Phys · general-medicine
Thyroid Status and Neck Examination — DCE Short-Case Routine
Also known as thyroid examination · thyroid status examination · neck examination · goitre examination · thyroid short case · DCE thyroid · PACES thyroid examination · examine the thyroid · Graves orbitopathy examination · thyroid system assessment
Consultant-physician guide to the systematic thyroid status examination for the DCE short case: the nine-step routine performed from behind the patient (general inspection, hands, pulse, eyes, neck inspection, neck palpation, percussion, auscultation, reflexes and legs), the hyperthyroid and hypothyroid clinical phenotypes, the Graves-specific eye and skin signs (exophthalmos, lid lag, lid retraction, ophthalmoplegia, thyroid acropachy, pretibial myxoedema), the NOSPECS and CAS scoring systems, the model presentation template, the examiner discussion questions, and the classic exam traps — the routine every FRACP, MRCP PACES, and ABIM candidate must perform flawlessly.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Thyroid Status and Neck Examination — DCE Short-Case Routine

The one-minute consultant answer
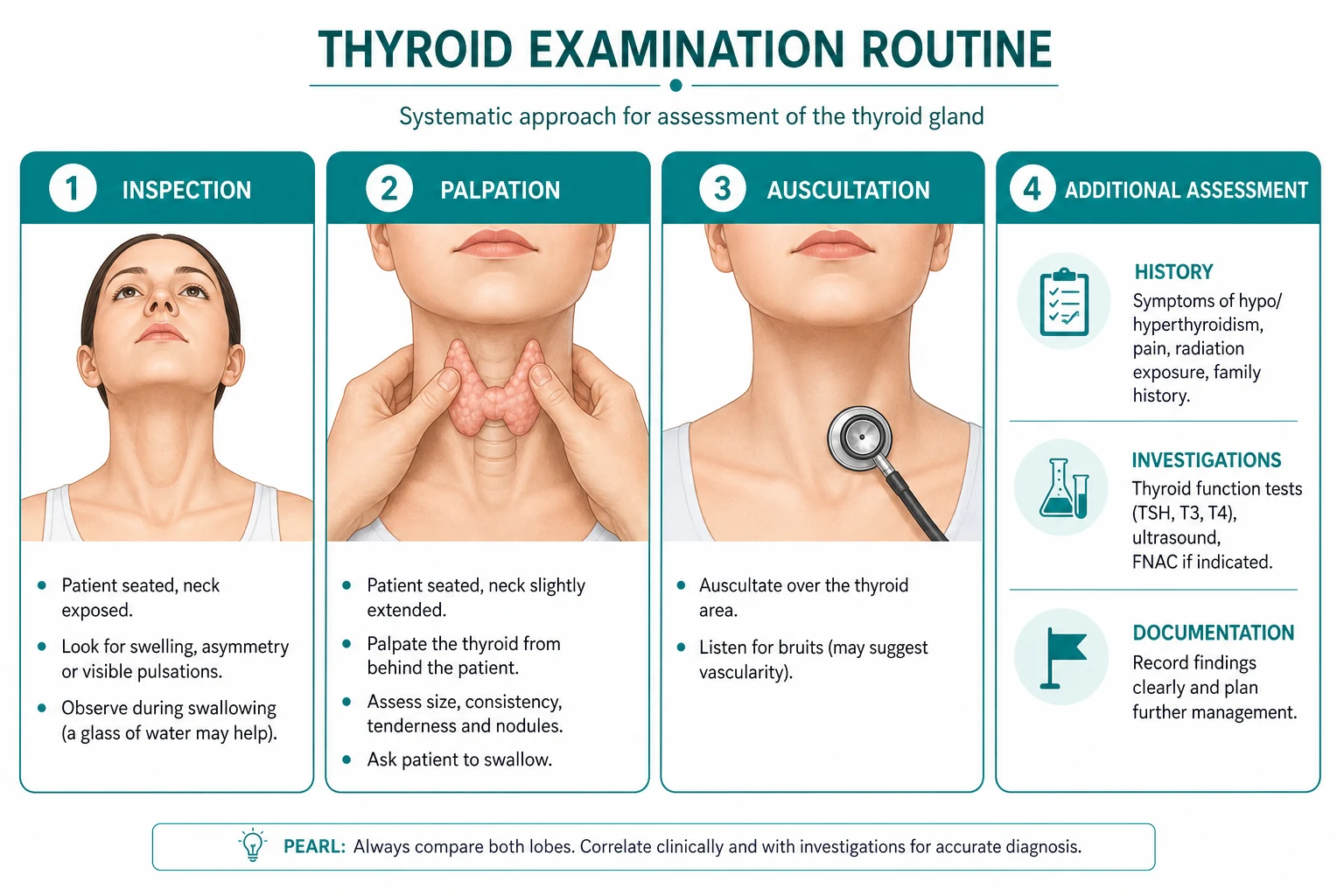
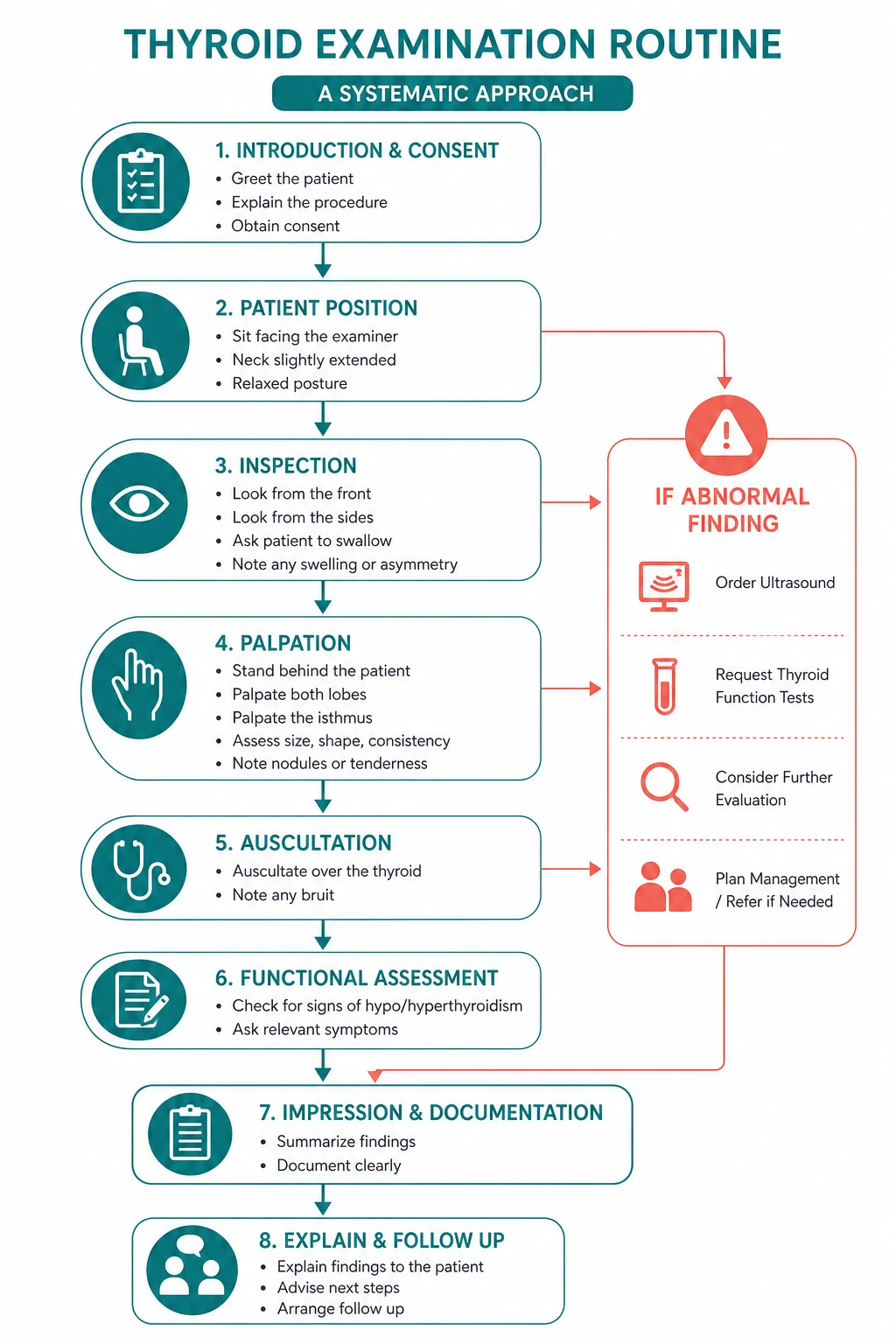
The thyroid examination is the most frequently encountered endocrine short case in the FRACP DCE and the MRCP PACES, and it follows an invariant nine-step routine performed from behind the seated patient: general inspection, hands, pulse, eyes, neck inspection, neck palpation, percussion over the sternum, auscultation of the thyroid, and reflexes plus legs. The instruction is almost always "Please examine this patient's thyroid status" — which means you are assessing two things in parallel: the patient's thyroid status (hyperthyroid, euthyroid, or hypothyroid) and the gland itself (size, consistency, nodularity, mobility, retrosternal extension). The candidate who palpates the neck and forgets the hands, the eyes, the reflexes and the shins has examined the gland but not the thyroid status, and loses marks for the more important half of the assessment [6].
The single most important principle is position. The thyroid examination is performed from behind the seated patient, not from the front. You stand behind the patient, place both hands around the neck, and palpate the gland with the fingers while the patient swallows a sip of water. The front-of-neck approach is for the airway and the trachea; the behind-the-patient approach is the only way to examine the gland systematically. The examiner is watching your position from the moment you begin, and the candidate who stands in front of the patient and palpates with the thumbs is demonstrating a fundamental technique error. [1]
