWS2. The principle is universal; the brand and the thresholds differ. [1]
Other systems and the regional delta
The Modified Early Warning Score (MEWS) predates NEWS and is still used in some institutions. COMPASS (COmposite Physiologic risk ASsessment, a deterioration prediction model) is used in some hospitals to supplement the aggregate score with a continuous risk estimate. The Paediatric Early Warning Score (PEWS) adapts the principle to age-specific physiology. In the United States, institution-specific early warning scores and calling criteria are common, and the National Early Warning Score is less uniformly adopted. [1]
The regional delta the registrar must carry: the principle is universal — track physiological parameters, score them, and trigger a graded response — but the specific thresholds and the brand differ by institution. Always confirm the local system on arrival. The worst of both worlds is to carry a NEWS2 habit into a Between the Flags hospital and escalate at the wrong thresholds, or to assume a single red score rule in a hospital that does not use it. [1]
MET call criteria — the single-parameter trigger
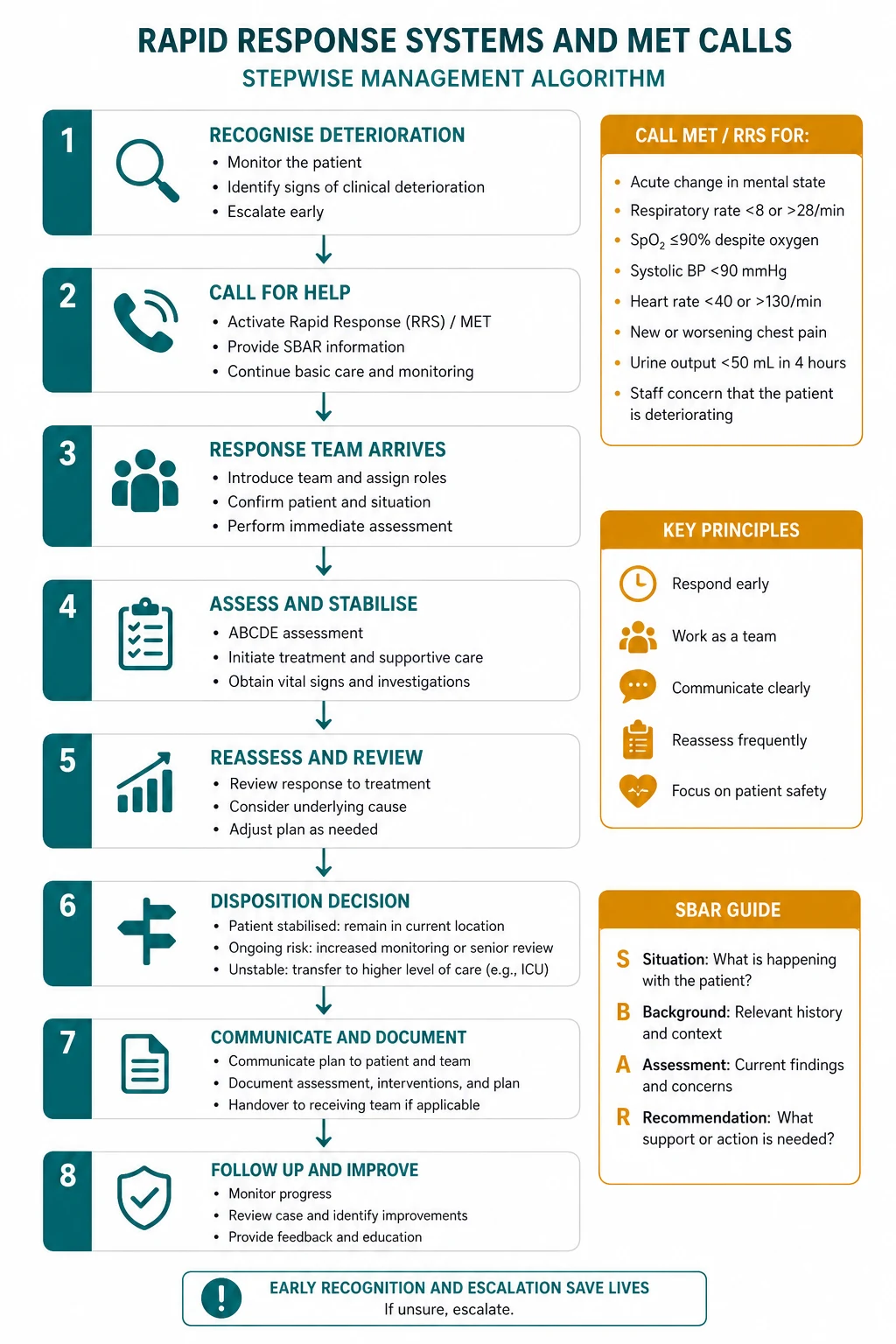
Most ANZ hospitals operate a Medical Emergency Team call with a defined set of calling criteria that any staff member can activate. The criteria combine single-parameter physiological derangements with the subjective concern of staff. A representative set — the specifics vary by institution but the structure is consistent: [1]

- Airway threat — any concern that the airway is or may become compromised.
