Phys · general-medicine
Undifferentiated Lymphadenopathy — A Systematic Diagnostic Approach
Also known as lymphadenopathy · enlarged lymph nodes · swollen glands · lymph node enlargement · cervical lymphadenopathy · supraclavicular lymphadenopathy · axillary lymphadenopathy · inguinal lymphadenopathy · generalised lymphadenopathy · Virchow node · Troisier sign · infectious mononucleosis · B symptoms · excisional biopsy · International Prognostic Index · R-IPI · Lugano classification · Kikuchi-Fujimoto disease · cat-scratch disease · pseudolymphoma
Consultant-physician-depth guide to the diagnostic approach to the patient with lymph node enlargement of unknown cause. Covers the localised-versus-generalised framework and its regional differentials (cervical, supraclavicular Virchow, axillary, inguinal, epitrochlear), the generalised causes (infection — EBV infectious mononucleosis, CMV, HIV, TB, toxoplasmosis, syphilis; haematological — Hodgkin and non-Hodgkin lymphoma, CLL, ALL; autoimmune — SLE, RA, sarcoid; drug — phenytoin pseudolymphoma; metastatic malignancy), the focused history and examination discriminators (node size, consistency, mobility, tenderness, matting; the B symptoms of lymphoma; the exposure history), the red-flag features that mandate biopsy (supraclavicular node, hard fixed node, node above 2 cm, persistence beyond 6 weeks, B symptoms, hepatosplenomegaly), the first-tier investigations (FBC, film, LDH, EBV serology, HIV, toxoplasma, syphilis, chest X-ray, ultrasound), the biopsy decision (excisional biopsy as the gold standard for lymphoma, FNA for metastatic or infective, core biopsy when excision is not feasible), the Lugano classification and the revised International Prognostic Index, and lymphadenopathy in the immunocompromised host. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Lymphadenopathy — A Systematic Diagnostic Approach

The answer first
The patient with lymphadenopathy of unknown cause is one of the commonest and most diagnostically loaded presentations in general medicine. The cause spans infection, haematological malignancy, metastatic carcinoma, autoimmune disease and drugs, and the registrar's job is to use the localised-versus-generalised distinction as the organising framework, then to discriminate by the node characteristics and the red-flag features, and finally to make the biopsy decision — because a node that meets a red-flag criterion is biopsied, not observed. [1]
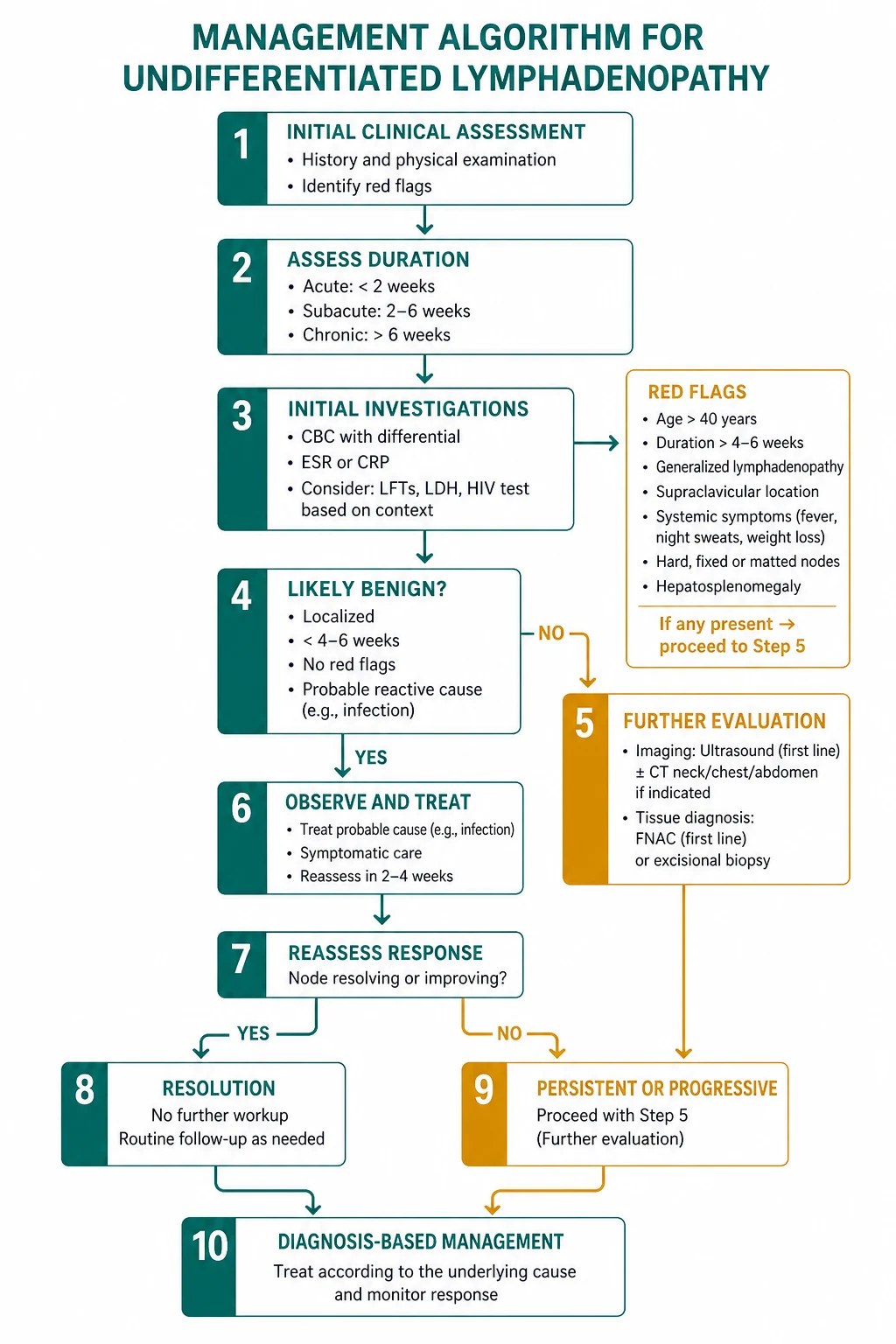
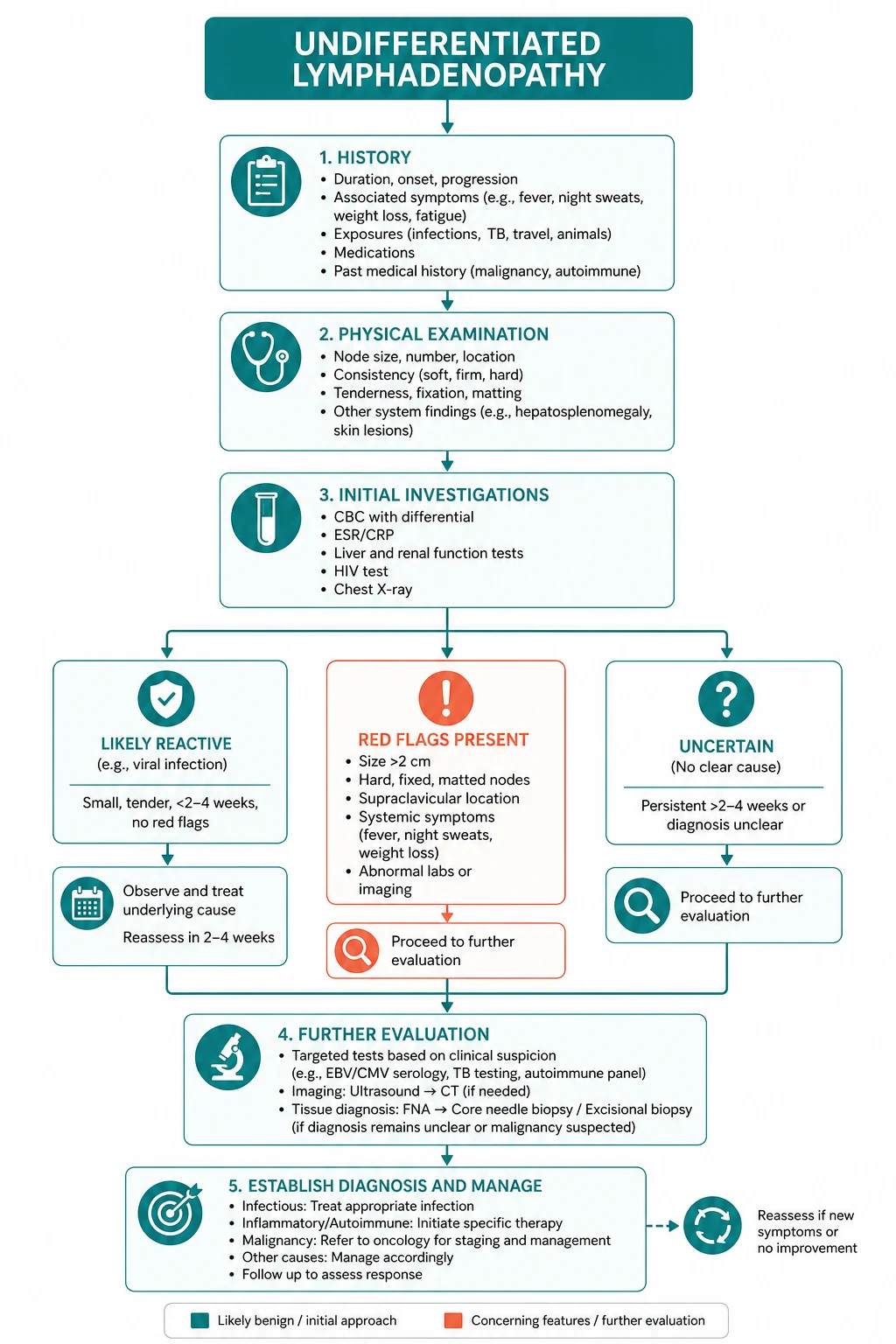
The reproducible sequence for any lymphadenopathy assessment is: [1]
- Characterise the node — size (with a ruler), consistency (soft, rubbery, hard), mobility (mobile, tethered, fixed), tenderness, matting, and the overlying skin. Examine all node groups, not just the one the patient noticed.
