Phys · general-medicine
Undifferentiated Dyspnoea — A Systematic Diagnostic Approach
Also known as dyspnoea · breathlessness · shortness of breath · undifferentiated breathlessness · acute dyspnoea · chronic dyspnoea · respiratory distress · breathing difficulty · diagnostic approach to breathlessness · cardiac versus respiratory dyspnoea · BNP · NT-proBNP · Wells score · two-level PE rule · CURB-65 · Light's criteria · BLUE protocol · A-a gradient
Consultant-physician-depth guide to the diagnostic approach to the patient with breathlessness of unknown cause. Covers the acute-to-chronic time-course framework and its differentials, the focused history and examination discriminators, the first-tier investigations (blood gas, chest X-ray, ECG, NT-proBNP, troponin, D-dimer, FBC, U&E) and second-tier investigations (echo, PFTs, CTPA, V/Q, HRCT, cardiopulmonary exercise testing), the clinical decision rules (two-level Wells score for PE, CURB-65 for pneumonia, Light's criteria for pleural effusion), the BLUE protocol for bedside lung ultrasound, the natriuretic peptide algorithm for cardiac versus respiratory dyspnoea, and the DCE long-case and short-case approach. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Dyspnoea — A Systematic Diagnostic Approach

The answer first
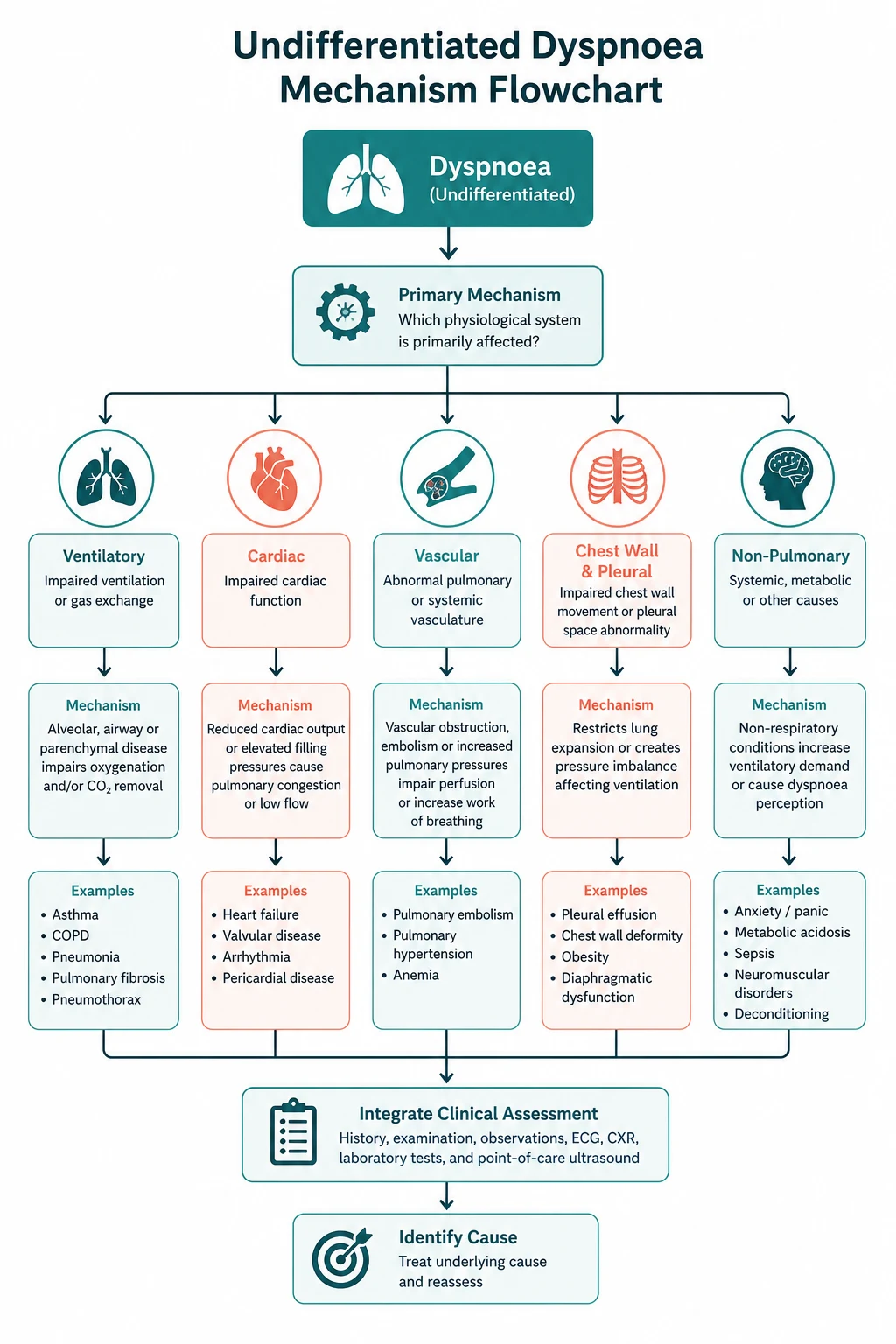
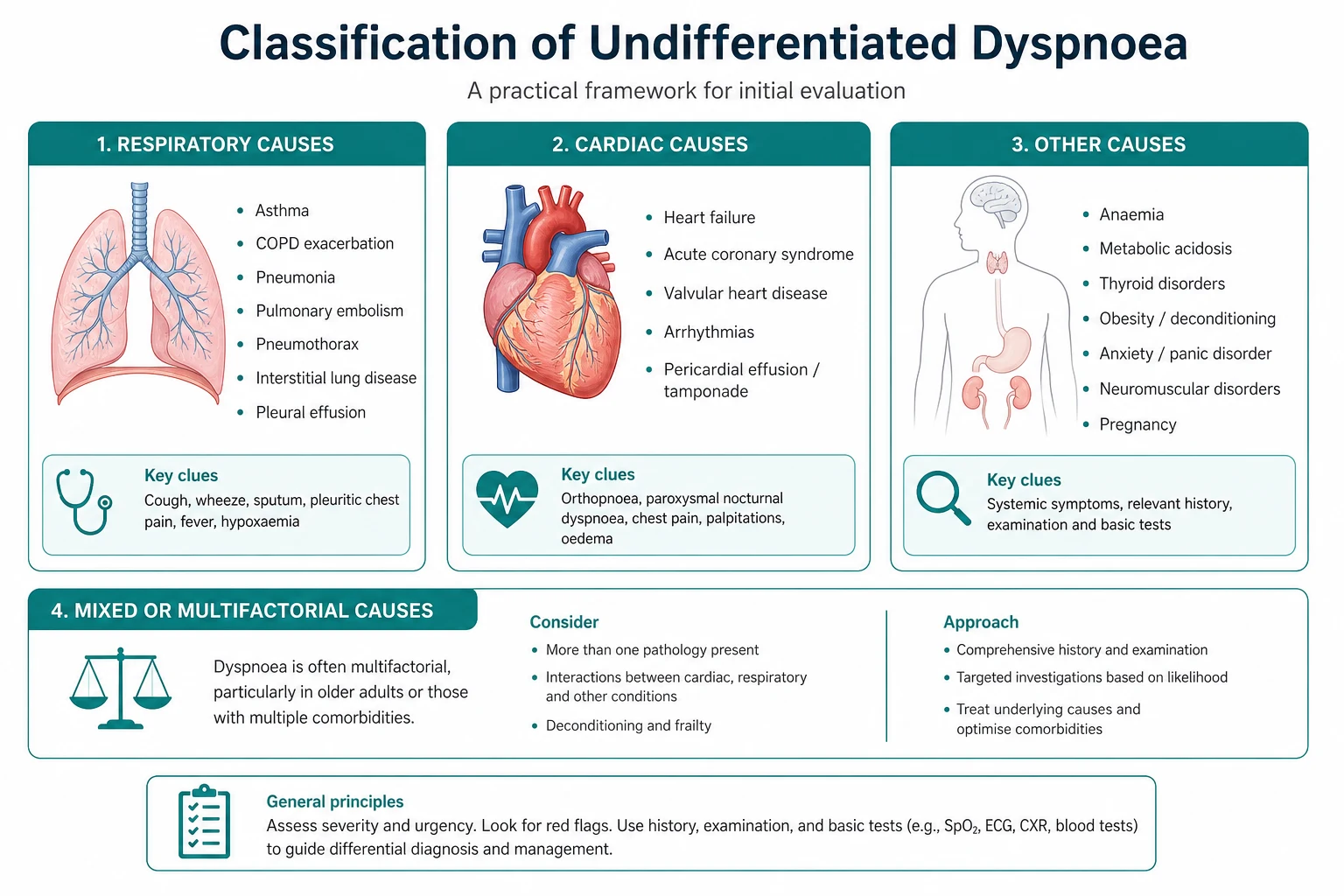
The breathless patient of unknown cause is one of the commonest and most cognitively demanding presentations in internal medicine. The cause spans at least five systems — cardiac, respiratory, metabolic, haematological and neuromuscular — and the first assessment must simultaneously stabilise the patient, generate a prioritised differential, and choose investigations that discriminate rather than confirm a single early guess. The registrar's job is to resist the pull of a premature diagnosis, to use the time course as the primary organising framework, and to let the history, examination and first-tier investigations narrow the differential before committing to a working diagnosis. [1]
The reproducible sequence for any dyspnoeic patient is: [1]
- Stabilise first if acute — ABCDE, high-flow oxygen to the hypoxaemic patient, treat the immediately reversible (anaphylaxis, tension pneumothorax, airway obstruction) before chasing the diagnosis.
