Phys · general-medicine
Undifferentiated Fatigue — A Systematic Diagnostic Approach
Also known as fatigue · tiredness · chronic fatigue · lassitude · malaise · lethargy · asthenia · lack of energy · low energy · excessive daytime sleepiness · undiagnosed fatigue · unexplained fatigue · post-viral fatigue · post-exertional malaise · myalgic encephalomyelitis · ME · CFS · ME/CFS · chronic fatigue syndrome · systemic exertion intolerance disease · long COVID · post-COVID condition · depression screen · PHQ-2 · iron deficiency fatigue · Addison disease · narcolepsy · obstructive sleep apnoea · STOP-Bang
Consultant-physician-depth guide to the diagnostic approach to the patient with chronic fatigue. Covers the three functional categories (physiological — sleep deprivation, overwork, deconditioning, pregnancy, post-viral; psychological — depression, anxiety, chronic stress, burnout, grief; physical or systemic — anaemia, thyroid disease, diabetes, cardiac failure, sleep apnoea, CKD, hepatic failure, COPD, malignancy, autoimmune disease, chronic infection, drug-related, nutritional, Addison disease, narcolepsy, myasthenia gravis), the focused history with the PHQ-2 and GAD-2 mood screens, the systematic examination with the bedside discriminators (pallor, koilonychia, clubbing, hyperpigmentation, the postural blood pressure, the thyroid), the two-tier investigation framework (Tier 1 — FBC, ferritin, B12, folate, U and E, LFTs, TFTs, CRP, glucose and HbA1c, vitamin D, urinalysis, CXR, ECG, pregnancy test; Tier 2 — autoimmune screen, HIV and hepatitis serology, troponin and BNP, sleep study, short Synacthen), the principle of avoiding over-investigation, the management of the cause and of the unexplained fatigue (reassurance, sleep hygiene, graded activity, CBT, medication review, depression treatment, planned review), and the specific guidance on ME and CFS (NICE 2021 NG206 — the withdrawal of graded exercise therapy, the pacing and energy management) and post-COVID condition (long COVID). Structured for FRACP DWE and DCE, MRCP and ABIM.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Fatigue — A Systematic Diagnostic Approach

The answer first
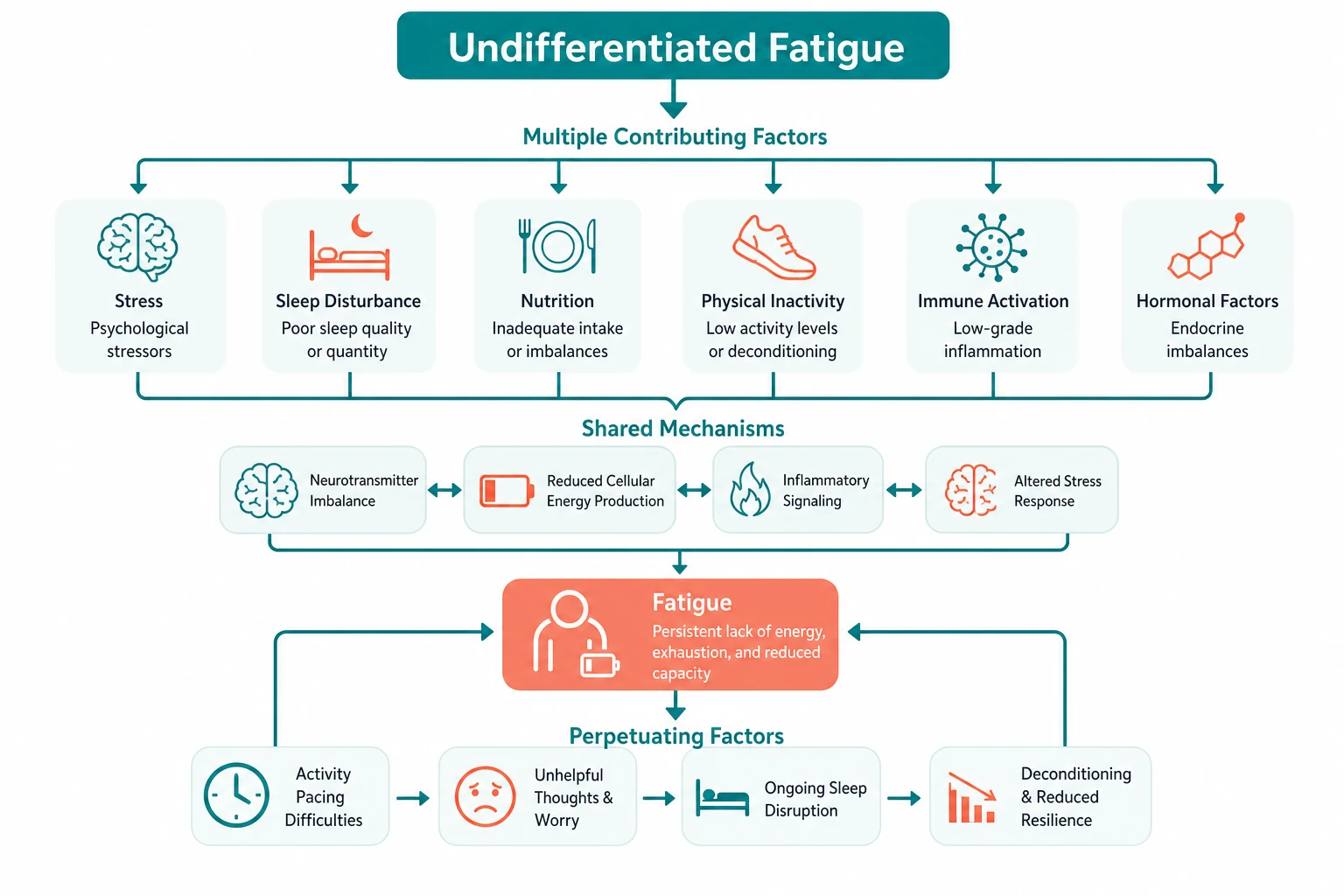
The patient who presents with fatigue of unknown cause is one of the commonest and most cognitively demanding presentations in internal medicine. Fatigue is a subjective symptom, not a sign, and it is common to the physiological, the psychological and the systemic causes. The registrar's job is to use a structured three-category framework (physiological, psychological, physical or systemic), to take a focused history that includes the mood screen, to perform a systematic examination that looks for the bedside discriminators, and to let the Tier 1 investigation screen narrow the differential before committing to a working diagnosis. [1]
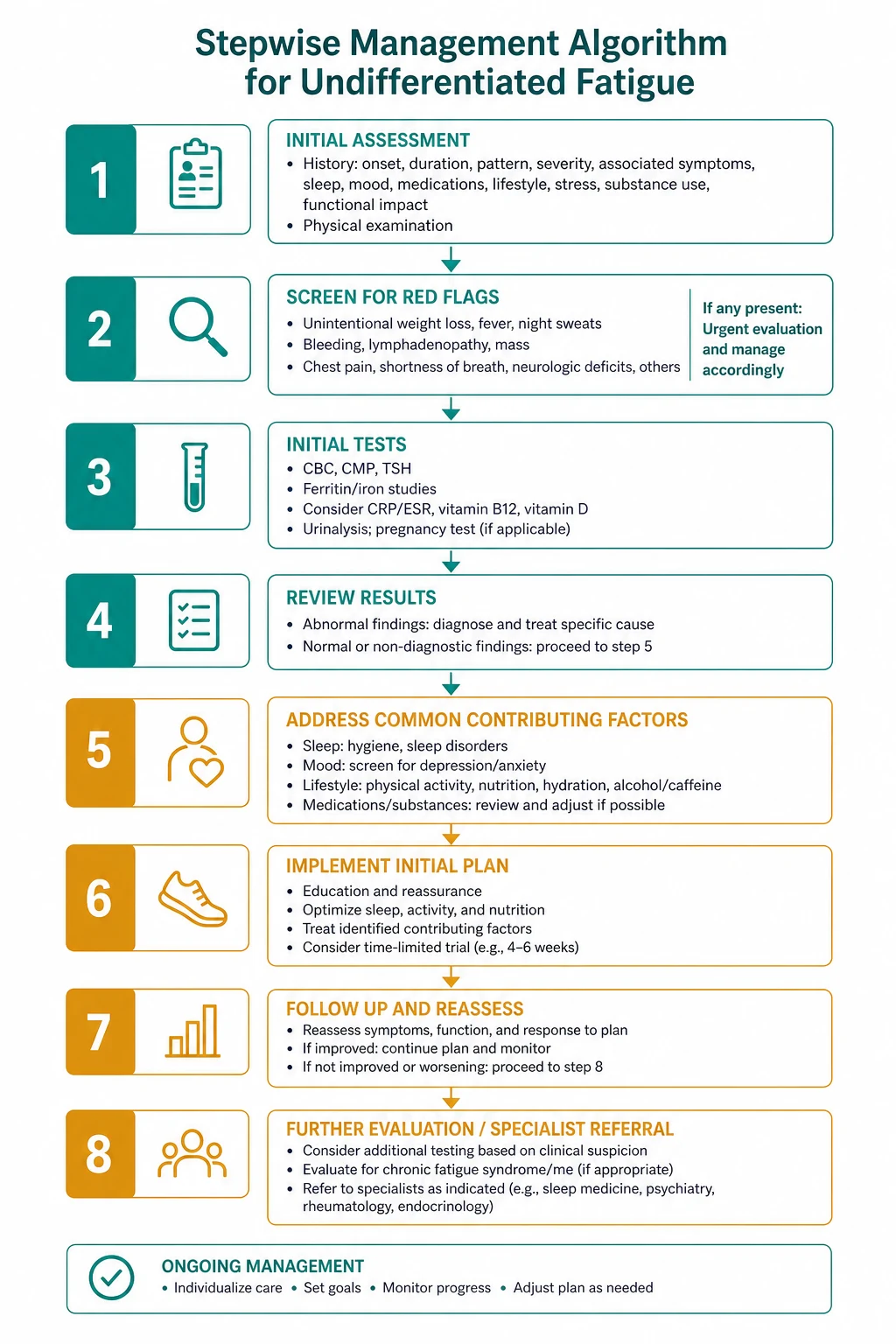
The reproducible sequence for any fatigued patient is: [1]
- Establish the duration and the impact. Acute or subacute fatigue (days to weeks) suggests an organic cause — infection, anaemia, a new endocrine or cardiac presentation. Chronic fatigue (more than 6 weeks) is the territory where the three-category framework earns its place.
- Take the focused history with the mood screen. The PHQ-2 (two questions on depressed mood and anhedonia) and the GAD-2 are the validated screens, and a positive score is the prompt to the formal mood assessment. Ask about the weight loss, the night sweats, the fever, the sleep quality and the medications.
- Examine for the systemic discriminators. The pallor and koilonychia of iron deficiency, the hyperpigmentation and the postural drop of Addison disease, the goitre of thyroid disease, the gallop of heart failure, the proximal weakness of a myopathy, and the fatigable ptosis of myasthenia gravis.
- Order the Tier 1 screen together and interpret it together. The full blood count, the ferritin, the B12 and folate, the U and E, the LFTs, the TFTs, the CRP, the glucose and HbA1c, the vitamin D, the urinalysis, the chest X-ray and the ECG. In women of reproductive age, the pregnancy test.
- Treat the cause if one is found. If the Tier 1 screen is normal and there are no red flags, the management is the reassurance, the lifestyle intervention (sleep hygiene, graded activity), the medication review, the depression treatment and the planned review — not a blanket Tier 2 panel and not a referral. [1]
