Phys · general-medicine
The Undifferentiated Altered Mental Status — A Systematic Diagnostic Approach
Also known as altered mental status · acute confusion · delirium · acute encephalopathy · confused patient · DIMTOP · Confusion Assessment Method · CAM · Wernicke encephalopathy · hepatic encephalopathy · sepsis-associated encephalopathy · non-convulsive status epilepticus · subdural haematoma · cognitive assessment · metabolic encephalopathy · hospital-acquired delirium
Consultant-physician-depth guide to the systematic approach to the acutely confused or delirious patient. Covers the ABCDE resuscitation-first principle, the DIMTOP mnemonic for causes (Drugs, Infection, Metabolic, Trauma, Oxygen, Psychiatric), the collateral history, the focused neurological and systemic examination, the tiered investigation ladder (bedside glucose, blood gas, electrolytes, infection screen, CT head, lumbar puncture, EEG), the rapidly reversible causes (glucose, oxygen, sodium, calcium, thiamine), the Confusion Assessment Method (CAM) diagnostic algorithm, the management principle of treating the underlying cause with symptomatic sedation as a last resort, and the special considerations for the elderly, the postoperative, and the immunocompromised patient. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The Undifferentiated Altered Mental Status — A Systematic Diagnostic Approach

The answer first
The acutely confused patient is a systemic emergency wearing a neurological disguise. The brain is the end-organ of every organ system in the body, and an acute change in mental status — whether confusion, agitation, drowsiness, or coma — means that something has gone wrong somewhere, and the brain is reporting it. The registrar's job is not to diagnose the confusion but to find the cause, because the confusion is a symptom and the cause is the disease, and treating the symptom without the cause is the surest way to miss a rapidly reversible and potentially fatal problem. [1]
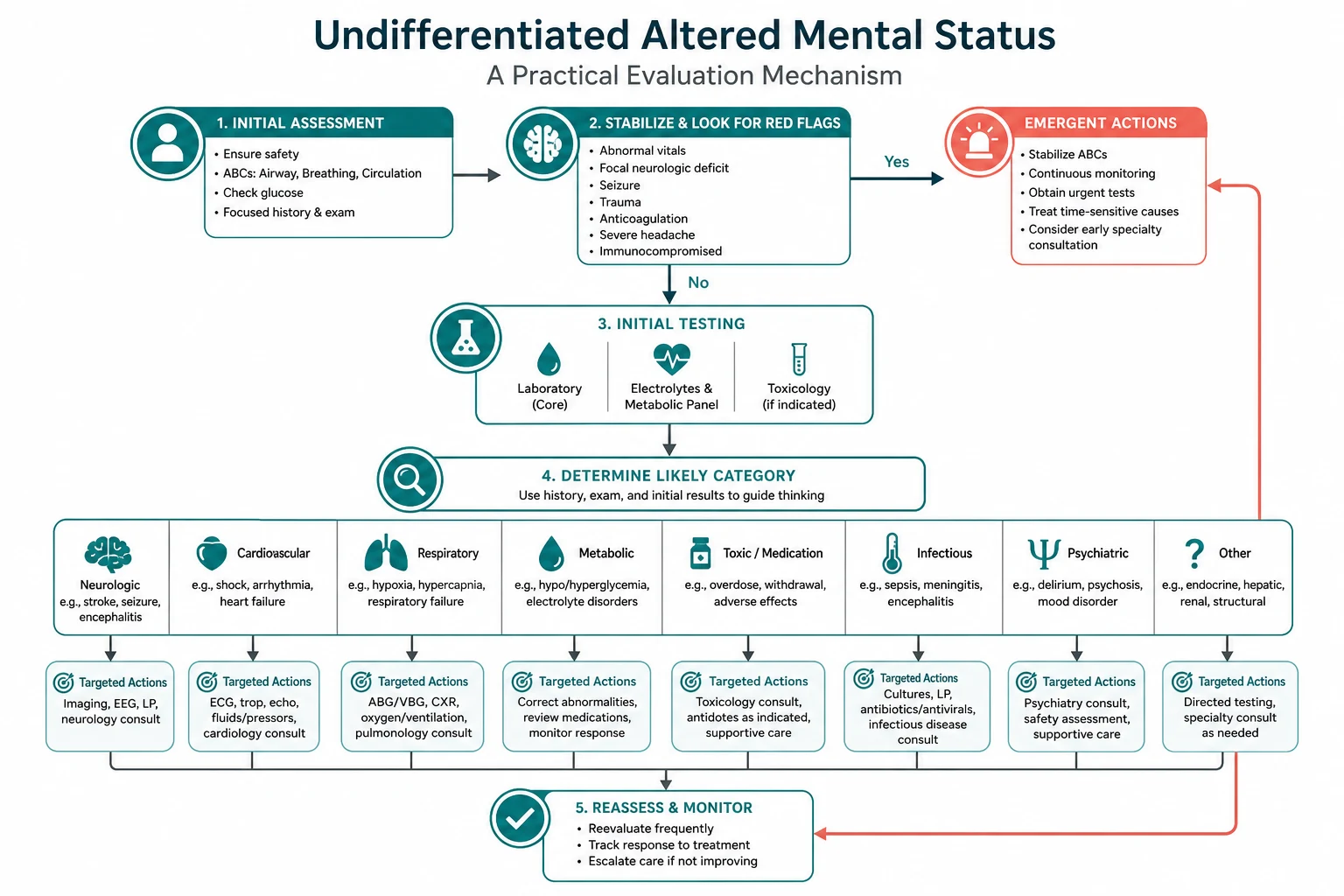
The reproducible sequence for any undifferentiated altered mental status is: [1]
- Resuscitate first (ABCDE). Secure the airway, give oxygen, support the circulation, and — within the first minute — check a finger-prick glucose. Hypoglycaemia is the single most rapidly reversible cause of altered mental status, and it is the one cause that kills you in minutes if you miss it.
- Establish the baseline and the change. The diagnosis of delirium (acute change, fluctuating, inattention) versus dementia (chronic, progressive) versus psychiatric disorder requires the collateral history. Ask: what is the baseline cognition, when did this start, has it fluctuated, and what has changed in the medications, the alcohol, and the intercurrent illness?
- Work the DIMTOP differential. Drugs, Infection, Metabolic, Trauma, Oxygen, Psychiatric — with Vascular added for the stroke and TIA. You do not anchor on the first plausible cause; you work through each category systematically.
- Target the investigation ladder to the clinical picture. The bedside panel (glucose, vital signs, ECG, blood gas) catches the immediate threats. The laboratory panel (FBC, U&E, LFTs, calcium, TSH, CRP, cultures, troponin) catches the systemic causes. The imaging and special tests (CT head, LP, EEG) are selective, guided by focal neurology, trauma, anticoagulation, or a failure to recover.
- Treat the cause; sedate last. The management is the treatment of the underlying cause — the infection, the electrolyte disturbance, the drug withdrawal, the hypoxia. Symptomatic sedation with low-dose haloperidol is reserved for the agitation that endangers the patient or the delivery of essential care. Benzodiazepines are avoided in delirium except in alcohol or benzodiazepine withdrawal, where they are first-line. [1]
The single most dangerous error is labelling the confusion as a primary psychiatric problem before excluding the medical causes. A first presentation of acute psychosis or mania in an older patient is, until proven otherwise, a delirium with a medical cause. The second error is omitting the finger-prick glucose — a failure that costs lives and careers. The third is giving glucose before thiamine in the patient at risk of Wernicke encephalopathy, a mistake that converts a reversible nutritional deficiency into an irreversible brainstem injury. [1]
Viva trap: "What is the first thing you do when called to see a confused patient?" The answer is not the cognitive assessment and not the CT scan — it is the ABCDE with a finger-prick glucose. The confused patient who is hypoxic, hypoglycaemic, or in shock needs those problems fixed before any diagnostic reasoning, because they will die of the metabolic derangement while you are testing their orientation. The glucose takes ten seconds, the oxygen takes thirty, and together they have saved the patient before the workup has begun. [1]
Defining the problem — delirium, dementia, and psychiatric disorder
Altered mental status is an umbrella term for an acute disturbance in attention, awareness, or cognition. The three entities it encompasses are distinct, and the distinction matters because the management diverges immediately. [1]
Delirium (also called acute encephalopathy) is defined by its acute onset, its fluctuating course, and the inattention that is its hallmark. The Confusion Assessment Method (CAM), developed by Inouye and colleagues in 1990 and validated across thousands of patients, captures the diagnostic algorithm in four features [1]:
| Feature | CAM criterion | What it looks like at the bedside |
|---|---|---|
| 1 | Acute onset and fluctuating course | A change from the baseline cognition, with symptoms that come and go through the day |
| 2 | Inattention | Difficulty focusing, easily distracted, losing track of the conversation, unable to do the months of the year backwards |
| 3 | Disorganised thinking | Rambling, irrelevant, or illogical flow of ideas; unpredictable switching between topics |
| 4 | Altered level of consciousness | Anything other than alert — vigilant (hyperalert), lethargic, stuporous, or comatose |
A diagnosis of delirium requires Features 1 and 2 plus either Feature 3 or 4. The beauty of the CAM is its simplicity — a trained clinician can apply it in under five minutes at the bedside, and the original validation showed a sensitivity of 94 to 100 per cent and a specificity of 90 to 95 per cent against psychiatrist assessment [1]. It is the tool the examiner expects you to name and to use.
