Phys · general-medicine
Undifferentiated Back Pain — A Systematic Diagnostic Approach
Also known as back pain · low back pain · lumbar pain · lumbago · non-specific back pain · mechanical back pain · undifferentiated back pain · diagnostic approach to back pain · red flag back pain · cauda equina syndrome · sciatica · radicular pain · neurogenic claudication · spinal stenosis · inflammatory back pain · ankylosing spondylitis · axial spondyloarthritis · vertebral osteomyelitis · discitis · spinal epidural abscess · osteoporotic vertebral fracture
Consultant-physician-depth guide to the systematic approach to back pain in the physician setting. Covers the triage framework (non-specific mechanical, radicular, or red-flag serious pathology); the complete differential — mechanical (musculoskeletal, disc herniation, facet joint, spinal stenosis), inflammatory (axial spondyloarthritis — ankylosing spondylitis, psoriatic and enteropathic spondylitis), infective (vertebral osteomyelitis, epidural abscess, discitis), malignant (bone metastases — breast, lung, prostate, kidney, thyroid; myeloma; primary bone tumour), metabolic (osteoporotic vertebral fracture) and referred (pancreatic cancer, AAA, renal, pelvic); the NICE NG59 red flags and cauda equina syndrome; the focused history and the systematic spine and lower-limb neurological examination (straight leg raise, femoral stretch test, per rectal); the targeted investigations (most mechanical pain needs no imaging; FBC, CRP, ESR, PSA, calcium, ALP, electrophoresis, Bence-Jones when red flags; X-ray, MRI, CT); and the management of mechanical back pain (analgesia, stay active, physiotherapy, CBT, multidisciplinary pain programme). Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Back Pain — A Systematic Diagnostic Approach

The answer first
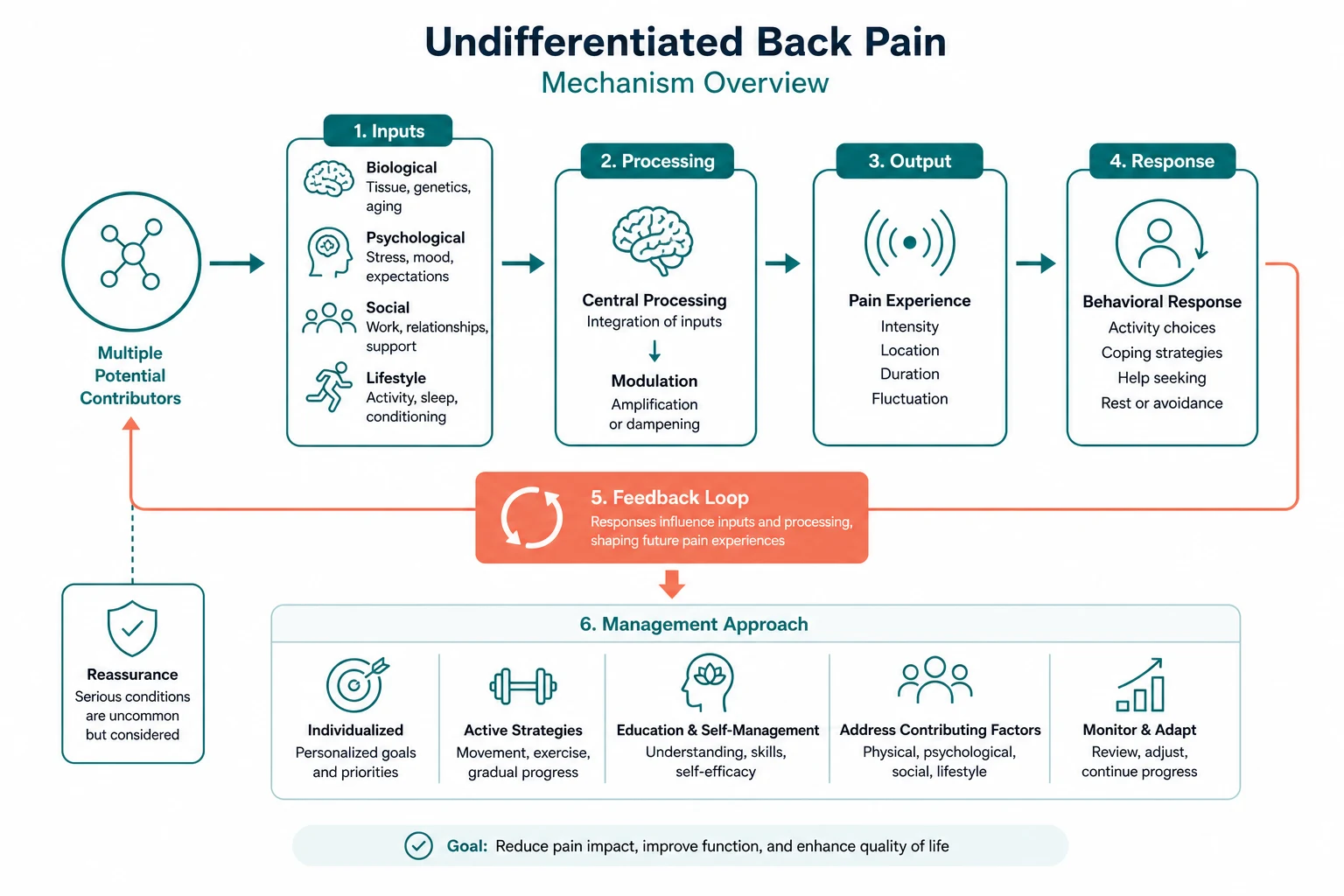
Back pain is one of the commonest presentations in general medicine — the lifetime prevalence is over 80 per cent, and it is the leading global cause of years lived with disability. The registrar's task is not to "diagnose" the back pain in most patients — it is to triage the patient. The triage sorts every back pain patient into one of three bins, and each bin has a different management logic: [1]
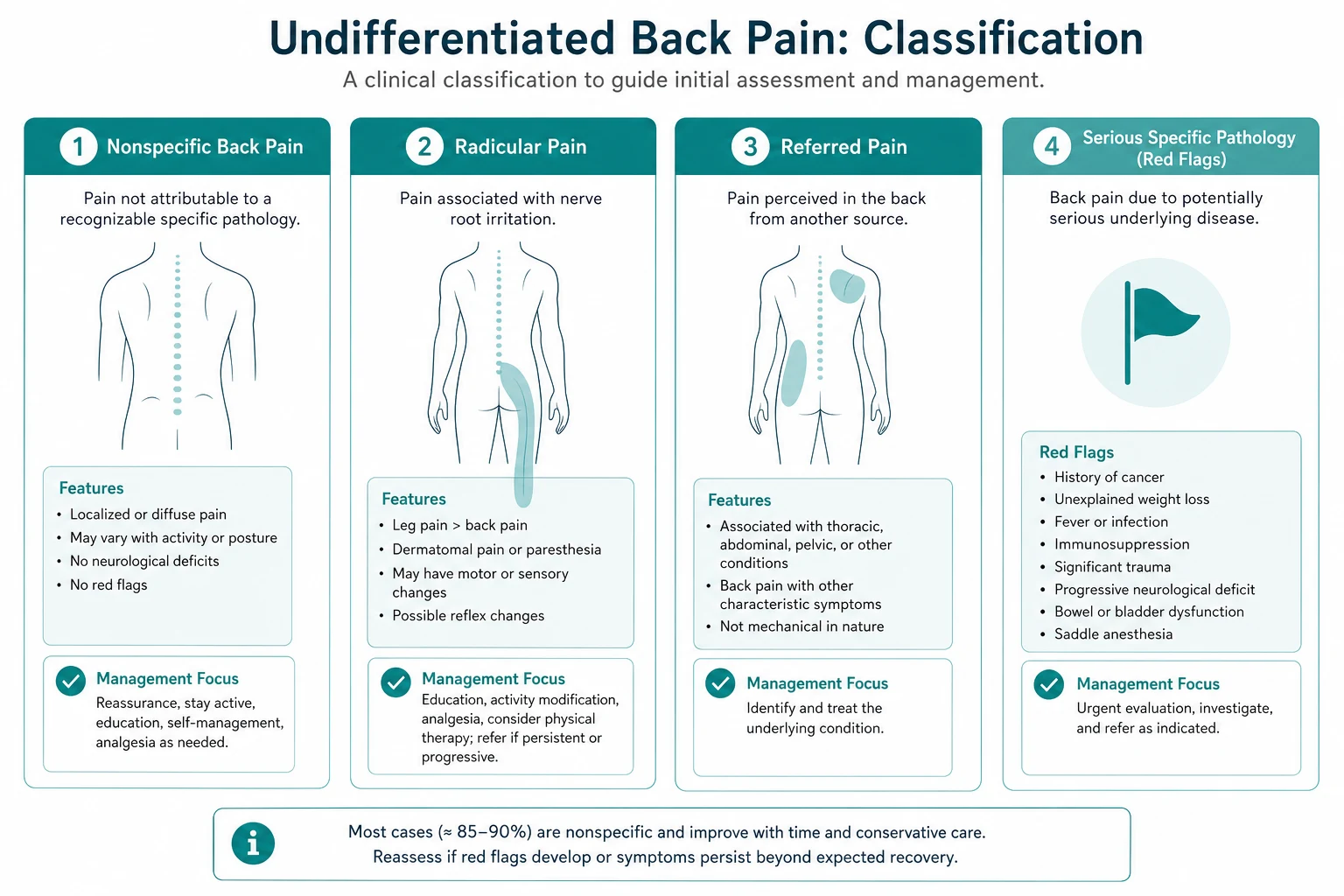
- Non-specific (mechanical) back pain — about 90 per cent of cases. The pain is reproduced by mechanical load and relieved by rest. There are no red flags, no neurological deficit, and no systemic symptoms. Management is reassurance, education, staying active and simple analgesia. No imaging is needed.