The single most dangerous error is the binary framing of organic versus functional. Fatigue is usually multifactorial. An organic cause (the iron deficiency, the under-treated hypothyroidism) does not exclude a psychological contributor (the depression, the burnout), and a psychological explanation is a positive diagnosis with DSM-5 criteria — not a label for the difficult patient. The registrar who stops at "it is just depression" after a normal Tier 1 screen has not performed the proper mood assessment. [1]
Viva trap: "What is the single most useful piece of information in the first minute with a fatigued patient?" The honest answer is the pattern and the impact. The patient whose fatigue is worse in the morning, with early-morning waking and anhedonia, is a different patient from the one whose fatigue builds through the day with exertion and a delayed recovery. The patient with weight loss and night sweats is a different patient again. The registrar who asks "tell me about a typical day, from the moment you wake to the moment you sleep" has organised the entire encounter. [1]
Fatigue is not sleepiness — and the distinction matters

The first distinction is between fatigue (a difficulty in initiating or sustaining activity — physical or mental — that is disproportionate to the effort) and sleepiness (the tendency to fall asleep, the excessive daytime somnolence). The two may coexist, but they have different differentials. Sleepiness points to sleep deprivation and sleep-disordered breathing (the obstructive sleep apnoea, the narcolepsy, the shift work). Fatigue points to the systemic, the metabolic, the endocrine and the psychological disease. The registrar who conflates the two will misdirect the investigation. [1]
The second distinction is between the acute and the chronic. Acute fatigue (days to a few weeks) is the territory of the infection, the acute anaemia, the new endocrine or cardiac presentation, and the medication side effect — and it usually declares itself. Chronic fatigue (more than 6 weeks) is the territory where the three-category framework earns its place, where the Tier 1 screen is the workhorse, and where the over-investigation is the commonest error. [1]
The third distinction is between the fatigue that is proportional to exertion (the deconditioning, the heart failure, the COPD, the chronic disease) and the fatigue that is disproportionate and followed by a delayed crash (the post-exertional malaise of ME/CFS and post-COVID condition). This single distinction — asked in the history and confirmed in the activity pattern — changes the management from the graded exercise to the pacing. [1]
The three-category framework
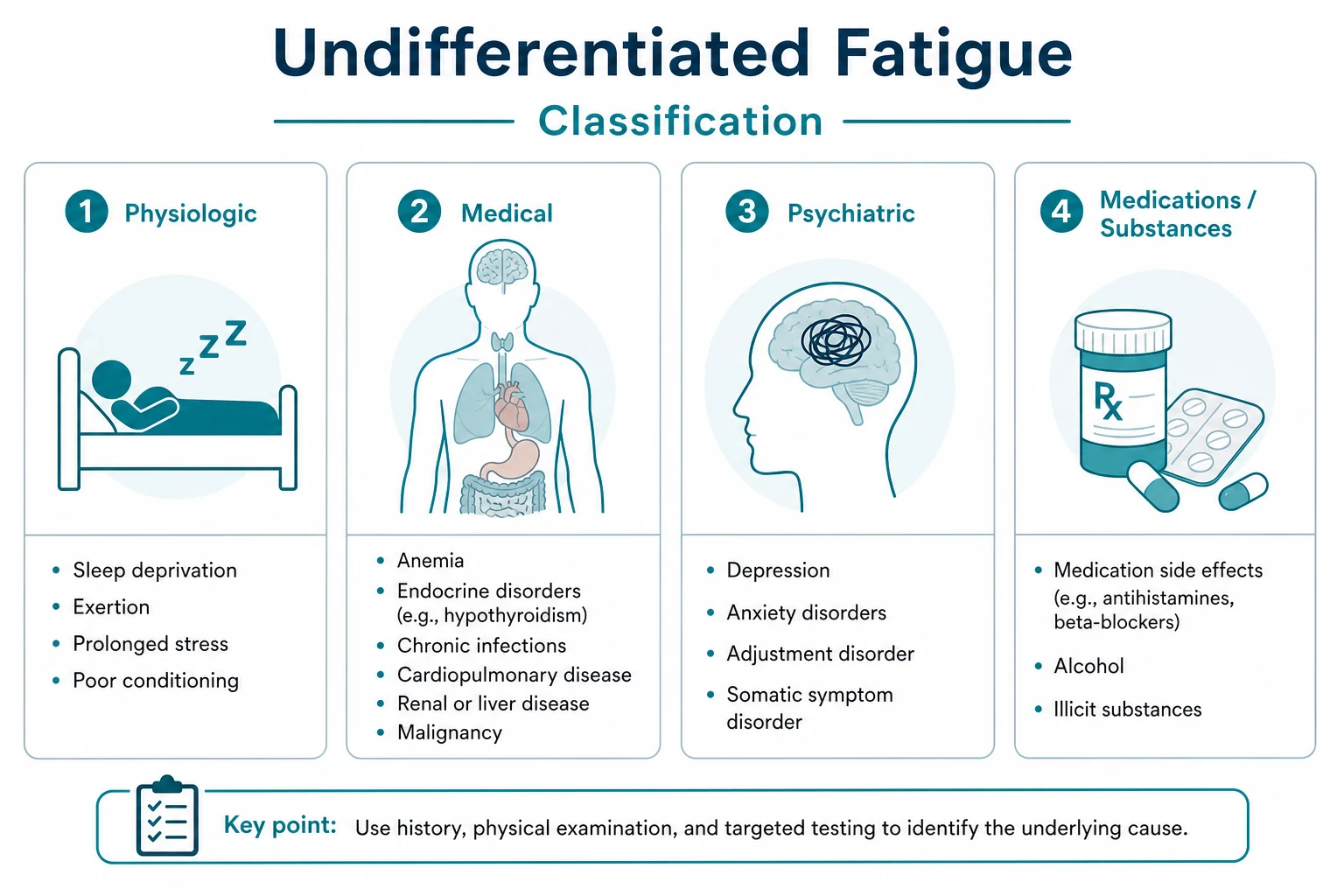
The organising framework for chronic fatigue is the three functional categories: the physiological, the psychological and the physical or systemic. Every fatigued patient is placed in one or more of these categories at the first encounter, and the framework is re-evaluated as the investigation returns. The categories are not mutually exclusive — the multimorbid patient with diabetes, hypothyroidism, iron deficiency and depression has a contributor in all three. [1]
The physiological causes
The physiological causes are the lifestyle and the bodily-state causes that generate fatigue through deconditioning, sleep disruption or the increased metabolic demand: [1]
- Sleep deprivation and poor sleep hygiene — the shift work, the caregiving, the screen use at night, the caffeine, the alcohol that fragments the sleep. The sleep history (the onset, the duration, the quality, the unrefreshing quality, the daytime somnolence) is the first question.
- Overwork and chronic stress — the registrar in the run of nights, the carer of the dependent relative, the person with two jobs and three children.
- Deconditioning — the prolonged bed rest, the post-hospitalisation weakness, the sedentary lifestyle, the obesity. Deconditioning generates a self-sustaining loop: the fatigue leads to the inactivity, the inactivity worsens the cardiovascular fitness and the muscle oxidative capacity, and the worsening fitness worsens the fatigue. The graded activity is the treatment — in the patient without post-exertional malaise.
- Pregnancy and the postpartum period — the physiological fatigue of the first and the third trimester, the iron and folate demands, the sleep disruption of the late pregnancy and the postpartum, and the depression and the thyroiditis of the postpartum.
- Post-viral fatigue — the Epstein-Barr, the influenza, the SARS-CoV-2. The post-viral fatigue is common and usually self-limiting over weeks to a few months; the persistence beyond 3 to 6 months with the post-exertional malaise is the transition to the ME/CFS or the post-COVID syndrome.