- Anchor on the time course — acute (minutes to hours), subacute (hours to days), chronic (weeks to months) — this single axis generates a more useful differential than any other feature.
- Take a focused history — onset, progression, orthopnoea and paroxysmal nocturnal dyspnoea (PND), cough, sputum, haemoptysis, chest pain, leg swelling, travel, smoking, occupation, drug history.
- Examine systematically — respiratory rate and effort first, then the integrated respiratory and cardiovascular examination.
- Order the first-tier investigations — arterial or venous blood gas, chest X-ray, 12-lead ECG, full blood count, urea and electrolytes, troponin, NT-proBNP, D-dimer (if PE is plausible).
- Apply the discriminators — the natriuretic peptide for cardiac versus respiratory, the Wells score for PE, the CURB-65 for pneumonia, Light's criteria for a pleural effusion.
- Tier the second-line investigations — echocardiography, pulmonary function tests, CTPA or V/Q scan, high-resolution CT, cardiopulmonary exercise testing — each chosen by the working diagnosis, not as a blanket work-up. [1]
The single most dangerous error is anchoring on the first plausible diagnosis. The COPD patient who is breathless is assumed to have an exacerbation, when the actual cause may be pulmonary embolism, pneumothorax, pneumonia or acute heart failure — each commoner in COPD than in the general population, and each missed if the registrar stops thinking after "exacerbation." The second error is treating the symptom without the cause — oxygen, positioning and reassurance buy time, but they do not replace a diagnosis. [1]
Viva trap: "What is the single most useful piece of information in the first minute with a breathless patient?" The honest answer is the time course. "Breathless for twenty minutes" is a different patient from "breathless for three weeks," and the differential generated by that single phrase is sharper than any single investigation. The registrar who asks "how long, and how did it start?" before reaching for the stethoscope has organised the entire encounter. [1]
Why the time course is the organising framework

Dyspnoea is defined by the American Thoracic Society as a subjective experience of breathing discomfort consisting of qualitatively distinct sensations that vary in intensity. That definition matters clinically because it reminds us that dyspnoea is what the patient reports — and the first task is to correlate the report with the measurable physiology (respiratory rate, oxygen saturation, blood gas, work of breathing). The patient who reports severe breathlessness with normal observations and a normal gas may have functional dyspnoea; the patient who reports mild breathlessness with a respiratory rate of 36 and an SpO2 of 84 per cent is in respiratory failure regardless of their report. [1]
The time course is the primary organising framework because each time window carries a characteristic differential: [1]
Acute dyspnoea (minutes to hours)
The acute differential is the life-threatening causes that must be identified and treated in the first minutes to hours: [1]
- Acute cardiogenic pulmonary oedema — orthopnoea, PND, bilateral crackles, raised JVP, frothy sputum, often preceded by ischaemic chest pain or a new arrhythmia.
- Pulmonary embolism — sudden-onset pleuritic chest pain and breathlessness, hypoxaemia, a normal or near-normal chest X-ray, risk factors (immobilisation, recent surgery, active cancer, pregnancy, oestrogen).
- Tension pneumothorax — sudden unilateral pleuritic chest pain, breathlessness, hypoxaemia, tracheal deviation, hyper-resonance and reduced breath sounds on the affected side, haemodynamic compromise.
- Severe asthma or COPD exacerbation — wheeze, hyperinflation, accessory muscle use, known history, triggers (infection, allergen, non-adherence, beta-blocker, NSAID).
- Acute myocardial infarction — may present with dyspnoea rather than chest pain, particularly in the diabetic and the elderly.
- Tachyarrhythmia — atrial fibrillation with rapid ventricular response, ventricular tachycardia — palpitation, dyspnoea, haemodynamic compromise depending on rate and underlying cardiac function.
- Anaphylaxis — acute dyspnoea with airway compromise (stridor, laryngeal oedema), circulatory compromise (hypotension) and a rash — give intramuscular adrenaline 0.5 mg immediately.
- Upper airway obstruction — stridor, foreign body, angioedema, infection (epiglottitis, retropharyngeal abscess) — a threatened airway requiring senior airway help before any investigation. [1]
Subacute dyspnoea (hours to days)
The subacute differential is the progressive but not instantaneous causes: [1]
- Pneumonia — fever, productive cough, focal chest signs, consolidation on the chest X-ray; the CURB-65 score stratifies severity.
- Pleural effusion — gradual dyspnoea, dullness to percussion and reduced breath sounds on the affected side; the BTS 2010 guideline frames the investigation of a unilateral effusion with Light's criteria [8].
- COPD exacerbation — increased dyspnoea, sputum volume or purulence over days, often triggered by infection.
- Decompensated heart failure — progressive orthopnoea, bilateral crackles, oedema, raised JVP; the NT-proBNP discriminates this from a respiratory cause [1][2].
- Anaemia — exertional dyspnoea, fatigue, pallor; the onset is often insidious but may present acutely with bleeding or haemolysis.
- Metabolic acidosis — Kussmaul breathing (deep, rapid, sighing respiration) as the body compensates for a metabolic acidosis; the causes are diabetic ketoacidosis, uraemia, lactic acidosis (sepsis, shock, metformin), and salicylate or toxic alcohol toxicity.
Chronic dyspnoea (weeks to months)
The chronic differential is the structural and progressive causes that require a different, tiered work-up: [1]
- COPD — exertional dyspnoea, chronic productive cough, smoking history, irreversible airflow obstruction on spirometry (FEV1 to FVC ratio below 0.7 post-bronchodilator).
- Interstitial lung disease — progressive exertional dyspnoea, dry cough, fine basal crackles (Velcro), finger clubbing in some forms, restrictive defect on pulmonary function tests, characteristic high-resolution CT appearances.
- Chronic heart failure — exertional dyspnoea, orthopnoea, oedema, fatigue; the echocardiogram defines the ejection fraction and the structural abnormality [6][11].
- Pulmonary arterial and chronic thromboembolic pulmonary hypertension — exertional dyspnoea out of proportion to the chest X-ray and spirometry, signs of right heart strain (loud P2, right ventricular heave, raised JVP), and the diagnosis requires echocardiography followed by right heart catheterisation [7].
- Lung cancer — progressive dyspnoea, weight loss, haemoptysis, clubbing, a mass on imaging; may present with a pleural effusion, atelectasis, or post-obstructive pneumonia.
- Neuromuscular weakness — motor neuron disease, myasthenia gravis, Guillain-Barre syndrome, muscular dystrophy, diaphragmatic paralysis — orthopnoea without cardiac or lung pathology, a weak cough, a fall in the forced vital capacity on lying supine, and respiratory failure that may be the presenting feature.
- Deconditioning and obesity — exertional dyspnoea without objective cardiac or respiratory disease, common in the sedentary and the bariatric patient; a diagnosis of exclusion after structural disease is ruled out.
- Functional (anxiety-related) dyspnoea — sighing respiration, a sense of inability to take a deep breath, normal oxygenation and a normal work-up, hyperventilation with a respiratory alkalosis on the blood gas — a diagnosis of exclusion made only after organic disease is confidently ruled out.
