Phys · general-medicine
Undifferentiated Chest Pain — A Systematic Diagnostic Approach
Also known as chest pain · undifferentiated chest pain · acute chest pain · chest pain of unknown cause · diagnostic approach to chest pain · central chest pain · pleuritic chest pain · atypical chest pain · non-cardiac chest pain · the deadly six · HEART score · troponin algorithm · Wellens syndrome · Sgarbossa criteria · aortic dissection · Boerhaave syndrome
Consultant-physician-depth guide to the diagnostic approach to the patient with chest pain of unknown cause. Covers the deadly six causes (acute coronary syndrome, pulmonary embolism, aortic dissection, tension pneumothorax, cardiac tamponade, oesophageal rupture), the OPQRST history framework, pain-character-based differential diagnosis (central crushing, pleuritic, tearing interscapular, burning epigastric, positional), the focused cardiovascular and respiratory examination, the mandatory ECG and its subtleties (STEMI equivalents including Wellens, hyperacute T waves, new LBBB, Sgarbossa criteria), the high-sensitivity troponin 0/1h and 0/3h algorithms, the chest X-ray discriminators, the Wells score and D-dimer pathway for pulmonary embolism, the HEART score for early risk stratification, the Modified Early Warning Score, the approach to atypical presentations (women, elderly, diabetic), and the DCE long-case and short-case approach. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Chest Pain — A Systematic Diagnostic Approach

The answer first
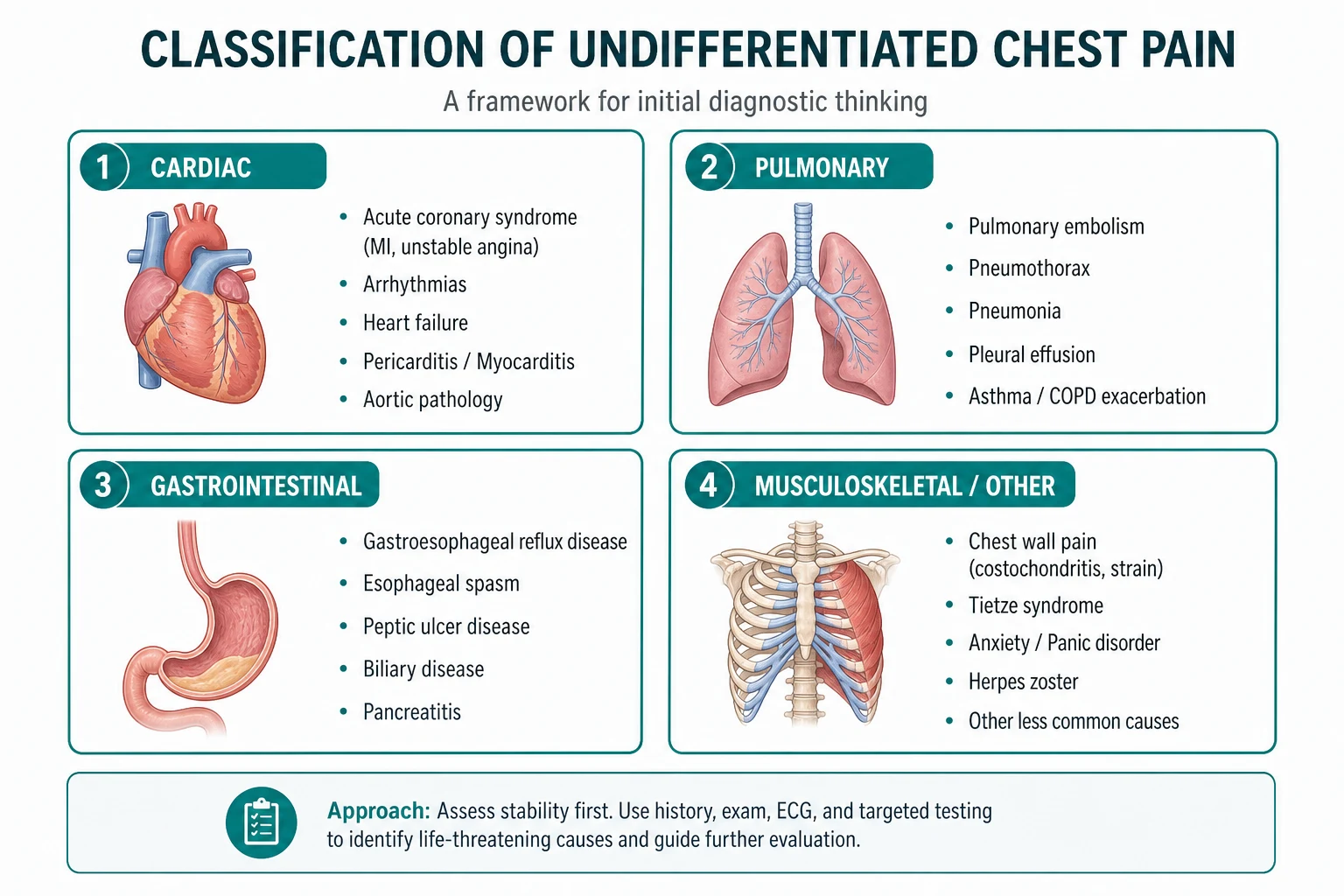
Chest pain is the commonest reason for emergency presentation in adult medicine and the presentation with the highest medicolegal and mortality risk if misdiagnosed. The cause spans at least six organ systems — cardiac, vascular, respiratory, gastrointestinal, musculoskeletal and psychiatric — and the registrar's job is to rapidly separate the six life-threatening causes (the deadly six) from the large majority of benign causes, without missing any of the former and without over-investigating the latter. The cognitive error that kills patients is not the missed rare diagnosis — it is the missed common diagnosis that was atypical in its presentation. [1]
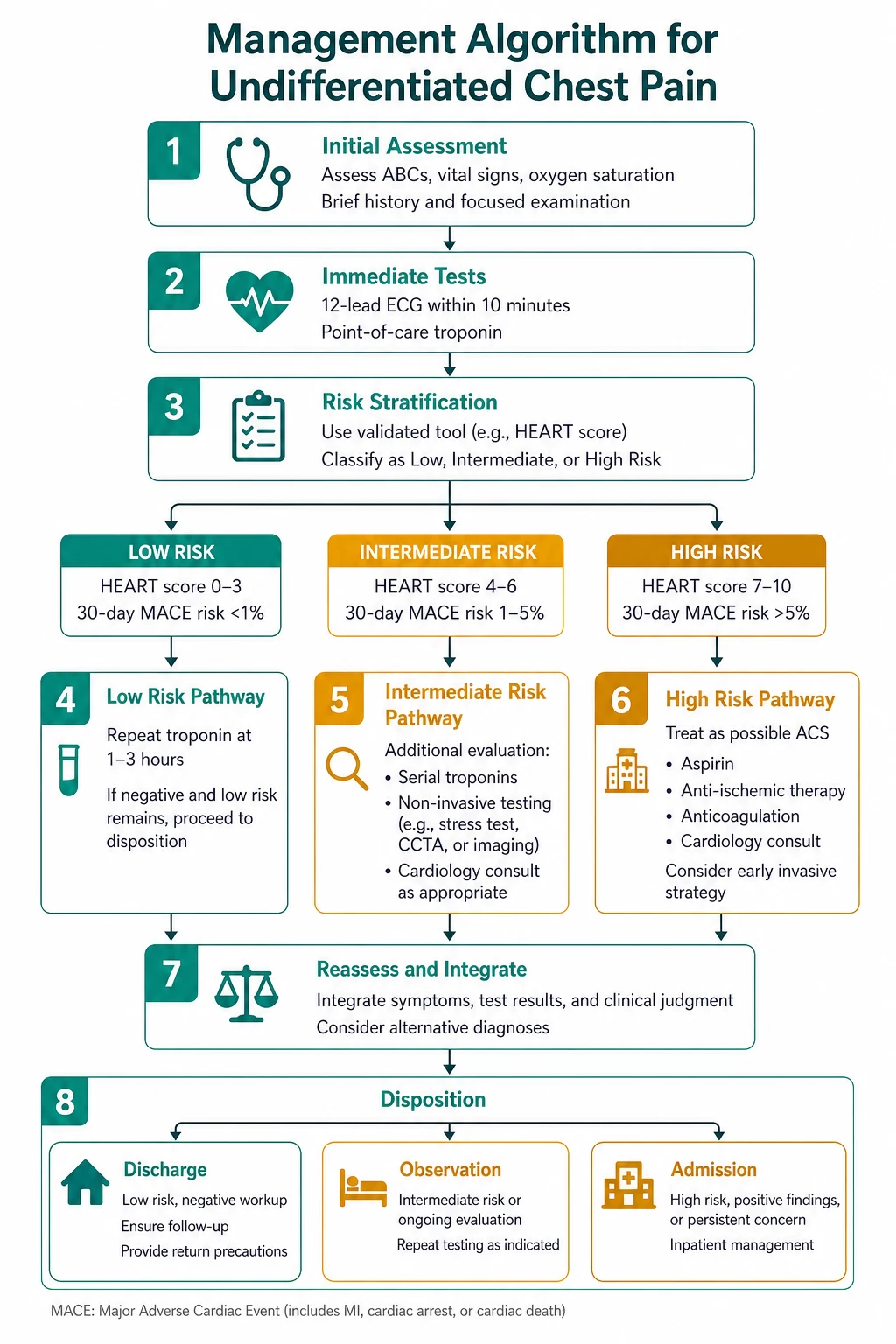
The reproducible sequence for every chest pain patient is: [1]
- Assess stability first — ABCDE. The patient in cardiogenic shock, tamponade, tension pneumothorax or massive PE needs resuscitation before the diagnostic work-up.