- Heat, dehydration and inadequate nutrition — the hot climate, the inadequate fluid intake, the restrictive diet, the eating disorder. [1]
The psychological causes
The psychological causes are the commonest single explanation for the chronic fatigue in the patient with a normal Tier 1 screen. They are positive diagnoses with DSM-5 criteria and validated screens — not labels of exclusion. [1]
- Major depressive disorder — the commonest single cause. The core criteria are the depressed mood, the anhedonia (the loss of interest or pleasure), the weight change, the sleep disturbance (the early-morning waking is characteristic), the fatigue, the psychomotor change, the feelings of worthlessness or guilt, the reduced concentration, and the recurrent thoughts of death. The fatigue is one of the nine criteria; it is not the diagnosis on its own, but it is the presenting complaint in many patients.
- Generalised anxiety disorder — the excessive worry, the restlessness, the fatigue, the difficulty concentrating, the irritability, the muscle tension, the sleep disturbance.
- Chronic stress and burnout — burnout is the occupational syndrome from the chronic workplace stress, with the three dimensions of the exhaustion, the cynicism (the depersonalisation) and the reduced professional efficacy. The WHO ICD-11 definition is the reference. Burnout is distinguished from depression by its occupational specificity, but the two frequently coexist.
- Bereavement — the normal grief that becomes the complicated grief or the major depressive episode. The fatigue, the weight loss and the sleep disturbance of the early bereavement are normal; the persistence beyond 6 to 12 months with the hopelessness and the worthlessness is the transition to the disorder. [1]
DWE high-yield: The PHQ-2 is the validated two-question screen for depression: "Over the past two weeks, have you been bothered by (1) little interest or pleasure in doing things, and (2) feeling down, depressed or hopeless?" Each item is scored 0 (not at all) to 3 (nearly every day). A score of 3 or more has a sensitivity of 83 per cent and a specificity of 92 per cent for the major depressive disorder, as established by Kroenke and colleagues [1]. The GAD-2 uses the same format for the anxiety (the feeling nervous, and the uncontrollable worrying). A positive screen is the prompt to the formal assessment and the treatment, not the diagnosis.
The physical and systemic causes
The physical and systemic causes are the organic diseases that generate fatigue through the reduced oxygen delivery, the metabolic disturbance, the inflammation, the cytokine effect or the endocrine failure. They are the focus of the Tier 1 investigation screen. [1]
The causes, grouped by the system, are: [1]
- Haematological — iron-deficiency anaemia (the commonest worldwide cause; the ferritin below 30 micrograms per litre is highly specific, but the iron deficiency causes fatigue even without anaemia, as the Favrat trials demonstrated [2]), the B12 and folate deficiency (the macrocytic anaemia and the subacute combined degeneration of the cord), the anaemia of chronic disease, the haemolytic anaemia, the haematological malignancy (the lymphoma, the leukaemia, the myeloma).
- Endocrine — hypothyroidism (the high TSH, the low free T4, the weight gain, the cold intolerance, the bradycardia, the delayed relaxation of the ankle jerk), hyperthyroidism (the fatigue of the muscle weakness and the high-output state), diabetes (the osmotic fatigue of the hyperglycaemia, the fatigue of the insulin resistance and the deconditioning), Addison disease (the high-yield exam trap), the hypopituitarism, the Cushing syndrome.
- Cardiovascular — heart failure (the fatigue of the low cardiac output is equal in importance to the dyspnoea and the oedema; the fatigue may be the only symptom in the early or the treated disease), the undiagnosed arrhythmia (the atrial fibrillation, the complete heart block), the ischaemic heart disease (the anginal equivalent in the women and the elderly).
- Respiratory — COPD (the fatigue of the hypoxia, the hypercapnia, the deconditioning and the work of breathing), the obstructive sleep apnoea (the daytime sleepiness with the snoring, the witnessed apnoea, the obesity, the STOP-Bang score of 3 or more and the polysomnogram with an apnoea-hypopnoea index above 5), the pulmonary hypertension, the interstitial lung disease.
- Renal and hepatic — the chronic kidney disease (the fatigue of the anaemia, the uraemia and the deconditioning), the chronic liver disease (the fatigue of the cirrhosis and the defining fatigue of the primary biliary cholangitis).
