Phys · general-medicine
Undifferentiated Palpitations — Diagnostic Challenge
Also known as palpitations · awareness of heartbeat · pounding heart · racing heart · missed beats · extra beats · ectopic beats · fluttering chest · undifferentiated palpitations diagnostic approach · palpitation workup
Consultant-physician guide to the patient presenting with undifferentiated palpitations — the awareness of heartbeat — at FRACP DWE and DCE depth: the four-descriptor classification (regular fast, irregular, missed beat or extra beat, forceful pounding), the discriminating history (sudden versus gradual onset and offset, polyuria after termination pointing to SVT, exercise provocation pointing to VT or structural disease, the family history of sudden death pointing to a channelopathy), the cardiovascular and thyroid examination, the mandatory 12-lead ECG interpretation (AF, SVT, VT, long QT, WPW delta wave, Brugada pattern, LVH, ischaemia), the tiered ambulatory ECG strategy matched to symptom frequency (Holter for daily, event monitor for weekly, implantable loop recorder for monthly or rarer), the echocardiogram for structural disease, the electrophysiology study, and the cause-directed management (vagal manoeuvres, AV nodal blockers and catheter ablation for SVT, rate or rhythm control and anticoagulation for AF, urgent cardiology referral and ICD for VT, specialist evaluation for the channelopathies and cardiomyopathies) — with the DCE long-case and short-case presentation templates, the examiner discussion questions, and the classic exam traps.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Undifferentiated Palpitations — Diagnostic Challenge

The one-minute consultant answer
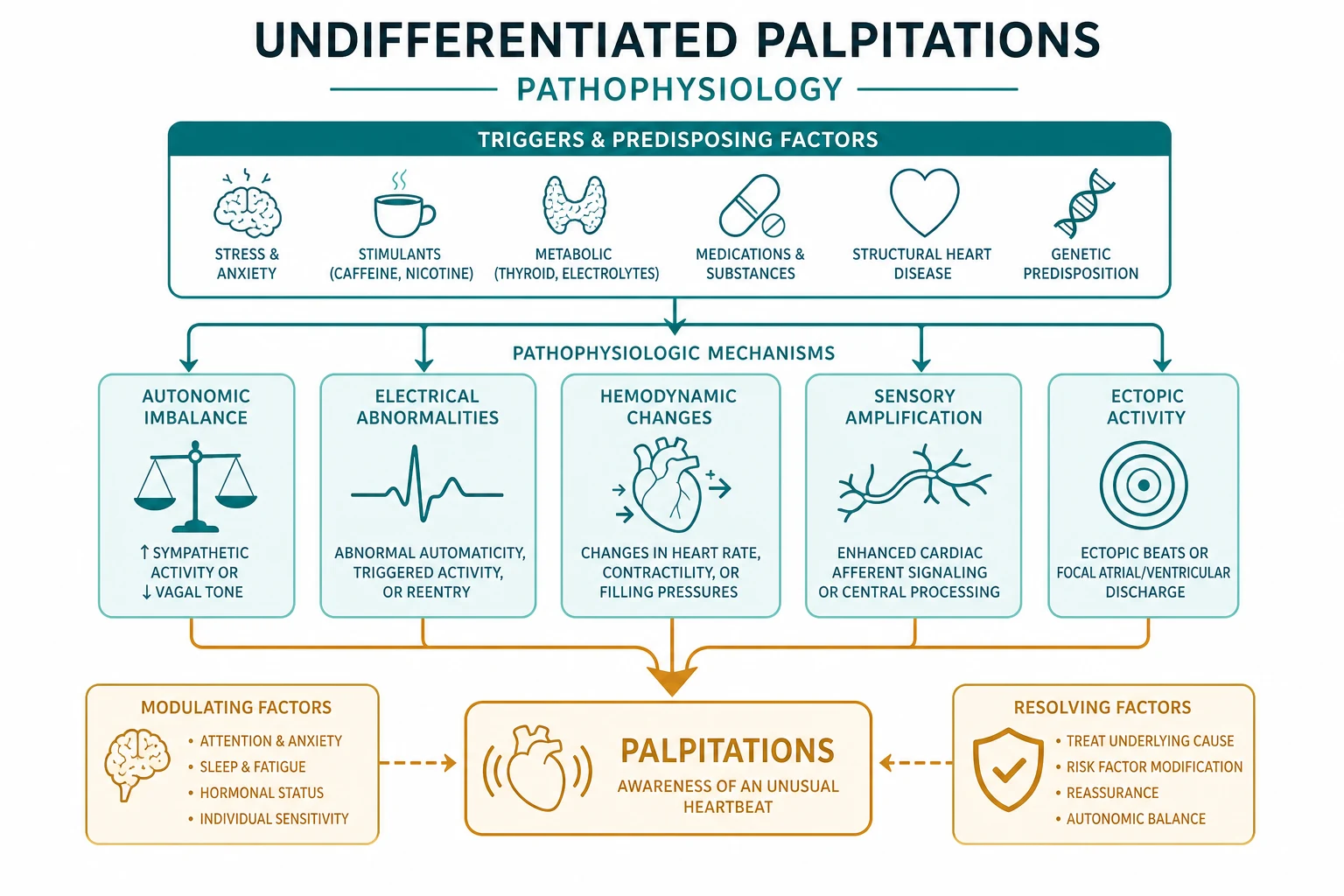
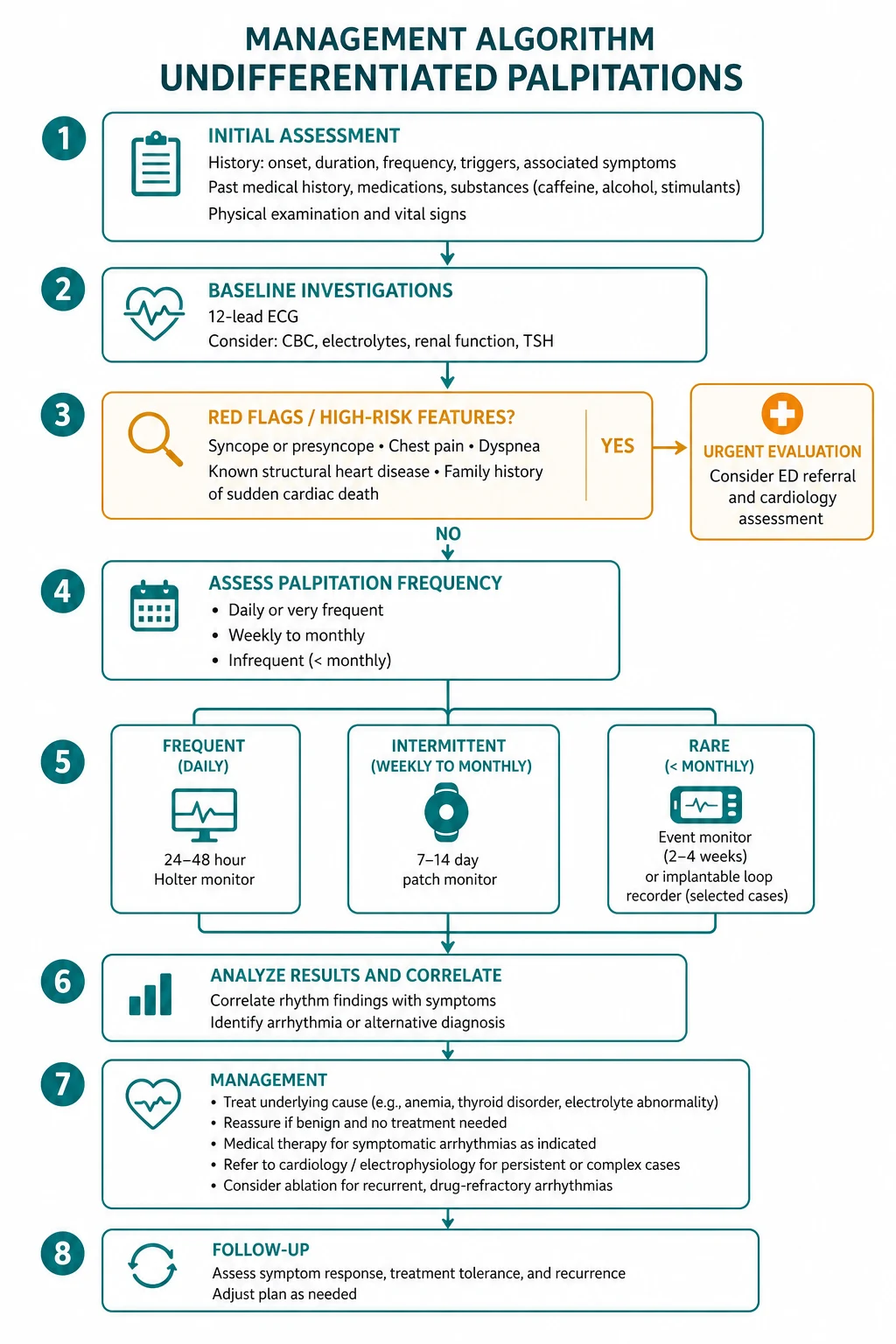
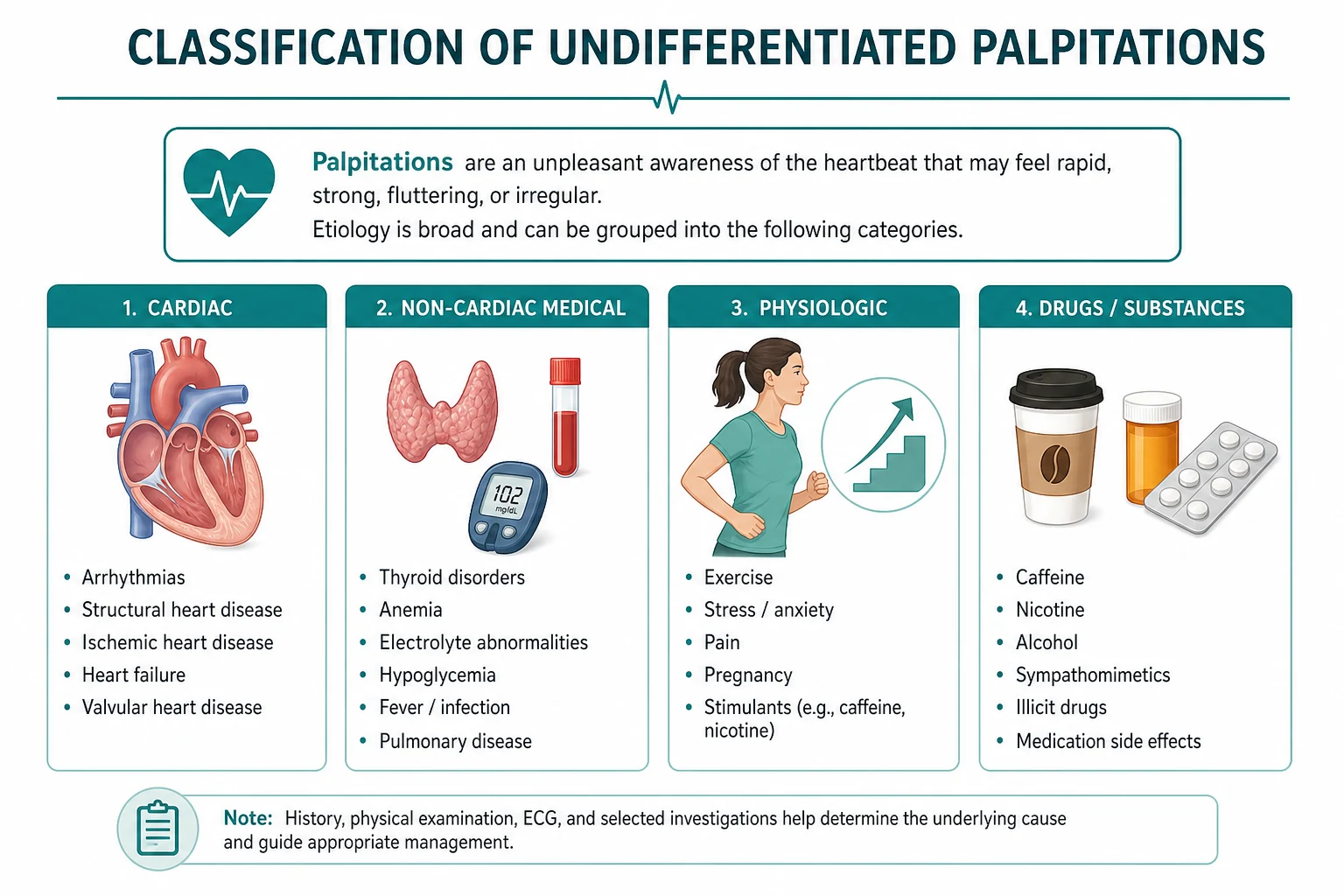
