Phys · general-medicine
Rheumatological Examination of the Hands — The DCE Short-Case Routine
Also known as hand examination · rheumatological examination of the hands · examine this patient hands · examination of the hands · hand examination rheumatology · DCE short case hands · PACES hand examination · Heberden nodes · Bouchard nodes · swan-neck deformity · boutonniere deformity · ulnar deviation · Z-deformity thumb · dactylitis · sausage digit · Jaccoud arthropathy · sclerodactyly · Gottron papules · rheumatoid nodules · gouty tophi · DAS28 joint count · carpal tunnel syndrome examination · Phalen test · Tinel sign · Dupuytren contracture
Consultant-physician-depth guide to the systematic rheumatological examination of the hands for the FRACP DCE short case and the MRCP PACES Station 3 — the single most frequently set short case in the examination. Covers the six-step routine (inspection, palpation, range of motion, function, additional sites, neurovascular), the discriminating deformities of RA (ulnar deviation, swan-neck, boutonniere, Z-deformity thumb), OA (Heberden and Bouchard nodes, first CMC squaring), PsA (dactylitis, nail pitting, onycholysis), gout (tophi), SLE (Jaccoud arthropathy), SSc (sclerodactyly) and dermatomyositis (Gottron papules), the synovitis versus bony swelling distinction, the DAS28 joint count, the carpal tunnel bedside tests, the say-aloud presentation templates, and the examiner discussion questions by finding.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Rheumatological Examination of the Hands — The DCE Short-Case Routine

The answer first
The instruction "Please examine this patient's hands" is the single most frequently set short case in the FRACP DCE and the most common station in the MRCP PACES examination. The reason is simple: the hands carry more diagnostic information per square centimetre than any other body system. A thirty-second inspection from the foot of the bed can declare rheumatoid arthritis, osteoarthritis, psoriatic arthritis, gout, systemic sclerosis, dermatomyositis, or a connective tissue disease — and each declaration changes the entire examination trajectory. The examiners are testing whether you can perform a fluent, systematic, reproducible routine, elicit and interpret the discriminating signs, and present a diagnosis supported by the evidence at the bedside. [1]
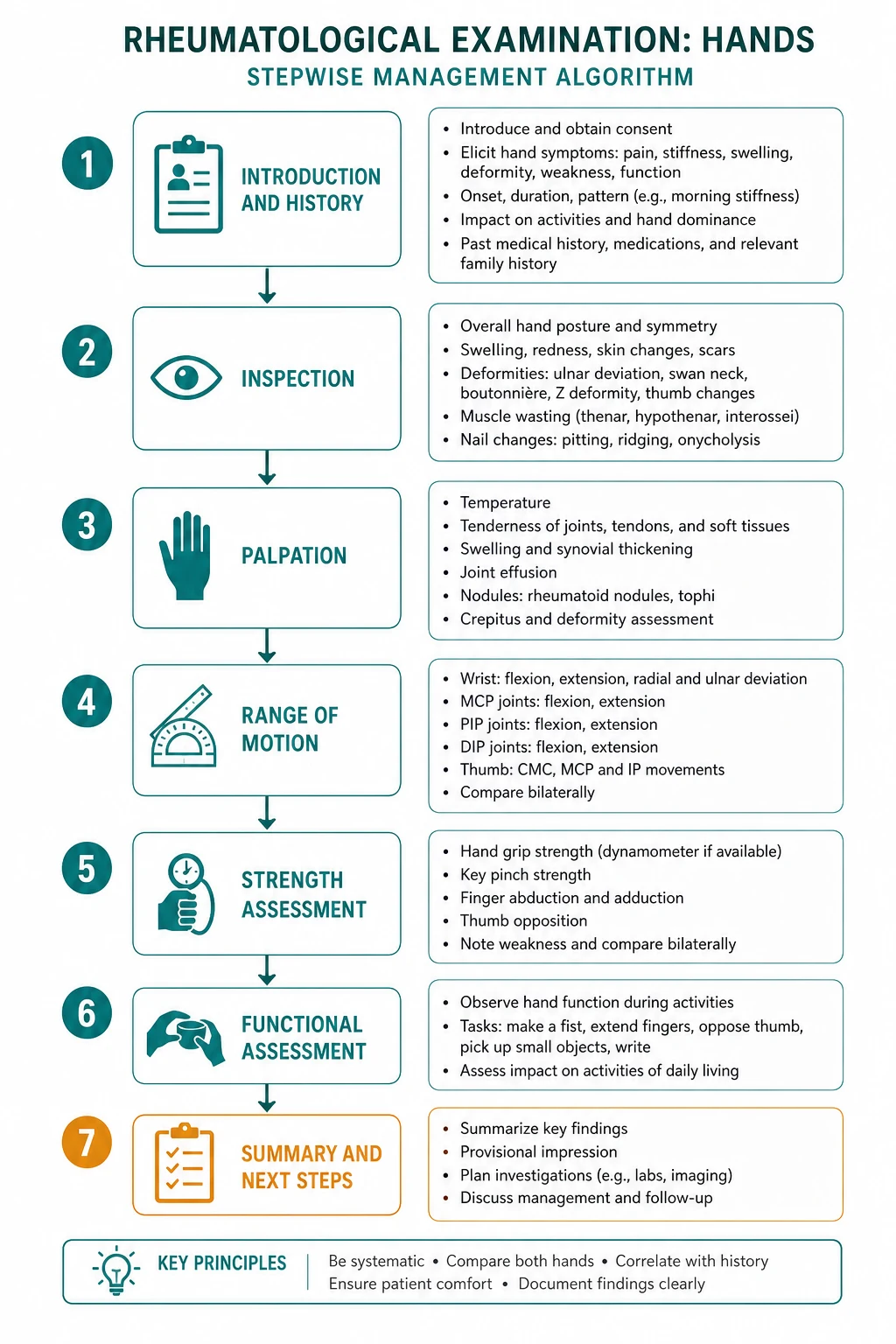
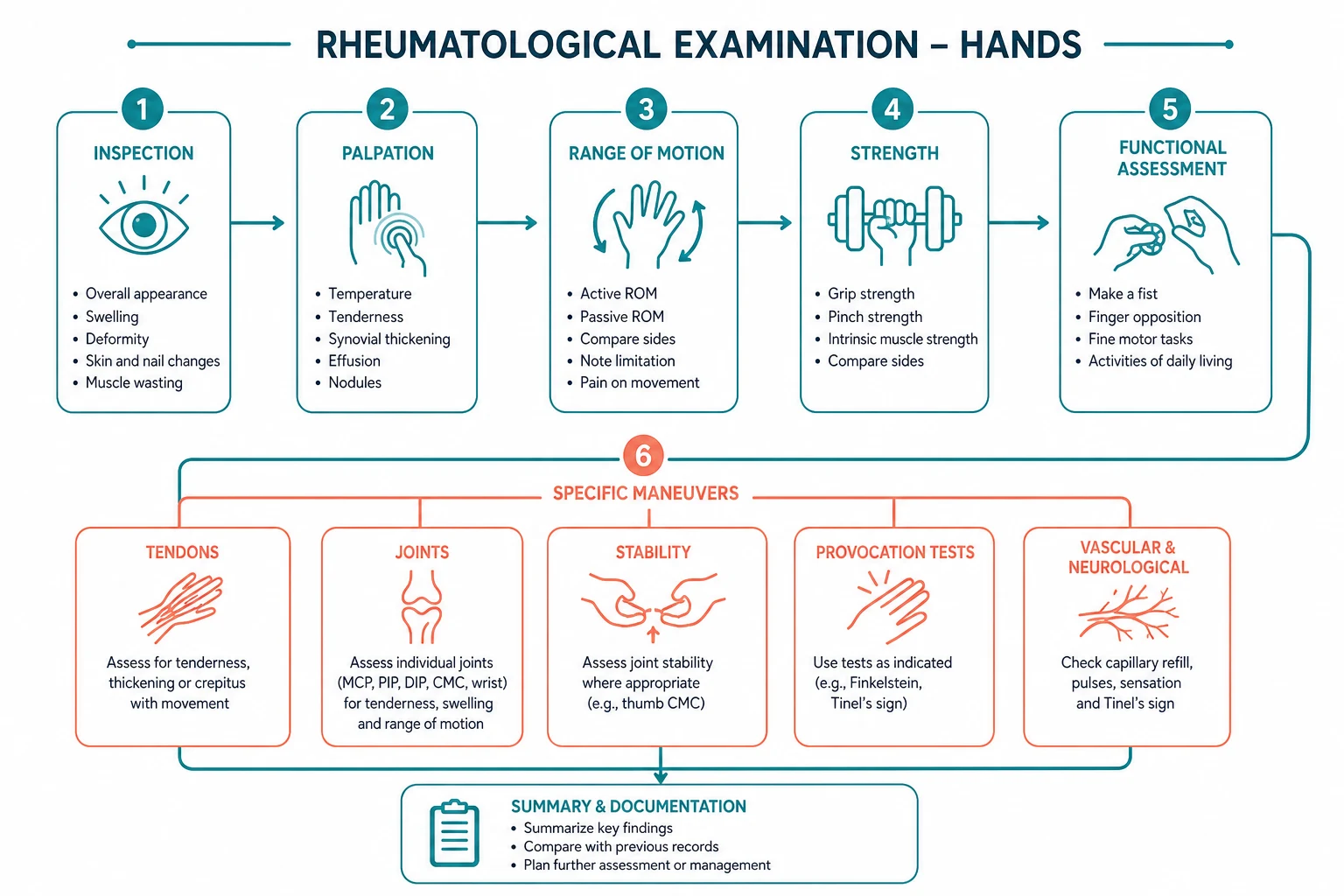
The routine is six steps, performed in the same order every time: [1]
- Inspection — posture, dexterity, swelling, deformity, skin, nails
- Palpation — temperature, sweating, texture, tenderness, crepitus
- Range of motion — active then passive at the MCPs, PIPs, DIPs, wrists, thumbs
- Function — grip, pinch, write, pick up a coin, turn a key
- Additional — elbows, shoulders, spine if relevant
- Neurovascular — pulses, sensation, Tinel sign, Phalen test [1]
The candidate who skips from inspection straight to a diagnosis, without palpating the joints for synovitis or testing function, has performed an incomplete examination and has forfeited the marks for the routine. The six steps are not optional — they are the sequence the examiner expects, and the sequence in which the findings declare the disease. [1]
Viva trap: "What is the single most discriminating observation in the first thirty seconds?" The honest answer is the type of swelling and the distribution of the deformity. The candidate who distinguishes symmetrical MCP and PIP synovitis with prolonged morning stiffness (rheumatoid arthritis) from asymmetrical bony hard nodes at the DIP and PIP with brief stiffness (osteoarthritis) has generated the differential before touching the patient. The candidate who calls all swelling "arthritis" has lost the diagnosis. [1]