- Classify as localised or generalised — localised points to the drainage territory or a regional malignancy; generalised indicates a systemic process (infection, haematological, autoimmune, drug).
- Apply the red-flag screen — supraclavicular location, hard or fixed, above 2 cm, persisting beyond 4 to 6 weeks, B symptoms, hepatosplenomegaly. Any red flag mandates biopsy.
- If no red flags and a plausible reactive cause is present (a viral URTI, a local skin infection), observe for 3 to 4 weeks and reassess. A node that persists or grows at 4 weeks is biopsied.
- Make the biopsy decision correctly — excisional biopsy is the gold standard for suspected lymphoma because it preserves the architecture and provides tissue for immunohistochemistry and flow cytometry. FNA is acceptable for the suspected metastatic carcinoma or the infective node, but FNA alone is never adequate for the primary diagnosis of lymphoma. [1]
The single most dangerous error is observing a supraclavicular node. Any supraclavicular node in an adult is a red flag, full stop — the left (Virchow node, signal node) drains the abdominal cavity via the thoracic duct and classically signals gastric, pancreatic or other intra-abdominal malignancy; the right drains the mediastinum, right lung and oesophagus. The registrar who reassures a patient with a left supraclavicular node that "it's probably nothing" and observes for a month has lost time that the underlying malignancy will use. The second error is giving corticosteroids before a tissue diagnosis — steroids can mask the histology of lymphoma by inducing apoptosis in the lymphoma cells and distorting the nodal architecture, and a registrar who prescribes prednisone for a suspected reactive node that is in fact lymphoma has compromised the diagnostic tissue. [1]
Viva trap: "What is the single most useful piece of information in the first minute with a lymph node?" The honest answer is the location. A left supraclavicular node is a different patient from an anterior cervical node in a 20-year-old with a sore throat, and the location alone sets the malignancy probability and the threshold to biopsy. The registrar who locates the node precisely and examines all the other groups before reaching for the investigation form has organised the entire encounter. [1]
Why the localised-versus-generalised distinction is the organising framework

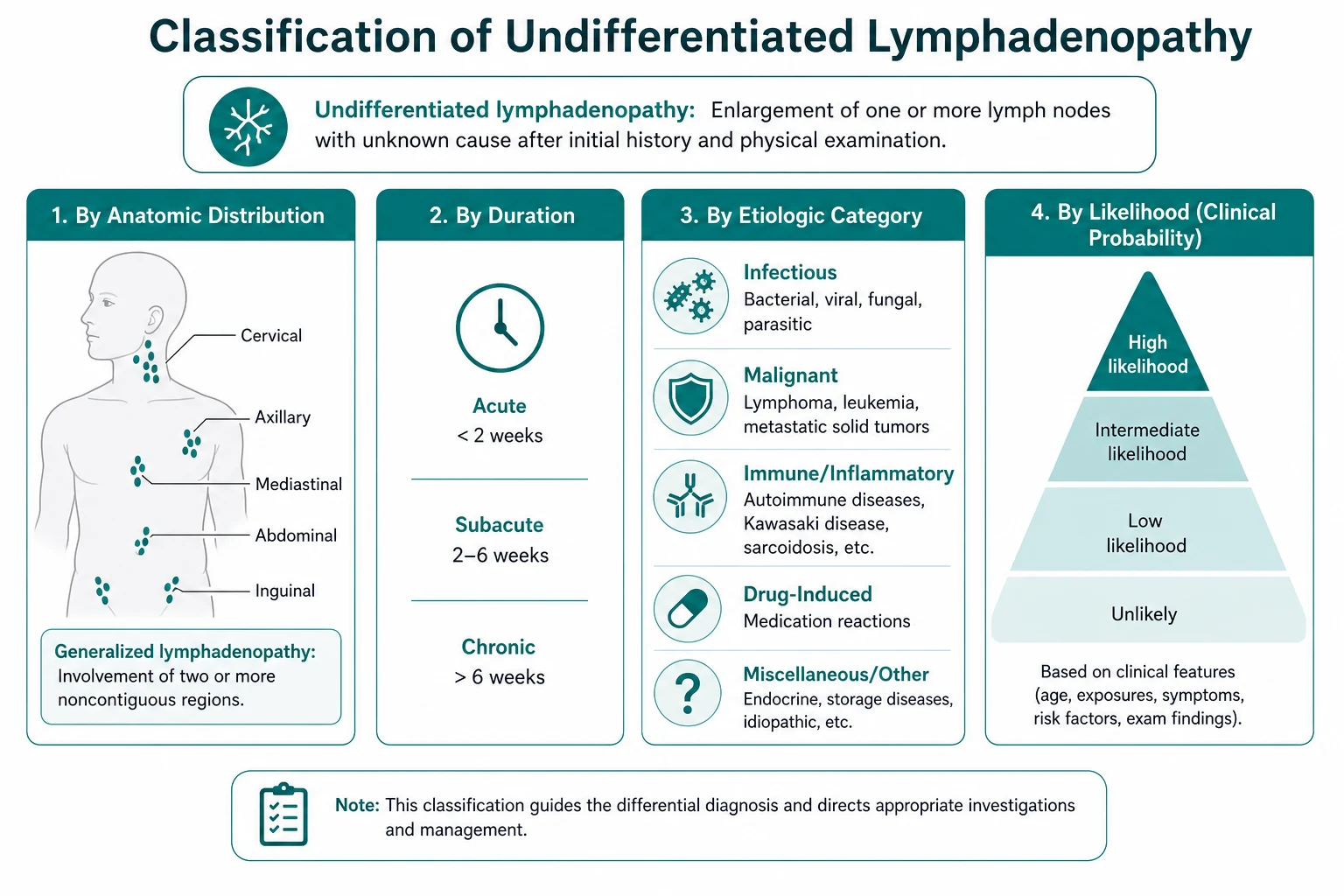
Lymphadenopathy is defined as a palpable enlargement of the lymph nodes. A node is considered enlarged when it exceeds 1 cm in most sites, 0.5 cm in the epitrochlear region, or any size in the supraclavicular, iliac or popliteal fossae [1]. The definition matters clinically because it tells the registrar which nodes are abnormal on palpation: an epitrochlear node of 6 mm is abnormal, and a supraclavicular node of any size is abnormal and is a red flag.
The distinction between lymphadenopathy (enlargement from any cause) and lymphadenitis (enlargement from acute inflammation, typically tender, warm and overlying erythema) frames the first clinical question. The tender, warm, erythematous node is lymphadenitis, and the differential is acute bacterial or atypical infection; the painless node is the diagnostic challenge, because it may be reactive, malignant, granulomatous or drug-related, and the discrimination rests on the history and the node characteristics. [1]
The localised-versus-generalised distinction is the organising framework because each carries a different differential and a different pre-test probability of malignancy. [1]
Localised lymphadenopathy
Localised lymphadenopathy is enlargement confined to a single anatomical region. The first question is which region, because each region has a characteristic differential and a characteristic primary drainage territory that must be examined: [1]
- Cervical (anterior triangle). The commonest localised lymphadenopathy. In the young patient, the differential is reactive — viral URTI, infectious mononucleosis from EBV, CMV, toxoplasmosis. In the older patient, the differential shifts to malignancy — lymphoma (Hodgkin and non-Hodgkin), head and neck squamous cell carcinoma (oral cavity, oropharynx, larynx, nasopharynx), thyroid cancer, and metastatic from a scalp or skin primary. The registrar examines the skin of the head and neck, the oral cavity (with attention to the base of tongue and the floor of mouth), the oropharynx, and the thyroid.
- Cervical (posterior triangle) and occipital. The posterior triangle drains the scalp and the back of the neck; the occipital nodes drain the scalp. The differential includes scalp skin conditions (seborrhoeic dermatitis, tinea capitis, pediculosis), local skin infection, and in the older patient, melanoma or squamous cell carcinoma of the scalp. The registrar examines the scalp through the hair.
- Supraclavicular. The single highest-risk location. A left supraclavicular node (Virchow node, signal node) drains the abdominal cavity via the thoracic duct and classically indicates gastric, pancreatic, hepatic, renal or testicular malignancy; the eponym Troisier sign describes an enlarged left supraclavicular node accompanying an intra-abdominal primary. A right supraclavicular node drains the mediastinum, the right lung and the oesophagus, and classically indicates lung cancer, oesophageal cancer or mediastinal lymphoma. Any supraclavicular node of any size in an adult is a red flag and mandates biopsy rather than observation.