Palpitations are the awareness of the heartbeat, and the single most important question is whether the rhythm during the symptom is regular or irregular, and whether the onset and offset are sudden or gradual. The history is the investigation — the ECG confirms what the history suspects, and ambulatory monitoring captures what the ECG between episodes misses. The triage that saves lives is the recognition of the high-risk features: syncope, exertional symptoms, a family history of sudden cardiac death under the age of 40, structural heart disease, and a broad-complex or pre-excited tachycardia on the ECG. These features escalate the patient from reassurance to urgent cardiology referral. [1]
The non-negotiable principle: every patient with palpitations gets a 12-lead ECG at presentation, no exceptions. The ECG between episodes may be normal in up to half of patients with a documented arrhythmia, so a normal resting ECG never excludes an arrhythmia — it merely means you need ambulatory monitoring. The diagnostic yield of ambulatory monitoring is directly proportional to how well the monitoring strategy is matched to the frequency of the symptoms: a 24-hour Holter for daily symptoms, a patient-activated event monitor or patch recorder for weekly symptoms, and an implantable loop recorder for symptoms that are monthly or rarer. A Holter for a patient whose palpitations come every six weeks is wasted effort — the diagnostic yield is near zero. [1]
The winning framework is the four-descriptor classification of the symptom character, which narrows the differential before any test is ordered: [1]
- Regular fast rhythm — sinus tachycardia (a physiological response to a systemic cause) or a paroxysmal supraventricular tachycardia (AVNRT, AVRT) or ventricular tachycardia.
- Irregular rhythm — atrial fibrillation (the irregular irregularity), atrial flutter with variable block (the regularly irregular pattern with grouped beating), or frequent ectopic beats (atrial or ventricular).
- Missed beat or extra beat — ectopic beats; the patient perceives the compensatory pause after an ectopic as a missed beat, and often the post-ectopic beat as a thud, because the next sinus beat has a larger stroke volume after the pause.
