Phys · general-medicine
Respiratory System Examination — DCE Short-Case Routine
Also known as respiratory examination · chest examination · lung examination · respiratory short case · DCE respiratory · PACES respiratory examination · IPAA examination · inspection palpation percussion auscultation · chest signs · respiratory system assessment
Consultant-physician guide to the systematic respiratory system examination for the DCE short case: the eleven-step routine (end of bed, hands, face, neck, anterior chest, posterior chest, legs, additional tests), the key physical signs and their physiological basis, the differential diagnosis from individual signs, the model presentation template, the examiner discussion questions, and the classic exam traps — the routine that every FRACP, MRCP PACES, and ABIM candidate must perform flawlessly.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Respiratory System Examination — DCE Short-Case Routine

The one-minute consultant answer
The respiratory system examination is the most commonly examined short case in the FRACP DCE and the MRCP PACES, and it follows an invariant eleven-step sequence that every candidate must perform fluently: end of bed, hands, face, neck, anterior chest (inspection, palpation, percussion, auscultation), posterior chest (the same IPAA sequence), legs, and additional bedside tests. The routine is not a checklist of isolated findings — it is an integrated assessment where each sign builds on the last and the synthesis at the presentation frames the differential diagnosis. The examiner is watching from the moment you enter the room: the five seconds at the end of the bed (is the patient breathless, cyanosed, cachectic, using accessory muscles, barrel-chested, with oxygen or an inhaler visible?) often reveals the diagnosis before you touch the patient [1].
