Phys · general-medicine
Undifferentiated Oedema — A Systematic Diagnostic Approach
Also known as oedema · edema · swelling · peripheral oedema · dependent oedema · generalised oedema · anasarca · undifferentiated swelling · leg swelling · bilateral leg oedema · unilateral leg swelling · diagnostic approach to oedema · Starling forces · serum-ascites albumin gradient · SAAG · Stemmer sign · cyclical oedema · myxoedema · pretibial myxoedema · lymphoedema · CEAP classification · venous insufficiency · amlodipine oedema · drug-induced oedema
Consultant-physician-depth guide to the diagnostic approach to the patient with oedema of unknown cause. Covers the Starling forces framework (capillary hydrostatic pressure, plasma oncotic pressure, capillary permeability, lymphatic drainage) and its revised glycocalyx model, the localised-versus-generalised classification (unilateral leg — DVT, cellulitis, chronic venous insufficiency, compartment syndrome, lymphoedema; bilateral legs — systemic causes), the systemic causes (cardiac — heart failure, cor pulmonale, constrictive pericarditis; hepatic — cirrhosis, ascites, the serum-ascites albumin gradient; renal — nephrotic, nephritic, CKD, AKI; drugs — calcium channel blockers, NSAIDs, steroids, pioglitazone, minoxidil; endocrine — myxoedema, pretibial myxoedema; nutritional — protein malnutrition, refeeding; idiopathic — cyclical oedema), the focused history and examination discriminators (distribution, pitting, the JVP, the Stemmer sign, the skin), the first-tier investigations (urinalysis, FBC, U&E, LFTs, albumin, TFTs, NT-proBNP) and second-tier investigations (echocardiogram, 24-hour urine protein, renal biopsy, diagnostic ascitic tap with SAAG), and the cause-specific management. Structured for FRACP DWE and DCE, MRCP and ABIM.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Oedema — A Systematic Diagnostic Approach

The answer first
The patient who presents with oedema of unknown cause is one of the commonest and most cognitively demanding presentations in internal medicine. The swelling is a non-specific physical sign that may arise from a cardiac, hepatic, renal, endocrine, drug, nutritional or lymphatic cause — and the registrar's job is to use the distribution and the Starling mechanism as the organising framework, to take a focused history and examine for the discriminators, and to let the first-tier investigations (the urinalysis, the albumin, the NT-proBNP and the thyroid function tests) narrow the differential before committing to a working diagnosis. [1]
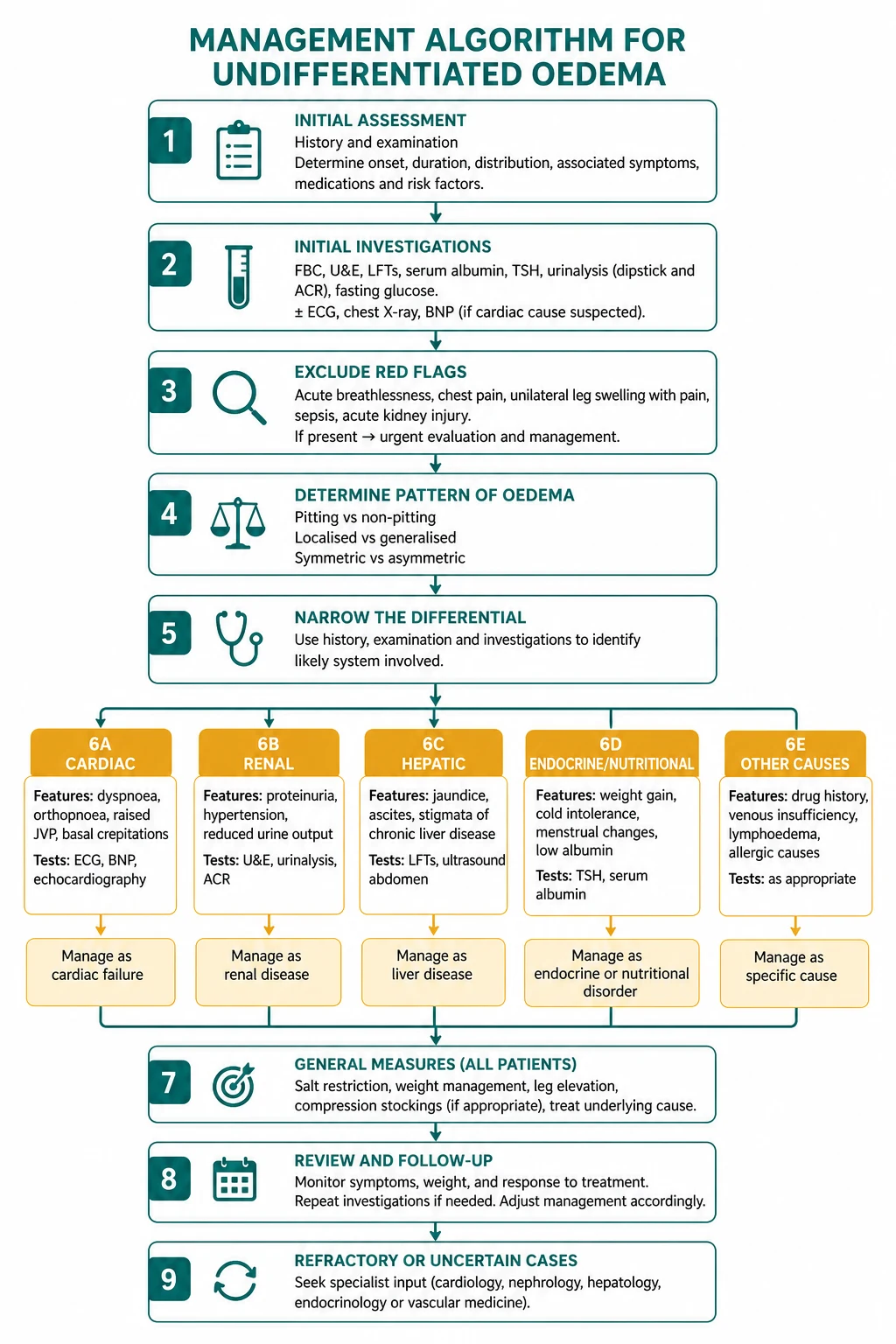
The reproducible sequence for any oedematous patient is: [1]
- Determine the distribution — localised (unilateral leg, single limb, facial, sacral) versus generalised (bilateral legs, face and legs, anasarca). This single axis generates a sharper differential than any other feature.
- Apply the Starling mechanism — which of the four forces (increased capillary hydrostatic pressure, reduced plasma oncotic pressure, increased capillary permeability, impaired lymphatic drainage) or the sodium-and-water retention of cirrhosis, heart failure and CKD is the cause?
- Take a focused history — onset, progression, positional behaviour (orthostatic worsening suggests venous or drug-induced; morning-worst suggests renal or hypothyroid), the associated symptoms (dyspnoea, frothy urine, jaundice, cold intolerance), and the drug history (amlodipine, NSAIDs, steroids, pioglitazone).
- Examine systematically — grade the pitting, assess the JVP, the cardiovascular and the abdominal examination, examine the skin for venous and lymphatic stigmata, and check the Stemmer sign.
- Order the first-tier investigations — urinalysis, full blood count, urea and electrolytes, liver function tests and albumin, thyroid function tests, NT-proBNP, 12-lead ECG, chest X-ray.
- Apply the discriminators — the urinalysis for the renal cause, the albumin and the SAAG for the hepatic cause, the NT-proBNP and the echocardiogram for the cardiac cause, the TSH for the thyroid cause, and the drug history for the pharmacological cause.