- Pounding or forceful beat in a regular rhythm — sinus rhythm with increased stroke volume: anaemia, thyrotoxicosis, pregnancy, fever, aortic regurgitation, mitral valve prolapse, anxiety, and sympathomimetic drugs (caffeine, salbutamol, decongestants containing pseudoephedrine). [1]
The classification tree — narrowing the differential from the history

The classification tree is built from three history questions: the rate (fast or normal), the rhythm (regular or irregular), and the onset and offset (sudden or gradual). A fourth question — the character (missed beat, pounding, fluttering) — refines the branches. Each leaf of the tree points to a small set of diagnoses, each with discriminating features that the history and the ECG confirm. [1]
Regular fast rhythm
A regular fast rhythm narrows the differential to sinus tachycardia, paroxysmal supraventricular tachycardia, and ventricular tachycardia. The discriminating history feature is the onset and offset. [1]
- Sinus tachycardia has a gradual onset and a gradual offset — the rate rises over minutes and falls over minutes in response to the physiological stimulus (fever, anxiety, pain, hypovolaemia, anaemia, thyrotoxicosis, pregnancy, sympathomimetic drugs). The rate does not exceed approximately 220 beats per minute minus the age. Sinus tachycardia at rest, without an identifiable stimulus, is inappropriate sinus tachycardia — a separate entity requiring specialist evaluation [1].
- Paroxysmal supraventricular tachycardia has a sudden onset and a sudden offset — the patient can often name the minute the episode started and the minute it stopped. The rate is typically 150 to 250 beats per minute, and the rhythm is regular. A terminating episode followed by a brisk polyuria is highly suggestive of SVT — the atrial natriuretic peptide released during the tachycardia drives the diuresis after the rhythm restores [2][6].
- Ventricular tachycardia may present with a regular fast rhythm, but the history usually carries a red flag: palpitations on exertion, palpitations with syncope or near-syncope, palpitations in a patient with known structural heart disease (prior infarction, cardiomyopathy), or a family history of sudden cardiac death. VT in a structurally normal heart is rarer and includes the idiopathic outflow-tract VTs and the channelopathy-related polymorphic VTs.
Irregular rhythm
An irregular rhythm narrows the differential to atrial fibrillation, atrial flutter with variable block, and frequent ectopic beats. The discriminating feature is the pattern of irregularity. [1]
- Atrial fibrillation is irregularly irregular — there is no pattern to the rhythm, and the pulse is chaotic. The rate may be fast (the presentation of new-onset AF with a rapid ventricular response) or normal (the well-rate-controlled chronic AF). The absence of P waves and the absence of a regular pattern on the ECG confirm the diagnosis [3].
- Atrial flutter with variable block is regularly irregular — there is a pattern (often grouped beating, such as a short-short-long sequence) because the atrial rate is regular (typically 300 per minute) and the ventricular response varies (2:1, 3:1, 4:1 conduction). The sawtooth flutter waves are visible in the inferior leads (II, III, aVF) when the ventricular rate is slowed.
- Frequent ectopic beats produce an irregular rhythm with a recognisable pattern — a normal beat followed by an early beat and then a compensatory pause, repeating in a cadence. The patient may describe a missed beat, a thud, or a flop. Atrial ectopics and ventricular ectopics produce the same symptom; the ECG distinguishes them.
Missed beat or extra beat sensation
The missed beat or extra beat sensation is the cardinal feature of ectopic beats — atrial or ventricular. The teaching point that examiners probe: the patient feels the compensatory pause after the ectopic as the missed beat, and the next sinus beat (with a larger stroke volume after the pause) as a thud or a pound. The ectopic itself is rarely felt. The history asks about the frequency (a few per day, or thousands per day), the triggers (caffeine, alcohol, stress, fatigue, the premenstrual phase), and the associated symptoms (dizziness, breathlessness). The investigation is the ECG (to confirm the ectopy if it is captured during the recording) and ambulatory monitoring (to quantify the burden). A ventricular ectopic burden of more than approximately 10 to 15 per cent of total beats on a 24-hour Holter, in a patient with structural heart disease, carries a risk of a cardiomyopathy and warrants a cardiology referral [9].
Pounding or forceful sensation in a regular rhythm
The pounding or forceful sensation in a regular rhythm is the awareness of an increased stroke volume in sinus rhythm. The differential is the systemic and cardiac causes of an increased stroke volume: anaemia (check the haemoglobin and the ferritin), thyrotoxicosis (check the TSH and the free T4 — the thyroid is the silent cause of many a pounding heart), pregnancy (the increased blood volume and cardiac output), fever (the tachycardia and the vasodilatation), aortic regurgitation (the high stroke volume from the regurgitant flow — feel the collapsing pulse, the water-hammer pulse of Corrigan), mitral valve prolapse (the mid-systolic click and the late systolic murmur, with the palpitations attributed to the autonomic dysregulation and the ectopy that accompanies the prolapse), anxiety (the diagnosis of exclusion, after the systemic and cardiac causes are excluded), and sympathomimetic drugs (caffeine in excess, salbutamol inhalers, the pseudoephedrine in over-the-counter decongestants, the thyroxine in over-replaced hypothyroidism, the cocaine and the amphetamines in recreational use). [1]
The focused history — the questions that change the diagnosis
The history is the most powerful investigation in the palpitations encounter. Six structured questions narrow the differential before any test is ordered. [1]
Question 1 — Onset: sudden or gradual?
Sudden onset (the patient can name the moment — at 3:14 pm, sitting at the desk, the heart jumped) points to a re-entrant tachycardia (AVNRT, AVRT) or to the initiation of atrial fibrillation. The re-entrant tachycardias are initiated by an ectopic beat that establishes a circus movement through the re-entrant circuit. Gradual onset (the heart rate climbed over several minutes, in response to a stimulus — exercise, emotion, fever, blood loss) points to sinus tachycardia, the physiological response to a systemic demand. [1]
Question 2 — Duration: seconds, minutes, or hours?
Seconds (a brief flutter or a thud, gone in a moment) points to ectopic beats or to a non-sustained tachycardia (a run of three or more ventricular beats that self-terminates within 30 seconds). Minutes (a sustained episode lasting 5 to 30 minutes) points to a paroxysmal SVT or a paroxysmal AF. Hours (an episode that lasts until the patient seeks medical attention) points to atrial fibrillation (which may persist for days before presentation), a persistent SVT (which is uncommon, as most SVTs terminate spontaneously within minutes to hours), or sustained VT (which is a medical emergency). [1]
Question 3 — Termination: sudden or gradual?
Sudden termination (the patient can name the moment the rhythm stopped — it just switched off) points to a re-entrant tachycardia that broke the circuit, often terminated by a vagal manoeuvre (the Valsalva, the carotid sinus massage, the cold water on the face). Gradual termination (the heart rate drifted down over minutes) points to sinus tachycardia resolving as the stimulus resolves. A terminating episode followed by a brisk polyuria is the discriminating feature of SVT — the atrial natriuretic peptide, released from the atrial myocardium during the tachycardia, drives a diuresis after the rhythm restores, and the patient passes large volumes of dilute urine for an hour or two [2].
Question 4 — Triggers and modifiers
Exercise-provoked palpitations are a red flag — they point to VT (ischaemic, idiopathic outflow-tract, or the channelopathy-related polymorphic VT such as catecholaminergic polymorphic ventricular tachycardia) or to structural disease (hypertrophic cardiomyopathy, aortic stenosis, ischaemic heart disease). Position-provoked palpitations (the sensation that comes on lying down, or on bending over, or on standing up suddenly) point to AVNRT (the increased venous return on lying down triggers an ectopic that initiates the circuit) or to the postural orthostatic tachycardia syndrome (POTS — a sinus tachycardia of more than 30 beats per minute on standing, without orthostatic hypotension). Substance-provoked palpitations (caffeine, alcohol — the holiday heart syndrome of AF after a weekend of binge drinking, cocaine, amphetamines, cannabis) point to a triggered arrhythmia. Stress and emotion-provoked palpitations point to sinus tachycardia or to the CPVT (the adrenergic surge provoking the bidirectional VT) [5].