- Get the ECG within ten minutes — it is the single highest-yield test in chest pain, it is cheap, it is immediate, and it identifies the STEMI and the STEMI-equivalent that need catheter-lab activation.
- Characterise the pain — the OPQRST history (Onset, Provocation, Quality, Radiation, Severity, Timing) and the pain-character framework (central crushing, pleuritic, tearing, burning, positional) narrow the differential faster than any investigation.
- Identify the deadly six — acute coronary syndrome, pulmonary embolism, aortic dissection, tension pneumothorax, cardiac tamponade, oesophageal rupture. Every chest pain patient is screened for all six in the first assessment, even if the presentation seems benign.
- Risk-stratify — the HEART score for the ACS question, the Wells score for the PE question, the Modified Early Warning Score for the deteriorating patient.
- Decide: admit, observe, or discharge — based on the working diagnosis, the risk stratification and the response to the initial assessment. [1]
The single most dangerous error is premature closure on a benign diagnosis. The young patient with 'musculoskeletal' chest pain who is discharged and dies of aortic dissection two hours later; the woman with 'anxiety' who is having an inferior STEMI; the patient with 'reflux' who has oesophageal rupture — these are not hypothetical scenarios, they are the recurring failures that the systematic approach is designed to prevent. The second error is over-reliance on a single negative test — the normal ECG does not exclude ACS, the normal troponin at the wrong time does not exclude infarction, the normal chest X-ray does not exclude dissection or PE. [1]
Viva trap: "What is the single most useful piece of information in the first minute with a chest pain patient?" The honest answer is the pain character and its onset. "Sudden tearing pain between the shoulder blades" is a different patient from "gradual heavy central chest pain over two hours," and the differential generated by that single phrase is sharper than any single investigation. The registrar who asks "describe the pain in your own words" before reaching for the ECG has organised the entire encounter — but the registrar who does not also get the ECG within ten minutes has failed the patient. [1]
The deadly six — the life-threatening causes that must not be missed

Every chest pain patient is screened for six life-threatening causes in the first assessment. These are the deadly six — each can kill within hours, each is treatable if identified promptly, and each is commonly missed because the presentation is atypical or the registrar anchored on a benign alternative. [1]
1. Acute coronary syndrome
Acute coronary syndrome encompasses unstable angina, non-ST-elevation myocardial infarction (NSTEMI) and ST-elevation myocardial infarction (STEMI). The pain is classically central, crushing or pressure-like, lasting more than twenty minutes, radiating to the left arm, right arm, jaw or back, associated with diaphoresis, nausea, dyspnoea and a sense of doom. The pain may be atypical — burning, epigastric, sharp or even absent — in women, the elderly and the diabetic patient, and the registrar who requires classic pain to investigate for ACS will miss the atypical presentation. [1]
The ECG identifies the STEMI (ST elevation in two contiguous leads, or a new left bundle branch block in the right clinical context, or a true posterior infarct with ST depression in V1 to V3). The troponin identifies the NSTEMI and the unstable angina is ruled out by serial troponins. The 2023 ESC ACS Guidelines and the Fourth Universal Definition of Myocardial Infarction frame the diagnostic pathway — the high-sensitivity troponin at presentation and at one or three hours, the 0/1h or 0/3h algorithm, and the invasive strategy guided by the risk stratification [3][5].
The management of STEMI is immediate reperfusion — primary percutaneous coronary intervention if available within the recommended timeframe, or fibrinolysis if not. The management of NSTEMI is dual antiplatelet therapy, anticoagulation and an early invasive strategy within 24 to 72 hours for the intermediate- and high-risk patient. [1]
2. Pulmonary embolism
The pain is classically pleuritic — sharp, worse on inspiration, localised to one side of the chest — with sudden-onset dyspnoea. The patient may have haemoptysis. The risk factors are the venous thromboembolism risks — recent surgery, immobilisation, active cancer, pregnancy, oestrogen therapy, a long-haul flight, a family history of VTE. The chest X-ray is typically normal or near-normal — and the registrar who is reassured by a normal film in a breathless patient with pleuritic pain has misread the situation. [1]
The diagnostic pathway is the two-level Wells score (PE unlikely if 4 or less, PE likely if more than 4), the D-dimer if PE unlikely, and the CT pulmonary angiogram if PE likely or if the D-dimer is positive [9][10]. The management of confirmed PE is therapeutic anticoagulation (low-molecular-weight heparin transitioning to a direct oral anticoagulant), with thrombolysis for the massive PE with haemodynamic compromise.
3. Aortic dissection
The pain is classically tearing, ripping, of sudden onset, maximal at its onset (unlike the crescendo of ACS), radiating to the interscapular area or the back. The patient may have a blood-pressure differential between the arms (greater than 20 mmHg), a new aortic regurgitation murmur, neurological symptoms (stroke, paraplegia from spinal cord ischaemia), or pulse deficits. The Stanford classification divides dissections into type A (involving the ascending aorta — surgical emergency) and type B (distal to the left subclavian — medical management initially). [1]
The IRAD registry (Hagan and colleagues, 2000 — 464 patients) established that while sudden onset of severe pain was the most common presenting symptom (85 per cent), the classic physical findings such as pulse deficits (19 per cent) and blood-pressure differentials were frequently absent — the clinical presentation is diverse, and the diagnosis requires a high index of suspicion [6]. The chest X-ray may show a widened mediastinum (greater than 8 cm), but it is normal in up to 20 per cent of dissections. The definitive investigation is the CT angiogram of the chest and abdomen, which shows the intimal flap and the true and false lumens. The transoesophageal echocardiogram is the alternative if the patient is too unstable for CT.
The 2024 ESC Guidelines on aortic diseases and the 2014 ESC Guidelines frame the management — type A dissection is a surgical emergency (repair of the ascending aorta), type B is managed medically with blood-pressure control (intravenous beta-blocker first to reduce the systolic to below 120, then vasodilator), with endovascular or surgical intervention for the complicated type B [8][11].