- Respiratory distress, or respiratory rate below 8 or above 30 breaths per minute.
- SpO2 below 90 per cent despite supplemental oxygen.
- Heart rate below 40 or above 130 beats per minute.
- Systolic blood pressure below 90 mmHg despite a fluid challenge.
- An acute change in conscious state — new confusion, agitation, drowsiness, or a fall in GCS.
- Repeated or prolonged seizure.
- Staff worried — any staff member who is seriously concerned about a patient, even if the observations have not yet crossed a threshold. [1]
The "worried" criterion is the most important and the most underused. Experienced ward nurses detect deterioration before the observations cross a threshold — the change in the patient's appearance, the subtle increase in work of breathing, the restlessness, the "they just don't look right." The system is designed to support, not penalise, the call based on that judgement. The cultural message, from the top of the organisation down, is that it is always acceptable to call, and never acceptable to delay a call for a patient you are worried about. A false-positive MET call costs the team a few minutes; a delayed call costs a life. [1]
The lesson from MERIT is sobering: the MET was called to only about 30 per cent of patients who met the calling criteria and were subsequently admitted to ICU [3]. The afferent limb — the recognition and the call — was the failure point. The team was available; the call was not made. This is why the governance and education investment in the afferent limb is as important as the investment in the team.
Who can call, and the consumer-activated escalation
Any staff member — nurse, junior doctor, allied health — is empowered to call a MET. Increasingly, the afferent limb extends to patients and families through consumer-activated escalation: Ryan's Rule in Queensland and the REACH program in NSW allow a patient or family member to trigger an independent clinical review when they are concerned about a deterioration that they feel has not been adequately addressed. The principle is the same: the person closest to the patient — whether a nurse, a doctor, or a family member — may detect the deterioration first, and the system must have a channel for their concern. [1]
Failure to rescue — the three failure modes
The conceptual core of the RRS is the prevention of failure to rescue — the inability to recognise, communicate, or respond to a patient's clinical deterioration, leading to preventable harm. Failure to rescue is widely used as a quality-of-care metric, and the RRS is specifically designed to interrupt the evolutionary cascade of deterioration at each of the three points where it fails. [1]
1. Failure to recognise. The abnormal observations are not measured, not recorded, not scored, or not recognised as dangerous. The respiratory rate is omitted (it is the most informative and the most neglected vital sign); the trend is not appreciated; the score is not calculated; the single red score is diluted into an acceptable aggregate. This is the dominant failure mode, and it is the reason the afferent limb is the weakest link. [1]
2. Failure to communicate. The deterioration is recognised but not communicated effectively. The handover is poor, the escalation does not happen, the SBAR recommendation is under-specified — "I just thought I would let you know" instead of "I would like you to come now." The call is delayed because the caller is unsure whether it is justified. This is where the SBAR tool and the cultural permission to call intervene. [1]
3. Failure to respond. The deterioration is recognised and communicated, but the response is delayed or inadequate. The team arrives late, the interventions are insufficient, the reversible cause is not identified, the escalation to ICU is deferred. This is where the efferent limb's composition, its response time, and its competencies matter. [1]
The registrar's role at a MET call spans all three: the recognition (did the afferent limb fire appropriately?), the communication (the SBAR handover to the team and to the treating consultant), and the response (the ABCDE assessment, the identification and treatment of the cause, and the escalation decision). [1]
SBAR — the communication tool
The standardised handover tool is SBAR — Situation, Background, Assessment, Recommendation. It delivers a complete clinical picture in under a minute and is embedded in acute-care communication across the English-speaking world. [1]
- Situation — who you are, who the patient is, where they are, and what has happened. "This is Dr Lee, the ward registrar. I am calling about Mr Chen in bed 12, a 68-year-old man who has acutely deteriorated in the last hour with a NEWS2 of 9."