DWE high-yield: The single most testable fact about chronic dyspnoea is that pulmonary hypertension and neuromuscular weakness are the diagnoses most often missed, because both may have a normal or near-normal chest X-ray and spirometry in the early stage. The registrar who evaluates chronic exertional dyspnoea with a chest X-ray and spirometry alone, and concludes "no cause found," has not excluded pulmonary hypertension (which needs an echocardiogram) or diaphragmatic weakness (which needs supine spirometry). The corollary is that chronic dyspnoea with a normal chest X-ray and normal spirometry is an indication for an echocardiogram, not a conclusion. [1]
The focused history — the questions that change the differential
The history in dyspnoea is high-yield precisely because each answer narrows the differential. The registrar should ask, in order: [1]
Onset and progression. Sudden onset (seconds to minutes) points to PE, pneumothorax, anaphylaxis, arrhythmia or airway obstruction. Subacute onset (hours to days) points to pneumonia, effusion, COPD exacerbation, decompensated heart failure. Chronic progressive onset (weeks to months) points to COPD, ILD, chronic heart failure, pulmonary hypertension, lung cancer, neuromuscular weakness, anaemia. [1]
Orthopnoea and paroxysmal nocturnal dyspnoea. Orthopnoea (breathlessness lying flat) and PND (waking breathless at night) classically indicate left heart failure — but the registrar must remember that orthopnoea also occurs in diaphragmatic weakness (the diaphragm must work harder against the abdominal contents when supine) and in severe bilateral COPD. The discriminator is the rest of the picture: heart failure gives a raised JVP, bilateral crackles, a gallop and often a murmur; diaphragmatic weakness gives orthopnoea with a weak cough and a fall in FVC supine; COPD gives hyperinflation and wheeze. [1]
Cough, sputum and haemoptysis. A productive cough with purulent sputum points to infection (pneumonia, COPD exacerbation, bronchiectasis). A dry persistent cough points to interstitial lung disease, asthma, gastro-oesophageal reflux, ACE-inhibitor effect, or a pulmonary malignancy. Haemoptysis is a red flag that mandates investigation — the differential includes lung cancer, pulmonary embolism, tuberculosis, pneumonia, bronchiectasis and pulmonary oedema (pink frothy sputum). [1]
Chest pain. Pleuritic chest pain (sharp, worse on inspiration) points to PE, pneumonia, pneumothorax, pericarditis or a pleural effusion. Central pressure-like chest pain points to acute coronary syndrome. Tearing pain radiating to the back points to aortic dissection, which may present with dyspnoea from acute aortic regurgitation, tamponade or stroke. [1]
Leg swelling, travel and immobilisation. These are the Venous thromboembolism risk factors that raise the pre-test probability of PE — recent surgery, immobilisation, active cancer, pregnancy, oestrogen therapy, a long-haul flight, a family history of VTE. [1]
Smoking, occupation and environment. The smoking history quantifies pack-years and frames the COPD and lung cancer risk. The occupational history uncovers the pneumoconioses and hypersensitivity pneumonitis — silica (mining, stonemasonry, sandblasting), asbestos (construction, shipbuilding, plumbing), coal (mining), bird fancier's lung (aviary keepers, pigeon breeders), farmer's lung (mouldy hay). The environmental history may reveal an allergen (occupational asthma) or a carbon monoxide source (faulty heater). [1]
Drug history. The drug history is a high-yield discriminator that is often omitted. Beta-blockers precipitate COPD and asthma exacerbations. NSAIDs cause fluid overload and renal impairment. Amiodarone causes pulmonary toxicity and interstitial pneumonitis. Methotrexate causes pneumonitis. ACE inhibitors cause a dry cough that may be mistaken for dyspnoea. Bleomycin causes pulmonary fibrosis. The patient on a combination of drugs for heart failure with reduced ejection fraction (ACE inhibitor or ARNI, beta-blocker, mineralocorticoid receptor antagonist, SGLT2 inhibitor) is at risk of hyperkalaemia, hypotension and volume depletion that may present as dyspnoea. [1]
The examination — what changes the differential and the urgency
The examination begins at the end of the bed. Before the stethoscope, the registrar gathers the observations that set the urgency and frame the differential. [1]
The end-of-bed observations
The first observations that change the differential and the urgency are: [1]
- Respiratory rate — the single most informative and most neglected vital sign. A respiratory rate above 30 is a sign of severe respiratory distress; a rate below 8 suggests opioid, sedative or neurological depression. A rate in the normal range (12 to 20) in a patient who reports severe dyspnoea should raise the question of functional dyspnoea — but it should never reassure the registrar into inaction in a patient who is objectively unwell.
- Oxygen saturation — a lagging marker. A falling saturation indicates the patient has exhausted respiratory reserve; a normal saturation does not exclude serious disease (the PE patient may have a near-normal saturation at rest and desaturate on exertion).
- Accessory muscle use, tracheal tug and intercostal recession — visible signs of increased work of breathing that indicate significant respiratory distress regardless of the saturation.
- Ability to speak in full sentences — the patient who can speak in full sentences is less acutely distressed than the patient who can manage only one or two words.
- Stridor — an emergency indicating upper airway obstruction; inspiratory stridor suggests an extrathoracic lesion, expiratory stridor an intrathoracic lesion, and biphasic stridor a critical fixed obstruction. Stridor mandates senior airway assessment before any investigation.
- Cyanosis and sweating — signs of severe physiological compromise. [1]
The cardiovascular examination
The cardiovascular examination in dyspnoea is often the discriminator that separates cardiac from respiratory causes: [1]
- Jugular venous pressure — elevated in heart failure, cor pulmonale, pulmonary embolism, cardiac tamponade and superior vena cava obstruction. A raised JVP with bilateral crackles and a third heart sound is the bedside signature of acute decompensated heart failure.
- Apex beat — displaced laterally in dilated cardiomyopathy, volume overload and severe valvular regurgitation; tapping and non-displaced in mitral stenosis; heaving in pressure overload (aortic stenosis, hypertension).
- Murmurs — the systolic murmur of aortic stenosis or mitral regurgitation, the diastolic murmur of aortic or mitral stenosis. A new murmur in the acutely dyspnoeic patient raises the question of acute valve failure (chordal rupture, endocarditis) or a papillary muscle rupture post-infarction.
- Third heart sound (gallop) — the auscultatory hallmark of heart failure with elevated filling pressure.
- Peripheral oedema — a sign of right heart failure, cor pulmonale, or volume overload.
- Signs of pulmonary hypertension — a loud pulmonary component of the second heart sound (P2), a right ventricular heave, a tricuspid regurgitation murmur, a raised JVP with prominent v waves — these point to pulmonary arterial or chronic thromboembolic pulmonary hypertension, which is a commonly missed cause of chronic dyspnoea [7].
The respiratory examination
The respiratory examination systematically maps the chest: [1]
- Chest expansion — reduced bilaterally in COPD and restrictive disease; reduced unilaterally in pleural effusion, consolidation and pneumothorax.
- Percussion — dull in pleural effusion and consolidation; hyper-resonant in pneumothorax and hyperinflation.
- Tactile vocal fremitus and vocal resonance — increased over consolidation (pneumonia), decreased over effusion and pneumothorax.
- Auscultation — wheeze (asthma, COPD, heart failure — the "cardiac wheeze"), crackles (fine and Velcro-like in pulmonary fibrosis and early pulmonary oedema; coarse and bubbling in pneumonia and bronchiectasis), bronchial breathing over consolidation, reduced breath sounds over effusion and pneumothorax, a pleural rub. [1]
The extra-pulmonary examination
The extra-pulmonary signs refine the chronic differential: [1]
- Finger clubbing — lung cancer, pulmonary fibrosis, bronchiectasis, infective endocarditis, congenital cyanotic heart disease, inflammatory bowel disease-associated lung disease.
- Cyanosis — central (warm, hypoxaemic) or peripheral (cold, vasoconstricted).
- Asterixis — a flapping tremor indicating CO2 retention and type 2 respiratory failure.
- Cervical and supraclavicular lymphadenopathy — lung cancer, tuberculosis, lymphoma.
- Signs of connective tissue disease — sclerodactyly and telangiectasia (systemic sclerosis, associated with ILD and pulmonary hypertension), rheumatoid changes, lupus.
- Muscle wasting and fasciculations — motor neuron disease, a neuromuscular cause of dyspnoea that must not be missed. [1]
DCE short-case high-yield: "Examine this patient's respiratory system." The registrar who walks to the chest first has failed the question. The correct routine is hands (clubbing, cyanosis, tremor, asterixis, fine-palmar creases), face (Horner, plethoric, parotid), neck (JVP, trachea, cervical and supraclavicular nodes), then chest (inspection, expansion, percussion, auscultation), then back (expansion, percussion, auscultation), then legs (oedema, DVT signs, deep vein tenderness). The integrated examination that ends with the cardiovascular system when the respiratory findings suggest a cardiac cause is the senior approach the examiner is looking for. [1]
First-tier investigations — the tests that discriminate

The first-tier investigations are the bedside and laboratory tests that discriminate the major categories of dyspnoea within minutes. They are ordered together, interpreted together, and they frame the second-tier work-up. [1]
The blood gas — the highest-yield single test
The arterial blood gas is the highest-yield single investigation in acute dyspnoea because it discriminates: [1]
- Type 1 respiratory failure — PaO2 below 8 kPa (60 mmHg) with a normal or low PaCO2. The causes are V/Q mismatch (pneumonia, pulmonary oedema, PE, COPD with a mild exacerbation), shunt (pneumonia, ARDS, intracardiac shunt), and diffusion impairment (interstitial lung disease).
- Type 2 respiratory failure — PaO2 below 8 kPa with PaCO2 above 6 kPa (45 mmHg). The cause is ventilatory failure — COPD with a severe exacerbation, neuromuscular weakness, opioid or sedative depression, obesity hypoventilation, chest wall deformity.