4. Tension pneumothorax
The pain is sudden, pleuritic, unilateral, with severe dyspnoea. The examination reveals respiratory distress, tachycardia, hypoxaemia, hypotension, reduced air entry and hyper-resonance on the affected side, and tracheal deviation away from the affected side (a late sign). This is a clinical diagnosis — the registrar who waits for a chest X-ray to confirm tension pneumothorax before decompressing has allowed the patient to die. Immediate needle decompression at the second intercostal space mid-clavicular line (or the fifth intercostal space mid-axillary line, per the newer guidelines), followed by a chest drain. [1]
5. Cardiac tamponade
The pain may be pleuritic or dull, or it may be absent — the presentation is often dominated by dyspnoea, hypotension and collapse. Beck triad — hypotension, muffled heart sounds, raised JVP — is the classic bedside signature, and pulsus paradoxus (a fall in systolic blood pressure greater than 10 mmHg on inspiration) is the supporting sign. The ECG may show electrical alternans (alternating QRS amplitude as the heart swings in the pericardial fluid). The echocardiogram confirms the pericardial effusion with right ventricular diastolic collapse. The management is immediate pericardiocentesis. [1]
6. Oesophageal rupture (Boerhaave syndrome)
The pain is severe, excruciating, often following an episode of forceful vomiting or retching, localised to the chest or the epigastrium, and rapidly progressive. The patient may have subcutaneous emphysema (crackling under the skin at the neck or chest wall), and the chest X-ray may show pneumomediastinum, a left pleural effusion or subcutaneous air. The diagnosis is confirmed by a contrast swallow or a CT chest with oral contrast showing the extravasation. The mortality rises by approximately 2 per cent per hour of delayed diagnosis — this is a surgical emergency, and the registrar who diagnoses gastritis or reflux has missed a fatal condition. [1]
DWE high-yield: The single most testable fact about the deadly six is that the normal ECG does not exclude ACS, the normal chest X-ray does not exclude PE or aortic dissection, and the normal examination does not exclude tamponade or oesophageal rupture. The registrar who is reassured by any single negative investigation in a chest pain patient has misread the situation. The deadly six are excluded by a combination of history, examination, ECG, troponin, chest X-ray and — where the index of suspicion is high — the definitive imaging (CTPA for PE, CT angiogram for dissection, contrast swallow for Boerhaave). [1]
The OPQRST history — the questions that change the differential
The history in chest pain is the highest-yield single assessment. The OPQRST framework organises the questions so that each answer narrows the differential: [1]
Onset. Sudden onset (seconds to a peak within a minute) points to aortic dissection, tension pneumothorax, massive PE or arrhythmia. Gradual onset (crescendo over minutes to hours) points to ACS, pericarditis, pneumonia. Onset after vomiting points to oesophageal rupture. [1]
Provocation and palliation. Pain worse on inspiration (pleuritic) points to PE, pneumonia, pneumothorax, pericarditis or musculoskeletal pain. Pain worse on lying flat and better sitting forward points to pericarditis. Pain worse on exertion and better on rest points to angina. Pain better on sitting forward and worse on lying flat also occurs in pancreatitis. Pain reproduced by palpation points to musculoskeletal, but — and this is the critical teaching point — reproducibility on palpation does not exclude a serious cause; up to 15 per cent of ACS patients have chest-wall tenderness. [1]
Quality. The patient's own description is more informative than the registrar's leading question. Crushing, heavy, pressure-like or squeezing pain is ACS. Tearing or ripping pain is aortic dissection. Sharp, stabbing, knifelike pain that is pleuritic is PE, pneumothorax, pericarditis or musculoskeletal. Burning pain is reflux, peptic ulcer, oesophageal spasm or — if severe and after vomiting — Boerhaave. [1]
Radiation. Radiation to the left arm, right arm, jaw, neck or back is ACS. Radiation to the interscapular area or the lower back is aortic dissection. Radiation to the shoulder tip is diaphragmatic irritation (pericarditis, subdiaphragmatic abscess, splenic rupture). Radiation to the back is also pancreatitis and posterior duodenal ulcer. [1]
Severity. The severity out of ten is less useful than the patient's description of the severity relative to their previous pain — the patient who says "this is the worst pain I have ever felt" is the patient with dissection, STEMI or Boerhaave until proven otherwise. [1]
Timing. Pain lasting seconds is rarely cardiac (consider musculoskeletal, oesophageal spasm). Pain lasting minutes that comes and goes with exertion is angina. Pain lasting more than twenty minutes at rest is ACS until proven otherwise. Pain lasting hours to days that is positional is pericarditis or musculoskeletal. [1]
The pain-character framework
The pain character is the organising framework for the differential: [1]
- Central crushing pain — ACS (the priority), then aortic dissection (the mimic that kills), then oesophageal spasm.
- Pleuritic pain — PE, pneumonia, pneumothorax, pericarditis, musculoskeletal (costochondritis). The discriminator is the clinical context: the febrile patient with focal consolidation is pneumonia; the immobilised patient with sudden-onset dyspnoea is PE; the patient with positional pain and a pericardial rub is pericarditis.
- Tearing interscapular pain — aortic dissection (until proven otherwise).
- Burning epigastric pain — GORD, peptic ulcer, biliary colic, pancreatitis, and — critically — the atypical ACS presentation.
- Positional pain — pericarditis (worse lying flat, better sitting forward), pancreatitis (worse lying flat, better leaning forward). [1]
The risk-factor history
The risk factors frame the pre-test probability of the deadly six: [1]
- Cardiac risk factors — age, smoking, hypertension, diabetes, dyslipidaemia, family history of premature coronary disease, prior ACS, obesity, renal disease.
- VTE risk factors — recent surgery or immobilisation, active cancer, pregnancy or oestrogen therapy, long-haul travel, family history of VTE, known thrombophilia.
- Aortic risk factors — longstanding uncontrolled hypertension, Marfan syndrome, Ehlers-Danlos syndrome (vascular type), bicuspid aortic valve, prior aortic surgery, aortitis (giant cell, Takayasu), cocaine use, trauma. [1]
The examination — what changes the differential and the urgency
The examination in chest pain is the systematic search for the signs that confirm or exclude the deadly six. It begins at the end of the bed. [1]
Vital signs
The vital signs are the first and the most important observations: [1]
- Blood pressure in both arms — a differential greater than 20 mmHg suggests aortic dissection. This is a mandatory part of the chest pain examination and it is omitted in the majority of assessments.
- Heart rate — tachycardia suggests pain, hypovolaemia, arrhythmia, PE, tamponade or shock. Bradycardia suggests beta-blockade, heart block (inferior MI), or pre-terminal deterioration.
- Respiratory rate — the most neglected vital sign; tachypnoea is the hallmark of PE, pneumonia, pneumothorax and pulmonary oedema.
- Oxygen saturation — hypoxaemia in a patient with a normal chest X-ray is PE until proven otherwise.
- Temperature — fever suggests infection (pneumonia, mediastinitis), pericarditis or pancreatitis. [1]
The cardiovascular examination
The cardiovascular examination is the discriminator that separates the cardiac from the non-cardiac causes: [1]
- Pulses — check all four limb pulses and compare (pulse deficit or differential suggests dissection). The carotids (for radiation of a murmur), the femorals.
- JVP — elevated in heart failure, cor pulmonale, PE, cardiac tamponade, constrictive pericarditis. The raised JVP with hypotension and muffled heart sounds is tamponade.
- Apex — displaced in dilated cardiomyopathy and volume overload; tapping in left ventricular hypertrophy; hyperdynamic in volume overload or hyperthyroidism.
- Auscultation — murmurs (aortic stenosis, aortic regurgitation in dissection, mitral regurgitation in papillary muscle dysfunction, tricuspid regurgitation in pulmonary hypertension), gallop rhythm (third heart sound in heart failure), pericardial rub (pericarditis — best heard with the patient sitting forward and holding breath in expiration), pleural rub (pleurisy, PE). [1]
The respiratory examination
The respiratory examination maps the chest for the respiratory causes of chest pain: [1]
- Inspection — chest-wall deformity, scars, symmetrical movement (reduced on one side in pneumothorax, effusion, consolidation).
- Palpation — chest expansion (reduced unilaterally in pneumothorax, effusion, consolidation; reduced bilaterally in COPD). Chest-wall tenderness (reproducible pain suggests musculoskeletal, but does not exclude ACS).
- Percussion — resonant (normal, hyperinflation); dull (effusion, consolidation); hyper-resonant (pneumothorax).
- Auscultation — breath sounds (reduced in effusion, pneumothorax; bronchial in consolidation), added sounds (wheeze, crackles, pleural rub), vocal resonance. [1]
The abdominal examination
The abdominal examination is the often-omitted component that identifies the gastrointestinal causes of chest pain: [1]
- Epigastric tenderness — peptic ulcer, pancreatitis, biliary disease, and the atypical ACS presentation (the inferior MI with epigastric pain and nausea).
- Guarding or rigidity — peritonitis from a perforated viscus or pancreatitis.
- Hepatomegaly — right heart failure, metastatic disease. [1]
The extra-thoracic examination
- Subcutaneous emphysema at the neck or chest wall — pneumomediastinum, oesophageal rupture, tension pneumothorax.
- Calf swelling, tenderness, warmth — deep vein thrombosis, the source of the PE.
- Signs of Marfan or Ehlers-Danlos — tall, arachnodactyly, arm span greater than height, pectus deformity, high-arched palate, lens dislocation — the connective tissue diseases that predispose to aortic dissection.