- Radicular (nerve root) pain — back pain radiating below the knee in a dermatomal distribution, with or without a neurological deficit. The common cause is a lumbar disc herniation compressing a nerve root. Most settle with conservative therapy; the minority need imaging and, rarely, surgery.
- Back pain with red flags — the minority that harbour serious pathology: fracture, infection, malignancy, inflammatory disease, or cord or cauda equina compromise. These need targeted investigation and urgent, cause-specific management. [1]
The reproducible sequence for any back pain patient is: [1]
- Screen for the emergency first — cauda equina syndrome, cord compression, a ruptured AAA. Ask about saddle anaesthesia, bladder and bowel function, and palpate the abdomen. These cannot wait.
- Take the red flag history — age, cancer, weight loss, night pain, fever, steroids, intravenous drug use, immunocompromise, trauma, a progressive neurological deficit.
- Triage — mechanical, radicular, or red-flag, by the history and the examination.
- Investigate the red flags only — most mechanical pain needs no imaging; the red flags drive the bloods and the MRI.
- Manage the cause — reassure and mobilise the mechanical patient; investigate and treat the serious pathology. [1]
The single most dangerous error is assuming the pain is mechanical without screening for the red flags. The cauda equina syndrome missed because the registrar did not ask about urinary function or perform a per rectal examination; the vertebral osteomyelitis called "muscular pain" in the intravenous drug user; the pancreatic cancer presenting as "upper back pain" for three months — these are the misses that define a poor physician. The second error is over-investigating the mechanical patient — the MRI that reveals an age-related disc bulge in an asymptomatic person, the cascade of referrals and injections and surgery that follows, none of which improves the outcome. [1]
Viva trap: "What is the first question you ask a patient with back pain?" The honest answer is "Tell me about your bladder and your bowels." The triage of back pain begins with the cauda equina screen, because cauda equina syndrome is the time-critical emergency that is missed if the registrar reaches for the musculoskeletal history first. The registrar who screens for cauda equina in the first minute of every back pain encounter has organised the entire assessment. [1]
Why the triage framework is the organising principle
The triage framework matters because back pain is not a single disease — it is a symptom with a vast differential, and over 90 per cent of patients have a benign mechanical cause that needs no investigation and no intervention [1]. The cost — to the patient, to the system — of treating every back pain as a potential malignancy or a potential surgical case is enormous, and the evidence is unambiguous that routine imaging in non-specific back pain does not improve outcomes and drives low-value care [2]. The registrar's discipline is to find the few who need investigation among the many who do not, and the red flag screen is the instrument that does this.
The triage is built on the red flag history and examination, performed on every patient, and it sorts the patient into one of the three bins. The bin then drives the investigation and the management. This is the logic of the NICE NG59 guideline, the American College of Physicians 2017 guideline, and the 2018 Lancet Low Back Pain Series — three converging, authoritative syntheses of the same evidence [3][4].
DWE high-yield: The single most testable fact about back pain is that most mechanical back pain needs no imaging. The registrar who orders an MRI for every patient with non-specific back pain has misunderstood the evidence and is practising low-value medicine. The corollary is that the red flag screen is not optional — it is the only safeguard against missing the serious pathology in the minority who have it. [1]
The differential — mechanical causes (about 90 per cent)

Mechanical (non-specific) back pain is the musculoskeletal pain of the spine and its supporting structures — the muscles, the ligaments, the facet joints, the intervertebral discs and the sacroiliac joints. The term "non-specific" is deliberate: in most cases, a single pain generator cannot be identified, and the attempt to do so (the "disc" versus the "facet" versus the "SI joint") does not change the management. The clinical signature of mechanical back pain is the discriminator: [1]
- Aggravated by movement and mechanical load — lifting, bending, prolonged sitting or standing.
- Relieved by rest — the patient is better lying down.
- Worse at the end of the day — the pain accumulates with activity.
- No night pain that wakes the patient from sleep (the pain may be present at night, but it is not the unremitting, progressive night pain of malignancy or infection).
- No systemic symptoms — no fever, no weight loss, no night sweats.
- No red flags on the history. [1]
Within the mechanical category, the clinician may recognise specific syndromes that have a distinct management: [1]
Disc herniation with radiculopathy
A herniated lumbar disc compresses a nerve root and produces radicular pain in a dermatomal distribution — the classic "sciatica." The L4, L5 and S1 roots are most commonly affected because the L4 to L5 and L5 to S1 discs bear the greatest load. The pain radiates below the knee (this is the discriminator from mechanical back pain, which typically refers to the buttock and the thigh but not below the knee), and it is often sharper, more electric, and accompanied by numbness and weakness in the affected myotome. [1]
The level is localised by the examination: [1]
| Root | Pain and sensory change | Weakness | Reflex |
|---|---|---|---|
| L4 | Anterior thigh, medial shin | Knee extension (quadratus), hip adduction | Knee jerk reduced |
| L5 | Lateral leg, dorsum of foot, great toe | Ankle dorsiflexion (foot drop), great toe extension | (no primary reflex) |
| S1 | Posterior leg, lateral foot, little toe | Ankle plantar flexion (calf) | Ankle jerk reduced |
The straight leg raise reproduces the L4 to S1 radicular pain; the femoral stretch test reproduces the L2 to L4 radicular pain (see Examination below). Most disc herniations settle with conservative therapy over 6 to 12 weeks; surgery (microdiscectomy) is reserved for the persistent or progressive deficit, the cauda equina, or the intractable pain. [1]
Facet joint pain
The facet (zygapophyseal) joints are the synovial joints between the posterior elements of the vertebrae, and they degenerate with age. Facet joint pain is worse on extension and rotation (the loading position of the facets), and it refers to the buttock and the thigh, rarely below the knee. Morning stiffness is common. The syndrome is over-diagnosed — the facet joints are a common finding on imaging in asymptomatic people — and the diagnosis is clinical, confirmed (if necessary) by a diagnostic block. [1]
Lumbar spinal stenosis with neurogenic claudication
Lumbar spinal stenosis is the narrowing of the spinal canal from a combination of degenerative disc bulging, facet joint hypertrophy and ligamentum flavum thickening. The clinical syndrome is neurogenic claudication — bilateral leg pain, numbness or weakness brought on by walking and relieved by sitting and by spinal flexion. The discriminator from vascular claudication is the position of relief: [1]
| Feature | Neurogenic claudication | Vascular claudication |
|---|---|---|
| Relieved by | Sitting, bending forward, walking uphill (flexion opens the canal) | Standing still (the leg re-perfuses) |
| Worse by | Walking downhill, standing (extension narrows the canal) | Walking uphill (the demand rises) |
| Pulses | Present | Absent or diminished |
| Pain with | Often back pain, numbness, and the pain may be above the knee | Calf pain, typically below, no back pain |
| Cycle test | Cycling tolerated well (flexed posture) | Cycling limited by claudication |
Management is conservative first (physiotherapy, flexion-based exercise, weight loss, analgesia); decompressive laminectomy — with or without fusion — is reserved for the refractory, disabling case. [1]
The differential — inflammatory causes (axial spondyloarthritis)
Inflammatory back pain is the signature of axial spondyloarthritis (axial SpA) — the umbrella term that includes ankylosing spondylitis and the spondyloarthritis associated with psoriasis, inflammatory bowel disease and reactive arthritis. The clinical signature is distinct from mechanical pain, and missing it delays the diagnosis by 6 to 10 years on average — a delay during which irreversible structural damage and disability accrue. [1]
The inflammatory back pain criteria (the ASAS criteria) are the questions to ask [8]:
- Age of onset under 40 — mechanical pain peaks in the 40s and 50s; inflammatory pain begins in the late teens, the 20s and the 30s.