- Metabolic acidosis with respiratory compensation — a low pH, a low bicarbonate, and a low or low-normal PaCO2 (Kussmaul breathing). The causes are diabetic ketoacidosis, uraemia, lactic acidosis (sepsis, shock, metformin), and toxic alcohol or salicylate toxicity.
- The A-a gradient — the difference between the alveolar and the arterial oxygen tension. A raised A-a gradient (above 2 to 2.5 kPa in a young patient, or above 4 to 5 kPa in an older patient) indicates that the hypoxaemia is of pulmonary origin (V/Q mismatch, shunt, diffusion impairment). A normal A-a gradient with hypoxaemia indicates a non-pulmonary cause (hypoventilation, high altitude). The A-a gradient is the key to separating hypoxaemia of lung disease from hypoxaemia of central hypoventilation. [1]
The venous blood gas is a reasonable surrogate for the arterial gas for pH, PaCO2 and bicarbonate, and it is faster and less painful; the PaO2 on a venous gas is not interpretable and must not be used to assess oxygenation. The registrar who sends only a venous gas in a hypoxaemic patient has not measured the oxygenation. [1]
The chest X-ray — useful but limited
The chest X-ray is the second investigation, and it is useful but limited. It identifies consolidation (pneumonia), pleural effusion, pneumothorax, cardiomegaly and pulmonary oedema, the classical masses of lung cancer, and the hyperinflation of COPD. It is normal in asthma, pulmonary embolism, early pneumonia, pulmonary vascular disease, and many cases of early heart failure — a normal chest X-ray does not exclude serious respiratory disease, and the registrar who is reassured by a normal film in a breathless, hypoxaemic patient has misread the situation. [1]
The 12-lead ECG
The ECG is mandatory in any dyspnoeic patient. It identifies acute coronary syndrome (ST elevation or depression, T wave inversion), arrhythmia (atrial fibrillation with rapid ventricular response, ventricular tachycardia), the right heart strain of pulmonary embolism (S1Q3T3, right bundle branch block, T wave inversion in V1 to V4 — none sensitive, none specific, but suggestive in context), and the tall peaked T waves of hyperkalaemia. [1]
Full blood count, urea and electrolytes
The full blood count identifies anaemia (a cause of exertional dyspnoea and a contributor to acute decompensation), the leukocytosis of infection, and the eosinophilia of asthma or eosinophilic pneumonia. The urea and electrolytes identify renal failure (a cause of metabolic acidosis and fluid overload), and they frame the safety of contrast imaging (CTPA) and diuretic therapy. [1]
Troponin
The troponin identifies myocardial injury. It is elevated in acute coronary syndrome, but it is also elevated in PE, sepsis, heart failure, renal failure and rapid tachyarrhythmia — troponin indicates myocardial injury, not necessarily infarction. The registrar who interprets an elevated troponin in a breathless patient as acute coronary syndrome without weighing the alternatives has misread the biomarker. [1]
NT-proBNP and BNP — the cardiac versus respiratory discriminator

The natriuretic peptides are the single most useful biomarker for distinguishing cardiac from respiratory causes of acute dyspnoea. The B-type natriuretic peptide (BNP) and the N-terminal pro-BNP (NT-proBNP) are released by the cardiac ventricles in response to wall stretch, and their elevation correlates with the severity of heart failure. [1]
The foundational evidence is the Breathing Not Properly study (Maisel and colleagues, 2002), a prospective multicentre study of 1586 patients presenting to the emergency department with acute dyspnoea. BNP was more accurate than any historical, physical or laboratory finding in identifying heart failure as the cause; at a cutoff of 100 pg/mL the diagnostic accuracy was 83.4 per cent, and a BNP below 50 pg/mL had a negative predictive value of 96 per cent for heart failure [1].
The PRIDE study (Januzzi and colleagues, 2005) established the age-stratified NT-proBNP cutpoints that are now standard: [1]
- Rule-out cutpoint (age-independent): NT-proBNP below 300 pg/mL excludes acute heart failure with a high negative predictive value.
- Rule-in cutpoints (age-stratified): NT-proBNP above 450 pg/mL for patients under 50 years; above 900 pg/mL for patients 50 years and older. The age stratification accounts for the rise in natriuretic peptide with age [2].
The 2021 ESC Heart Failure Guidelines and the HFA-ESC practical guidance on natriuretic peptides embed NT-proBNP as the rule-out test in the emergency department dyspnoea pathway — a value below the rule-out cutpoint, in a patient without a high pre-test probability, makes heart failure unlikely and redirects the work-up to respiratory and other causes [6][10].
The false positives and false negatives
The registrar must carry the false positives and false negatives: [1]
- False positives (elevated peptide without heart failure): renal failure (reduced clearance), atrial fibrillation, pulmonary embolism (right heart strain), pulmonary hypertension, sepsis, advanced age. The elevated value in these contexts does not diagnose heart failure — it reflects wall stretch from another cause.
- False negatives (normal peptide with heart failure): obesity (the peptide is diluted in the larger plasma volume and the wall stretch is masked), flash pulmonary oedema (the peptide has not yet risen — the time course of the rise is hours, and a patient who presents within the first hour may have a falsely low value). [1]
The synthesis: the natriuretic peptide is an adjunct to clinical assessment, not a replacement. The value is interpreted in the clinical context — the patient with a raised NT-proBNP, bilateral crackles, a raised JVP and orthopnoea has heart failure; the patient with a raised NT-proBNP, renal failure and a clear chest has an elevated peptide of uncertain significance that does not, by itself, diagnose heart failure. [1]
The D-dimer and the Wells score — the pulmonary embolism pathway
The pulmonary embolism pathway is a paradigm of the diagnostic algorithm in dyspnoea — a clinical prediction rule (the Wells score) sets the pre-test probability, and the D-dimer and imaging (CTPA or V/Q) follow. [1]
The two-level Wells score
The two-level Wells score stratifies the pre-test probability of PE: [1]
| Item | Points |
|---|---|
| Clinical signs and symptoms of DVT (minimum of leg swelling and pain with palpation of the deep veins) | 3 |
| PE is the most likely diagnosis (or equally likely) | 3 |
| Heart rate greater than 100 beats per minute | 1.5 |
| Immobilisation for at least 3 days, or surgery in the previous 4 weeks | 1.5 |
| Previous, objectively diagnosed deep vein thrombosis or PE | 1.5 |
| Haemoptysis | 1 |
| Malignancy (on treatment, treated in the last 6 months, or palliative) | 1 |
The two-level interpretation: PE unlikely (score 4 or less) and PE likely (score more than 4) [3]. The single highest-weighted subjective item — "PE is the most likely diagnosis" — determines which limb the patient enters, and the registrar who miscalculates this item has misclassified the patient.
The diagnostic algorithm
The validated algorithm (the Christopher study, van Belle and colleagues, 2006 — a prospective cohort of 3306 patients) combines the Wells score with D-dimer and CTPA [4]:
- PE unlikely plus a negative D-dimer — PE is excluded without imaging. The 3-month incidence of symptomatic VTE in this group was 0.5 per cent.
- PE likely, or PE unlikely with a positive D-dimer — proceed to CTPA. [1]
The age-adjusted D-dimer (cutoff equals age multiplied by 10 in micrograms per litre for patients over 50) increases the proportion of patients in whom PE can be excluded without imaging, particularly in the older patient in whom a fixed cutoff of 500 micrograms per litre is rarely normal. [1]
The D-dimer traps
The D-dimer is a rule-out test, not a rule-in test. The traps are: [1]
- Ordering a D-dimer in a patient with a high pre-test probability of PE — it will be positive and the test adds nothing; the patient should proceed directly to CTPA.
- Interpreting a positive D-dimer as confirming PE — the D-dimer is elevated in almost any inflammatory, infectious, malignant, postoperative, traumatic or pregnancy state; it is sensitive but not specific.
- Using the D-dimer in a patient in whom it is universally elevated — postoperative, malignancy, active infection, pregnancy — where it cannot exclude PE. [1]
CURB-65 and Light's criteria — the pneumonia and pleural effusion rules
CURB-65 for community-acquired pneumonia
The CURB-65 score (Lim and colleagues, 2003, derived and validated in an international study of community-acquired pneumonia) stratifies severity and guides the site of care [5]. One point each for:
- Confusion (new — mental test score 8 or less, or new disorientation)
- Urea greater than 7 mmol/L [1]- Respiratory rate 30 or more per minute
- Blood pressure — systolic below 90 or diastolic 60 or below
- 65 — age 65 or older [1]
The risk stratification: [1]
- Score 0 to 1 — low mortality; consider outpatient management.
- Score 2 — moderate mortality; hospital admission.