The single most important principle is asymmetry. The respiratory examination is a comparison of the two sides of the chest, and the finding that one side is different from the other — reduced expansion, dull or stony dull percussion, absent or bronchial breath sounds, reduced vocal resonance — is the finding that localises the pathology. The candidate who percusses the right base then the right mid-zone then the left base has lost the comparison; the correct technique is right base then left base, right mid-zone then left mid-zone, comparing symmetrical areas at each step [1].
The non-negotiable principles: start at the end of the bed, because the general inspection reveals the diagnosis in a significant proportion of cases; examine the hands before the chest, because the clubbing, the cyanosis, the tremor and the asterixis frame the differential before you reach the stethoscope; assess the tracheal position and the JVP, because they localise the pathology and reveal the complications (cor pulmonale); examine the back as well as the front, because the posterior chest provides the best acoustic window to the lower lobes; and offer additional bedside tests (pulse oximetry, peak flow, sputum pot, inhaler technique), because the examination is not complete without them. [1]
The examination routine — the eleven-step sequence

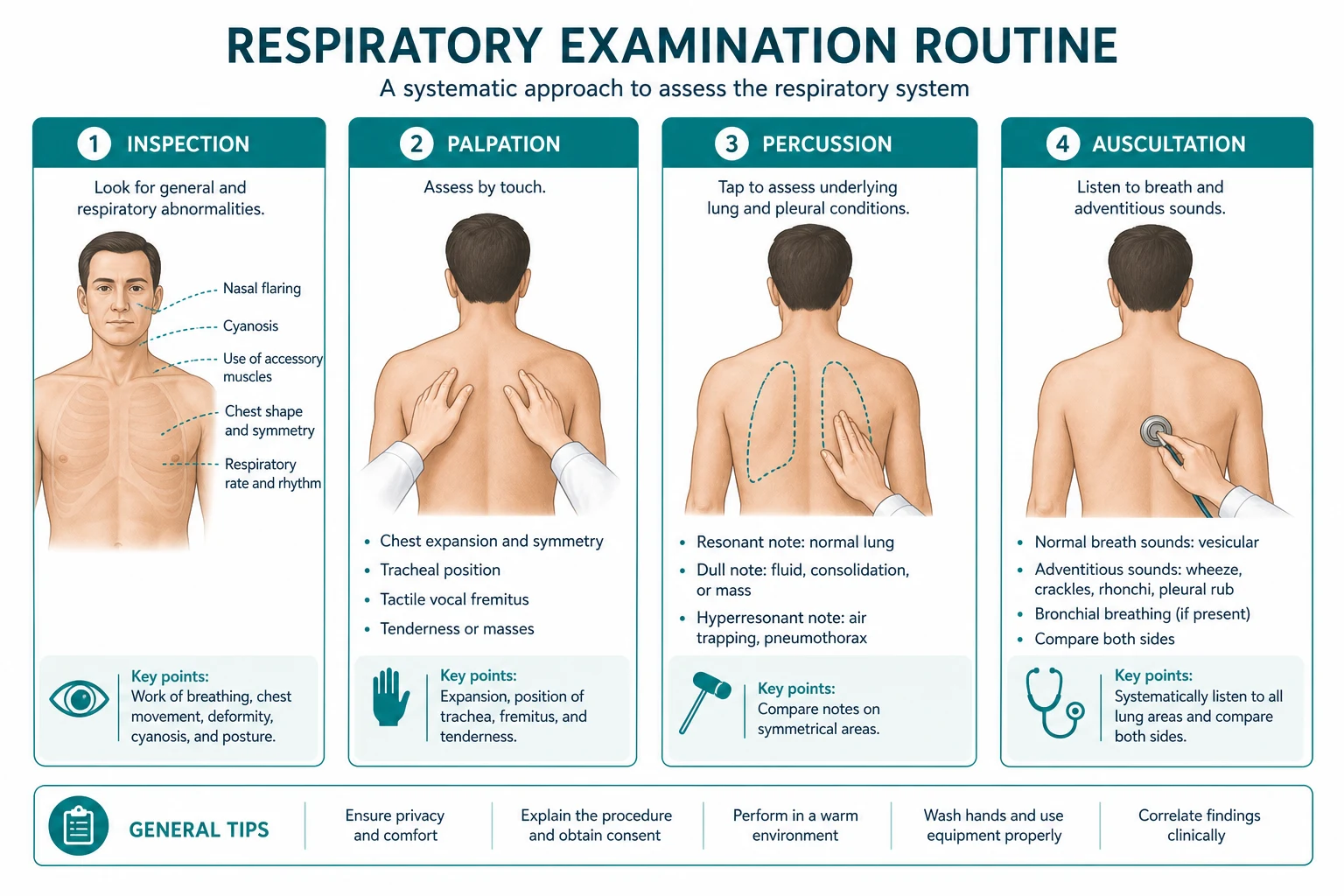
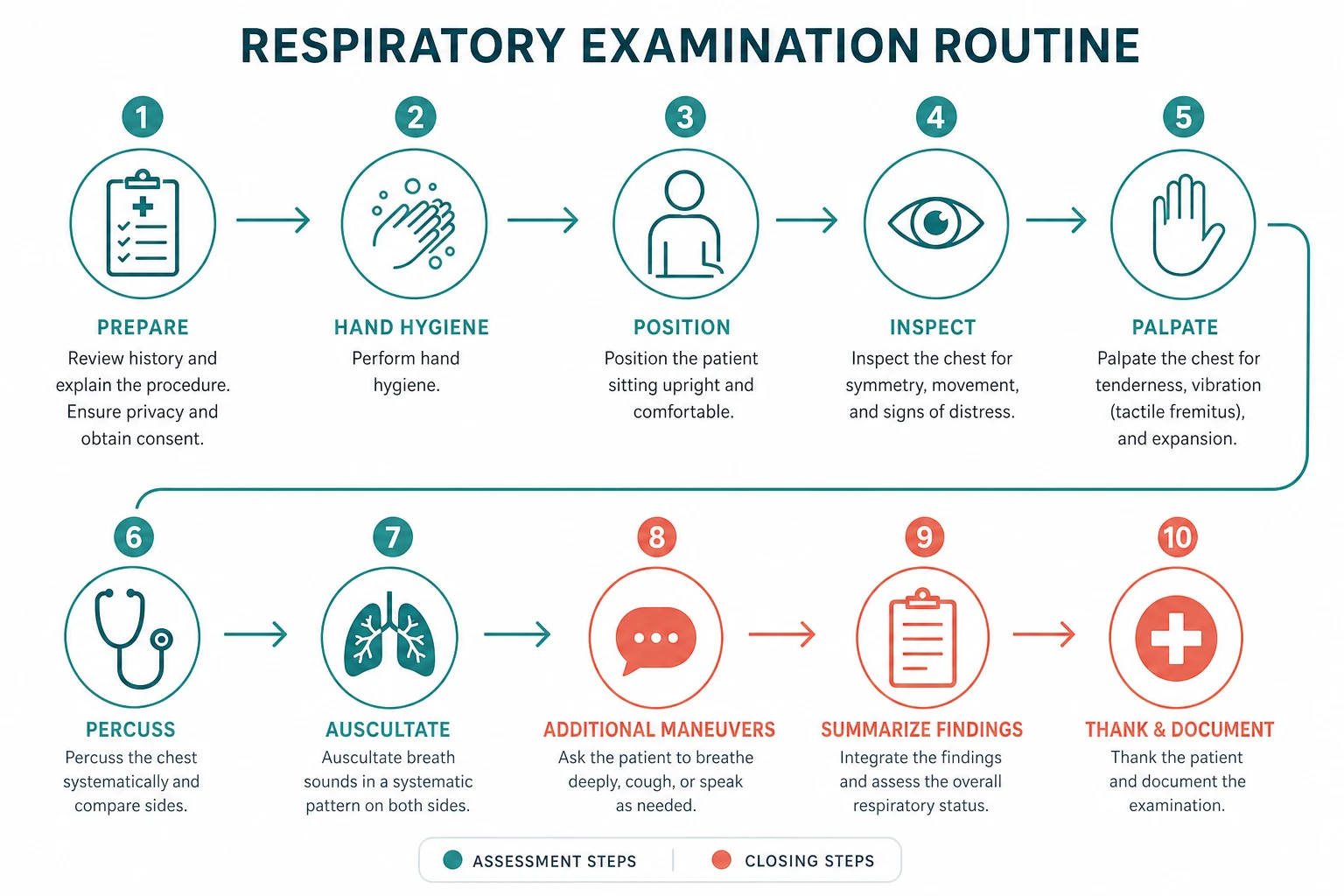
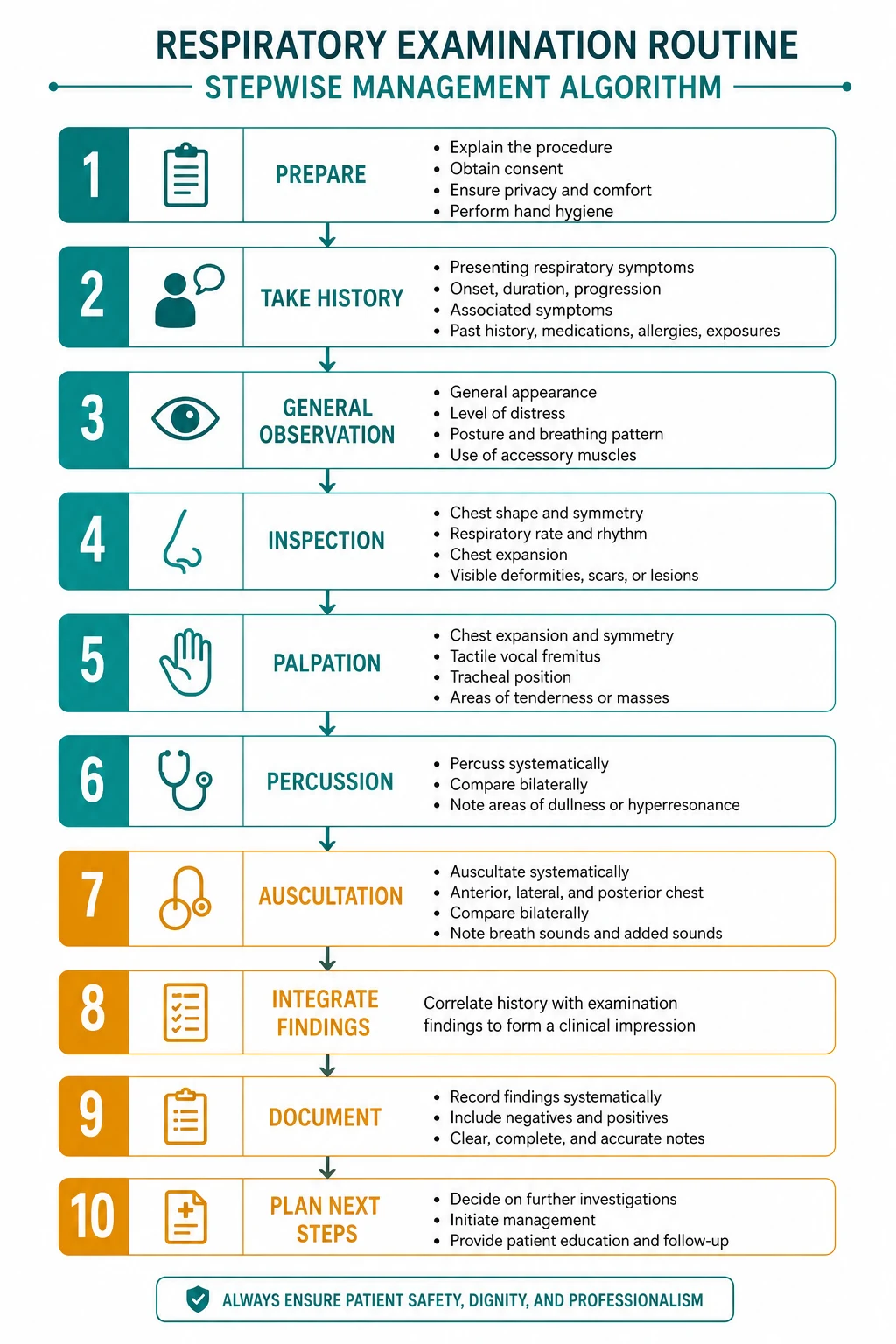
The respiratory examination follows the mnemonic IPAA (Inspection, Palpation, Percussion, Auscultation), applied systematically to the anterior chest and then the posterior chest, preceded by the end-of-bed assessment, the hands, the face and the neck, and followed by the legs and the additional bedside tests. The sequence is invariant and every candidate must perform it in the same order every time, so that the routine becomes automatic under examination pressure. [1]