- Stigmata of hyperlipidaemia — tendon xanthomata, xanthelasma, arcus juvenilis. [1]
The ECG — mandatory for every chest pain patient, interpreted with care
The 12-lead ECG is the single highest-yield investigation in chest pain and it is mandatory within ten minutes of arrival for every patient presenting with chest pain. The ECG identifies the STEMI and the STEMI-equivalent, and it frames the subsequent pathway — but the registrar must carry the subtleties and the limitations. [1]
The STEMI
ST elevation in two contiguous leads (at least 1 mm in the limb leads, at least 2 mm in the chest leads in men or 1.5 mm in women) is the criterion for STEMI. The territory is mapped: anterior (V1 to V4), inferior (II, III, aVF), lateral (I, aVL, V5, V6), right ventricular (V4R in the setting of inferior MI), and posterior (tall R waves and ST depression in V1 to V3, confirmed with posterior leads V7 to V9). The management is immediate reperfusion — primary PCI or fibrinolysis. [1]
The STEMI-equivalents — the patterns that are not obvious ST elevation but are equally urgent
The registrar must recognise the STEMI-equivalent patterns that do not show classic ST elevation but represent occlusion requiring urgent reperfusion: [1]
- Left bundle branch block, new or presumed new, in the right clinical context — this is a STEMI-equivalent that triggers the catheter-lab activation. The Sgarbossa criteria (Sgarbossa and colleagues, 1996) are used to identify acute infarction in the setting of LBBB: concordant ST elevation of 1 mm or more in a lead with a positive QRS (5 points); concordant ST depression of 1 mm or more in V1 to V3 (3 points); excessively discordant ST elevation of 5 mm or more in a lead with a negative QRS (2 points). A score of 3 or more is highly specific for acute infarction [7].
- Wellens syndrome — deeply inverted or biphasic T waves in V2 and V3 (often extending to V1 and V4) in a patient who is now pain-free, with minimal or no cardiac enzyme elevation, and critical proximal left anterior descending stenosis. The ECG is typically recorded when the pain has resolved, and the registrar who misses it — or who performs a stress test, which precipitates infarction — has caused a catastrophic outcome.
- Hyperacute T waves — broad-based, tall, asymmetrical T waves in the territory of the occlusion, preceding the ST elevation by minutes. They are the earliest ECG sign of infarction, and they are missed because the registrar is looking for ST elevation that has not yet developed.
- De Winter T waves — upsloping ST depression at the J point in the anterior leads with tall, symmetrical T waves, representing proximal LAD occlusion — a STEMI-equivalent.
- Posterior MI — horizontal ST depression in V1 to V3 with tall R waves and upright T waves, confirmed by posterior leads V7 to V9 showing ST elevation; this is a STEMI-equivalent that is missed on the standard 12-lead.
The NSTEMI
The NSTEMI shows ST depression, T wave inversion, or transient ST elevation, or it may be electrically silent. The diagnosis is made by the troponin. The management is dual antiplatelet therapy, anticoagulation, and an early invasive strategy within 24 to 72 hours for the intermediate- and high-risk patient. [1]
The non-ACS ECG patterns
The ECG also identifies the non-ACS causes: [1]
- Diffuse ST elevation with PR depression — pericarditis. The ST elevation is concave (saddle-shaped), widespread (not confined to a coronary territory), and accompanied by PR depression and a pericardial rub. The registrar who interprets diffuse pericarditis as an extensive anterior STEMI has misread the pattern — but the registrar who interprets an anterior STEMI as pericarditis has killed the patient. The discriminators are the distribution (pericarditis is diffuse, STEMI is territorial) and the morphology (pericarditis is concave, STEMI is convex).
- S1Q3T3, right axis deviation, right bundle branch block, T wave inversion in V1 to V4 — right heart strain from PE. These are neither sensitive nor specific, but in the right clinical context (sudden-onset dyspnoea, pleuritic pain, hypoxaemia) they support the diagnosis.
- Electrical alternans — cardiac tamponade (the heart swinging in the pericardial fluid).
- Peaked T waves — hyperkalaemia (not ACS, but a differential of chest pain with ECG changes). [1]
Exam trap — the normal ECG: The most common ECG error in chest pain is reassuring the patient and the registrar on the basis of a normal ECG. A normal ECG does not exclude ACS — up to 4 per cent of patients with a normal initial ECG have an acute infarction. The NSTEMI may be electrically silent. The Wellens patient has a normal or near-normal ECG by the time the registrar sees them. The patient with aortic dissection has a normal ECG (unless the dissection compromises the coronary ostium, typically the right coronary artery, giving an inferior MI pattern). The ECG is mandatory and high-yield, but it is interpreted with the clinical context — a normal ECG in a patient with ongoing central crushing chest pain is ACS until proven otherwise, not a reassurance. [1]
The troponin — the 0/1h and 0/3h algorithms
The high-sensitivity cardiac troponin (hs-cTn) is the cornerstone biomarker for the diagnosis of myocardial infarction, and the modern algorithms allow rapid rule-out or rule-in within one to three hours. The 2023 ESC ACS Guidelines and the Fourth Universal Definition of Myocardial Infarition frame the pathway [3][5].
The Universal Definition of Myocardial Infarction
The Fourth Universal Definition (Thygesen and colleagues, 2018) requires a rise and/or fall of cardiac troponin, with at least one value above the 99th percentile upper reference limit, plus at least one of: symptoms of myocardial ischaemia; new ischaemic ECG changes; development of pathological Q waves; imaging evidence of new loss of viable myocardium or new regional wall motion abnormality; identification of a coronary thrombus by angiography or autopsy [5].
The definition also distinguishes the five types of MI:
- Type 1 — atherothrombotic plaque rupture or erosion (the classic plaque-event infarction).
- Type 2 — supply-demand mismatch (demand ischaemia from tachyarrhythmia, hypotension, hypoxia, severe anaemia, hypertensive emergency). This is the type that is overdiagnosed when the troponin is elevated in a sick patient without a plaque event.
- Type 3 — MI causing cardiac death before biomarkers could be obtained.
- Type 4a — MI related to PCI. Type 4b — stent thrombosis. Type 4c — restenosis.
- Type 5 — MI related to CABG. [1]
The 0/1h algorithm
The high-sensitivity troponin 0/1h algorithm (Mueller and colleagues, 2016 — a multicentre evaluation of the hs-cTnT 0/1h algorithm in 1282 patients) stratifies patients into rule-out, observe, or rule-in based on the presentation troponin and the absolute change at one hour [4]. The algorithm is assay-specific (the cutpoints differ by assay), and it applies to patients with chest pain of suspected cardiac origin who have had symptoms for more than a few minutes. The algorithm:
- Rule-out — a very low presentation troponin (below the limit of detection) with a small one-hour delta excludes MI and allows safe early discharge.
- Observe — the intermediate group that requires further serial troponins and observation.
- Rule-in — a high presentation troponin or a large one-hour delta confirms MI and triggers the invasive pathway. [1]
The 0/1h algorithm reduces the ED length of stay and the proportion of patients requiring prolonged observation, and it is embedded in the ESC ACS Guidelines as a Class I recommendation. [1]
The 0/3h algorithm
For the centres without a validated 0/1h assay, the 0/3h algorithm is the alternative — troponin at presentation and at three hours, with a dynamic rise or fall indicating infarction and a stable low value excluding it. [1]
The troponin traps
The registrar must carry the troponin traps: [1]
- An elevated troponin does not equal infarction. The troponin is elevated in type 2 MI (demand ischaemia), PE, sepsis, heart failure, renal failure, rapid tachyarrhythmia, myocarditis, pericarditis, strenuous exercise, and critically ill patients of any cause. The elevated troponin indicates myocardial injury, and the job of the registrar is to determine whether the injury is type 1 (plaque event — treat as ACS) or non-type-1 (treat the underlying cause).
- A normal troponin at the wrong time does not exclude infarction. The troponin rises 3 to 6 hours after infarction. The patient who presents within the first hour of pain may have a normal troponin that rises on the repeat — this is the rationale for the serial troponin.
- Renal failure — the troponin is chronically elevated in renal failure, and the interpretation requires the baseline and the dynamic change. A chronically elevated troponin of 40 ng/L that rises to 200 with chest pain is an infarction; a chronically elevated troponin of 40 that remains at 42 is not. [1]
The chest X-ray — useful but limited
The chest X-ray is the second investigation after the ECG, and it identifies the radiographic signatures of the deadly six: [1]
- Pneumothorax — the visible visceral pleural line with absent lung markings beyond it. The tension pneumothorax is a clinical diagnosis — the X-ray is not required before decompression.