Setting up and the opening from the foot of the bed
Position the patient seated comfortably at your eye level with both hands and forearms fully exposed to above the elbows. Support the hands on a pillow on the patient's lap, palms down for the dorsal inspection, then palms up for the volar inspection. State your plan aloud: "I will examine this patient's hands systematically — inspection, palpation, range of movement, function, related sites, and a neurovascular assessment." [1]
Before you touch the patient, ask them to perform a functional task: button and unbutton a shirt, or undo and redo a button on their sleeve. This is the single highest-yield opening maneuver because it reveals pain, stiffness, dexterity, grip, pinch, and the adaptive strategies the patient has developed — all in ten seconds. A patient who struggles to fasten a button has functional impairment, and the quality of the struggle (which fingers, which movement, which compensation) frames the rest of the examination. [1]
Step 1 — Inspection: the thirty seconds that generate the differential
Inspect the dorsum of both hands first, comparing left with right, then the palms. The five observations that frame the rheumatological differential are posture and alignment, the type and distribution of swelling, the deformities, the skin changes, and the nail changes. [1]
Swelling — synovitic versus bony is the first fork
The type of joint swelling is the first and most important discriminating observation, because it separates inflammatory from mechanical arthritis at a glance. [1]
Soft, boggy, fusiform swelling around a joint — the joint looks swollen, the skin contour is full, and the swelling has a fluid or doughy quality — is synovitis. Synovitis is the hallmark of inflammatory arthritis: rheumatoid arthritis, psoriatic arthritis, and the spondyloarthropathies. The swelling is tender and warm on palpation (Step 2 confirms this). The distribution is typically symmetrical in RA (both hands, MCPs and PIPs) and asymmetrical in PsA (one finger, or dactylitis of a single digit). [1]
Hard, bony, irregular swelling at a joint — the joint looks knobbly, the swelling is firm and non-tender, and the skin moves freely over it — is osteophyte formation, the hallmark of osteoarthritis. The distribution is characteristically asymmetrical and involves the DIP (Heberden nodes), the PIP (Bouchard nodes), and the first carpometacarpal joint (squaring of the thumb base). [1]
This single distinction — soft-boggy-symmetrical versus hard-bony-asymmetrical — separates RA from OA before a single joint is palpated. Every subsequent observation builds on this fork. [1]
Deformities — the pattern identifies the disease

Rheumatoid arthritis deformities
Rheumatoid arthritis is a symmetrical, small-joint polyarthritis that predominantly affects the MCP joints and the PIP joints and the wrists, with sparing of the DIP joints. The deformities arise from synovial proliferation, pannus formation, and the progressive destruction of cartilage, bone, ligaments and tendons. The classic RA hand shows several recognisable patterns [1]:
- Ulnar deviation of the fingers at the MCP joints — the fingers drift ulnarly (toward the little finger) at the knuckles. This results from stretching of the radial collateral ligaments and the extensor tendons sliding ulnarly off the metacarpal heads. The MCPs also show palmar subluxation (the proximal phalanx slides off the palmar surface of the metacarpal head) and radial deviation of the wrist (the wrist deviates radially to compensate), producing the classic zigzag deformity of the rheumatoid hand.