Dementia is the contrast. It is chronic, progressive, and — in its early stages — characterised by preserved attention. The patient with early Alzheimer disease can still focus, still track a conversation, still do the months of the year backwards; their problem is one of memory and new learning, not of attention. The acute deterioration in a patient with known dementia is still a delirium until proven otherwise — the dementia is the predisposing factor, and the acute change is the precipitant that must be found. This is the single most common error at the bedside: the nurse says "he has dementia" and the team stops looking for the reversible cause. Dementia is the background; delirium is the foreground; the acute change is the emergency. [1]
Primary psychiatric disorders — depression with pseudodementia, psychotic disorders, manic episodes — can present with acute confusion, but they are rare as first presentations in older adults, and they are diagnoses of exclusion. The cardinal rule: a first episode of acute psychosis or mania in a patient over 40 has a medical cause until proven otherwise. The psychiatric diagnosis is made only after the metabolic, infectious, toxic, and structural causes have been excluded by the workup described below. [1]
The reason this distinction matters is that the management diverges. Delirium is treated by finding and reversing the precipitant; dementia is managed with cognitive support, cholinesterase inhibitors in selected cases, and advance care planning; primary psychiatric disorder is treated with psychotropics and psychiatric referral. The misdiagnosis — treating a delirium as a dementia, or a delirium as a psychiatric disorder — delays the reversal of a treatable cause and causes avoidable harm. [1]
DWE high-yield: The most testable fact about delirium is the multifactorial model. Inouye's 2006 NEJM review established that delirium is almost always the result of the interaction between a vulnerable patient (predisposing factors — age, baseline cognitive impairment, sensory deprivation, polypharmacy, multimorbidity) and an acute insult (precipitating factors — infection, surgery, drugs, electrolyte disturbance, hypoxia, urinary retention, constipation) [2]. The implication for management is that there is rarely a single cause to find and fix; there are usually several, and the workup must address all of them. The corollary is that delirium is preventable in a large proportion of cases through the targeting of the predisposing and precipitating factors — this is the basis of the delirium prevention bundles (HELP — the Hospital Elder Life Program — and the NICE CG103 recommendations).
The ABCDE resuscitation gate

The approach to the confused patient begins with resuscitation, not diagnosis. The principle is the same as for any acutely unwell patient: assess and treat in order, and do not move past a compromised system until it is either resolved or supported. [1]
A — Airway
Is the airway patent? The confused patient may have a depressed conscious level (GCS 8 or below) that compromises airway protection, or they may be agitated and at risk of aspiration. Assess with the look-listen-feel technique: chest movement, breath sounds, expired air. Signs of obstruction include snoring (tongue), gurgling (secretions), and stridor (upper-airway obstruction). Basic manoeuvres (head tilt, chin lift, jaw thrust) and adjuncts (oropharyngeal if GCS is low, nasopharyngeal if gag is intact) are the first interventions. If the airway cannot be secured, call for senior airway help immediately — the confused patient who cannot protect their airway is an anaesthetic emergency. [1]
B — Breathing
Once the airway is patent or supported, assess breathing. Measure the respiratory rate, the oxygen saturation, and the work of breathing. Give oxygen to the acutely hypoxaemic patient — high-flow via a reservoir mask at 15 L/min for the critically ill, titrated down once the saturation is in the safe range (92 to 96 per cent for most patients; 88 to 92 per cent for the known chronic CO2 retainer). Check a blood gas early if there is any concern about ventilation or acid-base — a rising CO2 is a cause of confusion in its own right (CO2 narcosis in the COPD patient, the oversedated patient, or the patient with a neuromuscular respiratory failure), and an arterial or venous gas catches the metabolic acidosis that underlies DKA, lactic acidosis from sepsis, and uraemia. The respiratory rate is the leading indicator; a high rate signals hypoxia, acidaemia, pain, or sepsis, and a low rate signals opioid, sedative, or neurological depression. [1]
C — Circulation
Assess heart rate and rhythm (a 12-lead ECG plus continuous monitoring), blood pressure, capillary refill, peripheral pulses, JVP, skin temperature and mottling, and urine output. Two large-bore cannulae, a fluid challenge of balanced crystalloid for the hypovolaemic or septic patient, and the cause-specific therapy. The ECG is mandatory in every confused patient — a silent myocardial infarction presenting as confusion in the elderly diabetic, a fast atrial fibrillation causing cerebral hypoperfusion, and the peaked T waves of hyperkalaemia are all diagnoses that the ECG catches in under a minute. Interpret the blood pressure against the patient's baseline — a systolic of 110 in a chronic hypertensive whose baseline is 170 is a 60 mmHg drop and represents significant shock. [1]
D — Disability
This is where the altered mental status lives, but it comes after the airway, breathing, and circulation have been secured. The D-step has four components, and the order within them matters: [1]
- Conscious level. Record the GCS (eye, verbal, motor — out of 15) or AVPU (Alert, Voice, Pain, Unresponsive). The trend is more informative than a single value.
- Pupils. Size, symmetry, reactivity. Pinpoint pupils suggest opioids; dilated pupils suggest anticholinergics or tricyclic antidepressants; a unilateral fixed and dilated pupil is uncal herniation until proven otherwise and requires immediate imaging and neurosurgical consultation.
- Focal neurology. A quick screen of limb power, tone, reflexes, and plantar responses. An asymmetry — a weak arm, an upgoing plantar, a facial droop — changes the differential immediately and mandates a CT head.
- Finger-prick glucose. This is the single most important investigation in the entire workup. Hypoglycaemia is rapidly reversible, common (especially in the diabetic on insulin or sulfonylurea), and catastrophically missed if not measured. A glucose of 2.0 mmol/L can present as anything from mild confusion to seizure to coma, and the treatment — 50 mL of 50 per cent dextrose intravenously, or 1 mg of glucagon intramuscularly if no IV access — reverses it in minutes. [1]
The thiamine rule. In any patient at risk of thiamine deficiency (alcohol use disorder, malnutrition, prolonged vomiting, hyperemesis gravidarum, post-bariatric surgery, malabsorption, dialysis dependence), give thiamine before or alongside the glucose. Giving dextrose to a thiamine-depleted patient precipitates acute Wernicke encephalopathy by forcing the depleted pyruvate dehydrogenase pathway to fail catastrophically [4]. The dose in Australia is 500 mg intravenously, and it should be given routinely to every patient at risk — the downside of giving it unnecessarily is negligible, and the downside of omitting it in the patient who needs it is irreversible brain injury.
