Phys · general-medicine
Undifferentiated Fever and Fever of Unknown Origin — Definition, Differential and Staged Diagnostic Approach
Also known as FUO · fever of unknown origin · pyrexia of unknown origin · PUO · undifferentiated fever · prolonged fever · classic FUO · nosocomial FUO · neutropenic FUO · HIV-associated FUO · drug fever · factitious fever · Petersdorf and Beeson criteria · Durack and Street definition
Consultant-physician-depth guide to undifferentiated fever and fever of unknown origin (FUO). Covers the classic Petersdorf and Beeson definition and the modern Durack and Street revision with the four subclasses (classic, nosocomial, neutropenic, HIV-associated); the four diagnostic buckets (infection, malignancy, non-infectious inflammatory disease, miscellaneous) and the high-yield members of each; the focused history (travel, animal exposure, occupation, drugs, immunosuppression); the examination targets including fundoscopy, lymph nodes, murmurs, skin and temporal arteries; the staged investigation protocol from Tier 1 (FBC, CRP, ESR, blood cultures, urinalysis, CXR, HIV) through Tier 2 (autoimmune screen, IGRA, viral serology, echocardiogram, CT chest abdomen pelvis, LDH, beta-2 microglobulin) to Tier 3 (FDG-PET-CT, bone marrow biopsy, temporal artery biopsy, liver biopsy); the principle that empiric antibiotic and steroid therapeutic trials obscure diagnosis and are reserved for the deteriorating patient; factitious and fraudulent fever; and the favourable prognosis of the stable undiagnosed FUO. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Fever and Fever of Unknown Origin — Definition, Differential and Staged Diagnostic Approach

The answer first
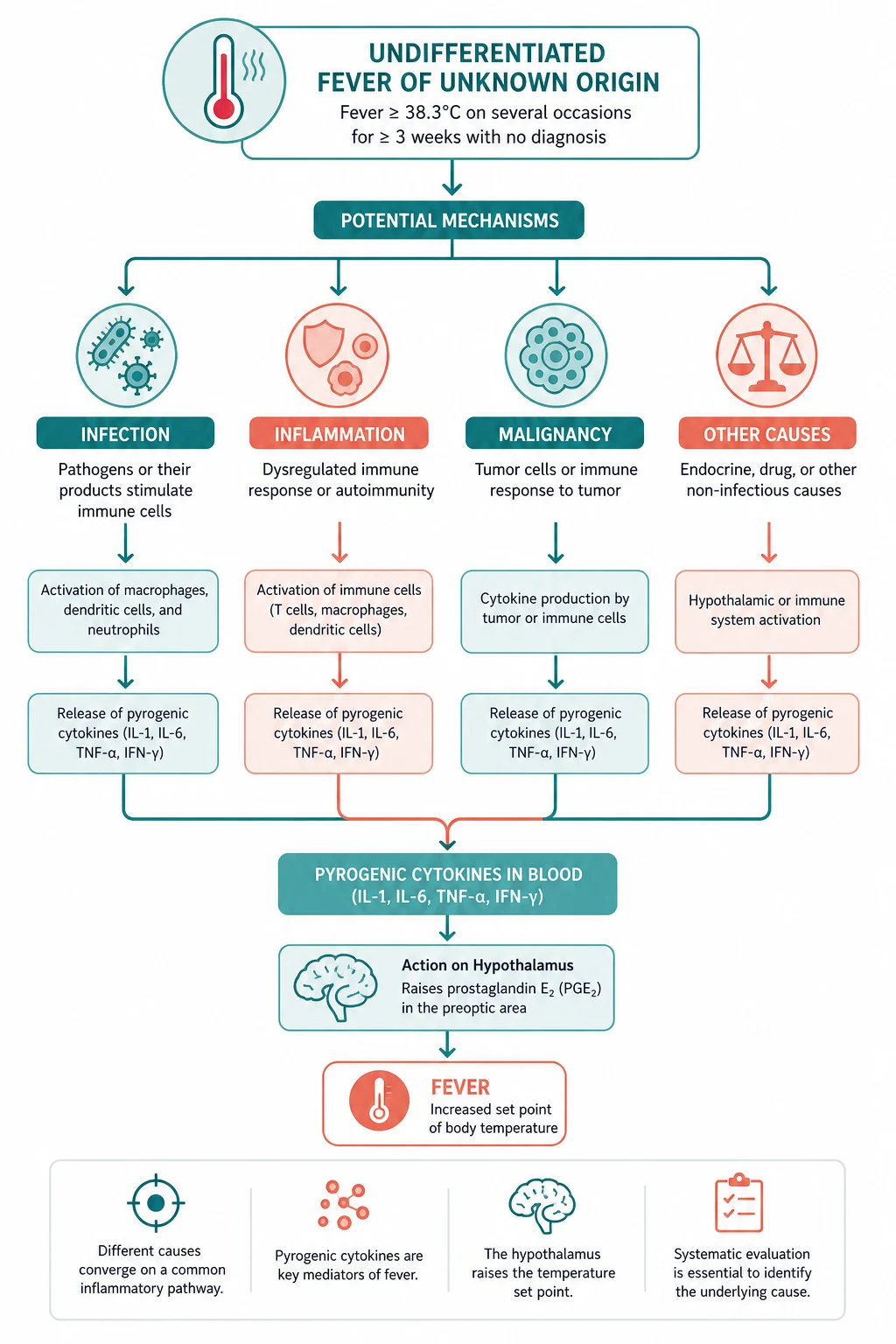
Fever of unknown origin is a syndrome, not a disease. The registrar's job is not to treat a fever but to hunt its cause, and that cause is found by a careful, repeated history and a careful, repeated examination more often than by a scattergun battery of tests. Petersdorf and Beeson defined the syndrome in 1961 — a temperature above 38.3 degrees Celsius on several occasions, lasting more than three weeks, with no diagnosis after one week of inpatient investigation [1] — and that definition has shaped the clinical reasoning for sixty years. The third criterion was modernised by Durack and Street in 1991 to three outpatient visits or three days in hospital, because modern outpatient diagnostics make a week of inpatient investigation unnecessary [2].