- Widened mediastinum (greater than 8 cm at the aortic knob) — aortic dissection. But the chest X-ray is normal in up to 20 per cent of dissections, and the registrar who is reassured by a normal mediastinum in a patient with tearing interscapular pain has misread the situation.
- Pulmonary oedema — cardiomegaly, upper-lobe venous diversion, interstitial and alveolar shadowing, Kerley B lines, pleural effusions. This is the radiographic signature of acute decompensated heart failure, which may complicate ACS.
- Consolidation — pneumonia, which may present with pleuritic chest pain and fever.
- Pneumomediastinum and subcutaneous emphysema — oesophageal rupture.
- Pleural effusion — on the left in Boerhaave syndrome; on either side in PE, pneumonia, heart failure. [1]
Risk stratification — the HEART score and the Wells score
The HEART score for the ACS question

The HEART score is the risk-stratification tool designed specifically for the emergency department chest pain patient. It was developed and prospectively validated by Backus and colleagues (2013) in a study of 2440 unselected chest pain patients, and it was validated in a multinational Asia-Pacific study of 2906 patients [1][2]. The score outperformed the TIMI and GRACE scores (which were designed for the inpatient ACS population, not the undifferentiated ED patient).
The five components, each scored 0 to 2: [1]
| Component | 0 points | 1 point | 2 points |
|---|---|---|---|
| History | Slightly suspicious | Moderately suspicious | Highly suspicious |
| ECG | Normal | Non-specific repolarisation | Significant ST deviation |
| Age | Under 45 | 45 to 64 | 65 or over |
| Risk factors | No risk factors | 1 to 2 risk factors | 3 or more risk factors, or known CAD |
| Troponin | Normal | 1 to 3 times normal | Elevated above 3 times normal |
The risk stratification:
- Low risk (score 0 to 3) — MACE rate 1.7 per cent at six weeks. These patients can be considered for early discharge with outpatient follow-up and a safety-net.
- Intermediate risk (score 4 to 6) — MACE rate around 20 per cent. These patients require admission, serial troponins and observation, and an invasive strategy guided by the ongoing assessment.
- High risk (score 7 to 10) — MACE rate exceeding 50 per cent. These patients are admitted for urgent investigation and management. [1]
The HEART score is a decision-support tool, not a substitute for clinical judgement. The registrar who discharges a patient with a HEART score of 3 on the basis of the score alone, without considering the clinical context and the patient's own risk tolerance, has misused the tool. [1]
The Wells score for the PE question
The two-level Wells score stratifies the pre-test probability of PE (PE unlikely if 4 or less, PE likely if more than 4), and it integrates with the D-dimer and CTPA in the validated algorithm (the Christopher study, van Belle and colleagues, 2006 — 3306 patients) [9][10]:
- PE unlikely plus negative D-dimer — PE excluded without imaging. The 3-month VTE incidence was 0.5 per cent.
- PE likely or positive D-dimer — proceed to CTPA. [1]
The age-adjusted D-dimer (cutoff equals age multiplied by 10 in micrograms per litre for patients over 50) increases the proportion of patients in whom PE can be excluded without imaging. [1]
The Modified Early Warning Score (MEWS)
The Modified Early Warning Score is the ward-based track-and-trigger system that flags the deteriorating patient. It scores the systolic blood pressure, heart rate, respiratory rate, temperature, and conscious level (AVPU), and a rising score triggers an escalation of care. The chest pain patient who is deteriorating — the falling blood pressure, the rising heart rate, the falling oxygen saturation — is the patient who needs the senior review and the high-dependency or ICU bed, regardless of the working diagnosis. [1]
The diagnostic pathway — from the undifferentiated patient to the working diagnosis

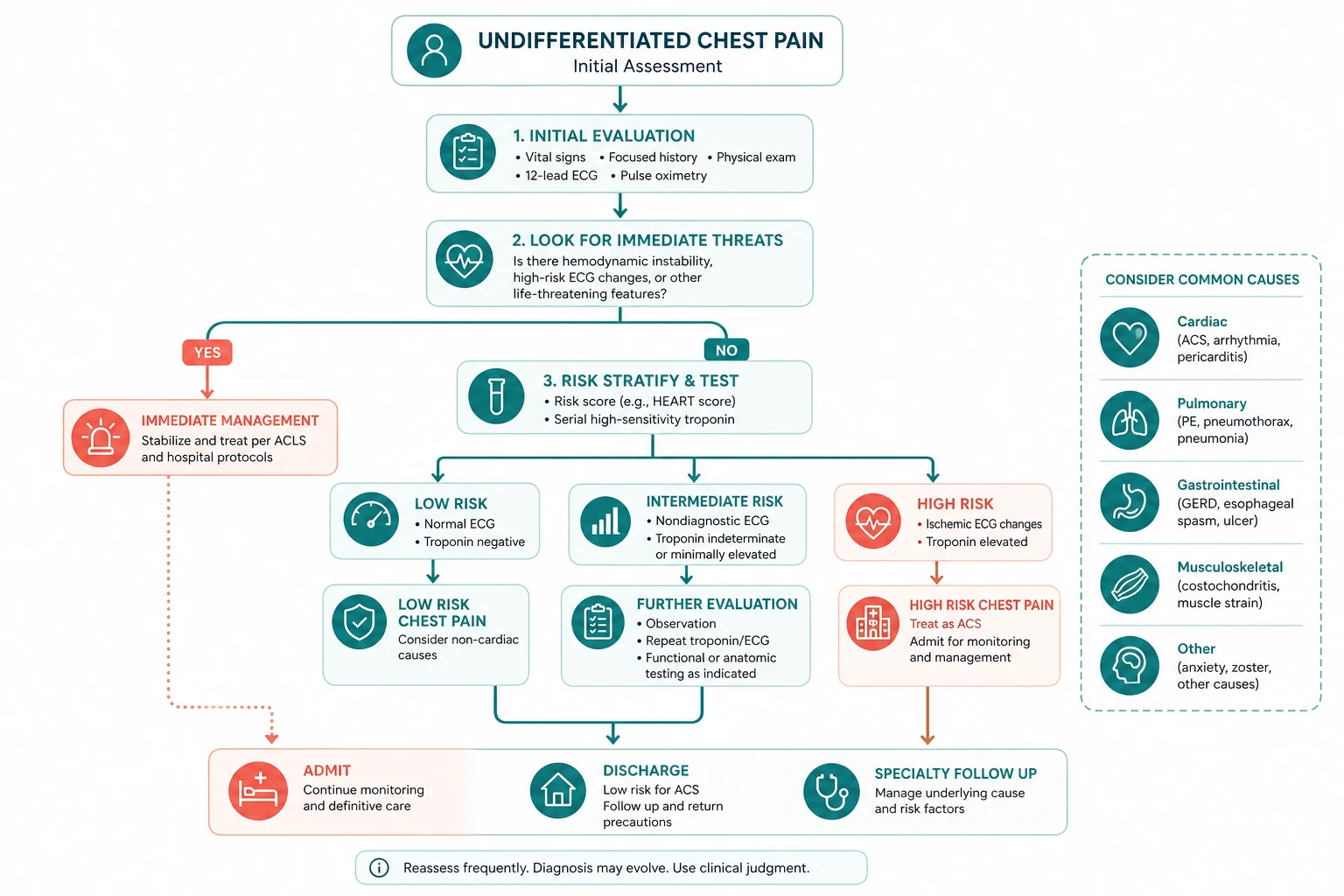
The diagnostic pathway for undifferentiated chest pain follows a disciplined sequence: [1]
- ABCDE — assess and stabilise. The unstable patient is resuscitated before the diagnostic work-up is pursued.
- ECG within ten minutes — interpreted with the STEMI and the STEMI-equivalents in mind. The catheter lab is activated for the STEMI and the new LBBB with ischaemic features.
- OPQRST history and risk factors — the pain character and the risk-factor profile narrow the differential.
- Focused examination — vital signs (including blood pressure in both arms), cardiovascular, respiratory, abdominal, extra-thoracic.
- Bloods — troponin (0/1h or 0/3h), full blood count, urea and electrolytes, D-dimer if PE suspected and Wells low or intermediate, lipids, glucose.
- Chest X-ray — the radiographic signatures of the deadly six.
- Risk stratification — HEART score for the ACS question, Wells score for the PE question, MEWS for the deteriorating patient.