The non-negotiable principles: state the thyroid status from the general inspection and the hands before you touch the neck, because the thin agitated patient with a fine tremor and a stare is hyperthyroid and the slow puffy patient with dry skin and bradycardia is hypothyroid before you ever reach the gland; examine the eyes from in front, because the eye signs of Graves orbitopathy (exophthalmos, lid retraction, lid lag, ophthalmoplegia) are the most discriminating findings in the short case; palpate the gland from behind during swallowing, because the thyroid moves up with the trachea and larynx on deglutition, and a nodule or an enlargement that does not move on swallowing is either not the thyroid or is fixed by malignancy; percuss the sternum for retrosternal extension, because a dull percussion note over the upper sternum means the goitre extends behind the sternum and you cannot get your fingers below it; and score the eye signs with the Clinical Activity Score, because the examiner will ask you to distinguish active from inactive Graves orbitopathy, and that distinction drives the decision to treat with immunosuppression [1][2].
The examination routine — the nine-step sequence, from behind the patient

The thyroid examination is the only system examination that the candidate performs from behind the patient. The reason is anatomical: the thyroid gland wraps around the anterior and lateral trachea from the second to the fourth tracheal ring, and the isthmus and the two lobes are best palpated with the fingertips placed from the posterior approach, with the patient seated upright and the neck slightly flexed to relax the sternocleidomastoid and the strap muscles. The sequence is invariant and every candidate must perform it in the same order every time. [1]
Step 1 — General inspection (from the end of the bed)
Before you touch the patient, stand at the end of the bed and take five seconds. You are looking for the two thyroid phenotypes — the hyperthyroid and the hypothyroid — because the general inspection often reveals the thyroid status before you reach the hands or the neck: [1]
- Hyperthyroid phenotype — the patient is thin, restless, fidgeting, with a fine tremor of the outstretched hands, proximal muscle wasting (difficulty rising from a chair, a myopathic gait), a stare from lid retraction, agitation and a rapid speech pattern. The patient may be dressed lightly despite a warm room (heat intolerance). There may be a visible neck swelling, a thyroid bruit heard from the end of the bed, or the characteristic exophthalmos of Graves disease.