- Swan-neck deformity — hyperextension of the PIP joint with flexion of the DIP joint. The mechanism is imbalance between the flexor and extensor mechanisms: the intrinsic muscles (lumbricals and interossei) tighten and pull the extensor hood proximally, causing PIP hyperextension, while the flexor digitorum superficialis insertion is overridden, allowing the DIP to flex.
- Boutonniere deformity — flexion of the PIP joint with hyperextension of the DIP joint. The name means "buttonhole" — the central slip of the extensor tendon ruptures at its insertion on the base of the middle phalanx, and the lateral bands slip volarly (palmarly) through the gap like a button through a buttonhole, turning them from extensors into flexors of the PIP. This is the mirror image of the swan-neck.
- Z-deformity of the thumb — hyperextension of the interphalangeal joint with flexion of the MCP joint, giving the thumb a Z shape. The mechanism is the same intrinsic-extensor imbalance applied to the thumb.
- Ulnar head prominence (caput ulnae syndrome) — the distal ulna subluxes dorsally and the extensor tendons of the ring and little fingers may displace or rupture, producing a sudden inability to extend those fingers (the extensor digitorum communis rupture). This is a surgical problem. [1]
The teaching point: RA saves the DIP. A patient with characteristic MCP and PIP deformities who also has DIP involvement has either OA coexisting with RA, or a different diagnosis (PsA, gout). The DIP is the joint that excludes RA. [1]
Osteoarthritis deformities
Osteoarthritis is a mechanical, wear-and-tear arthritis that predominantly affects the DIP, the PIP, and the first carpometacarpal joint, with relative sparing of the MCP joints. The deformities are bony: [1]
- Heberden nodes — hard, bony, pea-sized nodules on the dorsolateral aspect of the DIP joints. These are osteophytes and are the most specific sign of hand OA. They are often symmetrical and may be associated with small mucous cysts.
- Bouchard nodes — similar hard bony nodules at the PIP joints. Less specific than Heberden nodes but strongly suggestive of OA when combined with them.
- Squaring of the first carpometacarpal joint — a squared, angular contour at the base of the thumb (the first CMC joint) from subluxation and osteophyte formation. This is also called the "shelf sign" and is one of the earliest signs of hand OA. It causes pain on pinch and grip.
- Deviation and subluxation of the DIP and PIP in advanced OA — but the deformity pattern is asymmetrical, bony, and non-reducible, distinguishing it from the symmetrical, soft, and partially-reducible deformities of RA. [1]
The teaching point: OA saves the MCP. A patient with Heberden and Bouchard nodes and a squared thumb base but normal MCP joints has hand OA. The MCP is the joint that excludes OA as the primary process. [1]
Psoriatic arthritis deformities
Psoriatic arthritis is an asymmetrical inflammatory arthritis that can affect any joint but has a predilection for the DIP joints — the joint RA spares. The distinctive hand findings are: [1]
- Dactylitis ("sausage digit") — uniform swelling of an entire finger or toe, so that the digit looks like a sausage. This is the combined inflammation of the joint and the tendon sheath (enthesitis) and is one of the most specific signs of PsA. A single sausage digit in a patient with psoriasis or nail changes is PsA until excluded [3].
- Nail changes — pitting (small depressions in the nail plate), onychia (discolouration), subungual hyperkeratosis, and onycholysis (separation of the nail from the nail bed, giving an oil-drop appearance). Nail involvement is present in the majority of PsA patients because the nail bed and the distal interphalangeal joint share a common enthesis. The CASPAR criteria incorporate current psoriasis, a personal or family history, nail dystrophy, dactylitis, RF negativity, and juxta-articular new bone formation [3].
- Distal interphalangeal predominant arthritis — isolated DIP involvement with nail changes in the adjacent nail is the most pattern-specific PsA presentation.
- Arthritis mutilans — the "opera-glass hand" or "pencil-in-cup" deformity, with telescoping of the fingers from severe osteolysis of the phalanges. This is the most destructive form and is now rare with modern therapy.
The teaching point: PsA is the great mimicker — it can look like RA (symmetrical polyarthritis), like OA (DIP involvement), like gout (acute monoarthritis), or like a spondyloarthropathy (enthesitis and dactylitis). The keys to recognition are the asymmetry, the DIP involvement, the nail changes, and the dactylitis. Always examine the scalp, umbilicus, and natal cleft for hidden psoriasis, and ask about a family history. [1]
Gout
Chronic tophaceous gout produces: [1]
- Gouty tophi — chalky white or yellowish subcutaneous nodules, anywhere over joints, tendons, or the pinna of the ear. They are deposits of monosodium urate and may discharge a white chalky material. In the hands they cluster around the MCP joints, the PIP joints, and the extensor surfaces of the fingers. The 2015 ACR/EULAR gout classification criteria give the presence of a tophus four points (out of a threshold of eight), reflecting its high diagnostic specificity [4].
- Acute gouty arthritis — a single hot, red, swollen, exquisitely tender joint (classically the first MTP, but the hands are commonly affected). The swelling is diffuse and erythematous, distinct from the boggy synovitis of RA.
The teaching point: a chalky white nodule over a hand joint, especially with a history of episodic acute monoarthritis and hyperuricaemia, is a gouty tophus. The examination clue is the asymmetry, the chalky material, and the pinna of the ear (examine the ears routinely). [1]
Systemic lupus erythematosus — Jaccoud arthropathy
SLE produces a distinctive non-erosive, reducible arthropathy called Jaccoud arthropathy. The hands show: [1]
- Ulnar deviation and subluxation of the MCP joints — superficially resembling RA, but the deformities are correctable (the examiner can push the fingers back into normal alignment) because there is no bony destruction. The mechanism is ligamentous laxity and tendon imbalance from recurrent inflammation, not synovial erosion.
- Swan-neck and boutonniere-type deformities — also reducible.
- No joint swelling, no synovitis, no bony erosion — the joints look deformed but feel normal on palpation, and X-rays show no erosions (the "non-erosive" arthropathy). [1]
The teaching point: the reducibility is the discriminator. The candidate who sees ulnar deviation and immediately calls it RA has missed Jaccoud arthropathy. The test: ask the patient to place their hands palms-down on the table, or passively correct the deviation — in Jaccoud it corrects, in RA it does not. The 2019 EULAR/ACR SLE criteria require a positive ANA (entry criterion) and the accumulation of clinical and immunological points [5].
Systemic sclerosis and dermatomyositis — the skin tells the story
Systemic sclerosis (SSc) produces characteristic hand skin changes: [1]
- Sclerodactyly — thickening and tightening of the skin of the fingers, extending distal to (in limited cutaneous) or proximal to (in diffuse cutaneous) the MCP joints. The skin is hard, bound down, and cannot be pinched. The fingers become tapered and clawed.
- Digital pulp pitting scars — small, depressed, hyperkeratotic scars on the fingertips, the residue of healed digital ischaemic ulcers from Raynaud phenomenon.