- Infectious — the tuberculosis (the weight loss, the night sweats, the chronic cough), the HIV (the seroconversion illness and the chronic fatigue of the uncontrolled viraemia), the chronic viral hepatitis (the hepatitis B and C), the infective endocarditis (the subacute presentation with the murmur and the constitutional symptoms), the Epstein-Barr and the post-viral syndrome.
- Autoimmune and inflammatory — the systemic lupus erythematosus (the fatigue affects more than 80 per cent and is often the most disabling symptom), the rheumatoid arthritis, the inflammatory bowel disease, the polymyalgia rheumatica in the older patient (the proximal stiffness, the elevated ESR and CRP, the dramatic response to the low-dose prednisolone, and the temporal artery assessment for the giant cell arteritis).
- Malignancy — the fatigue of the cytokine-mediated sickness behaviour, the anaemia, the weight loss and the hypercalcaemia. The lymphoma with the B symptoms (the fever, the night sweats, the weight loss), the myeloma with the hypercalcaemia and the anaemia, the occult solid tumour with the progressive weight loss.
The drug causes — the most often missed and the most reversible
The medication review is the single most cost-effective intervention in the fatigued patient, especially the older patient with the polypharmacy. The common drugs and their mechanisms are: [1]
- Beta-blockers — the reduced cardiac output and the direct central sedation. The fatigue is a well-recognised effect of the beta-blockade, and the dose reduction or the switch to a selective agent or a different antihypertensive class is the treatment.
- Statins — the statin-associated muscle symptoms (the myalgia, the fatigue, the weakness) are common and dose-dependent; the creatine kinase may be normal. The severe rhabdomyolysis is rare. The approach is the statin holiday, the rechallenge at a lower dose or with a different statin (the rosuvastatin or the pravastatin), or the switch to the ezetimibe or the PCSK9 inhibitor.
- Sedating antihistamines (the first-generation H1 blockers) — the promethazine, the chlorphenamine, the diphenhydramine cross the blood-brain barrier and cause the hangover sedation. The switch to the second-generation (the cetirizine, the loratadine, the fexofenadine) is the treatment.
- Benzodiazepines and the Z-drugs — the hangover sedation, the cumulative risk in the older patient, the falls and the cognitive impairment. The deprescribing is the treatment — the slow taper, the cognitive behavioural therapy for the insomnia, and the sleep hygiene.
- Opioids — the sedation, the constipation, the hypogonadism, the respiratory depression. The deprescribing and the multimodal pain management are the treatment.
- Antipsychotics — the sedation (especially the olanzapine, the quetiapine, the clozapine) and the metabolic syndrome with the weight gain and the diabetes.
- Gabapentinoids (the gabapentin, the pregabalin) — the sedation and the dizziness, the common cause of the fatigue in the chronic-pain patient.
- Others — the levetiracetam and the other antiepileptics, the isotretinoin, the interferon, the chemotherapy, the immunotherapy (the immune-related adverse events, including the thyroiditis and the hypophysitis). [1]
Viva trap: "The patient on a beta-blocker and a statin who presents with fatigue and muscle aching." The reflex is to attribute it to the depression or the ageing. The correct answer is to recognise the drug contribution, to check the creatine kinase, to consider the statin holiday and the beta-blocker dose reduction, and to reassess at 4 weeks. The registrar who reaches for the antidepressant without the medication review has missed the reversible cause. [1]
The nutritional causes
The nutritional causes are the deficiencies that generate fatigue through the impaired oxygen transport (the iron), the impaired neurological function (the B12, the folate) or the impaired muscle and bone metabolism (the vitamin D). [1]
- Iron deficiency — the heavy menstruation, the gastrointestinal loss (the peptic ulcer, the colorectal cancer, the angiodysplasia), the coeliac disease, the vegetarian or vegan diet, the pregnancy, the malabsorption. The ferritin below 30 micrograms per litre is highly specific; the ferritin of 30 to 50 micrograms per litre warrants a trial of the oral iron with the reassessment. The Favrat trials established that the oral iron (the ferrous sulfate or the ferrous fumarate, 65 to 100 mg of the elemental iron daily or on alternate days, with the vitamin C) reduces the fatigue in the non-anaemic iron-deficient woman [2]. The investigation of the cause — the gastrointestinal work-up in the older patient, the gynaecological work-up in the younger woman, the coeliac screen in all — is the next step.
- Vitamin B12 deficiency — the pernicious anaemia (the autoimmune gastric atrophy), the ileal disease (the Crohn, the resection), the metformin, the gastric surgery, the vegan diet. The presentation is the macrocytic anaemia, the fatigue, the glossitis, the neurological features (the peripheral neuropathy, the subacute combined degeneration of the cord with the loss of the vibration and the proprioception, the cognitive change). The B12 is low; the homocysteine and the methylmalonic acid are raised if the level is borderline. The treatment is the intramuscular hydroxocobalamin (the loading then the maintenance) or the high-dose oral in selected patients.
- Folate deficiency — the poor intake, the malabsorption, the increased demand (the pregnancy, the haemolysis), the drugs (the methotrexate, the phenytoin, the trimethoprim). The macrocytic anaemia without the neurological features.
- Vitamin D deficiency — the controversial association with the fatigue and the muscle weakness, the proven association with the bone pain and the osteomalacia. The level below 30 nmol per litre is deficient; the replacement is the cholecalciferol.
- Thiamine deficiency — the alcohol-use disorder and the refeeding syndrome. The Wernicke encephalopathy (the confusion, the ataxia, the ophthalmoplegia) is the emergency; the high-dose intravenous thiamine (the 500 mg intravenously three times daily for 3 to 5 days, before any glucose) is the treatment. [1]
The rare but high-yield causes — the exam favourites
The rare causes of fatigue are the exam favourites because they are the missed diagnoses with the serious consequences. The registrar must know them cold. [1]
Addison disease (primary adrenal insufficiency)
Addison disease is the classic exam and clinical trap because the fatigue, the weight loss and the postural hypotension are easily attributed to the depression or the chronic stress. The missed diagnosis is the missed adrenal crisis. [1]
The discriminators are: [1]
- The fatigue and the weight loss — the insidious onset over the months.
- The hyperpigmentation — the palmar creases, the buccal mucosa, the gingiva, the recent scars, the areolae, the sun-exposed areas. The pigmentation is from the elevated pro-opiomelanocortin (the precursor of the ACTH and the melanocyte-stimulating hormone) in the uncontrolled primary adrenal failure.
- The postural hypotension — from the mineralocorticoid deficiency.
- The salt craving — a characteristic and often-missed symptom.
- The hyponatraemia with the hyperkalaemia — from the mineralocorticoid deficiency. The hypoglycaemia and the mild metabolic acidosis may be present.
- The abdominal pain, the nausea, the vomiting — the non-specific gastrointestinal presentation. [1]
The diagnosis is the low morning cortisol (below 100 nmol per litre is highly suggestive) with the elevated ACTH, confirmed by the short Synacthen test (the 250 microgram tetracosactide intravenously or intramuscularly, with the cortisol at 0, 30 and 60 minutes; a peak cortisol below 500 nmol per litre confirms the adrenal insufficiency). The 2016 Endocrine Society guideline (Bornstein and colleagues) establishes the short Synacthen test as the gold standard and emphasises that the treatment should never be delayed in the suspected adrenal crisis [6].