- Treat the underlying cause, not the symptom — the diuretic is a bridge to the definitive diagnosis, never a substitute for it. [1]
The single most dangerous error is reaching for a diuretic before the diagnosis. The oedema from amlodipine does not respond to furosemide (it worsens the intravascular depletion). The oedema from nephrotic syndrome requires intravenous albumin and the treatment of the glomerular disease. The oedema from lymphoedema requires complete decongestive therapy, not a loop diuretic. The registrar who treats the sign before the mechanism has confused a bridge with a destination. [1]
Viva trap: "What is the single most useful piece of information in the first minute with an oedematous patient?" The honest answer is the distribution. "Swollen one leg for two days" is a different patient from "swollen both legs and the face for three months," and the differential generated by that single phrase is sharper than any single investigation. The registrar who asks "which part of you is swollen, and when is it worst?" before reaching for the stethoscope has organised the entire encounter. [1]
Why the Starling forces are the organising framework

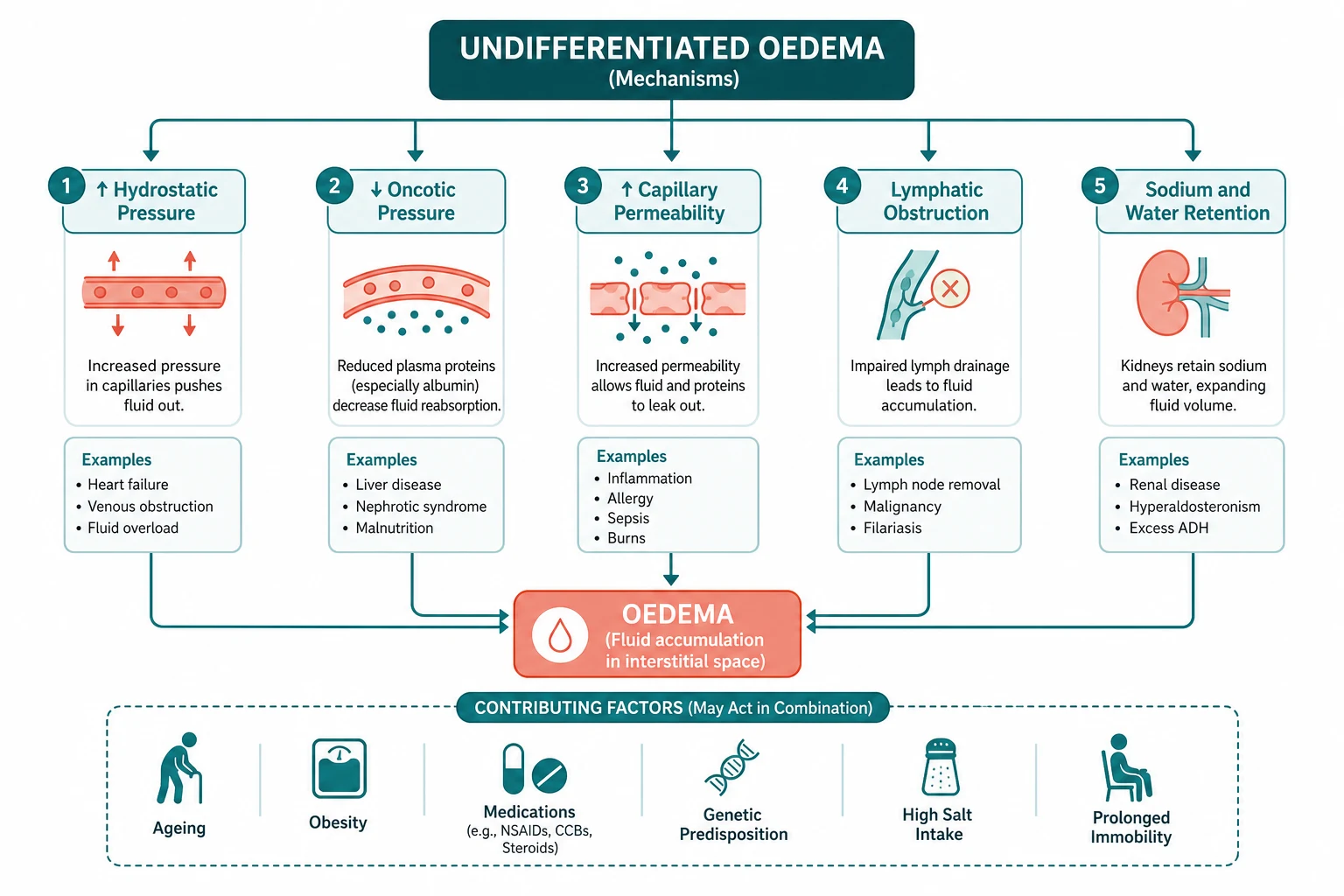
Oedema is defined as an accumulation of excess fluid in the interstitial or the potential spaces. Clinically apparent oedema implies that the interstitial fluid volume has expanded by approximately 2.5 to 3 litres — a reminder that the visible sign is a late marker of a substantial fluid shift. The mechanism, taught first by Ernest Starling in 1896, is that fluid moves across the capillary wall in response to a balance of hydrostatic and oncotic forces. When that balance is disturbed, fluid accumulates in the interstitium faster than the lymphatics can remove it. [1]
The classical Starling forces are four: [1]
- Capillary hydrostatic pressure (pushing fluid out of the capillary) — elevated in heart failure, venous obstruction, the arteriolar vasodilatation of the dihydropyridine calcium channel blockers, and the dependent posture.
- Plasma oncotic pressure (pulling fluid back into the capillary, generated almost entirely by albumin) — reduced in the nephrotic syndrome, the cirrhotic hypoalbuminaemia, protein-losing enteropathy, severe malnutrition, and the burns patient.
- Capillary permeability (the leakiness of the endothelium to fluid and protein) — increased in sepsis, the systemic inflammatory response, the anaphylaxis and the allergic reactions, the hereditary angioedema, and the toxins.
- Lymphatic drainage (the return of the filtered fluid and protein to the venous circulation) — impaired in the primary lymphoedema, the secondary lymphoedema after surgery or radiation, the filariasis, and the malignant lymphatic obstruction. [1]
The revised Starling model and the glycocalyx
The classical model taught that fluid is filtered at the arteriolar end of the capillary and reabsorbed at the venular end, with a small net filtrate returned by the lymphatics. The revised Starling model, reviewed by Woodcock and Woodcock, corrects this: under normal physiology, there is no significant venular reabsorption, because the endothelial glycocalyx layer (a thin layer of membrane-bound macromolecules on the luminal surface of the endothelium) generates the oncotic gradient across itself, not across the whole capillary wall [2]. The practical consequence is that almost all the filtered fluid is returned by the lymphatics, and the fluid that does re-enter the capillary at the venular end is a small fraction of the classical estimate.