- Hypothyroid phenotype — the patient is slow, with a puffy face (periorbital myxoedema), dry coarse skin, thinning hair and loss of the outer third of the eyebrows, a hoarse voice, slow speech and delayed responses, and a general appearance of physical and mental slowing. There may be weight gain and cold intolerance. [1]
The teaching point: the five seconds at the end of the bed frame your entire examination. State your impression: "On general inspection, this thin, agitated woman with a stare and a visible neck swelling appears clinically hyperthyroid." Then confirm or refute that impression with the hands, the pulse, the reflexes and the skin. The synthesis is the mark-winner, not the list of isolated signs. [1]
Step 2 — The hands
The hands are the first structure you examine after the general inspection, and they reveal the thyroid status and the specific Graves manifestations: [1]
- Fine tremor — the single most reliable sign of thyrotoxicosis in the hands. Ask the patient to stretch out both hands with the fingers spread, palms down, and observe for a fine, rapid tremor. To amplify it, place a sheet of paper on the outstretched hands and watch the paper tremble. The tremor is fine (unlike the coarse tremor of Parkinson disease or the intention tremor of cerebellar disease) and present at rest, worsened by extension. It reflects the beta-adrenergic hypersensitivity of thyrotoxicosis.
- Warm, sweaty palms — thyrotoxic patients have warm, moist, sweaty hands from the increased metabolic rate and the peripheral beta-adrenergic vasodilation. Contrast with the cold, dry, rough palms of hypothyroidism.
- Palmar erythema — a diffuse redness of the palms, present in thyrotoxicosis (and in pregnancy, chronic liver disease and rheumatoid arthritis).
- Thyroid acropachy — the Graves-specific analogue of finger clubbing, characterised by digital swelling and periosteal bone formation in the metacarpals and phalanges. Unlike ordinary clubbing, the nail-fold angle is not always lost; the finding is a diffuse, firm, doughy swelling of the fingers with new bone formation on X-ray. It is rare — fewer than 1 per cent of Graves patients — but pathognomonic when present, and it completes the triad of exophthalmos, myxoedema (dermopathy) and osteoarthropathy (acropachy) that defines severe Graves autoimmune disease [3].
- Onycholysis (Plummer nails) — the separation of the nail from the nail bed, beginning distally and laterally, so the free edge of the nail turns up and catches on clothing. It is a sign of thyrotoxicosis (not specific to Graves — it occurs in any cause of hyperthyroidism) and is best seen in the ring finger.
- Proximal muscle wasting — inspect the thenar and forearm muscles for wasting. Thyrotoxic myopathy produces proximal muscle weakness (the patient has difficulty rising from a squat or lifting the arms above the head), and chronic severe disease produces visible wasting.
- Cold, dry, coarse skin (hypothyroidism) — the palms are cold and dry, the skin is rough and scaly, and there may be a yellowish tint (carotenaemia from impaired conversion of carotene to vitamin A).
Step 3 — The pulse
Take the radial pulse for rate and rhythm. The pulse is a key discriminator of thyroid status: [1]
- Tachycardia and atrial fibrillation (hyperthyroid) — a resting tachycardia (above 90 to 100 beats per minute) is common, and atrial fibrillation occurs in approximately 10 to 15 per cent of thyrotoxic patients, rising to 20 to 25 per cent in older patients. Any older patient with new atrial fibrillation should have thyroid function checked, because thyrotoxicosis is a reversible cause. The pulse is also bounding, with a wide pulse pressure (see blood pressure below).
- Bradycardia (hypothyroid) — a resting bradycardia (below 60 beats per minute) is common in overt hypothyroidism, though it is less pronounced than the tachycardia of thyrotoxicosis because the bradycardia is partly offset by the deconditioning of the slow, sedentary patient. [1]
Step 4 — The eyes (examined from in front)

The eye signs are the centrepiece of the thyroid short case, because they distinguish Graves disease (which causes orbitopathy) from the other causes of thyrotoxicosis (toxic multinodular goitre, toxic adenoma, thyroiditis), which do not. Examine the eyes from in front of the patient, sitting face to face, with good lighting. [1]
The Graves orbitopathy signs — what to look for and what they mean: [1]
- Exophthalmos (proptosis) — the forward protrusion of the eyeball, caused by the swelling of the retro-orbital muscles and fat from lymphocytic infiltration and glycosaminoglycan deposition. Assess by looking from the side (the sclera is visible above the iris when the patient looks straight ahead — the "scleral show"), and measure with an exophthalmometer if available. Proptosis is the hallmark of Graves orbitopathy and does not occur in the other causes of thyrotoxicosis.
- Lid retraction (Dalrymple sign) — the upper eyelid is retracted so that the sclera is visible above the upper limbus of the iris when the patient looks straight ahead. The mechanism is the sympathetic overactivity of thyrotoxicosis (Muller muscle over contraction) combined with the mechanical retraction from the swollen inferior rectus. Lid retraction occurs in any cause of thyrotoxicosis (it is not specific to Graves).
- Lid lag (von Graefe sign) — the upper eyelid lags behind the downward movement of the eyeball as the patient follows your finger from above down to below. The white sclera appears between the upper lid and the iris during the descent. Lid lag is a sign of thyrotoxicosis (not specific to Graves) and reflects the sympathetic overdrive of the levator palpebrae.
- Ophthalmoplegia — impaired eye movements, most commonly impaired upgaze (from inferior rectus involvement) and impaired convergence. Ask the patient to follow your finger through the six cardinal directions of gaze and to converge on your finger as you bring it toward the nose. The inferior and medial recti are the most commonly affected muscles. Ophthalmoplegia is specific to Graves orbitopathy (it does not occur in the other causes of thyrotoxicosis).
- Chemosis and conjunctival injection — the conjunctiva is oedematous (chemosis — a "bag of water" appearance over the conjunctiva) and injected (red). These are signs of active inflammation and contribute to the Clinical Activity Score [1].
The Clinical Activity Score (CAS) is the seven-item bedside score used to distinguish active from inactive Graves orbitopathy. A score of three or more out of seven indicates active disease, which predicts a response to immunosuppression. The seven items are: spontaneous retrobulbar pain, pain on eye movement, eyelid erythema, conjunctival injection, chemosis, swelling of the caruncle, and eyelid oedema or fullness. The CAS is the examiner's most likely follow-up question after you describe the eye signs, and you should state it and score it at the bedside [1][2].