- Axillary. The axillary nodes (apical, central, pectoral, lateral, subscapular groups) drain the breast, the arm, the hand, and the chest wall. The differential includes breast cancer, skin and soft tissue infection of the arm or hand, cat-scratch disease from a scratch on the hand, lymphoma, melanoma (the primary may be on the arm, the chest wall or the back), hidradenitis suppurativa, and the reactive node after a BCG vaccination in the ipsilateral arm. The registrar examines both breasts, the chest wall, the whole arm and hand, and the skin of the upper trunk.
- Epitrochlear. The epitrochlear node drains the medial forearm and the ulnar aspect of the hand. Any palpable epitrochlear node above 5 mm is abnormal. The differential includes secondary syphilis, lymphoma, infectious mononucleosis, and skin infection of the hand or forearm. An epitrochlear node is a classic exam finding in secondary syphilis and in non-Hodgkin lymphoma, and the registrar who dismisses one as reactive has missed a red flag.
- Inguinal. The inguinal nodes (horizontal and vertical groups) drain the lower limb, the external genitalia, the perineum, the lower anal canal, and the lower abdominal wall. The differential is broad — STI (syphilis, chancroid, lymphogranuloma venereum, herpes simplex), skin and soft tissue infection of the leg, lymphoma, metastatic from skin (melanoma, squamous), vulvar, penile or anal squamous cancer, and cat-scratch. The registrar examines the skin of the legs, the external genitalia, and performs a digital rectal examination when an anal or rectal primary is suspected. A small number of small, mobile, non-tender inguinal nodes are common in adults from the recurrent minor skin trauma of the lower limb, and are not, by themselves, a red flag — but a single dominant, hard or enlarging inguinal node is investigated. [1]
Generalised lymphadenopathy
Generalised lymphadenopathy is enlargement in two or more non-contiguous anatomical regions. It indicates a systemic process, and the differential is: [1]
- Infection. EBV (infectious mononucleosis), CMV, primary HIV infection (acute retroviral syndrome) or AIDS, disseminated tuberculosis, toxoplasmosis, secondary syphilis, brucellosis, viral exanthems (measles, rubella), and in the returning traveller, dengue and other tropical infections.
- Haematological. Hodgkin lymphoma, non-Hodgkin lymphoma, chronic lymphocytic leukaemia (CLL), acute lymphoblastic leukaemia (ALL), acute myeloid leukaemia (AML), and the rare haemophagocytic lymphohistiocytosis (HLH).
- Autoimmune and inflammatory. Systemic lupus erythematosus, rheumatoid arthritis, sarcoidosis, Kikuchi-Fujimoto disease, dermatomyositis, adult-onset Still disease.
- Drug-induced (pseudolymphoma). Phenytoin is the classic cause; others include carbamazepine, allopurinol, the sulfonamides, the penicillins, atenolol and captopril. The node regresses on drug withdrawal, and the registrar who asks the drug history has uncovered a reversible cause.
- Metastatic malignancy. Disseminated carcinoma — melanoma, breast, lung, gastric, renal — with deposits in multiple node chains. [1]
DWE high-yield: The single most testable fact about generalised lymphadenopathy is that the pre-test probability of a serious cause is much higher than in localised lymphadenopathy, and the threshold to investigate is correspondingly lower. A generalised lymphadenopathy in an adult with B symptoms is investigated for lymphoma and for the systemic infections (HIV, EBV, TB) in parallel from the first encounter — the observation period that is reasonable for a localised cervical node in a young patient with a viral illness does not apply. [1]
The focused history — the questions that change the differential
The history in lymphadenopathy is high-yield precisely because each answer narrows the differential. The registrar should ask, in order: [1]
Onset, duration and progression. Acute onset (days) with tenderness points to infection — a viral URTI, a local skin infection, an acute lymphadenitis. Insidious onset (weeks to months) with a painless enlarging node points to malignancy (lymphoma, metastatic carcinoma) or a chronic infection (tuberculosis). A node that is growing is investigated; a node that is static or regressing may be observed if there are no other red flags. [1]
Pain. Painful nodes suggest infection (acute capsule stretch) or rapid growth (the lymphoma that is enlarging quickly may be tender). Painless nodes suggest chronic inflammation, malignancy or tuberculosis. The registrar must not be falsely reassured by pain — an enlarging lymphoma can be tender, and the absence of pain does not exclude malignancy. [1]
The B symptoms. The B symptoms — drenching night sweats (soaking the sheets, not mild diaphoresis), unintentional weight loss (more than 10 per cent body weight over 6 months) and unexplained fever — are the B-symptom triad of lymphoma. They must be asked explicitly and separately, because the patient often does not volunteer them, and each independently raises the pre-test probability of lymphoma. Their presence with any lymphadenopathy mandates investigation for haematological malignancy. In the Lugano classification, the A/B symptom designation is now applied to Hodgkin lymphoma only, because it lacks prognostic value in most non-Hodgkin lymphomas [5] — but in the undifferentiated patient, the B symptoms remain a red flag that drives the work-up, regardless of the eventual lymphoma subtype.
Localising symptoms. The registrar asks about the throat (sore throat, tonsillar exudate — infectious mononucleosis, head and neck cancer), the skin (any new lesion, ulcer, changing mole — the primary that drains to the node), the breast (any lump or change — the axillary node), the thyroid (any neck swelling or voice change — the cervical node), the chest (cough, haemoptysis — the lung primary draining to the supraclavicular or mediastinal nodes), the abdomen (abdominal pain, dyspepsia, change in bowel habit, melena — the gastric primary draining to the left supraclavicular node), and the genitourinary system (any testicular swelling, any perineal lesion — the inguinal node). [1]
Exposure history. The exposure history is a high-yield discriminator that is often under-asked. The specific exposures: [1]
- Cats — Bartonella henselae, cat-scratch disease. Ask about recent scratches or bites, especially kittens.
- Undercooked meat — Toxoplasma gondii. Ask about the consumption of undercooked pork or lamb.
- Farm animals and unpasteurised milk — Brucella. Relevant in the patient with a rural or occupational exposure.
- Tuberculosis contact or country of origin — Ask about TB contacts, a country of origin with a high TB prevalence, and prior BCG vaccination.
- Tick exposure — Borrelia burgdorferi (Lyme disease), Rickettsia (in ANZ, the spotted fevers and scrub typhus).
- IV drug use and sexual exposure — HIV, hepatitis B and C, secondary syphilis. The sexual history must be explicit: number of partners, new partners, condom use, history of STI, and in the patient at risk, the HIV test is non-negotiable.
- Travel — The returning traveller from a tropical region has a broader differential (dengue, typhoid, malaria, viral haemorrhagic fever, and the regional mycoses).
- Blood transfusion — HIV, hepatitis C, EBV, CMV. [1]
Drug history. The drug history uncovers the pseudolymphoma syndrome. The classic culprits are phenytoin (the textbook cause), carbamazepine, allopurinol, the sulfonamides, the penicillins, atenolol and captopril. The node regresses on drug withdrawal, and a careful drug history spares the patient a biopsy. The registrar who omits the drug history in a patient with generalised lymphadenopathy on phenytoin has missed the diagnosis. [1]
Past history and constitutional history. The registrar asks about prior malignancy (the lymphadenopathy may be a recurrence or a new primary), prior transplant or immunosuppression (which broadens the differential to include the opportunistic infections and the post-transplant lymphoproliferative disorder), autoimmune disease (SLE, RA), recurrent infections suggesting an immunodeficiency, and occupational exposure (veterinary workers, farmers, abattoir workers). [1]
The examination — what changes the differential and the urgency

The examination begins with the node characteristics, then extends to all node groups, then to the primary drainage sites, and finally to the systemic signs. The registrar who examines only the node the patient noticed has examined only a fraction of the patient. [1]
The node characteristics
Each node is characterised by five features at the bedside: [1]
- Size. Measure with a ruler, never an estimate. A node greater than 1 cm in most sites, greater than 0.5 cm in the epitrochlear region, or any size in the supraclavicular fossa is abnormal [1]. Nodes greater than 2 cm without an obvious infective cause are concerning; nodes greater than 3 cm in the cervical chain are highly concerning.
- Consistency. Soft and mobile is reactive (the viral illness, the local skin infection). Rubbery is the classic consistency of lymphoma — a Hodgkin lymphoma node is classically "rubbery." Hard is metastatic carcinoma (the stony-hard node of metastatic squamous cell carcinoma). Matted nodes (a conglomerate that moves as a single mass) suggest malignancy or tuberculosis.
- Mobility. Mobile nodes are reactive or early lymphoma. Tethered nodes are more advanced. Fixed nodes — fixed to the skin or to the deep structures — indicate advanced malignancy or invasive infection (tuberculosis).
- Tenderness. Tender is infection or rapid capsule stretch. Painless is malignancy or chronic inflammation. The registrar must not be falsely reassured by pain.
- The overlying skin. Erythema, warmth and fluctuance suggest abscess or acute lymphadenitis. A sinus tract suggests tuberculosis or actinomycosis. An ulcerated overlying lesion may be the primary (the melanoma, the squamous cell carcinoma).
All node groups
The systematic examination of all node groups, in order, prevents the error of classifying a localised node as generalised (or vice versa) by an incomplete examination: [1]
- Occipital — drains the scalp.