- Background — the relevant history, the admission, the comorbidities, and the recent course. "He was admitted three days ago with cellulitis. He has type 2 diabetes and ischaemic heart disease. He has been on IV flucloxacillin."
- Assessment — the current observations, the examination, and the working diagnosis. "His respiratory rate is 30, his SpO2 is 88 per cent on room air, his heart rate is 128, his blood pressure is 84 over 52, his GCS is 14 with new confusion, and his temperature is 38.8. His lactate is 4.2. My working diagnosis is septic shock."
- Recommendation — what you want, when you want it, and from whom. "I would like you to come and review him on the ward now. I think he needs ICU admission for vasopressor support." [1]
The common SBAR failure is the under-specified Recommendation — to deliver a thorough Assessment and then trail off with "I just thought I would let you know." The Recommendation must be specific, timed, and must name the action. "I would like you to come now" is the recommendation the deteriorating patient needs. [1]
The clinical response to a MET call
When the MET arrives, the response follows the universal ABCDE structure, treating life-threats in the order they are found. The detail of the ABCDE assessment is covered in the companion topic on the deteriorating ward patient; the systems-level teaching point here is the sequence of decisions the registrar makes at a MET call: [1]
1. ABCDE assessment and immediate resuscitation. Secure the airway, give high-flow oxygen to the hypoxaemic patient, establish intravenous access, give a fluid challenge to the hypotensive patient, check a bedside glucose and a venous gas, and start continuous monitoring. In parallel, identify the likely cause — sepsis is the single commonest precipitant of ward deterioration, and the first question is "where is the infection?" [7].
2. Identify and treat the reversible cause. The common precipitants of a MET call cluster into sepsis, hypovolaemia (bleeding or dehydration), cardiac (new arrhythmia, infarction, failure), respiratory (pneumonia, PE, aspiration), neurological (stroke, seizure, metabolic encephalopathy), drug-related (opioid depression, adverse effect, withdrawal), and metabolic (DKA, hypoglycaemia, hyperkalaemia, acid-base disorder). The blood gas, the ECG, the glucose, the drug chart, and the focused examination together discriminate these in minutes. [1]
3. Make the escalation decision. The question is whether the patient needs ICU admission. The decision is based on the failure to respond to ward-level therapy or the need for organ support the ward cannot provide: airway support (intubation), respiratory support (non-invasive or invasive ventilation), circulatory support (vasopressors or inotropes), neurological support (a falling GCS that threatens the airway), or renal support (renal replacement therapy for refractory hyperkalaemia or fluid overload). [1]
4. Document, debrief, and implement the post-MET plan. The MET call is documented — the assessment, the interventions, the escalation decision, the goals of care. The team debriefs, if only briefly, to identify any system gap and to support the staff. And the post-MET plan is implemented. [1]

The post-MET plan — goals of care and the ceiling of treatment
The post-MET plan is the registrar's ongoing responsibility, and it is the part the DCE long-case examiner will probe. It comprises: [1]
- The goals of care — what the treatment is aiming to achieve (cure, stabilise, palliate), and how the aims align with the patient's expressed wishes and baseline function.
- The ceiling of treatment — the most intensive level of treatment that is appropriate for this patient at this time: ward-based supportive care (no escalation, no CPR), ward-based active treatment (fluid, antibiotics, oxygen, but not ventilation), high-dependency (single-organ support), or full ICU and resuscitation.
- The monitoring frequency — hourly, two-hourly, or four-hourly, set by the NEWS2 and the clinical concern. [1]- The named responsible consultant — the senior clinician who owns the plan and who is contactable.
- The review timeline — when the patient will next be reviewed, and by whom.
- The communication with the team and family — the post-MET plan is communicated to the nursing staff, to the treating team, and to the family. [1]
The observation from MERIT that the MET system influenced end-of-life care — with a higher rate of not-for-resuscitation orders after MET-attended events — is not a side effect; it is part of the system's function [3]. The MET call surfaces the patient who is deteriorating despite treatment, and that is precisely the moment when the ceiling-of-care conversation should occur. Every deterioration is a trigger for the goals-of-care conversation, not an automatic trigger for ICU. The system that escalates every patient without surfacing the ceiling of care has misunderstood its purpose.