The NOSPECS mnemonic is the older severity classification, where each letter corresponds to a class of severity: No signs, Only soft tissue involvement (lid oedema, chemosis), Soft tissue plus proptosis, Proptosis plus extraocular muscle involvement, Extraocular muscle plus corneal involvement, Corneal involvement plus sight loss (optic nerve). NOSPECS is less used clinically than the CAS (which measures activity, not severity), but you should be able to name it when asked [1].
Step 5 — The neck: inspection
Ask the patient to sit upright on the edge of the bed. Inspect the neck from in front, looking for: [1]
- Goitre — any enlargement of the thyroid gland. Note the shape: a diffuse, smooth, symmetric enlargement suggests Graves disease (or Hashimoto thyroiditis, or iodine deficiency); a multinodular goitre is asymmetric, lumpy, with distinct nodules; a solitary nodule raises the question of a benign adenoma or a malignancy. Offer the patient a glass of water and ask them to swallow — the goitre moves upward on swallowing.
- Scars — a transverse cervical (Kocher) scar indicates previous thyroid surgery; a scar along the sternocleidomastoid indicates a previous lymph node biopsy or a neck dissection.
- Skin changes — redness and warmth over the gland suggest subacute (de Quervain) thyroiditis; a sinus or a fistula is rare but may indicate a thyroglossal duct cyst or a branchial cleft anomaly.
- Dilated veins — over the neck and upper chest, suggesting superior vena cava obstruction from a large retrosternal goitre. [1]
Step 6 — The neck: palpation (from behind)
This is the core of the thyroid examination and the step most candidates perform poorly. Stand behind the seated patient. Ask the patient to flex the neck slightly forward and to the side to relax the sternocleidomastoid. Place both hands around the neck with the fingers anterior and the thumbs behind. Identify the thyroid cartilage and the cricoid cartilage, then move down to find the thyroid isthmus (across the trachea, just below the cricoid) and the two lobes (either side of the trachea). Give the patient a sip of water and ask them to hold it in the mouth; ask them to swallow as you palpate. The gland moves up with swallowing. [1]
Palpate systematically for: [1]
- Size — is the gland enlarged, normal or absent? A normal thyroid is each lobe the size of a teaspoon; the isthmus is a thin band across the trachea. Grade the goitre: stage 1 (palpable but not visible), stage 2 (visible at the normal neck position), stage 3 (visible at a distance or very large).
- Consistency — is the gland smooth and soft (normal, or Graves disease), firm and granular (Hashimoto thyroiditis), hard and irregular (malignancy, anaplastic carcinoma), or tender and warm (subacute thyroiditis)? A hard, fixed, irregular nodule in an older patient is anaplastic or poorly differentiated thyroid carcinoma until proven otherwise.
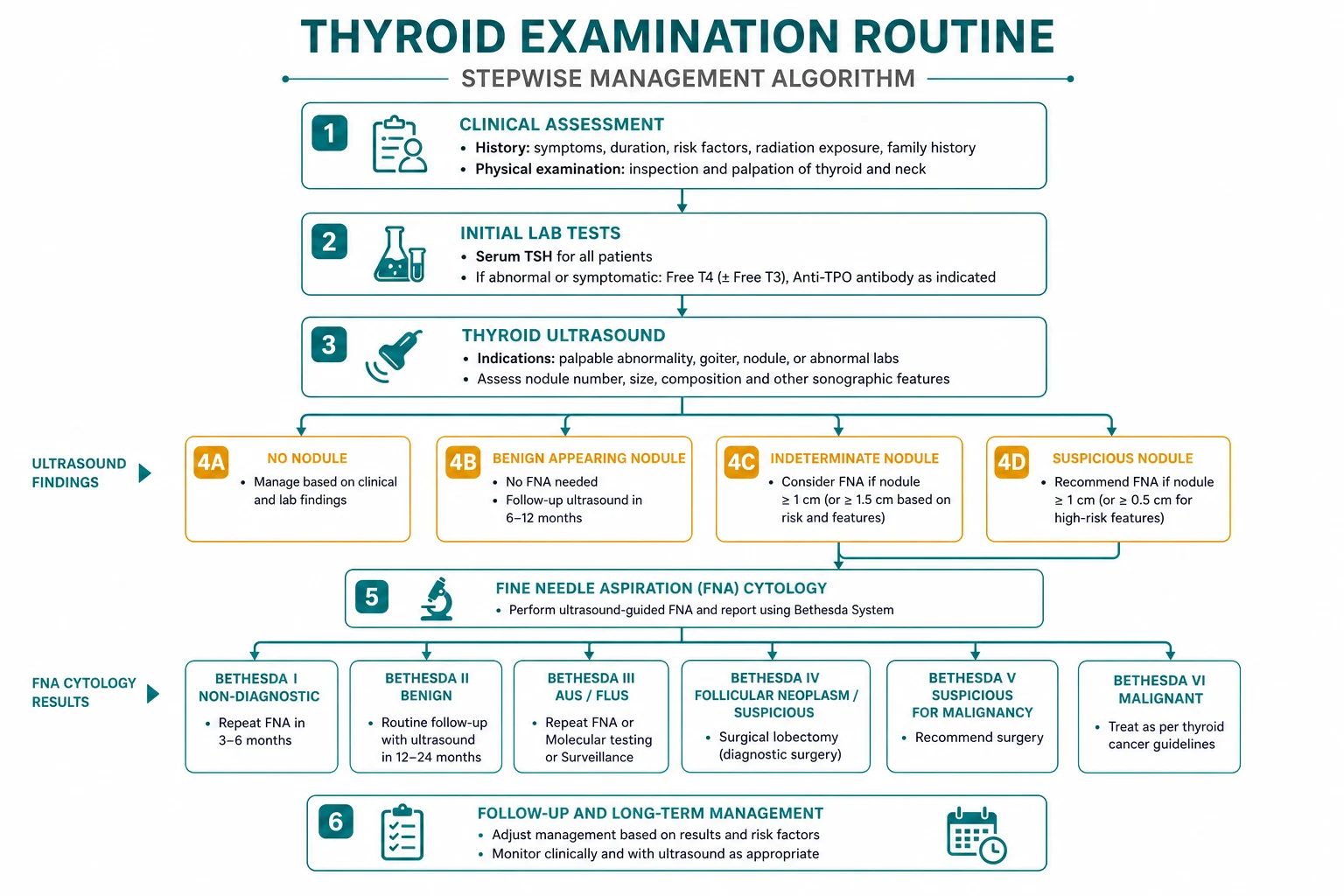
- Nodularity — is there a single dominant nodule (solitary thyroid nodule — investigate for malignancy with ultrasound and fine-needle aspiration), a multinodular gland (multinodular goitre — the commonest goitre in adults), or a smooth diffuse enlargement (Graves disease, Hashimoto thyroiditis)?