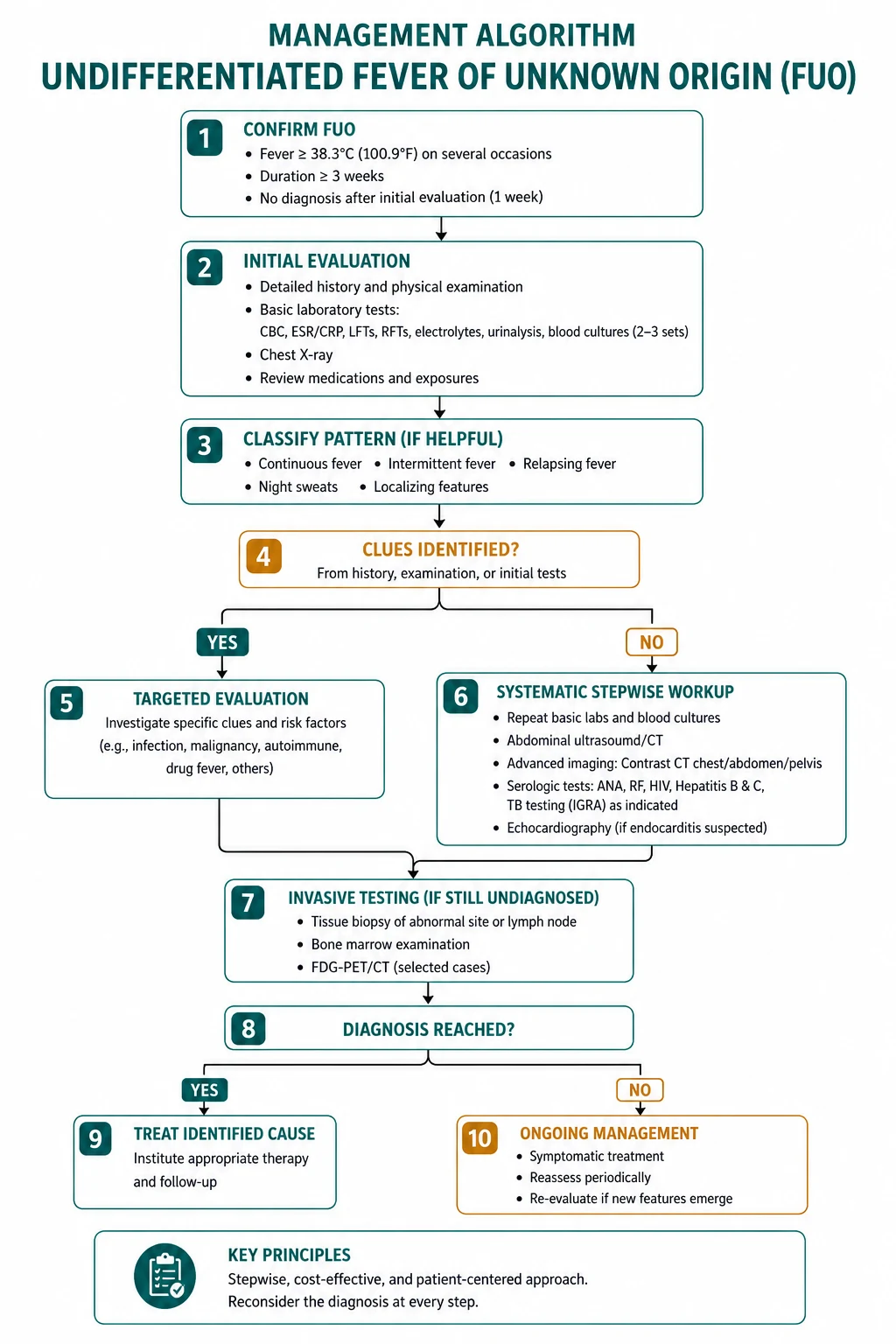
The reproducible sequence for any FUO patient is: [1]
- Confirm the syndrome — verify the temperature, the duration, and the absence of a diagnosis after a competent initial workup.
- Take the focused history — travel, animals, occupation, drugs, immunosuppression, family history, and the fever pattern with its associated symptoms.
- Examine, then examine again — fundoscopy, lymph nodes, murmurs, skin, joints, abdomen, and the temporal arteries in the elderly. The finding that emerges on day 5 is often the one that cracks the case.
- Investigate in stages — Tier 1 (the basic laboratory and microbiological workup), Tier 2 (the targeted autoimmune, microbiological and imaging workup), Tier 3 (FDG-PET-CT and directed biopsy). Each tier is directed by the findings of the last.
- Treat the cause when found; observe the undiagnosed who are stable. Empiric antibiotics and steroids obscure the diagnosis and are reserved for the deteriorating patient. [1]
The single most dangerous error is starting empiric therapy too early — a round of broad-spectrum antibiotics collapses the blood culture yield, a course of steroids masks lymphoma and tuberculosis, and both convert a solvable diagnostic problem into a longer one. The second most dangerous error is the scattergun workup — a battery of undirected tests before a focused history and a careful examination. The diagnosis in FUO is made at the bedside. [1]
Viva trap: "What is the single most important principle in the FUO workup?" The honest answer is never biopsy blindly and never treat empirically unless the patient is deteriorating. Every invasive test should be directed at a lesion found on examination or imaging, and every therapeutic trial should be reserved for the patient whose clinical course no longer permits the luxury of patience. [1]
Definition — the Petersdorf and Beeson criteria, and the Durack and Street revision
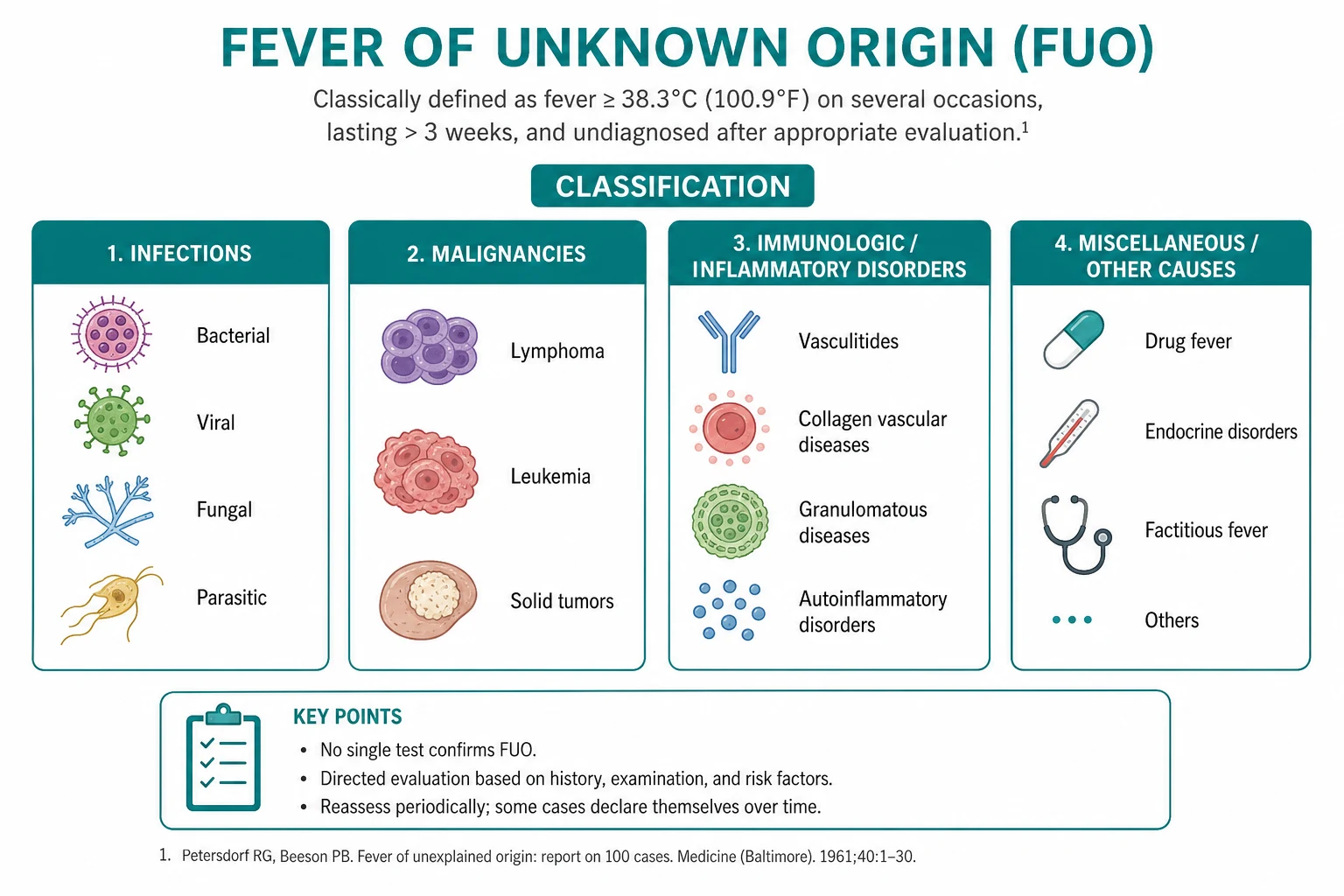
The classic definition of FUO was established by Petersdorf and Beeson in their 1961 report of 100 cases [1]. The three criteria, and the reasoning behind each, are the foundation of the modern approach:
- Temperature above 38.3 degrees Celsius (101 degrees Fahrenheit) on several occasions. The threshold of 38.3 — not the lower 38.0 — excludes the minor diurnal temperature excursions of normal physiology and the "habitual hyperthermia" of anxious or chronically stressed patients. "On several occasions" excludes the single transient spike of a self-limiting viral illness or an isolated environmental exposure.