- Score 3 or more — high mortality; consider ICU admission. [1]
Light's criteria for pleural effusion
The investigation of a pleural effusion is framed by the BTS 2010 guideline (Hooper and colleagues) and by Light's criteria [8]. An effusion is an exudate if any one of the following is met:
- Pleural fluid protein to serum protein ratio greater than 0.5
- Pleural fluid LDH to serum LDH ratio greater than 0.6
- Pleural fluid LDH greater than two-thirds of the upper limit of normal for serum LDH [1]
If none is met, the effusion is a transudate. The transudates are caused by heart failure, cirrhosis, nephrotic syndrome, hypoalbuminaemia and constrictive pericarditis; the exudates by infection, malignancy, pulmonary embolism, autoimmune disease and pancreatitis. [1]
The false-positive exudate — a transudate that meets the Light's criteria because the patient is on diuretics (the diuresis concentrates the pleural fluid protein and LDH) — is reclassified by the serum-to-pleural-fluid albumin gradient: a gradient greater than 1.2 g per dL indicates a transudate despite the Light's criteria. [1]
Exam trap — the GALLINI myth: A candidate may be asked about a "GALLINI score" for pleural effusion. There is no GALLINI score. The validated criterion for the transudate versus exudate classification is Light's criteria, with the serum-to-pleural-fluid albumin gradient as the rescue test for the false-positive exudate in diuretic-treated heart failure. A candidate who cites GALLINI in a viva has revealed a knowledge gap; the correct answer is Light's criteria. [1]
The BLUE protocol and bedside ultrasound
The BLUE protocol (Lichtenstein and Meziere, 2008) demonstrated that a standardised bedside lung ultrasound protocol achieved a diagnostic accuracy of 90.5 per cent in the acute respiratory failure patient [9]. The protocol uses the lung artefacts and real findings — lung sliding, A-lines, B-lines (also called lung rockets), alveolar consolidation and pleural effusion — to generate profiles that map to the common causes:
- The A-profile (A-lines with lung sliding on the anterior chest) suggests asthma, COPD or pulmonary embolism. The addition of a deep venous thrombosis on the leg compression ultrasound makes the "A-profile plus DVT" the signature of PE.
- The B-profile (multiple bilateral B-lines with lung sliding) suggests cardiogenic pulmonary oedema. The loss of lung sliding with B-lines suggests pneumonia or interstitial syndrome of another cause.
- The A or B profile with abolished lung sliding and a lung point diagnoses pneumothorax.
- The C-profile (anterior alveolar consolidation) suggests pneumonia. [1]
The value of the BLUE protocol is that it brings a bedside, repeatable, radiation-free assessment to the dyspnoeic patient in the first minutes, and it sharpens the early differential before the chest X-ray and the blood gas are back. The focused cardiac ultrasound, performed at the same bedside assessment, adds the left ventricular function, the right ventricular size (dilatation in PE), the pericardial effusion, and the inferior vena cava collapsibility as a marker of volume status. The registrar trained in point-of-care ultrasound has a diagnostic advantage in the acute dyspnoeic patient that is difficult to overstate. [1]
Management principles — stabilise, diagnose, treat the cause
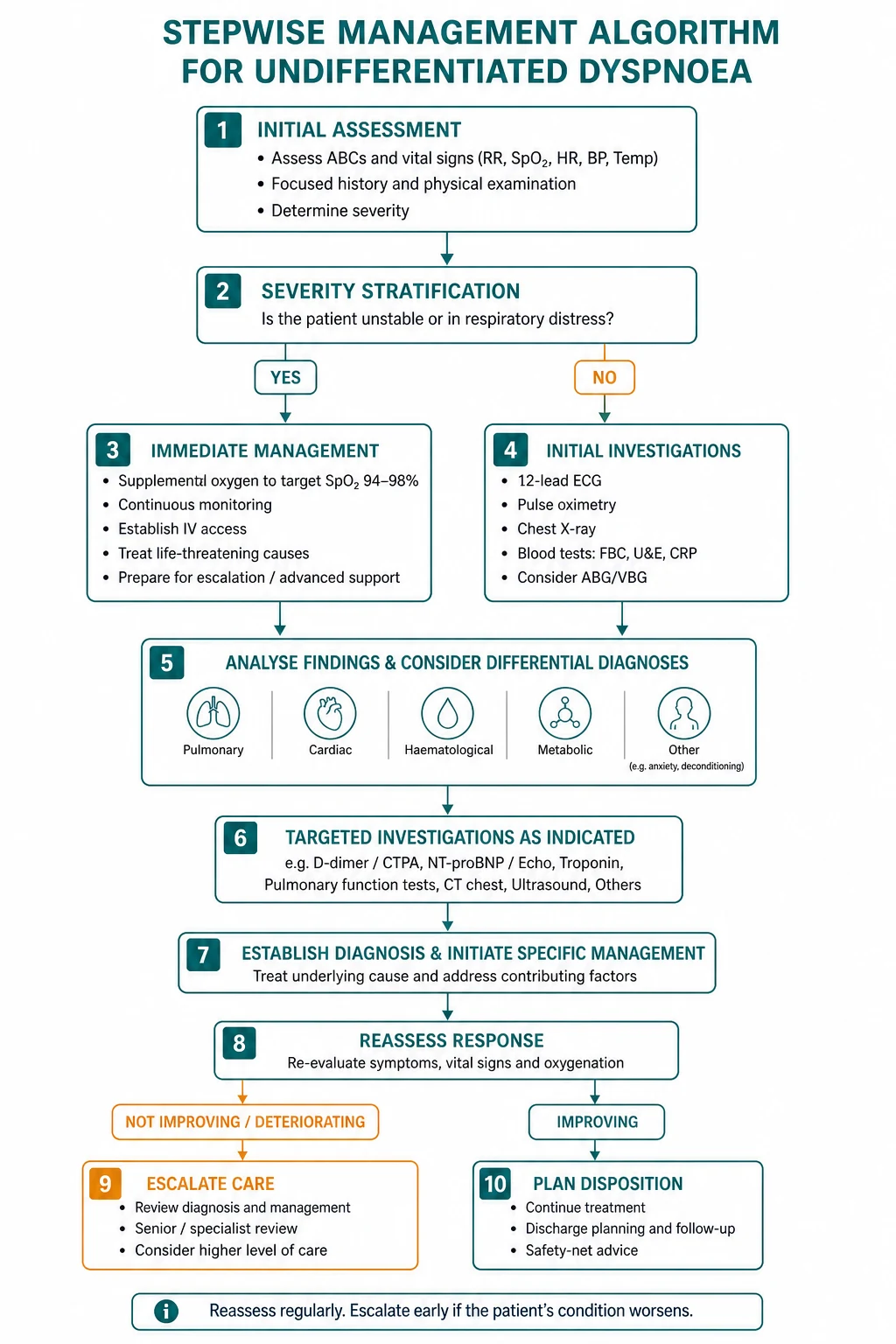
The management of undifferentiated dyspnoea follows the same sequence as the diagnostic approach — stabilise first, then treat the cause. The principles: [1]
Oxygen therapy. Give high-flow oxygen via a reservoir mask at 15 L per minute to the hypoxaemic, critically ill patient, and titrate down to a target saturation of 94 to 98 per cent (or 88 to 92 per cent for the known or at-risk chronic CO2 retainer). The common error is to under-oxygenate the critically ill patient for fear of CO2 retention — the risk of CO2 retention in an unknown patient is far smaller than the risk of prolonged hypoxaemia. The corollary: check a blood gas within 30 to 60 minutes of starting oxygen in the patient at risk of hypercapnia. [1]
Positioning. Sit the patient upright to reduce the work of breathing and the venous return; this single manoeuvre relieves orthopnoea in the heart failure patient and improves the mechanical advantage of the diaphragm in the COPD patient. [1]
Non-invasive ventilation. Indicated in cardiogenic pulmonary oedema (CPAP or bilevel positive airway pressure, which reduce the work of breathing and the afterload), in COPD with type 2 respiratory failure and a pH below 7.35 (bilevel, which improves the ventilatory failure and the acidosis), and in the immunocompromised patient with hypoxaemic respiratory failure (early NIV reduces intubation and mortality). [1]
Treat the cause. The diuresis, vasodilator and inotrope for acute heart failure; the antibiotics for pneumonia (the CURB-65 guides the site of care and the antibiotic choice); the bronchodilators and corticosteroids for asthma and COPD exacerbation; the therapeutic anticoagulation for PE; the needle decompression for tension pneumothorax; the adrenaline for anaphylaxis. The registrar who has stabilised the patient but not identified and treated the cause has bought time, not solved the problem. [1]
Symptom relief at the end of life. The patient with end-stage COPD, heart failure, ILD or lung cancer may benefit from opioids (low-dose morphine or oxycodone for the sensation of breathlessness), benzodiazepines (for the anxiety component), and oxygen (for the hypoxaemic symptom, with the recognition that oxygen relieves the symptom more than the physiology in the chronically hypoxaemic patient). The decision to focus on symptom relief rather than escalation is a ceiling-of-care decision made with the patient and family, documented and communicated. [1]
Regional guideline anchoring
The guidelines that frame the work-up of dyspnoea converge across regions, with local deltas the registrar must carry: [1]
- The 2021 ESC Heart Failure Guidelines (McDonagh and colleagues) embed NT-proBNP as the rule-out test for heart failure in the dyspnoea pathway, define the HFrEF, HFmrEF and HFpEF phenotypes by the ejection fraction, and frame the four pillars of HFrEF therapy (ACE inhibitor or ARNI, beta-blocker, mineralocorticoid receptor antagonist, SGLT2 inhibitor) [6]. The Universal Definition of Heart Failure (Bozkurt and colleagues, 2021) defines heart failure as a clinical syndrome with symptoms and signs caused by a structural or functional cardiac abnormality and corroborated by an elevated natriuretic peptide and objective evidence of pulmonary or systemic congestion [11].