- Insidious onset — not a sudden injury.
- Improvement with exercise — the opposite of mechanical pain, which is worsened by activity.
- No improvement with rest — again, the opposite of mechanical pain.
- Pain at night, with improvement on rising — the patient wakes in the second half of the night with back pain and stiffness, and gets up to move around.
- Morning stiffness over 30 minutes — the stiffness of inflammation, not the brief stiffness of osteoarthritis. [1]
Four out of five of these criteria have a sensitivity of over 70 per cent and a specificity of over 80 per cent for axial SpA. [1]
The extra-articular features that should prompt a search for axial SpA are: [1]
- Anterior uveitis (iritis) — unilateral, painful, red eye with photophobia.
- Psoriasis — ask and examine the scalp, the natal cleft, the umbilicus, the extensor surfaces.
- Inflammatory bowel disease — Crohn's disease, ulcerative colitis; ask about chronic diarrhoea, abdominal pain, rectal bleeding.
- Enthesitis — inflammation at the insertion of tendons and ligaments, classically at the heel (Achilles tendon insertion, plantar fascia).
- Dactylitis — a "sausage digit," the diffuse swelling of a whole finger or toe.
- A family history of spondyloarthritis, psoriasis, inflammatory bowel disease or uveitis. [1]
The modified New York criteria for ankylosing spondylitis require bilateral sacroiliitis grade 2 or above on the plain X-ray plus one clinical criterion (low back pain and stiffness over 3 months improving with exercise, limited lumbar motion, or limited chest expansion). The limitation is that radiographic sacroiliitis takes years to develop, which is the source of the diagnostic delay. The ASAS classification criteria address this by allowing MRI evidence of active sacroiliitis (bone marrow oedema) in the imaging arm, or an HLA-B27 plus two SpA features in the clinical arm, for patients with chronic back pain and onset under 45 years [8].
Management of axial SpA is a trial of NSAIDs first-line (the response to NSAIDs is itself a SpA feature in the criteria), a tumour necrosis factor inhibitor (adalimumab, etanercept, infliximab) or an IL-17 inhibitor (secukinumab) for the refractory disease, physiotherapy and exercise, and a treat-to-target approach under rheumatology guidance. [1]
Exam trap: The axial SpA question is one of the highest-yield DCE short-case and long-case discrimators. A young man with insidious-onset back pain, morning stiffness, a history of "eye problems" (uveitis) and psoriasis, and a rigid lumbar spine on examination (a modified Schober test under 5 cm) is axial SpA until proven otherwise. The registrar who attributes this to a "lumbar strain" has missed the diagnosis by a decade. [1]
The differential — infective causes (vertebral osteomyelitis, discitis, epidural abscess)

Vertebral osteomyelitis (which includes discitis, the infection of the disc space, and septic arthritis of the facet) is an infection of the vertebral body and the adjacent disc, usually by haematogenous spread. The risk groups are the intravenous drug user, the immunocompromised host, the diabetic, the patient with an indwelling line or a recent bacteraemia, the patient with endocarditis, and the post-procedure patient (after spinal surgery, after an epidural or a spinal injection). The commonest organism is Staphylococcus aureus (including methicillin-resistant); Gram-negatives from the urinary tract (Escherichia coli) and, in specific contexts, tuberculosis (Pott's disease) and brucellosis are important in the ANZ and migrant populations. [1]
The clinical signature, from the systematic review by Mylona and colleagues, is progressive, unremitting back pain that is not relieved by rest, often with night pain, and with fever in only about half of patients — the absence of fever does not exclude the diagnosis [7]. The inflammatory markers (CRP, ESR) are raised, often markedly; the white cell count may be normal. The X-ray can be normal for two to four weeks (the bone must lose 30 to 50 per cent of its mineral content before the X-ray changes), which is the classic trap — a normal X-ray does not exclude vertebral osteomyelitis, and the MRI is the modality of choice. The management is blood cultures and a guided biopsy for the organism, a prolonged course of targeted intravenous then oral antibiotics (typically 6 weeks), and surgery for the unstable spine, the epidural abscess or the failure of medical therapy.
The spinal epidural abscess is the surgical emergency within the infective category. The classic triad of back pain, fever and a neurological deficit is present in only a minority at presentation, which is why it is so often missed; the abscess can enlarge rapidly and compress the cord or the cauda equina, producing irreversible paraplegia or incontinence [6]. Any patient with back pain, fever and any neurological symptom — or any patient with the severe, knife-like back pain of an expanding abscess — needs an emergency MRI and urgent surgical decompression plus antibiotics. The mortality and the permanent neurological injury rise sharply with delay.
The differential — malignant causes (metastases and myeloma)
The spine is the commonest site of bony metastasis, and back pain is often the presenting symptom. The primaries that metastasise to bone are remembered by the mnemonic "BLT with a Kosher Pickle" — Breast, Lung, Thyroid, Kidney, Prostate — and the haematological malignancies, especially multiple myeloma, must be added. The clinical signature of malignant back pain is: [1]
- Progressive, unremitting pain that is not relieved by rest.
- Night pain that wakes the patient from sleep and that may be worse on lying flat (the venous congestion and the loss of the muscular splinting raise the pressure in the involved vertebra).
- Pain at multiple spinal levels or pain that moves between levels.
- Weight loss, fatigue, and other systemic symptoms.
- A history of known cancer — the single strongest predictor. [1]
In a patient with known cancer and new or worsening back pain, the assumption is malignant spinal cord compression until proven otherwise, and the management is dexamethasone 16 mg immediately plus an emergency MRI whole spine within 24 hours — do not wait for the neurological deficit, because back pain precedes the deficit in over 95 per cent of cases (see the spinal-cord-disease topic for the full Patchell criteria and the radiotherapy versus surgery decision) [5].
Multiple myeloma is the haematological malignancy to consider in any patient over 50 with back pain. The clinical picture is the CRAB triad — hyperCalcaemia, Renal impairment, Anaemia, and lytic Bone lesions — with bone pain (especially back pain from vertebral lytic lesions or fractures) as the commonest presentation. The screening investigations are the full blood count (anaemia), the calcium (hypercalcaemia), the renal function, the ESR (often markedly raised from the high globulins), the serum protein electrophoresis (a monoclonal band), the urinary Bence-Jones protein (free light chains), and the serum free light chain assay. The imaging of choice for myeloma is the whole-body low-dose CT (more sensitive than the skeletal survey); the MRI is used for the symptomatic site and for cord compromise. [1]
The differential — metabolic (osteoporotic vertebral fracture) and referred (visceral) causes
The osteoporotic vertebral fracture presents as a sudden, severe back pain on minimal trauma — often after a bending or a lifting manoeuvre, sometimes after a cough or a sneeze — in the patient at risk: the postmenopausal woman, the chronic corticosteroid user, the patient with low body weight, smoking, rheumatoid arthritis, hyperthyroidism, premature menopause, or a prior fragility fracture. The pain is at the thoracolumbar junction most commonly, it is worse on any movement, and it may radiate around the rib. The examination may reveal a kyphosis, a loss of height, and a tender spinous process at the fracture level. The X-ray or the CT shows the wedge compression; the MRI differentiates an acute (oedematous) fracture from a chronic one and excludes malignancy. The management is analgesia, early mobilisation, and bone protection — a bisphosphonate (alendronate, zoledronate) or denosumab, calcium and vitamin D, and the investigation and treatment of the underlying osteoporosis. Vertebroplasty and kyphoplasty (the injection of cement into the fractured vertebra) are reserved for the severe persistent pain after an acute fracture in selected patients, and the evidence for them is mixed. [1]
The referred (visceral) causes of back pain are the diagnoses that are missed when the registrar thinks only of the spine. The pain pattern is the key discriminator: somatic (mechanical) pain is sharp, localised, and reproduced by movement and palpation; visceral (referred) pain is deep, diffuse, poorly localised, not reproduced by spinal movement, and often accompanied by systemic or abdominal symptoms. The high-yield referred causes are: [1]
- Pancreatic cancer — deep, boring, upper abdominal pain radiating to the back, worse on lying flat, often relieved by leaning forward; weight loss; painless obstructive jaundice if the head of the pancreas is involved.