- Pre-auricular and post-auricular — drain the scalp, the external ear and the face.
- Submental and submandibular — drain the floor of mouth, the tongue tip and the lower lip.
- Upper, middle and lower deep cervical (anterior triangle) — drain the oral cavity, the oropharynx, the nasopharynx, the larynx and the thyroid.
- Posterior triangle — drains the back of the scalp, the neck and the nasopharynx (the nasopharyngeal primary classically spreads to the posterior triangle).
- Supraclavicular (left and right) — palpated from behind the patient, with the patient's head slightly flexed forward to relax the sternocleidomastoid, and the examiner's fingers placed deep to the clavicle in the supraclavicular fossa. The registrar who palpates the supraclavicular fossa from the front with the patient's head extended misses the node.
- Axillary — with the patient's arm supported by the examiner's hand, palpate against the chest wall in all five positions (apical, central, pectoral, lateral, subscapular). The registrar who examines the axilla with the patient's arm raised and unsupported misses the central and apical nodes.
- Epitrochlear — with the patient's elbow flexed, palpate 2 to 3 cm above the medial epicondyle, in the groove between the biceps and the triceps. Any palpable epitrochlear node above 5 mm is abnormal.
- Intraclavicular.
- Inguinal (horizontal and vertical groups) — the horizontal group runs along the inguinal ligament; the vertical group runs along the saphenous vein.
- Popliteal. [1]
The deep node groups — the mediastinal, the hilar, the para-aortic, the iliac and the mesenteric — are assessed by imaging, not by palpation. A chest X-ray showing mediastinal or hilar widening raises the question of mediastinal lymphadenopathy; an abdominal CT showing para-aortic nodes raises the question of lymphoma or metastatic disease. [1]
The primary drainage sites
The registrar extends the examination to the primary site that drains to the enlarged node: [1]
- Skin of the head, neck, scalp and ears — for the cervical, occipital and pre-auricular nodes. The scalp must be examined through the hair, because the melanoma or the squamous cell carcinoma of the scalp is easily missed.
- The oral cavity and oropharynx — for the cervical nodes. Examine the tongue (including the base and the lateral borders), the floor of mouth, the buccal mucosa, the palate, the tonsils and the posterior pharyngeal wall. The oropharyngeal squamous cell carcinoma classically spreads to the upper deep cervical nodes.
- The breast — for the axillary nodes. Examine both breasts and both axillae.
- The thyroid — for the cervical and the supraclavicular nodes.
- The skin of the whole arm and hand — for the epitrochlear and axillary nodes.
- The external genitalia and the perineum — for the inguinal nodes.
- A digital rectal examination — when an anal or rectal primary is suspected (the anal squamous cell carcinoma classically spreads to the inguinal nodes). [1]
The systemic signs
The systemic signs refine the generalised differential: [1]
- Hepatosplenomegaly — with generalised lymphadenopathy, indicates a systemic process (EBV, CMV, lymphoma, leukaemia, sarcoid, viscer-otropic infection).
- The jaundice — of haemolysis (EBV), of hepatic infiltration (lymphoma, metastatic), or of biliary obstruction (the pancreatic head mass with the left supraclavicular node).
- The skin lesions — of sarcoid (erythema nodosum, lupus pernio), of lymphoma (cutaneous T-cell lymphoma, the mycosis fungoides and Sezary syndrome), of secondary syphilis (the maculopapular rash involving the palms and soles), of infectious mononucleosis (the amoxicillin-induced rash).
- The testicular mass — the testicular primary draining to the para-aortic nodes (and classically to the left supraclavicular node via the thoracic duct).
- The pallor, the bruising and the petechiae — of the marrow failure of leukaemia or advanced lymphoma. [1]
DCE short-case high-yield: "Examine this patient's lymph nodes." The registrar who examines only the neck has failed the question. The correct routine is the neck (occipital, pre- and post-auricular, submental and submandibular, anterior and posterior triangles, supraclavicular from behind with the head flexed), then the axillae (arm supported, against the chest wall, all five groups), then the epitrochlear nodes, then the inguinal nodes, then the popliteal fossae. The integrated examination that extends to the primary drainage sites (the skin, the oral cavity, the breast, the thyroid) and the systemic signs (the abdomen for hepatosplenomegaly, the skin for rashes) is the senior approach the examiner is looking for. [1]
The red-flag screen — the features that mandate biopsy
The red-flag screen is the single most important clinical step in lymphadenopathy, because it separates the node that is biopsied from the node that is observed. The red flags, drawn from the Gaddey and Riegel framework and the NICE NG12 suspected-cancer pathway, are [1]:
- A supraclavicular node of any size. Any supraclavicular node in an adult is abnormal and warrants biopsy. The malignancy probability is high (30 to 90 per cent across series), and observation is not appropriate.
- A hard or fixed node. Hard is metastatic carcinoma; fixed is advanced malignancy or invasive infection. Both mandate biopsy.
- A node above 2 cm without an obvious infective cause. The larger the node, the higher the probability of malignancy. Nodes above 3 cm in the cervical chain are highly concerning.
- A node persisting beyond 4 to 6 weeks. Reactive nodes from a viral illness resolve within 2 to 4 weeks. A node that does not regress, or that grows, is biopsied.
- The B symptoms — drenching night sweats, unintentional weight loss, unexplained fever. Any lymphadenopathy with B symptoms is investigated for lymphoma.
- Hepatosplenomegaly. Lymphadenopathy with hepatosplenomegaly indicates a systemic process and mandates investigation.
- Age above 40 years. The risk of malignancy in a lymph node rises sharply after age 40. The older the patient, the lower the threshold for biopsy [2].
The prevalence of malignancy in primary care lymphadenopathy is low overall — Bazemore and Smucker estimated it at approximately 1.1 per cent in the primary care setting [2] — but it rises steeply with each red-flag feature. The registrar's job is to identify the small minority with malignancy without over-investigating the large majority with reactive nodes, and the red-flag screen is the discriminator that achieves both.
Exam trap — the observation window: The "observe for 4 to 6 weeks" rule applies only to the low-risk node without red flags. A supraclavicular node, a hard fixed node, a node with B symptoms, or a node in the older patient is biopsied immediately — the observation window is not appropriate. The registrar who observes a supraclavicular node for a month has lost time that the underlying malignancy will use. [1]
First-tier investigations — the tests that frame the work-up

The first-tier investigations are the blood and imaging tests that frame the biopsy decision and the directed work-up. They are not a substitute for the biopsy in the patient with red-flag features. [1]
Full blood count, film, ESR and CRP
The full blood count with differential and a blood film is the first test. It identifies the leukaemic picture (the lymphocytosis of CLL, the blasts of ALL or AML), the atypical lymphocytes of EBV infectious mononucleosis, the eosinophilia of lymphoma or parasitic infection, and the pancytopenia of marrow infiltration. The ESR and CRP are non-specific markers of inflammation that are elevated in infection, malignancy and autoimmune disease; a markedly elevated ESR with lymphadenopathy raises the probability of a systemic process. [1]
Lactate dehydrogenase (LDH)
LDH is the non-specific tumour marker of lymphoma. It is a marker of high cell turnover, it is elevated in aggressive non-Hodgkin lymphoma (especially the Burkitt and the diffuse large B-cell lymphoma), and it is a component of the International Prognostic Index (IPI) and the revised International Prognostic Index (R-IPI) in diffuse large B-cell lymphoma [4]. An elevated LDH in the undiagnosed lymphadenopathy raises the probability of lymphoma, though it is not diagnostic. The registrar who sends an LDH in undifferentiated lymphadenopathy is using it as a red-flag adjunct, not as a diagnostic test.
Urea, electrolytes, liver function tests
The U&E and LFTs identify the renal and hepatic involvement of systemic disease, and they frame the safety of the imaging (the contrast CT) and the biopsy. An elevated alkaline phosphatase with lymphadenopathy raises the question of hepatic or bone infiltration. [1]
Directed microbiology and serology
The directed microbiological and serological tests are chosen by the clinical picture: [1]
- EBV — the monospot (heterophile antibody) test is the first-line screen for infectious mononucleosis; the EBV serology (VCA IgM, VCA IgG, EBNA IgG) is the definitive test when the monospot is negative but the clinical suspicion is high. The monospot is sensitive in the second week but may be negative in the first week and in young children.
- CMV — serology (IgM and IgG) for the CMV mononucleosis that mimics EBV.
- HIV — the fourth-generation antigen-antibody combination test is the preferred test because it shortens the window period to 2 to 4 weeks (the third-generation antibody test has a window period of 4 to 6 weeks, and the rapid test may have a longer window). The registrar who orders an HIV test only when the patient is "at risk" by an imperfect sexual history has missed the primary HIV infection that presents as a mononucleosis-like illness — the HIV test is part of the generalised lymphadenopathy work-up.
- Toxoplasma — serology (IgM and IgG) for the toxoplasmosis that presents with cervical lymphadenopathy.
- Syphilis — the treponemal test (TPPA or EIA) and the non-treponemal test (RPR or VDRL) for secondary syphilis, which presents with generalised lymphadenopathy, a maculopapular rash involving the palms and soles, and condylomata lata.
- Bartonella — serology for cat-scratch disease.