- Tenderness — a tender, painful goitre is subacute (de Quervain) thyroiditis, or suppurative thyroiditis, or haemorrhage into a cyst. Graves disease and Hashimoto thyroiditis are painless.
- Mobility — the thyroid should move freely on swallowing and should be mobile within the neck. A fixed gland (tethered to the trachea or the strap muscles) suggests malignancy or Riedel thyroiditis (a rare fibrosing disorder).
- Can you get below it? — place the fingers below the lower pole of each lobe. If you can get your fingers below the gland, it is entirely in the neck. If you cannot get below it, the gland extends retrosternally (behind the sternum), and you must percuss the sternum and image the chest. [1]
Palpate the cervical lymph nodes — the cervical chain (submental, submandibular, jugulodigastric, mid-jugular, lower jugular, posterior triangle) and the supraclavicular nodes. Cervical lymphadenopathy with a thyroid nodule is malignant until proven otherwise (papillary thyroid carcinoma metastasises to the cervical nodes; anaplastic carcinoma invades locally and metastasises widely). [1]
Palpate the trachea — place two fingers in the suprasternal notch and assess the tracheal position. A large goitre may deviate or compress the trachea. [1]
Step 7 — Percussion
Percuss the upper sternum (the manubrium) with the index finger. A dull percussion note over the upper sternum, where the note should be resonant (over the air-filled trachea), indicates a retrosternal goitre extending into the mediastinum. This is the bedside sign of retrosternal extension, confirmed by a chest X-ray or a CT scan. If you cannot get below the gland and the sternum is dull, state "There is retrosternal extension and I would image with a CT of the neck and chest." [1]
Step 8 — Auscultation
Auscultate over each lobe of the thyroid with the diaphragm of the stethoscope, while the patient holds the breath (to exclude the bruit of the carotid or the tracheal breath sounds). A thyroid bruit — a soft, continuous, systolic or to-and-fro murmur over the gland — indicates increased vascularity and is a sign of Graves disease (the gland is hyperaemic from the thyroid-stimulating immunoglobulins). A bruit does not occur in toxic multinodular goitre or toxic adenoma (which are less vascular), so the bruit is a discriminating sign for Graves among the causes of thyrotoxicosis. Distinguish the thyroid bruit from the carotid bruit (best heard over the carotid bifurcation, in the anterior triangle, and radiating toward the angle of the jaw) and from a venous hum (abolished by gentle compression of the jugular vein). [1]
Step 9 — Reflexes and legs
Complete the thyroid status assessment with the reflexes and the legs: [1]
- Reflexes — test the biceps, the triceps, the supinator and the knee jerks. In thyrotoxicosis the reflexes are brisk with a rapid, snapped contraction and relaxation. In hypothyroidism the reflexes show delayed relaxation — the muscle contracts normally but relaxes slowly, so the limb swings out and returns slowly (the "hung-up" reflex). Delayed relaxation of the ankle jerks is one of the most specific bedside signs of hypothyroidism and was the basis of the historical Achilles tendon reflex test.
- Pretibial myxoedema (thyroid dermopathy) — inspect the shins for raised, firm, non-pitting, waxy plaques or nodules, typically bilateral and symmetric over the pretibial area (and occasionally the dorsum of the feet). The lesions are caused by the deposition of glycosaminoglycans (hyaluronic acid) in the dermis, stimulated by the thyroid-stimulating hormone receptor antibodies acting on the skin fibroblasts. Pretibial myxoedema is specific to Graves disease (it does not occur in the other causes of thyrotoxicosis) and is almost always associated with orbitopathy. It completes the triad of orbitopathy, dermopathy and acropachy [3][4][5].
- Proximal muscle weakness — test the proximal muscles by asking the patient to rise from a squat (hip girdle) and to hold the arms out against resistance (shoulder girdle). Thyrotoxic myopathy produces proximal weakness, which may be the presenting complaint.
The thyroid status comparison — hyperthyroid versus hypothyroid

The thyroid short case requires you to commit to a thyroid status — hyperthyroid, euthyroid, or hypothyroid — based on the constellation of findings. The following table is the synthesis you present at the bedside: [1]
| Domain | Hyperthyroid (thyrotoxic) | Hypothyroid (myxoedematous) |
|---|---|---|
| General | Thin, agitated, restless, heat intolerance | Slow, puffy, lethargic, cold intolerance |
| Hands | Fine tremor, warm sweaty palms, palmar erythema, onycholysis, thyroid acropachy (Graves) | Cold, dry, coarse skin, slow movements |
| Pulse | Tachycardia, atrial fibrillation, bounding | Bradycardia |
| Blood pressure | Systolic hypertension, wide pulse pressure | Diastolic hypertension, narrow pulse pressure |
| Eyes | Exophthalmos, lid retraction, lid lag, ophthalmoplegia (Graves); lid lag and retraction (any cause) | Periorbital oedema, loss of outer third of eyebrows |
| Reflexes | Brisk | Delayed relaxation (hung-up) |
| Skin | Warm, moist, fine, pretibial myxoedema (Graves) | Cold, dry, coarse, yellow (carotenaemia) |
| Goitre | Diffuse smooth (Graves), multinodular, solitary toxic nodule; bruit (Graves) | May be present (Hashimoto), atrophic |
| Mental | Agitation, anxiety, proximal muscle weakness | Lethargy, depression, slow cognitive speed |
The exam principle: the examiner will ask you to state the thyroid status and defend it with the findings. The discriminating signs are the fine tremor, the warm sweaty palms and the brisk reflexes for hyperthyroid; the delayed-relaxation reflexes, the cold dry skin and the bradycardia for hypothyroid. The Graves-specific signs (exophthalmos, ophthalmoplegia, thyroid acropachy, pretibial myxoedema, thyroid bruit) identify the cause as Graves disease among the causes of thyrotoxicosis [6].