- Duration of more than three weeks. The three-week threshold excludes the common self-limiting infections — most viral syndromes, bacterial upper respiratory infections, uncomplicated bacterial gastroenteritis — which resolve within two weeks. It also excludes the prolonged but still self-limiting post-viral fatigue syndromes.
- No diagnosis after one week of inpatient investigation. This criterion excludes the patient who has not yet had a competent workup. Petersdorf and Beeson framed it as inpatient investigation because, in 1961, the diagnostic workup required admission for serial blood cultures, imaging, and procedural biopsies. [1]
The third criterion was revised by Durack and Street in 1991 [2]. Modern outpatient diagnostics — day-unit blood cultures, ambulatory CT, same-day echocardiography, outpatient serology — make a week of inpatient investigation unnecessary and, for many patients, inappropriate. The revised criterion is three outpatient visits or three days in hospital, whichever comes first, of active investigation.
Durack and Street also introduced the four subclasses of FUO, because the patient who develops a fever on the transplant ward, or the chemotherapy patient with a neutrophil count of zero, is a fundamentally different problem from the previously well adult with six weeks of unexplained fever [2]:
- Classic FUO — the previously defined syndrome in the immunocompetent adult or child.
- Nosocomial FUO — fever in a hospitalised patient that was not present or incubating on admission, with the investigation threshold met after three days in hospital. The differential is dominated by line infection, surgical site infection, Clostridioides difficile colitis, sinusitis from nasogastric tubes, catheter-related infection, and healthcare-associated pneumonia.
- Neutropenic FUO — fever in a patient with an absolute neutrophil count below 500 per microlitre, with the investigation threshold met after three days. This is a medical emergency governed by the febrile neutropenia algorithm, not the classic FUO algorithm, because the absence of neutrophils allows overwhelming infection with minimal signs.
- HIV-associated FUO — fever in a patient with confirmed HIV infection, with the investigation threshold met after three days as an inpatient or four weeks as an outpatient. The differential is entirely different (opportunistic infection, AIDS-defining malignancy, immune reconstitution inflammatory syndrome). [1]
The practical point the registrar must carry: this topic is about classic FUO. The other three subclasses have their own algorithms, their own differentials, and their own time pressures. The candidate who confuses them has answered the wrong question. [1]
DWE high-yield: The single most examinable definitional fact is the 38.3 degree threshold. A patient with a temperature of 38.0 for six weeks does not meet the FUO definition, however frustrating the clinical picture — the threshold exists precisely to exclude minor thermal excursions. The second most examinable fact is that the third criterion has been modernised to 3 outpatient visits or 3 days in hospital, not 1 week inpatient. The candidate who answers "1 week of inpatient investigation" is correct for the 1961 definition but out of date for the modern definition, and the examiner wants the modern answer qualified by the historical context. [1]
The four diagnostic buckets — and what is in each

Modern prospective series of classic FUO converge on a remarkably stable distribution of causes. The Bleeker-Rovers 2007 prospective multicenter study of 167 patients reported infections in 16 per cent, neoplasms in 7 per cent, non-infectious inflammatory diseases in 22 per cent, miscellaneous causes in 4 per cent, and no diagnosis reached in 51 per cent [3]. The undiagnosed fraction is consistently the largest single category in modern series — a counterintuitive finding that reflects the effectiveness of modern imaging in confirming or excluding the structural causes (infection, abscess, malignancy) and leaving behind a residue of self-limiting inflammatory illness [4].
The four diagnostic buckets, with their high-yield members, are: [1]
Infections (around 20 to 25 per cent of modern classic FUO)
| Infection | Why it causes FUO | High-yield diagnostic clue |
|---|---|---|
| Tuberculosis (extrapulmonary, miliary) | Occult site, paucibacillary, blunted immunology | IGRA, sputum and biopsy AFB, CT for miliary nodules, bone marrow or liver biopsy in disseminated disease |
| Infective endocarditis (including culture-negative) | Intermittent or fastidious bacteraemia | Three sets of blood cultures before antibiotics; Coxiella, Bartonella, HACEK serology if culture-negative; transoesophageal echo; modified Duke criteria |
| Intra-abdominal or pelvic abscess | Walled-off, no bacteraemia | CT abdomen and pelvis with contrast; liver, subphrenic, psoas, pelvic sites |
| Osteomyelitis | Chronic, deep, often spinal | CT and MRI of the spine if back pain; blood cultures; PET-CT localises occult focus |
| Viral — EBV, CMV, HIV | Atypical or prolonged primary infection | Heterophile antibody and EBV serology; CMV PCR; HIV serology is non-negotiable in every FUO |
| Regional — brucellosis, Q fever, melioidosis, leptospirosis, scrub typhus, visceral leishmaniasis | Travel and exposure history is decisive | Region-specific serology; blood cultures on appropriate media (Castaneda for Brucella, Ashdown's for Burkholderia pseudomallei) |
The two infections the registrar must not miss are tuberculosis and infective endocarditis, because both are treatable, both kill if missed, and both are masters of disguise. Extrapulmonary and miliary TB may have a normal chest X-ray and negative sputum; the diagnosis requires IGRA, biopsy of accessible tissue (bone marrow, liver, lymph node) with AFB staining and mycobacterial culture, and a low threshold for empirical anti-TB therapy in the deteriorating patient. Culture-negative endocarditis requires Coxiella burnetii, Bartonella, and HACEK organism serology, a transoesophageal echocardiogram, and the modified Duke criteria applied honestly [4].
Malignancy (around 10 to 20 per cent)
| Malignancy | Why it causes FUO | High-yield diagnostic clue |
|---|---|---|
| Lymphoma (Hodgkin and non-Hodgkin) | Cytokine-driven fever, often without a palpable node | LDH, beta-2 microglobulin, CT CAP for nodal disease, FDG-PET-CT for occult disease, bone marrow biopsy, excisional node biopsy |
| Leukaemia | Marrow infiltration with cytokine release | FBC with differential, peripheral film, flow cytometry, bone marrow biopsy |
| Renal cell carcinoma | Paraneoplastic cytokine release, often before the primary is large | CT abdomen (the classic incidental finding); haematuria may be absent |
| Hepatocellular carcinoma | Inflamed cirrhotic liver | AFP, CT or MRI liver in the at-risk patient |
Lymphoma is the single most important malignancy in FUO. The patient with fever, drenching night sweats and weight loss has lymphoma until proven otherwise, and the proof is anatomical — a node, a marrow focus, a PET-avid lesion. The LDH is a marker of high-grade lymphoproliferative disease and should be in the Tier 2 panel. The blind bone marrow is lower-yield than the directed biopsy of a PET-avid lesion, but it is still performed because it may make the diagnosis when imaging is equivocal. [1]
Non-infectious inflammatory diseases (around 20 to 30 per cent)
| NIID | Why it causes FUO | High-yield diagnostic clue |
|---|---|---|
| Adult-onset Still disease | Spiking fever, evanescent rash, arthralgia | Ferritin in the thousands, a double-quotidian fever, salmon-pink evanescent rash, arthralgia; the Yamaguchi criteria; exclusion of infection and malignancy |
| Giant cell arteritis and polymyalgia rheumatica | Systemic inflammation in the elderly | Age over 50, markedly raised ESR, new headache or jaw claudication, temporal artery tenderness, raised limb girdle pain; temporal artery biopsy |
| ANCA-associated vasculitis and polyarteritis nodosa | Multi-organ inflammation | ANCA, cryoglobulins, hepatitis B and C serology, mesenteric angiography for PAN aneurysms, biopsy of involved tissue |
| Systemic lupus erythematosus | Multi-system autoimmune disease | ANA, anti-dsDNA, complement, urinary sediment; the SLICC or ACR criteria |
| Sarcoidosis | Granulomatous inflammation | Bilateral hilar lymphadenopathy on CXR, ACE level (low specificity), biopsy of involved tissue showing non-caseating granulomas |
| Reactive arthritis and inflammatory bowel disease | Sterile inflammation triggered by infection or mucosal disease | Joint examination, stool studies, colonoscopy and biopsy |
Adult-onset Still disease is the classic examinable NIID because it has a striking phenotype: a spiking (often double-quotidian) fever, an evanescent salmon-pink rash that appears with the fever and fades as it settles, an arthralgia or arthritis, a markedly raised ferritin (often in the thousands) and, characteristically, a response to NSAIDs that is itself diagnostic. The diagnosis is clinical, by the Yamaguchi criteria, and is one of exclusion — infection and malignancy must be ruled out first. [1]
Giant cell arteritis is the NIID most often missed in the elderly FUO patient, because it may present with systemic fever, weight loss and a markedly raised ESR but without the classic headache or jaw claudication. The diagnosis requires a high index of suspicion, a temporal artery biopsy (ideally within one to two weeks of starting steroids to preserve histology), and a low threshold for empirical high-dose steroids — because delay risks irreversible blindness. [1]
Miscellaneous (around 10 to 20 per cent)
The miscellaneous bucket is the catch-all, and it contains some of the most easily missed and most easily treated causes of FUO: [1]
- Drug fever — the patient who has been on the same antibiotic (or anticonvulsant, or allopurinol, or sulfonamide) for a week and develops a new fever, with a relative bradycardia and often an eosinophilia. Cessation of the offending drug is both diagnostic and curative. The fever may take 48 to 72 hours to settle after cessation.