- Abdominal aortic aneurysm — a tearing back pain in an older man (or woman), often with a pulsatile abdominal mass; the ruptured AAA is a catastrophe with a mortality over 80 per cent and it needs immediate surgical and vascular help before any imaging.
- Renal colic — a colicky loin-to-groin pain with haematuria, often with nausea and vomiting; not reproduced by spinal movement.
- Pyelonephritis — flank pain, fever, rigors, dysuria.
- Retrocaecal appendicitis — atypical back or flank pain in the pregnant or the elderly patient.
- Pelvic pathology — endometriosis, ectopic pregnancy, pelvic inflammatory disease, prostatitis. [1]
The registrar who examines the abdomen, the pulses, and the urine in the patient with "back pain" has protected against the missed visceral cause. [1]
The red flags — the screen on every patient
The red flag screen is the instrument that sorts the patient into the bin. The NICE NG59 red flags, grouped by the pathology they suggest, are [3][4]:
| Category | Red flags |
|---|---|
| Cauda equina / cord | Saddle anaesthesia; urinary retention or incontinence; faecal incontinence; bilateral or severe leg symptoms; a sensory level; a progressive neurological deficit |
| Fracture | Age of onset under 20 or over 50; sudden severe trauma; a history of osteoporosis or chronic corticosteroid use |
| Infection | Fever; recent bacterial infection; intravenous drug use; immunocompromise |
| Malignancy | A history of cancer; weight loss; night pain; constant progressive non-mechanical pain; age over 50 |
| Inflammation | Age of onset under 20; morning stiffness over 30 minutes; improvement with exercise; alternating buttock pain; the extra-articular features of SpA |
| Other | Thoracic pain (the thoracic spine is an uncommon site of mechanical pain — think malignancy and infection); structural deformity; systemically unwell |
The single most important red flag constellation is cauda equina syndrome. The features are: [1]
- Severe low back pain — often bilateral.
- Bilateral sciatica (or a change in the pattern of an existing sciatica).
- Saddle anaesthesia — numbness in the perianal, perineal and genital regions (the S2 to S4 dermatomes). Ask: "Can you feel the toilet paper when you wipe?"
- Urinary retention or incontinence — painless retention is the classic sign; a post-void residual on the bladder scan is more sensitive than the history.
- Faecal incontinence or loss of the sensation of rectal fullness.
- Reduced anal tone on the per rectal examination.
- Lower limb motor deficit, often bilateral. [1]
The teaching from the Lavy review is that the classic complete triad is often absent at presentation — the diagnosis is made by a high index of suspicion and the objective findings (a post-void residual, a per rectal examination), and the management is an emergency MRI within 24 hours and urgent surgical decompression, ideally within 24 to 48 hours of the onset of the deficit [5]. The prognosis for the recovery of the bladder and the bowel function is better the earlier the decompression, and it is the sphincter function that recovers least well — which is why the cauda equina is a litigious diagnosis and why the threshold to image must be low.
The focused history — the questions that triage
The history in back pain is high-yield because each answer sorts the patient into the bin. The registrar should ask, in order: [1]
The cauda equina and the cord screen (first). "Any numbness around your back passage or genitals? Any change in your waterworks — difficulty starting, dribbling, or wetting yourself? Any change in your bowels — constipation or incontinence?" A single positive answer mandates the per rectal examination, the bladder scan, and the low threshold to image. [1]
Onset and progression. A sudden onset after a fall or a lift points to a mechanical injury or a fracture (in the at-risk patient). An insidious onset over weeks to months points to inflammation, infection or malignancy. A sudden, severe, "never-been-pain-like-it" back pain in an older man points to an AAA or an osteoporotic fracture. [1]
Site and radiation. Pain confined to the lower back and the buttock is typically mechanical. Pain radiating below the knee in a dermatomal band is radicular. Thoracic pain is a red flag. Pain that is deep, boring and poorly localised, not reproduced by movement, is referred. [1]
Character and pattern. Mechanical pain is sharp, reproduced by movement, relieved by rest. Inflammatory pain is worse in the morning and at night, better with activity. Malignant and infective pain is progressive, unremitting, and present at night. [1]
Aggravating and relieving factors. The position of relief is the key to neurogenic versus vascular claudication (above). The response to NSAIDs is a feature of inflammatory back pain. [1]
Systemic symptoms. Fever, night sweats, weight loss — the screen for infection and malignancy. [1]
Risk factors. A history of cancer; chronic corticosteroid use; intravenous drug use; immunocompromise; recent trauma; a recent infection; a known osteoporosis. [1]
The inflammatory screen. The ASAS criteria questions (age of onset under 40, insidious onset, improvement with exercise, no improvement with rest, night pain improving on rising, morning stiffness over 30 minutes). The extra-articular features (uveitis, psoriasis, inflammatory bowel disease, heel pain, dactylitis). [1]
Psychosocial (the yellow flags). Job satisfaction, mood, fear-avoidance beliefs, time off work. The yellow flags predict the progression to chronicity and they frame the biopsychosocial management of the persistent pain. [1]
The examination — the spine, the nerves, and the abdomen
The examination begins with the look test from the end of the bed. Before touching the patient, the registrar observes the posture (a list, a scoliosis, an antalgic lean), the gait (an antalgic gait, a foot drop, a wide-based ataxic gait), and the difficulty the patient has sitting, standing and undressing. The systematic examination then proceeds: [1]
Inspection and palpation of the spine
Inspect the back for scoliosis, kyphosis, a step in the spine (suggesting spondylolisthesis), muscle spasm, scars, and skin lesions — a hairy patch, a lipoma or a sinus over the lumbar spine suggests a spinal dysraphism (spina bifida occulta, a tethered cord). Palpate the spinous processes for a step and for tenderness, the paraspinal muscles for spasm and trigger points, and the sacroiliac joints. A step between adjacent spinous processes suggests spondylolisthesis. [1]
Movement
Assess the flexion (modified Schober test — mark the lumbosacral junction and 10 cm above, then ask the patient to bend forward; an increase of less than 5 cm indicates reduced lumbar flexion, the screening test for axial SpA), the extension (limited and painful in spinal stenosis and in facet joint disease), the lateral flexion, and the rotation. [1]
The nerve root tests
- The straight leg raise (Lasegue test) — with the patient supine, lift the straight leg; reproduction of the radicular pain (not back pain) between 30 and 70 degrees is positive, indicating L4, L5 or S1 root irritation. Dorsiflexion of the ankle (the Bragard test) worsens the pain. The crossed straight leg raise — lifting the asymptomatic leg reproduces the pain in the symptomatic leg — is highly specific for a large central disc, often with cauda equina involvement.
- The femoral stretch test (reverse straight leg raise) — with the patient prone, extend the hip with the knee flexed; reproduction of the anterior thigh pain is positive, indicating L2, L3 or L4 root irritation. [1]
The lower limb neurological examination
Examine the power (hip flexion L2, knee extension L3 to L4, ankle dorsiflexion L4 to L5, great toe extension L5, ankle plantar flexion S1 to S2), the sensation (the dermatomes — medial shin L4, dorsum of foot and great toe L5, lateral foot and little toe S1, posterior thigh and perianal S2 to S4), the reflexes (knee L3 to L4, ankle S1 to S2, and the plantar response), and the gait (a foot drop, a heel-to-toe walk). A reproducible motor deficit is a red flag that mandates imaging. [1]
The per rectal examination
In the suspected cauda equina, the per rectal examination is mandatory and it must never be omitted. Assess the anal tone at rest and on squeeze, the perianal sensation to pinprick (the S2 to S4 dermatomes), and the bulbocavernosus reflex (the contraction of the anal sphincter on squeezing the glans or tugging a urinary catheter — its absence indicates spinal shock and a severe cord or cauda lesion). [1]
The extra-spinal examination
The extra-spinal signs refine the differential: [1]
- The abdomen — a pulsatile mass (AAA), the organomegaly and the masses of malignancy, the tenderness of pyelonephritis or appendicitis.