E — Exposure
Fully expose the patient and examine systematically. Temperature (fever or hypothermia suggests infection; hyperthermia suggests sepsis, heat stroke, serotonin syndrome, neuroleptic malignant syndrome, or anticholinergic toxicity). The skin — rashes (meningococcal, vasculitic, drug eruption), bruises (coagulopathy, trauma), pressure areas, surgical wounds, line sites, the diabetic foot. The abdomen — distension, tenderness, rigidity (peritonitis, urinary retention, constipation, mesenteric ischaemia). The drug chart — every drug, every dose, every recent change. And the personal belongings — an empty medication bottle, a hospital wristband from another institution, a diabetic card, a heroin-user's needle track. [1]
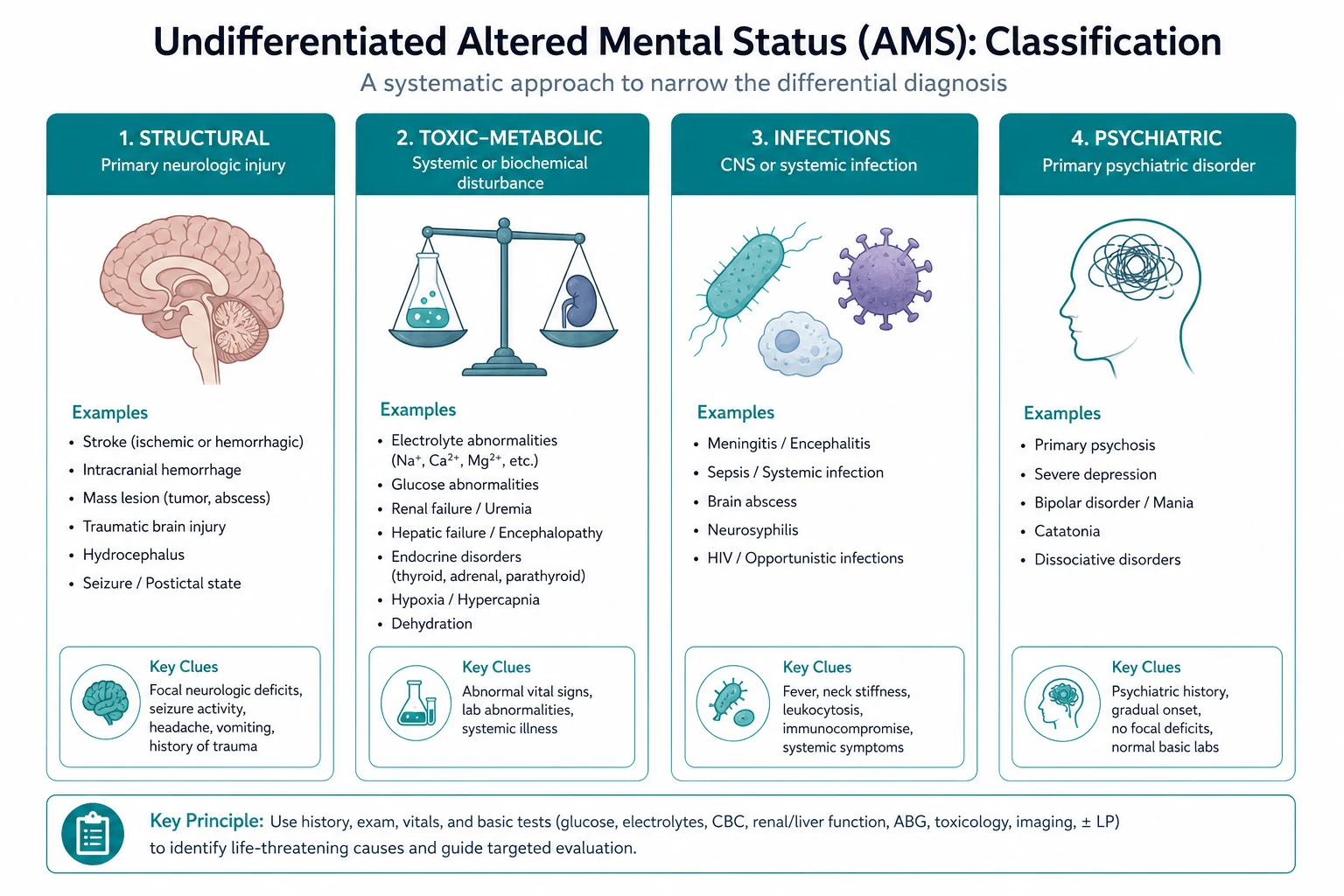
The DIMTOP differential
Once the resuscitation is under way and the immediate reversible causes have been checked, the diagnostic workup proceeds systematically through the causes of acute confusion. The DIMTOP mnemonic (with Vascular as a seventh category in many curricula) is the framework that ensures no category is missed. [1]
D — Drugs
Drugs are the single most common iatrogenic cause of acute confusion, and the drug chart is the highest-yield document in the unexplained delirium. The high-yield culprits: [1]
| Drug class | Mechanism of confusion | Clinical clues |
|---|---|---|
| Anticholinergics (oxybutynin, hyoscine, tricyclics, first-generation antihistamines) | Central muscarinic blockade | Dry mouth, dilated pupils, urinary retention, flushed dry skin, mydriasis |
| Opioids (morphine, oxycodone, fentanyl, codeine) | Mu-receptor-mediated sedation and respiratory depression | Pinpoint pupils, low respiratory rate, drowsiness |
| Benzodiazepines (diazepam, lorazepam, temazepam) | GABA-A potentiation | Sedation, ataxia, slurred speech; reversed selectively by flumazenil |
| Anticonvulsants (valproate, phenytoin, levetiracetam, gabapentin) | Dose-dependent cerebellar and cortical effects | Ataxia, nystagmus; check levels for phenytoin and valproate |
| Corticosteroids (prednisolone, dexamethasone) | Steroid-induced psychosis or affective change | High-dose, recent initiation or escalation |
| Digoxin | Digoxin toxicity, especially in renal failure and hypokalaemia | Visual disturbance (yellow vision), nausea, arrhythmia |
| Lithium | Narrow therapeutic index; toxicity in dehydration or renal failure | Coarse tremor, hyperreflexia, ataxia; check level |
| Dopaminergics (levodopa, pergolide) | Dopamine excess in the limbic system | Visual hallucinations, vivid dreams, agitation in Parkinson disease |
| Drug withdrawal | Alcohol, benzodiazepine, opioid withdrawal | Tremor, autonomic hyperactivity (tachycardia, hypertension, fever), hallucinations |
The approach is to review every drug on the chart, hold the causative agents, and check levels where relevant (lithium, digoxin, valproate, phenytoin). The specific antidotes belong to the D-step of the resuscitation: naloxone for opioid (0.4 to 2 mg intravenously, repeated up to 10 mg if no response), flumazenil for benzodiazepine (0.2 mg intravenously, repeated with caution — it can precipitate seizures in the benzodiazepine-dependent patient), and physostigmine for severe anticholinergic toxicity (used selectively, not routinely). [1]
Drug withdrawal is the one delirium where benzodiazepines are first-line, not last-resort. Alcohol withdrawal classically presents 6 to 48 hours after the last drink with tremor, autonomic hyperactivity (tachycardia, hypertension, fever), anxiety, insomnia, and progression to visual hallucinations, seizures, and delirium tremens. The CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol, revised) score guides the symptom-triggered diazepam regimen. The confused patient with a history of heavy alcohol use, a high CIWA score, and autonomic signs has alcohol withdrawal until proven otherwise, and the treatment is a long-acting benzodiazepine — not haloperidol. [1]
I — Infection
Infection is the commonest single cause of acute confusion in the elderly hospitalised patient, and the search must be systematic. The sources, in order of frequency: [1]
- Urinary tract infection — the commonest source in the elderly; check the urine (dipstick and MC&S), but remember that asymptomatic bacteriuria is common in the elderly and catheterised patient, and a positive urine culture alone does not prove the UTI is the cause of the confusion.
- Pneumonia — check the chest (examination, oxygen saturation, chest X-ray), and look for the atypical presentation in the elderly (no fever, no cough, just confusion).
- Skin and soft tissue — cellulitis, infected pressure ulcers, infected diabetic foot ulcers, necrotising fasciitis.
- Intra-abdominal — biliary sepsis, diverticulitis, perforated viscus, appendicitis (atypical in the elderly), peritonitis, intra-abdominal abscess.
- Central nervous system — meningitis, encephalitis, brain abscess. The confused patient with fever and headache or neck stiffness has meningitis or encephalitis until proven otherwise, and the management is the antibiotic within one hour, the CT head, and the lumbar puncture — in that order.
- Line-related and device-related — central line infection, peripheral cannula site infection, infected urinary catheter, prosthetic device infection. [1]
Sepsis-associated encephalopathy — a diffuse brain dysfunction secondary to the systemic inflammatory response, in the absence of direct CNS infection — is a distinct entity and a diagnosis of exclusion. The pathophysiology involves neuroinflammation, blood-brain barrier dysfunction, cerebral perfusion alterations, and neurotransmitter imbalance, and it is strongly associated with increased mortality and long-term cognitive impairment in survivors [6]. The clinical point: in the septic patient, the confusion may be the brain's response to the systemic inflammation rather than a direct CNS infection, but the workup must still exclude the latter.
The infection screen for the confused patient is: blood cultures (two sets, before the antibiotic), urine MC&S, chest X-ray, and CRP. The antibiotic is broad-spectrum, guided by the suspected source and the local guideline, and given within one hour of the recognition of sepsis. The lumbar puncture is reserved for the patient with suspected CNS infection, after the CT has excluded a mass lesion. [1]
M — Metabolic
The metabolic causes of confusion are the most easily missed and the most easily treated, and the bedside panel catches the majority. The high-yield derangements: [1]
- Hypoglycaemia — glucose below 3.0 mmol/L causes confusion; below 2.0, seizure and coma. The cause is usually diabetic medication (insulin, sulfonylurea), and the treatment is intravenous dextrose (50 mL of 50 per cent) with the thiamine caveat above. The sulfonylurea-induced hypoglycaemia is prolonged (the insulin secretion continues for hours); give dextrose and admit for ongoing monitoring and octreotide if refractory.
- Hyponatraemia — sodium below 125 mmol/L causes confusion; below 120, seizure and coma. The correction must be controlled — no more than 8 to 10 mmol per litre in 24 hours — to prevent osmotic demyelination syndrome, the devastating and largely irreversible pontine injury first described by Sterns in 1986 [7].
- Hypercalcaemia — calcium above 3.0 mmol/L causes confusion, constipation, abdominal pain, and dehydration ("stones, bones, groans, and psychic moans"). The treatment is intravenous normal saline rehydration followed by a bisphosphonate (zoledronic acid 4 mg intravenously).
- Uraemia — a rising creatinine with uraemic encephalopathy; the treatment is renal replacement therapy if severe.
- Hepatic encephalopathy — the cirrhotic patient with new confusion has hepatic encephalopathy until proven otherwise, but the diagnosis is one of exclusion — exclude the other causes (infection, bleed, electrolyte disturbance, drug effect) first. The West Haven criteria grade the severity from minimal (grade 0 to 1) through asterixis (grade 2) to coma (grade 4), and the treatment is lactulose (30 mL orally, titrated to two to three soft stools daily) with rifaximin as a second-line agent [3]. The precipitants must be sought and corrected: infection, gastrointestinal bleed, constipation, electrolyte disturbance, sedatives, and dietary protein excess.
- Thyroid disease — both hypothyroidism (myxoedema madness, an insidious cognitive decline) and thyrotoxicosis (agitation, confusion, thyroid storm) can present as altered mental status. Check the TSH in every confused patient.
- Acid-base disturbance — a metabolic or respiratory acidosis causes confusion through the effect on cerebral function. The blood gas catches it.
- Hypoxia and hypercapnia — see the Oxygen category below.