Question 5 — Associated symptoms
The associated symptoms separate the benign from the dangerous. Syncope or near-syncope during the palpitations is a red flag — it indicates cerebral hypoperfusion from a haemodynamically compromising tachycardia (fast VT, a very rapid SVT with a poor cardiac reserve, or a profound pause on termination of a tachycardia — the overdrive suppression of the sinus node). Chest pain during the palpitations may indicate ischaemia (a demand ischaemia from a fast heart rate, or the supply ischaemia of coronary artery disease precipitating VT), or it may be the atypical chest pain of the mitral valve prolapse syndrome. Dyspnoea during the palpitations indicates a loss of the atrial contribution to filling (AF in a stiff ventricle) or a haemodynamically compromising rate. Polyuria after the episode is the SVT discriminator [2]. A flushed sensation, sweating, or nausea may accompany the autonomic surge of any tachycardia and is non-discriminating.
Question 6 — The drug, the family, and the past cardiac history
The drug history asks specifically about the sympathomimetics (the salbutamol inhaler for asthma, the pseudoephedrine in the cold-and-flu tablets, the caffeine in the energy drinks and the coffee, the thyroxine in over-replaced hypothyroidism), the QT-prolonging drugs (the macrolide antibiotics — erythromycin, clarithromycin; the fluoroquinolones — ciprofloxacin, moxifloxacin; the antipsychotics — haloperidol, ziprasidone; the antiemetics — ondansetron; the methadone), and the antiarrhythmics (the pro-arrhythmic potential of flecainide and propafenone, especially in structural heart disease — the CAST trial finding). [1]
The family history asks specifically about sudden cardiac death under the age of 40, unexplained drowning (the long QT syndrome type 1, triggered by swimming), a family member with a pacemaker or an ICD at a young age, and the inherited cardiomyopathies (hypertrophic cardiomyopathy — the leading cause of sudden cardiac death in the young athlete; arrhythmogenic right ventricular cardiomyopathy; the channelopathies — long QT, Brugada, CPVT). A first-degree relative with sudden cardiac death under 40 is a red flag that mandates an ECG, an echocardiogram, and a specialist evaluation [5].
The past cardiac history asks about prior myocardial infarction (the substrate for VT — the scarred myocardium is the re-entrant circuit), heart failure (the substrate for AF and VT), valve disease (the mitral stenosis that predisposes to AF, the mitral regurgitation, the aortic stenosis), prior cardiac surgery, and the congenital heart disease (the repaired tetralogy of Fallot that predisposes to VT late after the repair). [1]
The focused examination

The examination in the palpitations encounter has two goals: to identify a structural cardiac cause, and to identify a systemic cause. The examination is the full cardiovascular examination plus the thyroid and the general inspection for the systemic causes. [1]
General inspection and vital signs
General inspection notes the distress, the pallor (anaemia), the flushing (thyrotoxicosis, the carcinoid), the sweating (thyrotoxicosis, phaeochromocytoma, anxiety), the tremor (thyrotoxicosis, the sympathomimetics), and the signs of chronic disease (cachexia, the chronic heart failure, the chronic renal failure). The vital signs are mandatory: the heart rate (and the confirmation at the radial and the apex — the apex-radial deficit of AF), the blood pressure (the wide pulse pressure of aortic regurgitation, the postural drop of dehydration or autonomic failure), the respiratory rate (the acidosis of the metabolic causes — the Kussmaul breathing of the ketoacidosis), the temperature (the fever of the infective trigger), and the oxygen saturation. [1]
The cardiovascular examination
The pulse is the first discriminator. Assess the rate, the rhythm, the character, and the volume. A fast regular pulse with a sudden history is SVT until proven otherwise; a fast irregular pulse is AF until the ECG shows otherwise; a bounding collapsing pulse is aortic regurgitation; a small-volume pulse is the low-output state of heart failure or pericardial tamponade. The apex beat assesses the location (displaced in cardiomegaly, dilated cardiomyopathy, volume overload), the character (the thrusting volume-loaded apex of aortic regurgitation, the pressure-loaded sustained apex of aortic stenosis or hypertension, the double impulse of hypertrophic cardiomyopathy, the tapping apex of mitral stenosis). A right ventricular heave (a sustained impulse felt at the left parasternal edge) suggests right ventricular hypertrophy or dilatation (pulmonary hypertension, the arrhythmogenic right ventricular cardiomyopathy, cor pulmonale). [1]
The heart sounds and the murmurs complete the cardiac examination. The first heart sound is loud in mitral stenosis (the taut valve leaflets snapping shut) and soft in mitral regurgitation or first-degree AV block. The second heart sound — the splitting (the wide splitting of the right bundle branch block, the paradoxical splitting of the left bundle branch block or the aortic stenosis, the fixed splitting of the atrial septal defect). The added sounds — the third heart sound of heart failure, the fourth heart sound of the stiff ventricle (hypertension, aortic stenosis, hypertrophic cardiomyopathy), the opening snap of mitral stenosis, the pericardial knock of constrictive pericarditis. The murmurs — the ejection systolic of the aortic stenosis (radiating to the carotids, the right upper sternal border, the slow-rising pulse) and the pulmonary stenosis; the pansystolic of the mitral regurgitation (the apex, the axilla) and the tricuspid regurgitation (the left lower sternal border, the increased with inspiration — Carvallo sign, the prominent v waves in the JVP, the pulsatile liver); the early diastolic of the aortic regurgitation (the left lower sternal border, the sitting forward, the end-expiration, the decrescendo, the blowing) and the pulmonary regurgitation; the mid-diastolic of the mitral stenosis (the low-pitched rumble, the apex, the left lateral position, the opening snap); the late systolic click and murmur of the mitral valve prolapse (the mid-systolic click followed by a late systolic murmur, the click moves earlier with the Valsalva and the standing, later with the squatting). [1]
The thyroid examination
The thyroid examination is mandatory in the palpitations encounter — thyrotoxicosis is the silent cause of many a pounding heart and many a new AF. Inspect the neck (the goitre, the thyroid nodules), palpate the thyroid (the smooth, firm, symmetric enlargement of Graves disease; the nodular, asymmetric enlargement of the multinodular goitre; the tender, enlarged thyroid of the subacute or de Quervain thyroiditis; the hard, irregular, fixed thyroid of the anaplastic carcinoma), listen for a bruit (the increased vascularity of Graves disease), and examine for the eye signs of Graves orbitopathy (the exophthalmos — the proptosis measured with the Hertel exophthalmometer; the lid retraction — the sclera visible above the iris; the lid lag — von Graefe sign, the lag of the upper lid on downward gaze; the ophthalmoplegia — the diplopia from the involvement of the extraocular muscles). Cross-link to the thyroid examination topic for the full Graves orbitopathy assessment. [1]
The general medical examination for systemic causes
The systemic examination for the causes of a pounding heart includes the hands (the nail-bed pallor of anaemia, the palmar erythema, the thyroid acropachy of Graves disease, the fine tremor of thyrotoxicosis — the outstretched hands, the fine rapid tremor), the face (the malar flush of the mitral stenosis, the anxious facies of the phaeochromocytoma, the exophthalmos of Graves disease), the eyes (the conjunctival pallor of anaemia, the lid lag, the chemosis and the proptosis of the severe Graves orbitopathy), and the skin (the warm, moist skin of thyrotoxicosis, the cold, dry skin of hypothyroidism — hypothyroidism does not cause palpitations, but over-replacement with thyroxine does). [1]
The investigations — the mandatory and the tiered
The 12-lead ECG — mandatory for every patient
The 12-lead ECG is the mandatory first investigation for every patient with palpitations, no exceptions. Even if the ECG is normal between episodes (as it is in up to half of patients with a documented arrhythmia), it may reveal the substrate for the arrhythmia: the delta wave and the short PR interval of Wolff-Parkinson-White syndrome; the left ventricular hypertrophy with the strain pattern (the lateral T-wave inversions) of hypertensive heart disease or hypertrophic cardiomyopathy; the pathological Q waves of the old myocardial infarction (the substrate for VT); the deep T-wave inversions in the right precordial leads (V1 to V3) of the arrhythmogenic right ventricular cardiomyopathy; the Brugada pattern — the coved-type ST elevation in V1 to V3 with the right bundle branch block pattern; the long QT interval — corrected QT of more than 470 milliseconds in a male or more than 480 milliseconds in a female, with the broad-based T waves of LQT1, the notched T waves of LQT2, or the late-onset T waves of LQT3; the short PR interval without a delta wave — the Lown-Ganong-Levine syndrome or the junctional tachycardia; the epsilon wave — the small deflection at the end of the QRS in the right precordial leads, a marker of the arrhythmogenic right ventricular cardiomyopathy; and the U waves of hypokalaemia (a cause of the torsades de pointes). [1]
The ECG during an episode is diagnostic. The narrow-complex regular tachycardia at 150 to 250 per minute is SVT — AVNRT (the commonest, with the invisible or the pseudo R-prime in V1 from the retrograde P waves) or AVRT (the orthodromic, with the narrow QRS and the retrograde P waves in the ST segment) [1][2]. The broad-complex regular tachycardia is VT until proven otherwise — do not assume SVT with aberrancy in a patient with structural heart disease. The irregularly irregular narrow-complex tachycardia is AF; the irregularly irregular broad-complex tachycardia is AF with conduction down an accessory pathway (pre-excited AF) — a medical emergency, do not give AV nodal blockers [3].