- The pulses — absent or diminished pulses point to vascular claudication, not neurogenic.
- The skin — psoriasis (axial SpA), the erythema nodosum of sarcoidosis, the stigmata of intravenous drug use (the injection sites, the track marks).
- The eyes — a red, painful, photophobic eye (anterior uveitis in axial SpA).
- The chest — a breast lump, a lung mass (the primaries of bony metastasis).
- The prostate on the per rectal — a hard, nodular prostate (prostate metastases). [1]
DCE short-case high-yield: "Examine this patient's spine." The registrar who walks to the back first has failed the question. The correct routine is end of bed (the look test, the gait), then hands (psoriasis, the stigmata of SpA), then the abdomen (the AAA, the organomegaly), then the spine (inspection, palpation, movement), then the nerve root tests (straight leg raise, femoral stretch), then the lower limb neurological examination (power, sensation, reflexes), then the per rectal in the suspected cauda equina, then the extra-spinal signs (the eyes, the skin, the pulses). The integrated examination that does not stop at the musculoskeletal system is what the examiner is looking for. [1]
Investigations — most mechanical back pain needs no imaging

The cardinal principle of investigation in back pain is that most mechanical back pain needs no imaging. The evidence, from Deyo and Weinstein's foundational review onward, is unambiguous: imaging does not improve outcomes in non-specific back pain; it reveals age-related abnormalities (disc bulges, degenerative change) in asymptomatic people; and it drives a cascade of low-value downstream care (referrals, injections, surgery) that does not improve the outcome and that carries its own harms [1][2]. The NICE NG59 guideline, the ACP 2017 guideline and the Lancet series all converge on this point [3][4]. The registrar who orders an MRI for every back pain patient has misunderstood the evidence.
When to investigate
The investigations are driven by the red flags — they are not routine. The framework: [1]
- No red flags, no neurological deficit, no systemic symptoms — no imaging, no bloods. Reassure, mobilise, review at 4 to 6 weeks if the pain has not settled.
- A red flag or a neurological deficit — investigate. The bloods and the imaging are chosen by the suspected pathology. [1]
The bloods (when red flags are present)
- Full blood count — anaemia of malignancy or myeloma; leukocytosis of infection.
- CRP and ESR — raised in infection, in malignancy, and often in axial SpA; a normal ESR and CRP argue strongly against infection and most malignancy (a useful negative).
- PSA in a man over 50 — prostate metastases.
- Calcium and ALP — hypercalcaemia and raised ALP of myeloma and bony metastases.
- Protein electrophoresis and urinary Bence-Jones protein (and the serum free light chains) — myeloma.
- Liver function, renal function, and the bone profile — the systemic work-up of the suspected malignancy. [1]
The imaging
- Plain X-ray — the suspected fracture (after trauma, in the osteoporotic); the suspected ankylosing spondylitis (the anteroposterior view of the sacroiliac joints for the squared vertebrae, the syndesmophytes and the sacroiliitis). The limitation: the X-ray is normal in early infection and early malignancy, and it does not show the cord or the roots.
- MRI spine — the modality of choice for the suspected cauda equina, the suspected cord compression, the suspected infection (vertebral osteomyelitis, epidural abscess, discitis), the suspected malignancy, and the progressive neurological deficit. The MRI is the emergency within 24 hours for the cauda equina and the cord compression.
- CT — the fracture assessment (the bony architecture), the guided biopsy in vertebral osteomyelitis, and the alternative to MRI (the pacemaker, some implants) with CT myelography for the cord compromise.
- Bone scan or PET-CT — the multi-level bony metastases, the search for the occult primary, the staging of the known malignancy. [1]
The Choosing Wisely principle
The Choosing Wisely principle — endorsed by the Australian Rheumatology Association, the American College of Physicians and the American College of Radiology — is that imaging for non-specific back pain within the first 6 weeks, in the absence of red flags, is low-value care and should not be routine. The registrar who internalises this principle protects the patient from the cascade of over-diagnosis and over-treatment. [1]
Management of mechanical back pain — reassure, mobilise, treat the pain
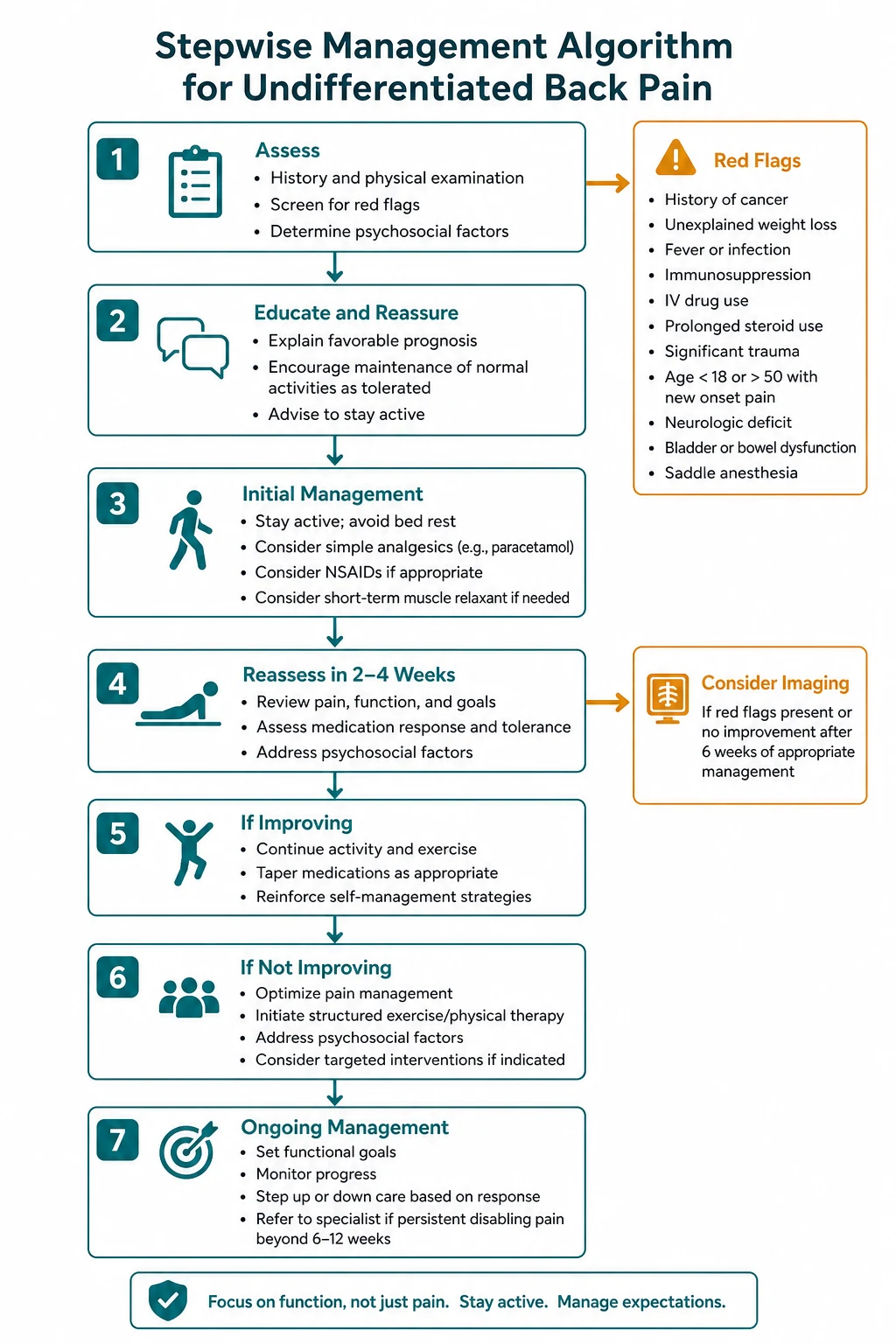
The management of acute, non-specific mechanical back pain is reassurance, education, staying active and simple analgesia — and the avoidance of bed rest. The evidence base, synthesised in the ACP 2017 guideline and the Lancet series, is as follows [3][4]:
Reassurance and education. Tell the patient that most back pain settles within 6 weeks, that the spine is strong, that the pain does not mean damage, and that activity is safe and helpful. The fear-avoidance message — "hurt does not equal harm" — is the single most effective psychological intervention. [1]
Stay active, avoid bed rest. Bed rest delays recovery, increases the risk of chronicity and deconditions the patient. The patient should continue their normal activities, including work, to the extent that the pain allows. The evidence is strong and consistent. [1]
Simple analgesia, in a stepwise fashion. The ACP 2017 guideline recommends non-pharmacological therapy first (heat, massage, acupuncture, spinal manipulation), then NSAIDs or skeletal muscle relaxants second-line, and opioids only as a last resort, and explicitly against paracetamol alone for acute low back pain (the PACE trial showed no benefit over placebo) [3]. The stepwise approach in the physician setting is: paracetamol 1 g four times daily (with the caveat that it is often ineffective alone); a short course of an NSAID (ibuprofen 400 mg three times daily, naproxen 500 mg twice daily, with a proton pump inhibitor for the at-risk patient); a short course of a weak opioid (codeine, tramadol) for the severe pain, with a clear endpoint and a plan to step down [3].