This matters clinically in three ways. First, it explains why lymphatic failure causes protein-rich oedema (the filtered fluid is not reabsorbed and the protein accumulates in the interstitium) while hydrostatic oedema is protein-poor (the fluid is pushed out under pressure but the protein is retained in the capillary). Second, it explains why colloid resuscitation is less effective than the classical model predicted — the oncotic pull operates across the glycocalyx, not across the whole vessel, and when the glycocalyx is damaged by sepsis or inflammation, the colloid leaks into the interstitium and may worsen the oedema. Third, it explains why a low albumin alone is rarely sufficient to cause oedema until it falls below approximately 25 g per litre — the oncotic reserve is substantial, and the patient with a mildly low albumin and oedema usually has a second mechanism (sodium retention, venous obstruction, or a drug) operating alongside. [1]
The sodium-and-water-retention mechanism
A fifth mechanism, not captured in the classical Starling forces, is the renal retention of sodium and water in response to a perceived underfill of the arterial circulation. This is the dominant mechanism in cirrhosis (splanchnic vasodilatation from nitric oxide triggers the renin-angiotensin-aldosterone system and the non-osmotic vasopressin release, causing sodium and water retention and the dilutional hyponatraemia), in heart failure (the low cardiac output is sensed as underfill, the RAAS and the sympathetic nervous system are activated, and the sodium and water are retained), and in advanced CKD (the reduced nephron mass limits sodium excretion and the volume accumulates). This mechanism explains why the cirrhotic and the cardiac patient develop oedema even when the albumin is near-normal, and why the management must address the sodium retention (diuretics, sodium restriction, the treatment of the underlying disease) and not just the oncotic pressure. [1]
DWE high-yield: The single most testable fact about oedema pathophysiology is that a low serum albumin alone rarely causes oedema until it falls below approximately 25 g per litre, and that the commonest mechanisms of generalised oedema are the sodium and water retention of heart failure and cirrhosis and the hydrostatic and venous causes — not the pure oncotic failure. The registrar who attributes every oedema to a low albumin has misread the mechanism. [1]
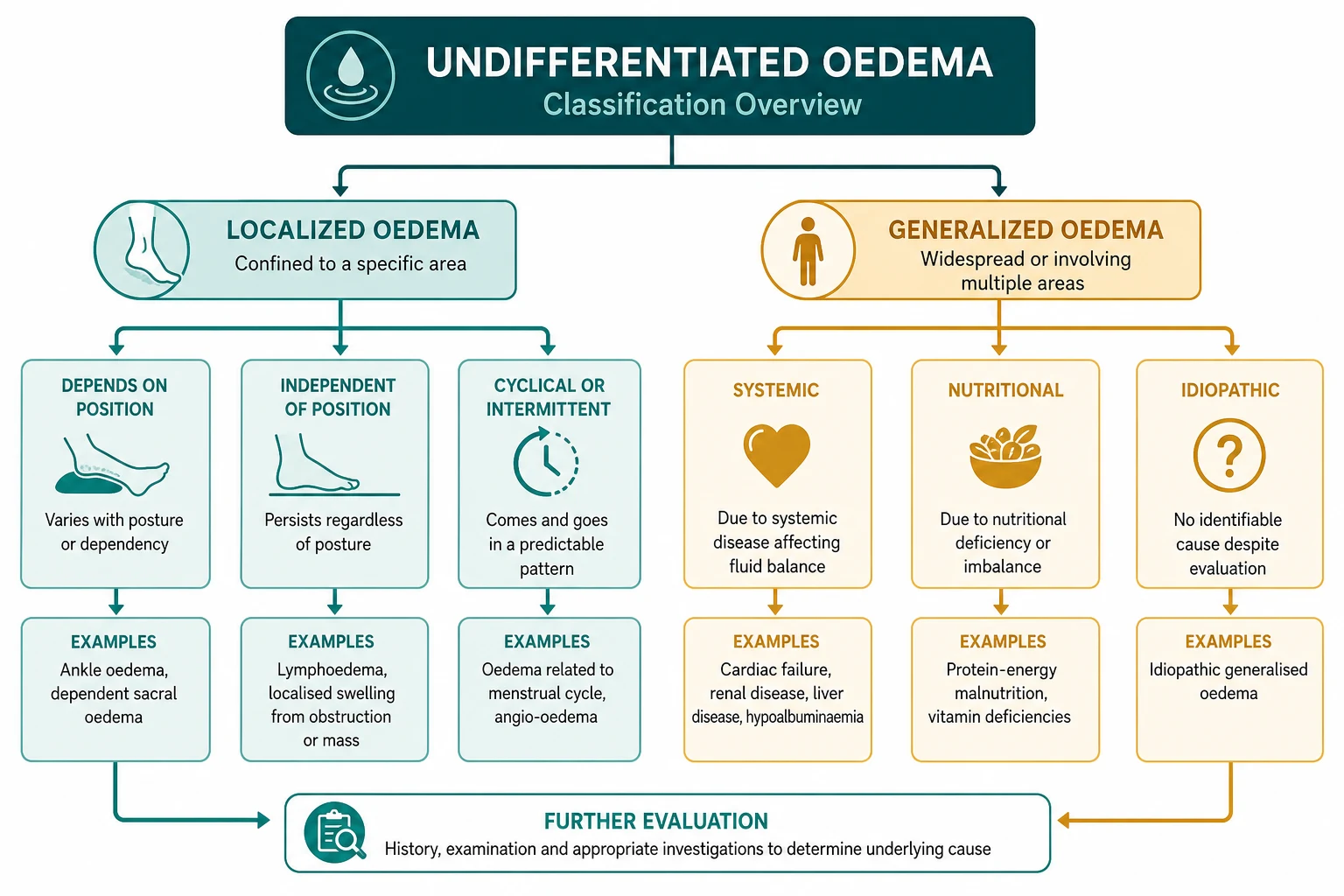
Localised versus generalised oedema — the first discriminator
The single most useful piece of information in the first minute with an oedematous patient is the distribution. Localised oedema (one leg, one limb, the face, the sacrum) points to a local cause — venous, lymphatic, infective, traumatic, or compartmental. Generalised oedema (both legs, the face and the legs, the sacrum and the legs, anasarca) points to a systemic cause — cardiac, hepatic, renal, endocrine, drug, or nutritional. [1]
Localised oedema — the unilateral swollen leg
The unilateral swollen leg is a high-yield presentation because the differential is finite and the consequences of a missed diagnosis (a pulmonary embolism from an undiagnosed DVT, a limb loss from a missed compartment syndrome) are severe. The causes are: [1]
- Deep vein thrombosis — calf pain, warmth, swelling, the risk factors (immobilisation, recent surgery, active cancer, pregnancy, oestrogen, a family history of VTE), and the Wells DVT score to stratify the probability. A Wells DVT score of 2 or more (PE likely) or a positive D-dimer in a patient with a Wells score of 1 or less mandates a compression ultrasound.
- Cellulitis — a warm, erythematous, tender, swollen leg with a defined advancing margin, often with a fever and a systemic upset, and a portal of entry (tinea pedis, an ulcer, a wound). The discriminator from DVT is the erythema with a defined margin and the systemic upset; the two may coexist (the cellulitis on a background of chronic venous insufficiency).
- Chronic venous insufficiency — bilateral or unilateral, with varicose veins, haemosiderin staining (the brown discoloration from extravasated red cells), lipodermatosclerosis (the induration of the skin and subcutaneous tissue), atrophie blanche (the white scarred areas), and a venous ulcer at the medial gaiter (the saphenous vein territory). The CEAP classification (Clinical, Etiological, Anatomical, Pathophysiological), revised by Eklöf and colleagues, grades the severity from C0 (no visible signs) to C6 (an active ulcer) [7].
- Compartment syndrome — a surgical emergency. The signs are pain disproportionate to the injury, pain on passive stretch of the muscles in the compartment, a tense and swollen compartment, paraesthesia, pallor, and (late) pulselessness. The cause is a fracture, a crush injury, a reperfusion injury, or a bleed into a tight fascial space. The management is an urgent compartment pressure measurement and a fasciotomy before the irreversible ischaemia.
- Ruptured Baker cyst — a sudden onset of calf pain and swelling in a patient with osteoarthritis or rheumatoid arthritis, often mimicking a DVT. The discriminator is the knee effusion and the history of arthritis; the ultrasound confirms the cyst rupture and excludes a DVT.
- Lymphoedema — a non-pitting, woody, protein-rich oedema from lymphatic obstruction or failure. Primary lymphoedema is congenital (Milroy disease) or of adult onset (lymphoedema tarda). Secondary lymphoedema follows axillary or groin lymph node dissection (especially after breast cancer surgery with radiotherapy), radiation, filariasis (the commonest cause worldwide), or a malignant lymphatic obstruction. The Stemmer sign — the inability to pinch a fold of skin at the base of the second toe — is positive in lymphoedema and negative in venous oedema.
- Trauma and post-traumatic oedema — a fracture, a soft tissue injury, a haematoma, or a ruptured tendon. The history and the imaging discriminate.