- Calcinosis cutis — hard, subcutaneous calcium deposits (CREST syndrome: Calcinosis, Raynaud phenomenon, Esophageal dysmotility, Sclerodactyly, Telangiectasia).
- Telangiectasia — dilated capillaries on the fingers, palms, and face (matted, rectangular macules distinct from the spider naevi of chronic liver disease).
- Raynaud phenomenon — often the presenting complaint, with triphasic colour change (white, blue, red) of the fingers on cold exposure.
- Nailfold capillary abnormalities — dilated, tortuous, or dropout capillary loops visible with an ophthalmoscope or capillaroscope with oil immersion. [1]
The 2013 ACR/EULAR classification criteria give skin thickening of the fingers proximal to the MCP joints as a sufficient criterion (enough alone to classify SSc). If skin thickening is confined to the fingers, the additive score uses sclerodactyly (4 or 2 points), fingertip lesions (pitting scars 3 or ulcers 2), telangiectasia (2), abnormal nailfold capillaries (2), PAH or ILD (2), Raynaud phenomenon (3), and SSc-specific autoantibodies (3), with a threshold of nine [6].
Dermatomyositis produces: [1]
- Gottron papules — violaceous (purplish), slightly raised, scaly papules over the MCP and PIP joint extensor surfaces (the knuckles). These are pathognomonic of dermatomyositis and are the single most specific cutaneous finding.
- Gottron sign — a symmetric, confluent, violaceous erythema over the extensor surfaces (also the knuckles, but also the elbows, knees, and medial malleoli), without papules.
- Mechanic's hands — hyperkeratotic, fissured, dirty-appearing skin on the radial and palmar aspects of the fingers, resembling the hands of a manual worker. This is associated with antisynthetase syndrome.
- Periungual telangiectasia and nailfold capillary changes — similar to SSc. [1]
The teaching point: Gottron papules over the knuckles are dermatomyositis; sclerodactyly with digital pulp pitting scars is systemic sclerosis. Both are connective tissue diseases where the skin, not the joints, is the primary finding. [1]
Other inspection findings
- Rheumatoid nodules — firm, non-tender, subcutaneous nodules over pressure points: the olecranon, the extensor surface of the forearm, the MCP joints, and the Achilles tendon. They are found in seropositive (RF-positive) RA and indicate more severe disease.
- Dupuytren contracture — thickening and shortening of the palmar aponeurosis, producing flexion contractures of the fingers (classically the ring and little fingers) with palpable cords and pits in the palm. It is idiopathic but associated with age, alcohol, diabetes, epilepsy (phenytoin), and manual labour.
- Erythema nodosum — tender, erythematous nodules on the shins (not the hands), but a clue to sarcoidosis, inflammatory bowel disease, streptococcal infection, or a drug reaction in a patient with an inflammatory arthropathy.
- Purpura and palpable purpura — on the fingers and nailfolds, indicating small-vessel vasculitis (in RA with extra-articular disease, cryoglobulinaemia, or ANCA-associated vasculitis).
- Clubbing — of the fingernails, indicating suppurative lung disease (in a patient with inflammatory bowel disease and arthropathy, think bronchiectasis and IBD-associated arthritis), cyanotic congenital heart disease, or pulmonary fibrosis (in a patient with RA or a connective tissue disease, think interstitial lung disease). [1]
Nail changes — the five-pathway framework
The nails carry diagnostic information that rivals the joints. Inspect each nail carefully from the dorsal and lateral aspects, looking for: [1]
- Nail pitting — small depressions in the nail plate, the hallmark of psoriasis and PsA. More than ten pits or any large, deep, irregular pit is suggestive of psoriatic disease.
- Onycholysis — separation of the nail plate from the nail bed, producing a white or yellow discolouration. Seen in PsA, in fungal infection (tinea unguium), and in hyperthyroidism (Plummer nails).
- Clubbing — loss of the normal Lovibond angle (the angle between the nail plate and the proximal nail fold, normally 160 degrees but increased to over 180 in clubbing), with bulbous enlargement of the distal digit and a spongy, floating nail bed. Associated with pulmonary, cardiac, gastrointestinal, and endocrine disease.
- Splinter haemorrhages — tiny, linear, reddish-brown streaks under the nail, aligned with the long axis. While classically associated with infective endocarditis, they are also common in manual workers (trauma) and in RA with vasculitis.
- Periungual erythema and telangiectasia — dilated, tortuous capillary loops at the nailfold, visible with the naked eye or with an ophthalmoscope plus a drop of oil. The hallmark of the connective tissue diseases (SSc, dermatomyositis, SLE), indicating microvascular disease.
- Nail dystrophy without pitting — thickening, ridging, and discolouration in the CASPAR criteria for PsA (includes onycholysis, pitting, and hyperkeratosis) [3].
Step 2 — Palpation: synovitis versus osteophyte, confirmed by touch
Palpation confirms or refutes the inspection-generated differential. Feel each joint systematically — the MCP joints (metacarpal heads), the PIP joints, the DIP joints, the wrists, and the first CMC — comparing left with right, and ask the patient to report any tenderness. [1]
Temperature. Feel the dorsum of the hand and each joint with the back of your hand. Warm joints indicate active inflammation (RA, PsA, acute gout). Cold hands with tight, shiny skin and a history of colour change on cold exposure suggest Raynaud phenomenon and SSc. Generalised cold hands without skin changes suggest a vascular or neurological cause. [1]
Sweating. Examine the palmar surfaces. Sweating is preserved in OA and lost in SSc (the tight, dry skin of sclerodactyly). Hyperhidrosis may accompany hyperthyroidism (with a fine tremor). [1]
Texture. Pinch the skin over the dorsum of the fingers. Thick, tight, bound-down skin that cannot be pinched or folded is sclerodactyly (SSc). Normal, supple skin rules out SSc at that site. Peau d'orange (orange peel) texture or woody induration suggests eosinophilic fasciitis or chronic lymphoedema. [1]
Tenderness and swelling — the synovitis assessment. Palpate each MCP joint by squeezing it between your thumb and index finger (the "squeeze test" across the metacarpal heads). Then palpate each PIP and DIP joint individually, feeling for boggy, tender, warm swelling. Active synovitis is defined as joint swelling (boggy) with tenderness on pressure or on movement. This is the clinical finding that defines inflammatory arthritis, and it is what you count for the DAS28 score [2].
The DAS28 (Disease Activity Score, 28 joints) is the standard composite measure of RA disease activity. The 28 joints are: the ten MCPs, the ten PIPs, both wrists, both elbows, both shoulders, and both knees — the DIPs, the ankles, and the MTPs are not counted. For each joint, record whether it is swollen and whether it is tender, giving a swollen joint count (0 to 28) and a tender joint count (0 to 28). The DAS28 combines these with the ESR (or CRP) and the patient's global assessment on a visual analogue scale, producing a single score: over 5.1 is high disease activity, 3.2 to 5.1 moderate, 2.6 to 3.2 low, and under 2.6 is remission [2]. The candidate who counts the swollen and tender joints at the bedside demonstrates exactly what the rheumatologist does in clinic, and it earns marks in the DCE.