Physiotherapy and exercise in the subacute and chronic phase. Core strengthening, aerobic exercise, and a structured programme — the strongest evidence is for exercise in preventing the progression from acute to chronic back pain. [1]
Cognitive behavioural therapy and the multidisciplinary pain programme. For the chronic back pain, addressing the fear-avoidance, the catastrophising, the mood and the disability — the biopsychosocial model the Lancet series advocates. [1]
What not to do. Do not routinely image the non-specific pain. Do not routinely prescribe opioids, benzodiazepines or gabapentinoids first-line. Do not routinely refer for an epidural corticosteroid injection (reserved for the persistent radicular pain that fails conservative therapy). Do not routinely refer for surgery (reserved for the cauda equina, the progressive deficit, and the intractable radicular pain). [1]
Management of the specific causes
- Cauda equina syndrome — emergency MRI within 24 hours, urgent surgical decompression (ideally within 24 to 48 hours of the onset of the deficit) [5].
- Malignant spinal cord compression — dexamethasone 16 mg immediately, emergency MRI whole spine within 24 hours, and the radiotherapy versus surgery decision on the Patchell criteria (see the spinal-cord-disease topic) [5].
- Vertebral osteomyelitis — blood cultures and a guided biopsy for the organism, a prolonged course of targeted intravenous then oral antibiotics (typically 6 weeks), and surgery for the unstable spine, the epidural abscess or the failure of medical therapy.
- Spinal epidural abscess — emergency MRI, urgent surgical decompression, and antibiotics.
- Lumbar spinal stenosis — conservative first (physiotherapy, flexion-based exercise, weight loss, analgesia); decompressive laminectomy, with or without fusion, for the refractory disabling case.
- Axial spondyloarthritis — NSAIDs first-line, a TNF inhibitor or an IL-17 inhibitor for the refractory disease, physiotherapy, and a treat-to-target approach under rheumatology (NICE NG65).
- Osteoporotic vertebral fracture — analgesia, early mobilisation, bone protection (a bisphosphonate or denosumab, calcium and vitamin D), and the investigation and treatment of the underlying osteoporosis.
- Disc herniation with radiculopathy — conservative for 6 to 12 weeks (analgesia, physiotherapy, staying active); microdiscectomy for the persistent or progressive deficit, the cauda equina, or the intractable pain.
Regional guideline anchoring
The guidelines that frame the approach to back pain converge across regions, with local deltas the registrar must carry: [1]
- NICE Guideline NG59 (Low back pain and sciatica in over 16s) is the UK primary reference — the triage, the discouragement of routine imaging, the non-pharmacological first-line, the cautious use of NSAIDs and weak opioids, and the avoidance of paracetamol-alone and of routine epidural steroids [3].
- The American College of Physicians 2017 Guideline (Chou) is the US primary reference — non-pharmacological therapy first, then NSAIDs or skeletal muscle relaxants, opioids as a last resort, and against the routine use of paracetamol for acute low back pain [3].
- The 2018 Lancet Low Back Pain Series (Foster) is the global synthesis — the reduction of low-value care (unnecessary imaging, opioids and surgery), the biopsychosocial model, and the alignment of policy and reimbursement with the evidence [4].
- NICE Guideline NG65 (Spondyloarthritis in over 16s) frames the axial SpA pathway — the referral if inflammatory back pain is suspected, the MRI of the sacroiliac joints, the treat-to-target approach, and the TNF inhibitor for the refractory disease.
- Choosing Wisely Australia and the Australian Rheumatology Association carry the ANZ deltas — the same principles, with the local pathway and the local rheumatology referral thresholds confirmed on arrival at a new hospital.
The regional delta the registrar must carry: the principles converge (triage, no routine imaging, non-pharmacological first, cautious analgesia, the biopsychosocial model), but the specific institutional pathways differ — the rheumatology referral threshold for axial SpA, the MRI access for the suspected cauda equina, the local epidural and surgical referral thresholds. The registrar confirms the local pathway on arrival at a new hospital. [1]
DCE long-case approach
Patient scenario
Mr David Tran, 34, software engineer, presents to the outpatient clinic with a three-year history of progressive low back pain and morning stiffness, with a worsening over the last three months. The pain is in the lower back and the buttocks, it is worse in the morning, it improves with exercise, and it wakes him in the second half of the night — he gets up and walks around for relief. He has morning stiffness for over an hour. He has a history of psoriasis (on the scalp and the extensor surfaces, treated with a topical corticosteroid) and a single episode of a painful red right eye six months ago, treated as "iritis" by his optometrist. He has no bladder or bowel symptoms, no weight loss, no fever. He takes ibuprofen as needed, which helps. He is a non-smoker, he drinks alcohol in moderation, and there is no family history of note. [1]
On examination: he is afebrile, alert and oriented. The spine examination shows a reduced lumbar flexion (the modified Schober test increases by 3 cm), reduced chest expansion (4 cm at the fourth intercostal space), and tenderness over both sacroiliac joints. The straight leg raise is full and painless bilaterally. The lower limb neurological examination is normal. The skin shows psoriatic plaques on the scalp and the extensor surfaces of the elbows and the knees. There is no active eye inflammation. The abdomen is soft and non-tender, the pulses are present, and the per rectal examination is normal. The FBC, the renal and the liver function are normal. The CRP is raised at 24 (normal less than 5), the ESR is 38 mm per hour. The HLA-B27 is positive. The pelvic X-ray shows bilateral grade 2 sacroiliitis. [1]
Candidate's opening statement (SASPOP)
"Mr David Tran is a 34-year-old software engineer presenting with a three-year history of progressive inflammatory low back pain — pain that is worse in the morning, that improves with exercise, that wakes him at night and improves on rising, with morning stiffness over an hour — on a background of psoriasis and a prior episode of anterior uveitis. His main problem is axial spondyloarthritis, most likely ankylosing spondylitis, supported by the inflammatory back pain criteria, the psoriasis, the uveitis, the raised inflammatory markers, the HLA-B27 positivity and the bilateral sacroiliitis on the pelvic X-ray. My priorities are the confirmation of the diagnosis with an MRI of the sacroiliac joints to assess for active inflammation, the rheumatology referral for the treat-to-target management, the assessment of his cardiovascular and pulmonary risk (the association with aortic regurgitation, conduction disease and apical pulmonary fibrosis), the screening of his eyes for recurrent uveitis, and the discussion of the prognosis and the lifestyle — smoking cessation (he is a non-smoker, which I will reinforce), exercise and physiotherapy." [1]
Problem list
- Axial spondyloarthritis (ankylosing spondylitis), active — inflammatory back pain, psoriasis, uveitis, raised CRP and ESR, HLA-B27 positive, bilateral grade 2 sacroiliitis.
- Psoriasis — scalp and extensor surfaces.
- A prior episode of anterior uveitis — at risk of recurrence.
- Functional limitation — reduced lumbar flexion and chest expansion; risk of progressive spinal rigidity. [1]
Integrated management plan
- Confirm the diagnosis and assess the activity — MRI of the sacroiliac joints for the active (oedematous) sacroiliitis, which guides the escalation to a biologic.