The management is the hydrocortisone replacement (the 15 to 25 mg daily in two or three divided doses, or the modified-release once-daily preparation) and the fludrocortisone (the 50 to 200 micrograms daily). The patient education on the sick-day rules (the doubling of the hydrocortisone during the illness, the emergency intramuscular hydrocortisone, the medical alert) and the adrenal crisis prevention is the critical, life-saving component. [1]
Narcolepsy
Narcolepsy is the excessive daytime sleepiness with the cataplexy (the sudden loss of the muscle tone triggered by the emotion), the sleep paralysis, and the hypnagogic hallucinations. The cataplexy with the narcolepsy is the type 1 (the hypocretin-deficient); the narcolepsy without the cataplexy is the type 2. The diagnosis is the polysomnogram followed by the multiple sleep latency test (the mean sleep latency of 8 minutes or less with the 2 or more sleep-onset REM periods), and (in the type 1) the low CSF hypocretin. The management is the modafinil or the armodafinil for the sleepiness, the sodium oxybate for the cataplexy, and the planned naps. [1]
Myasthenia gravis
Myasthenia gravis is the fatigable weakness that worsens with the sustained activity and improves with the rest. The fatigue is the muscular fatigue (the ptosis after the sustained upgaze, the diplopia, the dysarthria and the dysphagia after the prolonged speech or the meal, the limb weakness after the exertion) — not the systemic fatigue, but the two overlap and the myasthenia is a recognised cause of the fatiguing presentation. The diagnosis is the acetylcholine receptor antibodies (positive in 85 per cent of the generalised disease), the single-fibre EMG, and the CT of the thymus (the thymoma in 10 to 15 per cent). The management is the pyridostigmine, the immunosuppression (the prednisolone, the azathioprine, the mycophenolate, the rituximab), and the thymectomy in the selected patients. [1]
Polymyalgia rheumatica and giant cell arteritis
The polymyalgia rheumatica is the high-yield diagnosis in the older fatigued patient. The average age of onset is 73; the presentation is the proximal stiffness (the shoulders and the hips, worse in the morning), the fatigue, the weight loss, and the elevated ESR (typically above 40) and CRP. The response to the low-dose prednisolone (the 15 mg daily) is dramatic and diagnostic. The untreated disease carries the high risk of the giant cell arteritis and the blindness — the temporal artery assessment (the headache, the scalp tenderness, the jaw claudication, the visual disturbance) and the urgent treatment with the high-dose glucocorticoid are mandatory if the giant cell arteritis is suspected. [1]
Myalgic encephalomyelitis and chronic fatigue syndrome (ME/CFS)
ME/CFS is the complex multisystem disease defined by the specific positive diagnostic criteria. It is NOT a diagnosis of exclusion in the traditional sense — the 2021 NICE NG206 guideline and the 2015 IOM (now National Academy of Medicine) report establish the diagnosis by the four core criteria, and the diagnosis should be made and the management begun as soon as the criteria are met, not after the years of the negative investigations. [1]
The diagnostic criteria
The 2015 IOM report (the Committee on the Diagnostic Criteria for ME/CFS) renamed the condition the systemic exertion intolerance disease and defined the four core criteria [4]:
- A substantial reduction or impairment in the ability to engage in the pre-illness levels of the occupational, educational, social or personal activity, that persists for more than 6 months and is accompanied by the fatigue that is often profound, of new onset, not the result of the ongoing exertion, and not substantially alleviated by the rest.
- The post-exertional malaise (PEM) — the worsening of the symptoms after the physical, mental or emotional exertion that would not have caused the problem before the illness. The cardinal feature, distinguishing the ME/CFS from the simple chronic fatigue.
- The unrefreshing sleep — the patient does not feel rested after the full night of sleep, even in the absence of the objective sleep alterations.
- Either the cognitive impairment OR the orthostatic intolerance (at least one is required) — the cognitive impairment (the problems with the thinking, the memory, the executive function, the information processing), and the orthostatic intolerance (the symptoms that worsen on the standing and improve on the lying). [1]
The post-exertional malaise — the cardinal feature
The PEM is the cardinal feature that distinguishes the ME/CFS from the simple chronic fatigue, the deconditioning and the depression. The PEM is the worsening of the symptoms 12 to 72 hours after the physical, cognitive or emotional exertion, with the slow recovery over the hours to the days. The patient describes the "crash" after the activity that previously was tolerated — the day of the shopping that is followed by the three days of the bed rest. The PEM is the feature that mandates the different management from the graded exercise therapy. [1]
The 2021 NICE NG206 guideline — the withdrawal of the graded exercise therapy
The 2021 NICE NG206 guideline is the landmark revision that withdrew the graded exercise therapy (GET) as a treatment for the ME/CFS, on the grounds that the committee found that the GET could cause the harm by forcing the patients to exceed the energy limits and triggering the PEM. The GET — defined as the programme using the fixed incremental increases in the physical activity — should not be offered to the ME/CFS patients. [1]
The management, per the NG206, is the: [1]
- Energy management or pacing — the approach of staying within the energy envelope (the "energy envelope" is the level of the activity that the patient can sustain without triggering the PEM). The pacing is the opposite of the graded exercise — it is the maintenance, not the incremental increase.
- Activity management — the practical strategies to prioritise, plan and pace the daily activities. [1]- Symptom control — the pain, the sleep, the nausea, the orthostatic intolerance (the compression garments, the fludrocortisone, the midodrine in selected patients).
- Cognitive behavioural therapy (CBT) — offered as a supportive treatment to help the patient cope with the chronic illness, NOT as a curative treatment. The CBT does not cure the ME/CFS, and the patient who is offered the CBT as a cure has been misinformed.
- Sleep management — the sleep hygiene without the forced sleep restriction or the forced sleep extension.
- The coordinated multidisciplinary approach — the GP, the specialist ME/CFS service, the physiotherapy, the occupational therapy, the psychology, the dietetics.
- The acknowledgement of the severity — the severe ME/CFS (the housebound or the bedbound patient) requires the home-based care, the very gentle approach, and the avoidance of the any activity that triggers the PEM. [1]
DWE high-yield: The single most testable fact about the ME/CFS management is that the 2021 NICE NG206 guideline withdrew the graded exercise therapy because of the risk of the post-exertional malaise. The registrar who prescribes the graded exercise to a ME/CFS patient has misread the guideline and may worsen the patient. The management is the pacing, the energy management, the symptom control and the supportive CBT. [1]
The PACE trial controversy
The PACE trial (published 2011) claimed the benefit of the CBT and the GET for the chronic fatigue syndrome, and was the basis of the earlier NICE CG53 guideline (2007) that recommended the CBT and the GET. The PACE trial has been heavily criticised for the outcome switching (the primary outcomes were changed after the trial began), the loose recovery criteria, the lack of the objective measures, and the failure to report the harm. The 2021 NICE revision reflects the weight of the patient-reported harm and the re-evaluation of the evidence, and the GET was withdrawn on the principle that the committee could not rule out the harm. [1]
Post-COVID condition (long COVID)
The post-COVID condition (the long COVID) is the persistent symptoms beyond the 12 weeks from the acute infection, not explained by the alternative diagnosis. The fatigue is the commonest symptom, followed by the breathlessness and the cognitive dysfunction (the "brain fog"). The post-COVID condition overlaps substantially with the ME/CFS — a significant proportion of the post-COVID patients meet the ME/CFS criteria, with the post-exertional malaise, the unrefreshing sleep and the orthostatic intolerance. [1]
The NICE NG188 guideline (the COVID-19 rapid guideline: managing the long-term effects) frames the management: the staged investigation (the FBC, the CRP, the troponin if the cardiac involvement, the D-dimer if the thromboembolism, the TFTs, the vitamin D, the chest X-ray and the spirometry), the multidisciplinary rehabilitation, the pacing and the caution against the forced incremental exercise, and the screening for the complications (the thromboembolism, the cardiac, the respiratory, the psychiatric). The systematic review of the post-COVID fatigue (Wong and colleagues) identified the older age, the female sex, the severe acute illness, the comorbidities and the pre-existing depression or anxiety as the risk factors [7].