Crepitus. Feel for crepitus while passively moving each joint. Coarse, bony, hard crepitus (like crushing sand under the fingers) indicates the cartilage loss and osteophyte-on-osteophyte grinding of OA. Soft, fine crepitus (like crinkling cellophane) may indicate tenosynovitis or early synovitis. The quality of crepitus is a bedside discriminator between OA (coarse, bony) and RA (soft, boggy, with less crepitus because the joint is filled with synovium, not osteophytes). [1]
Step 3 — Range of motion: active then passive
Test active movement first at each joint group, then passive movement if active is limited. The sequence: [1]
Make a fist — the patient flexes all the fingers. This tests MCP flexion, PIP flexion, and DIP flexion together. Assess whether the fist is complete (the fingertips should touch the palm) or incomplete, and note which joints are limited. [1]
Extend the fingers — the patient opens the hand fully. MCP extension and PIP/DIP extension. [1]
Spread the fingers apart and bring them back together — MCP abduction and adduction (dorsal interossei and palmar interossei). [1]
Wrist movements — flexion, extension, ulnar deviation, and radial deviation. Compare with the normal range (flexion 80 degrees, extension 70 degrees, ulnar deviation 30 degrees, radial deviation 20 degrees). In RA, wrist involvement with radial deviation and limited extension is common; in OA, the first CMC is the more relevant site. [1]
Thumb movements — opposition (touch the thumb to each fingertip, testing the thenar muscles and the median nerve), abduction (spread the thumb away from the palm), and adduction. The first CMC joint of OA is tested by compressing the thumb metacarpal against the trapezium and rotating (the grind test), which reproduces the pain. [1]
If active movement is limited, test passive movement to determine whether the limitation is from a fixed structural deformity (RA with bony ankylosis or tendon rupture), from pain inhibition (active inflammatory arthritis), or from soft tissue contracture (Dupuytren). A joint that is limited actively but full passively suggests pain or weakness, not a fixed deformity. [1]
Step 4 — Function: the real-world assessment
Functional testing is mandatory and often the highest-yield step for demonstrating the impact of the hand disease. Five tasks: [1]
- Grip strength — ask the patient to squeeze two of your fingers as hard as they can, comparing left and right. A formal grip dynamometer may be used in clinic, but the qualitative assessment at the bedside suffices for the DCE.
- Pinch grip — ask the patient to pinch their thumb and index finger together (the "OK" sign). This tests the precision pinch, which is the first to be lost in first CMC OA (the thumb base pain) and in median nerve lesions (thenar weakness).
- Write their name — hand the patient a pen and paper. Writing integrates grip, precision, coordination, and dexterity, and reveals tremor (Parkinson, essential), weakness (myasthenia, motor neuron disease), or pain (inflammatory or mechanical arthritis).
- Pick up a coin from the table — tests the pincer grasp and the fine motor coordination.
- Turn a key in a lock — or simulate the motion. This is the classic functional test for first CMC OA, because the key-turning motion loads the thumb base and reproduces the characteristic pain. [1]
The candidate who skips functional testing misses the opportunity to demonstrate that the hand disease is not just a collection of signs but a cause of real-world disability — and this is what the examiner and the patient care about most. [1]
Step 5 — Additional sites: the hands are not isolated
The rheumatological hand examination extends to the sites that share the disease: [1]
- Elbows — inspect and palpate the olecranon bursa and the extensor surface of the forearm for rheumatoid nodules (firm, non-tender, mobile subcutaneous nodules in seropositive RA). Look for psoriatic plaques (well-demarcated, scaly, erythematous plaques over the extensor surface). Look for gouty tophi over the olecranon. Test elbow flexion, extension, pronation, and supination.
- Shoulders — inspect for deformity and wasting, palpate for tenderness (the acromioclavicular joint is a common OA site), and test active and passive range of movement. RA commonly involves the glenohumeral joint; rotator cuff pathology and adhesive capsulitis (frozen shoulder) are frequent secondary complications.
- Spine — if the hand findings suggest a spondyloarthropathy (PsA, ankylosing spondylitis), examine the lumbar spine for tenderness and the modified Schober test for reduced forward flexion. Cervical spine involvement in RA (atlantoaxial subluxation) is a critical safety consideration before intubation or manipulation. [1]
Step 6 — Neurovascular: do not miss the entrapment and the ischaemia
Pulses — palpate the radial pulse and assess capillary refill time at the fingertips. Delayed capillary refill (over 2 seconds) or digital ischaemia suggests vasculitis or SSc-related vascular disease. [1]
Raynaud assessment — if the history or the inspection (digital pulp pitting scars, sclerodactyly) suggests Raynaud phenomenon, ask the patient to immerse the hand in cold water or to describe the triphasic colour change (white ischaemia, blue cyanosis, red hyperaemia) they experience on cold exposure. [1]
Sensation — test light touch and pinprick in the median nerve territory (the palmar surfaces of the thumb, index, and middle fingers, and the lateral half of the ring finger, sparing the palm) and the ulnar nerve territory (the palmar surfaces of the medial half of the ring finger and the little finger). Median nerve sensory loss with thenar wasting indicates carpal tunnel syndrome, the commonest entrapment neuropathy in RA (from tenosynovitis at the wrist) and in pregnancy, diabetes, hypothyroidism, and acromegaly. [1]
Tinel sign — tap over the flexor retinaculum at the wrist (the carpal tunnel) with your index or middle finger. Reproduction of tingling or paraesthesia in the median nerve distribution is a positive Tinel sign, supporting carpal tunnel syndrome. Note that the Tinel sign has variable sensitivity (approximately 45 per cent) and specificity (approximately 78 per cent) on meta-analysis and should not be used in isolation. [1]
Phalen test — ask the patient to hold both wrists in maximal palmar flexion (the backs of the hands pressed together, like an inverted prayer) for 60 seconds. Reproduction of median-nerve-distribution paraesthesia is a positive Phalen test, also supporting carpal tunnel syndrome. The Phalen test has moderate sensitivity (approximately 57 per cent) and specificity (approximately 67 per cent) on meta-analysis. [1]
Thenar muscle assessment — test thumb opposition (abductor pollicis brevis, median nerve, T1) by asking the patient to touch the thumb to the little finger against resistance. Thenar wasting and weak opposition indicate advanced carpal tunnel syndrome. The hypothenar muscles (ulnar nerve) are assessed by finger abduction. [1]
The deformity comparison table: the synthesis at the bedside
| Feature | Rheumatoid arthritis | Osteoarthritis | Psoriatic arthritis | Gout | SLE (Jaccoud) | Systemic sclerosis |
|---|---|---|---|---|---|---|
| Symmetry | Symmetrical | Asymmetrical | Asymmetrical | Asymmetrical | Symmetrical | Symmetrical |
| Joints | MCP, PIP, wrist (spares DIP) | DIP, PIP, first CMC (spares MCP) | DIP, any joint, dactylitis | Any joint, tophi | MCP (reducible) | Skin, not joints |
| Swelling | Soft, boggy, warm, tender | Hard, bony, non-tender | Soft, boggy (dactylitis) | Tophi, acute red hot | Minimal or none | Tight skin |
| Morning stiffness | Prolonged (over 60 min) | Brief (under 30 min) | Variable | Brief (acute attack) | Variable | Variable |
| Deformity | Ulnar deviation, swan-neck, boutonniere, Z-thumb | Heberden, Bouchard, CMC squaring | Dactylitis, pencil-in-cup, arthritis mutilans | Tophi, chalky white | Reducible ulnar deviation | Sclerodactyly, contractures |
| Nails | Normal (or splinters with vasculitis) | Normal | Pitting, onycholysis | Normal | Normal | Periungual telangiectasia |
| Skin | Rheumatoid nodules | Heberden (bony) | Psoriatic plaques | Tophi | Normal | Sclerodactyly, telangiectasia, calcinosis, pulp scars |
| Reducible | No | No | No | No | Yes | N/A |
The candidate who can reproduce this table from memory and apply it at the bedside has the core rheumatological competency the examiners are testing [1][3][5][6].