The presentation template
The model presentation follows a fixed structure: the summary statement with the thyroid status call, the positive findings grouped by examination stage, the relevant negatives, the cause (Graves versus other), the differential of the goitre, and the proposed investigation plan (blood pressure, height and weight, thyroid function tests, and the appropriate imaging). The presentation takes under two minutes and the examiner can interrupt at any point. [1]
Model presentation — Graves disease (hyperthyroid): [1]
"On general inspection, this thin, restless woman has a visible diffuse neck swelling and a staring appearance. In the hands, there is a fine tremor of the outstretched fingers, warm moist palms, and palmar erythema. The pulse is 110 beats per minute and irregularly irregular, consistent with atrial fibrillation. On examination of the eyes, there is bilateral exophthalmos with scleral show, lid retraction (the Dalrymple sign), and lid lag on downward gaze (the von Graefe sign). There is impaired upgaze and impaired convergence, consistent with ophthalmoplegia from Graves orbitopathy. There is conjunctival injection and chemosis. On examination of the neck from behind, there is a smooth, diffuse, symmetric enlargement of the thyroid gland, with a soft, firm consistency, no nodularity, no tenderness, and the gland is mobile on swallowing. I can get below the gland. There is no cervical lymphadenopathy. The trachea is central. Percussion over the sternum is resonant. On auscultation, there is a soft bruit over the gland. The reflexes are brisk. On the shins, there are raised, firm, waxy plaques consistent with pretibial myxoedema. In summary, this patient is clinically hyperthyroid, with the findings of Graves disease — the diffuse goitre with a bruit, the Graves orbitopathy, and the pretibial myxoedema. I would like to measure the blood pressure for a wide pulse pressure, measure the height and weight, and check the thyroid function tests — I expect a suppressed TSH with an elevated free T4 and free T3, and positive thyroid-stimulating immunoglobulins and TSH receptor antibodies." [1]
Model presentation — multinodular goitre (euthyroid or subclinical): [1]
"On general inspection, this comfortable woman has a visible asymmetric neck swelling. The pulse is 78 and regular. The hands are normal — no tremor, no thyroid acropachy, no onycholysis. The eyes are normal — no exophthalmos, no lid lag, no lid retraction, no ophthalmoplegia. On examination of the neck from behind, there is an asymmetric, multinodular enlargement of the thyroid gland, with a firm consistency, several discrete nodules of varying size, no tenderness, and the gland is mobile on swallowing. I cannot get below the lower pole of the right lobe. The trachea is central. Percussion over the upper sternum is dull, suggesting retrosternal extension. There is no bruit. The reflexes are normal. In summary, this patient has a multinodular goitre with retrosternal extension. I would like to check the thyroid function tests, perform a thyroid ultrasound, and image the retrosternal extension with a CT of the neck and chest." [1]
Model presentation — hypothyroidism (myxoedema): [1]
"On general inspection, this woman appears slow and puffy-faced, with dry skin and a general appearance of physical and mental slowing. The pulse is 52 and regular. The hands are cold and dry, with coarse skin. The eyes show periorbital oedema and loss of the outer third of the eyebrows. There is no exophthalmos, no lid retraction. On examination of the neck, there is a small, firm, granular, diffuse enlargement of the thyroid, consistent with Hashimoto thyroiditis. The reflexes show delayed relaxation, particularly at the ankle jerks. In summary, this patient is clinically hypothyroid, with the findings of Hashimoto thyroiditis — the firm granular goitre, the myxoedematous appearance, and the delayed-relaxation reflexes. I would like to check the thyroid function tests — I expect an elevated TSH with a low free T4 — and the anti-thyroid peroxidase antibodies, which I expect to be strongly positive." [1]
Examiner discussion questions — by finding
The examiner will ask probing questions after the examination. The common questions and the model answers: [1]
Q: "How do you distinguish Graves disease from the other causes of thyrotoxicosis clinically?" [1]
"The clinical distinction is the presence of Graves-specific signs. Graves disease is the only cause of thyrotoxicosis that produces orbitopathy (exophthalmos, ophthalmoplegia), so the presence of eye signs makes the diagnosis. The other Graves-specific findings are pretibial myxoedema, thyroid acropachy, and a thyroid bruit (from the hyperaemic, vascular gland). Toxic multinodular goitre produces a multinodular goitre without eye signs or a bruit; toxic adenoma produces a single palpable nodule without eye signs; and thyroiditis produces a tender or normal gland with a transient thyrotoxicosis. The laboratory confirmation is the TSH receptor antibody or the thyroid-stimulating immunoglobulin, which is positive in Graves disease and negative in the other causes [6]."
Q: "What is the Clinical Activity Score and when do you use it?" [1]
"The Clinical Activity Score, the CAS, is the seven-item bedside score for the activity of Graves orbitopathy. The seven items are spontaneous retrobulbar pain, pain on eye movement, eyelid erythema, conjunctival injection, chemosis, swelling of the caruncle, and eyelid oedema or fullness — each scores one point, for a maximum of seven. A score of three or more out of seven indicates active disease, which predicts a response to immunosuppression with intravenous methylprednisolone. I use the CAS at the bedside to decide whether the orbitopathy is active (and may benefit from glucocorticoids) or inactive (where treatment is rehabilitative surgery). The CAS measures activity, while the severity is graded separately as mild, moderate-to-severe, or sight-threatening, based on the degree of proptosis, diplopia, and optic nerve function [1][2]."