- Rheumatology referral and the treat-to-target approach — a trial of a full-dose NSAID (naproxen 500 mg twice daily, with a proton pump inhibitor), with regular reassessment of the disease activity (the BASDAI score); escalation to a TNF inhibitor (adalimumab, etanercept) or an IL-17 inhibitor (secukinumab) for the refractory or the high-activity disease, guided by the NICE NG65 and the international recommendations [8].
- Physiotherapy and exercise — a structured programme of spinal mobility, postural exercise and core strengthening, the cornerstone of the long-term management.
- The uveitis — the ophthalmology link for the early treatment of recurrence (the uveitis of axial SpA is typically acute, unilateral, and responsive to topical corticosteroids, but the severe case may need systemic immunosuppression).
- The cardiovascular and the pulmonary surveillance — the association with aortic regurgitation, the conduction disease (heart block) and the apical pulmonary fibrosis; a baseline echocardiogram and a chest X-ray, and the vigilance for the chest pain and the breathlessness.
- The lifestyle and the psychosocial — the smoking cessation (smoking accelerates the radiographic progression), the ergonomic advice, the occupational therapy for the workplace, and the discussion of the prognosis — a treatable, manageable condition with a good functional outcome in the modern era.
Examiner probing questions and model answers
Q1: "How do you distinguish his inflammatory back pain from mechanical back pain?" [1]
"The ASAS inflammatory back pain criteria are my framework. Mr Tran meets at least four of the five: the age of onset under 40 (he is 34), the insidious onset, the improvement with exercise, the lack of improvement with rest, and the night pain improving on rising. He also has morning stiffness over an hour, which is the inflammatory signature. The discrimators from mechanical pain are the opposite response to activity (inflammatory improves, mechanical worsens), the night pain that improves on rising (mechanical pain is typically relieved by lying down), and the morning stiffness over 30 minutes. The extra-articular features — the psoriasis and the uveitis — are the clinching evidence that this is a spondyloarthritis. The registrar who attributes this presentation to a 'lumbar strain' has missed the diagnosis by years." [1]
Q2: "His pelvic X-ray shows grade 2 bilateral sacroiliitis. Does he need an MRI?" [1]
"The X-ray confirms the structural sacroiliitis, which is sufficient for the modified New York criteria for ankylosing spondylitis. The MRI is not needed to make the diagnosis in this case — but I would arrange it to assess the active inflammation (the bone marrow oedema), because the presence and the degree of active inflammation guides the escalation to a biologic. The MRI also detects the early sacroiliitis that the X-ray misses, which is the value of the ASAS imaging arm in the patient with the clinical picture but the normal X-ray. The teaching point is that the X-ray confirms the structural damage, and the MRI assesses the active inflammation — they answer different questions." [1]
Q3: "He is HLA-B27 positive. Does that confirm the diagnosis?" [1]
"No. The HLA-B27 is neither necessary nor sufficient for the diagnosis of axial SpA. It is a supporting feature in the ASAS clinical arm (HLA-B27 positive plus at least two SpA features), but Mr Tran already meets the imaging arm (sacroiliitis on imaging plus one SpA feature), so the HLA-B27 is confirmatory rather than diagnostic. The HLA-B27 is present in about 90 per cent of patients with ankylosing spondylitis but also in about 8 per cent of the general population, most of whom never develop the disease — so a positive test in isolation does not diagnose axial SpA, and a negative test does not exclude it." [1]
Q4: "What is your approach to his pharmacological management?" [1]
"The first-line is a full-dose NSAID at the maximum tolerated dose for at least two to four weeks — naproxen 500 mg twice daily, or celecoxib 200 mg twice daily, with gastroprotection. The response to NSAIDs is itself a SpA feature in the criteria, and about half to two-thirds of patients respond adequately [8]. If the NSAID is insufficient, or if there are contraindications (renal impairment, peptic ulcer, cardiovascular disease), or if the disease is high-activity, I escalate to a biologic under rheumatology guidance — a TNF inhibitor (adalimumab 40 mg subcutaneously every two weeks) or an IL-17 inhibitor (secukinumab), guided by the NICE NG65 and the international treat-to-target recommendations [8]. I avoid the systemic corticosteroid for the axial disease (it is largely ineffective) and I reserve the intra-articular corticosteroid for the peripheral joint or the sacroiliac joint injection in selected cases. The local anaesthetic and the corticosteroid are not a substitute for the disease-modifying therapy."
Q5: "What are the extra-articular complications you would screen for?" [1]
"The anterior uveitis (the commonest, in about a third of patients — I ask about eye pain, redness and photophobia, and I link him to ophthalmology), the cardiovascular associations (aortic regurgitation from aortic root dilatation, and conduction disease — I arrange a baseline echocardiogram and an ECG), the pulmonary associations (apical pulmonary fibrosis and the restrictive chest wall disease from the costovertebral rigidity — I monitor the chest expansion and the spirometry), the osteoporosis (the inflammation and the immobility increase the fracture risk — I monitor the bone density), and the inflammatory bowel disease (I ask about the chronic diarrhoea, the abdominal pain and the rectal bleeding). The teaching point is that axial SpA is a systemic disease, not just a back pain, and the surveillance spans the eyes, the heart, the lungs, the bones and the gut." [1]
Q6: "He is a software engineer. What occupational and lifestyle advice would you give?" [1]
"The smoking cessation is the single most important lifestyle message — smoking accelerates the radiographic progression, the spinal rigidity and the functional limitation, and it worsens the pulmonary complications. He is a non-smoker, which I reinforce. The exercise is the second cornerstone — a daily programme of spinal mobility, postural exercise, swimming and core strengthening, ideally with a physiotherapist. The ergonomic advice — the upright posture at the desk, the standing desk, the regular breaks — protects the spine. And the occupational therapy and the workplace accommodation — the flexible hours, the adjustable workstation — support the function. The psychological support — the reassurance that the condition is manageable, the link to a patient support group — addresses the anxiety that comes with a chronic inflammatory diagnosis." [1]
DCE short-case discussion: the spine examination
Instruction: "Examine this patient's spine. Present your findings and offer a differential diagnosis." [1]
Systematic examination routine
- End of the bed — the look test. Is the patient in pain? Is the posture abnormal (a list, a scoliosis, a kyphosis, a forward stoop)? Is the gait abnormal (an antalgic gait, a foot drop)? Is there difficulty undressing and sitting?
- Hands — psoriasis (the nails and the extensor surfaces), the stigmata of spondyloarthritis (dactylitis), and the general inspection.
- Abdomen — a pulsatile mass (AAA), the organomegaly.
- Spine — inspection — scoliosis, kyphosis, a step, muscle spasm, scars, skin lesions (a hairy patch, a sinus).
- Spine — palpation — tenderness over the spinous processes, the sacroiliac joints and the paraspinal muscles; a step suggesting spondylolisthesis.
- Spine — movement — flexion (the modified Schober test), extension (limited in stenosis and facet disease), lateral flexion, rotation; the chest expansion (reduced in ankylosing spondylitis).
- Nerve root tests — the straight leg raise (L4 to S1), the crossed straight leg raise (highly specific for a large central disc), the femoral stretch test (L2 to L4).
- Lower limb neurological examination — power (hip flexion, knee extension, ankle dorsiflexion, great toe extension, ankle plantar flexion), sensation (the dermatomes), reflexes (knee, ankle, plantar), gait (the heel and the toe walk).
- Per rectal examination — anal tone, perianal sensation (the S2 to S4 dermatomes), the bulbocavernosus reflex (in the suspected cauda equina).