- Tuberculosis — the interferon-gamma release assay (IGRA, the QuantiFERON-TB Gold) or the tuberculin skin test (the Mantoux), with sputum for acid-fast bacilli if there is a productive cough or a chest X-ray abnormality. [1]
The chest X-ray
The chest X-ray identifies the mediastinal or hilar lymphadenopathy (lymphoma, tuberculosis, sarcoid), the lung lesion (the primary lung cancer that drains to the right supraclavicular node), the pleural effusion, and the pulmonary metastases. A normal chest X-ray does not exclude mediastinal lymphadenopathy, and a contrast CT of the chest is the more sensitive test when the chest X-ray is normal but the suspicion of mediastinal disease is high. [1]
Ultrasound of the node
The ultrasound assesses the node morphology — the size, the shape (a rounded node with a loss of the normal oval shape is concerning), the cortical thickness, the preservation or loss of the fatty hilum (the loss of the hilum and the eccentric cortical thickening are concerning for malignancy), the matting, and the vascularity on Doppler (a hilar pattern is benign; a peripheral or mixed pattern is concerning). The ultrasound can guide the FNA or the core biopsy, and it helps select the most abnormal node for the biopsy. However, ultrasound cannot replace histology in the patient with red-flag features — the decision to biopsy is made on the clinical red flags, not on the ultrasound appearance. [1]
The biopsy decision — the critical step
The biopsy is the definitive investigation in lymphadenopathy of unknown cause, and the choice of biopsy technique is the single most important decision the registrar makes after deciding to biopsy. The three techniques — FNA, core biopsy, excisional biopsy — are not interchangeable, and the wrong choice compromises the diagnosis. [1]
Fine-needle aspiration (FNA)
FNA is rapid, minimally invasive and can be performed at the bedside or under ultrasound guidance. It samples cells, not architecture, and it is the appropriate first test for: [1]
- The suspected metastatic carcinoma — a supraclavicular node in a patient with a known or suspected lung, gastric or breast primary. The FNA identifies the malignant cells and may permit immunohistochemistry (the thyroid markers, the prostate marker, the oestrogen and progesterone receptors) that identify the primary.
- The suspected infective node — tuberculosis (the acid-fast bacilli on the Ziehl-Neelsen stain, the mycobacterial culture, the PCR for M. tuberculosis complex), the bacterial lymphadenitis (the Gram stain and culture).
- The suspected reactive node with a need for a rapid screen (though the excisional biopsy remains the gold standard if lymphoma is suspected). [1]
FNA is inadequate for the primary diagnosis of lymphoma. It samples cells not architecture, and it cannot provide the nodal architecture (the follicular versus diffuse pattern), the full immunophenotyping or the molecular studies (the clonality, the translocations) that sub-classify lymphoma and direct therapy. The registrar who accepts an FNA report of "atypical lymphoid cells" on a node that is in fact lymphoma has compromised the diagnostic work-up and will need to repeat the biopsy as an excisional biopsy. [1]
Core needle biopsy
The core biopsy (usually ultrasound-guided, 14- to 18-gauge) provides a core of tissue that includes some architecture, and it is a reasonable second-line when an excisional biopsy is not feasible (the deep node, the patient who is not fit for a general anaesthetic). It provides tissue for immunohistochemistry and for some molecular studies, but it is inferior to the excisional biopsy for the sub-classification of lymphoma, and a definitive diagnosis is not always achievable. The core biopsy is an acceptable option when the excisional biopsy is not technically possible, but it is not the gold standard. [1]
Excisional biopsy — the gold standard for lymphoma
The excisional biopsy is the gold standard for the diagnosis of lymphoma. It removes the entire node, it preserves the architecture (the follicular versus diffuse pattern, the growth pattern, the capsule), it provides ample tissue for the immunohistochemistry (the B-cell and T-cell markers, the Hodgkin markers, the cell-cycle markers), the flow cytometry (the surface immunophenotyping), and the molecular studies (the clonality by PCR, the translocations by FISH) that sub-classify lymphoma and direct therapy [5].
The principles of the excisional biopsy: [1]
- Choose the most abnormal node — the largest, the hardest, or the most rapidly growing node. A small reactive node in the same patient may not give the diagnosis; the most abnormal node is most likely to.
- Avoid the inguinal node if possible — the inguinal nodes are often fibrotic and reactive from the recurrent minor skin trauma of the lower limb, and the histology may be non-specific. If a generalised lymphadenopathy is present, prefer a cervical or a supraclavicular node.
- Do not crush the node — the surgical technique must preserve the node intact; a crushed node compromises the architecture.
- Send the node fresh to the laboratory for the flow cytometry and the molecular studies, in addition to the formalin-fixed sample for the histology.
- Never give corticosteroids before the biopsy — corticosteroids induce apoptosis in the lymphoma cells and distort the nodal architecture, and a registrar who prescribes prednisone for a suspected reactive node that is in fact lymphoma has compromised the diagnostic tissue. If the patient is critically ill with a mediastinal mass and airway compromise, the steroids may be necessary — but only after a tissue diagnosis has been obtained (a rapid FNA or core biopsy), and with the explicit understanding that the definitive excisional biopsy will follow. [1]
DWE high-yield: The single most testable fact about the lymphoma biopsy is that FNA is not adequate for the primary diagnosis of lymphoma, and excisional biopsy is the gold standard. The registrar who accepts an FNA diagnosis, or who gives corticosteroids before the biopsy, has revealed a knowledge gap that the examiner will press on. The corollary is that the choice of node matters — the most abnormal node is biopsied, the inguinal node is avoided when alternatives are available, and the node is sent fresh for the flow cytometry. [1]
Staging and prognostication — the Lugano classification and the R-IPI
Once the histological diagnosis of lymphoma is made, the staging and the prognostication follow. The Lugano classification (Cheson and colleagues, 2014, endorsed by the international haematology and oncology societies including the Australasian Leukaemia and Lymphoma Group) is the modern standard for the initial evaluation, the staging and the response assessment of Hodgkin and non-Hodgkin lymphoma [5]. The key elements:
- PET-CT is the standard for staging and response assessment of the FDG-avid lymphomas (Hodgkin lymphoma, diffuse large B-cell lymphoma, follicular lymphoma, mantle cell lymphoma). For the non-avid lymphomas (the marginal zone, the small lymphocytic), the contrast CT remains the standard.
- The Ann Arbor staging (stage I — single node group or single extranodal site; stage II — two or more node groups on the same side of the diaphragm; stage III — node groups on both sides of the diaphragm; stage IV — disseminated extranodal involvement) remains the anatomical framework, with the addition of the E designation for the contiguous extranodal extension.
- The A/B symptom designation is now applied to Hodgkin lymphoma only, because the B symptoms lack prognostic value in most non-Hodgkin lymphomas [5].
- Routine bone marrow biopsy is no longer indicated for the staging of Hodgkin lymphoma or of most diffuse large B-cell lymphomas if the PET-CT is performed and shows no marrow involvement [5] — a major change from the earlier Ann Arbor framework, sparing the patient a painful and often non-contributory procedure.
- The Deauville 5-point scale is the standard for the PET-CT response assessment (1 — no uptake; 2 — uptake less than or equal to the mediastinum; 3 — uptake greater than the mediastinum but less than or equal to the liver; 4 — uptake moderately greater than the liver; 5 — uptake markedly greater than the liver or new lesions).
The revised International Prognostic Index (R-IPI) (Sehn and colleagues, 2007) stratifies the outcome of diffuse large B-cell lymphoma treated with R-CHOP into three risk groups, using the five IPI factors — age over 60, stage III or IV (Lugano), more than one extranodal site, performance status 2 to 4 (ECOG), and elevated LDH [4]. The R-IPI distributes the patients into:
- Very good (R-IPI 0) — 4-year progression-free survival 94 per cent, overall survival 94 per cent.
- Good (R-IPI 1 to 2) — 4-year PFS 80 per cent, OS 79 per cent.
- Poor (R-IPI 3 to 5) — 4-year PFS 53 per cent, OS 55 per cent. [1]
The R-IPI is the modern prognostic framework for the diffuse large B-cell lymphoma, and it frames the discussion of prognosis and the consideration of the high-risk subgroups for the clinical trials of intensified therapy. The registrar who stages and prognosticates a newly diagnosed lymphoma uses the Lugano classification and the R-IPI (or the subtype-specific index — the FLIPI for the follicular, the MIPI for the mantle cell), and carries the LDH and the performance status as the two most clinically accessible predictors of outcome. [1]
The specific syndromes — the high-yield exam patterns
Infectious mononucleosis (EBV)
Infectious mononucleosis is the classic generalised lymphadenopathy of the young patient. The triad of fever, tonsillar pharyngitis with an exudate, and generalised lymphadenopathy (especially the cervical nodes), with splenomegaly, the atypical lymphocytes on the blood film, and the positive heterophile antibody (monospot) test, is the clinical signature. The Hoagland sign — the bilateral palpebral (eyelid) oedema — is the classic but under-recognised early sign, first described by Hoagland in his 1952 paper [3]. The amoxicillin- or ampicillin-induced maculopapular rash occurs in over 90 per cent of patients with EBV given these antibiotics, and it is the classic exam discriminator — a tonsillitis with a widespread rash after amoxicillin is infectious mononucleosis until proven otherwise, and it is not a true penicillin allergy (the rash does not recur with penicillin in the absence of EBV). The spleen enlargement and the rare but catastrophic splenic rupture in the second to third week is the reason the patient is advised to avoid contact sport for 3 to 4 weeks.