The principle for the registrar is the same as the ME/CFS: the pacing, the symptom control, the gradual and the patient-led rehabilitation, and the avoidance of the forced incremental exercise that triggers the post-exertional malaise. The post-COVID fatigue is a new and the common problem, and the registrar who applies the pre-pandemic graded-exercise paradigm will harm the patient. [1]
The focused history — the questions that change the differential
The history in the fatigued patient is the single highest-yield investigation. The history directs the examination, the examination directs the Tier 1 screen, and the Tier 1 screen directs the Tier 2. The registrar should ask, in the order: [1]
Onset, duration and pattern. The acute or the subacute onset points to the organic cause — the infection, the anaemia, the new endocrine or the cardiac presentation. The chronic, insidious onset points to the physiological or the psychological. The pattern matters: the fatigue that is worse in the morning (with the early-morning waking and the anhedonia) points to the depression; the fatigue that builds through the day (with the exertion and the delayed recovery) points to the deconditioning, the heart failure or the COPD; the fatigue that crashes 12 to 72 hours after the exertion points to the ME/CFS or the post-COVID condition. [1]
Impact on the activities of daily living. The fatigue that limits the work, the social life or the self-care is the significant fatigue; the fatigue that is the complaint but that does not limit the activity may still be the genuine symptom, but the functional impact is the guide to the severity and the urgency. [1]
The sleep history. The onset, the duration, the quality, the unrefreshing quality. The snoring, the witnessed apnoea, the partner's report of the gasping. The restless legs. The shift work and the sleep opportunity. The caffeine, the alcohol and the screen use at night. The sleep history is the first screen for the sleep disorders and the physiological fatigue. [1]
The mood screen. The PHQ-2 and the GAD-2, administered verbatim. The positive score is the prompt to the formal assessment. The core symptoms of the depression (the low mood, the anhedonia, the hopelessness, the guilt, the suicidal ideation, the early-morning waking, the reduced appetite, the reduced libido) should be asked directly. The suicidal ideation is the mandatory safety assessment. [1]
The red flags. The unintentional weight loss (more than 5 per cent in 6 months), the fever, the night sweats, the progressive anaemia symptoms, the new lymphadenopathy, the new mass, the haemoptysis, the change in the bowel habit, the postmenopausal bleeding, the dysphagia. The red flags escalate the work-up to the CT imaging, the targeted endoscopy and the myeloma screen. [1]
The medication and the substance history. The beta-blocker, the statin, the sedating antihistamine, the benzodiazepine, the opiate, the gabapentinoid, the antipsychotic, the over-the-counter and the herbal. The alcohol (the AUDIT-C), the recreational drugs, the caffeine. [1]
The past history. The cardiovascular disease, the diabetes, the thyroid disease, the autoimmune disease, the malignancy, the psychiatric history, the recent pregnancy, the recent surgery or the hospitalisation, the recent infection (including the COVID-19). [1]
The social history. The occupation and the shift work, the relationships and the dependants, the financial stress, the bereavement, the caregiving burden, the exercise and the diet, the housing and the social support. The social context is often the key to the management even when the organic cause is found. [1]
The family history. The autoimmune disease (the thyroid, the type 1 diabetes, the Addison, the pernicious anaemia), the malignancy (the colorectal, the breast, the haematological), the psychiatric, the sleep disorders. [1]
The examination — the discriminators at the bedside
The examination of the fatigued patient is the systematic assessment of the general state, the vital signs, and the systems, with the specific search for the bedside discriminators of the systemic disease. [1]
The general inspection and the vital signs
The general inspection identifies the cachexia (the malignancy, the chronic disease, the eating disorder), the obesity (the sleep apnoea, the deconditioning, the metabolic syndrome), the pallor (the anaemia), the pigmentation (the Addison disease), and the signs of the distress. The vital signs are the postural blood pressure (the drop on the standing suggests the Addison disease, the autonomic dysfunction, the dehydration or the over-diuresis), the resting heart rate (the tachycardia of the anaemia or the thyrotoxicosis; the bradycardia of the hypothyroidism or the beta-blockade), the respiratory rate, the oxygen saturation, the temperature, and the body mass index (the obesity, the cachexia). [1]
The hands
The hands identify the pallor of the palmar creases (the anaemia — the pallor of the creases when the hand is extended and the fingers extended suggests the haemoglobin below 70 to 80 g per litre), the koilonychia (the spoon-shaped, the thin, the brittle nails of the iron deficiency), the clubbing (the malignancy, the inflammatory bowel disease, the cyanotic congenital heart disease, the infective endocarditis, the cirrhosis, the pulmonary fibrosis), the palmar erythema (the chronic liver disease, the pregnancy, the thyrotoxicosis), the Dupuytren contracture (the chronic liver disease, the diabetes), and the tremor (the thyrotoxicosis, the anxiety, the essential tremor, the alcohol withdrawal). [1]
The thyroid
The thyroid examination identifies the goitre (the diffuse, the multinodular, the solitary nodule), the bruit (the Graves disease), the eye signs (the exophthalmos, the lid lag, the ophthalmoplegia of the Graves disease), and the general signs of the hypothyroidism (the bradycardia, the cold intolerance, the delayed relaxation of the ankle jerk, the dry skin, the thinning of the hair, the slow speech) and the hyperthyroidism (the tachycardia, the hot intolerance, the weight loss, the proximal weakness, the hyperreflexia). [1]
The cardiovascular system
The cardiovascular examination identifies the raised JVP (the heart failure, the cor pulmonale), the displaced apex (the left ventricular dilatation), the gallop (the third heart sound of the systolic heart failure), the murmurs (the valvular disease, the prosthetic valve — and the infective endocarditis on the prosthetic or the previously damaged valve), the peripheral oedema (the right heart failure), and the postural drop (the Addison disease, the dehydration, the autonomic dysfunction, the over-diuresis). [1]
The respiratory system
The respiratory examination identifies the crackles (the pulmonary oedema, the interstitial lung disease, the infection), the wheeze (the COPD, the asthma), the hyperinflation (the COPD), the pleural effusion (the dullness, the reduced breath sounds, the decreased vocal resonance), and the cyanosis (the hypoxia). The chest signs of the fatiguing respiratory disease are often subtle, and the spirometry and the chest X-ray are the confirmatory investigations. [1]
The abdominal examination
The abdominal examination identifies the hepatomegaly (the malignancy, the cirrhosis, the right heart failure), the splenomegaly (the portal hypertension, the haematological malignancy, the infection), the masses (the colorectal, the ovarian, the gastric), the ascites (the cirrhosis, the malignancy, the heart failure), and the palpable bladder (the obstructive uropathy). [1]
The lymph node examination
The lymph node examination is mandatory in every fatigued patient. The cervical, the supraclavicular (the Virchow node — the left supraclavicular node is the gastric or the abdominal malignancy until proven otherwise), the axillary, the epitrochlear, and the inguinal nodes. The palpable supraclavicular node, the hard fixed node, the node above 1 to 2 cm, or the node that is growing, is the malignancy until proven otherwise. [1]
The skin and the specific signs
The skin examination identifies the hyperpigmentation of the Addison disease (the palmar creases, the buccal mucosa, the recent scars, the sun-exposed areas), the pallor, the bruising (the thrombocytopenia, the coagulopathy, the chronic liver disease), the spider naevi and the palmar erythema (the chronic liver disease), and the proximal muscle weakness (the myopathy of the Cushing syndrome, the statin, the hypothyroidism, the inflammatory myopathy). The fatigable ptosis (the ptosis that worsens with the sustained upgaze) and the diplopia (the fatigable diplopia) are the bedside signs of the myasthenia gravis. [1]
The Tier 1 investigation screen

The Tier 1 investigation screen is the bedside and the laboratory tests that discriminate the major categories of the fatigue within hours to days. They are ordered together, interpreted together, and they frame the Tier 2 work-up. [1]