The communication skill is to reframe the conversation from "we are giving up" to "we are focusing on what will help." The time-limited trial of ICU care is the considered middle path: a defined period — perhaps 48 to 72 hours — of maximal support, after which the team and the family reassess together. If the treatment is working, it continues; if it is not, the care refocuses on comfort. The patient or family who hears "we will focus on what will help, alongside the active treatment of the reversible elements" hears care, not abandonment. [1]
Governance, audit, and the quality improvement limb
The administrative and quality improvement limbs are what separate a mature RRS from a standalone team. The governance committee oversees the system; the audit cycle measures it; the education invests in the afferent limb; and the outcome review learns from every event. [1]
The audit cycle
The metrics a mature RRS tracks include: [1]
- The number of MET calls per 1000 admissions. The MERIT benchmark — 3.1 per 1000 at baseline, rising to 8.7 per 1000 with a mature system — gives a reference. A very low call rate in a hospital with average acuity suggests the afferent limb is under-firing, not that the patients are well.
- The proportion of patients meeting criteria who were called — the afferent limb sensitivity, the metric MERIT exposed at 30 per cent.
- The outcome of calls — ward (the majority), ICU, palliative or ceiling-of-care change, and the cardiac arrests that occurred despite the system.
- The time-to-response — the interval between the call and the team's arrival, a marker of the efferent limb's function.
- The cardiac arrest rate outside the ICU — the primary outcome metric, the one the meta-analyses track. [1]
Education and the afferent limb
The investment in the afferent limb is the investment in ward staff: training nurses and junior doctors to measure the full vital sign set (including the respiratory rate), to calculate the score, to recognise the trend, and to escalate without hesitation. The simulation training, the case-based teaching, the feedback after each call, and the visible support of senior staff for the call that turned out to be unnecessary — these are the interventions that build the afferent limb. A hospital that funds a MET team but does not fund the ward education has funded the efferent limb and neglected the limb that determines whether the team is called. [1]
Debriefing and outcome review
After a MET call, a brief team debrief identifies what went well and what did not — the system gap, the delayed call, the communication failure, the intervention that was late. After a cardiac arrest or an unexpected death, the root cause analysis reviews whether the afferent limb fired (was the deterioration recognised?) and whether the efferent limb responded (did the team arrive in time, and was the response adequate?). The learning feeds back into the system: the refinement of the calling criteria, the targeted education of a ward or a team, the system change that prevents the next event. This is the quality improvement limb, and without it the system does not learn. [1]
Do rapid response systems work? The evidence
The evidence base is the question every acute physician must answer with nuance, because the data are mixed and the examiners know it. [1]
The MERIT study (Hillman and colleagues, 2005) was the landmark cluster-randomised controlled trial of the MET system across 23 Australian hospitals. It found that introducing the MET system increased the rate of emergency team calls (from 3.1 to 8.7 per 1000 admissions, p equal to 0.0001) but did not significantly reduce the composite primary outcome of cardiac arrest, unexpected death, or unplanned ICU admission (5.31 versus 5.86 per 1000 admissions, p equal to 0.640) [3]. The trial was criticised for inadequate statistical power, contamination (control hospitals increased their own MET-like calls during the study), and a short implementation period — but it remains the only randomised evidence and the result must be carried honestly.
The meta-analytic evidence is more favourable. Chan and colleagues' 2010 systematic review and meta-analysis of 18 studies found that rapid response teams were associated with a 33.8 per cent reduction in non-ICU cardiopulmonary arrests (relative risk 0.66) but no significant reduction in overall hospital mortality (RR 0.96) [5]. Maharaj and colleagues' 2015 systematic review and meta-analysis of 29 studies suggested reductions in both adult mortality (RR 0.87) and cardiopulmonary arrests (RR 0.65), but assessed the evidence as limited by substantial heterogeneity and the before-and-after design of most studies [6].
The synthesis the registrar should carry: [1]
- Rapid response systems reduce non-ICU cardiac arrests — this is the consistent finding across studies and meta-analyses.
- The mortality signal is diluted — by the patients for whom escalation is appropriately withheld (the ceiling-of-care decision), and by the before-and-after design of most studies. The mortality benefit is plausible but not conclusively demonstrated by a single randomised trial.