Step 1 — The end of the bed
Before you touch the patient, stand at the end of the bed and take five seconds. The examiner is watching from this moment. What you see at the end of the bed often reveals the diagnosis: [1]
- Breathlessness — is the patient breathless at rest, on minimal exertion, or on conversation? The patient who cannot complete a sentence in one breath is in significant respiratory distress.
- Use of accessory muscles — the sternocleidomastoid, the scalenes, the intercostals, and the abdominal muscles. The patient who is tripoding (sitting forward, leaning on the arms) is using every available muscle to maintain the airway.
- Pursed-lip breathing — the characteristic breathing pattern of the COPD patient, who exhales through pursed lips to maintain a positive end-expiratory pressure that splints the small airways open.
- Barrel chest — the increased anteroposterior diameter of the hyperinflated chest (the normal AP-to-lateral ratio is less than 1:2; in hyperinflation it approaches 1:1).
- Cachexia — the muscle wasting of the patient with advanced lung cancer, severe COPD (the work of breathing consumes calories), or chronic infection.
- Cyanosis — central (bluish tongue and mucous membranes) versus peripheral (bluish fingers and toes with warm mucous membranes).
- Oxygen tubing — nasal cannulae, a Venturi mask (the precise oxygen concentration), a simple face mask. The fact that the patient is on oxygen tells you the disease is significant.
- Inhaler or spacer on the bedside table — the patient with obstructive airway disease (asthma or COPD).
- Position — sitting forward in respiratory distress (the tripoding position), or lying flat (orthopnoea suggests cardiac failure).