Primary HIV infection (acute retroviral syndrome)
The primary HIV infection presents 2 to 4 weeks after the exposure as a mononucleosis-like illness — fever, generalised lymphadenopathy, mucocutaneous ulceration (the oral or genital ulcers), a maculopapular rash, and a meningitic or encephalitic picture. The antibody test may be negative in the window period, and the fourth-generation antigen-antibody test (which detects the p24 antigen) is the preferred test because it shortens the window period to 2 to 4 weeks. The viral load is high (often above 1 million copies per mL) in the acute phase, and the diagnosis is missed because the registrar does not think of HIV in the patient with "a viral illness." The registrar who orders the HIV test in any patient with a mononucleosis-like illness — especially with the mucocutaneous ulceration or the rash — has closed the diagnostic gap. The diagnosis of primary HIV is the opportunity to initiate antiretroviral therapy early and to counsel the patient on the high infectivity of the acute phase. [1]
Kikuchi-Fujimoto disease (histiocytic necrotising lymphadenitis)
The Kikuchi-Fujimoto disease is a self-limited, benign cause of painful cervical lymphadenopathy in the young woman (the female-to-male ratio is approximately 4 to 1, the median age around 25). The presentation — a painful cervical lymphadenopathy with fever and a self-limited course over weeks to months — mimics lymphoma clinically, and the diagnosis requires a biopsy (the histology shows the paracortical necrosis with the karyorrhectic debris and the crescentic histiocytes, without the neutrophils). The importance is that the disease is self-limiting and the steroids are not first-line; the registrar who makes the diagnosis avoids the unnecessary chemotherapy of a misdiagnosed lymphoma. The disease is associated with the systemic lupus erythematosus (the patient with Kikuchi should be screened for the evolving SLE), and it is commoner in the East Asian populations. [1]
Cat-scratch disease (Bartonella henselae)
The cat-scratch disease presents as a regional lymphadenitis — usually cervical or axillary — developing 1 to 3 weeks after a cat scratch (especially a kitten), with a papule or a pustule at the inoculation site. The course is self-limited over weeks to months, and the management is symptomatic. The risk of dissemination is higher in the immunocompromised host, where the Bartonella may cause the bacillary angiomatosis and the peliosis hepatis. The diagnosis is serological (the Bartonella henselae IgG), and the node is biopsied when the diagnosis is unclear or when the lymphoma is in the differential. [1]
Lymphogranuloma venereum (Chlamydia trachomatis L1 to L3)
The lymphogranuloma venereum presents with a painless genital ulcer, followed in 1 to 3 weeks by the tender inguinal and femoral lymphadenopathy that classically forms the groove sign — the depression between the enlarged inguinal nodes (above the inguinal ligament) and the enlarged femoral nodes (below the ligament), produced by the ligament itself. The nodes may progress to buboes (the fluctuant, suppurating masses), and the late complication is the genitoanorectal syndrome (the proctocolitis, the fistulae, the strictures). The diagnosis is by the NAAT for the C. trachomatis L serovars on the ulcer swab or the lymph node aspirate, and the treatment is doxycycline. [1]
Lymphadenopathy in the immunocompromised host
The differential in the immunocompromised host — the patient with HIV, the solid-organ or stem-cell transplant, the chemotherapy, or the immunosuppressive therapy — is broader and the threshold to biopsy is lower. [1]
The immunocompromised host is at risk for: [1]
- The same reactive and malignant causes as the immunocompetent host.
- The opportunistic infections — the mycobacteria (M. tuberculosis and the non-tuberculous mycobacteria, especially the Mycobacterium avium complex in advanced HIV), CMV, EBV, the cryptococcus (the cryptococcal lymphadenitis), toxoplasma, the endemic mycoses (histoplasma, coccidioides, talaromyces in the relevant geography).
- The AIDS-defining malignancies — the diffuse large B-cell lymphoma, the Burkitt lymphoma, the primary CNS lymphoma, the Kaposi sarcoma (from the human herpesvirus 8), the cervical cancer.
- The post-transplant lymphoproliferative disorder (PTLD) — the lymphadenopathy or the extranodal mass in the solid-organ or stem-cell transplant recipient, driven by the EBV in most cases, with a spectrum from the polymorphic hyperplasia to the monomorphic lymphoma. The first management step is the reduction of the immunosuppression, and the biopsy with the EBV testing (the EBER in-situ hybridisation) is the diagnostic step. [1]
The principle in the immunocompromised host is that the threshold to biopsy is lower. An enlarging node in a patient with a CD4 count below 200, or on a calcineurin inhibitor, or on the anti-TNF therapy, is biopsied early, with the stains and the cultures for the mycobacteria and the fungi, and the EBV testing. The observation period that is reasonable in the immunocompetent patient does not apply. [1]
Regional guideline anchoring
The guidelines that frame the work-up of lymphadenopathy converge across regions, with local deltas the registrar must carry: [1]
- The NICE NG12 suspected cancer guideline (2015, updated) embeds the urgent suspected-cancer referral for the patient with unexplained lymphadenopathy or splenomegaly, the persistent unexplained lymphadenopathy, or the associated systemic symptoms; the supraclavicular node carries the highest priority for the urgent referral. The 2-week-wait suspected-cancer pathway is the UK route to the biopsy.
- The American Family Physician framework (Gaddey and Riegel, 2016) provides the systematic classification (localised versus generalised), the regional differential, the red-flag screen, and the biopsy decision, and it emphasises the harm of corticosteroids before biopsy [1].
- The British Society for Haematology (BSH) guidelines frame the lymphoma diagnosis (the excisional biopsy as the gold standard, the SIHMDS — the Specialist Integrated Haematological Malignancy Diagnostic Service — for the expert review of the node).
- The Haematology Society of Australia and New Zealand (HSANZ) and the Cancer Council Australia frame the ANZ practice, with the local pathways to the haematology and the head-and-neck multidisciplinary teams.
The regional delta the registrar must carry: the principles converge (the supraclavicular node is biopsied, the B symptoms are a red flag, the excisional biopsy is the gold standard for lymphoma), but the specific referral pathways differ — the registrar confirms the local urgent-cancer pathway on arrival at a new hospital, and uses it for the patient with the red-flag node. [1]
DCE long-case approach
Patient scenario
Mr David Okafor, 58, a Nigerian-born taxi driver who migrated to Australia 10 years ago, presents to the outpatient clinic with a six-week history of a painless lump in the left supraclavicular fossa. He reports three months of intermittent night sweats that soak the sheets, a 6 kg unintentional weight loss (from 82 to 76 kg), and early satiety. He has a past history of hypertension (on amlodipine) and gastro-oesophageal reflux (on pantoprazole). He has never smoked. He drinks 4 standard drinks a week. He works long hours and has not seen a doctor in three years. [1]
On examination: he is thin but comfortable. There is a 2 cm rubbery, mobile, non-tender node in the left supraclavicular fossa, with a separate 1.5 cm rubbery node in the right supraclavicular fossa and shotty nodes in both axillae. The abdomen reveals a liver edge palpable 3 cm below the costal margin and a spleen palpable 2 cm. There is no pallor, no jaundice, no bruising. The chest is clear. Observations: temperature 37.6, heart rate 88, blood pressure 138/86, respiratory rate 16, SpO2 98 per cent on room air. [1]
Investigations: haemoglobin 118, white cell count 9.2, platelets 210, ESR 68, CRP 42, LDH 520 (upper limit of normal 250). U&E and LFTs normal apart from an albumin of 32. EBV serology consistent with remote infection (VCA IgG positive, IgM negative). HIV fourth-generation test negative. IGRA positive. Chest X-ray shows a widened mediastinum. CT of the neck, chest, abdomen and pelvis shows enlarged supraclavicular, mediastinal, para-aortic and iliac nodes, with the largest node measuring 3.5 cm in the mediastinum. [1]
Candidate's opening statement (SASPOP)
"Mr Okafor is a 58-year-old Nigerian-born man presenting with a six-week history of a painless left supraclavicular node, three months of drenching night sweats, a 6 kg weight loss and early satiety. His main problems are: first, a generalised lymphadenopathy with supraclavicular, mediastinal, para-aortic and iliac nodes on the CT, with B symptoms and a raised LDH, in a man of his age — the leading diagnosis is lymphoma, with the differential of disseminated tuberculosis given the positive IGRA and his country of origin, and metastatic carcinoma from an intra-abdominal primary given the left supraclavicular node; second, the hepatosplenomegaly, which is consistent with a systemic haematological or infiltrative process; and third, the constitutional decline with the weight loss and the low albumin. My immediate priority is a tissue diagnosis — the next step is an excisional biopsy of the most accessible abnormal node, with the tissue sent fresh for the histology, the immunohistochemistry, the flow cytometry and the molecular studies, and I would not give corticosteroids at any point before the biopsy. I would investigate for tuberculosis in parallel — the positive IGRA and his background raise the possibility, and the node will be sent for the acid-fast bacilli stain, the culture and the PCR. I would stage the disease with a PET-CT after the histology, per the Lugano classification." [1]
Problem list
- Generalised lymphadenopathy with B symptoms and a raised LDH — leading diagnosis lymphoma; differential disseminated tuberculosis, metastatic carcinoma.