Blood tests
The full blood count excludes anaemia (a cause of the pounding heart and a trigger for the high-output state). The thyroid-stimulating hormone with the free T4 excludes thyrotoxicosis (the silent cause of AF and of the pounding heart). The urea, electrolytes and creatinine exclude the electrolyte disturbances that trigger arrhythmias — the hypokalaemia (the torsades, the digitalis toxicity), the hypomagnesaemia, the hypocalcaemia (the long QT). The magnesium is worth checking separately in the patient with ectopy or a long QT. The glucose excludes the hypoglycaemia (a trigger of the catecholamine surge and the sinus tachycardia). The drug levels — the digoxin level if the patient is on digoxin (the toxicity with the atrial tachycardia with block), the lithium level if the patient is on lithium (the sinus node dysfunction). The cardiac biomarkers (the troponin) are indicated if there is chest pain or if the palpitations are secondary to an acute coronary syndrome; a troponin rise after a tachycardia alone is common and non-specific. [1]
Ambulatory ECG monitoring — the tiered strategy
The ambulatory ECG monitoring is matched to the frequency of the symptoms. The teaching point: a Holter for a patient whose palpitations come every two months is wasted effort — the diagnostic yield is near zero. The strategy is: [1]
- A 24-hour or 48-hour Holter monitor for symptoms that occur daily or near-daily. The Holter records continuously; the patient keeps a symptom diary. The diagnostic yield is highest when the symptoms occur during the recording window [9].
- A patient-activated event monitor (the cardio-memo, the external loop recorder, the patch recorder such as the Zio XT for up to 14 days) for symptoms that occur weekly or every few weeks. The event monitor records only when the patient activates it (the cardio-memo) or continuously but stores a loop that the patient saves (the external loop recorder). The patch recorder (the Zio, the SEERT) records continuously for up to 14 days without the patient activation — the diagnostic yield is high for the infrequent symptoms.
- An implantable loop recorder (the small subcutaneous device, the Medtronic Reveal LINQ, the Abbott Confirm RX) for symptoms that occur monthly or rarer, or for the investigation of unexplained syncope with a suspected arrhythmic cause. The device monitors continuously for up to three years and transmits the recorded events to the cardiac service. The diagnostic yield for the infrequent but potentially dangerous arrhythmias (the pauses, the non-sustained VT, the paroxysmal AF in the cryptogenic stroke) is high over the extended monitoring period [9].
The emerging technologies — the smartwatch with the single-lead ECG (the Apple Watch, the Fitbit), the smartphone-connected handheld ECG (the KardiaMobile) — have a role in the ambulatory capture of the symptomatic arrhythmia, especially for the patient who is adept with the technology. The single-lead tracing is sufficient for the diagnosis of AF and for the recognition of a broad-complex versus a narrow-complex tachycardia, but it is not a substitute for the 12-lead ECG. [1]
The echocardiogram — for the suspected structural heart disease
The transthoracic echocardiogram is indicated when there is a clinical suspicion of structural heart disease: the abnormal physical findings (a murmur, a displaced apex, a right ventricular heave, the signs of heart failure); the abnormal ECG (the left ventricular hypertrophy, the pathological Q waves, the regional wall motion abnormality, the right ventricular abnormalities); the high-risk history (the exertional syncope, the family history of the cardiomyopathy or the sudden cardiac death). The echo assesses the left ventricular size and the systolic function (the ejection fraction — the threshold for the ICD in the ischaemic cardiomyopathy is an EF of 35 per cent or less, and for the non-ischaemic cardiomyopathy it is also 35 per cent or less, both at least 40 days after the myocardial infarction or 90 days after the diagnosis respectively, per the current guidelines), the valve structure and function, the right ventricle (the dilatation and the dysfunction of the ARVC, the pulmonary hypertension), the atria (the left atrial dilatation of the chronic AF), and the pericardium (the effusion, the constriction). [1]
The echo is not indicated for the patient with a normal history (the typical SVT story, the typical ectopic story, the typical pounding-heart-in-a-regular-rhythm story), a normal examination, and a normal ECG — the yield of structural heart disease in this group is very low. [1]
The electrophysiology study
The electrophysiology (EP) study is the invasive investigation that maps the re-entrant circuit or the ectopic focus and can proceed directly to the catheter ablation in the same procedure. The EP study is indicated for the confirmation and the ablation of the SVT (the AVNRT, the AVRT, the atrial tachycardia, the typical atrial flutter), for the induction and the mapping of the VT (especially the idiopathic VT in the structurally normal heart, where the ablation is curative), and for the risk stratification of the WPW syndrome (the measurement of the antegrade effective refractory period of the accessory pathway — the short ERP identifies the patient at risk of sudden death and the candidate for the prophylactic ablation) [1][2][7].
The management — the cause-directed approach

The management is directed by the cause. There is no role for empirical treatment of undifferentiated palpitations — the diagnosis must be established first. [1]
Sinus tachycardia — treat the cause
Sinus tachycardia is a physiological response to a stimulus. The management is to identify and treat the underlying cause — the fever (antipyretics, the antibiotics for the infection), the hypovolaemia (the fluid resuscitation, the blood transfusion for the haemorrhage), the anaemia (the iron studies, the iron replacement, the investigation of the cause), the thyrotoxicosis (the carbimazole or the propylthiouracil, the beta-blocker for the symptom control, the definitive treatment with the radioactive iodine or the surgery), the pain (the analgesia), the anxiety (the assessment and the treatment of the anxiety disorder, the cognitive behavioural therapy, the SSRI if indicated), the drugs (the reduction of the caffeine, the withdrawal of the sympathomimetics, the dose adjustment of the thyroxine). Inappropriate sinus tachycardia (the persistent sinus tachycardia without an identifiable stimulus, in the absence of structural heart disease) is a separate entity requiring specialist evaluation — the ivabradine (the selective inhibitor of the If current in the sinus node) is the targeted therapy [1].