T — Trauma
The trauma category is dominated by subdural haematoma, the diagnosis most likely to be missed in the elderly. The mechanism: the atrophic brain of the older patient stretches the bridging veins that traverse the subdural space, and a minor fall — often unwitnessed, often forgotten — tears one. The blood accumulates slowly, over days to weeks, and the clinical picture is a gradual cognitive decline, a fluctuating confusion, a headache, or a focal deficit. The risk factors are age, anticoagulation (warfarin or a DOAC), antiplatelet therapy, alcohol use disorder (repeated falls and coagulopathy), and the dementia patient who cannot give a reliable history. The CT head is indicated in any elderly patient with new or worsening confusion, especially on anticoagulation — and the subdural that is found may be chronic (hypodense, well-organised), acute (hyperdense), or mixed-density (acute-on-chronic), and the management ranges from observation and coagulation reversal to burr-hole evacuation. [1]
Traumatic brain injury (TBI) itself causes confusion — the concussed patient with a transient loss of consciousness and post-traumatic amnesia — and the workup includes the CT head if there are red flags (loss of consciousness more than 5 minutes, persistent confusion, vomiting, seizure, focal neurology, suspected skull fracture, or the patient is on anticoagulation). The diffuse axonal injury of severe TBI presents with immediate and prolonged coma. [1]
O — Oxygen (and carbon dioxide)
The brain requires a continuous supply of oxygenated, glucose-rich blood, and any failure of that supply produces confusion before it produces coma. The two categories: [1]
- Hypoxia — any cause of low oxygen saturation (pneumonia, pulmonary embolism, pulmonary oedema, COPD exacerbation, severe anaemia, carbon monoxide poisoning). The treatment is oxygen and the correction of the underlying cause. The pulse oximeter on the finger is the first measurement, and the blood gas (with the carboxyhaemoglobin level if carbon monoxide is suspected) is the confirmatory test.
- Hypercapnia (CO2 narcosis) — a rising CO2 causes confusion, drowsiness, asterixis (the metabolic flap), and ultimately coma. The classic setting is the COPD patient on excessive oxygen (the oxygen displaces CO2 from haemoglobin, worsens V/Q matching, and depresses the respiratory drive), but any cause of hypoventilation (opioid, neuromuscular weakness, obesity hypoventilation, the oversedated patient) produces it. The treatment is the reduction of the oxygen target to 88 to 92 per cent in the known CO2 retainer, and ventilatory support (non-invasive ventilation — BiPAP — or intubation) if the hypercapnia is severe. [1]
The blood gas is the investigation that catches both — and in the confused patient, the venous blood gas (with the lactate and the electrolytes) is one of the highest-yield single tests in the entire workup. [1]
P — Psychiatric
Primary psychiatric disorders — depression (including the pseudodementia of late-life depression), psychotic disorders (schizophrenia, brief psychotic disorder), and manic episodes (bipolar disorder) — can present with acute confusion, but they are diagnoses of exclusion and they are rare as first presentations in older adults. The cardinal rule, restated: a first episode of acute psychosis or mania in a patient over 40 has a medical cause until proven otherwise. The workup — glucose, electrolytes, infection screen, toxicology, thyroid function, neuroimaging — must be completed before the psychiatric diagnosis is entertained. The history is the key: a documented prior psychiatric history, a clear psychiatric syndrome (not just confusion), and the absence of any medical precipitant together support the psychiatric diagnosis. The danger is the premature psychiatric label that delays the treatment of a reversible medical cause. [1]
V — Vascular (the seventh category)
Stroke and transient ischaemic attack can present with confusion — especially the right hemisphere stroke (the right parietal neglect, the contralateral hemianopia that the patient does not recognise, the agitated delirium of the acute right middle cerebral artery territory infarct) and the posterior circulation stroke (the confusional state of a bilateral thalamic or mesial temporal infarct, the Top of the Basilar syndrome). The vertebrobasilar territory stroke may present with sudden-onset confusion, vertigo, diplopia, ataxia, and bilateral visual disturbance — and the CT may be normal in the early hours, requiring an MRI. The FAST test (Face, Arm, Speech, Time) screens for the anterior circulation stroke but does not capture the posterior circulation or the right hemisphere confusional presentation; the high index of suspicion and the imaging are the answer. [1]
The collateral history — five questions
The collateral history is the cornerstone of the confused-patient workup, and it is obtained from the family, the nursing staff, the general practitioner, the medication list, and the old medical record — because the confused patient cannot give a reliable history of their own confusion. The five questions: [1]
-
What is the baseline cognition? Is the patient normally fully independent and cognitively intact, or do they have a known dementia, mild cognitive impairment, or a prior delirium? The baseline determines whether this is an acute change from a normal baseline (delirium in a previously well patient — the workup is for a single acute precipitant) or an acute deterioration from a chronically impaired baseline (delirium superimposed on dementia — the workup is the same, but the predisposing vulnerability is the dementia). [1]
-
When did the change start, and was it sudden or gradual? The sudden onset (over hours) suggests an acute vascular event (stroke), a metabolic derangement (hypoglycaemia, hypercapnia), or a drug effect. The onset over days suggests an infection, an electrolyte disturbance, or a slowly accumulating subdural. The gradual onset over weeks to months raises the possibility of a chronic process — a dementia, a brain tumour, a chronic subdural, a metabolic disorder (hypercalcaemia, thyroid disease, B12 deficiency). [1]
-
Has the confusion fluctuated? Fluctuation — lucid intervals interspersed with confused periods — is the hallmark of delirium and is one of the four CAM features. It also raises the possibility of a subdural (the fluctuating cognitive state of the chronic subdural) and of non-convulsive status epilepticus (the fluctuating confusion of intermittent electrographic seizures). [1]
-
What are the medications, the alcohol, and the recreational drugs? Every drug on the chart, every over-the-counter medication, every recent change, every dose alteration. The alcohol history is critical — the amount, the frequency, the last drink (for withdrawal risk), and the nutritional status (for Wernicke risk). The recreational drug history (cannabis, opioids, stimulants, benzodiazepines) is taken non-judgmentally and is essential for the toxicology differential. [1]
-
What intercurrent illness or event has occurred? A recent fall (subdural), a recent surgery (postoperative delirium), a recent infection (sepsis-associated encephalopathy), a recent medication change (drug-induced delirium), a recent urinary symptom or constipation (the common precipitants in the elderly), a recent bereavement or relocation (the psychosocial precipitants). The intercurrent event is often the precipitant that interacts with the predisposing vulnerability to produce the delirium. [1]
DCE high-yield: The examiner will test your collateral-history skill by asking, "What are the five questions you ask the family of a newly confused elderly patient?" The answer is the five questions above, and the registrar who can deliver them fluently has demonstrated the clinical maturity that the DCE rewards. The corollary question is, "How do you establish the baseline cognition if the family is not available?" The answer is the old medical record, the GP, the residential aged-care facility notes, and — if all else fails — the assumption that the change is acute until proven otherwise, with the workup proceeding accordingly. [1]
The focused examination

The examination of the confused patient extends from the neurological system through every other system, because the cause is usually systemic. [1]
The neurological examination
The structured neurological examination in the confused patient: [1]
- Conscious level. The GCS (eye 1 to 4, verbal 1 to 5, motor 1 to 6, total 3 to 15) or the AVPU (Alert, Voice, Pain, Unresponsive). Record it and track the trend — a falling GCS is an emergency regardless of the cause.
- Pupils. Size, symmetry, reactivity. Pinpoint (less than 2 mm) suggests opioids or a pontine lesion. Dilated (more than 5 mm) suggests anticholinergics, tricyclic antidepressants, or sympathetic surge. A unilateral fixed and dilated pupil is uncal herniation (the third nerve compressed against the tentorial edge by a expanding mass) until proven otherwise. Symmetric midposition (3 to 5 mm) and unreactive pupils suggest a midbrain or severe metabolic depression.
- Cranial nerves. Eye movements (the ophthalmoplegia of Wernicke — a lateral rectus palsy, a horizontal gaze palsy, or a vertical gaze palsy; the internuclear ophthalmoplegia of a brainstem stroke); facial symmetry (the upper motor neuron pattern of a stroke); fundoscopy (papilloedema for raised intracranial pressure, subhyaloid haemorrhage for a subarachnoid haemorrhage).
- Motor. Tone (the rigidity of serotonin syndrome or neuroleptic malignant syndrome; the hypotonia of a cerebellar lesion or a diffuse metabolic encephalopathy), power (an asymmetry suggests a focal lesion), and the reflexes (hyperreflexia in an upper motor neuron lesion, hyporeflexia in a peripheral or acute spinal cord lesion; the plantar response — upgoing suggests a corticospinal tract lesion).
- Coordination and gait. The ataxia of Wernicke, cerebellar stroke, or acute alcohol intoxication. Test finger-to-nose and heel-to-shin if the patient can cooperate; test the gait if it is safe to do so (the ataxic gait is a high-yield finding in the Wernicke patient and in the cerebellar stroke).
- Meningeal signs. Neck stiffness (passive flexion of the neck meets resistance), Kernig sign (resistance to extension of the knee from a flexed hip), and Brudzinski sign (flexion of the neck causes flexion of the hips). These suggest meningeal irritation — bacterial meningitis, subarachnoid haemorrhage, or meningoencephalitis. The limitation: the signs may be absent in the deeply comatose patient and in the elderly patient with early meningitis, and their absence does not exclude meningitis. [1]
The general examination
- Temperature. Fever suggests infection; hyperthermia suggests sepsis, serotonin syndrome, neuroleptic malignant syndrome, heat stroke, or anticholinergic toxicity. Hypothermia suggests sepsis (especially in the elderly), hypothyroidism, hypoglycaemia, or environmental exposure.