- Hepatosplenomegaly — consistent with a systemic process.
- Positive IGRA — latent or active tuberculosis to be excluded before the immunosuppressive therapy that may follow a lymphoma diagnosis.
- Constitutional decline — weight loss, low albumin, early satiety.
- Hypertension — a background comorbidity. [1]
Integrated management plan
The management is diagnosis-led and integrated: [1]
- Excisional biopsy of the most accessible abnormal node — the supraclavicular node is the most accessible; the tissue is sent fresh to the laboratory for the histology, the immunohistochemistry (the B-cell and T-cell markers, the Hodgkin markers, the cell-cycle markers), the flow cytometry, and the molecular studies (the clonality by PCR, the translocations by FISH). The biopsy is the priority, and it is performed within days, not weeks.
- Tuberculosis work-up in parallel — three sputum samples for the acid-fast bacilli stain, the mycobacterial culture and the PCR (the nucleic acid amplification test for the M. tuberculosis complex); the node is sent for the same stains and cultures. The latent TB treatment (the rifampicin for 4 months or the isoniazid for 6 to 9 months, per the local guideline) is considered after the active TB is excluded, and before any immunosuppressive or cytotoxic therapy.
- No corticosteroids before the biopsy — the steroids may compromise the histology of lymphoma and the granulomatous architecture of tuberculosis.
- PET-CT for staging after the histology, per the Lugano classification [5]. The bone marrow biopsy is not routine if the PET-CT shows no marrow involvement and the diagnosis is Hodgkin lymphoma or diffuse large B-cell lymphoma.
- Multidisciplinary review — the haematology and the infectious diseases teams are involved from the biopsy stage, given the diagnostic uncertainty (lymphoma versus TB) and the management implications.
- Supportive care — the nutrition, the analgesia, the psychological support, and the communication of a possible cancer diagnosis with the patient and the family.
Examiner probing questions and model answers
Q1: "Why an excisional biopsy rather than a fine-needle aspiration?" [1]
"The FNA samples cells, not architecture, and it is inadequate for the primary diagnosis of lymphoma. The excisional biopsy preserves the nodal architecture — the follicular versus diffuse pattern, the growth pattern, the capsule — and it provides ample tissue for the immunohistochemistry, the flow cytometry and the molecular studies that sub-classify the lymphoma and direct therapy [5]. An FNA might identify 'atypical lymphoid cells,' but it cannot distinguish the Hodgkin from the non-Hodgkin lymphoma, it cannot distinguish the diffuse large B-cell from the follicular, and it cannot provide the cell-of-origin or the translocation status that the modern therapy requires. The principle is that the choice of biopsy technique is as important as the decision to biopsy — FNA is acceptable for the suspected metastatic carcinoma or the infective node, but the excisional biopsy is the gold standard for the suspected lymphoma, and Mr Okafor's leading diagnosis is lymphoma."
Q2: "He has a positive IGRA. How does that change your management?" [1]
"The positive IGRA indicates a latent tuberculosis infection, which is common in a man born in a high-prevalence country. It raises two issues. First, I must exclude active tuberculosis before I consider any immunosuppressive or cytotoxic therapy — the lymphoma, if confirmed, will be treated with immunochemotherapy that would reactivate a latent TB, and the TB itself is in the differential of the lymphadenopathy (the granulomatous lymphadenitis of TB mimics lymphoma clinically). I send three sputum samples for the acid-fast bacilli and the PCR, and the node is sent for the AFB stain, the culture and the PCR. Second, I will treat the latent TB (the rifampicin for 4 months or the isoniazid for 6 to 9 months per the local guideline) after the active TB is excluded, and before or during the lymphoma therapy, in consultation with the infectious diseases team. The teaching point is that the latent TB is not the explanation for the B symptoms or the LDH — the night sweats, the weight loss and the LDH are more consistent with the lymphoma — but it is a comorbidity that must be managed alongside the lymphoma to prevent the reactivation." [1]
Q3: "How would you stage him once the histology is back?" [1]
"I would stage with a PET-CT, per the Lugano classification [5]. The PET-CT is the standard for the staging and the response assessment of the FDG-avid lymphomas — the Hodgkin lymphoma, the diffuse large B-cell lymphoma, the follicular and the mantle cell. The Ann Arbor staging (I to IV) provides the anatomical framework, and the PET-CT identifies the metabolically active disease. The routine bone marrow biopsy is no longer indicated if the PET-CT shows no marrow involvement and the diagnosis is Hodgkin lymphoma or diffuse large B-cell lymphoma — a change that spares the patient a painful and often non-contributory procedure. I would prognosticate with the revised International Prognostic Index if the diagnosis is diffuse large B-cell lymphoma — the R-IPI uses the age over 60, the stage III or IV, the more than one extranodal site, the performance status 2 to 4, and the elevated LDH, and it stratifies the outcome into the very good, the good and the poor risk groups [4]. Mr Okafor's LDH is elevated (520), his stage is likely IV by the CT (the para-aortic and the iliac nodes are below the diaphragm), and his performance status would need to be assessed — he is likely in the good or the poor R-IPI group, and this frames the discussion of the prognosis and the consideration of the clinical trials."
Q4: "Could this be metastatic gastric cancer? He has a left supraclavicular node." [1]
"Yes, it is in the differential. The left supraclavicular node — the Virchow node — drains the abdominal cavity via the thoracic duct, and it classically signals a gastric, pancreatic, hepatic, renal or testicular primary. The early satiety and the weight loss raise the gastric cancer possibility. However, the picture overall is more consistent with a lymphoma than a gastric cancer: the generalised lymphadenopathy (the supraclavicular, the mediastinal, the para-aortic, the iliac nodes are all involved), the hepatosplenomegaly, and the raised LDH. A gastric cancer would more typically give a single dominant left supraclavicular node with the intra-abdominal primary, not the generalised nodal pattern. I would request an upper endoscopy as part of the work-up if the histology of the node is metastatic adenocarcinoma — but I expect the histology to show lymphoma, and the endoscopy is not the first step. The teaching point is that the Virchow node is a red flag that mandates the biopsy, and the histology directs the search for the primary — I do not speculate on the primary before the biopsy, because the biopsy answers the question." [1]
Q5: "What is your plan for his long-term management after the diagnosis?" [1]
"The plan is integrated and stage-dependent. If the diagnosis is a diffuse large B-cell lymphoma, the standard therapy is the R-CHOP (the rituximab, the cyclophosphamide, the doxorubicin, the vincristine, the prednisone) for six cycles, with the intrathecal prophylaxis if there is a high-risk subtype (the testicular, the paranasal sinus involvement). The PET-CT response assessment after 2 to 4 cycles and at the end of therapy uses the Deauville scale. If the diagnosis is a Hodgkin lymphoma, the therapy is the ABVD (the doxorubicin, the bleomycin, the vinblastine, the dacarbazine) or the escalated BEACOPP for the high-risk, with the PET-CT response-adapted therapy. If the diagnosis is an indolent lymphoma (the follicular), the therapy may be deferred (the watch-and-wait) if the disease is asymptomatic, or the rituximab with or without the chemotherapy if it is symptomatic. The latent TB is treated alongside. The supportive care — the nutrition, the psychosocial support, the fertility preservation (the sperm banking before the chemotherapy) — is integrated from the start. And the communication — the honest discussion of the diagnosis, the prognosis and the treatment plan, with the patient and the family, in the language he understands, with the interpreter if needed — is the foundation of the long-term management." [1]
Q6: "What is the single most important lesson from this case for a registrar managing undifferentiated lymphadenopathy?" [1]
"The single most important lesson is that the biopsy is the priority, and the choice of biopsy matters. Mr Okafor has a supraclavicular node with B symptoms and a raised LDH — the leading diagnosis is lymphoma, and the next step is an excisional biopsy, not an observation period and not an FNA. The registrar who observes a supraclavicular node, or who accepts an FNA diagnosis, has lost time and compromised the diagnostic tissue. The corollary is the parallel work-up — the tuberculosis is in the differential, and the latent TB is a comorbidity that must be managed before the immunosuppressive therapy. The integrated approach — the red-flag screen, the correct biopsy, the parallel work-up of the differential, the staging per the Lugano classification, and the prognostication per the R-IPI — is what keeps the complex lymphadenopathy patient safe and gets the diagnosis right the first time." [1]
DCE short-case discussion: the lymph node examination
Instruction: "Examine this patient's lymph nodes. Present your findings and offer a differential diagnosis." [1]
Systematic examination routine
- End of the bed — the look test. Is the patient cachectic (weight loss), pale (anaemia), icteric (haemolysis or infiltration)? Are there skin lesions (the rash of secondary syphilis, the erythema nodosum of sarcoid)? Is there a surgical scar (a previous biopsy, a previous thyroid or breast surgery)?
- Hands and arms — for the peripheral stigmata (the pallor, the bruising of marrow failure) and the epitrochlear node.
- The neck — inspect for asymmetry and scars, then palpate in sequence: occipital, pre-auricular, post-auricular, submental, submandibular, the upper-middle-lower deep cervical (anterior triangle, along the anterior border of the sternocleidomastoid), the posterior triangle (along the posterior border of the sternocleidomastoid), and the supraclavicular fossae. The supraclavicular fossa is palpated from behind the patient, with the patient's head slightly flexed forward to relax the sternocleidomastoid, and the examiner's fingers placed deep to the clavicle. The registrar who palpates from the front with the head extended misses the node.