Paroxysmal supraventricular tachycardia — vagal manoeuvres, AV nodal blockers, ablation
The acute termination of the SVT follows the stepwise approach: [1]
- The vagal manoeuvres first. The modified Valsalva manoeuvre (the REVERT trial) is the most effective: the patient blows into a 10 mL syringe to move the plunger to 40 mmHg for 15 seconds in the semi-recumbent position, then the operator immediately repositions the patient supine with the legs passively raised at 45 degrees for 15 seconds. The modified Valsalva terminated the SVT in 43 per cent versus 17 per cent for the standard Valsalva — a number needed to treat of approximately 4 [4]. The carotid sinus massage (the firm circular massage of the carotid bifurcation for 5 to 10 seconds, after auscultating for a bruit to exclude the carotid stenosis) is the alternative, but it is less effective and carries the small risk of the embolic stroke in the patient with the carotid atheroma.
- The intravenous adenosine if the vagal manoeuvres fail. The dose is 6 mg as a rapid intravenous bolus through a large peripheral cannula, followed immediately by a 20 mL saline flush, then 12 mg if no response, then a further 12 mg if still no response. Adenosine causes a transient asystole (often 2 to 5 seconds) and the patient must be warned of the unpleasant sensation — the chest tightness, the breathlessness, the flushing, the sense of doom. Adenosine is contraindicated in the asthmatic (it can precipitate the bronchospasm) and in the patient with the severe aortic stenosis or the hypertrophic cardiomyopathy (the profound hypotension). Adenosine must not be given if the broad-complex tachycardia could be VT — the adenosine may provoke the VF or the haemodynamic collapse in the VT patient [1][6].
- The intravenous verapamil (5 to 10 mg over 2 minutes, repeated after 15 minutes if required) is the alternative for the patient who cannot have the adenosine (the asthmatic, the patient who has declined the adenosine sensation). Verapamil must not be given if the broad-complex tachycardia could be VT — it may precipitate the haemodynamic collapse. Verapamil must not be given immediately after the beta-blocker (the risk of the complete heart block and the asystole from the combined AV nodal blockade).
The long-term management of the recurrent SVT: [1]
- Catheter ablation is the preferred definitive treatment for the symptomatic recurrent SVT — the AVNRT (the ablation of the slow pathway, the success rate over 95 per cent, the risk of the AV block requiring a pacemaker at 1 per cent or less), the AVRT (the ablation of the accessory pathway, the success rate over 95 per cent), the atrial tachycardia, the typical atrial flutter (the cavotricuspid isthmus ablation, the success rate over 90 per cent). The ablation offers the prospect of the cure and the freedom from the long-term medication [2].
- The AV nodal blocking agents (the verapamil, the diltiazem, the beta-blockers, the digoxin) are the alternative for the patient who declines the ablation or who is not a candidate. The agent is chosen for the side-effect profile and the comorbidities.
- The flecainide (the class 1c) is an option for the patient without structural heart disease — the pill-in-the-pocket strategy (the single oral dose of the flecainide at the onset of the episode, suitable for the infrequent, well-tolerated SVT in the patient with the normal heart).
Atrial fibrillation — rate or rhythm control, anticoagulation
The management of AF is a large topic, addressed in the atrial fibrillation management topic. The summary for the palpitations context: [1]
- Rate control (the beta-blocker, the diltiazem, the verapamil, the digoxin — the digoxin for the sedentary patient, the beta-blocker and the rate-limiting calcium channel blocker for the active patient) is the first-line strategy for the older patient with the asymptomatic or the mildly symptomatic AF.
- Rhythm control (the electrical cardioversion, the pharmacological cardioversion with the flecainide or the amiodarone, the catheter ablation of the pulmonary vein triggers) is the strategy for the young patient, the patient with the heart failure with the reduced ejection fraction (the AF is poorly tolerated, the rhythm control with the restoration of the atrial contribution to the filling improves the cardiac output), and the patient with the symptomatic AF despite the adequate rate control.
- Anticoagulation (the CHA2DS2-VASc score for the stroke risk — the score of 2 or more in a male or 3 or more in a female indicates the oral anticoagulation; the HAS-BLED score for the bleeding risk — a high score does not preclude the anticoagulation but prompts the correction of the modifiable bleeding factors). The direct oral anticoagulants (the apixaban, the rivaroxaban, the dabigatran, the edoxaban) are preferred over the warfarin for the non-valvular AF. The warfarin remains the agent for the valvular AF (the mitral stenosis, the mechanical valve) [3].
Ectopic beats — reassurance in the normal heart
The ectopic beats (the atrial and the ventricular) in a structurally normal heart, with a normal ECG and a normal echocardiogram, are benign and the management is the reassurance and the trigger avoidance — the reduction of the caffeine, the alcohol, the stress, the correction of the sleep deprivation, the treatment of the anxiety. The beta-blocker is an option for the highly symptomatic patient with the ectopy that impairs the quality of life, after the reassurance has been offered and the benign prognosis has been explained. The ventricular ectopic burden of more than approximately 10 to 15 per cent of the total beats, in a patient with the structural heart disease or the reduced ejection fraction, warrants the cardiology referral — there is a risk of the ectopy-induced cardiomyopathy, and the ablation of the ectopic focus may improve the ventricular function [9].
Ventricular tachycardia — urgent cardiology referral, ICD
The VT is a medical emergency. The haemodynamically unstable VT (the hypotension, the shock, the cardiac arrest, the altered mental state) requires the immediate synchronised DC cardioversion (the 200 joules biphasic, escalating). The haemodynamically stable VT requires the intravenous amiodarone (the 300 mg over 20 to 60 minutes, then the infusion of 900 mg over 24 hours) or the intravenous procainamide or the intravenous lignocaine (the class 1b for the ischaemic VT), with the synchronised DC cardioversion if the pharmacological conversion fails or the haemodynamics deteriorate. The broad-complex tachycardia of uncertain origin is treated as VT until proven otherwise. [1]
The long-term management after the termination of the VT: the urgent cardiology referral, the investigation for the substrate (the coronary angiogram for the ischaemic heart disease, the cardiac MRI for the cardiomyopathy and the scar, the EP study for the inducibility), and the implantable cardioverter-defibrillator (the ICD) for the secondary prevention of the sudden cardiac death. The patient with the VT and the structural heart disease is the candidate for the ICD [8].
The channelopathies and the cardiomyopathies — specialist evaluation
The long QT syndrome, the Brugada syndrome, the catecholaminergic polymorphic ventricular tachycardia, the hypertrophic cardiomyopathy, and the arrhythmogenic right ventricular cardiomyopathy require the specialist evaluation by the inherited cardiac conditions service — the genetic testing, the family screening, the risk stratification, and the decision on the beta-blockade (the long QT type 1 and type 2 respond to the beta-blocker; the CPVT responds to the beta-blocker and the flecainide), the left cardiac sympathetic denervation (the long QT with the recurrent events despite the beta-blocker), and the ICD (the high-risk patient with the prior cardiac arrest, the recurrent syncope, or the documented polymorphic VT despite the medical therapy) [5].