- Extra-spinal — the eyes (uveitis), the pulses (vascular claudication), the chest (the breast, the lung). [1]
Presentation template
"I have examined Mr Tran's spine. At the end of the bed he is a young man with a mildly stooped posture and a reduced lumbar lordosis. His gait is normal. His hands show psoriatic plaques on the extensor surfaces. The abdomen is soft with no pulsatile mass. The spine shows a reduced lumbar flexion — the modified Schober test increases by only 3 cm — and a reduced chest expansion of 4 cm. There is tenderness over both sacroiliac joints. The extension and the lateral flexion are reduced. The straight leg raise is full and painless bilaterally. The lower limb neurological examination is normal. My findings are most consistent with an axial spondyloarthritis — the reduced lumbar flexion, the reduced chest expansion, the sacroiliac tenderness and the psoriasis — and I would confirm with an MRI of the sacroiliac joints, the HLA-B27 and the inflammatory markers, and a rheumatology referral." [1]
Discussion questions
Examiner: "Why is the chest expansion reduced in ankylosing spondylitis?" [1]
"The inflammation and the syndesmophyte formation at the costovertebral and the costotransverse joints stiffen the rib cage, so the patient cannot expand the ribs on inspiration and becomes dependent on the diaphragm. A chest expansion of less than 2.5 cm at the fourth intercostal space is one of the modified New York criteria for ankylosing spondylitis. The reduction in chest expansion is a marker of the spinal rigidity, and it predicts the restrictive lung disease that complicates the advanced condition." [1]
Examiner: "How would you investigate this patient?" [1]
"My framework is triage. Mr Tran has the inflammatory back pain criteria and the extra-articular features, so he is in the 'suspected axial SpA' bin. My investigations are: the inflammatory markers (CRP and ESR, raised), the HLA-B27 (positive, supportive), the pelvic X-ray for the sacroiliitis (the structural change), and the MRI of the sacroiliac joints for the active inflammation. I would also screen for the extra-articular associations — the echocardiogram for the aortic regurgitation, the chest X-ray for the apical pulmonary fibrosis, the ophthalmology review for the uveitis, and the questions for the inflammatory bowel disease. The registrar who investigates the 'back pain' with a lumbar spine MRI has missed the diagnosis, because the pathology is at the sacroiliac joints, not the lumbar spine." [1]
Examiner: "What is the single most important lesson from this case for a registrar managing back pain?" [1]
"The single most important lesson is to ask the inflammatory back pain questions in every patient under 40 with back pain. Mr Tran's diagnosis was delayed for three years because the registrar who saw him first attributed the pain to a 'lumbar strain' and did not ask about the morning stiffness, the night pain improving on rising, the improvement with exercise, or the psoriasis and the uveitis. The registrar who asks the inflammatory back pain criteria, examines for the extra-articular features, and measures the modified Schober and the chest expansion has made the diagnosis that day, and the patient is spared the years of untreated inflammation and progressive structural damage. The corollary is the triage: most back pain is mechanical and needs no imaging, but the minority with the inflammatory, the infective, the malignant and the cauda equina features must not be missed — and the red flag and the inflammatory screen on every patient is the safeguard." [1]
Key DWE MCQ patterns
- Discriminate the cause by the pain pattern. The pain that improves with exercise and is worse in the morning is inflammatory (axial SpA); the pain that worsens with activity and is relieved by rest is mechanical; the pain that is progressive and present at night is malignant or infective; the pain relieved by sitting and by flexion is neurogenic claudication.
- The cauda equina emergency. The patient with saddle anaesthesia, urinary retention and bilateral sciatica needs an emergency MRI and surgical decompression — not analgesia and review.
- The imaging trap. The normal X-ray in vertebral osteomyelitis for two to four weeks — the MRI is the modality of choice; the normal X-ray does not exclude the infection.
- The management of mechanical back pain. The first-line is reassurance, staying active, avoiding bed rest, and simple analgesia (NSAIDs second-line, opioids last resort) — not imaging and not bed rest.
- The referred pain trap. The deep, boring, poorly localised back pain not reproduced by movement is referred (pancreatic cancer, AAA, renal colic) — examine the abdomen, the pulses and the urine.
- The spinal stenosis discriminator. Neurogenic claudication is relieved by sitting and by flexion (walking uphill, cycling); vascular claudication is relieved by standing still and is associated with absent pulses.
- The inflammatory back pain criteria. Age under 40, insidious onset, improvement with exercise, no improvement with rest, night pain improving on rising — four of five has a high sensitivity and specificity for axial SpA.
- The cancer and the back pain. The known-cancer patient with new back pain has malignant spinal cord compression until proven otherwise — dexamethasone 16 mg and emergency MRI within 24 hours; do not wait for the neurological deficit [5].
References
[1] Deyo RA, Weinstein JN. Low back pain. N Engl J Med 2001;344(5):363–9. The foundational review of the assessment and the management of low back pain, arguing against the over-medicalisation, the routine imaging and the surgical over-treatment, and for the conservative, evidence-based approach to the majority of patients.
[2] Koes BW, van Tulder MW, Thomas S. Diagnosis and treatment of low back pain. BMJ 2006;332(7555):1430–4. A clinical review of the evidence-based diagnosis and the management of low back pain, including the triage, the discouragement of the routine imaging, and the active management of the non-specific majority.
[3] Chou R, Deyo R, Friedly J, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med 2017;166(7):514–30. The American College of Physicians guideline, recommending the non-pharmacological therapy first, the NSAIDs or the skeletal muscle relaxants second-line, the opioids as a last resort, and against the routine use of paracetamol for acute low back pain.
[4] Foster NE, Anema JR, Cherkin D, et al.; Lancet Low Back Pain Series Working Group. Prevention and treatment of low back pain: evidence, challenges, and promising directions. Lancet 2018;391(10137):2368–83. The Lancet Low Back Pain Series, the global synthesis calling for the reduction of the low-value care (unnecessary imaging, opioids and surgery), the biopsychosocial model, and the alignment of the policy and the reimbursement with the evidence-based practice.
[5] Lavy C, James A, Wilson-MacDonald J, Fairbank J. Cauda equina syndrome. BMJ 2009;338:b936. The clinical review of the cauda equina syndrome, highlighting the diagnostic difficulty (the classic triad is often incomplete), the high risk of litigation, the necessity of the emergency MRI, and the worse prognosis once the urinary retention has developed.
[6] Darouiche RO. Spinal epidural abscess. N Engl J Med 2006;355(19):2012–20. The review of the spinal epidural abscess, covering the diagnostic and the therapeutic challenges — the classic triad of back pain, fever and a neurological deficit is present in only a minority at presentation, and the risk is the irreversible cord damage from the delay.
[7] Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A. Pyogenic vertebral osteomyelitis: a systematic review of clinical characteristics. Semin Arthritis Rheum 2009;39(1):10–17. The systematic review of the clinical characteristics of the pyogenic vertebral osteomyelitis — the progressive unremitting back pain, the night pain, and the fever in only about half of the patients.
[8] Rudwaleit M, van der Heijde D, Landewe R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis 2009;68(6):777–83. The ASAS classification criteria for the axial spondyloarthritis — the imaging arm (sacroiliitis on imaging plus one SpA feature) and the clinical arm (HLA-B27 positive plus two SpA features) for the patient with the chronic back pain and the onset under 45 years.
Deyo & Weinstein, NEJM 2001; Koes et al., BMJ 2006; Chou et al. (ACP), Ann Intern Med 2017; Foster et al. (Lancet Series), Lancet 2018; Lavy et al. (Cauda equina), BMJ 2009; Darouiche (Spinal epidural abscess), NEJM 2006; Mylona et al. (Pyogenic vertebral osteomyelitis), Semin Arthritis Rheum 2009; Rudwaleit et al. (ASAS criteria), Ann Rheum Dis 2009; NICE NG59 (Low back pain and sciatica); NICE NG65 (Spondyloarthritis); NICE NG12 (Suspected cancer); American College of Physicians; Choosing Wisely Australia; Australian Rheumatology Association. [1]
References
- [1]Deyo RA, Weinstein JN Low back pain N Engl J Med, 2001.PMID 11172169
- [2]Koes BW, van Tulder MW, Thomas S Diagnosis and treatment of low back pain BMJ, 2006.PMID 16777886
- [3]Chou R, Deyo R, Friedly J, et al. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline From the American College of Physicians Ann Intern Med, 2017.PMID 28192789
- [4]Foster NE, Anema JR, Cherkin D, et al.; Lancet Low Back Pain Series Working Group Prevention and treatment of low back pain: evidence, challenges, and promising directions Lancet, 2018.PMID 29573872
- [5]Lavy C, James A, Wilson-MacDonald J, Fairbank J Cauda equina syndrome BMJ, 2009.PMID 19336488
- [6]Darouiche RO Spinal epidural abscess N Engl J Med, 2006.PMID 17093252
- [7]Mylona E, Samarkos M, Kakalou E, Fanourgiakis P, Skoutelis A Pyogenic vertebral osteomyelitis: a systematic review of clinical characteristics Semin Arthritis Rheum, 2009.PMID 18550153
- [8]Rudwaleit M, van der Heijde D, Landewe R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection Ann Rheum Dis, 2009.PMID 19297344