- The mechanism of benefit is broader than the arrest count — the system changes the safety culture of the hospital, surfaces deterioration earlier, supports ward staff, facilitates appropriate escalation, and surfaces the goals-of-care conversation.
- The afferent limb determines the effect — a system with a strong team but weak detection fails (the MERIT lesson); a system with strong detection and education succeeds. [1]
The honest synthesis for a hospital executive: implement the system, invest in both limbs (detection and response), embed the governance and quality improvement, and measure the cardiac arrest rate, the call rate, and the outcome of calls. The benefit is real even if the mortality signal is diluted. [1]
DCE long-case approach — the post-MET-call patient
Patient scenario
Mr David Chen, 68, retired engineer, was admitted three days ago with a left lower limb cellulitis treated with IV flucloxacillin. He has a background of type 2 diabetes (metformin and empagliflozin, HbA1c 64), ischaemic heart disease (prior NSTEMI two years ago, on aspirin, atorvastatin, bisoprolol), and stage 3 chronic kidney disease (baseline creatinine 130). At 22:00 on day 3, the nursing staff activated a MET call because his NEWS2 had risen from 2 to 8 over four hours and he had become confused and breathless. The MET attended, assessed him, gave high-flow oxygen, a fluid challenge, and broad-spectrum antibiotics, and contacted you — the medical registrar — for the ongoing review and the post-MET plan. [1]
On your assessment: respiratory rate 28, SpO2 90 per cent on 15 L via reservoir mask, temperature 38.9, heart rate 124 in new atrial fibrillation, blood pressure 88/54 after 500 mL crystalloid, GCS 14 with new confusion, capillary refill 4 seconds, mottled peripheries, urine output 20 mL/hour. Lactate 4.0. Creatinine 195 (up from 130). Potassium 5.6. Blood cultures taken. The MET team leader suspects septic shock from progression of the cellulitis to necrotising infection or a nosocomial pneumonia. [1]
Candidate's opening statement (SASPOP)
"Mr Chen is a 68-year-old retired engineer who was admitted three days ago with cellulitis and has acutely deteriorated overnight with a rising NEWS2 from 2 to 8, precipitating a MET call. He has type 2 diabetes, ischaemic heart disease, and chronic kidney disease stage 3. His main problems are septic shock with multi-organ involvement — refractory hypotension, new atrial fibrillation, acute kidney injury with hyperkalaemia, and a rising lactate — and the question of the source and the ceiling of care. My immediate priorities are to continue the ABCDE resuscitation, to identify and control the source, to treat the hyperkalaemia, to decide on ICU escalation, and to have an early, honest conversation with the family about his wishes given the comorbidities and the severity of the acute illness." [1]
Problem list and integrated management plan
- Septic shock — refractory hypotension, lactate 4.0, mottled peripheries. Continue the Sepsis Six with broad-spectrum antibiotics, cautious fluid resuscitation given his ischaemic heart disease, and early vasopressor (noradrenaline) if he is not fluid-responsive [7]. Identify the source — examine the limb for necrotising infection, send a chest X-ray for nosocomial pneumonia, and arrange surgical review if the cellulitis has progressed.
- Acute kidney injury with hyperkalaemia — creatinine risen from 130 to 195, potassium 5.6. Withhold the nephrotoxins (metformin, empagliflozin, NSAIDs), give calcium gluconate for myocardial stabilisation and insulin-dextrose to shift the potassium, monitor the ECG, and prepare for renal replacement therapy if refractory.
- New atrial fibrillation — almost certainly secondary to the sepsis and the electrolyte disturbance. Treat the cause; do not give a rate-control agent in the hypotensive state. Consider amiodarone if the AF is itself the haemodynamic problem.
- The ceiling of care — weigh the reversibility of the acute illness (the sepsis is potentially reversible), his baseline function (independent, retired engineer — favouring escalation), and his expressed wishes. Ask the family early. Offer a time-limited trial of ICU if the sepsis does not respond to the ward-level resuscitation.
- The afferent limb review — the NEWS2 rose from 2 to 8 over four hours; at what point should the call have occurred? The trend was the signal, and the intermediate thresholds (NEWS2 of 5 to 6) should have triggered the earlier review. The system learning feeds into the ward education and the feedback loop.