- The skin. Rashes (the petechial rash of meningococcal septicaemia; the purpura of a coagulopathy; the livedo of a vasculitis), bruises (the pattern of a fall, the distribution of anticoagulant-related bleeding), pressure areas, line sites, surgical wounds, and the diabetic foot.
- The abdomen. Distension (urinary retention, constipation, ascites), tenderness (peritonitis, biliary sepsis, diverticulitis), rigidity, and the palpable bladder or the palpable mass.
- The chest and heart. The crackles of pneumonia or pulmonary oedema; the murmurs of endocarditis; the irregular pulse of atrial fibrillation.
- The specific signs. Asterixis (the metabolic flap — extend the wrists and watch for a rapid flexion-extension movement; it is the hallmark of metabolic encephalopathy, especially hepatic and uraemic); the tremor of alcohol withdrawal (coarse, 6 to 8 Hz, present at rest and worse with posture); the rigidity and hyperreflexia of serotonin syndrome; the lead-pipe rigidity of neuroleptic malignant syndrome. [1]
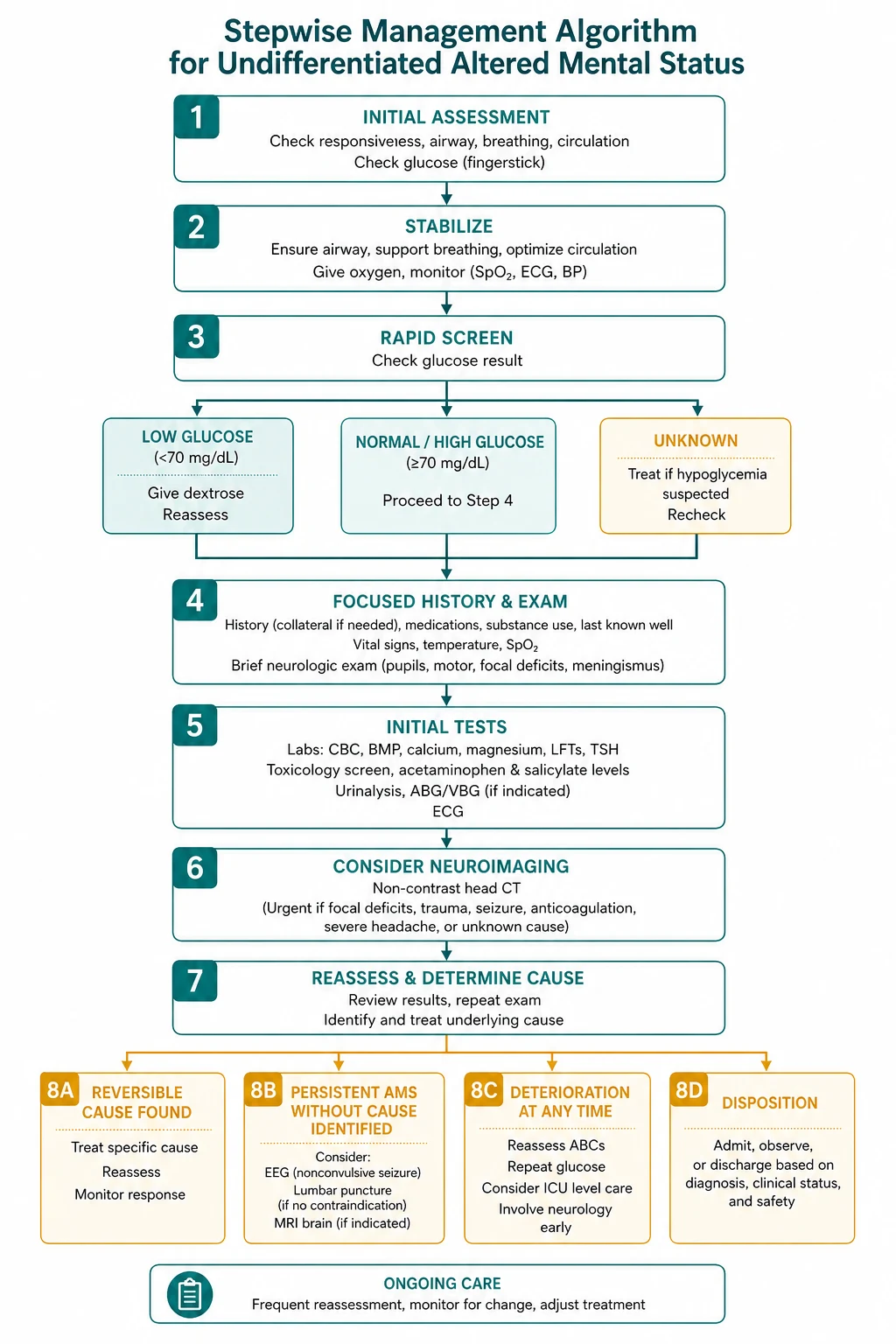
The investigation ladder
The investigation strategy for the confused patient is tiered — start with the bedside panel, add the laboratory panel, and reserve the imaging and the special tests for the clinical indications. The principle is not to over-investigate (the blanket CT for every confused patient is low-yield and expensive) and not to under-investigate (the glucose, the gas, the electrolytes, and the infection screen are non-negotiable). [1]
Tier one — the bedside panel (within minutes)
| Investigation | What it catches |
|---|---|
| Finger-prick glucose | Hypoglycaemia or hyperglycaemia — the single most important test |
| Vital signs (RR, SpO2, HR, BP, temperature) | Hypoxia, shock, sepsis, hyperthermia or hypothermia |
| 12-lead ECG | Silent myocardial infarction, arrhythmia, hyperkalaemia |
| Venous blood gas with lactate | Acid-base status, CO2 retention, lactate (sepsis), electrolytes |
Tier two — the laboratory panel (within hours)
| Investigation | What it catches |
|---|---|
| Full blood count | Anaemia, leukocytosis (infection), thrombocytopenia |
| Urea and electrolytes (including sodium, potassium, creatinine) | Hyponatraemia, hyper/hypokalaemia, uraemia, dehydration |
| Liver function tests and coagulation | Hepatic encephalopathy, synthetic liver failure |
| Calcium (corrected for albumin) and magnesium | Hypercalcaemia, hypocalcaemia, hypomagnesaemia |
| Thyroid-stimulating hormone (TSH) | Hypothyroidism, thyrotoxicosis |
| C-reactive protein | Infection, inflammation |
| Blood cultures (two sets, before antibiotic) | Bacteraemia, source of sepsis |
| Urine MC&S | Urinary tract infection |
| Troponin | Acute coronary syndrome (a common precipitant in the elderly) |
| Chest X-ray | Pneumonia, pulmonary oedema, pneumothorax |
| Drug levels where indicated | Lithium, digoxin, valproate, phenytoin; alcohol level; paracetamol and salicylate in the overdose context; urine drug screen |
Tier three — selective imaging and special tests (guided by the clinical picture)
| Investigation | Indication |
|---|---|
| CT head (non-contrast) | Focal neurology, head trauma, anticoagulation, deep or fluctuating coma, progressive deterioration, seizures, suspected raised intracranial pressure; also the prerequisite before lumbar puncture in most patients |
| Lumbar puncture (after CT) | Suspected meningitis or encephalitis — send CSF for cell count, protein, glucose (with a paired serum glucose), Gram stain and culture, viral PCR (especially herpes simplex), and consider cytology and specialized tests |
| MRI brain | Suspected posterior circulation stroke, herpes simplex encephalitis (temporal lobe signal change), Creutzfeldt-Jakob disease, or a structural lesion not seen on CT |
| EEG | Suspected non-convulsive status epilepticus (the patient who fails to recover from a convulsive seizure, or the persistently confused patient with no identified metabolic or structural cause); also supports a diagnosis of metabolic encephalopathy (triphasic waves in hepatic encephalopathy) |
| Autoimmune and paraneoplastic antibodies | Suspected autoimmune encephalitis (especially NMDA receptor encephalitis in the young patient with a movement disorder and psychiatric features) — a specialised test for the atypical or non-resolving case |
The EEG deserves a specific note. Non-convulsive status epilepticus is an under-recognised cause of altered mental status, particularly in the ICU and the elderly, and it presents as a fluctuating or persistent confusion without overt convulsive activity. The diagnosis requires an EEG — and the threshold to request one should be low in the patient who fails to recover from a convulsive seizure (the post-ictal state that does not resolve), the patient with a known seizure disorder who is confused, and the patient with unexplained persistent confusion despite a negative metabolic and structural workup [5].
When to image — and when not to
The CT head is not a blanket reflex in every confused patient. It is indicated for: [1]
- Focal neurology on examination — an asymmetry of power, tone, reflexes, or the plantar response.
- Head trauma — any history of a fall or a head injury, especially in the elderly and the anticoagulated patient.
- Anticoagulation — warfarin, a DOAC, or antiplatelet therapy, because the threshold for an intracranial bleed is lower.