- Respiratory rate and pattern — count the rate for 30 seconds (the normal is 12 to 16). The pattern: Cheyne-Stokes (cardiac failure, neurological disease), Kussmaul (metabolic acidosis), rapid shallow breathing (restrictive disease, pulmonary embolism), or prolonged expiration (COPD). [1]
The teaching point: the respiratory rate is the most informative and the most neglected vital sign. A rate above 20 is tachypnoea; a rate above 30 is severe respiratory distress. Count it, document it, and act on it. [1]
Step 2 — The hands
The hands reveal the systemic signs that frame the differential before you reach the chest: [1]
- Clubbing — the loss of the nail-fold angle (Schamroth's window test: when the nails of the index fingers are placed together, the normal diamond-shaped window disappears in clubbing). Grade 1 (boggy nail bed), Grade 2 (loss of nail-fold angle), Grade 3 (bulbous, drumstick appearance), Grade 4 (periostosis with hypertrophic pulmonary osteoarthropathy). The lung causes of clubbing are lung cancer, bronchiectasis, pulmonary fibrosis (especially idiopathic pulmonary fibrosis and asbestosis), mesothelioma, and lung abscess or empyema. Clubbing does NOT occur in uncomplicated asthma or COPD — if the COPD patient has clubbing, there is a complication (lung cancer, bronchiectasis, or coexisting fibrosis) [4][5].
- Peripheral cyanosis — bluish discoloration of the fingers and toes with cold peripheries, caused by poor perfusion or vasoconstriction rather than arterial hypoxaemia.
- Fine tremor — from beta-agonist use (salbutamol, terbutaline). The tremor is present at rest and with the arms outstretched.
- Asterixis — the flapping tremor assessed with the patient holding the arms outstretched with the wrists dorsiflexed for 30 seconds. The sudden, irregular, downward flap of the hands indicates CO2 retention (the metabolic flap, NOT the liver flap — the same physical sign with a different significance in the respiratory patient).
- Tar staining — the yellow-brown staining of the fingers from cigarette smoking, localised to the index and middle fingers of the dominant hand.
- Peripheral stigmata of endocarditis (splinter haemorrhages, Osler nodes, Janeway lesions) and connective tissue disease (rheumatoid arthritis, systemic sclerosis, systemic lupus) — because these conditions cause respiratory disease.
Step 3 — The face
The face reveals signs that localise the disease: [1]
- Plethoric facies — the red, congested face of polycythaemia (secondary to chronic hypoxaemia in COPD, or primary polycythaemia rubra vera). The patient with a plethoric face and a smoker's cough has COPD with secondary polycythaemia.
- Horner syndrome — ptosis (drooping of the upper eyelid), miosis (constricted pupil), and anhidrosis (absent sweating on the affected side of the face). Horner syndrome in the respiratory patient indicates an apical lung tumour (Pancoast tumour) invading the cervical sympathetic chain. The tumour is in the superior sulcus, and Horner syndrome is present in about 25 per cent of cases [7].
- Nasal polyps — the pale, gelatinous, bilateral masses in the nasal cavity, associated with cystic fibrosis, allergic rhinitis, and aspirin-sensitive asthma (Samter's triad: asthma, nasal polyps, aspirin sensitivity).
- Central cyanosis — bluish discoloration of the tongue and the mucous membranes. Clinically detectable when deoxyhaemoglobin exceeds 5 g per dL, which means a polycythaemic patient shows cyanosis at a higher saturation and an anaemic patient may not show cyanosis until severely hypoxaemic.
- Oral candidiasis — the white patches on the tongue and buccal mucosa from inhaled corticosteroid use, a sign of poor inhaler technique and failure to rinse the mouth.
- Conjunctival pallor — anaemia (which worsens dyspnoea and may coexist with respiratory disease).
Step 4 — The neck
The neck reveals the tracheal position (localising the pathology) and the JVP (revealing the complications): [1]
- Jugular venous pressure (JVP) — elevated in right heart failure, cor pulmonale (the right heart failure of chronic lung disease), pulmonary embolism, and tricuspid regurgitation. A raised JVP in a patient with COPD or pulmonary fibrosis suggests cor pulmonale.
- Tracheal position — place the index and middle fingers in the suprasternal notch. The trachea is central in health. Deviated AWAY from a space-occupying lesion (tension pneumothorax, large pleural effusion). Deviated TOWARDS a volume-loss lesion (atelectasis, lung collapse, pulmonary fibrosis, pneumonectomy). The way to remember: air and fluid push; scar and collapse pull [2][3].
- Cricosternal distance — the gap between the cricoid cartilage and the sternal notch. Reduced (less than 3 cm) in hyperinflation (the diaphragm is flattened and the chest is held in the inspiratory position).
- Tracheal tug — the downward movement of the thyroid cartilage on inspiration, indicating severe hyperinflation with a flattened diaphragm that pulls on the mediastinum.
- Cervical and supraclavicular lymphadenopathy — the Virchow node (left supraclavicular) in lung cancer; the generalized lymphadenopathy in lymphoma, sarcoidosis, and tuberculosis.
Step 5 — Anterior chest: inspection
Inspect the chest for: [1]
- Shape — barrel chest (hyperinflation), pectus excavatum (funnel chest, congenital depression of the sternum), pectus carinatum (pigeon chest, congenital protrusion of the sternum), kyphoscoliosis (the spinal deformity that restricts lung expansion).
- Symmetry — the two sides should move equally with respiration. Asymmetry of movement is a significant finding.