- Deep vein thrombosis and pulmonary embolism — venous thromboembolism causes fever through infarction and inflammation; the D-dimer is unhelpful in FUO because it is usually elevated, but a CT pulmonary angiogram or a Doppler ultrasound of the legs closes the diagnosis.
- Factitious and fraudulent fever — self-induced or simulated. The classic clues are a healthcare-worker background, a fever that does not follow the normal diurnal pattern, the absence of tachycardia during the spike (true fever produces a proportional tachycardia), normal inflammatory markers between spikes, and a charted spike that cannot be reproduced under supervision. The diagnosis is made by a supervised, freshly calibrated temperature measurement.
- Subacute thyroiditis — neck pain, a raised T4 with a suppressed TSH, a markedly raised ESR, and a low radioactive iodine uptake on thyroid scan distinguish it from Graves disease.
- Kikuchi-Fujimoto disease (histiocytic necrotising lymphadenitis) — a self-limiting cervical lymphadenopathy with fever, common in young women of East Asian background, diagnosed by excisional node biopsy; often mistaken for lymphoma.
- Castleman disease — a lymphoproliferative disorder, multicentric cases associated with human herpesvirus 8 (HHV-8), may present with FUO. [1]
DWE exam trap: The most testable epidemiological fact in FUO is that the undiagnosed fraction is the largest single category in modern series. This is not a failure of the workup — it is a consequence of modern imaging excluding the structural causes and leaving behind a residue of self-limiting inflammatory illness that resolves without a diagnosis. The undiagnosed FUO patient who is stable and improving should be observed, not subjected to escalating invasive testing. [1]
The focused history — five domains that change the differential
The history in FUO is not a recitation of the standard medical interview. It is a focused, iterative interrogation of the five domains that actively change the differential. Each domain, and what it changes: [1]
1. Travel and residence
The travel history is decisive in FUO because it shifts the probability of regional infections by orders of magnitude. Malaria is the first consideration in any returning traveller with fever, and thick and thin blood films are non-negotiable in the unstable patient. Enteric (typhoid) fever is considered in travellers to South Asia and parts of Africa. Amebic liver abscess is considered in travellers to endemic areas with right upper quadrant pain. Melioidosis (Burkholderia pseudomallei) is a particular concern in tropical northern Australia and Southeast Asia — it is a great mimic of TB and of abscess, and the culture requires specific media (Ashdown's). Scrub typhus (Orientia tsutsugamushi) is considered in rural tropical Asia and northern Australia, with the classic eschar at the inoculation site. Visceral leishmaniasis is considered in travellers to the Mediterranean, South Asia, East Africa and Latin America, with splenomegaly, pancytopenia and fever. The regional and exposure-specific serology panel should be built around the geography of the patient's travel, not ordered generically. [1]
2. Animal and vector exposure
| Exposure | Infection |
|---|---|
| Cattle, sheep, unpasteurised dairy | Brucellosis |
| Sheep, cattle, parturient cats, abattoir | Q fever (Coxiella burnetii) |
| Rodents, contaminated fresh water | Leptospirosis |
| Birds, especially psittacines | Psittacosis (Chlamydia psittaci) |
| Cats, especially kittens and scratches | Cat-scratch disease (Bartonella henselae) |
| Ticks (bush, endemic regions) | Rickettsial disease (Queensland tick typhus, Flinders Island spotted fever), Lyme-like illness |
| Mosquitoes in endemic regions | Malaria, dengue, chikungunya, Ross River, Barmah Forest, Japanese encephalitis, Murray Valley encephalitis |
3. Occupational and recreational
Abattoir work and veterinary practice raise Q fever and brucellosis. Farming raises Q fever and leptospirosis. Sewage work, mining, and military field training raise leptospirosis. Spelunking (caving) raises histoplasmosis. Hunting raises tularemia and brucellosis. Healthcare work raises the index of suspicion for factitious fever and for needlestick-acquired infection (HIV, hepatitis B and C). [1]
4. Drugs and immunosuppression
The drug chart is reviewed for every drug started in the month before the fever began. Drug fever is most commonly caused by beta-lactam antibiotics, sulfonamides, anticonvulsants (phenytoin, carbamazepine), allopurinol, and the anti-TNF biologics; it may also complicate antituberculous therapy (particularly rifampicin and isoniazid hepatotoxicity) and antifungal therapy. The immunosuppression history shifts the entire differential — a patient on anti-TNF therapy (adalimumab, infliximab, etanercept) is at high risk of TB reactivation, atypical mycobacterial infection, and opportunistic fungal infection; a patient on rituximab is at risk of progressive multifocal leukoencephalopathy and hepatitis B reactivation; a transplant patient is at risk of the full opportunistic spectrum. [1]
5. Family and social history
A family history of autoimmune disease (SLE, vasculitis, inflammatory bowel disease) raises those conditions in the differential. A family history of tuberculosis or of haematological malignancy is relevant. The social history must include a frank assessment of substance use (injecting drug use raises endocarditis, hepatitis, HIV, and soft tissue infection) and of sexual risk (HIV, syphilis). [1]
Fever pattern and associated symptoms
The fever pattern — sustained, intermittent, remittent, tertian, quartan, double-quotidian — is less discriminant than historically taught, but two patterns carry weight: the double-quotidian fever (two spikes in 24 hours) is associated with adult-onset Still disease, miliary TB, and visceral leishmaniasis; and the tertian or quartan periodicity raises malaria. The associated symptoms are more discriminant than the pattern: drenching night sweats and weight loss raise lymphoma and TB; arthralgia and rash raise Still disease, vasculitis, and SLE; back pain raises osteomyelitis, endocarditis (embolic), and psoas abscess; abdominal pain raises abscess, inflammatory bowel disease, and mesenteric vasculitis; a new headache in the elderly raises giant cell arteritis. [1]
The examination — look where the diagnosis hides

The examination in FUO is the single highest-yield diagnostic intervention, and it must be repeated over days. The finding that emerges on day 5 of the workup — a new murmur, a new lymph node, a new skin lesion, a new conjunctival haemorrhage — is often the one that makes the diagnosis. The targets: [1]
- Fundoscopy — the one examination most often omitted and most often rewarding. Roth spots (white-centred haemorrhages) suggest infective endocarditis. Choroidal tubercles suggest miliary tuberculosis. Cytoid bodies suggest SLE. A direct ophthalmoscope at the bedside is sufficient.
- The skin — palms and soles (Janeway lesions and Osler nodes of endocardism); the trunk and proximal limbs (the evanescent salmon-pink rash of Still disease, the erythema nodosum of sarcoid, TB and IBD, the livedo reticularis of polyarteritis nodosa and antiphospholipid syndrome, the petechiae of vasculitis and meningococcaemia); the nailfold (splinter haemorrhages of endocarditis); the conjunctivae (petechiae of endocarditis).