- The 2022 ESC/ERS Pulmonary Hypertension Guidelines (Humbert and colleagues) frame the work-up of suspected pulmonary hypertension — echocardiography as the screening test, right heart catheterisation for confirmation — and define the haemodynamic and clinical classification that guides management [7].
- The BTS Pleural Disease Guideline (Hooper and colleagues, 2010, updated 2023) frames the investigation of a unilateral pleural effusion — the role of the history, the imaging, the diagnostic aspiration, and the application of Light's criteria [8].
- ANZ primary: the Heart Foundation of Australia heart failure guidance, the TSANZ position papers on COPD and ILD, and the Australian Asthma Handbook. UK secondary: the NICE guidelines on heart failure (NG106), pneumonia (CG191), and COPD (NG115), and the BTS and SIGN guidelines. US tertiary: the ACC/AHA heart failure guideline, the ATS guidelines on COPD and ILD, and the IDSA/ATS guidelines on community-acquired pneumonia.
The regional delta the registrar must carry: the principles converge (use NT-proBNP to rule out heart failure, use the Wells score and D-dimer for PE, use CURB-65 for pneumonia, use Light's criteria for the effusion), but the specific cutpoints and the institutional pathways differ — the registrar confirms the local pathway on arrival at a new hospital. [1]
DCE long-case approach
Patient scenario
Mr Robert Chen, 72, retired engineer, presents to the emergency department with two days of worsening breathlessness, a productive cough with yellow sputum, and orthopnoea. He has a background of COPD (FEV1 50 per cent predicted), ischaemic heart disease (prior NSTEMI five years ago, currently on aspirin, atorvastatin, bisoprolol, ramipril), type 2 diabetes (metformin), and hypertension. He smoked 40 pack-years and stopped five years ago. He lives with his wife and is normally independent, walking 200 metres on the flat before stopping with breathlessness. [1]
On assessment: respiratory rate 28, SpO2 88 per cent on room air rising to 93 per cent on 4 L via nasal cannulae, temperature 38.2, heart rate 108 in atrial fibrillation, blood pressure 144/88, JVP raised 4 cm above the sternal angle, bilateral expiratory wheeze and fine basal crackles, peripheral oedema to the mid-shin. Chest X-ray shows hyperinflated lung fields, increased bronchovascular markings, and no focal consolidation. ECG shows atrial fibrillation at 108 with no acute ischaemic changes. NT-proBNP 1800 pg/mL. Troponin 45 ng/L (upper limit of normal 14). Haemoglobin 132. Urea 9.2, creatinine 130 (baseline 110). D-dimer 1200 micrograms per litre. CURB-65 is 2 (respiratory rate, urea). [1]
Candidate's opening statement (SASPOP)
"Mr Chen is a 72-year-old retired engineer presenting with two days of worsening breathlessness, a productive cough and orthopnoea, on a background of COPD, ischaemic heart disease, type 2 diabetes and hypertension. He is a 40-pack-year ex-smoker. His main problems are an acute respiratory deterioration that is most likely an infective COPD exacerbation with a coexisting cardiac component suggested by the raised JVP, fine basal crackles, the new atrial fibrillation and the NT-proBNP of 1800; he also has a raised troponin that may be type 2 myocardial injury from the tachyarrhythmia and the respiratory distress. My immediate priorities are the ABCDE assessment with controlled oxygen targeting 88 to 92 per cent given his COPD, an arterial blood gas to assess for hypercapnia, nebulised bronchodilators and systemic corticosteroids for the COPD exacerbation, antibiotics for the suspected infection, and a careful diuresis for the cardiac component while I discriminate the relative contributions of the COPD, the heart failure and the infection." [1]
Problem list
- Acute COPD exacerbation with possible coexisting decompensated heart failure — wheeze, crackles, raised JVP, raised NT-proBNP.
- New atrial fibrillation with a moderately rapid ventricular response — likely secondary to the acute illness; rate control rather than rhythm control initially.
- Type 2 myocardial injury — the raised troponin is from demand ischaemia in the context of the tachyarrhythmia and respiratory distress, not necessarily an acute coronary syndrome.
- The raised D-dimer — non-specific in this context (infection, atrial fibrillation, COPD); the pre-test probability of PE is moderate, and PE cannot be excluded without imaging if clinically suspected.
- Multimorbidity and polypharmacy — the bisoprolol may be contributing to the COPD exacerbation; the ramipril and the bisoprolol require review with the new AF and the troponin rise. [1]
Integrated management plan
The management is cause-specific and integrated — the COPD exacerbation and the heart failure are treated in parallel, and the relative contributions are weighed at each reassessment: [1]
- ABCDE with controlled oxygen — target SpO2 88 to 92 per cent given the COPD; check an arterial blood gas within 30 to 60 minutes for hypercapnia and acidosis. Sit him upright.
- Bronchodilators and corticosteroids — salbutamol 5 mg and ipratropium 500 micrograms nebulised, repeated as needed; prednisone 50 mg daily for five days (or hydrocortisone 100 mg intravenously if he cannot take oral). [1]3. Antibiotics — a COPD exacerbation with increased sputum purulence and volume warrants antibiotics; amoxicillin-clavulanate 875/125 mg twice daily (or doxycycline 100 mg daily if penicillin-allergic), guided by the local guideline and the sputum culture.
- Diuresis for the cardiac component — furosemide 40 mg intravenously, with reassessment of the response (a fall in JVP, a reduction in the crackles, an improvement in the oxygenation and the dyspnoea). The diuresis is cautious given the COPD (over-diuresis dries the secretions and worsens the work of breathing) and the renal function.
- Rate control for the atrial fibrillation — a beta-blocker is relatively contraindicated in the COPD exacerbation; the options are digoxin or a rate-limiting calcium-channel blocker (diltiazem), with the recognition that the AF is likely to settle as the acute illness is treated. Anticoagulate once the acute phase is resolving, weighing the CHA2DS2-VASc and the HAS-BLED.
- Review the cardiac biomarkers — repeat the troponin at 3 hours; if it is stable or falling, the type 2 myocardial injury interpretation is supported; if it is rising dynamically, investigate for an acute coronary syndrome.
- Reassess the PE question — the D-dimer is unhelpful in this context; the clinical assessment (pleuritic chest pain, leg swelling, risk factors) determines whether CTPA is warranted. If the clinical picture does not settle with the above therapy, CTPA excludes PE.
- Review the drug chart — the bisoprolol may be reduced or held during the exacerbation, with a plan to reintroduce; the ramipril is continued unless the renal function or the potassium contraindicate it; the metformin is continued unless he becomes hypoxic or the renal function deteriorates. [1]
Examiner probing questions and model answers
Q1: "His NT-proBNP is 1800. How does that change your management?" [1]
"The NT-proBNP of 1800 is above the PRIDE rule-in cutpoint for a patient over 50 (greater than 900 pg/mL), which supports the clinical diagnosis of heart failure as a contributor to this presentation [2]. But I interpret it in the clinical context — he has COPD, atrial fibrillation and an acute infection, all of which can elevate the peptide, and the value does not by itself distinguish how much of his dyspnoea is heart failure and how much is COPD. The value confirms that there is a cardiac component, and it shifts my management towards a cautious diuresis alongside the bronchodilator and corticosteroid therapy. The trap to avoid is treating the number rather than the patient — the diuresis is titrated to the clinical response, not to a target NT-proBNP."