- Scars — thoracotomy (the posterolateral incision for lung resection, pneumothorax repair, or pleural procedures), chest drain sites (the small scars at the second intercostal space anteriorly or the fifth intercostal space mid-axillary line), median sternotomy (cardiac surgery), and video-assisted thoracoscopic surgery (VATS) scars (the small port-site scars).
- Respiratory rate and pattern — counted again from the end of the bed, confirming the earlier observation. [1]
Step 6 — Anterior chest: palpation
- Chest expansion — place the hands firmly on the lower chest wall with the thumbs meeting in the midline and the fingers gripping the lateral chest wall. Ask the patient to take a deep breath in. The thumbs move apart symmetrically (normal). Reduced expansion on one side indicates pathology on that side (consolidation, effusion, pneumothorax, collapse, fibrosis). Reduced expansion bilaterally suggests COPD, restrictive disease (pulmonary fibrosis, ankylosing spondylitis, kyphoscoliosis), or bilateral effusions. The normal expansion is at least 5 cm.
- Tactile vocal fremitus — place the flat of the distal phalanx of the index finger on the chest wall, ask the patient to say "ninety-nine," and compare symmetrical areas. Increased fremitus indicates consolidation (the solid lung conducts the vibration); decreased fremitus indicates pleural effusion or pneumothorax (the fluid or air blocks the vibration). Most modern examinations use vocal resonance (the auscultatory equivalent) preferentially [1].
- Apex beat — displaced by a tension pneumothorax or a large pleural effusion (pushed away), or by a lung collapse or fibrosis (pulled towards). The apex beat position confirms the tracheal deviation finding.
Step 7 — Anterior chest: percussion
Percuss symmetrically, comparing right with left at each level. The four cardinal percussion notes: [1]

- Resonant — the normal lung (and the hyperinflated lung of COPD, which is still resonant but with a lower-pitched, more drum-like quality).
- Dull — consolidation (pneumonia), collapse, or a solid mass. The dullness is the same quality as percussion over the liver or the heart.
- Stony dull — pleural effusion. The very short, thuddy, low-pitched note of a fluid-filled space, qualitatively different from the dullness of consolidation. This is the single most useful percussion finding in the short case [3].
- Hyperresonant — pneumothorax or severe hyperinflation. The increased resonance of an air-filled space, like percussion over a distended abdomen.
The teaching point: the distinction between dull (solid lung) and stony dull (fluid in the pleural space) is the single most useful percussion finding in the respiratory short case. The examiner may ask you to describe the quality of the dullness, and the correct answer (stony dull for effusion, dull for consolidation) demonstrates the discriminating ear. [1]
Step 8 — Anterior chest: auscultation
Auscultate symmetrically, comparing right with left at each level, using the diaphragm of the stethoscope. Listen to: [1]
- Breath sounds — vesicular (the normal, soft, low-pitched sound with a longer inspiratory than expiratory phase) or bronchial (the abnormal, loud, high-pitched sound with an equal or longer expiratory phase, heard normally over the trachea but abnormally at the lung periphery in consolidation).
- Added sounds:
- Crackles (rales): fine (late-inspiratory, high-pitched, Velcro-like, NOT clearing with coughing — interstitial lung disease, early pulmonary oedema) versus coarse (mid-inspiratory, low-pitched, bubbling, MAY clear with coughing — pneumonia, bronchiectasis, chronic bronchitis) [1].
- Wheeze: the high-pitched, musical, expiratory sound of airway narrowing (asthma, COPD). Wheeze is not an all-or-nothing finding — the severity of airway obstruction correlates with the pitch and the duration of the wheeze, not the volume. The silent chest (no wheeze in a distressed patient) is a sign of life-threatening asthma with insufficient airflow to generate a sound.
- Pleural rub: the creaking, leathery sound of inflamed pleural surfaces rubbing together (pleurisy, pulmonary embolism with infarction).
- Vocal resonance — ask the patient to say "ninety-nine" and auscultate. Increased vocal resonance indicates consolidation; decreased vocal resonance indicates pleural effusion or pneumothorax. The pathognomonic findings are whispering pectoriloquy (the whispered voice is transmitted clearly and distinctly through consolidated lung, as if the patient is whispering directly into the stethoscope) and aegophony (the spoken voice has a bleating, nasal, goat-like quality, because the higher frequencies are transmitted preferentially through the solid lung).
Step 9 — Posterior chest: the same IPAA sequence
Ask the patient to sit forward (cross the arms in front to move the scapulae laterally and expose more lung). Repeat the entire IPAA sequence on the back: [1]
- Inspection — scars, symmetry, and the spinal deformity (kyphoscoliosis).
- Palpation — chest expansion (posteriorly, the same technique as anteriorly) and tactile vocal fremitus.
- Percussion — compare right with left at each level, percussing from the apices to the bases.
- Auscultation — breath sounds, added sounds, and vocal resonance. [1]
The posterior chest provides the best acoustic window to the lower lobes — the largest lung segments and the most common site of pathology. The candidate who percusses and auscultates only the anterior chest has missed half the examination. Check for sacral oedema (a sign of right heart failure or cor pulmonale). [1]
Step 10 — The legs
The legs reveal the complications of respiratory disease: [1]
- DVT signs — calf swelling, tenderness, warmth, and a positive Homan's sign (calf pain on dorsiflexion of the foot). The deep vein thrombosis is the source of the pulmonary embolism, and a breathless patient with a swollen, tender calf has a pulmonary embolism until proven otherwise.