- Deep or fluctuating coma (GCS less than 12), progressive deterioration of the conscious level, or a failing GCS trend.
- Seizures — a first seizure or a new-onset status epilepticus.
- Suspected raised intracranial pressure — papilloedema, vomiting, headache, or a Cushing response (bradycardia with hypertension).
- Before a lumbar puncture — to exclude a mass lesion that could precipitate herniation. [1]
It is not indicated for the alert, non-focal, non-traumatised patient with a clear metabolic or infectious cause for their confusion — the metabolic derangement or the infection is the cause, and the CT adds nothing. The registrar who scans every confused patient has not understood the differential. [1]
The rapidly reversible causes — GHOST
Before the full workup is complete, and in parallel with it, the five rapidly reversible causes must be checked and treated. The GHOST acronym captures them: [1]
- G — Glucose. Hypoglycaemia. Check it, treat it, repeat it. The finger-prick glucose takes ten seconds.
- O — Oxygen. Hypoxia. Give it by mask or nasal speculum, and check the saturation and the blood gas.
- S — Sodium (and other electrolytes). Hyponatraemia, hyper/hypokalaemia, hypercalcaemia. Check the U&E and the calcium, and correct the derangement at the safe rate.
- T — Thiamine. Give it to every patient at risk of Wernicke — 500 mg intravenously in Australia, before or alongside the glucose. The classic triad (ataxia, ophthalmoplegia, confusion) is present in only about 10 per cent of cases; the absence of the triad does not exclude the diagnosis, and the consequences of omission are irreversible [4].
- H — Hypertension and hypotension. The hypertensive encephalopathy (a rapidly rising blood pressure with confusion, headache, and visual disturbance, often with posterior white matter changes on MRI — posterior reversible encephalopathy syndrome) and the hypotensive confusion (cerebral hypoperfusion from any cause of shock).
The GHOST approach is the registrar's bedside checklist — it takes five minutes, and it has saved more confused patients than any imaging study or specialist referral. [1]
Management — treat the cause, sedate last

The management of the undifferentiated altered mental status is the management of the underlying cause. This is the single most important principle, and it bears repeating: the confusion is a symptom, the cause is the disease, and the treatment of the confusion without the cause is the surest way to harm the patient. [1]
Treat the underlying cause
| Cause | Treatment |
|---|---|
| Hypoglycaemia | 50 mL of 50 per cent dextrose IV (with thiamine first if at risk); ongoing monitoring for sulfonylurea-induced recurrence |
| Sepsis | Sepsis Six — oxygen, cultures, antibiotic within one hour, fluid, lactate, urine output; source control |
| Hyponatraemia | Controlled correction — no faster than 8 to 10 mmol/L in 24 hours; hypertonic saline for severe symptomatic hyponatraemia (seizure, coma) |
| Hepatic encephalopathy | Lactulose (30 mL orally titrated to two to three soft stools daily); rifaximin second-line; correct the precipitant |
| Subdural haematoma | Neurosurgical consultation; coagulation reversal; burr-hole or craniotomy evacuation for the symptomatic acute or acute-on-chronic |
| Drug toxicity | Withdraw the offending drug; specific antidote (naloxone for opioid, flumazenil for benzodiazepine, physostigmine for anticholinergic, digoxin Fab for digoxin) |
| Alcohol withdrawal | Symptom-triggered long-acting benzodiazepine (diazepam 10 to 20 mg, guided by CIWA-Ar); thiamine 500 mg IV |
| Meningitis / encephalitis | Antibiotic within one hour (ceftriaxone 2 g IV plus vancomycin, plus ampicillin for the listeria risk in the elderly and immunocompromised); aciclovir 10 mg/kg IV three times daily for suspected HSV encephalitis; dexamethasone for suspected pneumococcal meningitis |
| Stroke | Thrombolysis or thrombectomy if within the window; stroke unit care |
| Non-convulsive status epilepticus | IV antiseizure medication (lorazepam 4 mg, or levetiracetam or fosphenytoin); continuous EEG; ICU for refractory cases |
Non-pharmacological measures
Every confused patient benefits from the non-pharmacological bundle, and it is the foundation of the management regardless of the cause: [1]
- Orientation cues — a clock, a calendar, a board with the date and the day of the week, the name of the hospital and the ward. Place them in the patient's line of sight.
- Sensory aids — glasses and hearing aids, cleaned, charged, and in use. Sensory deprivation is a powerful precipitant of delirium, and its correction is a powerful intervention.
- Sleep protection — minimise nighttime interruptions (cluster the observations and the medications, reduce the noise, manage the lighting). Sleep deprivation perpetuates delirium.
- Family presence — a familiar face, a familiar voice, and the reassurance of a known person. The family is part of the treatment, not a visitor.
- Minimise the line and catheter burden — remove the urinary catheter as soon as possible (it is a source of infection and a restraint), remove the peripheral cannula when it is no longer needed, and avoid physical restraints (they worsen agitation and increase the risk of injury).
- Communication — speak slowly, clearly, and calmly. Reorient the patient at every interaction. Explain every procedure before it is done. The confused patient is frightened, and the calm, consistent, reorienting clinician is a therapeutic intervention in their own right. [1]
Symptomatic sedation — haloperidol as the last resort
Pharmacological sedation is reserved for the agitation that endangers the patient or the delivery of essential care. It is not for the confusion itself, and it is not for the convenience of the staff. The agent of choice is haloperidol — a typical antipsychotic with a dopamine D2 antagonist action: [1]
- Dose: 0.5 to 1 mg intramuscularly or intravenously (0.25 mg in the elderly and the debilitated), repeated after 30 to 60 minutes and titrated to effect. The oral route (0.5 to 2 mg) is used for the less agitated patient who can swallow.
- Cautions: the QTc interval — haloperidol prolongs it and can precipitate torsades de pointes, especially in the patient with electrolyte disturbance or on other QT-prolonging drugs. Check the ECG and the potassium and magnesium before and during the treatment. Avoid haloperidol in Parkinson disease and Lewy body dementia (the dopamine blockade worsens the motor symptoms and can precipitate a severe neuroleptic sensitivity reaction). Avoid in the neuroleptic malignant syndrome and the serotonin syndrome — these are diagnoses where haloperidol is contraindicated, not indicated. [1]
Benzodiazepines are avoided in delirium — they worsen the confusion, prolong the duration, and cause respiratory depression — except in two specific situations: [1]
- Alcohol or benzodiazepine withdrawal — the only delirium where benzodiazepines are first-line. The long-acting diazepam (10 to 20 mg orally, or 5 to 10 mg intravenously), guided by the CIWA-Ar score, is the standard regimen. Lorazepam is preferred in the patient with liver failure (no active metabolites).