The presentation templates

After completing the six steps, turn to the examiner and present. The template is a structured summary — highlight the abnormal findings and offer the diagnosis supported by the discriminating evidence. [1]
Template — Rheumatoid arthritis hands
"I have examined this patient's hands. On inspection, there is symmetrical deformity of both hands with ulnar deviation and palmar subluxation at the MCP joints, swan-neck deformity of the index and middle fingers, and a Z-deformity of both thumbs. The DIP joints are spared. There is soft, boggy, tender swelling consistent with synovitis at the second and third MCP joints bilaterally and at the wrists. The skin over the joints is warm. There are firm, non-tender subcutaneous nodules on the extensor surface of the right forearm and at the right olecranon, consistent with rheumatoid nodules. Range of movement is reduced at the wrists and the MCPs, with pain on flexion and extension. Function is impaired — the patient has a weak grip bilaterally and difficulty making a full fist, but can perform a pinch grip and write. There is no sclerodactyly, no Gottron papules, and no nail pitting. The pulses are present and the sensation is intact, with a negative Tinel and Phalen test. [1]
In summary, these findings are consistent with seropositive rheumatoid arthritis with active synovitis and extra-articular nodular disease. I would confirm with a history of morning stiffness and systemic symptoms, serology for rheumatoid factor and anti-CCP, inflammatory markers, and hand X-rays looking for periarticular osteopenia, joint space narrowing, and marginal erosions. I would calculate a DAS28 score to quantify disease activity. [1]
To complete my examination, I would examine the other joints (especially the feet and the cervical spine), listen to the heart and lungs (for pulmonary fibrosis and valvular disease), and examine the eyes for episcleritis and sicca." [1]
Template — Osteoarthritis hands
"I have examined this patient's hands. On inspection, there are hard, bony, irregular nodules at the DIP joints bilaterally (Heberden nodes) and at the PIP joints (Bouchard nodes), with squaring of the first carpometacarpal joints bilaterally. The MCP joints are normal. There is no soft swelling, no warmth, and no synovitis. Crepitus is palpable at the DIP and PIP joints and at the first CMC joints on movement. The pain is reproduced by the grind test at the first CMC. Morning stiffness is brief. Function is impaired for pinch grip (from the first CMC OA) but grip strength is preserved. [1]
In summary, these findings are consistent with primary nodal osteoarthritis with first CMC involvement. This is a clinical diagnosis; I would confirm with hand X-rays showing osteophytes, subchondral sclerosis, asymmetrical joint space narrowing, and subchondral cysts. I would assess the knees, hips, and spine for the generalised pattern of OA. [1]
To complete my examination, I would examine the other weight-bearing joints and assess for Heberden and Bouchard nodes at the toes." [1]
Template — Psoriatic arthritis hands
"I have examined this patient's hands. On inspection, there is an asymmetrical pattern of joint involvement, with swelling of the right third finger as a uniform sausage digit (dactylitis) and isolated swelling of the left index DIP joint. The nails show multiple pits and onycholysis of several fingernails. There is no rheumatoid factor-type deformity and the MCP joints are relatively spared. There are scaly, erythematous, well-demarcated plaques on the extensor surface of the right elbow and at the umbilicus, consistent with psoriasis. Palpation confirms boggy, tender swelling at the affected DIP joints. Function is impaired for the dactylitic finger. [1]
In summary, these findings are consistent with psoriatic arthritis, distal interphalangeal predominant pattern, with dactylitis and nail involvement. I would confirm the diagnosis by applying the CASPAR criteria (inflammatory articular disease plus current psoriasis, nail dystrophy, dactylitis, and RF negativity), and I would arrange HLA-B27 and hand X-rays looking for the pencil-in-cup deformity and juxta-articular new bone formation. [1]
To complete my examination, I would examine the scalp, umbilicus, and natal cleft for further psoriasis, examine the other joints and the spine for spondyloarthropathy features, and look for nail involvement at the toenails." [1]
Discussion by finding — the examiner questions
Finding: symmetrical MCP and PIP synovitis with morning stiffness over one hour
Examiner: "What is your diagnosis, and what would you do next?" [1]
"The symmetrical small-joint polyarthritis involving the MCPs and PIPs with sparing of the DIPs, the boggy tender warm swelling indicating active synovitis, and the prolonged morning stiffness are consistent with rheumatoid arthritis. The 2010 ACR/EULAR classification criteria combine joint involvement (the number and size of swollen joints), serology (rheumatoid factor and anti-CCP), acute phase reactants (CRP and ESR), and symptom duration (over six weeks) — a score of six or more classifies definite RA [1]. My next step is to take a detailed history (duration, diurnal variation, systemic symptoms, functional impact, family history), arrange serology for RF and anti-CCP, inflammatory markers, a full blood count, and hand and foot X-rays (looking for periarticular osteopenia, marginal erosions at the MCPs and MTPs, and joint space narrowing). I would refer urgently to a rheumatologist because early DMARD therapy within the window of opportunity (the first three to six months) prevents erosive damage and improves long-term outcomes. I would calculate a DAS28 to quantify disease activity and guide the treat-to-target strategy."