- Lymph nodes — a complete survey including the occipital, pre- and post-auricular, cervical, supraclavicular (Virchow node, a sentinel for upper abdominal malignancy), axillary, epitrochlear, and inguinal regions. A new or changing node is biopsied; excisional biopsy is preferred over core or fine-needle because the nodal architecture is often the diagnosis (lymphoma, Kikuchi, Castleman).
- The heart — a new or changing murmur raises endocarditis even if clinically subtle. The absence of a murmur does not exclude endocarditis, particularly right-sided or culture-negative.
- The abdomen — hepatomegaly, splenomegaly, and localised tenderness (abscess, IBD, mesenteric ischaemia). Rectal examination for a perianal mass or prostate tenderness.
- The joints — synovitis raises Still disease, rheumatoid arthritis, SLE, reactive arthritis, and the seronegative spondyloarthropathies.
- The temporal arteries — in any patient over 50 with an unexplained fever and a raised ESR, palpate the temporal arteries for thickening, tenderness, or an absent pulse. This single examination may prevent blindness from giant cell arteritis.
- Genital examination — epididymal tenderness raises brucellosis and TB. [1]
DCE high-yield: "How do you examine the FUO patient?" The answer that earns marks is the systematic, complete, repeatable examination — fundoscopy, complete skin including palms and soles, complete lymph node survey including epitrochlear and supraclavicular, the cardiovascular system for a new murmur, the abdomen for organomegaly and localised tenderness, the joints, the temporal arteries in the elderly, and the genitalia — and the explicit commitment to repeat the examination daily. The candidate who lists only the standard head-to-toe examination has missed the point. [1]
The staged investigation protocol

The investigation of FUO is staged, not simultaneous. Each tier is directed by the findings of the previous tier. The scattergun battery is the single most common error, because it generates incidental abnormalities that lead the investigation astray. [1]
Tier 1 — the basic workup (every FUO patient)
| Test | What it finds |
|---|---|
| Full blood count with differential | Eosinophilia (drug, parasitic, vasculitis, malignancy); atypical lymphocytes (EBV, CMV); blasts (leukaemia) |
| CRP and ESR | Acute and chronic inflammation; a markedly raised ESR in the elderly raises GCA and myeloma |
| Urea, electrolytes, creatinine | Renal involvement (vasculitis, SLE, subacute endocarditis) |
| Liver function tests | Hepatic involvement (granulomatous disease, lymphoma, viral hepatitis, abscess) |
| Creatine kinase | Myositis (polymyositis, dermatomyositis, rhabdomyolysis from infection) |
| Blood cultures — at least three sets, separate sites, before antibiotics | Continuous bacteraemia (endocarditis) and intermittent bacteraemia (abscess, osteomyelitis) |
| Urinalysis and urine culture | Occult urinary tract infection, and sterile pyuria (TB, leptospirosis, reactive) |
| Chest X-ray | Tuberculosis (military, apical), lymphoma (mediastinal widening), sarcoidosis (bilateral hilar lymphadenopathy), abscess |
| HIV serology | Non-negotiable — HIV changes the entire differential |
| Hepatitis B and C serology | Chronic viral hepatitis, and the context for polyarteritis nodosa (HBV) and cryoglobulinaemia (HCV) |
The single highest-yield test in Tier 1 is three sets of blood cultures drawn before any antibiotic, because a positive culture confirms a bacteraemic infection and identifies the organism and its sensitivities. The HIV test is non-negotiable because HIV itself causes fever and because the differential in the HIV-positive patient is entirely different. [1]
Tier 2 — the targeted workup (directed by Tier 1 and the history and examination)
| Test | What it finds |
|---|---|
| ANA, ANCA, rheumatoid factor, anti-CCP, complement, immunoglobulins | SLE, ANCA-associated vasculitis, rheumatoid arthritis, cryoglobulinaemia, immunodeficiency |
| Interferon-gamma release assay (IGRA) | Prior tuberculosis infection; preferred to tuberculin skin testing in BCG-vaccinated patients |
| Sputum for acid-fast bacilli (3 specimens) and mycobacterial culture | Active pulmonary TB |
| EBV and CMV serology | Primary EBV infection (heterophile, viral capsid antigen IgM, early antigen); CMV infection (IgM and PCR) |
| Region-specific serology (Q fever, brucellosis, leptospirosis, melioidosis, scrub typhus, Bartonella, Coxiella) | The regional and exposure-specific infections — driven by the history |
| Transthoracic echocardiogram (and transoesophageal if suspicion of endocarditis) | Valvular vegetations, intracardiac abscess, perivalvular complication |
| CT of chest, abdomen and pelvis with contrast | The central Tier 2 investigation — localises abscess, malignancy, lymphadenopathy, and guides biopsy |
| Lactate dehydrogenase, beta-2 microglobulin | Lymphoma and lymphoproliferative disease |
| Serum protein electrophoresis, urine Bence-Jones, serum free light chains | Multiple myeloma and plasma cell dyscrasia |
| Serum ferritin | Adult-onset Still disease (ferritin in the thousands), haemophagocytic lymphohistiocytosis, malignancy |
The central Tier 2 investigation is CT of chest, abdomen and pelvis with contrast. It localises abscess, malignancy, lymphadenopathy, and the sites for directed biopsy. It has displaced the older blind investigations — blind liver biopsy, blind bone marrow, laparotomy — from the diagnostic pathway, because a directed biopsy has a far higher yield than a blind one [3].
Tier 3 — the advanced workup (when Tier 1 and Tier 2 are non-diagnostic)
| Test | What it finds |
|---|---|
| FDG-PET-CT | The single highest-yield Tier 3 test — localises occult malignancy (lymphoma), large-vessel vasculitis, focal infection (osteomyelitis, prosthetic joint infection), sarcoidosis, and guides the directed biopsy |
| Bone marrow biopsy | Haematological malignancy, disseminated infection (miliary TB, leishmaniasis, histoplasmosis), haemophagocytic lymphohistiocytosis |
| Temporal artery biopsy | Giant cell arteritis in the elderly patient with raised inflammatory markers and no localising signs |
| Liver biopsy | Granulomatous disease, lymphoma, miliary TB, sarcoid, when LFTs are abnormal without another explanation |
| Targeted tissue biopsy of any abnormality on imaging | Directed by PET-CT or CT — always target a lesion, never biopsy blindly |
FDG-PET-CT has transformed the Tier 3 workup. The Dong meta-analysis of nine studies reported a pooled FDG-PET-CT sensitivity of 0.982 (95 per cent CI 0.936 to 0.998) and specificity of 0.859 (95 per cent CI 0.750 to 0.934) [5]. FDG-PET-CT contributes to a final diagnosis in approximately half to two-thirds of patients in modern series [7], and its greatest value is in directing the biopsy — a PET-avid lesion is biopsied with a far higher yield than a non-targeted site. A negative FDG-PET-CT carries a high negative predictive value for focal malignancy and large-vessel vasculitis, and supports an observational strategy in the stable undiagnosed patient.
The principle that governs invasive investigation in FUO is: never biopsy blindly. Every bone marrow, every liver biopsy, every node biopsy should be directed at a lesion found on examination or imaging. The blind bone marrow is performed when haematological disease is suspected but imaging is non-diagnostic — and it is lower-yield than the directed biopsy of a PET-avid lesion, but it still makes the diagnosis in a minority of cases. [1]
Viva trap: The examiner will ask, "When would you do a FDG-PET-CT in the FUO workup?" The correct answer is after a negative Tier 1 and Tier 2 workup, and before or alongside the invasive biopsy, because the PET-CT identifies the site to biopsy. The candidate who orders PET-CT before the basic workup, or who proceeds to blind biopsy without PET-CT when PET is available, has the sequence wrong. [1]
Management — treat the cause; reserve empiric therapy for the deteriorating patient
The default management of FUO is diagnostic, not therapeutic. The cause is treatable in the majority once found, and the diagnostic workup is itself the treatment pathway. The two therapeutic principles the registrar must carry: [1]
1. Empiric antibiotics are discouraged as a diagnostic manoeuvre
A therapeutic trial of antibiotics in FUO suppresses blood culture yield, selects resistant organisms, causes antibiotic-related complications (particularly C. difficile colitis and line-related infection), and rarely cures a focal infection it has not been directed against. Empiric antibiotics are justified only in three situations: [1]
- The patient is clinically deteriorating — new hypotension, new organ dysfunction, rising lactate, falling platelet count — and the risk of waiting exceeds the risk of treating.