- Severe serotonin syndrome or catatonia — benzodiazepines are adjunctive, alongside the withdrawal of the serotonergic agent and, in the case of serotonin syndrome, the consideration of cyproheptadine. [1]
The evidence for the routine use of antipsychotics in delirium is nuanced. The MIND-USA trial (2018), a randomised placebo-controlled trial of low-dose haloperidol, ziprasidone, and placebo in ICU patients with delirium, found no difference in delirium duration or coma-free days between the groups — a result that has tempered the enthusiasm for routine antipsychotic use but has not displaced haloperidol from its role as the agent of choice for the acute severe agitation that has not responded to behavioural measures. [1]
Viva trap: "When would you give a benzodiazepine to a confused patient?" The answer is short and the examiner is testing the breadth of your knowledge: in alcohol or benzodiazepine withdrawal, and in severe serotonin syndrome or catatonia. In every other delirium, the benzodiazepine worsens the confusion, prolongs the course, and risks respiratory depression. The registrar who reaches for the midazolam for the agitated delirious elderly patient has made a serious error — the correct agent is haloperidol, at a low dose, titrated, with the ECG and the QTc monitored. The corollary question: "When would you not give haloperidol?" The answer is: in Parkinson disease, Lewy body dementia, neuroleptic malignant syndrome, serotonin syndrome, and the patient with a prolonged QTc. [1]
Special populations
The elderly patient
The elderly are the highest-risk group for acute confusion, and the predisposing factors are well described: age itself (the reduced cognitive reserve), baseline cognitive impairment, sensory deprivation, polypharmacy, multimorbidity, and the frailty that lowers the threshold for the decompensation. The precipitating factors in the elderly are the common events of hospital life — a urinary tract infection, a constipation, a new medication, a room change, a sleepless night, an urinary catheter, a physical restraint. The implication for prevention is the targeting of these factors, and the delirium prevention bundles (the HELP program, the NICE CG103 recommendations) have demonstrated a reduction in delirium incidence and duration through the systematic addressing of orientation, hydration, sleep, sensory aids, mobility, and medication review. [1]
The elderly patient with new confusion is the patient most likely to be mislabelled — as "just confused," as "dementia," as "a nursing home placement" — and the registrar's role is to reframe the confusion as a medical symptom with a medical cause, and to work the cause with the same rigour as for any younger patient. The elderly deserve the full workup, the full treatment, and the full reassessment — not the premature therapeutic nihilism that costs them their independence and their lives. [1]
The postoperative patient
Postoperative delirium is a specific entity — it complicates up to 50 per cent of major surgery in the elderly, and it is associated with prolonged hospital stay, increased mortality, and long-term cognitive decline. The precipitants are the surgical and anaesthetic insult itself, the pain, the opioid analgesia, the urinary retention, the constipation, the hypoxia, the blood loss, the electrolyte disturbance, and the sleep deprivation of the hospital environment. The differential also includes the surgical complication — the anastomotic leak, the intra-abdominal collection, the fat embolism after a long bone fracture, and the pulmonary embolism. The workup is the same DIMTOP approach, with a low threshold for the infection screen (the surgical site, the urine, the chest) and the imaging (the CT abdomen for the suspected collection, the CTPA for the suspected PE). [1]
The immunocompromised patient
The immunocompromised patient — the transplant recipient, the chemotherapy patient, the HIV patient with a low CD4 count, the patient on chronic immunosuppression — expands the differential of confusion to include the opportunistic CNS infections (cryptococcal meningitis, cerebral toxoplasmosis, CMV encephalitis, progressive multifocal leukoencephalopathy) and the immune-related conditions (the post-transplant lymphoproliferative disorder, the immune reconstitution inflammatory syndrome, the posterior reversible encephalopathy syndrome from calcineurin inhibitors). The threshold for the CT head, the lumbar puncture, and the MRI is lower, and the microbiological and virological workup is broader. The patient on a checkpoint inhibitor (pembrolizumab, nivolumab, ipilimumab) adds the immune-related adverse events to the differential — the autoimmune encephalitis, the hypophysitis, the aseptic meningitis — and the management is the withdrawal of the agent and the high-dose corticosteroid. [1]
DCE long-case approach
Patient scenario
Mr Robert Chen, 82, retired engineer, is brought to the emergency department by his daughter, who found him confused and dishevelled at his home this morning. He was well and independent when she last visited four days ago. His background includes vascular dementia (mild, MMSE 24 six months ago), type 2 diabetes (on gliclazide and insulin), hypertension, atrial fibrillation (on apixaban), and chronic kidney disease stage 3 (baseline creatinine 150 micromol/L). He lives alone. [1]
On assessment: GCS 13 (E3 V4 M6), temperature 38.3, respiratory rate 22, SpO2 94 per cent on room air, heart rate 96 in atrial fibrillation, blood pressure 104/64, capillary refill 3 seconds. He is disoriented in time and place, inattentive (cannot do the months of the year backwards), and intermittently drowsy. Pupils are equal and reactive, no focal neurology, no neck stiffness, no asterixis. Finger-prick glucose 6.2. Sodium 124, potassium 4.8, creatinine 195 (up from baseline 150), calcium 2.35, TSH 3.2, CRP 96, WCC 16.2. Chest X-ray shows right lower lobe consolidation. Urine dipstick is positive for nitrites and leucocytes. CT head shows mild cerebral atrophy and a small chronic subdural haematoma on the left (hypodense, no mass effect). [1]
Candidate's opening statement (SASPOP)
"Mr Robert Chen is an 82-year-old retired engineer who has presented with an acute confusional state over the last four days, on a background of mild vascular dementia, type 2 diabetes on gliclazide and insulin, atrial fibrillation on apixaban, hypertension, and chronic kidney disease stage 3. He was previously independent. His main problems are delirium, most likely multifactorial — sepsis from a community-acquired pneumonia and a urinary tract infection, a severe hyponatraemia at 124, an acute kidney injury with the creatinine risen from 150 to 195, and a chronic subdural haematoma found on the CT head — in a patient on apixaban. My immediate priorities are the ABCDE assessment with the GHOST reversible causes checked, the intravenous antibiotic for the pneumonia and the UTI, the controlled correction of the hyponatraemia, the withholding of the nephrotoxic and harmful drugs (the gliclazide for the hypoglycaemia risk, the apixaban for the subdural, and the review of the antihypertensives), the reassessment of the subdural with the neurosurgical team, and the non-pharmacological delirium bundle alongside the medical management." [1]
Problem list
- Delirium — multifactorial, CAM-positive, secondary to the sepsis, the hyponatraemia, and the subdural, superimposed on the vascular dementia.
- Sepsis — community-acquired pneumonia and urinary tract infection; CRP 96, WCC 16.2, fever 38.3.
- Severe hyponatraemia — sodium 124, requiring controlled correction (no more than 8 to 10 mmol in 24 hours) to prevent osmotic demyelination. [1]4. Acute kidney injury — creatinine risen from 150 to 195, likely multifactorial (pre-renal from sepsis and dehydration, possibly nephrotoxic from the medications).
- Chronic subdural haematoma — found on the CT, on apixaban; requires coagulation reversal, neurosurgical consultation, and serial imaging.
- Drug review — gliclazide (hypoglycaemia risk in the AKI), apixaban (subdural bleeding risk), antihypertensives (hypotension risk).
- Baseline cognitive impairment — vascular dementia, MMSE 24; the delirium is superimposed, and the cognitive recovery may be incomplete. [1]
Integrated management plan
- ABCDE resuscitation and the GHOST check. Glucose 6.2 (normal — no hypoglycaemia). Oxygen — he is 94 per cent on room air, give 2 L via nasal speculum to target 94 to 98 per cent. Sodium 124 — controlled correction with normal saline and fluid restriction; check the sodium every 4 to 6 hours; no hypertonic saline unless he seizes. Thiamine — give 500 mg IV empirically (he is elderly, possibly nutritionally depleted, and the downside is negligible).
- Sepsis management. Blood cultures, urine MC&S (already dipped), commence intravenous antibiotics — ceftriaxone 1 g IV daily (dose-adjusted for the AKI) plus azithromycin for the pneumonia, guided by the local guideline and the culture results. Intravenous fluids (cautiously, given the hyponatraemia and the AKI — 1 L of normal saline over 4 to 6 hours, reassess). Paracetamol for the fever. Lactate checked (send it with the initial bloods).
- Hyponatraemia correction. The sodium of 124 is severe and is contributing to the confusion. The correction must be controlled — no more than 8 to 10 mmol in 24 hours. The approach is the treatment of the underlying cause (the sepsis, the dehydration, the resolution of the SIADH-like state that may accompany the pneumonia) and the cautious normal saline. I do not give hypertonic saline unless he seizes or his conscious level falls precipitously, and I check the sodium frequently. I am aware of the risk of osmotic demyelination and the risk factors (alcohol use, malnutrition, hypokalaemia, severe hyponatraemia) [7].
- The subdural haematoma. The CT shows a small chronic subdural on the left, hypodense, no mass effect. In a patient on apixaban, the risk is that a trivial further bleeding event will expand it. My management is to reverse the apixaban (discuss with haematology — andexanet alfa or prothrombin complex concentrate, depending on the local protocol and the severity), to consult the neurosurgical team for their opinion (a small chronic subdural with no mass effect may be managed conservatively with serial imaging, but the decision is the neurosurgeon's), and to monitor the GCS hourly. If the GCS falls or a new focal deficit emerges, I repeat the CT urgently and escalate.
- Drug review. Withhold the gliclazide (hypoglycaemia risk in the AKI — the sulfonylurea persists for hours and the renal clearance is reduced; manage the glucose with a sliding-scale insulin infusion). Withhold the apixaban (the subdural, the AKI, the fall risk). Withhold the antihypertensives (the blood pressure is already low at 104/64). Continue the insulin (adjusted for the AKI). Review every drug for the dose adjustment the renal failure requires.
- Non-pharmacological delirium bundle. Orientation cues, glasses and hearing aids, family presence (the daughter is here), sleep protection, early mobilisation, minimisation of lines and catheters (remove the urinary catheter as soon as possible), and consistent communication and reorientation.
- Symptomatic management. He is not severely agitated at present; the non-pharmacological measures and the treatment of the underlying causes are the primary management. If the agitation endangers him or the care, low-dose haloperidol (0.25 mg orally or intramuscularly) is the agent of choice, with the ECG and the QTc checked. [1]
Examiner probing questions
"How do you correct the hyponatraemia, and what is the danger?" → "The sodium of 124 is severe and is contributing to the confusion and the drowsiness. The correction is controlled — no more than 8 to 10 mmol per litre in 24 hours — because over-rapid correction risks osmotic demyelination syndrome, the devastating pontine injury first described by Sterns in 1986 [7]. The approach is the treatment of the underlying cause — the sepsis, the dehydration — with cautious normal saline and the serial monitoring of the sodium every 4 to 6 hours. I do not use hypertonic saline unless he seizes or his conscious level falls precipitously, because the risk of overcorrection is highest in the patient who is rapidly fluid-resuscitated and whose sodium rises faster than the 24-hour limit."
"What is the significance of the chronic subdural, and what do you do about it?" → "The chronic subdural is a known complication of the atrophic elderly brain on anticoagulation, and it may be contributing to the confusion, though the sepsis and the hyponatraemia are more likely the primary drivers. The management is the reversal of the apixaban (discuss with haematology), the neurosurgical consultation, and the serial imaging and the hourly GCS monitoring. A small chronic subdural with no mass effect is often managed conservatively, but the patient on anticoagulation is at risk of expansion, and the threshold for the surgical evacuation is lower if the GCS falls or a focal deficit emerges." [1]
DCE short-case discussion — the cognitive assessment
Instruction: "Examine this patient's cognitive function and present your findings." [1]
The systematic cognitive assessment routine
- Establish the baseline. Before testing, ensure the patient has their glasses and hearing aids, is comfortable, is not in pain, and is orientated to the examination. Explain what you are doing and why.