Q: "What are the sight-threatening complications of Graves orbitopathy that you must check for?" [1]
"The two sight-threatening complications are optic nerve compression and corneal exposure. Optic nerve compression occurs when the swollen extraocular muscles compress the optic nerve at the orbital apex; the signs are reduced visual acuity, impaired colour vision (red desaturation), a relative afferent pupillary defect, and visual field defects. Corneal exposure occurs from the severe proptosis and the lid retraction, which prevent eyelid closure (lagophthalmos), leading to exposure keratopathy. At the bedside, I check the visual acuity with a Snellen chart, the colour vision with an Ishihara plate or a red target (for red desaturation), the visual fields by confrontation, and the pupillary reflexes. Any abnormality is a sight-threatening emergency requiring urgent ophthalmology referral and high-dose intravenous glucocorticoids or urgent orbital decompression [1][2]."
Q: "How do you palpate the thyroid gland correctly, and why from behind?" [1]
"The thyroid gland is palpated from behind the seated patient. I ask the patient to sit upright on the edge of the bed with the neck slightly flexed to relax the sternocleidomastoid. I place both hands around the neck with the fingertips over the gland — the isthmus across the trachea below the cricoid, and the two lobes on either side. I identify the gland, then I give the patient a sip of water to hold in the mouth and ask them to swallow as I palpate. The gland moves upward on swallowing, which allows me to feel the lower border, the consistency, the nodularity and the mobility. The behind-the-patient approach is used because the thyroid sits deep to the strap muscles and the sternocleidomastoid, and the fingertips from behind can feel the gland between the trachea and the muscle, whereas the thumb approach from the front compresses the gland against the trachea and gives a less reliable assessment of consistency and nodularity." [1]
Q: "What does a thyroid bruit mean, and how do you distinguish it from a carotid bruit?" [1]
"A thyroid bruit is a soft, continuous, systolic or to-and-fro murmur heard over the thyroid gland, caused by the increased vascularity of Graves disease — the gland is hyperaemic from the thyroid-stimulating immunoglobulins acting on the TSH receptors of the follicular cells. A thyroid bruit does not occur in toxic multinodular goitre or toxic adenoma, so it is a discriminating sign for Graves among the causes of thyrotoxicosis. I distinguish it from a carotid bruit by the location — the thyroid bruit is over the gland (central, over the trachea), while the carotid bruit is over the carotid bifurcation (lateral, in the anterior triangle, and radiating to the angle of the jaw). I also distinguish it from a venous hum, which is abolished by gentle compression of the jugular vein." [1]
Q: "What does retrosternal extension mean, and how do you detect it at the bedside?" [1]
"Retrosternal extension means that the lower pole of the thyroid gland extends behind the sternum into the mediastinum. This is significant because the retrosternal goitre can compress the trachea (causing stridor and dyspnoea), the oesophagus (causing dysphagia), or the great veins (causing superior vena cava obstruction — facial plethora and dilated neck veins). At the bedside, I detect it by three signs: I cannot get my fingers below the lower pole of the gland (the gland extends below the clavicle), the percussion note over the upper sternum is dull (where it should be resonant over the trachea), and the Pemberton sign may be positive (the patient develops facial plethora and distended neck veins on raising both arms above the head, because the clavicles compress the retrosternal goitre against the great veins). I confirm with a CT of the neck and chest." [1]
Q: "Why does the patient with hypothyroidism have delayed-relaxation reflexes?" [1]
"The delayed-relaxation reflex — the hung-up reflex — is one of the most specific bedside signs of hypothyroidism. The muscle contracts normally in response to the tendon tap, but the relaxation phase is prolonged, so the limb swings out and returns slowly. The mechanism is the slowed contraction and relaxation of the skeletal muscle fibres, caused by the reduced availability of calcium to the sarcoplasmic reticulum and the slowed reuptake of calcium, in the hypothyroid state. The reflex is most apparent at the ankle jerks (the Achilles tendon reflex), and it was the basis of the historical Achilles tendon reflex recovery time test, which used a photomotograph to measure the relaxation half-time. A delayed-relaxation ankle jerk in a patient with a bradycardia and cold dry skin is clinically diagnostic of hypothyroidism before the blood test." [1]
Q: "What is the significance of pretibial myxoedema and how does it relate to the other Graves manifestations?" [1]
"Pretibial myxoedema, or thyroid dermopathy, is the deposition of glycosaminoglycans (hyaluronic acid) in the dermis of the shins, producing raised, firm, non-pitting, waxy plaques or nodules. It is caused by the thyroid-stimulating hormone receptor antibodies stimulating the skin fibroblasts to produce excess glycosaminoglycans, the same mechanism that operates in the orbit in Graves orbitopathy. Pretibial myxoedema is specific to Graves disease and is almost always associated with orbitopathy — in the review of 150 cases by Fatourechi, almost all patients with dermopathy had ophthalmopathy, and the dermopathy was a late manifestation following the hyperthyroidism and the orbitopathy. The rare thyroid acropachy completes the triad of exophthalmos, myxoedema (dermopathy) and osteoarthropathy (acropachy) that defines severe Graves autoimmune disease [3][4][5]."