DCE short-case discussion — reviewing the post-MET patient
Instruction: "You are the medical registrar called to review a patient who had a MET call one hour ago. Describe your systematic approach to the post-MET review, the key questions you would ask, and the plan you would communicate to the team." [1]
Systematic assessment routine
- Review the MET call record — the observations at the time of the call, the interventions, the working diagnosis, and the MET team's plan. The record is the handover.
- Reassess the ABCDE — has the resuscitation improved the observations, or is the patient still deteriorating? A patient whose NEWS2 is falling after the MET call is responding; a patient whose NEWS2 is still rising needs escalation now.
- Review the working diagnosis — is the cause identified, and is it being treated? The MET call buys time; the registrar's job is to use that time to nail the diagnosis.
- Review the drug chart — every drug, every dose, every recent change. The nephrotoxins and the harmful drugs in the acute illness are withheld.
- Make the escalation decision — ICU, high-dependency, ward, or a change in the goals of care.
- Set the post-MET plan — the monitoring frequency, the named consultant, the review timeline, and the communication with the team and family. [1]
Presentation template
"I have reviewed Mr Chen, who had a MET call one hour ago for septic shock with multi-organ involvement. Since the MET call, his NEWS2 has fallen from 8 to 6 with the fluid and the oxygen, but he remains hypotensive at 88 over 54 and oliguric. My working diagnosis is septic shock from a progressive soft-tissue infection, with acute kidney injury, hyperkalaemia, and new atrial fibrillation. My plan is to continue the broad-spectrum antibiotics, to arrange an urgent surgical review of the limb for necrotising infection, to treat the hyperkalaemia, to start a noradrenaline infusion if the blood pressure does not respond to the next fluid challenge, and to escalate to ICU for vasopressor and possibly renal replacement therapy. I have asked the family about his wishes, and I have set the goals of care as a time-limited trial of ICU given his previously independent baseline and the potentially reversible sepsis. I will review him in 30 minutes and I have handed over to the night consultant." [1]
Discussion questions
Examiner: "What is the role of the MET call in the ceiling-of-care conversation?" [1]
"The MET call surfaces the conversation. The patient who has deteriorated to the point of a MET call is the patient for whom the question of escalation is live — whether the deterioration is reversible, whether the treatment is working, and whether the patient would want the proposed level of support. The MET team's assessment gives the information; the registrar's job is to use that information to set the goals of care honestly with the patient, if they have capacity, or with the family. The observation from MERIT that the MET system increased the rate of not-for-resuscitation orders is not a side effect — it is the system functioning as designed, surfacing the conversation at the moment it matters [3]. The time-limited trial is the considered middle path: maximal support for a defined period, with a clear review point, and a commitment to revisit the plan with the family."
Examiner: "What would you change about the afferent limb in this case?" [1]
"The NEWS2 rose from 2 to 8 over four hours, which means the intermediate thresholds — the NEWS2 of 5 to 6 that should have triggered the urgent ward-registrar review — were crossed two to three hours before the MET call. The afferent limb fired late. The fix is the education of the ward staff in recognising the trend and acting at the intermediate threshold, not waiting for the emergency threshold. The observation chart that displays the trend, the bedside signage that flags the rising score, and the feedback to the ward team after the event — these are the interventions that build the afferent limb. The MERIT finding that the MET was called to only 30 per cent of patients who met criteria is the afferent-limb failure, and this case is a mild version of it [3]. The system learning feeds into the quality improvement limb: the audit, the education, and the feedback."
Examiner: "What is the evidence that the system you are invoking actually works?" [1]
"The evidence is nuanced, and I carry it honestly. The MERIT study, the only cluster-randomised trial, did not show a significant reduction in the composite of cardiac arrest, unexpected death, or unplanned ICU admission, though it was underpowered and contaminated [3]. The meta-analytic evidence is more favourable: Chan's 2010 review showed a 33.8 per cent reduction in non-ICU cardiopulmonary arrests [5], and Maharaj's 2015 review suggested reductions in both adult mortality and arrests, though the evidence quality is limited by heterogeneity and before-and-after design [6]. My reading is that the system works by changing the safety culture, surfacing deterioration earlier, and facilitating appropriate escalation — and the cardiac arrest reduction is the consistent signal. For this patient, the question is not whether the system works in aggregate but whether calling the team and setting the plan was the right thing for him — and it was."