Q2: "How do you decide how much of his breathlessness is COPD and how much is heart failure?" [1]
"I do not try to separate them at the first assessment — I treat both in parallel and I reassess. The COPD component is addressed with the controlled oxygen, the bronchodilators and the corticosteroids; the cardiac component is addressed with the cautious diuresis. The reassessment at 30 to 60 minutes tells me which is responding — if the wheeze improves and the saturations rise with the bronchodilator, the COPD component was dominant; if the JVP falls and the crackles reduce with the diuresis, the cardiac component was significant. In the patient with COPD and heart failure, the two are often coexistent and mutually exacerbating, and the integrated management — treating both — is safer than forcing a single diagnosis at the cost of missing the other." [1]
Q3: "He is in atrial fibrillation at 108. Do you cardiovert?" [1]
"No. The AF is almost certainly secondary to the acute illness — the infection, the hypoxia, the sympathetic surge, the electrolyte disturbance — and it will usually settle as the acute illness is treated. He is haemodynamically stable, so there is no indication for synchronised DC cardioversion. My approach is rate control with a drug that does not worsen the COPD — a beta-blocker is relatively contraindicated in the exacerbation, so I would use digoxin or a rate-limiting calcium-channel blocker such as diltiazem, with the recognition that the rate will often settle as the underlying illness improves. I would anticoagulate him once the acute phase is resolving, because the new AF carries a stroke risk and his CHA2DS2-VASc is high. The teaching point is the order: treat the cause of the AF, not the AF itself, and reserve specific antiarrhythmic therapy for the AF that persists or that is itself the haemodynamic problem." [1]
Q4: "His troponin is 45. Is this an acute coronary syndrome?" [1]
"Not necessarily. The troponin is elevated, which indicates myocardial injury — but the injury may be type 2 (demand ischaemia from the tachyarrhythmia, the hypoxia, the respiratory distress, and the sympathetic surge) rather than type 1 (a plaque rupture with thrombosis). The discriminator is the dynamic rise and fall of the troponin and the clinical and ECG context. I would repeat the troponin at 3 hours; if it is stable or falling, the type 2 interpretation is supported and I manage the underlying illness; if it is rising dynamically with chest pain or ischaemic ECG changes, I investigate for an acute coronary syndrome. The trap is interpreting a single elevated troponin in a breathless, tachycardic patient as an acute coronary syndrome and activating the catheter lab without weighing the type 2 alternative." [1]
Q5: "How would you investigate him for pulmonary embolism?" [1]
"The D-dimer is unhelpful here — it is elevated by the infection, the COPD and the atrial fibrillation, and it cannot exclude PE. I use the clinical assessment: does he have pleuritic chest pain, leg swelling, immobility, or a history of VTE? If the clinical picture is consistent with PE, I proceed to CTPA; if the clinical picture is not consistent and the patient is settling with the above therapy, I do not pursue PE. If the patient is not settling — if the hypoxaemia or the tachycardia persists despite the bronchodilators, the corticosteroids, the antibiotics and the diuresis — I reconsider PE and proceed to CTPA. The Wells score is a guide, not a substitute for clinical judgement, and the 'PE is the most likely diagnosis' item is the one I weigh most heavily." [1]
Q6: "What is your plan for his long-term management after this admission?" [1]
"The admission is an opportunity to optimise both the COPD and the heart failure, and to address the factors that precipitated the deterioration. For the COPD, I confirm the inhaler technique and the adherence, I optimise the dual bronchodilation, I enrol him in pulmonary rehabilitation, I check his vaccination status (influenza, pneumococcal, COVID-19), and I assess him for long-term oxygen therapy if he is chronically hypoxaemic. For the heart failure, I optimise the four pillars of HFrEF therapy if his echo shows a reduced ejection fraction — the bisoprolol, the ramipril (or an ARNI), a mineralocorticoid receptor antagonist, and an SGLT2 inhibitor — and I arrange follow-up echocardiography and a cardiology review. For the atrial fibrillation, I formalise the anticoagulation and the rate or rhythm strategy. And I address the smoking (he has stopped, but I reinforce), the nutrition, and the advance care planning — a patient with COPD and heart failure should have an early conversation about the goals of care and the ceiling of treatment, so that the next deterioration is met with a plan, not a crisis." [1]
DCE short-case discussion: the respiratory examination
Instruction: "Examine this patient's respiratory system." [1]
Systematic examination routine
- End of the bed — the look test. Is the patient in distress? Are they breathing comfortably, using accessory muscles, or see-saw breathing? Is the colour normal, pale, cyanosed, plethoric? Is the conscious level appropriate? Is there a cough, a wheeze audible from the end of the bed? Are there clues in the surroundings — oxygen, inhalers, a nebuliser, sputum pot?
- Hands — clubbing (lung cancer, pulmonary fibrosis, bronchiectasis, infective endocarditis), peripheral cyanosis, fine tremor (beta-agonist), asterixis (CO2 retention), palmar erythema and Dupuytren contracture (the patient with liver disease and a hepatic hydrothorax or hepatopulmonary syndrome).
- Face — Horner syndrome (apical lung tumour, Pancoast), plethoric facies (polycythaemia), parotid enlargement (sarcoid, bulimia, alcohol), nasal polyps (asthma, cystic fibrosis), cyanosis of the lips.
- Neck — JVP (elevated in heart failure, cor pulmonale, PE, tamponade), tracheal position (central; deviated away from a pneumothorax, effusion or mass; deviated towards a collapse or fibrosis), cricosternal distance (reduced in hyperinflation), cervical and supraclavicular lymphadenopathy (lung cancer, tuberculosis).
- Chest inspection — symmetry, scars (thoracotomy, drains), radiotherapy tattoos, deformity (pectus excavatum, kyphoscoliosis), paradoxical breathing (diaphragmatic weakness), the intercostal recessions and the accessory muscle use.
- Chest expansion — anterior and posterior, measured at the level of the fourth intercostal space; reduced bilaterally in COPD and restrictive disease, unilaterally in effusion, consolidation and pneumothorax.
- Percussion — dull in effusion and consolidation; stony dull in a large effusion; hyper-resonant in pneumothorax and hyperinflation.
- Auscultation — breath sounds (vesicular or bronchial), added sounds (wheeze, crackles — fine versus coarse — pleural rub), vocal resonance (increased over consolidation, decreased over effusion and pneumothorax).
- Back — repeat the percussion and auscultation posteriorly; check for sacral oedema.
- Legs — peripheral oedema (right heart failure, cor pulmonale), deep vein thrombosis signs (calf swelling, tenderness, warmth — the source of the PE), peripheral cyanosis. [1]
Presentation template
"I have examined Mr Chen's respiratory system. At the end of the bed he is breathless at rest, using accessory muscles, with an audible wheeze and a productive cough. His respiratory rate is 28, his oxygen saturation is 88 per cent on room air. His hands show no clubbing, no cyanosis, no asterixis. The JVP is raised 4 cm. The trachea is central. The chest is hyperinflated with reduced expansion bilaterally. Percussion is resonant bilaterally. Auscultation reveals bilateral expiratory wheeze and fine basal crackles. There is peripheral oedema to the mid-shin. My findings are consistent with an acute COPD exacerbation with a coexisting cardiac component, suggested by the raised JVP, the fine crackles and the oedema. I would now like to examine the cardiovascular system to characterise the cardiac contribution — specifically the apex, the murmurs, and the heart sounds." [1]
Discussion questions
Examiner: "What is the significance of the fine versus the coarse crackles?" [1]
"The fine, late-inspiratory, Velcro-like crackles suggest interstitial lung disease or early pulmonary oedema — the opening of small airways and alveoli that have been stuck together by surfactant deficiency or fluid. The coarse, bubbling, mid-inspiratory crackles suggest pneumonia or bronchiectasis — the movement of secretions in the larger airways. The crackles that clear with coughing are secretions; the crackles that persist are parenchymal. In a patient with COPD and heart failure, the fine basal crackles are more consistent with the pulmonary oedema than with the COPD itself, which is why they shift my differential towards the cardiac component." [1]
Examiner: "How would you investigate this patient further?" [1]
"The first-tier investigations I have already — the chest X-ray, the ECG, the bloods, the NT-proBNP and the troponin. The next step is the arterial blood gas, given his COPD and the risk of hypercapnia — I want to know the PaCO2 and the pH to assess for type 2 respiratory failure. If the gas shows hypercapnia with a low pH, he is in acute type 2 respiratory failure and I consider non-invasive ventilation. The echocardiogram, once he is stabilised, defines the ejection fraction and the structural abnormality, and it discriminates the HFrEF from the HFpEF phenotype — which changes the long-term management. The pulmonary function tests, once he is recovered, confirm the COPD severity and the response to bronchodilator. If the dyspnoea does not settle with the therapy, I reconsider the differential — PE with a CTPA, and a high-resolution CT if I am concerned about interstitial lung disease." [1]
Examiner: "What is the single most important lesson from this patient for a registrar managing undifferentiated dyspnoea?" [1]
"The single most important lesson is to resist the anchoring error. Mr Chen has COPD, and the easy diagnosis is an exacerbation — but the actual picture is a COPD exacerbation with a coexisting heart failure component, a new atrial fibrillation, a type 2 myocardial injury, and a possible PE that the D-dimer cannot exclude. The registrar who stops at 'exacerbation' and treats only with bronchodilators and corticosteroids has missed the cardiac component, the AF, the troponin rise, and the PE question. The integrated approach — the time-course framework, the focused history, the systematic examination, the first-tier investigations interpreted together, and the parallel management of the competing diagnoses — is what keeps the complex dyspnoeic patient safe. The corollary is the reassessment: the patient who is not settling at 30 to 60 minutes is not failing the therapy, he is telling me that my working diagnosis is incomplete, and I need to reconsider." [1]
Key DWE MCQ patterns
- Discriminate the cause by the time course. A sudden-onset dyspnoea with a normal chest X-ray and hypoxaemia is PE until proven otherwise; a subacute dyspnoea with fever and consolidation is pneumonia; a chronic progressive dyspnoea with fine crackles and clubbing is interstitial lung disease.