- Post-phlebitic syndrome — the chronic consequence of a prior DVT, with venous hypertension, leg swelling, pain, and the skin changes of chronic venous insufficiency. It may develop months to years after the DVT and is distinguished from an acute DVT by the chronicity and the absence of a new clot on the ultrasound.
DCE short-case high-yield: "Examine this patient's swollen leg." The registrar who walks to the calf and palpates for a tender cord has failed the question. The correct routine is inspect the distribution (unilateral versus bilateral, the skin changes of venous insufficiency, the woody non-pitting quality of lymphoedema), assess the pitting at the medial malleolus, grade the depth and the recovery time, measure the calf circumference at a fixed point, check the Stemmer sign, examine the arterial pulses and the ankle-brachial index, and examine the knee for a Baker cyst. The integrated examination that ends with the arterial assessment — because compression stockings are contraindicated if the arterial supply is compromised — is the senior approach the examiner is looking for. [1]
Generalised oedema — the systemic causes
Generalised oedema points to a systemic cause, and the registrar works through the cardiac, the hepatic, the renal, the drug, the endocrine and the nutritional mechanisms in turn. The mnemonic — CARDIAC, HEPATIC, RENAL, DRUG, ENDOCRINE, NUTRITIONAL, IDIOPATHIC — frames the differential and ensures no cause is missed. [1]
The cardiac causes of generalised oedema

The cardiac causes of generalised oedema are the diseases that raise the venous hydrostatic pressure or that retain sodium and water in response to a low cardiac output: [1]
- Right heart failure — the raised right ventricular filling pressure is transmitted to the jugular veins and the systemic venous circulation, causing a raised JVP, hepatomegaly (the congested liver), ascites, and bilateral dependent leg oedema. The causes include left heart failure (the commonest cause of right heart failure), right ventricular infarction, pulmonary hypertension (cor pulmonale), tricuspid regurgitation, and pulmonary embolism.
- Biventricular heart failure — the combination of the left heart failure signs (orthopnoea, paroxysmal nocturnal dyspnoea, bilateral basal crackles, a third heart sound, a displaced apex) and the right heart failure signs (raised JVP, hepatomegaly, dependent oedema). The NT-proBNP is the discriminator biomarker — the foundational Maisel study of 1586 patients established that a BNP above 100 pg/mL identified heart failure with an accuracy of 83.4 per cent and that a BNP below 50 pg/mL had a negative predictive value of 96 per cent [9]. The 2021 ESC Heart Failure Guidelines embed the NT-proBNP as the rule-out test in the dyspnoea and the oedema pathway [8].
- Constrictive pericarditis — one of the most commonly missed curable causes of generalised oedema. The signs are the raised JVP with the Kussmaul sign (the JVP rises on inspiration, the opposite of the normal, because the constricted right ventricle cannot accommodate the increased venous return), the pericardial knock (an early diastolic sound from the abrupt halt of the ventricular filling), the hepatomegaly, the ascites (often out of proportion to the leg oedema), and the cachexia. The history is critical — prior tuberculosis, prior mediastinal radiation, prior cardiac surgery, or a prior episode of viral or uraemic pericarditis. The echocardiogram, the CT (pericardial thickening and sometimes calcification), and the right and left heart catheterisation (the equalisation of the diastolic pressures and the dip-and-plateau waveform) confirm the diagnosis. The treatment is a pericardiectomy.
- Restrictive cardiomyopathy — the other cause of heart failure with a preserved ejection fraction and a restrictive physiology. The causes include amyloidosis (the echocardiographic findings of the thick walls with the granular sparkling texture, the low voltage on the ECG, and the discordance between the voltage and the wall thickness), the eosinophilic heart disease, the sarcoidosis, and the storage diseases. The discrimination from constrictive pericarditis requires the cardiac catheterisation and sometimes the cardiac MRI.
- Cor pulmonale — the right heart failure secondary to the pulmonary hypertension from the chronic lung disease (COPD, interstitial lung disease, the chronic thromboembolic pulmonary hypertension). The signs are the raised JVP, the peripheral oedema, the hepatomegaly, and the underlying respiratory signs (the loud P2, the right ventricular heave, the tricuspid regurgitation murmur, the wheeze, the crackles, the clubbing). The echocardiogram estimates the pulmonary artery pressure and the right heart catheterisation confirms.
The cardiac examination discriminators
The cardiac examination in the oedematous patient is often the single examination that identifies the mechanism: [1]
- JVP — elevated in all causes of right heart failure, constrictive pericarditis, restrictive cardiomyopathy, and cor pulmonale. The character matters: the Kussmaul sign (a rise on inspiration) suggests constriction; the prominent v waves suggest tricuspid regurgitation; the steep x and y descents suggest constriction or restrictive cardiomyopathy.
- Apex — displaced laterally in the dilated left ventricle; heaving in the pressure-overloaded left ventricle (aortic stenosis, hypertension); tapping and non-displaced in mitral stenosis.
- Murmurs — the systolic murmur of the aortic stenosis or the mitral regurgitation; the diastolic murmur of the aortic or the mitral stenosis; the pansystolic murmur of the tricuspid regurgitation (louder on inspiration — the Carvallo sign).
- Third heart sound — the gallop of the systolic heart failure.
- Pericardial knock — the early diastolic sound of the constrictive pericarditis.
- P2 — loud and palpable in the pulmonary hypertension. [1]
The hepatic causes of generalised oedema
The hepatic causes of generalised oedema are the diseases of the cirrhosis and the portal hypertension, and (less commonly) the acute liver failure. The oedema arises from a combination of the hypoalbuminaemia (reduced oncotic pressure), the portal hypertension (the splanchnic congestion and the ascites), and the sodium and water retention (the splanchnic vasodilatation from the nitric oxide triggers the RAAS and the non-osmotic vasopressin release). [1]
The clinical picture of the cirrhotic oedema is the combination of the stigmata of the chronic liver disease (the palmar erythema, the spider naevi, the gynaecomastia, the caput medusae from the recanalised umbilical vein, the jaundice, the asterixis, the clubbing, the Dupuytren contracture, the parotid enlargement), the hepatomegaly or the small shrunken liver, the splenomegaly (the portal hypertension), the ascites with a positive fluid thrill and a shifting dullness, and the bilateral dependent leg oedema. [1]
The serum-ascites albumin gradient (SAAG)
The single most important investigation in the hepatic oedema is the diagnostic ascitic tap and the serum-ascites albumin gradient (SAAG). The SAAG equals the serum albumin minus the ascitic fluid albumin. The Runyon study of 901 paired samples established that a SAAG of 11 g per litre or above identified portal hypertension with 96.7 per cent accuracy and that the SAAG was superior to the traditional transudate-exudate classification (which was correct only 55.6 per cent of the time) [4].
- SAAG of 11 g per litre or above (portal hypertension): cirrhosis, heart failure (including the constrictive pericarditis and the restrictive cardiomyopathy, where the right heart congestion raises the hepatic sinusoidal pressure and the ascitic albumin is low), the Budd-Chiari syndrome (the hepatic vein thrombosis).
- SAAG below 11 g per litre (no portal hypertension): the peritoneal carcinomatosis, the tuberculous peritonitis, the nephrotic syndrome (the ascitic albumin is relatively high because the albumin leaks globally), the pancreatic ascites, the chylous ascites, the serositis of the connective tissue disease. [1]
The registrar who applies the transudate-exudate concept to the ascites has revealed a knowledge gap — the validated criterion is the SAAG, and the cell count (a neutrophil count above 250 per microlitre indicates the spontaneous bacterial peritonitis) is the other mandatory result. [1]
The complications of cirrhotic ascites
The cirrhotic ascites carries the complications that change the management: [1]
- Spontaneous bacterial peritonitis — the infection of the ascitic fluid without an obvious intra-abdominal source, presenting with the abdominal pain, the fever, the worsening encephalopathy, or the unexplained renal dysfunction. The diagnosis is the ascitic neutrophil count above 250 per microlitre, and the treatment is the third-generation cephalosporin (cefotaxime 2 g every 12 hours intravenously).