- A single infection is highly probable (for example, miliary TB in a high-risk patient, or culture-negative endocarditis with embolic phenomena) and targeted therapy is justified pending the definitive workup.
- The patient is immunocompromised and febrile — the febrile neutropenia algorithm applies, and empiric broad-spectrum antibiotics are non-negotiable. [1]
2. Empiric steroids are discouraged as a diagnostic manoeuvre
A therapeutic trial of steroids is doubly dangerous in FUO: steroids mask lymphoma (producing a transient defervescence that is mistaken for a steroid-responsive vasculitis), they reactivate TB and fungal infection, and they convert a diagnostic problem into a longer one. The exception is the highly probable giant cell arteritis in the elderly patient with a markedly raised ESR and a threat to vision, in whom a temporal artery biopsy is arranged but steroids are started immediately because the risk of blindness outweighs the diagnostic risk of treatment. The biopsy should ideally be performed within one to two weeks of starting steroids to preserve histology. [1]
3. Symptom control and the prognosis of the undiagnosed
Antipyretics — paracetamol, NSAIDs — are used for symptom control. A fever that defervesces cleanly with NSAIDs is a clinical clue to adult-onset Still disease (which is characteristically responsive to NSAIDs). The prognosis of the undiagnosed FUO after a thorough workup is generally favourable: the majority resolve without a diagnosis and without recurrence, although older patients and those with malignancy have a worse prognosis [4]. The undiagnosed FUO patient who is stable and improving does not benefit from escalating invasive testing — observation is the appropriate strategy.
DWE exam trap: "A 60-year-old man has had fever for six weeks, with a non-diagnostic Tier 1 and Tier 2 workup and a normal CT. What is your next step?" The correct answer is FDG-PET-CT, not empiric steroids or antibiotics. The PET-CT localises occult malignancy, vasculitis and focal infection, and directs the biopsy. The candidate who starts empiric steroids "to see if the fever responds" has committed the classic error — masking lymphoma and TB — and the examiner will follow up with "what if it is lymphoma?" [1]
Factitious and fraudulent fever
Factitious (self-induced) and fraudulent (simulated) fever are rare but real, and they are over-investigated because they are not considered early enough. The classic clues: [1]
- The patient is often a healthcare worker or has access to medical equipment.
- The fever does not follow the normal diurnal pattern — the spike occurs at an unusual hour, often in the late afternoon or evening, and is not preceded by the rigors and malaise of a true fever.
- There is an absence of tachycardia during the spike. True fever produces a proportional tachycardia (approximately 10 beats per minute per 0.5 degrees Celsius), and the absence of tachycardia at a charted temperature of 39.5 degrees is a bedside red flag.
- The inflammatory markers (CRP, ESR) are normal between spikes, and the spikes do not correspond to any culture or imaging abnormality.
- The patient may have self-administered insulin (factitious hypoglycaemia mimicking fever with confusion), or contaminated material (self-inoculated faeces or saliva producing genuine bacteraemia), or simply heated the thermometer (fraudulent, the easiest and most common). [1]
The diagnosis is made by a supervised, freshly calibrated temperature measurement — typically an electronic oral or rectal thermometer, with the patient observed, and the result compared with the charted spike. A simultaneous urine temperature (the freshly passed urine approximates core temperature) is a useful confirmatory test. The conversation is handled with respect, never as an accusation; psychiatry is involved early; the goal is to stop the harm, not to expose or shame the patient. [1]
DCE long-case approach
Patient scenario
Mr James Whitlam, 62, retired park ranger, presents to the outpatient clinic with a six-week history of intermittent fever to 39.2 degrees Celsius, drenching night sweats, 6 kilograms of weight loss, and fatigue. He has a history of treated pulmonary tuberculosis 15 years ago (completed 6 months of rifampicin, isoniazid, pyrazinamide and ethambutol), psoriatic arthritis for which he has taken adalimumab 40 mg subcutaneously every two weeks for the past four years, and diet-controlled type 2 diabetes. He lives with his wife on a rural property in northern New South Wales; he keeps cattle and sheep, and he hunts feral pigs. He has travelled recently to Vietnam (3 months ago). He does not smoke and drinks alcohol occasionally. [1]
On examination: temperature 38.9, pulse 104, blood pressure 122/74, respiratory rate 18, SpO2 97 per cent on room air. He is thin and pale. There is no rash. Lymph node survey reveals a 1.5 cm firm, non-tender supraclavicular node on the left. Heart sounds are normal with no murmur. Chest is clear. Abdomen is soft with a spleen palpable 2 cm below the costal margin. Fundoscopy is normal. [1]
Tier 1 results: haemoglobin 104 g/L (normocytic), white cell count 9.2 with a mild eosinophilia of 0.6, platelets 280. CRP 96, ESR 78. U&E normal. ALT 62, ALP 140. Three sets of blood cultures (drawn before antibiotics) are negative at 5 days. Urinalysis normal. CXR shows bilateral upper zone apical scarring consistent with his old TB, no new infiltrate. HIV serology negative. Hepatitis B and C serology negative. [1]
Candidate's opening statement (SASPOP)
"Mr Whitlam is a 62-year-old retired park ranger who presents with six weeks of fever to 38.9, drenching night sweats, 6 kilograms of weight loss and fatigue. He has treated pulmonary TB 15 years ago, psoriatic arthritis on adalimumab, and diet-controlled type 2 diabetes. He is a rural cattle and sheep farmer, hunts feral pigs, and recently travelled to Vietnam. His main problems are a classic fever of unknown origin with high-risk features for both infection and malignancy — a left supraclavicular lymph node, splenomegaly, raised inflammatory markers, and a mild eosinophilia — in a patient on anti-TNF therapy with prior TB and significant animal and travel exposures. My immediate priorities are to stage the investigation systematically: to confirm the TB status with sputum AFB and IGRA, to exclude infective endocarditis with a transoesophageal echocardiogram given the night sweats and weight loss, to biopsy the supraclavicular node with excisional biopsy, to send region-specific serology for Q fever, brucellosis, melioidosis, leptospirosis and scrub typhus given his exposures, and to perform a CT of chest, abdomen and pelvis followed by FDG-PET-CT if the CT is non-diagnostic, to localise any occult malignancy or focal infection. I would withhold empiric therapy unless he deteriorates, because the workup depends on blood cultures and biopsy that empiric antibiotics or steroids would compromise." [1]
Problem list
- Classic FUO with high-risk features (B symptoms, supraclavicular node, splenomegaly, raised inflammatory markers).
- Lymphoma is the leading malignancy hypothesis — the supraclavicular node, the night sweats, the weight loss, and the splenomegaly.
- Tuberculosis reactivation is the leading infection hypothesis — prior TB, adalimumab therapy, and recent travel to a TB-endemic region.
- Region-specific infection is a serious consideration — Q fever (sheep and cattle), brucellosis (cattle), melioidosis (tropical exposure), scrub typhus (Vietnam), leptospirosis (rodents, fresh water).
- Adalimumab-related risk — reactivation of TB, atypical mycobacterial infection, and the increased risk of lymphoma (hepatosplenic T-cell lymphoma is a rare but recognised association). [1]
Integrated management plan
- Stage the investigation. Confirm the syndrome (already met). Move to a directed Tier 2 workup: IGRA and three sputum samples for AFB (given the prior TB and the anti-TNF therapy); transoesophageal echocardiogram (to exclude endocarditis); excisional biopsy of the supraclavicular node (with mycobacterial and fungal culture in addition to histology, given the TB and the immunosuppression); region-specific serology for Q fever, brucellosis, melioidosis, leptospirosis, scrub typhus and Bartonella; LDH, beta-2 microglobulin, serum protein electrophoresis and serum free light chains; CT of chest, abdomen and pelvis with contrast.