Finding: hard bony DIP and PIP nodules with first CMC squaring
Examiner: "What is the diagnosis, and how do you distinguish it from rheumatoid arthritis?" [1]
"The hard, bony, non-tender nodules at the DIP joints (Heberden nodes) and the PIP joints (Bouchard nodes), with squaring of the first carpometacarpal joints and sparing of the MCP joints, are diagnostic of primary nodal osteoarthritis. The distinction from RA rests on five points: first, the swelling is hard and bony, not soft and boggy; second, the joints are cool and non-tender, not warm and tender; third, the morning stiffness is brief (under 30 minutes), not prolonged; fourth, the distribution involves the DIP and the first CMC (which RA spares) and spares the MCP (which RA targets); and fifth, the inflammatory markers and the rheumatoid factor are typically normal. This is a clinical and radiological diagnosis — the X-rays show osteophytes, subchondral sclerosis, asymmetrical joint space narrowing, and subchondral cysts, not the periarticular osteopenia and symmetric marginal erosions of RA." [1]
Finding: a sausage digit with nail pitting and scaly elbow plaques
Examiner: "What is the diagnosis, and what are the classification criteria?" [1]
"The dactylitis (sausage digit), the nail pitting and onycholysis, and the psoriatic plaques on the extensor surface of the elbow are diagnostic of psoriatic arthritis. The CASPAR criteria (Classification Criteria for Psoriatic Arthritis) require inflammatory articular disease (joint, spine, or entheseal) plus three or more points from: current psoriasis (2 points), a personal or family history of psoriasis, current dactylitis or a history of dactylitis recorded by a rheumatologist, radiographic juxta-articular new bone formation, rheumatoid factor negativity, and nail dystrophy (including onycholysis, pitting, and hyperkeratosis) [3]. This patient scores the maximum. I would examine the scalp, umbilicus, and natal cleft for hidden psoriasis, test the HLA-B27, and arrange hand X-rays looking for the pencil-in-cup deformity (especially at the DIP), acro-osteolysis, and ankylosis. I would refer to a rheumatologist and a dermatologist for coordinated management."
Finding: reducible ulnar deviation with normal X-rays
Examiner: "What is the diagnosis, and how does it differ from RA?" [1]
"The reducible ulnar deviation of the MCP joints — the deformity corrects when the patient places the hands palms-down on the table — with no palpable synovitis and no bony erosion on X-ray, is Jaccoud arthropathy, classically seen in systemic lupus erythematosus but also in chronic recurrent rheumatic fever. The distinction from RA is that Jaccoud is a non-erosive, deforming but reducible arthropathy from ligamentous laxity and tendon imbalance, while RA is an erosive, fixed, deforming arthropathy from synovial proliferation and pannus. The 2019 EULAR/ACR SLE criteria require a positive ANA as the mandatory entry criterion, plus the accumulation of at least 10 points across clinical and immunological domains — musculoskeletal involvement (joint involvement) scores 6 points [5]. I would test the ANA, anti-dsDNA, anti-Smith, and complement levels, and screen for renal, cutaneous, haematological, and serosal involvement."
Finding: sclerodactyly with digital pulp pitting scars and Raynaud history
Examiner: "What is the diagnosis, and what is the classification system?" [1]
"The sclerodactyly (tight, thickened, bound-down skin of the fingers extending to but not proximal to the MCP joints), the digital pulp pitting scars (healed ischaemic ulcers), and the history of triphasic colour change on cold exposure (Raynaud phenomenon) are diagnostic of systemic sclerosis, likely limited cutaneous (CREST) subtype. The 2013 ACR/EULAR classification criteria give skin thickening of the fingers proximal to the MCP joints as a sufficient criterion (enough alone). If, as here, the skin thickening is confined to the fingers, the additive score uses sclerodactyly of the fingers (2 points for distal to PIP, 4 for distal to MCP), fingertip lesions (pitting scars 2 or ulcers 3), telangiectasia (2), abnormal nailfold capillaries (2), pulmonary arterial hypertension or interstitial lung disease (2), Raynaud phenomenon (3), and SSc-specific autoantibodies (anti-centromere, anti-topoisomerase I/Scl-70, anti-RNA polymerase III) (3), with a threshold of 9 [6]. I would test the autoantibody profile, perform nailfold capillaroscopy, screen the lungs (PFTs and HRCT for ILD), the heart (echo for PAH), and the kidneys (blood pressure monitoring for scleroderma renal crisis, especially in diffuse cutaneous disease)."
Common examination traps and pitfalls
Trap 1 — Calling all swelling "arthritis." The single most common error is failing to distinguish synovitic (soft, boggy, warm, tender, symmetrical) from bony (hard, irregular, cool, non-tender, asymmetrical) swelling. This one distinction separates RA from OA and frames the entire differential. Palpate every joint before you commit to a diagnosis. [1]
Trap 2 — Missing the DIP involvement. The DIP joint is the joint that discriminates: RA spares it, OA and PsA involve it. A candidate who does not specifically inspect and palpate the DIP joints has missed the fork between RA and OA/PsA. Examine every DIP. [1]
Trap 3 — Forgetting to look at the nails and the skin. Nail pitting (PsA), onycholysis (PsA), periungual telangiectasia (SSc, dermatomyositis), and Gottron papules (dermatomyositis) are signs that change the entire diagnosis. The candidate who examines only the joints and not the skin and nails has missed the connective tissue diseases. [1]
Trap 4 — Not testing for reducibility in suspected Jaccoud arthropathy. Ulnar deviation is RA until proven Jaccoud. The test is to ask the patient to place the hands palms-down on the table — if the deviation corrects, it is Jaccoud (SLE); if it does not, it is RA. Every candidate with a deformed hand should perform this test. [1]
Trap 5 — Not counting the swollen and tender joints for DAS28. The DAS28 is the standard RA disease activity score, and the candidate who can count the 28 joints and state whether the patient is in high, moderate, low, or remission disease activity demonstrates the clinical reasoning the examiner rewards [2]. Practice the 28-joint count until it is automatic.
Trap 6 — Skipping functional testing. The examiner cares about the patient's function, not just the signs. Grip, pinch, write, pick up a coin, turn a key — five tests, thirty seconds, and they reveal the real-world impact of the disease. A candidate who presents the deformities but does not test function has done half the examination. [1]
Trap 7 — Not examining the elbows for rheumatoid nodules and psoriatic plaques. The elbows are the classic site for rheumatoid nodules (seropositive RA), psoriatic plaques (PsA), and gouty tophi. The candidate who stops at the wrists has missed the extra-articular and cutaneous findings that confirm the diagnosis. [1]
Trap 8 — Not completing the examination. The hands are the entry point to a systemic disease. The candidate who presents the hand findings and stops has missed the opportunity to examine the other joints, the skin (for vasculitis, psoriasis, scleroderma), the lungs (for fibrosis), the heart (for valvular disease and PAH), and the eyes (for sicca and episcleritis). The closing statement — "to complete my examination, I would examine the other joints, the skin, the chest, and the eyes" — is mandatory. [1]
Key DWE MCQ patterns
- Distinguish RA from OA by the joint distribution. Symmetrical MCP and PIP involvement with morning stiffness over one hour is RA; asymmetrical DIP, PIP, and first CMC involvement with brief stiffness is OA. The MCQ may give a vignette and ask for the most likely diagnosis.
- Recognise the PsA pattern. Asymmetrical DIP involvement with nail pitting and dactylitis (sausage digit) is PsA, not RA. The CASPAR criteria incorporate current psoriasis, nail dystrophy, dactylitis, RF negativity, and juxta-articular new bone formation [3].