- Hepatorenal syndrome — the renal failure from the splanchnic vasodilatation and the renal vasoconstriction, diagnosed by the exclusion of the other causes of the AKI and treated with the terlipressin and the albumin.
- Hepatic hydrothorax — the pleural effusion (usually right-sided) from the ascitic fluid tracking through the diaphragmatic defects.
- Umbilical herniation — the risk of rupture and the infection. [1]
The safe diuresis of the cirrhotic ascites is the spironolactone (up to 400 mg daily) with the furosemide (up to 160 mg daily) in a ratio of 100 mg spironolactone to 40 mg furosemide to maintain the normokalaemia. The target weight loss is 0.5 kg per day in the patient without the peripheral oedema and 1 kg per day in the patient with the peripheral oedema — a faster diuresis precipitates the hepatorenal syndrome. [1]
The renal causes of generalised oedema
The renal causes of generalised oedema are the diseases that cause the protein loss (the nephrotic syndrome), the glomerular inflammation (the nephritic syndrome), the chronic kidney disease (the sodium retention), and the acute kidney injury (the oliguria). [1]
Nephrotic syndrome
The nephrotic syndrome is the tetrad of the heavy proteinuria (greater than 3.5 g per day), the hypoalbuminaemia, the oedema, and the hyperlipidaemia. The oedema is classically the periorbital and the facial (worst in the morning, the patient wakes with swollen eyes), the dependent leg, and the genital. The pathophysiology is a combination of the underfill (the hypoalbuminaemia reduces the oncotic pressure and the fluid leaks to the interstitium) and the overfill (a primary renal defect in the sodium excretion, independent of the oncotic pressure). [1]
The work-up of the nephrotic syndrome is the 24-hour urine protein or the spot urine protein-to-creatinine ratio (to quantify the protein loss), the serum albumin, the renal function, the serum complement (C3 and C4), the hepatitis B and C and the HIV serology (the secondary causes), the serum electrophoresis and the free light chains (the amyloidosis and the myeloma), the autoimmune screen (the ANA and the anti-dsDNA for the lupus nephritis), and the renal biopsy for the histological diagnosis. The KDIGO 2021 Glomerular Diseases Guideline frames the evaluation and the management of the nephrotic syndrome by the histological diagnosis [5]:
- Minimal change disease — the commonest cause in the children and the younger adults; the steroid-responsive; the diagnosis of the exclusion on the light microscopy (no change) and the electron microscopy (the effacement of the podocyte foot processes).
- Membranous nephropathy — the commonest cause in the older adults; the phospholipase A2 receptor antibody positive in 70 to 80 per cent of the primary cases; the treatment with the corticosteroids and the cyclophosphamide or the calcineurin inhibitors or the rituximab.
- Focal segmental glomerulosclerosis (FSGS) — the scarring of some but not all glomeruli; the primary (idiopathic, the steroid-responsive in a subset) and the secondary (the HIV, the heroin, the obesity, the sickle cell, the reduced renal mass).
- Membranoproliferative glomerulonephritis — the immune complex pattern (the hepatitis C, the cryoglobulinaemia, the lupus) and the C3 glomerulopathy.
- Amyloidosis — the AL (the light chain) and the AA (the secondary, the chronic inflammation); the Congo red positive on the biopsy.
- Diabetic nephropathy — the thickening of the glomerular basement membrane and the mesangial expansion; the Kimmelstiel-Wilson nodules; the commonest cause of the nephrotic syndrome in the developed world. [1]
The Sethi and the Renal Pathology Society consensus on the pathologic classification of the glomerulonephritis reframes the reporting from the morphological to the etiological, and it is the modern framework the registrar should carry [6].
Nephritic syndrome
The nephritic syndrome is the tetrad of the haematuria, the proteinuria (sub-nephrotic), the hypertension, and the renal impairment. The oedema is from the sodium retention (the reduced glomerular filtration and the RAAS activation). The causes include the post-streptococcal glomerulonephritis, the IgA nephropathy, the rapidly progressive glomerulonephritis (the crescentic, the ANCA-associated, the anti-GBM), the lupus nephritis, and the infective endocarditis-associated glomerulonephritis. [1]
The renal examination discriminators
The renal examination in the oedematous patient is the periorbital oedema, the frothy urine on the urinalysis (the 3+ or the 4+ proteinuria of the nephrotic syndrome, or the blood and the protein of the nephritic syndrome), the hypertension, the palpable bladder or the enlarged kidneys (the polycystic, the obstructive), and the peripheral stigmata of the systemic disease (the butterfly rash of the lupus, the purpura of the vasculitis, the nodules of the diabetes). [1]
The single highest-yield bedside investigation in the renal oedema is the urinalysis — the patient with the oedema and the 3+ proteinuria has the nephrotic syndrome until proven otherwise, and the registrar who does not dip the urine has missed the diagnosis at the bedside. [1]
Why the nephrotic patient is at high risk of VTE
The nephrotic patient is at a high risk of the venous thromboembolism because of the loss of the antithrombin III in the urine, the increased hepatic synthesis of the fibrinogen and the factor VIII, the hyperviscosity, and the immobilisation. The risk is highest with the membranous nephropathy and the serum albumin below 25 g per litre. The prophylactic anticoagulation is indicated when the albumin is below 25 g per litre, or when there is a known thrombosis. [1]
The drug causes of oedema — the most often missed
The drug history is the single most cost-effective investigation in the patient with the new-onset generalised oedema and a normal examination. The common drugs and their mechanisms are: [1]
- Dihydropyridine calcium channel blockers (amlodipine, nifedipine, felodipine) — the commonest drug cause. The mechanism, reviewed by Sica, is the preferential arteriolar vasodilatation that goes unmatched in the venous circulation, raising the capillary hydrostatic pressure and driving the fluid into the interstitium [3]. The oedema is a local vasodilatory phenomenon, not a systemic fluid retention — which is why the diuretics are unhelpful and potentially harmful (they reduce the plasma volume and may worsen the capillary pressure mismatch). The management is the dose reduction, the switch to a different agent (lercanidipine has less oedema; a non-dihydropyridine such as verapamil has a different mechanism), the addition of an ACE inhibitor or an ARB (the venodilatation balances the arteriolar vasodilatation), or the discontinuation and the use of a different antihypertensive class.
- NSAIDs — the sodium and water retention from the inhibition of the renal prostaglandin synthesis (the afferent arteriolar vasodilatation is lost, the renal blood flow falls, and the sodium and the water are retained). The oedema is often accompanied by the rising blood pressure and the rising creatinine.
- Corticosteroids — the sodium retention from the mineralocorticoid effect (especially the fludrocortisone and the high-dose hydrocortisone).
- Pioglitazone and rosiglitazone (the thiazolidinediones) — the PPAR-gamma-mediated plasma volume expansion. The pioglitazone is contraindicated in the NYHA class III and IV heart failure because of the risk of the pulmonary oedema.
- Minoxidil — the powerful arteriolar vasodilator; the oedema is the same mechanism as the dihydropyridines.
- Oestrogens and the oral contraceptives — the sodium and the water retention from the oestrogen effect.
- Diltiazem and verapamil (the non-dihydropyridines) — much less oedema than the dihydropyridines, because they do not cause the preferential arteriolar vasodilatation.
Viva trap: "The patient on amlodipine who develops leg oedema." The reflex is to add a diuretic. The correct answer is to recognise the mechanism (the arteriolar-venous mismatch), to stop the diuretic if one has been started (it worsens the intravascular depletion), and to reduce the amlodipine dose or to add an ACE inhibitor. The registrar who reaches for furosemide in the amlodipine oedema has misunderstood the mechanism and will make the patient worse. [1]
The endocrine causes of oedema
- Myxoedema (hypothyroid oedema) — the non-pitting oedema from the glycosaminoglycan (the hyaluronic acid) accumulation in the interstitium, classically the periorbital and the pretibial. The associated signs are the bradycardia, the cold intolerance, the delayed relaxation of the ankle jerk, the dry skin, the thinning of the hair, the slow speech, and the cognitive slowing. The diagnosis is the high TSH and the low free T4, and the treatment is the levothyroxine replacement.