- Peripheral oedema — the pitting oedema of right heart failure, cor pulmonale, or pulmonary hypertension. The level of the oedema (ankles, mid-shin, knee, thigh, sacral) reflects the severity of the venous congestion.
- Peripheral pulses — the dorsalis pedis and posterior tibial pulses, assessed for symmetry and quality. [1]
Step 11 — Additional bedside tests
The examination is not complete without offering the additional bedside tests: [1]
- Pulse oximetry — the SpO2 on room air or on the prescribed oxygen. A normal SpO2 does not exclude CO2 retention.
- Peak expiratory flow rate — for the asthmatic patient (compare to the predicted or the patient's best).
- Sputum pot — note the colour (white, yellow, green, rusty, blood-stained), the volume, and the presence of haemoptysis.
- Inhaler technique check — ask the patient to demonstrate their technique with their own inhaler device. Poor technique is the single most common reason for treatment failure.
- Spirometry — for the COPD patient (the FEV1/FVC ratio, the FEV1 per cent predicted, the reversibility).
- Chest X-ray — to confirm the clinical findings (effusion, consolidation, pneumothorax, hyperinflation, masses, interstitial changes). [1]
The chest signs — the four cardinal patterns
The four cardinal chest signs and their patterns are the diagnostic core of the respiratory examination. Each pattern combines the percussion note, the breath sounds, the vocal resonance, and the chest expansion into a signature that names the diagnosis: [1]
| Finding | Consolidation | Pleural effusion | Pneumothorax | Collapse/fibrosis |
|---|---|---|---|---|
| Expansion | Reduced on affected side | Reduced on affected side | Reduced on affected side | Reduced on affected side |
| Percussion | Dull | Stony dull | Hyperresonant | Dull |
| Breath sounds | Bronchial | Absent or reduced | Absent or reduced | Reduced or absent |
| Vocal resonance | Increased (whispering pectoriloquy, aegophony) | Decreased or absent | Decreased | Decreased |
| Added sounds | Coarse crackles (from exudate) | None (or a pleural rub at the upper margin) | None | Fine crackles (if fibrosis) |
| Trachea | Central | Pushed away (if large) | Pushed away (if tension) | Pulled towards |
| Pathology | Lobar pneumonia | Heart failure, malignancy, empyema, parapneumonic | Spontaneous, traumatic, iatrogenic | Atelectasis, post-surgical, pulmonary fibrosis |
The exam principle: the examiner will give you a short case and expect you to elicit the pattern (the combination of percussion, breath sounds, vocal resonance and expansion) and name the diagnosis. A patient with reduced expansion, dull percussion, bronchial breath sounds, increased vocal resonance with whispering pectoriloquy, and coarse crackles has consolidation from lobar pneumonia. A patient with reduced expansion, stony dull percussion, absent breath sounds, and reduced vocal resonance has a pleural effusion. A patient with reduced expansion, hyperresonant percussion, and absent breath sounds has a pneumothorax [2][3].
Clubbing — the single most important hand finding

Digital clubbing is the selective enlargement of the distal segments of the fingers (and toes) caused by the proliferation of connective tissue between the nail matrix and the distal phalanx. The pathophysiology involves the failure of the pulmonary circulation to filter megakaryocyte fragments and platelet-derived growth factors, which lodge in the digital capillary beds and stimulate connective tissue proliferation [4][5].
The lung causes of clubbing (the mnemonic to memorise): [1]
- Lung cancer — the most common cause in adults, especially non-small cell lung cancer (adenocarcinoma).
- Bronchiectasis — the chronic suppurative lung disease with permanently dilated bronchi.
- Pulmonary fibrosis — especially idiopathic pulmonary fibrosis and asbestosis [6].
- Mesothelioma — the malignant tumour of the pleura, strongly associated with asbestos exposure.
- Lung abscess or empyema — the chronic suppurative conditions.
Clubbing does NOT occur in uncomplicated asthma or COPD. This is the single most important point about clubbing in the respiratory examination. If the COPD patient has clubbing, there is a complication: lung cancer (the COPD patient who develops clubbing and weight loss), bronchiectasis (the COPD patient with chronic productive cough and daily purulent sputum), or coexisting pulmonary fibrosis (the combined pulmonary fibrosis and emphysema syndrome). The asthmatic with clubbing has a wrong diagnosis: the correct diagnosis is bronchiectasis, pulmonary fibrosis, or lung cancer. [1]
The non-lung causes of clubbing (relevant to the respiratory patient because they may coexist): infective endocarditis, cyanotic congenital heart disease, inflammatory bowel disease (Crohn disease, ulcerative colitis), coeliac disease, cirrhosis, and hyperthyroidism (thyroid acropachy). [1]
The presentation template
The model presentation follows a fixed structure: the summary statement, the positive findings grouped by system, the relevant negatives, the differential diagnosis, and the proposed investigation plan. The presentation takes under two minutes and the examiner can interrupt at any point to probe. [1]
Model presentation — consolidation (lobar pneumonia): [1]
"On general inspection, the patient is breathless at rest with an increased respiratory rate of 24. In the hands, there is no finger clubbing, no peripheral cyanosis, and no asterixis. In the face, there is no Horner syndrome and no central cyanosis; there is flushing consistent with fever. In the neck, the JVP is not elevated and the trachea is central. On examination of the chest, there is reduced expansion on the right side. Percussion is dull at the right lower zone. Auscultation reveals bronchial breath sounds and coarse crackles at the right lower zone, with increased vocal resonance and whispering pectoriloquy. The left side is normal. Posteriorly, the findings are confirmed, with no sacral oedema. In the legs, there is no peripheral oedema or DVT. These findings are consistent with right lower lobe consolidation. My differential diagnosis is lobar pneumonia, and I would like to check the temperature, the oxygen saturation, and order a chest X-ray and blood cultures." [1]
Model presentation — pleural effusion: [1]