- Distinguish Jaccoud arthropathy (SLE) from RA. Reducible, non-erosive ulnar deviation with a positive ANA is Jaccoud arthropathy in SLE; fixed, erosive ulnar deviation with RF positivity is RA. The 2019 EULAR/ACR SLE criteria require a positive ANA plus at least 10 points across clinical and immunological domains [5].
- Recognise gouty tophi. Chalky white subcutaneous nodules over joints and the pinna, with a history of episodic acute monoarthritis, are gouty tophi. The 2015 ACR/EULAR gout criteria give the presence of a tophus four points [4].
- Identify sclerodactyly as systemic sclerosis. Tight, thickened, bound-down skin of the fingers with digital pulp pitting scars and Raynaud phenomenon is SSc. The 2013 ACR/EULAR criteria use a weighted additive score with a threshold of nine, or skin thickening proximal to the MCP joints as a sufficient criterion [6].
- Recognise carpal tunnel syndrome in the rheumatological hand. Median-nerve-distribution sensory loss, thenar wasting, and a positive Tinel or Phalen test in a patient with RA indicate carpal tunnel syndrome from tenosynovitis at the wrist.
References
[1] Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 2010;62(9):2569–81. The 2010 ACR/EULAR RA classification criteria, shifting the focus to early synovitis and requiring a score of six or more from joint involvement, serology, acute phase reactants, and symptom duration, with the entry requirement of synovitis in at least one joint and the exclusion of alternative diagnoses.
[2] Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL. Modified disease activity scores that include twenty-eight-joint counts: development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum 1995;38(1):44–8. The DAS28, a composite measure of RA disease activity using 28 joints (the ten MCPs, ten PIPs, both wrists, both elbows, both shoulders, both knees), the ESR, and the patient global assessment, validated against radiographic progression and functional outcome.
[3] Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P, Mielants H; CASPAR Study Group. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum 2006;54(8):2665–73. The CASPAR criteria for psoriatic arthritis, requiring inflammatory articular disease plus three or more points from current psoriasis (2), personal or family history of psoriasis, dactylitis, juxta-articular new bone formation, RF negativity, and nail dystrophy.
[4] Neogi T, Jansen TL, Dalbeth N, et al. 2015 gout classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol 2015;67(10):2557–68. The 2015 ACR/EULAR gout classification criteria, using an entry criterion of at least one symptomatic episode, a sufficient criterion of MSU crystal identification, and an additive score of eight or more from clinical, laboratory, and imaging domains, with a tophus scoring four points.
[5] Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Arthritis Rheumatol 2019;71(9):1400–12. The 2019 EULAR/ACR SLE classification criteria, requiring a positive ANA as the mandatory entry criterion and the accumulation of at least 10 points across clinical and immunological domains, with musculoskeletal joint involvement scoring 6 points.
[6] van den Hoogen F, Khanna D, Fransen J, et al. 2013 classification criteria for systemic sclerosis: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum 2013;65(11):2737–47. The 2013 ACR/EULAR SSc classification criteria, with skin thickening of the fingers proximal to the MCP joints as a sufficient criterion, or an additive score of nine or more from skin thickening, fingertip lesions, telangiectasia, abnormal nailfold capillaries, PAH or ILD, Raynaud phenomenon, and SSc-specific autoantibodies.
Aletaha et al. (2010 ACR/EULAR RA criteria), Arthritis Rheum 2010; Prevoo et al. (DAS28), Arthritis Rheum 1995; Taylor et al. (CASPAR criteria), Arthritis Rheum 2006; Neogi et al. (2015 ACR/EULAR gout criteria), Arthritis Rheumatol 2015; Aringer et al. (2019 EULAR/ACR SLE criteria), Arthritis Rheumatol 2019; van den Hoogen et al. (2013 ACR/EULAR SSc criteria), Arthritis Rheum 2013; RACP DCE Examination Handbook; MRCP PACES; Hutchinson's Clinical Methods; Talley and O'Connor Clinical Examination; Macleod's Clinical Examination. [1]
References
- [1]Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO 3rd, Birnbaum NS, Burmester GR, Bykerk VP, Cohen MD, Combe B, Costenbader KH, Dougados M, Emery P, Ferraccioli G, Hazes JM, Hobbs K, Huizinga TW, Kavanaugh A, Kay J, Kvien TK, Laing T, Mease P, Ménard HA, Moreland LW, Naden RL, Pincus T, Smolen JS, Stanislawska-Biernat E, Symmons D, Tak PP, Upchurch KS, Vencovský J, Wolfe F, Hawker G The 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis: Phase 2 methodological report Arthritis Rheum, 2010.PMID 20872596
- [2]Prevoo ML, van 't Hof MA, Kuper HH, van Leeuwen MA, van de Putte LB, van Riel PL Modified disease activity scores that include twenty-eight-joint counts. Development and validation in a prospective longitudinal study of patients with rheumatoid arthritis Arthritis Rheum, 1995.PMID 7818570
- [3]Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P, Mielants H; CASPAR Study Group Classification criteria for psoriatic arthritis: development of new criteria from a large international study Arthritis Rheum, 2006.PMID 16871531
- [4]Neogi T, Jansen TL, Dalbeth N, Fransen J, Schumacher HR, Berendsen D, Brown M, Choi H, Edwards NL, Janssens HJ, Lioté F, Mallen CD, Nuki G, Ogdie A, Perez-Ruiz F, Saag K, Singh JA, Sundy JS, Tausche AK, Vaquez-Mellado J, Yarows SA, Taylor WJ 2015 Gout classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative Ann Rheum Dis, 2015.PMID 26359487
- [5]Aringer M, Costenbader K, Daikh D, Brinks R, Mosca M, Ramsey-Goldman R, Smolen JS, Wofsy D, Boumpas DT, Bolettis AJ, Cervera R, Doria A, Fischer-Betz R, Fritsch-Stork R, Gianfreda D, Gordon C, Hiepe F, Illei GG, Kallas P, Kamen DL, Kumanović G, Manger B, Massarotti EM, Maddison P, Matsoukas C, Mukhtyar C, Olszanecki R, O'Shaughnessy MM, Peñaloza R, Pettersson T, Popa CD, Rajaei A, Riemekasten G, Schneider M, Siebert M, Svenungsson E, Tzellos T, van Vollenhoven R, Werth VP, van Laar JM, Johnson SR 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus Arthritis Rheumatol, 2019.PMID 31385462
- [6]van den Hoogen F, Khanna D, Fransen J, Johnson SR, Baron M, Tyndall A, Matucci-Cerinic M, Naden RP, Medsger TA Jr, Carreira PE, Riemekasten G, Clements PJ, Denton CP, Distler O, Allanore Y, Furst DE, Gabrielli A, Mayes MD, van Laar JM, Seibold JR, Czirjak L, Steen VD, Inanc M, Kowal-Bielecka O, Müller-Ladner U, Valentini G, Veale DJ, Vonk MC, Walker UA, Chung L, Hummers LK, Silver RM, Steen RW, Torok KS, Pope JE 2013 classification criteria for systemic sclerosis: an American college of rheumatology/European league against rheumatism collaborative initiative Ann Rheum Dis, 2013.PMID 24092682