- Pretibial myxoedema (the Graves dermopathy) — the localised dermopathy over the shins in the hyperthyroidism (the Graves disease), with the non-pitting, the indurated, the orange-peel-textured plaques. The patient is hyperthyroid (the low TSH, the high free T4, the positive TSH receptor antibody) and may have the exophthalmos and the thyroid acropachy. The treatment is the treatment of the Graves disease and the topical corticosteroids. The two conditions — the myxoedema of the hypothyroidism and the pretibial myxoedema of the Graves disease — share a name but are the opposite thyroid states, and the registrar who confuses them has revealed a fundamental knowledge gap.
- Cushing syndrome — the mineralocorticoid effect of the cortisol; the oedema is usually mild and the other signs (the moon face, the buffalo hump, the striae, the proximal myopathy, the hypertension, the glucose intolerance) dominate.
- Hyperaldosteronism — the sodium retention and the potassium loss; the oedema is uncommon (the aldosterone escape) but the hypertension and the hypokalaemia are the clues. [1]
The nutritional, the idiopathic and the lymphatic causes
- Protein malnutrition — the kwashiorkor in the developing world; the cachectic patient with the malignancy, the advanced COPD, the advanced liver disease, or the eating disorder. The oedema is from the hypoalbuminaemia and is often multifactorial in the multimorbid patient.
- Refeeding syndrome — the insulin release on the refeeding drives the intracellular shifts of the phosphate, the potassium and the magnesium, and the sodium and the water retention, causing the oedema, the heart failure and the arrhythmia in the malnourished patient restarted on the nutrition. The prevention is the slow refeeding (the 5 to 20 kcal per kg per day, increasing over 4 to 7 days) and the replacement of the phosphate, the potassium and the magnesium.
- Idiopathic or cyclical oedema — a diagnosis of the exclusion, almost exclusively in the women of the reproductive age, with the cyclical weight gain and the dependent oedema worse premenstrually, the normal cardiac, the hepatic and the renal work-up. The management is the compression stockings, the reduced dietary salt, and the cautious trial of the spironolactone. The diagnosis is made only after the organic causes are confidently excluded.
- Lymphoedema — the protein-rich interstitial accumulation from the lymphatic obstruction or the failure. The primary (Milroy disease, the lymphoedema tarda) and the secondary (the axillary or the groin node dissection, the radiation, the filariasis, the malignancy). The Stemmer sign is the bedside discriminator. The management is the complete decongestive therapy (the manual lymphatic drainage, the multi-layer compression bandaging, the exercise, the skin care), the compression garments, and the intermittent pneumatic compression. The diuretics are generally unhelpful because the oedema is protein-rich, not water-rich. [1]
The focused history — the questions that change the differential
The history in the oedematous patient is high-yield precisely because each answer narrows the differential. The registrar should ask, in order: [1]
Onset and progression. The acute onset (hours to days) of a unilateral leg swelling points to the DVT, the cellulitis, the compartment syndrome, the ruptured Baker cyst. The subacute onset (days to weeks) of the generalised oedema points to the decompensated heart failure, the nephrotic syndrome, the cirrhotic ascites, the AKI. The chronic progressive onset (months) points to the chronic venous insufficiency, the lymphoedema, the chronic heart failure, the CKD, the idiopathic or the cyclical oedema. [1]
Distribution and timing. The periorbital and the facial oedema, worst in the morning, points to the renal (the nephrotic, the nephritic) or the hypothyroid. The bilateral leg oedema, worst in the evening, relieved by the recumbency, points to the cardiac (the hydrostatic) or the venous insufficiency. The sacral oedema points to the recumbent or the immobile patient, the right heart failure, or the hypoalbuminaemia. The abdominal distension points to the ascites (the hepatic, the cardiac, the nephrotic, the malignant). The unilateral leg oedema points to the DVT, the cellulitis, the chronic venous insufficiency, the lymphoedema, the compartment syndrome. The upper limb oedema points to the lymphoedema after the axillary surgery, the superior vena cava obstruction, or the DVT of the upper limb. [1]
Positional behaviour. The oedema that worsens on standing and improves overnight points to the venous insufficiency or the drug-induced (the amlodipine) oedema. The oedema that is present throughout the day and does not shift much with the posture points to the lymphoedema or the myxoedema (the non-pitting, the glycosaminoglycan-rich). [1]
Associated symptoms. The dyspnoea, the orthopnoea and the paroxysmal nocturnal dyspnoea point to the heart failure. The jaundice, the easy bruising, the abdominal distension and the confusion point to the cirrhosis. The frothy urine, the reduced urine output and the facial swelling point to the nephrotic or the nephritic syndrome. The cold intolerance, the bradycardia, the dry skin and the constipation point to the hypothyroidism. The hot intolerance, the weight loss, the palpitations and the exophthalmos point to the Graves disease. The calf pain, the warmth and the unilateral swelling point to the DVT. [1]
Drug history. The mandatory question. The amlodipine, the nifedipine, the felodipine (the dihydropyridines). The NSAIDs. The corticosteroids. The pioglitazone. The minoxidil. The oestrogens. The fludrocortisone. The drug history is often the entire diagnosis in the patient with the otherwise normal work-up, and the discontinuation or the dose reduction is the entire treatment. [1]
Past history. The ischaemic heart disease, the heart failure, the COPD, the cirrhosis, the viral hepatitis, the diabetes, the autoimmune disease, the malignancy, the prior DVT, the prior thyroid disease, the prior neck radiation or surgery. [1]
The examination — the discriminators at the bedside
The examination of the oedematous patient is the systematic assessment of the distribution, the pitting, the JVP, the cardiovascular system, the abdomen, the skin, and the lymph nodes. [1]
The pitting assessment
Press the thumb firmly on the medial malleolus (or the sacrum, or the dorsum of the foot) for 5 seconds. The grade the depth of the pit and the time to recovery: [1]
- Grade 1: 2 mm pit, recovers immediately.
- Grade 2: 4 mm pit, recovers in 10 to 15 seconds.
- Grade 3: 6 mm pit, recovers in more than 30 seconds.