The DCE long-case presentation
In the DCE long case, the patient with palpitations is a common presentation — the multi-morbid older patient with the AF (the hypertension, the diabetes, the heart failure, the chronic kidney disease, the valvular disease), or the younger patient with the SVT or the inherited arrhythmia syndrome. [1]
The SASPOP opening for a long case with palpitations
"Doctor, my patient is Mrs JM, a 68-year-old retired nurse who presents with a 6-month history of intermittent palpitations, an irregular pulse, and progressive exertional dyspnoea. She has coexisting hypertension, type 2 diabetes, and stage 3 chronic kidney disease. Her problems are: paroxysmal atrial fibrillation with a rapid ventricular response on the ECG; hypertension; type 2 diabetes; stage 3 chronic kidney disease (the eGFR of 45); and a CHA2DS2-VASc score of 4 (the hypertension, the diabetes, the female sex, the age of 65 to 74), indicating the oral anticoagulation." [1]
The integrated management plan
The integrated plan addresses each problem: the AF (the rate control with the beta-blocker, the anticoagulation with the apixaban dose-adjusted for the renal function, the consideration of the rhythm control with the cardioversion or the ablation if the rate control fails or the symptoms persist), the hypertension (the ACE inhibitor or the angiotensin receptor blocker for the renal protection, the calcium channel blocker, the target of 130 over 80 in the diabetic), the diabetes (the SGLT2 inhibitor for the renal and the cardiovascular protection, the metformin, the target HbA1c individualised), the chronic kidney disease (the renoprotective measures, the dose adjustment of the renally cleared drugs, the avoidance of the nephrotoxins — the NSAIDs, the contrast without the prophylaxis), and the lifestyle (the weight management, the alcohol reduction, the sleep apnoea screen — the sleep apnoea is a treatable driver of the AF). [1]
The DCE short-case — the cardiovascular examination with palpitations
The short case may present a patient with a murmur and palpitations (the mitral valve prolapse, the hypertrophic cardiomyopathy, the aortic regurgitation) or a patient with the irregular pulse of the AF and the signs of the underlying cause (the thyroid of the Graves disease, the pallor of the anaemia, the collapsing pulse of the aortic regurgitation). [1]
The presentation template
"I introduced myself to the patient, explained the examination, and obtained consent. On general inspection, the patient is comfortable at rest. The pulse is irregularly irregular at 85 beats per minute, with an apex rate of 95 — the apex-radial deficit is consistent with atrial fibrillation. The blood pressure is 145 over 90. The jugular venous pressure is not elevated. The apex beat is not displaced and is of normal character. The first and second heart sounds are normal, with no added sounds and no murmurs. There is a smooth, firm, non-tender goitre with a soft bruit and no eye signs. The chest is clear. There is no peripheral oedema. [1]
In summary, this patient has atrial fibrillation with an underlying goitre. I would like to take a full history including the weight loss, the heat intolerance, and the bowel pattern, and I would check the full blood count, the thyroid function with the TSH and the free T4 and the thyroid antibodies, the urea and electrolytes, and I would organise an echocardiogram. I would assess the stroke risk with the CHA2DS2-VASc score and the bleeding risk with the HAS-BLED score, and I would initiate the appropriate anticoagulation." [1]
Discussion questions
Q1: "How do you distinguish SVT from sinus tachycardia on the history alone?" [1]
"The two discriminating features are the onset and the offset. The SVT has a sudden onset and a sudden offset — the patient can name the minute the rhythm started and the minute it stopped, and the termination may be preceded by a successful vagal manoeuvre. The sinus tachycardia has a gradual onset and a gradual offset — the rate climbs over minutes in response to the stimulus and falls over minutes as the stimulus resolves. A third feature is the polyuria after the termination — the atrial natriuretic peptide released during the SVT drives a brisk diuresis, and the patient passes large volumes of dilute urine for an hour or two after the rhythm restores. This polyuria is highly suggestive of SVT and is not a feature of sinus tachycardia [2][6]."
Q2: "A 24-year-old man presents with palpitations and the ECG shows a short PR interval with a delta wave. What is the diagnosis, what is the significance, and what is the management?" [1]
"The diagnosis is the Wolff-Parkinson-White syndrome — the accessory pathway (the bundle of Kent) connects the atrium to the ventricle, bypassing the AV node, so the impulse pre-excites the ventricle (the delta wave) and the PR interval is short. The significance is the risk of the sudden cardiac death — if the patient develops atrial fibrillation, the rapid conduction down the accessory pathway can degenerate into the ventricular fibrillation. The risk is determined by the antegrade effective refractory period of the accessory pathway, measured at the electrophysiology study — a short ERP (less than 250 milliseconds) identifies the high-risk patient. The management is the specialist referral to the cardiac electrophysiology service for the risk stratification and the catheter ablation of the accessory pathway, which is curative. The asymptomatic WPW pattern on the ECG is also worth the specialist evaluation, especially in the high-risk occupations (the pilot, the diver, the competitive athlete) [1][7][8]."
Q3: "Why must you not give adenosine, verapamil, or a beta-blocker to a patient with a broad-complex tachycardia that might be VT?" [1]
"Because if the broad-complex tachycardia is the ventricular tachycardia, the AV nodal blocking agent does not terminate the rhythm (the circuit is below the AV node) and may precipitate the haemodynamic collapse — the verapamil is a negative inotrope and a vasodilator, and the patient with the VT is often already haemodynamically compromised. The correct approach is to treat the broad-complex tachycardia as VT until proven otherwise: the synchronised DC cardioversion if unstable, the intravenous amiodarone or the procainamide if stable. The adenosine has a small diagnostic role — if the adenosine transiently terminates the rhythm, the diagnosis is the SVT; if it has no effect, the diagnosis is more likely the VT — but the adenosine must not be given if there is any reasonable possibility of the VT, because the adenosine-induced vasodilatation in the patient with the poor cardiac reserve can precipitate the collapse [6]."
Q4: "A 28-year-old woman presents with a 2-year history of intermittent palpitations, each episode lasting 5 to 15 minutes, with a sudden onset and offset, and a brisk polyuria after the termination. The ECG between episodes is normal. What is the likely diagnosis, what is the best investigation to confirm it, and what is the definitive management?" [1]
"The history is the classic presentation of the paroxysmal supraventricular tachycardia — the sudden onset and offset, the short duration, the polyuria after the termination. The normal ECG between episodes is expected. The best investigation to confirm the diagnosis is the ambulatory ECG monitoring matched to the frequency of the symptoms — a patient-activated event monitor or a 14-day patch recorder, because the episodes are too infrequent for a 24-hour Holter. The definitive management is the catheter ablation — for the AVNRT (the commonest SVT in this age group, with the ablation of the slow pathway and a success rate over 95 per cent) or the AVRT (the ablation of the accessory pathway). The ablation offers the prospect of the cure and the freedom from the long-term medication, and it is the preferred strategy for the symptomatic recurrent SVT in the young woman of the reproductive age who wishes to avoid the medication in the future pregnancies [1][2]."
Q5: "How do you assess the risk of sudden cardiac death in a patient with palpitations?" [1]
"The risk of the sudden cardiac death is determined by the five high-risk features. First, the syncope during the palpitations — the cerebral hypoperfusion from a haemodynamically compromising tachycardia. Second, the exertional symptoms — the palpitations on exercise point to the VT, the channelopathies (the long QT type 1 is triggered by the exercise, the CPVT is triggered by the exercise and the emotion), and the structural disease (the hypertrophic cardiomyopathy). Third, the family history of the sudden cardiac death under the age of 40 — the inherited arrhythmia syndromes (the long QT, the Brugada, the CPVT, the arrhythmogenic right ventricular cardiomyopathy, the hypertrophic cardiomyopathy). Fourth, the structural heart disease — the prior infarction, the cardiomyopathy, the heart failure. Fifth, the abnormal ECG — the long QT, the Brugada pattern, the epsilon wave, the right precordial T-wave inversions, the pathological Q waves, the left ventricular hypertrophy with the strain. Any of these features mandates the urgent cardiology referral, the echocardiogram, the ambulatory monitoring, and the consideration of the EP study and the ICD [5][8]."
Q6: "What is the role of the implantable loop recorder, and when do you use it?" [1]
"The implantable loop recorder is the small subcutaneous device (the size of a paper clip, inserted under local anaesthesia over the left pectoral region) that monitors the cardiac rhythm continuously for up to three years. It is used for the symptoms that are too infrequent for the Holter or the event monitor — the monthly or the rarer palpitations, the unexplained syncope with the suspected arrhythmic cause, and the detection of the silent paroxysmal AF in the cryptogenic stroke (the ESUS — the embolic stroke of the undetermined source, where the detection of the AF changes the management from the antiplatelet to the anticoagulation). The device automatically detects the arrhythmias (the pauses, the bradycardia, the tachycardia, the AF) and transmits the recorded events to the cardiac service. The diagnostic yield for the infrequent but potentially dangerous arrhythmias is high over the extended monitoring period, and the device has transformed the investigation of the difficult palpitations and the unexplained syncope [9]."