Key DWE MCQ patterns
- Recognise the four limbs of the RRS and the question of which is the weakest link — the answer is almost always the afferent limb, the detection.
- Recognise the single-parameter MET criteria and the "worried" criterion — any one criterion triggers the call, and the worried criterion is the most important and the most underused.
- Interpret the NEWS2 thresholds — 0 to 4 ward, 5 to 6 urgent registrar review, 7 or more emergency critical care assessment — and the single red score rule.
- Interpret the MERIT study honestly — increased calls, no significant reduction in the composite primary outcome, and the reasons (underpowering, contamination, the afferent limb firing at only 30 per cent).
- Interpret the Chan and Maharaj meta-analyses — consistent reduction in cardiac arrests, less consistent effect on overall mortality, and the dilution by the ceiling-of-care patients.
- Recognise the three failure-to-rescue modes — recognise, communicate, respond — and the intervention for each (track-and-trigger for recognition, SBAR for communication, the team for response).
- Recognise that physician-led and nurse-led teams are equivalent in the meta-regression evidence — the model should fit the institution.
- Recognise that the MET call is a trigger for the goals-of-care conversation — not an automatic trigger for ICU. [1]
References
[1] Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest 1990;98(6):1388–92. The foundational prospective study showing that 84 per cent of in-hospital arrest patients had documented deterioration in the preceding eight hours — the empirical basis for the Rapid Response System.
[2] Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 2013;84(4):465–70. The validation of NEWS against 33 other early warning scores, demonstrating discrimination of cardiac arrest, unanticipated ICU admission, and death.
[3] Hillman K, Chen J, Cretikos M, et al.; MERIT study investigators. Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial. Lancet 2005;365:2091–7. The only randomised trial of a MET system — increased calls from 3.1 to 8.7 per 1000 admissions, no significant reduction in the composite primary outcome, and the finding that the team was called to only 30 per cent of patients who met criteria.
[4] DeVita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med 2006;34(9):2463–78. The consensus document that defined the four-limb model of the Rapid Response System (afferent, efferent, administrative, quality improvement) and standardised the terminology.
[5] Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C. Rapid Response Teams: a systematic review and meta-analysis. Arch Intern Med 2010;170(1):18–25. The meta-analysis of 18 studies showing a 33.8 per cent reduction in non-ICU cardiopulmonary arrests with rapid response teams, but no significant reduction in overall hospital mortality.
[6] Maharaj R, Raffaele I, Wendon J. Rapid response systems: a systematic review and meta-analysis. Critical Care 2015;19:254. The systematic review of 29 studies suggesting reductions in both adult mortality (RR 0.87) and cardiopulmonary arrests (RR 0.65), with the meta-regression finding that physician presence on the team was not a significant factor.
[7] Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med 2021;47(11):1181–1247. The international consensus on the recognition and management of sepsis, including the hour-1 bundle that frames the response to the commonest precipitant of a MET call.
Schein et al., Chest 1990; Smith et al., Resuscitation 2013; Hillman et al. (MERIT), Lancet 2005; DeVita et al., Crit Care Med 2006; Chan et al., Arch Intern Med 2010; Maharaj et al., Critical Care 2015; Evans et al. (Surviving Sepsis 2021), Intensive Care Med 2021; Royal College of Physicians NEWS2 2017; NICE CG50; Australian Commission on Safety and Quality in Health Care Standard 9; NSW Clinical Excellence Commission Between the Flags; Resuscitation Council UK. [1]
References
- [1]Schein RM, Hazday N, Pena M, Ruben BH, Sprung CL Clinical antecedents to in-hospital cardiopulmonary arrest Chest, 1990.PMID 2245680
- [2]Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death Resuscitation, 2013.PMID 23295778
- [3]Hillman K, Chen J, Cretikos M, et al.; MERIT study investigators Introduction of the medical emergency team (MET) system: a cluster-randomised controlled trial Lancet, 2005.PMID 15964445
- [4]DeVita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams Crit Care Med, 2006.PMID 16878033
- [5]Chan PS, Jain R, Nallmothu BK, Berg RA, Sasson C Rapid Response Teams: A Systematic Review and Meta-analysis Arch Intern Med, 2010.PMID 20065195
- [6]Maharaj R, Raffaele I, Wendon J Rapid response systems: a systematic review and meta-analysis Crit Care, 2015.PMID 26070457
- [7]Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021 Intensive Care Med, 2021.PMID 34599691