The full blood count
The full blood count identifies the anaemia (the microcytic of the iron deficiency or the thalassaemia; the macrocytic of the B12 or the folate deficiency or the alcohol; the normocytic of the chronic disease, the renal failure, the bone marrow failure), the macrocytosis without the anaemia (the early B12 or folate deficiency, the alcohol, the hypothyroidism, the myelodysplasia, the drug effect), the leucocytosis (the infection, the inflammation, the leukaemoid reaction), the leucopenia (the viral infection, the autoimmune disease, the leukaemia, the drug effect), the eosinophilia (the allergy, the parasitic infestation, the Addison disease, the eosinophilic disorder), and the thrombocytosis (the inflammation, the iron deficiency, the myeloproliferative disorder) or the thrombocytopenia (the sepsis, the ITP, the leukaemia, the chronic liver disease). [1]
The iron studies, the B12 and the folate
The ferritin is the key marker of the iron deficiency. A ferritin below 30 micrograms per litre is highly specific; a ferritin of 30 to 50 micrograms per litre warrants a trial of the oral iron with the reassessment at 4 weeks. The ferritin is the acute-phase reactant, and a normal or a high ferritin does not exclude the iron deficiency in the inflamed patient — the transferrin saturation (below 20 per cent suggests the functional iron deficiency) and the soluble transferrin receptor (raised in the true iron deficiency, normal in the inflammation) are the adjuncts. The B12 and the folate screen the macrocytic anaemia and the neurological disease; the homocysteine and the methylmalonic acid are the adjuncts when the level is borderline. [1]
The urea and electrolytes, the LFTs and the TFTs
The U and E identify the renal failure (the raised creatinine, the falling eGFR) and the hyponatraemia (the dilutional hyponatraemia of the heart failure, the cirrhosis and the SIADH; the hyponatraemia with the hyperkalaemia of the Addison disease). The LFTs identify the hepatic cause (the elevated transaminases of the acute hepatitis, the cholestatic pattern, the low albumin and the raised INR of the chronic liver disease, the hepatitis B and C serology when indicated). The TFTs (the TSH and the free T4) identify the hypothyroidism (the high TSH, the low free T4) and the hyperthyroidism (the low TSH, the high free T4). [1]
The CRP, the glucose and the HbA1c, the vitamin D
The CRP is the inflammation screen. A raised CRP points to the infection, the inflammation, the malignancy or the autoimmune disease and escalates the work-up. A normal CRP is reassuring but does not exclude the early autoimmune disease, the malignancy or the post-viral syndrome. The glucose and the HbA1c screen the diabetes. The vitamin D is the controversial but commonly checked marker. [1]
The urinalysis, the CXR and the ECG
The urinalysis identifies the glycosuria (the diabetes), the proteinuria (the renal disease), the haematuria (the urological malignancy, the glomerulonephritis), and the leucocytes and the nitrites (the infection). The chest X-ray identifies the malignancy, the tuberculosis, the heart failure, the interstitial lung disease, and the sarcoidosis; the negative chest X-ray is the cost-effective reassurance. The 12-lead ECG identifies the arrhythmia, the ischaemia, the left ventricular hypertrophy, the heart block, and the pericardial effusion (the low voltage, the electrical alternans). [1]
The pregnancy test
In the woman of the reproductive age, the pregnancy test (the beta-hCG) is the mandatory first investigation — the fatigue, the nausea and the amenorrhoea of the early pregnancy is the common and the easily-missed cause, and the imaging and the drug management are the consequences of the missed diagnosis. [1]
The Tier 2 investigations — the targeted, not the blanket
The Tier 2 investigations are the targeted, problem-oriented tests that are ordered when the Tier 1 is abnormal or when the clinical suspicion is high. The principle is the targeted, not the blanket — the registrar who orders the autoimmune screen, the tumour markers, the viral panels, the cortisol and the sex hormones in every fatigued patient has misunderstood the approach. [1]
The Tier 2 autoimmune and inflammatory screen
The antinuclear antibody (ANA), the rheumatoid factor, the anti-CCP, the extractable nuclear antigens (the anti-Ro, the anti-La, the anti-Sm, the anti-RNP, the anti-Jo-1, the anti-Scl-70, the anti-centromere), the complement (the C3, the C4), the myeloma screen (the serum electrophoresis, the serum free light chains), the creatine kinase (the myopathy), the ACE (the sarcoidosis), the tissue transglutaminase IgA with the total IgA (the coeliac disease). Indicated when the Tier 1 is abnormal (the raised CRP, the anaemia, the abnormal LFTs) or when the clinical suspicion is high (the arthralgia, the rash, the Raynaud, the sicca, the proximal weakness, the unexplained weight loss). [1]
The Tier 2 infection screen
The HIV, the hepatitis B and C serology, the QuantiFERON or the tuberculin skin test, the Epstein-Barr and the cytomegalovirus serology, the blood cultures (if the fever), the echocardiogram (if the murmur or the injected intravenous access), the atypical pneumonia serology. Indicated by the clinical suspicion or the abnormal Tier 1. [1]
The Tier 2 endocrine screen
The short Synacthen test (the 250 microgram tetracosactide with the cortisol at 0, 30 and 60 minutes; the peak below 500 nmol per litre confirms the adrenal insufficiency). Indicated when the clinical features (the weight loss, the postural drop, the hyperpigmentation) or the biochemistry (the hyponatraemia with the hyperkalaemia, the hypoglycaemia) suggest the Addison disease. The morning cortisol as the screening (above 500 nmol per litre effectively excludes; below 100 nmol per litre is highly suggestive). [1]
The Tier 2 cardiac and sleep investigations
The troponin (if the chest pain or the cardiac symptoms), the BNP or the NT-proBNP (if the clinical suspicion of the heart failure), the echocardiogram (the left and the right ventricular function, the valvular disease, the estimated pulmonary artery pressure), the polysomnogram (if the STOP-Bang score is 3 or more, or if the daytime sleepiness with the snoring), the Holter monitor (if the palpitations or the suspected arrhythmia). [1]
The Tier 2 imaging and the invasive tests
The CT imaging (the chest, the abdomen, the pelvis — if the red flags or the abnormal Tier 1 suggest the malignancy), the endoscopy (the gastroscopy and the colonoscopy — if the iron deficiency, the weight loss, the change in the bowel habit, the dysphagia, or the postmenopausal or the occult bleeding), the bone marrow biopsy (if the haematological malignancy is suspected), and the targeted biopsy of the mass or the node. [1]
The management — treat the cause, validate the symptom

The overarching principle of the fatigue management is the treat the cause if one is found, and the validate the symptom whether or not the cause is found. The patient who feels heard, who understands the findings, and who has a clear plan is far less likely to re-present or to seek the alternative-medicine pathway. [1]
The management of the identified cause
The cause-specific management is the: [1]
- Iron deficiency — the oral iron (the ferrous sulfate or the ferrous fumarate, the 65 to 100 mg of the elemental iron daily or on alternate days, with the vitamin C), the 4-week reassessment of the haemoglobin and the ferritin, and the investigation of the underlying cause (the gastrointestinal work-up in the older patient, the gynaecological work-up in the younger woman, the coeliac screen in all). The intravenous iron is the option in the severe deficiency, the intolerance of the oral, or the malabsorption.
- Hypothyroidism — the levothyroxine (the 1.6 micrograms per kg per day in the younger patient; the lower starting dose in the older or the cardiac patient, with the gradual titration), the 6-week reassessment of the TSH, and the annual monitoring.
- Diabetes — the glycaemic optimisation (the HbA1c target individualised, typically 53 to 64 mmol per mol), the lifestyle intervention, and the cardiovascular risk reduction.
- Heart failure — the four pillars of the guideline-directed therapy (the beta-blocker, the ACE inhibitor or the ARNI, the mineralocorticoid receptor antagonist, the SGLT2 inhibitor) for the HFrEF, with the awareness that the fatigue may be from the over-diuresis or the beta-blockade as much as from the disease.
- Obstructive sleep apnoea — the continuous positive airway pressure (CPAP) titrated to the polysomnogram, the weight loss and the exercise, the avoidance of the alcohol and the sedatives, and the cardiovascular risk reduction. The STOP-Bang score and the polysomnogram are the pathway [5].