- Orientation. Time (day, date, month, year, season), place (building, floor, city), and person (name, date of birth). Disorientation in time is the earliest and most sensitive marker of delirium.
- Attention. The months of the year backwards (December, November, October...) or the serial sevens (100 minus 7, minus 7...). Inattention is the hallmark of delirium and is the second CAM feature. The patient with dementia but no superimposed delirium can usually attend.
- Registration and recall. Name three objects (apple, table, penny), ask the patient to repeat them, and ask for them again after 5 minutes. This tests new learning and short-term memory.
- Language. Naming objects (a watch, a pen), following a three-step command ("take this paper in your right hand, fold it in half, and put it on the floor"), writing a sentence, and reading and obeying a command ("close your eyes").
- Visuospatial function. Copy a intersecting pentagons or a clock face (draw the numbers and set the hands at 11:10). The clock-drawing test is a sensitive screen for executive and visuospatial dysfunction.
- Apply the CAM. Feature 1 (acute onset and fluctuating course — from the collateral history), Feature 2 (inattention — from the attention testing), Feature 3 (disorganised thinking — from the conversation), Feature 4 (altered level of consciousness — from the AVPU/GCS). Delirium requires Features 1 and 2 plus either 3 or 4 [1].
Presentation template
"I have assessed Mr Chen's cognitive function. He is disoriented in time (he thinks it is March, it is July) and in place (he cannot name the hospital). He is inattentive — he cannot recite the months of the year backwards beyond September. He registered all three objects but recalled none at five minutes. His language is intact for naming and comprehension, but his writing is illogical. He copied the pentagons with errors. His CAM is positive — he has the acute onset and fluctuating course (from the daughter's history), the inattention (from the attention testing), the disorganised thinking (from the conversation), and a drowsy level of consciousness (GCS 13). He has delirium, superimposed on his known vascular dementia. The delirium is multifactorial — the sepsis, the hyponatraemia, and the chronic subdural are all contributing." [1]
Discussion questions
Examiner: "How do you distinguish the delirium from the underlying dementia?" → "I cannot, fully, at the bedside in the acute presentation — the two overlap, and the delirium is the foreground. What I can do is establish the baseline from the collateral history (the daughter's account of his function four days ago, the MMSE of 24 from six months ago), diagnose the acute change as a delirium by the CAM, and commit to the workup and the treatment of the precipitants. The delirium will resolve as the precipitants are treated, and the residual cognitive impairment at that point will be the underlying dementia. The teaching point is that I never attribute the acute confusion to the dementia without first diagnosing and treating the delirium — the dementia is the predisposing factor, not the explanation for the acute change." [1]
Examiner: "What is the prognosis of delirium in the elderly?" → "The prognosis is nuanced. The acute episode usually resolves over days to weeks if the precipitants are treated, but the full cognitive recovery may take months, and a proportion of elderly patients do not return to their baseline — the delirium has unmasked or accelerated an underlying neurodegenerative process. Delirium in the elderly is associated with prolonged hospital stay, increased institutionalisation, increased mortality, and an increased risk of subsequent dementia. The implication is that prevention is paramount — the delirium prevention bundles target the modifiable risk factors (orientation, hydration, sleep, sensory aids, mobility, medication review) and have demonstrated a reduction in incidence and duration. The registrar's role is not just to treat the delirium that has occurred but to prevent the delirium that has not yet occurred, in every elderly patient on every ward." [1]
Key DWE MCQ patterns
- The finger-prick glucose is the first bedside test in any patient with an altered conscious level. The stem will describe a confused or drowsy patient on a sulfonylurea or insulin; the answer is the bedside glucose, not the CT or the blood gas.
- The thiamine-before-glucose rule. The stem will describe a malnourished or alcoholic patient who is hypoglycaemic; the answer is to give thiamine alongside or before the dextrose, not the dextrose alone.
- The CAM diagnostic algorithm — Features 1 (acute onset and fluctuation) and 2 (inattention) plus either 3 (disorganised thinking) or 4 (altered level of consciousness). The stem will describe a patient and ask which feature is required; the answer is the combination.
- The CT head indications — focal neurology, trauma, anticoagulation, deteriorating GCS, seizures, raised ICP, before LP. The stem will describe a patient and ask whether the CT is indicated; the answer is the indication, not the blanket reflex.
- The hyponatraemia correction rate — no more than 8 to 10 mmol in 24 hours. The stem will describe a confused patient with a sodium of 118 and ask for the management; the answer is the controlled correction, not the rapid normalisation. [1]6. The benzodiazepine exception — alcohol or benzodiazepine withdrawal is the only delirium where benzodiazepines are first-line. The stem will describe an agitated confused patient and ask for the agent; the answer is haloperidol, except in the withdrawal context.
- The antibiotic-first rule in suspected meningitis — the antibiotic is given within one hour, before the CT and the LP. The stem will describe a patient with fever, headache, and confusion; the answer is the antibiotic now, not the imaging first.
- The subdural in the elderly on anticoagulation — the stem will describe a gradual cognitive decline in an elderly patient on warfarin or a DOAC; the answer is the CT head and the coagulation reversal. [1]
References
[1] Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113(12):941–8. The foundational paper that defined the CAM diagnostic algorithm and validated it with a sensitivity of 94 to 100 per cent and a specificity of 90 to 95 per cent against psychiatrist assessment — the most widely used delirium screening instrument in the world.
[2] Inouye SK. Delirium in older persons. N Engl J Med 2006;354(11):1157–65. The seminal review establishing the multifactorial model of delirium — the interaction between a vulnerable patient (predisposing factors) and an acute insult (precipitating factors) — and the implication that the management must address all the contributing factors, not just one. The basis of the delirium prevention bundles.
[3] Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the AASLD and the EASL. Hepatology 2014;60(2):715–35. The joint American and European guideline on the classification (West Haven criteria), the diagnosis (clinical, by exclusion), and the management (lactulose first-line, rifaximin second-line, and the correction of the precipitants) of hepatic encephalopathy.
[4] Isenberg-Grzeda E, Kutner HE, Nicolson SE. Wernicke-Korsakoff-syndrome: under-recognized and under-treated. Psychosomatics 2012;53(6):507–16. The review that highlights the under-recognition of Wernicke encephalopathy — the classic triad is present in only a minority, the condition occurs in non-alcoholic as well as alcoholic patients, and the empirical thiamine treatment carries negligible risk and prevents the irreversible Korsakoff syndrome.
[5] Rohr J, Chong DH, Gopalji R, Hamalian K, Derhammer BS, Wheeler K. Nonconvulsive status epilepticus: a review for emergency clinicians. Emerg Med Pract 2023. The practical review of the clinical presentation (altered mental status without overt convulsions), the diagnostic framework (the Salzburg consensus EEG criteria), and the management (intravenous antiseizure medication) of non-convulsive status epilepticus — an under-recognised cause of persistent confusion.
[6] Muzio BD, Peterson CD, Whitmill RA, et al. Sepsis-associated delirium: a narrative review. Cureus 2023. The review of the pathophysiology (neuroinflammation, blood-brain barrier dysfunction, neurotransmitter imbalance), the clinical presentation (the brain's response to the systemic inflammation), and the management (treat the sepsis) of sepsis-associated encephalopathy — the commonest cause of confusion in the septic patient.
[7] Sterns RH, Riggs JE, Schochet SS Jr. Osmotic demyelination syndrome following correction of hyponatremia. N Engl J Med 1986;314(24):1535–42. The landmark paper that established the link between the rapid correction of chronic hyponatraemia and the development of central pontine myelinolysis — the empirical basis for the modern correction-rate limits (no more than 8 to 10 mmol per litre in 24 hours) that prevent this devastating and largely irreversible complication.
Inouye et al., Ann Intern Med 1990; Inouye, N Engl J Med 2006; Vilstrup et al., Hepatology 2014; Isenberg-Grzeda et al., Psychosomatics 2012; Rohr et al., Emerg Med Pract 2023; Muzio et al., Cureus 2023; Sterns et al., N Engl J Med 1986; NICE CG103 Delirium; Australian Commission on Safety and Quality in Health Care Standard 9; RCP delirium care bundle; American Psychiatric Association Practice Guideline for the Treatment of Patients with Delirium. [1]
References
- [1]Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI Clarifying confusion: the confusion assessment method. A new method for detection of delirium Ann Intern Med, 1990.PMID 2240918
- [2]Inouye SK Delirium in older persons N Engl J Med, 2006.PMID 16540616
- [3]Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver Hepatology, 2014.PMID 25042402
- [4]Isenberg-Grzeda E, Kutner HE, Nicolson SE Wernicke-Korsakoff-syndrome: under-recognized and under-treated Psychosomatics, 2012.PMID 23157990
- [5]Rohr J, Chong DH, Gopalji R, Hamalian K, Derhammer BS, Wheeler K Nonconvulsive Status Epilepticus: A Review for Emergency Clinicians J Emerg Med, 2023.PMID 37661524
- [6]Heming N, Mazeraud A, Verdonk F, et al. Neuroanatomy of sepsis-associated encephalopathy Crit Care, 2017.PMID 28320461
- [7]Sterns RH, Riggs JE, Schochet SS Jr Osmotic demyelination syndrome following correction of hyponatremia N Engl J Med, 1986.PMID 3713747