- Withhold empiric therapy unless he deteriorates. The workup depends on the cultures and the biopsy. Empiric steroids would mask lymphoma and TB; empiric antibiotics would suppress the culture yield. The exception is clinical deterioration, which would justify empiric anti-TB therapy given his risk profile.
- Consider PET-CT after the CT. If the CT is non-diagnostic, an FDG-PET-CT localises occult lymphoma, large-vessel vasculitis, and focal infection, and directs the directed biopsy of any avid lesion.
- Hold the adalimumab. The anti-TNF therapy is held during the workup because it may be contributing to the fever (drug fever is less common with biologics than with small molecules, but possible) and because reactivation TB and atypical mycobacterial infection are the central infection hypotheses. The decision to resume is made after the diagnosis is clear.
- Communicate the uncertainty. Explain to Mr Whitlam and his wife that the workup is staged, that several diagnoses are being considered in parallel, and that the most important step is to localise the supraclavicular node for biopsy. Frame the conversation honestly — this is a diagnostic problem and the answer will come from the biopsy and the imaging, not from a single blood test. [1]
Examiner probing questions
"He has been on adalimumab for four years. How does that change your differential and your workup?" "The adalimumab shifts the infection differential decisively — reactivation TB is the central concern, particularly with his prior treated TB and his travel, and atypical mycobacterial infection and opportunistic fungal infection (Pneumocystis, histoplasmosis) are added. The IGRA may be blunted by the anti-TNF therapy and a negative IGRA does not exclude TB. I would send three sputum samples for AFB and mycobacterial culture, and I would culture the lymph node biopsy for mycobacteria and fungi in addition to the standard histology. The adalimumab also adds a small but real risk of hepatosplenic T-cell lymphoma, which is difficult to diagnose on peripheral blood and may require a bone marrow or liver biopsy. I would hold the adalimumab for the duration of the workup, and I would involve the rheumatology and infectious diseases teams early." [1]
"The supraclavicular node is palpable. How do you biopsy it?" "Excisional biopsy is preferred over core or fine-needle aspiration, because the nodal architecture is often the diagnosis — lymphoma is classified by architecture (follicular, diffuse, mantle zone), Kikuchi disease is defined by necrotising histiocytic infiltration, and Castleman disease has a characteristic hyaline-vascular appearance. The node is sent fresh to histology for routine staining, immunohistochemistry, flow cytometry, and mycobacterial and fungal culture. If the node is not accessible to excisional biopsy, a core biopsy is the next best option; fine-needle aspiration is inadequate for lymphoma subtyping." [1]
"The CT shows nothing beyond the palpable node. What is your next investigation?" "An FDG-PET-CT, because it localises metabolically active disease that the anatomical CT misses — occult lymphoma, large-vessel vasculitis, focal infection, sarcoid. The PET-CT also tells me whether the palpable node is the only site or one of several, and it identifies the highest-yield site for directed biopsy if the supraclavicular node is not diagnostic." [1]
"He deteriorates overnight with a temperature of 39.8, a new rigour, and a blood pressure of 92 over 58. What do you do?" "He has crossed from a diagnostic problem to a therapeutic emergency, and empiric therapy is now justified. I repeat the blood cultures, then start broad-spectrum antibiotics covering the most likely pathogens — given his exposures and his anti-TNF therapy, I cover TB (empirical quadruple therapy if TB is the leading hypothesis), atypical mycobacterial infection, melioidosis (meropenem or ceftazidime), brucellosis (doxycycline and gentamicin), and a hospital-acquired pathogen (piperacillin-tazobactam). I involve the infectious diseases team immediately and I admit him to a monitored bed. The deterioration does not abandon the diagnostic workup — the lymph node biopsy proceeds in parallel — but it justifies empiric therapy that would not have been justified in the stable patient." [1]
DCE short-case discussion — the focused examination of the FUO patient
Instruction: "You are asked to examine a 58-year-old woman who has been an inpatient for three weeks with an undiagnosed fever. Describe your systematic examination and the three findings you most hope to elicit." [1]
Systematic examination routine
- End of the bed — the general appearance. Is she cachectic (chronic illness, malignancy, TB)? Is there a rash visible from the door (Still disease, vasculitis)? Is she in pain (the abscess, the osteomyelitis, the mesenteric ischaemia)?
- Vital signs — temperature, pulse, blood pressure, respiratory rate, oxygen saturation. Note the relationship between the temperature and the pulse (relative bradycardia raises drug fever, typhoid, leptospirosis, factitious fever).
- Skin, including palms, soles, nailfold and conjunctiva — Janeway lesions and Osler nodes of endocarditis, splinter haemorrhages, the evanescent rash of Still disease, erythema nodosum, livedo reticularis, petechiae, conjunctival petechiae.
- Fundoscopy — Roth spots, choroidal tubercles, cytoid bodies.
- Lymph node survey — complete, including occipital, pre- and post-auricular, cervical, supraclavicular, axillary, epitrochlear, and inguinal regions.
- Cardiovascular — a careful auscultation for a new murmur, with attention to the timing, the site, the radiation, and the change with posture.
- Respiratory — percussion, expansion, breath sounds, added sounds, and the apical regions in particular for TB.
- Abdomen — hepatomegaly, splenomegaly, localised tenderness, and a rectal examination for a perianal mass or prostate tenderness.
- Joints — a screening for synovitis, with particular attention to the small joints of the hands and wrists, the knees, and the spine.
- Temporal arteries — palpation for thickening, tenderness, or an absent pulse, particularly in the patient over 50.
- Genitalia — epididymal tenderness (brucellosis, TB), penile and vulval ulceration (Behcet disease). [1]
The three findings I most hope to elicit
- A new or changing heart murmur — because it raises infective endocarditis, which is treatable, lethal if missed, and confirmable with a transoesophageal echocardiogram.
- A palpable lymph node, particularly supraclavicular — because it is biopsied, and the biopsy is often the diagnosis (lymphoma, Kikuchi, TB, Castleman, metastatic malignancy).
- A cutaneous clue — a Roth spot, a Janeway lesion, the salmon-pink rash of Still disease, the erythema nodosum of sarcoid — because each of these points to a specific diagnosis and its confirmatory test. [1]
Presentation template
"I have examined Mrs X, a 58-year-old woman with a three-week undiagnosed fever. She is comfortable at rest. Her vital signs are: temperature 38.7, pulse 96, blood pressure 118 over 72, respiratory rate 16, oxygen saturation 98 per cent on room air. Of note, she has a pulse-temperature relationship consistent with true fever. On examination, the key positive findings are: a 1 cm firm, non-tender left supraclavicular lymph node; a soft, apical pansystolic murmur not previously documented; and a palpable spleen 2 cm below the costal margin. There is no rash, no Janeway or Osler lesion, and fundoscopy is normal. The most likely diagnosis given these findings is infective endocarditis or lymphoma, with a number of other diagnoses in the differential. My immediate plan is to repeat the blood cultures, arrange a transoesophageal echocardiogram, and proceed to excisional biopsy of the supraclavicular node." [1]
Discussion questions
Examiner: "What is your working diagnosis, and how would you confirm it?" "My leading diagnosis is lymphoma, given the B symptoms, the supraclavicular node, and the splenomegaly. The competing diagnosis is infective endocarditis, given the new murmur — although the murmur may be functional or pre-existing. I confirm the lymphoma with an excisional biopsy of the node, a CT chest abdomen and pelvis to stage, and an LDH and beta-2 microglobulin. I confirm or exclude the endocarditis with a transoesophageal echocardiogram and the modified Duke criteria, with repeated blood cultures. The two diagnoses are not mutually exclusive — the patient with lymphoma is immunosuppressed and may also have endocarditis — but the node biopsy is the highest-yield next step." [1]
Examiner: "How do you decide when to stop investigating?" "I stop investigating when a thorough staged protocol is negative and the patient is stable or improving. The undiagnosed FUO after a competent workup — including a non-diagnostic CT and a negative FDG-PET-CT, with no localising signs on a careful repeated examination — is generally a self-limiting inflammatory illness with a favourable prognosis. I would arrange outpatient review, document the workup and the findings, and reassure the patient. I would not escalate to invasive testing — blind bone marrow, blind liver biopsy, laparoscopy — unless a new localising sign emerges or the fever recurs with new features. The principle is that the undiagnosed FUO that is getting better is best observed; the undiagnosed FUO that is getting worse is re-investigated from the beginning." [1]
Examiner: "What is the single most important piece of advice you would give a registrar starting an FUO workup?" "Take the history again, examine the patient again, and repeat the examination daily. The diagnosis in FUO is made at the bedside more often than in the laboratory, and the finding that emerges on day 5 of the workup is often the one that cracks the case. The registrar who orders a scattergun battery of tests before a focused history and a careful examination will be led astray by incidental abnormalities. The registrar who stages the workup, who waits for the cultures and the imaging, and who examines the patient every day will find the cause." [1]
Key DWE MCQ patterns
- Recognise the FUO definition. A patient with a temperature of 38.0 for six weeks does not meet the definition — the threshold is 38.3. A patient with a temperature of 38.5 for two weeks does not meet the definition — the duration is three weeks. A patient with a temperature of 38.5 for three weeks, undiagnosed after two outpatient visits, is on the way to meeting the definition but has not yet — the third criterion is three outpatient visits or three days in hospital.