- Grade 4: 8 mm or more, recovers in minutes. [1]
The pitting oedema is the hallmark of the hydrostatic and the oncotic causes (the cardiac, the hepatic, the renal, the drug, the venous insufficiency). The non-pitting oedema is the hallmark of the lymphoedema and the myxoedema (the glycosaminoglycan-rich, the protein-rich interstitium that does not pit). The grade and the recovery time give a semi-quantitative measure of the severity and the chronicity, and they track the response to the treatment. [1]
The Stemmer sign
The Stemmer sign — the inability to pinch a fold of skin at the base of the second toe — is the bedside discriminator between the lymphoedema (positive) and the venous oedema (negative). The skin is thickened and tethered in the lymphoedema and cannot be lifted; in the venous oedema the skin is of normal thickness and can be pinched. The Stemmer sign, combined with the non-pitting quality and the woody texture, makes the clinical diagnosis of the lymphoedema. [1]
The cardiovascular examination
The JVP is the single most important cardiovascular sign in the oedematous patient. The raised JVP (more than 3 cm of water above the sternal angle) indicates the right heart failure, the constrictive pericarditis, the restrictive cardiomyopathy, the cor pulmonale, the tricuspid regurgitation, and the fluid overload. The character of the JVP (the Kussmaul sign, the prominent v waves, the steep x and y descents) refines the differential. The apex (displaced in the dilated left ventricle; heaving in the pressure overload), the murmurs (the aortic stenosis, the mitral regurgitation, the tricuspid regurgitation), the third heart sound (the systolic heart failure), the pericardial knock (the constriction), the loud P2 (the pulmonary hypertension) — each discriminator points to a specific cardiac cause. [1]
The abdominal examination
The abdominal examination in the oedematous patient identifies the hepatomegaly (the congested liver of the right heart failure, the cirrhotic liver), the splenomegaly (the portal hypertension), the ascites (the positive fluid thrill and the shifting dullness), the caput medusae (the recanalised umbilical vein of the cirrhosis), and the palpable bladder or the enlarged kidneys (the obstructive or the polycystic renal cause). The diagnostic ascitic tap and the SAAG are the confirmatory investigations for the ascites. [1]
The skin examination
The skin examination identifies the haemosiderin staining, the lipodermatosclerosis, the atrophie blanche and the venous ulcer of the chronic venous insufficiency; the woody, non-pitting, Stemmer-positive skin of the lymphoedema; the palmar erythema, the spider naevi, the gynaecomastia of the cirrhosis; the butterfly rash of the lupus; the orange-peel-textured pretibial plaques of the Graves dermopathy; the dry, the coarse, the pale skin of the hypothyroidism; and the clubbing, the cyanosis and the asterixis of the systemic disease. [1]
The first-tier investigations

The first-tier investigations are the bedside and the laboratory tests that discriminate the major categories of the oedema within hours. They are ordered together, interpreted together, and they frame the second-tier work-up. [1]
The urinalysis — the highest-yield bedside test
The urinalysis is the single highest-yield bedside investigation in the oedematous patient. The 3+ or the 4+ proteinuria identifies the nephrotic syndrome; the blood and the protein identify the nephritic syndrome; the leucocytes and the nitrites identify the urinary tract infection (a rare cause of the oedema, but a common precipitant of the AKI). The registrar who does not dip the urine has missed the renal diagnosis at the bedside. [1]
The full blood count, the urea and the electrolytes
The full blood count identifies the anaemia (a contributor to the high-output heart failure and a marker of the chronic disease), the leukocytosis of the infection, and the eosinophilia of the eosinophilic heart disease or the vasculitis. The urea and the electrolytes identify the renal failure (the rising creatinine, the falling eGFR), the hyponatraemia (the dilutional hyponatraemia of the cirrhosis and the heart failure), and the hypokalaemia (the hyperaldosteronism, the diuretic use). [1]
The liver function tests and the albumin
The liver function tests identify the hepatic cause — the low albumin, the elevated bilirubin, the elevated transaminases (in the acute hepatitis), the elevated alkaline phosphatase (in the cholestatic disease), the elevated gamma-glutamyl transferase, and the prolonged INR (the synthetic failure). The albumin is the key marker of the oncotic pressure and the synthetic function, and the serum albumin below 25 g per litre is the threshold at which the hypoalbuminaemia contributes meaningfully to the oedema. [1]
The thyroid function tests
The thyroid function tests identify the hypothyroidism (the high TSH, the low free T4) and the hyperthyroidism (the low TSH, the high free T4). The myxoedema of the hypothyroidism and the pretibial myxoedema of the Graves disease are both confirmed by the TFTs. [1]
The NT-proBNP
The NT-proBNP is the discriminator biomarker between the cardiac and the non-cardiac oedema. The foundational Maisel study established that the BNP above 100 pg/mL identified the heart failure with an accuracy of 83.4 per cent and that the BNP below 50 pg/mL had a negative predictive value of 96 per cent [9]. The 2021 ESC Heart Failure Guidelines embed the NT-proBNP as the rule-out test in the oedema pathway [8]. The false positives (the renal failure, the atrial fibrillation, the PE, the sepsis, the advanced age) and the false negatives (the obesity, the flash pulmonary oedema) must be carried.
The chest X-ray
The chest X-ray identifies the cardiomegaly, the pulmonary oedema, the pleural effusion, the hyperinflation of the COPD, and the masses. It is normal in the early heart failure, the cirrhosis, and the renal disease — a normal chest X-ray does not exclude a cardiac cause, and the registrar who is reassured by a normal film in an oedematous patient has misread the situation. [1]
The 12-lead ECG
The ECG identifies the atrial fibrillation, the ischaemic changes, the left ventricular hypertrophy, the low voltage of the amyloidosis, and the right heart strain. [1]
The second-tier investigations
The second-tier investigations are the imaging and the invasive tests that confirm the working diagnosis: [1]
- Echocardiogram — the left and the right ventricular function, the valvular disease, the estimated pulmonary artery pressure, the pericardial thickening or the effusion, the inferior vena cava distensibility. Indicated when the clinical suspicion or the NT-proBNP suggests the cardiac cause.
- 24-hour urine protein or the spot urine protein-to-creatinine ratio — the quantification of the protein loss. Indicated when the urinalysis shows the significant proteinuria.
- Renal biopsy — the histological diagnosis of the glomerular disease. Indicated for the nephrotic-range proteinuria in the adult, the unexplained nephritic syndrome, the rapidly progressive glomerulonephritis, and the systemic disease with the renal involvement.
- Diagnostic ascitic tap with the SAAG and the cell count — the discrimination of the portal hypertensive from the non-portal ascites, and the identification of the spontaneous bacterial peritonitis.
- CT abdomen and pelvis — the identification of the cirrhosis, the malignancy, the lymphadenopathy, and the obstruction.
- Venous duplex ultrasound — the confirmation of the DVT, the assessment of the venous insufficiency, and the mapping of the varicose veins.
- Lymphoscintigraphy — the confirmation of the lymphoedema when the clinical diagnosis is uncertain. [1]
The management — treat the cause, not the symptom
The overarching principle of the oedema management is to treat the underlying cause, not the symptom. The diuretic is a bridge to the definitive diagnosis and the definitive therapy, never a substitute for it. The cause-specific management is: [1]
Cardiac oedema
The cardiac oedema is managed with the loop diuretic (furosemide 20 to 40 mg orally or intravenously, reassess the weight, the JVP and the renal function at 24 to 48 hours), the sodium restriction (2 g per day), and the four pillars of the guideline-directed therapy for the HFrEF — the beta-blocker, the ACE inhibitor or the ARNI, the mineralocorticoid receptor antagonist, and the SGLT2 inhibitor [8]. The oedema resolves as the ventricular function improves on the guideline-directed therapy. The over-diuresis is the common error — the dry mucous membranes, the postural drop, the rising creatinine, and the worsening renal function are the signs to stop.
Hepatic oedema (cirrhotic ascites)
The cirrhotic ascites is managed with the spironolactone (up to 400 mg daily) and the furosemide (up to 160 mg daily) in a 100-to-40 ratio to maintain the normokalaemia, the sodium restriction (2 g per day), the fluid restriction (only if the hyponatraemia is present), and the cautious diuresis with the target weight loss of 0.5 kg per day in the patient without the peripheral oedema and 1 kg per day in the patient with the peripheral oedema. The refractory ascites requires the large-volume paracentesis with the albumin replacement (6 to 8 g per litre of the ascitic fluid removed), the evaluation for the liver transplant, and (in selected patients) the transjugular intrahepatic portosystemic shunt (TIPS). The spontaneous bacterial peritonitis is treated with the third-generation cephalosporin. [1]
Renal oedema (nephrotic syndrome)
The nephrotic oedema is managed with the treatment of the underlying glomerular disease (the corticosteroids for the minimal change disease; the corticosteroids and the cyclophosphamide or the rituximab for the membranous nephropathy; the ACE inhibitor or the ARB for the proteinuria reduction), the sodium restriction, the judicious diuresis (the furosemide with the intravenous albumin in the severe hypoalbuminaemia), and the prophylactic anticoagulation when the albumin is below 25 g per litre. The KDIGO 2021 Glomerular Diseases Guideline frames the immunosuppressive therapy by the histological diagnosis [5]. The registrar must not diurese the nephrotic patient without treating the cause — the diuretic alone cannot mobilise the interstitial fluid when the oncotic pressure is critically low, and the patient develops the intravascular depletion and the pre-renal AKI.