Exam traps
The "normal ECG excludes the arrhythmia" trap. A normal ECG between episodes does not exclude an arrhythmia — it is normal in up to half of the patients with a documented arrhythmia. The normal ECG may, however, reveal the substrate (the delta wave, the long QT, the Brugada pattern, the LVH, the old Q waves) even when the rhythm is normal at the time of the recording. The candidate who is reassured by a normal ECG without the ambulatory monitoring has missed the diagnosis. [1]
The "broad-complex tachycardia is SVT with aberrancy" trap. The broad-complex tachycardia is VT until proven otherwise, especially in the patient with the structural heart disease. The AV nodal blockers (the adenosine, the verapamil, the beta-blocker, the digoxin) that terminate the SVT may precipitate the collapse in the VT. The candidate who gives the verapamil to the broad-complex tachycardia has made a dangerous error — treat as VT until proven otherwise. [1]
The "adenosine is safe in the broad-complex tachycardia" trap. Adenosine is contraindicated in the broad-complex tachycardia that could be VT — the adenosine-induced vasodilatation in the patient with the poor cardiac reserve can precipitate the collapse, and the adenosine may provoke the VF in the VT patient. Adenosine is for the narrow-complex regular tachycardia only (and with the defibrillator at the bedside). [1]
The "AV nodal blocker in the pre-excited AF" trap. The patient with the WPW syndrome who develops the AF has the irregularly irregular broad-complex tachycardia (the conduction down the accessory pathway produces the broad QRS, and the variable conduction produces the irregularity). The AV nodal blockers (the verapamil, the adenosine, the beta-blocker, the digoxin) block the AV node preferentially and accelerate the conduction down the accessory pathway, increasing the risk of the VF. The correct management is the synchronised DC cardioversion (if unstable) or the intravenous procainamide or the amiodarone (if stable). The candidate who gives the verapamil to the pre-excited AF has made a life-threatening error. [1]
The "Holter for the infrequent palpitations" trap. A 24-hour Holter for the patient whose palpitations come every two months is wasted effort — the diagnostic yield is near zero. The correct strategy is to match the monitoring to the frequency: the Holter for the daily symptoms, the event monitor or the patch recorder for the weekly symptoms, the implantable loop recorder for the monthly or rarer symptoms. The candidate who orders a Holter for the infrequent palpitations and concludes "no arrhythmia" has not excluded the diagnosis. [1]
The "sinus tachycardia is benign" trap. Sinus tachycardia is a physiological response to a stimulus — but the stimulus may be serious (the sepsis, the pulmonary embolism, the hypovolaemia, the thyrotoxicosis, the phaeochromocytoma). The candidate who labels the sinus tachycardia as anxiety without excluding the systemic causes has missed the diagnosis. The sinus tachycardia at rest, without an identifiable stimulus, is the inappropriate sinus tachycardia — a separate entity requiring the specialist evaluation. [1]
The "benign ectopics" trap. The ectopic beats in a structurally normal heart are benign — but the ectopic beats in the structurally abnormal heart (the reduced ejection fraction, the cardiomyopathy, the ischaemic heart disease) may be the marker of the risk of the sustained VT and the sudden cardiac death. The candidate who reassures the patient with the ectopics and the structural heart disease without the echocardiogram and the cardiology referral has missed the risk. The ventricular ectopic burden of more than approximately 10 to 15 per cent on the Holter warrants the cardiology referral, because of the risk of the ectopy-induced cardiomyopathy. [1]
The "family history does not matter" trap. The family history of the sudden cardiac death under the age of 40 is a red flag for the inherited arrhythmia syndrome (the long QT, the Brugada, the CPVT, the ARVC, the hypertrophic cardiomyopathy). The candidate who does not ask about the family history, or who dismisses the family history without the ECG and the specialist evaluation, has missed the opportunity for the early diagnosis, the family screening, and the prevention of the sudden cardiac death. [1]
Long-case integration and cross-links
In the DCE long case, the palpitations are one of the symptoms in the complex patient. The patient with the AF and the multiple comorbidities (the hypertension, the diabetes, the heart failure, the chronic kidney disease, the valvular disease) is the classic long case — the integrated management plan addresses the AF (the rate or the rhythm control, the anticoagulation with the CHA2DS2-VASc and the HAS-BLED), the comorbidities, the lifestyle, and the patient preferences. The patient with the SVT and the young age, the reproductive considerations, and the preference for the ablation over the long-term medication is the other classic presentation. [1]
Cross-link to the atrial fibrillation management topic for the detailed management of the AF, the rate and the rhythm control, the anticoagulation, and the ablation. Cross-link to the syncope and falls topic for the investigation of the unexplained syncope with the suspected arrhythmic cause. Cross-link to the cardiovascular examination routine topic for the full systematic cardiovascular examination. Cross-link to the chest pain topic for the evaluation of the chest pain that accompanies the palpitations. Cross-link to the sudden cardiac death prevention topic for the inherited arrhythmia syndromes, the cardiomyopathies, and the ICD. [1]
References
- [1]Page RL, Joglar JA, Caldwell MA, Calkins H, Conti JB, Deal BJ, et al. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society J Am Coll Cardiol, 2016.PMID 26409258
- [2]Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomstrom-Lundqvist C, et al. The 2019 ESC Guidelines for the Management of Patients with Supraventricular Tachycardia Eur Heart J, 2019.PMID 31837143
- [3]Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomstrom-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC Eur Heart J, 2021.PMID 32860505
- [4]Appelboam A, Reuben A, Mann C, Davies J, Ewings P, Barton A, et al. Postural modification to the standard Valsalva manoeuvre for emergency treatment of supraventricular tachycardias (REVERT): a randomised controlled trial Lancet, 2015.PMID 26314489
- [5]Abrams DJ Long QT syndrome Circulation, 2014.PMID 24709866
- [6]Link MS Clinical practice. Evaluation and initial treatment of supraventricular tachycardia N Engl J Med, 2012.PMID 23050527
- [7]Cohen MI, Triedman JK, Cannon BC, Davis AM, Drago F, Janousek J, et al. PACES/HRS expert consensus statement on the management of the asymptomatic young patient with a Wolff-Parkinson-White (WPW, ventricular preexcitation) electrocardiographic pattern: developed in partnership between the Pediatric and Congenital Electrophysiology Society (PACES) and the Heart Rhythm Society (HRS). Endorsed by the governing bodies of PACES, HRS, the American College of Cardiology Foundation (ACCF), the American Heart Association (AHA), the American Academy of Pediatrics (AAP), and the Canadian Heart Rhythm Society (CHRS) Heart Rhythm, 2012.PMID 22579340
- [8]Benredisyte R, Riaukaite G, Juceviciene A, Zdanyte M, Zilinskas K, Semetaite S, et al. Sudden Cardiac Death: The Most Feared but Potentially Preventable Presentation of Wolff-Parkinson-White Syndrome Case Rep Cardiol, 2021.PMID 34840830
- [9]Majeed MW, Khan A, Aasim M, Ullah W, Sattar Y Ambulatory ECG Monitoring 2026.PMID 37983350
- [10]Nery PB, Belliveau D, Nair GM, et al. Relationship Between Pulmonary Vein Reconnection and Atrial Fibrillation Recurrence: A Systematic Review and Meta-Analysis JACC Clin Electrophysiol, 2016.PMID 29759868