- Identify the highest-yield next investigation. The CT chest abdomen and pelvis is the central Tier 2 investigation; the FDG-PET-CT is the central Tier 3 investigation; the blood cultures before antibiotics are the highest-yield Tier 1 microbiological test.
- Recognise the empiric-therapy trap. A patient with FUO who is deteriorating is a candidate for empiric therapy; a patient with FUO who is stable is not, because the therapy will obscure the diagnosis.
- Identify the regional infection by the history. A rural Australian farmer with sheep exposure and a fever has Q fever until proven otherwise; a returned traveller from Southeast Asia with fever has melioidosis, scrub typhus, typhoid, or malaria on the differential; a returned traveller from South Asia with fever has enteric fever, malaria, or visceral leishmaniasis.
- Recognise adult-onset Still disease. The double-quotidian fever, the evanescent salmon-pink rash, the arthralgia, the ferritin in the thousands, and the NSAID responsiveness.
- Recognise giant cell arteritis in the elderly FUO patient. The age over 50, the markedly raised ESR, the new headache or jaw claudication, and the temporal artery biopsy as the confirmatory test.
- Recognise culture-negative endocarditis. The patient with FUO, a new murmur, and negative routine cultures requires Coxiella, Bartonella, and HACEK serology and a transoesophageal echocardiogram. [1]
References
[1] Petersdorf RG, Beeson PB. Fever of unexplained origin: report on 100 cases. Medicine (Baltimore) 1961;40:1–30. The foundational study that defined the syndrome of fever of unknown origin with the three classic criteria — temperature above 38.3 degrees, duration above 3 weeks, no diagnosis after 1 week of inpatient investigation — and established the framework that has shaped the clinical reasoning for sixty years.
[2] Durack DT, Street AC. Fever of unknown origin — reexamined and redefined. Current Clinical Topics in Infectious Diseases 1991;11:35–51. The modernisation of the classic definition, replacing the third criterion (1 week inpatient investigation) with 3 outpatient visits or 3 days in hospital, and the introduction of the four subclasses (classic, nosocomial, neutropenic, HIV-associated) that recognise the different spectrum and urgency of the immunocompromised and hospitalised patient.
[3] Bleeker-Rovers CP, Vos FJ, de Kleijn EMHA, et al. A prospective multicenter study on fever of unknown origin: the yield of a structured diagnostic protocol. Medicine (Baltimore) 2007;86(1):26–38. The prospective multicenter study of 167 patients with classic FUO showing the modern distribution of causes — infections 16 per cent, neoplasms 7 per cent, non-infectious inflammatory diseases 22 per cent, miscellaneous 4 per cent, no diagnosis reached 51 per cent — and the yield of a staged diagnostic protocol with imaging-directed biopsy.
[4] Hayakawa K, Ramasamy B, Chandrasekar PH. Fever of unknown origin: an evidence-based review. Am J Med Sci 2012;344(4):307–16. The evidence-based review that synthesises the modern approach to classic FUO — the four subclasses, the staged diagnostic protocol, the role of FDG-PET-CT, and the favourable prognosis of the undiagnosed patient after a thorough workup.
[5] Dong MJ, Liu C, Zhao D, et al. A meta-analysis of the value of fluorodeoxyglucose-PET/PET-CT in the evaluation of fever of unknown origin. Eur J Radiol 2011;80(3):834–44. The pooled analysis of nine studies reporting a PET-CT sensitivity of 0.982 (95 per cent CI 0.936 to 0.998) and specificity of 0.859 (95 per cent CI 0.750 to 0.934), establishing FDG-PET-CT as the central Tier 3 investigation for localising occult malignancy, vasculitis, and focal infection.
[6] Wright WF, Auwaerter PG. Fever and fever of unknown origin: review, recent advances, and lingering dogma. Open Forum Infect Dis 2020;7(5):ofaa132. The modern review covering the pathophysiology of fever, the lingering dogma of the normal 37 degree temperature, the role of modern imaging including FDG-PET, and the principle that clinical judgement remains paramount.
[7] Wright WF, Durso SC, Forry C, Rovers CP. Fever of unknown origin. BMJ 2025;386-2:e080847. The current authoritative review of classic FUO in the immunocompetent adult, covering the updated diagnostic criteria, the four diagnostic buckets, the staged investigation with FDG-PET-CT as a central Tier 3 test, and the management principle that empiric therapy is reserved for the deteriorating patient.
Petersdorf and Beeson, Medicine (Baltimore) 1961; Durack and Street, Current Clinical Topics in Infectious Diseases 1991; Bleeker-Rovers et al., Medicine (Baltimore) 2007; Hayakawa et al., Am J Med Sci 2012; Dong et al., Eur J Radiol 2011; Wright and Auwaerter, Open Forum Infect Dis 2020; Wright et al., BMJ 2025; Therapeutic Guidelines eTG Antibiotic (ANZ); NICE Clinical Knowledge Summaries; EANM 2024 FDG-PET consensus; IDSA practice guidelines. [1]
References
- [1]Petersdorf RG, Beeson PB Fever of unexplained origin: report on 100 cases Medicine (Baltimore), 1961.PMID 13734791
- [2]Durack DT, Street AC Fever of unknown origin--reexamined and redefined Curr Clin Top Infect Dis, 1991.PMID 1651090
- [3]Bleeker-Rovers CP, Vos FJ, de Kleijn EM, Mudde AH, Dofferhoff TS, Richter C, Smilde TJ, Krabbe PF, van Dijk AP, van der Meer JW, Oyen WJ A prospective multicenter study on fever of unknown origin: the yield of a structured diagnostic protocol Medicine (Baltimore), 2007.PMID 17220753
- [4]Hayakawa K, Ramasamy B, Chandrasekar PH Fever of unknown origin: an evidence-based review Am J Med Sci, 2012.PMID 22475734
- [5]Dong MJ, Liu C, Zhao D, Yang MF, Liu Z, Wang Q, Zhao J A meta-analysis of the value of fluorodeoxyglucose-PET/PET-CT in the evaluation of fever of unknown origin Eur J Radiol, 2011.PMID 21131151
- [6]Wright WF, Auwaerter PG Fever and Fever of Unknown Origin: Review, Recent Advances, and Lingering Dogma Open Forum Infect Dis, 2020.PMID 32462043
- [7]Wright WF, Durso SC, Forry C, Rovers CP Fever of unknown origin BMJ, 2025.PMID 39761983