- Definitive imaging if indicated — CTPA for suspected PE, CT angiogram for suspected dissection, contrast swallow for suspected Boerhaave, echocardiogram for suspected tamponade or pericardial effusion.
- Disposition decision — admit (the unstable, the high-risk, the confirmed or strongly suspected deadly six), observe (the intermediate-risk, the indeterminate troponin), discharge (the low-risk with a negative serial troponin and a reassuring HEART score, with a safety-net and outpatient follow-up). [1]
The atypical presentation — women, the elderly and the diabetic
The atypical presentation of ACS is the single largest source of missed diagnosis and delayed treatment. Women, the elderly and the diabetic patient frequently present without classic central crushing chest pain — they present with dyspnoea, fatigue, nausea, vomiting, epigastric discomfort, syncope, or just feeling unwell. The registrar who requires classic chest pain to investigate for ACS in these populations has excluded the majority of infarctions. [1]
The teaching points: [1]
- Women — more likely to present with dyspnoea, nausea, vomiting, back or jaw pain, and fatigue. The classic central chest pain is absent or atypical in up to 40 per cent of women with ACS.
- The elderly — may present with confusion, syncope, falls, or dyspnoea. The pain may be absent or attributed to other causes (arthritis, musculoskeletal). The threshold for the ECG and the troponin must be lower in the older patient.
- The diabetic patient — autonomic neuropathy blunts the pain sensation, and the diabetic patient may have a silent infarction presenting as dyspnoea, heart failure, syncope, or an arrhythmia. [1]
The corollary: the registrar maintains a low threshold for the ECG and the troponin in the woman, the elderly and the diabetic patient who presents with any of the atypical symptoms, even without classic chest pain. The missed atypical ACS is the commonest and the most consequential error in chest pain assessment. [1]
Regional guideline anchoring
The guidelines that frame the work-up of chest pain converge across regions, with local deltas the registrar must carry: [1]
- The 2023 ESC ACS Guidelines (Byrne and colleagues) integrate the management of the entire ACS spectrum (unstable angina through STEMI) into a single document, embed the 0/1h troponin algorithm, and frame the invasive strategy and the antithrombotic therapy [3].
- The Fourth Universal Definition of Myocardial Infarction (Thygesen and colleagues, 2018) defines the types of MI and the diagnostic criteria, and it is the global standard [5].
- The 2024 ESC Guidelines on peripheral arterial and aortic diseases (Conte and colleagues) frame the diagnosis and management of aortic dissection and the other aortic syndromes, merging the 2014 aortic diseases guideline [8][11].
- NICE CG95 (Chest pain of recent onset) frames the UK pathway — CT coronary angiography as the first-line investigation for the stable chest pain patient, and the standard ACS pathway for the acute patient.
- The Heart Foundation of Australia frames the ANZ approach to the ACS patient, with the local pathways for the catheter-lab activation.
The regional delta the registrar must carry: the principles converge (ECG within ten minutes, troponin with the 0/1h or 0/3h algorithm, risk stratification with HEART, PE with Wells and D-dimer and CTPA, dissection with CT angiogram), but the specific institutional pathways differ — the registrar confirms the local catheter-lab activation criteria, the local troponin assay cutpoints, and the local observation-unit protocols on arrival at a new hospital. [1]
DCE long-case approach
Patient scenario
Mrs Margaret O'Sullivan, 68, retired schoolteacher, presents to the emergency department with two hours of central chest pain that started at rest, described as a heavy pressure radiating to the left arm and the jaw, associated with diaphoresis and nausea. She has a background of type 2 diabetes (HbA1c 64 mmol/mol, on metformin and gliclazide), hypertension (on perindopril and amlodipine), hyperlipidaemia (on atorvastatin, LDL 2.1 mmol per L), and hypothyroidism (on thyroxine). She smoked 30 pack-years and stopped ten years ago. Her father had an MI at 55 and her brother had a CABG at 60. She is normally independent, walking 30 minutes daily. [1]
On assessment: alert and diaphoretic, blood pressure 152/94 in the right arm and 138/90 in the left, heart rate 96 in sinus rhythm, respiratory rate 20, SpO2 97 per cent on room air, temperature 36.8. The ECG shows ST elevation of 2 mm in the inferior leads (II, III, aVF) with reciprocal ST depression in I and aVL. The troponin at presentation is 45 ng per L (99th percentile 14). The chest X-ray shows clear lung fields, a normal cardiac silhouette, no widened mediastinum. [1]
Candidate's opening statement (SASPOP)
"Mrs O'Sullivan is a 68-year-old retired schoolteacher presenting with two hours of central crushing chest pain radiating to the left arm and jaw, with diaphoresis and nausea, on a background of type 2 diabetes, hypertension, hyperlipidaemia and hypothyroidism. She is a 30-pack-year ex-smoker with a strong family history of premature coronary disease. Her ECG shows an inferior STEMI with reciprocal changes, and her troponin is elevated. This is an acute ST-elevation myocardial infarction. My immediate priority is to activate the catheter lab for primary percutaneous coronary intervention, while I initiate the antiplatelet and anticoagulant therapy, control her pain and her sympathetic drive, and assess for the complications of the infarction — in particular, right ventricular involvement, which is common in inferior MI and which changes the fluid management." [1]
Problem list
- Acute inferior STEMI — ST elevation in II, III, aVF, reciprocal changes, elevated troponin. Primary PCI is the immediate priority.
- Cardiovascular risk factors — type 2 diabetes, hypertension, hyperlipidaemia, ex-smoker, strong family history. These frame the secondary prevention.
- Right ventricular involvement to be assessed — the inferior STEMI may involve the right ventricle (in up to 40 per cent), which is diagnosed by ST elevation in V4R and which makes the patient preload-sensitive (nitrates and diuretics may cause hypotension).
- Diabetes management during the ACS — the stress hyperglycaemia, the metformin (held for the contrast of the angiogram), the insulin sliding scale if the glucose is very high. [1]
Integrated management plan
The management is protocol-driven and time-critical: [1]
- Activate the catheter lab — primary PCI is the gold standard for STEMI if it can be delivered within the recommended timeframe (door-to-balloon within 90 minutes). If PCI is not available within the required timeframe, fibrinolysis is the alternative (tenecteplase, a single intravenous bolus, followed by transfer to a PCI-capable centre).
- Antiplatelet and anticoagulant therapy — aspirin 300 mg loading then 100 mg daily, a P2Y12 inhibitor (ticagrelor 180 mg loading then 90 mg twice daily, or prasugrel 60 mg loading then 10 mg daily, or clopidogrel 300 to 600 mg loading then 75 mg daily), and an anticoagulant (unfractionated heparin or bivalirudin during the PCI). [1]3. Pain and sympathetic-drive control — morphine 2.5 to 5 mg intravenously (with an antiemetic), sublingual glyceryl trinitrate (unless hypotensive or the right ventricle is involved).
- Assess for right ventricular involvement — the right-sided ECG (V4R) is mandatory in the inferior STEMI. If ST elevation is present in V4R, the right ventricle is involved and the patient is preload-sensitive — avoid nitrates and diuretics, and give fluid if hypotensive.
- Assess for complications — heart failure, arrhythmia (the inferior MI may cause bradycardia and heart block from vagal stimulation or AV nodal ischaemia), pericarditis, ventricular septal rupture, papillary muscle dysfunction.