- The axillae — with the patient's arm supported by the examiner's hand, palpate against the chest wall in all five axillary positions: the apical (high in the axilla, against the clavicle), the central (the bulk of the axilla), the pectoral (anterior, against the pectoralis major), the lateral (against the humerus), and the subscapular (posterior, against the latissimus dorsi and the teres major).
- The epitrochlear nodes — with the patient's elbow flexed to 90 degrees, palpate 2 to 3 cm above the medial epicondyle, in the groove between the biceps and the triceps.
- The intraclavicular nodes — just below the clavicle, in the deltopectoral groove.
- The inguinal nodes — the horizontal group along the inguinal ligament, and the vertical group along the saphenous vein.
- The popliteal fossae.
- The primary drainage sites and the systemic signs — the skin of the head, neck and scalp; the oral cavity and the oropharynx; the breast; the thyroid; the abdomen for hepatosplenomegaly; the testes; the skin of the limbs. [1]
Presentation template
"I have examined all the peripheral lymph node groups. The significant findings are a 2 cm rubbery, mobile, non-tender node in the left supraclavicular fossa, with a separate 1.5 cm rubbery node in the right supraclavicular fossa and shotty nodes in both axillae. The epitrochlear, the intraclavicular and the inguinal nodes are not enlarged. The abdomen reveals a liver edge palpable 3 cm and a spleen palpable 2 cm. My findings are consistent with a generalised lymphadenopathy with hepatosplenomegaly, and my leading differential is lymphoma, with the differential of disseminated tuberculosis and a systemic infection such as EBV or CMV. The supraclavicular node is a red flag, and I would arrange an excisional biopsy of the most accessible abnormal node, with the tissue sent fresh for the histology, the immunohistochemistry, the flow cytometry and the molecular studies, and I would investigate for tuberculosis and the systemic infections in parallel." [1]
Discussion questions
Examiner: "Why do you examine the supraclavicular fossa from behind the patient?" [1]
"Because the supraclavicular nodes lie deep to the clavicle and the sternocleidomastoid, and they are best palpated from behind with the patient's head flexed forward to relax the sternocleidomastoid. The examiner's fingers are placed in the supraclavicular fossa, deep to the clavicle, and the patient is asked to cough or to perform a Valsalva manoeuvre, which may push a deep node up against the examining fingers. The registrar who palpates the supraclavicular fossa from the front with the head extended is palpating the overlying sternocleidomastoid, not the node, and will miss it. The supraclavicular node is the single highest-risk location, and the technique of the examination is the difference between finding it and missing it." [1]
Examiner: "What is the significance of an epitrochlear node?" [1]
"Any palpable epitrochlear node above 5 mm is abnormal [1]. The epitrochlear node drains the medial forearm and the ulnar aspect of the hand. The differential includes secondary syphilis (the classic association), lymphoma (especially the non-Hodgkin lymphoma), infectious mononucleosis, and the skin infection of the hand or forearm. An epitrochlear node is a red flag in the same way that a supraclavicular node is — it is never a normal reactive node — and the registrar who dismisses one as reactive has missed a significant finding. The active search for the secondary syphilis (the rash involving the palms and soles, the condylomata lata, the treponemal serology) and the lymphoma (the blood film, the LDH, the biopsy) follows the finding."
Examiner: "What is the single most important lesson from this examination for a registrar managing lymphadenopathy?" [1]
"The single most important lesson is that the examination is not complete until all node groups have been examined, and the examination extends to the primary drainage sites and the systemic signs. The registrar who examines only the node the patient noticed has examined only a fraction of the patient. The supraclavicular node, the epitrochlear node and the systemic hepatosplenomegaly are the findings that change the differential and the urgency, and they are found only by the systematic examination. The corollary is the characterisation of the node — the size with a ruler, the consistency (soft, rubbery, hard), the mobility, the tenderness, the matting — because these features, with the location and the B symptoms, drive the decision to biopsy." [1]
Key DWE MCQ patterns
- Discriminate the cause by the location. A left supraclavicular node in an adult is metastatic gastric cancer or lymphoma until proven otherwise; an anterior cervical node in a young patient with a sore throat is infectious mononucleosis; an inguinal node with a painless genital ulcer is lymphogranuloma venereum.
- Choose the biopsy technique. A suspected lymphoma is biopsied by the excisional biopsy, not the FNA; the FNA is acceptable for the suspected metastatic carcinoma or the infective node. The corticosteroids are never given before the biopsy.
- Recognise the B symptoms. Drenching night sweats, unintentional weight loss and unexplained fever with lymphadenopathy mandate investigation for lymphoma.
- Recognise the amoxicillin rash. A tonsillitis with a widespread maculopapular rash after amoxicillin is infectious mononucleosis until proven otherwise, not a penicillin allergy.
- Recognise the primary HIV infection. A mononucleosis-like illness with mucocutaneous ulceration and a rash, 2 to 4 weeks after an exposure, is the acute retroviral syndrome, and the fourth-generation antigen-antibody test is the diagnostic test.
- Recognise the groove sign. The depression between the enlarged inguinal and femoral nodes is the groove sign of lymphogranuloma venereum.
- Recognise the Hoagland sign. The bilateral palpebral oedema of infectious mononucleosis.
- Choose the staging test. The PET-CT is the standard for the staging and the response assessment of the FDG-avid lymphomas per the Lugano classification; the routine bone marrow biopsy is not required if the PET-CT shows no marrow involvement.
- Prognosticate with the R-IPI. The age over 60, the stage III or IV, the more than one extranodal site, the performance status 2 to 4, and the elevated LDH stratify the diffuse large B-cell lymphoma into the very good, the good and the poor risk.
- Lower the threshold to biopsy in the immunocompromised host. The differential is broader (the mycobacteria, the fungi, the EBV-driven lymphoproliferative disorder) and the observation period that is reasonable in the immunocompetent patient does not apply. [1]
References
[1] Gaddey HL, Riegel AM. Unexplained Lymphadenopathy: Evaluation and Differential Diagnosis. Am Fam Physician 2016;94(11):896–903. The systematic clinical framework for the evaluation of unexplained lymphadenopathy — the localised-versus-generalised classification, the regional differential, the red-flag screen, the 3- to 4-week observation in the low-risk patient, the biopsy decision (FNA, core, excisional), and the explicit warning against the corticosteroids before a tissue diagnosis.
[2] Bazemore AW, Smucker DR. Lymphadenopathy and malignancy. Am Fam Physician 2002;66(11):2103–10. The primary-care estimate that the prevalence of malignancy in unexplained lymphadenopathy is as low as 1.1 per cent, and the framework for the clinical identification of the minority with malignancy (the older age, the fixed or firm nodal character, the long duration, the supraclavicular location, the systemic symptoms).
[3] Hoagland RJ. Infectious mononucleosis. Am J Med 1952;13(2):158–71. The classic description of infectious mononucleosis, including the Hoagland sign (the bilateral palpebral oedema) that bears the author's name.
[4] Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood 2007;109(5):1857–61. The retrospective analysis of 365 patients treated at the British Columbia Cancer Agency, redistributing the five IPI factors (age over 60, stage III or IV, more than one extranodal site, performance status 2 to 4, elevated LDH) into the R-IPI risk groups (very good, good, poor) with the 4-year overall survival of 94, 79 and 55 per cent.
[5] Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 2014;32(27):3059–68. The international consensus on the modern staging and the response assessment of lymphoma — the PET-CT as the standard for the FDG-avid lymphomas, the restriction of the A/B symptom designation to Hodgkin lymphoma, the redundancy of the routine bone marrow biopsy for Hodgkin and most diffuse large B-cell lymphomas if the PET-CT is performed, and the Deauville 5-point scale for the PET-CT response assessment.
Gaddey and Riegel (AFP 2016); Bazemore and Smucker (AFP 2002); Hoagland (Am J Med 1952); Sehn et al. (Blood 2007); Cheson et al. Lugano classification (JCO 2014); NICE NG12 suspected cancer; British Society for Haematology guidelines; Haematology Society of Australia and New Zealand (HSANZ); Cancer Council Australia. [1]
References
- [1]Gaddey HL, Riegel AM Unexplained Lymphadenopathy: Evaluation and Differential Diagnosis Am Fam Physician, 2016.PMID 27929264
- [2]Bazemore AW, Smucker DR Lymphadenopathy and malignancy Am Fam Physician, 2002.PMID 12484692
- [3]Hoagland RJ Infectious mononucleosis Am J Med, 1952.PMID 12976417
- [4]Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP Blood, 2007.PMID 17105812
- [5]Cheson BD, Fisher RI, Barrington SF, et al.; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium; Italian Lymphoma Foundation; European Organisation for Research and Treatment of Cancer/Dutch Hemato-Oncology Group; Grupo Espanol de Medula Osea; German High-Grade Lymphoma Study Group; German Hodgkin's Study Group; Japanese Lymphorra Study Group; Lymphoma Study Association; NCIC Clinical Trials Group; Nordic Lymphoma Study Group; Southwest Oncology Group; United Kingdom National Cancer Research Institute Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification J Clin Oncol, 2014.PMID 25113753