"On general inspection, the patient is comfortable at rest. In the hands, there is grade 2 finger clubbing with no peripheral cyanosis. In the neck, the JVP is not elevated and the trachea is central. On examination of the chest, there is reduced expansion on the right side. Percussion is stony dull from the right mid-zone to the base. Auscultation reveals absent breath sounds and reduced vocal resonance at the right base, with normal vesicular breath sounds at the right apex. The left side is normal. These findings are consistent with a right-sided pleural effusion. Given the clubbing, my differential diagnosis includes a malignant pleural effusion, a parapneumonic effusion, and a tuberculous effusion. I would like to order a chest X-ray, a diagnostic pleural aspiration with fluid sent for protein, LDH, glucose, pH, cell count, culture, and cytology, and apply Light's criteria to classify the effusion as a transudate or an exudate." [1]
Model presentation — COPD with cor pulmonale: [1]
"On general inspection, the patient is cachectic with a barrel-shaped chest, pursed-lip breathing, and the use of accessory muscles. There is oxygen tubing in situ. In the hands, there is no finger clubbing (an important negative — if clubbing were present, I would investigate for a complication), a fine tremor consistent with beta-agonist use, and no asterixis. In the face, there is a plethoric complexion. In the neck, the JVP is elevated 4 cm. On examination of the chest, there is reduced expansion bilaterally, a hyperresonant percussion note, globally reduced breath sounds with expiratory wheeze, and no crackles. Posteriorly, there are bilateral coarse crackles at the bases. In the legs, there is peripheral oedema to the mid-shin. These findings are consistent with COPD complicated by an infective exacerbation and cor pulmonale. I would like to check the oxygen saturation, an arterial blood gas for CO2 retention, a chest X-ray, and the inhaler technique." [1]
Examiner discussion questions — by finding
The examiner will ask probing questions after the examination. The common questions and the model answers: [1]
Q: "What is the significance of clubbing in your patient?" [1]
"Clubbing does not occur in uncomplicated COPD or asthma. The lung causes are lung cancer, bronchiectasis, pulmonary fibrosis, mesothelioma, and lung abscess or empyema. In this patient with COPD, the presence of clubbing would prompt me to investigate for a complication — a chest X-ray and a CT chest to look for lung cancer, bronchiectasis, or coexisting pulmonary fibrosis. The non-lung causes I would also consider are infective endocarditis, inflammatory bowel disease, and cirrhosis, depending on the clinical context." [4][5]
Q: "What is the significance of a stony dull percussion note?" [1]
"Stony dullness is the characteristic percussion note of a pleural effusion. The quality is different from the dullness of consolidation — it is shorter, lower-pitched, and thuddier. My next step is a chest X-ray to confirm the effusion, then a diagnostic pleural aspiration with the fluid sent for protein, LDH, glucose, pH, cell count, culture, and cytology. I would apply Light's criteria to classify the effusion: if the pleural-to-serum protein ratio is above 0.5 or the pleural-to-serum LDH ratio is above 0.6, the effusion is an exudate (malignancy, infection, pulmonary embolism); if neither criterion is met, it is a transudate (heart failure, cirrhosis, nephrotic syndrome)." [3]
Q: "What is the significance of fine versus coarse crackles?" [1]
"Fine crackles are late-inspiratory, high-pitched, and Velcro-like, and they do not clear with coughing. They indicate interstitial lung disease (especially idiopathic pulmonary fibrosis) or early pulmonary oedema. Coarse crackles are mid-inspiratory, low-pitched, and bubbling, and they may clear with coughing. They indicate pneumonia, bronchiectasis, or chronic bronchitis. The crackles that clear with coughing are secretions; the crackles that persist are parenchymal." [1]
Q: "What is the significance of the tracheal deviation?" [1]
"The trachea is pushed away from a space-occupying lesion — a tension pneumothorax or a large pleural effusion — and pulled towards a volume-loss lesion — atelectasis, lung collapse, pulmonary fibrosis, or pneumonectomy. The way to remember: air and fluid push; scar and collapse pull. In this patient with a deviated trachea, I would assess the percussion note and the breath sounds to determine the cause: if the trachea is pushed away and the percussion is stony dull, it is a large pleural effusion; if the trachea is pushed away and the percussion is hyperresonant, it is a tension pneumothorax; if the trachea is pulled towards and the percussion is dull, it is a collapse or fibrosis." [2]
Q: "What is the significance of a raised JVP in the respiratory patient?" [1]
"A raised JVP in the respiratory patient suggests cor pulmonale — the right heart failure of chronic lung disease. The mechanism is pulmonary hypertension (the pulmonary vascular resistance rises from chronic hypoxaemia, from the destruction of the pulmonary vascular bed in emphysema or fibrosis, or from recurrent pulmonary embolism), which leads to right ventricular hypertrophy and eventually right ventricular failure. The signs are a raised JVP, a parasternal heave, a tricuspid regurgitation murmur, a loud pulmonary component of the second heart sound, and peripheral and sacral oedema. I would confirm the diagnosis with an echocardiogram." [1]
Q: "What is the significance of asterixis in the respiratory patient?" [1]
"Asterixis (the metabolic flap) in the respiratory patient indicates CO2 retention, not hepatic failure. The patient with COPD who has a flapping tremor when the hands are held in dorsiflexion is retaining carbon dioxide, and I need an arterial blood gas immediately. The finding may indicate type 2 respiratory failure (a high PaCO2 with a low pH), which may require non-invasive ventilation. The same physical sign is called the liver flap in the hepatic patient and the metabolic flap in the renal patient, but in the respiratory patient, the mechanism is the depressant effect of CO2 on the central nervous system." [1]
High-yield exam traps
- The omitted end-of-bed inspection. The five-second observation reveals the diagnosis in a significant proportion of cases. The candidate who walks straight to the chest has demonstrated a failure of the systematic approach and has lost the first-impression marks.