- Depression — the evidence-based psychological therapy (the CBT or the interpersonal therapy), the antidepressant (the SSRI as the first-line, with the 4 to 6 week onset of action and the awareness of the side-effect profile), the addressing of the psychosocial stressors, and the safety assessment for the suicidal ideation.
- Addison disease — the hydrocortisone and the fludrocortisone replacement, the patient education on the sick-day rules, and the adrenal crisis prevention [6].
- The medication cause — the deprescribing of the beta-blocker, the statin holiday, the switch to the second-generation antihistamine, the slow taper of the benzodiazepine, the multimodal pain management to reduce the opiate and the gabapentinoid.
The management of the unexplained fatigue
If the Tier 1 screen is normal, there are no red flags, and the clinical assessment is low-risk, the management is the: [1]
- Reassurance and the validation of the symptom. The explanation of the negative investigations as the reassuring finding (not the dismissal of the symptom), the acknowledgement that the fatigue is the real and the disabling symptom, and the setting of the clear and the realistic expectation.
- The lifestyle intervention. The sleep hygiene (the regular sleep and the wake time, the dark and the cool bedroom, the avoidance of the caffeine and the alcohol and the screens at night), the graded activity (the gradual increase in the aerobic and the resistance exercise, in the patient WITHOUT the post-exertional malaise), the balanced diet, the reduction of the alcohol and the caffeine.
- The medication review. The identification and the deprescribing of the contributory drugs.
- The depression screen and the treatment. The PHQ-2 and the GAD-2, the formal mood assessment if positive, and the evidence-based treatment.
- The planned review. The follow-up at 4 to 6 weeks to reassess the symptom, the investigation results, and the response to the intervention. The planned review is the safety net — the persistent or the worsening fatigue, or the new red flag, is the prompt to the Tier 2 work-up. [1]
The CBT and the graded activity for the unexplained fatigue
The cognitive behavioural therapy has the most consistent evidence for the improvement of the fatigue and the function in the unexplained chronic fatigue (the fatigue without the ME/CFS criteria). The graded activity (the gradual increase in the activity, the opposite of the pacing) improves the chronic fatigue without the post-exertional malaise. The two are distinct from the ME/CFS management, where the CBT is the supportive treatment and the graded exercise is contraindicated. [1]
The common exam traps
- The binary-framing trap — the "organic versus functional." Fatigue is usually multifactorial; an organic cause does not exclude a psychological contributor, and a psychological explanation is a positive diagnosis with the DSM-5 criteria, not a label for the difficult patient.
- The over-investigation trap — the blanket "fatigue panel" of the autoimmune screen, the tumour markers, the viral panels, the cortisol and the sex hormones. The yield is low, the false positives drive the harm, and the targeted Tier 1 and the problem-oriented Tier 2 are the guideline-supported approach.
- The ME/CFS graded-exercise trap — prescribing the graded exercise therapy to the patient with the post-exertional malaise. The 2021 NICE NG206 withdrew the GET because of the harm; the management is the pacing, the energy management, the symptom control and the supportive CBT.
- The Addison trap — attributing the fatigue, the weight loss and the postural drop of the adrenal insufficiency to the depression or the chronic stress. The hyperpigmentation, the hyponatraemia with the hyperkalaemia, and the failed short Synacthen test are the discriminators.
- The iron trap — accepting the normal or the borderline ferritin in the inflamed patient. The ferritin is the acute-phase reactant; the functional iron deficiency may be masked by the raised CRP.
- The depression-as-exclusion trap — labelling the patient as depressed after the normal Tier 1 screen without performing the proper mood assessment. The PHQ-2 and the DSM-5 criteria are the diagnostic standard.
- The medication trap — forgetting the medication review. The beta-blocker, the statin, the sedating antihistamine, the benzodiazepine, the opiate and the gabapentinoid are the commonest and the most reversible causes in the older patient.
- The sleep-apnoea trap — missing the diagnosis in the obese, the hypertensive, the middle-aged patient with the daytime sleepiness and the witnessed apnoea. The STOP-Bang score and the polysomnogram are the pathway.
- The communication trap — the dismissive "there is nothing wrong." The validation, the explanation, the plan and the planned review are the treatment. [1]
The DCE long-case integration
In the DCE long case, the fatigued patient is presented with the SASPOP format (Symptoms, Age, Sex, Presentation, Occupation, Problems), the structured problem list (the fatigue and its contributors, the comorbidities, the medications, the functional and the social context), and the integrated management plan (the cause-specific treatment, the lifestyle intervention, the symptom relief, the prevention of the complications, the follow-up, and the communication). [1]
The registrar's job is to resist the pull of a single diagnosis. The patient with the type 2 diabetes, the hypothyroidism, the obesity, the obstructive sleep apnoea, the iron deficiency and the depression has the contributors in all three categories, and the integrated management — the glycaemic optimisation, the thyroid replacement, the CPAP, the iron replacement, the depression treatment, the graded activity (in the patient without the PEM), and the medication review — is what keeps the complex patient functioning. The registrar who stops at "depression" or at "sleep apnoea" and treats the single cause has missed the rest. [1]
The communication and the shared decision-making — the validation of the symptom, the explanation of the contributors, the prioritisation of the management, the expectations and the timeline, and the red flags to report — are the final layer of the senior management. The patient who understands the plan and who has the follow-up arranged is the patient who improves. [1]
References
Kroenke, Spitzer, Williams, Med Care 2003 (PHQ-2, PMID 14583691); Verdon et al., BMJ 2003 (oral iron for unexplained fatigue in non-anaemic women, PMID 12763985); Krayenbuehl et al., Blood 2011 (iron deficiency without anaemia, PMID 21705493); IOM (National Academy of Medicine) 2015, Beyond ME/CFS (PMID 34454716); Nagappa, Chung et al., PLoS One 2015 (STOP-Bang validation, PMID 26658438); Bornstein et al., J Clin Endocrinol Metab 2016 (Endocrine Society adrenal insufficiency guideline, PMID 26760044); Wong, Weitzer, Longo, Bonilla, Front Psychiatry 2022 (post-COVID fatigue systematic review, PMID 34973396); NICE NG206 2021 (ME/CFS); NICE NG188 (COVID-19 long-term effects); RACGP Red Book. [1]
References
- [1]Kroenke K, Spitzer RL, Williams JB The Patient Health Questionnaire-2: validity of a two-item depression screener Med Care, 2003.PMID 14583691
- [2]Verdon F, Burnand B, Stubi CLF, et al. Iron supplementation for unexplained fatigue in non-anaemic women: double blind randomised placebo controlled trial BMJ, 2003.PMID 12763985
- [3]Krayenbuehl PA, Battegay E, Breymann C, Furrer J, Schulzki N, Hirt A, Favrat B Intravenous iron for the treatment of fatigue in nonanemic, premenopausal women with low serum ferritin concentration Blood, 2011.PMID 21705493
- [4]Bateman L, Bested AC, Bonilla HF, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Essentials of Diagnosis and Management Mayo Clin Proc, 2021.PMID 34454716
- [5]Nagappa M, Liao P, Wong J, Auckley D, Ramachandran SK, Memtsoudis S, Mokhlesi B, Chung F Validation of the STOP-Bang Questionnaire as a Screening Tool for Obstructive Sleep Apnea among Different Populations: A Systematic Review and Meta-Analysis PLoS One, 2015.PMID 26658438
- [6]Bornstein SR, Allolio B, Arlt W, et al. Diagnosis and Treatment of Primary Adrenal Insufficiency: An Endocrine Society Clinical Practice Guideline J Clin Endocrinol Metab, 2016.PMID 26760044
- [7]Ceban F, Ling S, Lui LMW, et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: A systematic review and meta-analysis Brain Behav Immun, 2022.PMID 34973396