High-yield exam traps
-
The omitted end-of-bed inspection. The five-second observation reveals the thyroid status before you touch the patient. The candidate who walks straight to the neck has demonstrated a failure of the systematic approach and has lost the first-impression marks. State your impression of hyperthyroid, euthyroid or hypothyroid before you begin. [1]
-
The position trap — palpating from the front. The thyroid examination is performed from behind the seated patient. The candidate who stands in front and palpates with the thumbs has demonstrated a fundamental technique error. Stand behind, place the fingertips over the gland, and palpate during swallowing. [1]
-
The thyroid status versus the gland trap. The instruction "examine the thyroid status" means you must assess the patient's thyroid status (hyperthyroid, euthyroid, hypothyroid) AND the gland. The candidate who examines only the neck has done half the examination. The hands (tremor, acropachy, onycholysis), the pulse, the eyes, the reflexes and the shins are all part of the thyroid status assessment, and they are the findings that win marks. [1]
-
The eye signs trap — attributing all eye signs to Graves. Lid retraction (Dalrymple sign) and lid lag (von Graefe sign) occur in any cause of thyrotoxicosis from the sympathetic overdrive; they are not specific to Graves. The signs specific to Graves are exophthalmos (proptosis), ophthalmoplegia, chemosis and conjunctival injection — because only Graves orbitopathy involves the retro-orbital tissues. The candidate who attributes lid lag to Graves has overstated the specificity of the sign. [1]
-
The CAS trap — confusing activity with severity. The Clinical Activity Score (CAS) measures the inflammatory activity of Graves orbitopathy (a score of three or more out of seven indicates active disease). It does not measure severity. The severity is graded separately (mild, moderate-to-severe, sight-threatening) based on the degree of proptosis, diplopia and optic nerve function. The candidate who uses the CAS as a severity score has confused the two domains [1][2].
-
The goitre consistency trap. A smooth, diffuse, soft goitre is Graves disease (or Hashimoto thyroiditis in the hypothyroid patient). A firm, granular, asymmetric goitre with a pyramidal lobe is Hashimoto thyroiditis. A hard, irregular, fixed goitre in an older patient is anaplastic or poorly differentiated thyroid carcinoma until proven otherwise. A tender, warm, painful goitre is subacute (de Quervain) thyroiditis. The candidate who describes a goitre without stating the consistency has not completed the examination. [1]
-
The "get below it" trap. If you cannot get your fingers below the lower pole of the gland, the goitre has retrosternal extension. The candidate who fails to check this sign, and who fails to percuss the sternum for the dull note of retrosternal extension, has missed a critical finding that determines the imaging and the surgical approach. [1]
-
The forgotten Pemberton sign. In a patient with a retrosternal goitre, the Pemberton sign (facial plethora and distended neck veins on raising both arms) demonstrates the thoracic inlet obstruction. The candidate who does not offer the Pemberton sign in the retrosternal goitre has missed a discriminating bedside test that the examiner expects. [1]
-
The reflex trap — failing to test for delayed relaxation. The delayed-relaxation ankle jerk is one of the most specific bedside signs of hypothyroidism. The candidate who tests the reflexes for presence and briskness but does not assess the relaxation phase has missed the finding. The relaxation phase is where the sign lives. [1]
-
The closure trap — failing to offer the complete investigations. The candidate who presents the findings and stops has not closed the examination. The closure must include: measure the blood pressure (for the wide pulse pressure of thyrotoxicosis), measure the height and weight, and order the thyroid function tests (TSH, free T4, free T3), the thyroid antibodies (TSH receptor antibodies for Graves, anti-thyroid peroxidase antibodies for Hashimoto), and the appropriate imaging (thyroid ultrasound for a nodule, CT of the neck and chest for a retrosternal goitre). The closure is where the synthesis marks are won. [1]
Key points for the viva
- The thyroid examination is performed from behind the seated patient, in a nine-step sequence: general inspection, hands, pulse, eyes, neck inspection, neck palpation (during swallowing), percussion over the sternum, auscultation of the thyroid, and reflexes plus legs. Perform it in the same order every time.
- State the thyroid status (hyperthyroid, euthyroid, hypothyroid) before you reach the gland, and defend it with the findings — the fine tremor and brisk reflexes for hyperthyroid, the delayed-relaxation reflexes and cold dry skin for hypothyroid.
- The Graves-specific signs are exophthalmos, ophthalmoplegia, thyroid acropachy, pretibial myxoedema and a thyroid bruit. These do not occur in the other causes of thyrotoxicosis (toxic multinodular goitre, toxic adenoma, thyroiditis).
- Lid retraction (Dalrymple sign) and lid lag (von Graefe sign) occur in any cause of thyrotoxicosis from sympathetic overdrive; they are not specific to Graves.
- Score the eye signs with the Clinical Activity Score (CAS): a score of three or more out of seven indicates active Graves orbitopathy, which predicts a response to immunosuppression. The seven items are pain (retrobulbar and on movement), eyelid erythema, conjunctival injection, chemosis, caruncle swelling, and eyelid oedema.
- Palpate the gland from behind during swallowing for size, consistency, nodularity, tenderness, mobility, and whether you can get below it. Percuss the sternum for retrosternal extension. Auscultate for a bruit.
- Always check for retrosternal extension: you cannot get below the gland, the sternum is dull to percussion, and the Pemberton sign may be positive.
- Always close the examination: measure the blood pressure and the height and weight, and order the thyroid function tests with the appropriate antibodies and imaging.
- Cross-link the management of Graves disease, hyperthyroidism, hypothyroidism and thyroid storm to the dedicated thyroid-disorders topic, which carries the drug doses, the radioactive iodine and surgery pathways, and the long-term follow-up. [1]
References
- [1]Bartalena L, Baldeschi L, Boboridis K, Eckstein A, Kahaly GJ, et al.; European Group on Graves' Orbitopathy (EUGOGO) The 2016 European Thyroid Association/European Group on Graves' Orbitopathy Guidelines for the Management of Graves' Orbitopathy Eur Thyroid J, 2016.PMID 27099835
- [2]Bartalena L, Kahaly GJ, Baldeschi L, Dayan CM, Eckstein A, et al. The 2021 European Group on Graves' orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves' orbitopathy Eur J Endocrinol, 2021.PMID 34297684
- [3]Bartalena L, Fatourechi V Extrathyroidal manifestations of Graves' disease: a 2014 update J Endocrinol Invest, 2014.PMID 24913238
- [4]Fatourechi V Pretibial myxedema: pathophysiology and treatment options Am J Clin Dermatol, 2005.PMID 16252929
- [5]Fatourechi V, Pajouhi M, Fransway AF Dermopathy of Graves disease (pretibial myxedema). Review of 150 cases Medicine (Baltimore), 1994.PMID 8309359
- [6]Ross DS, Burch HB, Cooper DS, Greenlee MC, Laurberg P, Maia AL, et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis Thyroid, 2016.PMID 27521067