- Secondary prevention — dual antiplatelet therapy for 12 months, a high-intensity statin (atorvastatin 80 mg), an ACE inhibitor (or ARB), a beta-blocker (once the acute phase is stable), cardiac rehabilitation, glycaemic optimisation, smoking-cessation reinforcement, and an echocardiogram to assess the ejection fraction and the wall-motion abnormality. [1]
Examiner probing questions and model answers
Q1: "Her blood pressure is 152 over 94 in the right arm and 138 over 90 in the left. Is this aortic dissection?" [1]
"The blood-pressure differential of 14 mmHg is below the 20 mmHg threshold that raises the concern for aortic dissection, and her clinical picture — the inferior STEMI on the ECG, the classic cardiac pain, the cardiac risk factors — is overwhelmingly consistent with ACS. The differential is noted and documented, and I am aware that dissection can compromise the coronary ostium (typically the right coronary artery, giving an inferior MI pattern). But the clinical picture does not support dissection as the primary diagnosis — the pain is central crushing rather than tearing interscapular, there is no new aortic regurgitation murmur, no pulse deficit, and the chest X-ray shows no widened mediastinum. I proceed to primary PCI, and the coronary angiogram will definitively exclude dissection as the cause. If the angiogram shows normal coronaries in the setting of an inferior STEMI pattern, I immediately reconsider dissection and proceed to an aortogram." [1]
Q2: "What if she develops complete heart block during the infarction?" [1]
"Complete heart block occurs in up to 10 per cent of inferior STEMIs, typically from ischaemia of the AV node (supplied by the right coronary artery in 90 per cent of patients). The management is transcutaneous pacing as a bridge, with the recognition that the inferior-MI heart block is often transient and resolves with reperfusion. If the heart block persists or is symptomatic with hypotension, a temporary transvenous pacemaker is inserted. The teaching point is the difference between the inferior-MI heart block (usually transient, often has a stable escape rhythm, and often resolves with reperfusion) and the anterior-MI heart block (from extensive septal and bundle-branch infarction, often a sign of a large infarct with a poor prognosis, and more likely to need a permanent pacemaker). The inferior-MI complete heart block that persists beyond the acute phase is assessed for a permanent pacemaker on its own merits." [1]
Q3: "How do you manage her diabetes during the admission?" [1]
"I hold the metformin for the angiogram because of the risk of contrast-induced nephropathy and lactic acidosis, and I manage the hyperglycaemia with an insulin sliding scale if the glucose is above 10 mmol per L. The target during the acute ACS is a glucose of 6 to 10 mmol per L — the tight control of the DIGAMI trial showed a mortality benefit, but the hypoglycaemia risk must be managed. Once the acute phase resolves and the renal function is confirmed, I restart the metformin and optimise the oral therapy or add a basal insulin, guided by the diabetes team. I also ensure that an SGLT2 inhibitor is considered for the cardiorenal protection, in line with the current guidelines. The long-term glycaemic target is an HbA1c of 53 mmol per L or less, with the individualised targets for the older or frailer patient." [1]
Q4: "What is your secondary prevention plan?" [1]
"The secondary prevention is the four pillars: antiplatelet therapy (dual for 12 months, then lifelong single), lipid-lowering (atorvastatin 80 mg, target LDL below 1.4 mmol per L), neurohormonal modulation (ACE inhibitor and beta-blocker, titrated to the maximum tolerated dose), and lifestyle (smoking cessation reinforcement, cardiac rehabilitation, Mediterranean diet, regular exercise). I add an SGLT2 inhibitor for the cardiorenal benefit. I arrange the echocardiogram to assess the ejection fraction and the wall-motion abnormality, and the cardiology follow-up at six weeks. The teaching point is that the secondary prevention is as important as the acute reperfusion — the patient who has the PCI and then stops the medications at three months has squandered the benefit of the intervention." [1]
Q5: "She is a woman. Does this change anything?" [1]
"It changes the index of suspicion — women are more likely to present atypically, and they are more likely to be under-investigated and under-treated. But Mrs O'Sullivan has presented classically, and her sex does not change the acute management. What it changes is the counselling — the woman who has had an ACS is at higher risk of being under-treated at follow-up, and I am explicit about the importance of the medications and the rehabilitation. I also address the cardiac rehabilitation, which is under-used in women, and the psychosocial support, because the anxiety and the depression after an ACS are commoner in women and are independent risk factors for a poor outcome." [1]
Q6: "What is the single most important lesson from this patient for a registrar managing undifferentiated chest pain?" [1]
"The single most important lesson is that the systematic approach — the ECG within ten minutes, the pain-character history, the focused examination, the risk stratification — identified this STEMI within minutes and triggered the time-critical pathway. The registrar who added the pain-character history to the classic crushing central pain, the diaphoresis, the nausea and the cardiac risk factors, and who got the ECG within ten minutes, has done everything right. The corollary is the atypical patient — the woman with dyspnoea and nausea, the elderly patient with confusion, the diabetic with fatigue — these patients do not present with the classic picture, and the registrar who maintains the low threshold for the ECG and the troponin in these populations will catch the atypical ACS that the classic approach would miss." [1]
DCE short-case discussion: the cardiovascular examination in the chest pain patient
Instruction: "Examine this patient's cardiovascular system. Present your findings and offer a differential diagnosis." [1]
Systematic examination routine
- End of the bed — the look test. Is the patient in pain, distress, comfortable? Pale, diaphoretic, cyanosed, breathless? Are there clues in the surroundings — oxygen, a cardiac monitor, a nitrate spray?
- Hands — peripheral cyanosis, cold and clammy skin (cardiogenic shock), splinter haemorrhages and Osler nodes (endocarditis), tendon xanthomata (hyperlipidaemia), clubbing (cyanotic heart disease, endocarditis). The pulse — rate, rhythm, character (collapsing pulse of aortic regurgitation, slow-rising of aortic stenosis, alternating of severe left ventricular failure).
- Face — plethoric (polycythaemia), corneal arcus and xanthelasma (hyperlipidaemia), malar flush (mitral stenosis), high-arched palate and lens dislocation (Marfan — dissection risk). The mouth — poor dentition (endocarditis risk).
- Neck — the JVP (elevated in heart failure, PE, tamponade; the Kussmaul sign of constrictive pericarditis), the carotid pulse (character, radiation of murmurs), the cervical and supraclavicular nodes.
- Praecordium — inspect for scars (sternotomy, PCI access sites), visible pulsations. Palpate the apex (position, character — displaced in dilated cardiomyopathy, tapping in AS, heaving in hypertension or HOCM), the left parasternal heave (right ventricular hypertrophy, pulmonary hypertension), and thrills. Auscultate systematically — the apex with the bell for the low-frequency sounds (mitral stenosis), then the diaphragm moving from the apex to the lower left sternal edge, the upper left sternal edge (pulmonary area), and the upper right sternal edge (aortic area). Listen for the heart sounds (S1, S2 — the loud P2 of pulmonary hypertension, the reverse split of LBBB or aortic stenosis), the added sounds (S3 gallop of heart failure, S4 of hypertrophy or acute ischaemia, the pericardial rub of pericarditis, the opening snap of mitral stenosis), and the murmurs (systolic — aortic stenosis, mitral regurgitation, tricuspid regurgitation, HOCM; diastolic — aortic regurgitation, mitral stenosis). Listen at the left axillary radiation of mitral regurgitation and the carotid radiation of aortic stenosis. Sit the patient forward and listen at the lower left sternal edge in expiration for the diastolic murmur of aortic regurgitation and the pericardial rub.
- Back — auscultate the lung bases (effusion, pulmonary oedema), check for sacral oedema.
- Abdomen — hepatomegaly (right heart failure), hepatojugular reflux, ascites, epigastric tenderness (the atypical ACS, peptic ulcer, pancreatitis).
- Legs — peripheral oedema, the DVT signs (calf swelling, tenderness, warmth — the source of the PE), the peripheral pulses (femoral, popliteal, posterior tibial, dorsalis pedis — the pulse deficits of dissection or peripheral arterial disease). [1]
Presentation template
"I have examined Mrs O'Sullivan's cardiovascular system. At the end of the bed she is diaphoretic and in pain, holding her chest. Her pulse is 96 in sinus rhythm, regular, of normal volume. Her blood pressure is 152 over 94 in the right arm, 138 over 90 in the left. Her JVP is not elevated. Her hands show no stigmata of endocarditis or hyperlipidaemia. Her apex is not displaced and is of normal character. Her heart sounds are normal with no added sounds and no murmurs. Her chest is clear. She has no peripheral oedema and all her peripheral pulses are present and symmetrical. My examination is consistent with an acute coronary syndrome without clinical evidence of heart failure, valvular disease or pericardial involvement. I would now like to review her ECG, which I expect will show the inferior ST elevation, and I would arrange the troponin and the catheter-lab activation." [1]
Discussion questions
Examiner: "What is the significance of the blood-pressure differential between the arms?" [1]
"A differential greater than 20 mmHg between the arms raises the concern for aortic dissection, subclavian stenosis or severe peripheral arterial disease. Mrs O'Sullivan's differential of 14 mmHg is within the range of normal variation (up to 15 mmHg is accepted as normal), and her clinical picture is overwhelmingly cardiac. But I document it, and if the differential were greater than 20 mmHg in a patient with tearing pain, I would proceed to the CT angiogram of the aorta before or alongside the catheter-lab activation. The teaching point is that the blood pressure in both arms is a mandatory part of the chest pain examination — it is the single bedside sign that raises the dissection question, and it is omitted in the majority of assessments." [1]
Examiner: "How would your management change if she had signs of heart failure?" [1]
"If she had pulmonary oedema — bilateral crackles, a gallop rhythm, a raised JVP — her Killip class would be 2 or 3, and her in-hospital mortality would be significantly higher. My management would add cautious oxygen, diuresis (furosemide intravenously), and an assessment of the need for non-invasive ventilation. The primary PCI is still the priority, and the heart failure is managed in parallel. The teaching point is the Killip classification — class 1 (no heart failure), class 2 (basal crackles, S3, raised JVP), class 3 (frank pulmonary oedema), class 4 (cardiogenic shock) — which stratifies the in-hospital mortality from under 5 per cent in class 1 to over 50 per cent in class 4." [1]
Examiner: "What is the single most important lesson from this examination for a registrar managing undifferentiated chest pain?" [1]
"The single most important lesson is that the cardiovascular examination is the discriminator that separates the cardiac from the non-cardiac causes, and that it must be complete — the blood pressure in both arms, the murmurs, the pericardial rub, the signs of heart failure, the DVT signs, and the peripheral pulses. The registrar who examines only the heart sounds in a chest pain patient has examined only a fraction of what is needed. The corollary is the integration — the vital signs, the cardiovascular findings, the respiratory findings and the abdominal findings are not isolated observations but a single picture that, read together, discriminates the deadly six from the benign causes and frames the investigations." [1]
Key DWE MCQ patterns
- Discriminate the cause by the pain character. A tearing interscapular pain with a blood-pressure differential is aortic dissection; a sudden-onset pleuritic pain with hypoxaemia and a normal chest X-ray is PE; a central crushing pain with diaphoresis and ST elevation is STEMI.