- Apply the NT-proBNP cutpoints. A patient under 50 with an NT-proBNP above 450 has heart failure; a patient over 50 with an NT-proBNP above 900 has heart failure; a patient of any age with an NT-proBNP below 300 does not have acute heart failure (PRIDE rule-out).
- Apply the Wells score and the D-dimer algorithm. A patient with a Wells score of 4 or less and a negative D-dimer has PE excluded; a patient with a Wells score above 4 proceeds to CTPA without a D-dimer.
- Interpret the troponin in context. An elevated troponin in a breathless, tachycardic patient is type 2 myocardial injury until proven otherwise — do not automatically activate the catheter lab.
- Recognise the false-positive D-dimer. A positive D-dimer in a postoperative, malignant, pregnant or septic patient does not diagnose PE; the test is a rule-out, not a rule-in.
- Apply the CURB-65 for pneumonia. A score of 3 or more warrants consideration of ICU admission; a score of 0 or 1 may be managed as an outpatient.
- Recognise the GALLINI myth. There is no GALLINI score for pleural effusion; the validated criterion is Light's criteria, with the serum-to-pleural-fluid albumin gradient as the rescue test.
- Recognise the missed diagnoses in chronic dyspnoea. Pulmonary hypertension and neuromuscular weakness are missed when the work-up is limited to a chest X-ray and spirometry — a normal chest X-ray and normal spirometry in chronic dyspnoea is an indication for an echocardiogram and, if indicated, supine spirometry.
- Do not under-oxygenate the critically ill patient. Give high-flow oxygen to the hypoxaemic, critically ill patient and titrate down; the fear of CO2 retention does not justify prolonged hypoxaemia. [1]
References
[1] Maisel AS, Krishnaswamy P, Nowak RM, et al.; Breathing Not Properly Multinational Study Investigators. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002;347(3):161–7. The foundational study of 1586 patients with acute dyspnoea, showing that BNP at a cutoff of 100 pg/mL had a diagnostic accuracy of 83.4 per cent for heart failure, and that a BNP below 50 pg/mL had a negative predictive value of 96 per cent.
[2] Januzzi JL Jr, Camargo CA, Anwaruddin S, et al. The N-terminal pro-BNP investigation of dyspnea in the emergency department (PRIDE) study. Am J Cardiol 2005;95(8):948–54. The PRIDE study, establishing the age-stratified NT-proBNP rule-in cutpoints (greater than 450 pg/mL under 50; greater than 900 pg/mL over 50) and the age-independent rule-out cutpoint (less than 300 pg/mL).
[3] Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer. Thromb Haemost 2000;83(3):416–20. The derivation of the Wells clinical prediction rule for PE, with the dichotomised PE unlikely (4 or less) and PE likely (more than 4) interpretation.
[4] van Belle A, Buller HR, Huisman MV, et al.; Christopher Study Investigators. Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA 2006;295(2):172–9. The Christopher study of 3306 patients, validating the algorithm of Wells dichotomisation plus D-dimer plus CTPA, with a 3-month VTE incidence of 0.5 per cent in the PE-unlikely plus negative D-dimer group.
[5] Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study. Thorax 2003;58(5):377–82. The derivation and validation of the CURB-65 score, stratifying community-acquired pneumonia mortality and guiding the site of care.
[6] McDonagh TA, Metra M, Adamo M, et al.; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42(36):3599–726. The European Society of Cardiology consensus on heart failure, embedding NT-proBNP in the dyspnoea pathway and defining the HFrEF, HFmrEF and HFpEF phenotypes and the four pillars of therapy.
[7] Humbert M, Kovacs G, Hoeper MM, et al.; ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022;43(38):3618–731. The ESC and ERS consensus on pulmonary hypertension, framing the echocardiographic screening and the right heart catheterisation confirmation that frame the work-up of the missed cause of chronic dyspnoea.
[8] Hooper C, Lee YCG, Maskell N; BTS Pleural Guideline Group. Investigation of a unilateral pleural effusion in adults: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010;65(Suppl 2):ii4–ii17. The BTS guidance on the investigation of a unilateral pleural effusion, including the application of Light's criteria.
[9] Lichtenstein DA, Meziere GA. Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol. Chest 2008;134(1):117–25. The BLUE protocol, demonstrating a 90.5 per cent diagnostic accuracy for a standardised bedside lung ultrasound in the acute respiratory failure patient.
[10] Mueller C, McDonald K, de Boer RA, et al.; Heart Failure Association of the European Society of Cardiology. Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations. Eur J Heart Fail 2019;21(6):715–31. The HFA-ESC practical guidance on the interpretation of natriuretic peptides, including the false positives and false negatives.
[11] Bozkurt B, Coats AJS, Tsutsui H, et al. Universal definition and classification of heart failure. Eur J Heart Fail 2021;23(3):352–80. The universal definition of heart failure, defining the syndrome as symptoms and signs caused by a structural or functional cardiac abnormality and corroborated by an elevated natriuretic peptide and objective evidence of congestion.
Maisel et al., NEJM 2002; Januzzi et al. (PRIDE), Am J Cardiol 2005; Wells et al., Thromb Haemost 2000; van Belle et al. (Christopher), JAMA 2006; Lim et al., Thorax 2003; McDonagh et al. (ESC HF), Eur Heart J 2021; Humbert et al. (ESC/ERS PH), Eur Heart J 2022; Hooper et al. (BTS Pleural), Thorax 2010; Lichtenstein and Meziere (BLUE), Chest 2008; Mueller et al. (HFA-ESC peptides), Eur J Heart Fail 2019; Bozkurt et al. (Universal Definition), Eur J Heart Fail 2021; NICE NG106, NG12; BTS Pleural Disease; Heart Foundation of Australia; TSANZ. [1]
References
- [1]Maisel AS, Krishnaswamy P, Nowak RM, et al.; Breathing Not Properly Multinational Study Investigators Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure N Engl J Med, 2002.PMID 12124404
- [2]Januzzi JL Jr, Camargo CA, Anwaruddin S, et al. The N-terminal Pro-BNP investigation of dyspnea in the emergency department (PRIDE) study Am J Cardiol, 2005.PMID 15820160
- [3]Wells PS, Anderson DR, Rodger M, et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: increasing the models utility with the SimpliRED D-dimer Thromb Haemost, 2000.PMID 10744147
- [4]van Belle A, Buller HR, Huisman MV, et al.; Christopher Study Investigators Effectiveness of managing suspected pulmonary embolism using an algorithm combining clinical probability, D-dimer testing, and computed tomography JAMA, 2006.PMID 16403929
- [5]Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneumonia severity on presentation to hospital: an international derivation and validation study Thorax, 2003.PMID 12728155
- [6]McDonagh TA, Metra M, Adamo M, et al.; ESC Scientific Document Group 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure Eur Heart J, 2021.PMID 34447992
- [7]Humbert M, Kovacs G, Hoeper MM, et al.; ESC/ERS Scientific Document Group 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension Eur Heart J, 2022.PMID 36017548
- [8]Hooper C, Lee YCG, Maskell N; BTS Pleural Guideline Group Investigation of a unilateral pleural effusion in adults: British Thoracic Society Pleural Disease Guideline 2010 Thorax, 2010.PMID 20696692
- [9]Lichtenstein DA, Meziere GA Relevance of lung ultrasound in the diagnosis of acute respiratory failure: the BLUE protocol Chest, 2008.PMID 18403664
- [10]Mueller C, McDonald K, de Boer RA, et al.; Heart Failure Association of the European Society of Cardiology Heart Failure Association of the European Society of Cardiology practical guidance on the use of natriuretic peptide concentrations Eur J Heart Fail, 2019.PMID 31222929
- [11]Bozkurt B, Coats AJS, Tsutsui H, et al. Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure: Endorsed by the Canadian Heart Failure Society, Heart Failure Association of India, Cardiac Society of Australia and New Zealand, and Chinese Heart Failure Association Eur J Heart Fail, 2021.PMID 33605000