Drug-induced oedema
The drug-induced oedema is managed by the discontinuation or the dose reduction of the offending drug. The amlodipine oedema is managed by the dose reduction, the switch to the lercanidipine or the non-dihydropyridine, the addition of the ACE inhibitor, or the discontinuation. The NSAID oedema is managed by the discontinuation. The pioglitazone oedema is managed by the discontinuation (and the pioglitazone is contraindicated in the heart failure). The corticosteroid and the fludrocortisone oedema is managed by the dose reduction and the transition to an alternate-day regimen or a mineralocorticoid-sparing alternative. [1]
Venous insufficiency and lymphoedema
The venous insufficiency is managed with the graduated compression stockings (20 to 40 mmHg at the ankle, applied before standing, replaced every 3 to 6 months), the leg elevation, the exercise, the weight management, the skin care, and the treatment of the varicose veins (the endovenous laser ablation, the radiofrequency ablation, the ultrasound-guided foam sclerotherapy). The compression is contraindicated in the significant arterial disease (the ankle-brachial index below 0.8), and the ABI must be checked before the compression is prescribed. [1]
The lymphoedema is managed with the complete decongestive therapy (the manual lymphatic drainage, the multi-layer compression bandaging, the exercise, the skin care), the compression garments, and the intermittent pneumatic compression. The diuretics are generally unhelpful because the oedema is protein-rich, not water-rich. The cellulitis is a common complication of the lymphoedema (the compromised skin barrier, the protein-rich interstitium that is a culture medium), and the prompt antibiotic treatment is essential. [1]
Endocrine oedema
The myxoedema is managed with the levothyroxine replacement (1.6 micrograms per kg per day in the younger patient; a lower starting dose in the older patient or the cardiac patient, with the gradual titration). The oedema resolves over weeks to months as the thyroid status normalises. The pretibial myxoedema of the Graves disease is managed with the treatment of the Graves disease and the topical corticosteroids under occlusion. [1]
The common exam traps
- The diuretic-before-diagnosis trap — reaching for the furosemide before the mechanism is identified. The amlodipine oedema does not respond to the furosemide (it worsens the intravascular depletion). The nephrotic oedema requires the albumin and the treatment of the glomerular disease. The lymphoedema requires the complete decongestive therapy, not the loop diuretic.
- The SAAG-versus-transudate-exudate trap — applying the transudate-exudate concept to the ascites. The validated criterion is the SAAG, and the candidate who cites the transudate-exudate classification has revealed a knowledge gap.
- The constrictive pericarditis trap — missing the curable cause. The patient with the generalised oedema, the raised JVP with the Kussmaul sign, the pericardial knock and the history of the prior radiation or the tuberculosis has the constrictive pericarditis, and the registrar who anchors on the cirrhosis or the heart failure has missed the diagnosis.
- The urinalysis trap — failing to dip the urine. The patient with the oedema and the 3+ proteinuria has the nephrotic syndrome until proven otherwise, and the registrar who does not dip the urine has missed the renal diagnosis at the bedside.
- The drug history trap — forgetting the drug history. The amlodipine, the NSAIDs, the steroids and the pioglitazone are among the commonest causes of the new-onset oedema, and the discontinuation or the dose reduction is the entire treatment.
- The myxoedema-versus-pretibial-myxoedema trap — confusing the two. The myxoedema is the hypothyroid (the high TSH, the non-pitting, the bradycardia). The pretibial myxoedema is the Graves disease (the low TSH, the hyperthyroid, the localised dermopathy). The two share a name but are the opposite thyroid states.
- The compression-in-arterial-disease trap — applying the compression stockings to a limb with the significant arterial disease. Check the ABI first, and contraindicate the compression if the ABI is below 0.8.
- The over-diuresis trap in cirrhosis — the faster diuresis than the target weight loss precipitates the hepatorenal syndrome. The target is 0.5 kg per day without the peripheral oedema and 1 kg per day with the peripheral oedema.
- The lymphoedema-as-venous-insufficiency trap — diagnosing the venous insufficiency in the patient with the non-pitting, the woody leg and the positive Stemmer sign. The two are managed differently, and the lymphoedema requires the complete decongestive therapy. [1]
The DCE long-case integration
In the DCE long case, the oedematous patient is presented with the SASPOP format (Symptoms, Age, Sex, Presentation, Occupation, Problems), the structured problem list (the oedema and its mechanism, the underlying cause, the complications, the comorbidities, the drug list, the functional and the social context), and the integrated management plan (the cause-specific treatment, the symptom relief, the prevention of the complications, the follow-up, and the communication and the shared decision-making). [1]
The registrar's job is to resist the pull of a single diagnosis. The patient with the bilateral leg oedema, the raised JVP, the ascites and the proteinuria has the cardiac, the hepatic and the renal mechanisms operating together, and the integrated management — the cautious diuresis, the treatment of the glomerular disease, the management of the cirrhosis, and the review of the drug list — is what keeps the complex patient safe. The registrar who stops at "heart failure" and treats only with the loop diuretic has missed the nephrotic syndrome, the cirrhosis, and the amlodipine. [1]
The communication and the shared decision-making — the explanation of the mechanism, the expectations of the treatment, the monitoring plan, and the red flags to report — are the final layer of the senior management. [1]
References
Cho and Atwood, Am J Med 2002; Woodcock and Woodcock, Br J Anaesth 2012; Sica, J Clin Hypertens 2003; Runyon et al., Ann Intern Med 1992; KDIGO Glomerular Diseases Guideline, Kidney Int 2021; Sethi et al. (Mayo Clinic/RPS GN consensus), JASN 2016; Eklöf et al. (CEAP revision), J Vasc Surg 2004; McDonagh et al. (ESC HF Guidelines), Eur Heart J 2021; Maisel et al. (BNP), NEJM 2002; NICE NG106; KDIGO Glomerular Diseases Guideline; GESA; Kidney Health Australia; ESC Heart Failure Guidelines. [1]
References
- [1]Cho S, Atwood JE Peripheral edema Am J Med, 2002.PMID 12459405
- [2]Woodcock TE, Woodcock TM Revised Starling equation and the glycocalyx model of transvascular fluid exchange: an improved paradigm for prescribing intravenous fluid therapy Br J Anaesth, 2012.PMID 22290457
- [3]Sica DA Calcium channel blocker-related periperal edema: can it be resolved? J Clin Hypertens (Greenwich), 2003.PMID 12939574
- [4]Runyon BA, Montano AA, Akriviadis EA, Antillon MR, Irving MA, McHutchison JG The serum-ascites albumin gradient is superior to the exudate-transudate concept in the differential diagnosis of ascites Ann Intern Med, 1992.PMID 1616215
- [5]Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases Kidney Int, 2021.PMID 34556300
- [6]Sethi S, Haas M, Markowitz GS, et al. Mayo Clinic/Renal Pathology Society Consensus Report on Pathologic Classification, Diagnosis, and Reporting of GN J Am Soc Nephrol, 2016.PMID 26567243
- [7]Eklöf B, Rutherford RB, Bergan JJ, et al.; American Venous Forum International Ad Hoc Committee for Revision of the CEAP Classification Revision of the CEAP classification for chronic venous disorders: consensus statement J Vasc Surg, 2004.PMID 15622385
- [8]McDonagh TA, Metra M, Adamo M, et al.; ESC Scientific Document Group 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure Eur Heart J, 2021.PMID 34447992
- [9]Maisel AS, Krishnaswamy P, Nowak RM, et al.; Breathing Not Properly Multinational Study Investigators Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure N Engl J Med, 2002.PMID 12124404