- Recognise the STEMI-equivalent. A new left bundle branch block in the right clinical context, the Wellens syndrome ECG, the De Winter T waves and the posterior MI are STEMI-equivalents that trigger the catheter-lab activation.
- Apply the Sgarbossa criteria. The three criteria for infarction in the setting of LBBB — concordant ST elevation, concordant ST depression in V1 to V3, excessively discordant ST elevation.
- Use the HEART score. A score of 0 to 3 allows consideration of early discharge; a score of 7 or more mandates admission for inpatient investigation.
- Interpret the troponin with the clinical context. An elevated troponin in a septic, tachycardic or uraemic patient may be type 2 injury, not infarction.
- Apply the Wells score and the D-dimer for PE. PE unlikely plus negative D-dimer excludes PE without imaging.
- Recognise the atypical presentation. The woman with dyspnoea, the elderly patient with syncope, the diabetic with fatigue — these are ACS until proven otherwise.
- Recognise the deadly six. Every chest pain patient is screened for ACS, PE, dissection, tension pneumothorax, tamponade and oesophageal rupture in the first assessment. [1]
References
[1] Backus BE, Six AJ, Kelder JC, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol 2013;164(3):425–30. The prospective validation of the HEART score in 2440 unselected chest pain patients, showing that a low score (0 to 3) excluded major adverse cardiac events within six weeks with a MACE rate of 1.7 per cent.
[2] Backus BE, Six AJ, Kelder JC, et al. The HEART score for the assessment of patients with chest pain in the emergency department: a multinational validation study. Crit Pathw Cardiol 2013;12(3):115–9. The multinational Asia-Pacific validation of the HEART score in 2906 patients, confirming its utility and showing that it outperformed the TIMI score.
[3] Byrne RA, Rossello X, Coughlan JJ, et al.; ESC Scientific Document Group. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J 2023;44(38):3720–826. The European Society of Cardiology consensus integrating the management of the entire ACS spectrum, embedding the high-sensitivity troponin 0/1h algorithm and framing the invasive strategy and the antithrombotic therapy.
[4] Mueller C, Giannitsis E, Christ M, et al. Multicenter evaluation of a 0-hour/1-hour algorithm in the diagnosis of myocardial infarction with high-sensitivity cardiac troponin T. Ann Emerg Med 2016;68(1):76–87. The multicentre evaluation of the hs-cTnT 0/1h algorithm in 1282 patients, establishing the rule-out, observe and rule-in cutpoints.
[5] Thygesen K, Alpert JS, Jaffe AS, et al.; Executive Group on behalf of the Joint ESC/ACC/AHA/WHF Task Force. Fourth universal definition of myocardial infarction (2018). J Am Coll Cardiol 2018;72(18):2231–64. The global consensus defining the five types of MI and the diagnostic criteria, distinguishing myocardial injury from myocardial infarction.
[6] Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 2000;283(7):897–903. The seminal IRAD study of 464 patients with acute aortic dissection, establishing that the clinical presentation is diverse and the classic physical findings are frequently absent.
[7] Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. N Engl J Med 1996;334(8):481–7. The original Sgarbossa criteria for the ECG diagnosis of acute infarction in LBBB — concordant ST elevation, concordant ST depression in V1 to V3, and excessively discordant ST elevation.
[8] Conte MS, Bradbury AW, Kolh P, et al.; ESC Scientific Document Group. 2024 ESC Guidelines for the management of peripheral arterial and aortic diseases. Eur Heart J 2024;45(38):3925–4020. The European Society of Cardiology consensus on aortic diseases, merging the 2014 aortic diseases guideline and framing the diagnosis and management of aortic dissection.
[9] Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism. Thromb Haemost 2000;83(3):416–20. The Wells clinical prediction rule for PE, with the PE-unlikely and PE-likely dichotomisation.
[10] van Belle A, Buller HR, Huisman MV, et al.; Christopher Study Investigators. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 2006;295(2):172–9. The Christopher study of 3306 patients, validating the Wells plus D-dimer plus CTPA algorithm.
[11] Erbel R, Aboyans V, Boileau C, et al.; ESC Committee for Practice Guidelines. 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J 2014;35(41):2873–926. The 2014 ESC consensus on aortic diseases, defining the Stanford classification and the management of acute aortic syndromes.
Backus et al., Int J Cardiol 2013; Backus et al., Crit Pathw Cardiol 2013; Byrne et al. (ESC ACS), Eur Heart J 2023; Mueller et al. (0/1h troponin), Ann Emerg Med 2016; Thygesen et al. (Fourth Universal Definition), JACC 2018; Hagan et al. (IRAD), JAMA 2000; Sgarbossa et al., NEJM 1996; Conte et al. (ESC Aortic), Eur Heart J 2024; Wells et al., Thromb Haemost 2000; van Belle et al. (Christopher), JAMA 2006; Erbel et al. (ESC Aortic 2014), Eur Heart J 2014; NICE CG95; Heart Foundation of Australia; Therapeutic Guidelines Australia. [1]
References
- [1]Backus BE, Six AJ, Kelder JC, et al. A prospective validation of the HEART score for chest pain patients at the emergency department Int J Cardiol, 2013.PMID 23465250
- [2]Backus BE, Six AJ, Kelder JC, et al. The HEART score for the assessment of patients with chest pain in the emergency department: a multinational validation study Crit Pathw Cardiol, 2013.PMID 23892941
- [3]Byrne RA, Rossello X, Coughlan JJ, et al.; ESC Scientific Document Group 2023 ESC Guidelines for the management of acute coronary syndromes Eur Heart J, 2023.PMID 37622654
- [4]Mueller C, Giannitsis E, Christ M, et al. Multicenter Evaluation of a 0-Hour/1-Hour Algorithm in the Diagnosis of Myocardial Infarction With High-Sensitivity Cardiac Troponin T Ann Emerg Med, 2016.PMID 26794254
- [5]Thygesen K, Alpert JS, Jaffe AS, et al.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018) J Am Coll Cardiol, 2018.PMID 30153967
- [6]Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease JAMA, 2000.PMID 10685714
- [7]Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators N Engl J Med, 1996.PMID 8559200
- [8]Conte MS, Bradbury AW, Kolh P, et al.; ESC Scientific Document Group 2024 ESC Guidelines for the management of peripheral arterial and aortic diseases Eur Heart J, 2024.PMID 39210722
- [9]Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer Thromb Haemost, 2000.PMID 10744147
- [10]van Belle A, Buller HR, Huisman MV, et al.; Christopher Study Investigators Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography JAMA, 2006.PMID 16403929
- [11]Erbel R, Aboyans V, Boileau C, et al.; ESC Committee for Practice Guidelines 2014 ESC Guidelines on the diagnosis and treatment of aortic diseases: Document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC) Eur Heart J, 2014.PMID 25173340