- The clubbing trap. Clubbing does NOT occur in uncomplicated asthma or COPD. If the COPD patient has clubbing, there is a complication. The lung causes are lung cancer, bronchiectasis, pulmonary fibrosis, mesothelioma, and lung abscess or empyema [4][5].
- The asterixis trap. Asterixis in the respiratory patient indicates CO2 retention, not hepatic failure. Check an arterial blood gas.
- The tracheal deviation trap. The trachea is pushed AWAY from a space-occupying lesion (tension pneumothorax, large effusion) and pulled TOWARDS a volume-loss lesion (collapse, fibrosis, pneumonectomy). Air and fluid push; scar and collapse pull [2][3].
- The percussion note trap. Stony dullness is qualitatively different from dullness. Stony dull is the very short, thuddy, low-pitched note of a pleural effusion; dull is the note of consolidation [3].
- The bronchial breathing trap. Bronchial breath sounds at the lung periphery indicate consolidation. The candidate who describes central bronchial breath sounds (heard normally over the trachea) as a finding has described a normal variant.
- The crackles trap. Fine crackles (late-inspiratory, Velcro-like, not clearing with coughing) indicate interstitial lung disease or pulmonary oedema. Coarse crackles (mid-inspiratory, bubbling, clearing with coughing) indicate pneumonia or bronchiectasis. The crackles that clear with coughing are secretions [1].
- The Horner syndrome trap. Horner syndrome (ptosis, miosis, anhidrosis) in the respiratory patient indicates an apical lung tumour (Pancoast tumour). The tumour invades the cervical sympathetic chain, and the sign is present in about 25 per cent of superior sulcus tumours [7].
- The silent chest trap. A silent chest (no wheeze in a distressed asthmatic) is a sign of life-threatening asthma with insufficient airflow to generate a sound. It is a pre-arrest sign requiring immediate intervention, not a sign of improvement.
- The incomplete examination trap. The candidate who percusses and auscultates only the anterior chest has missed the examination. The posterior chest provides the best acoustic window to the lower lobes, and the back is where the consolidation, the effusion, the fibrosis, and the crackles are most often heard.
Key points for the viva
- The respiratory examination follows an invariant eleven-step sequence: end of bed, hands, face, neck, anterior chest (IPAA), posterior chest (IPAA), legs, additional bedside tests. Perform it in the same order every time.
- The single most important principle is asymmetry — compare the two sides of the chest at every step. The finding that one side is different is the finding that localises the pathology.
- The five-second end-of-bed inspection reveals the diagnosis in a significant proportion of cases. Never skip it.
- Clubbing does NOT occur in uncomplicated asthma or COPD. The lung causes are lung cancer, bronchiectasis, pulmonary fibrosis, mesothelioma, and lung abscess or empyema.
- The four cardinal percussion notes are resonant (normal), dull (consolidation), stony dull (effusion), and hyperresonant (pneumothorax). The distinction between dull and stony dull is the single most useful percussion finding.
- Fine crackles indicate interstitial lung disease; coarse crackles indicate infection or bronchiectasis. The crackles that clear with coughing are secretions.
- The trachea is pushed away from a space-occupying lesion and pulled towards a volume-loss lesion. Air and fluid push; scar and collapse pull.
- Asterixis in the respiratory patient indicates CO2 retention — check an arterial blood gas.
- Horner syndrome indicates an apical lung tumour (Pancoast tumour) until proven otherwise.
- The examination is not complete without the additional bedside tests: pulse oximetry, peak flow, sputum pot, and inhaler technique. [1]
References
- [1]Bohadana A, Izbicki G, Kraman SS Fundamentals of lung auscultation N Engl J Med, 2014.PMID 24552321
- [2]MacDuff A, Arnold A, Harvey J; BTS Pleural Disease Guideline Group Management of spontaneous pneumothorax: British Thoracic Society Pleural Disease Guideline 2010 Thorax, 2010.PMID 20696690
- [3]Hooper C, Lee YCG, Maskell N; BTS Pleural Guideline Group Investigation of a unilateral pleural effusion in adults: British Thoracic Society Pleural Disease Guideline 2010 Thorax, 2010.PMID 20696692
- [4]Sarkar M, Mahesh DM, Madabhavi I Digital clubbing Lung India, 2012.PMID 23243350
- [5]Burcovschii S, Aboeed A. Nail Clubbing 2026.PMID 30969535
- [6]Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline Am J Respir Crit Care Med, 2018.PMID 30168753
- [7]Fatima SA, Rauf MA. Lung Pancoast Tumor 2026.PMID 32310569