Phys · general-medicine
Undifferentiated Weight Loss — A Systematic Diagnostic Approach
Also known as involuntary weight loss · unintentional weight loss · weight loss of unknown cause · cachexia · cancer cachexia · malnutrition · sarxopenia · failure to thrive · anorexia of ageing
Consultant-physician-depth guide to the diagnostic approach to the patient with involuntary weight loss of unknown cause. Covers the definition of clinically significant loss (greater than 5 per cent of body weight in 6 months), the two first-minute branch points (intentional versus involuntary; appetite preserved versus lost), the seven-category differential (malignancy — GI, lung, haematological, prostate, ovarian; endocrine — hyperthyroidism, new-onset type 1 diabetes, adrenal insufficiency; GI — coeliac, chronic pancreatitis, IBD, SIBO, dysphagia, obstruction; chronic infection — TB, HIV, endocarditis, osteomyelitis; psychiatric — depression, anorexia nervosa, dementia; drugs — metformin, SGLT2i, topiramate, levothyroxine excess, chemotherapy; social), the two-tier investigation strategy (Tier 1 bloods plus CXR and ultrasound, Tier 2 CT CAP and endoscopy), the Hernandez prediction score for malignancy, the Metalidis evidence supporting observation after a normal workup, the Fearon cancer cachexia consensus, the nutritional assessment (MUST, MNA) and the management ladder (oral supplements, enteral, parenteral), the refeeding syndrome, and the exam traps that cost marks.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags

Undifferentiated Weight Loss — A Systematic Diagnostic Approach
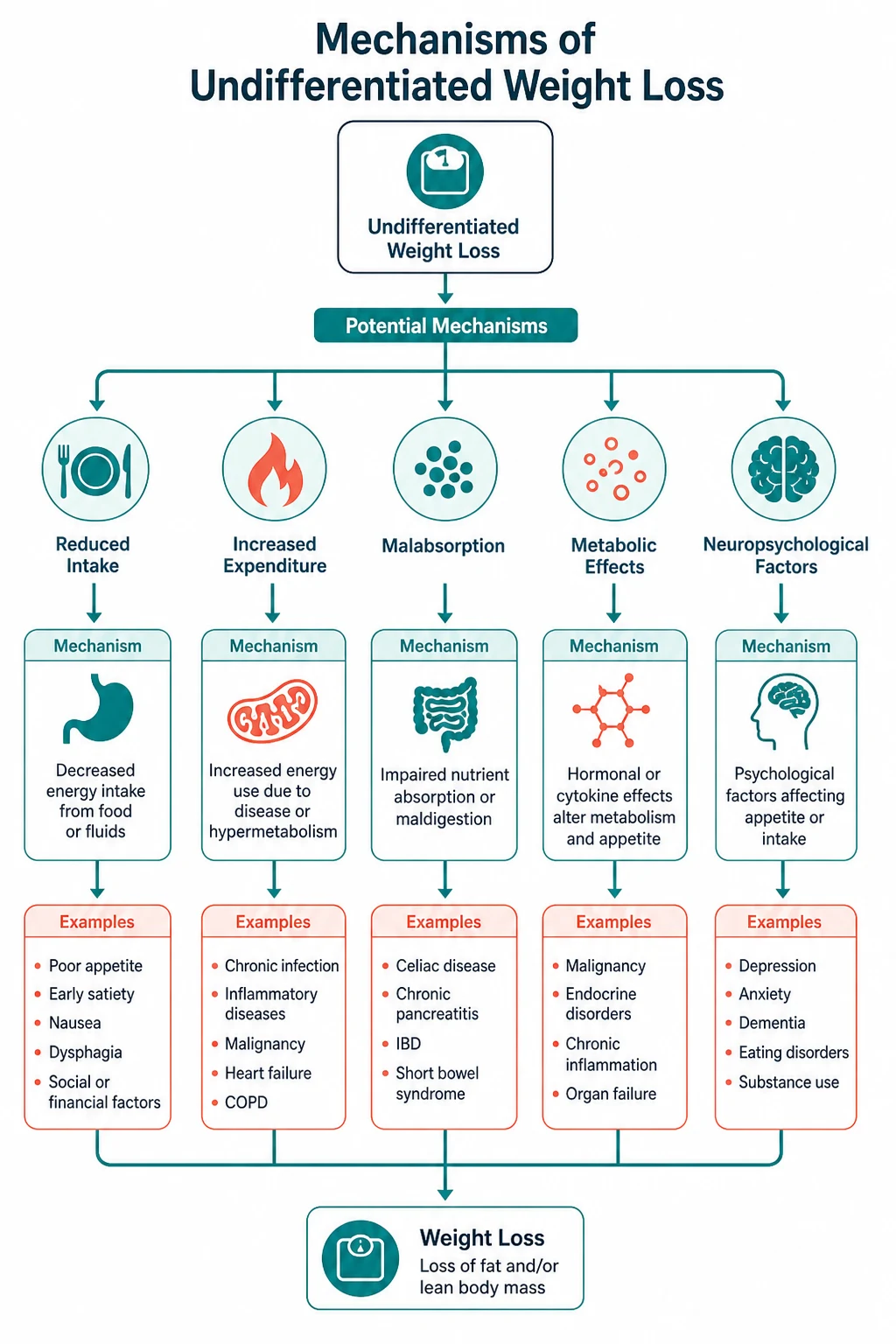
The patient who presents with involuntary weight loss is one of the commonest and most cognitively demanding presentations in internal medicine. The weight loss is a non-specific symptom that may arise from a malignancy, an endocrine cause, a GI malabsorption, a chronic infection, a psychiatric condition, a drug, or a social factor — and the registrar's job is to use the history (the appetite, the rate, the associated symptoms), the examination (the cachexia, the pallor, the organomegaly, the lymphadenopathy), and the first-tier investigations to narrow the differential before committing to a working diagnosis. [1]
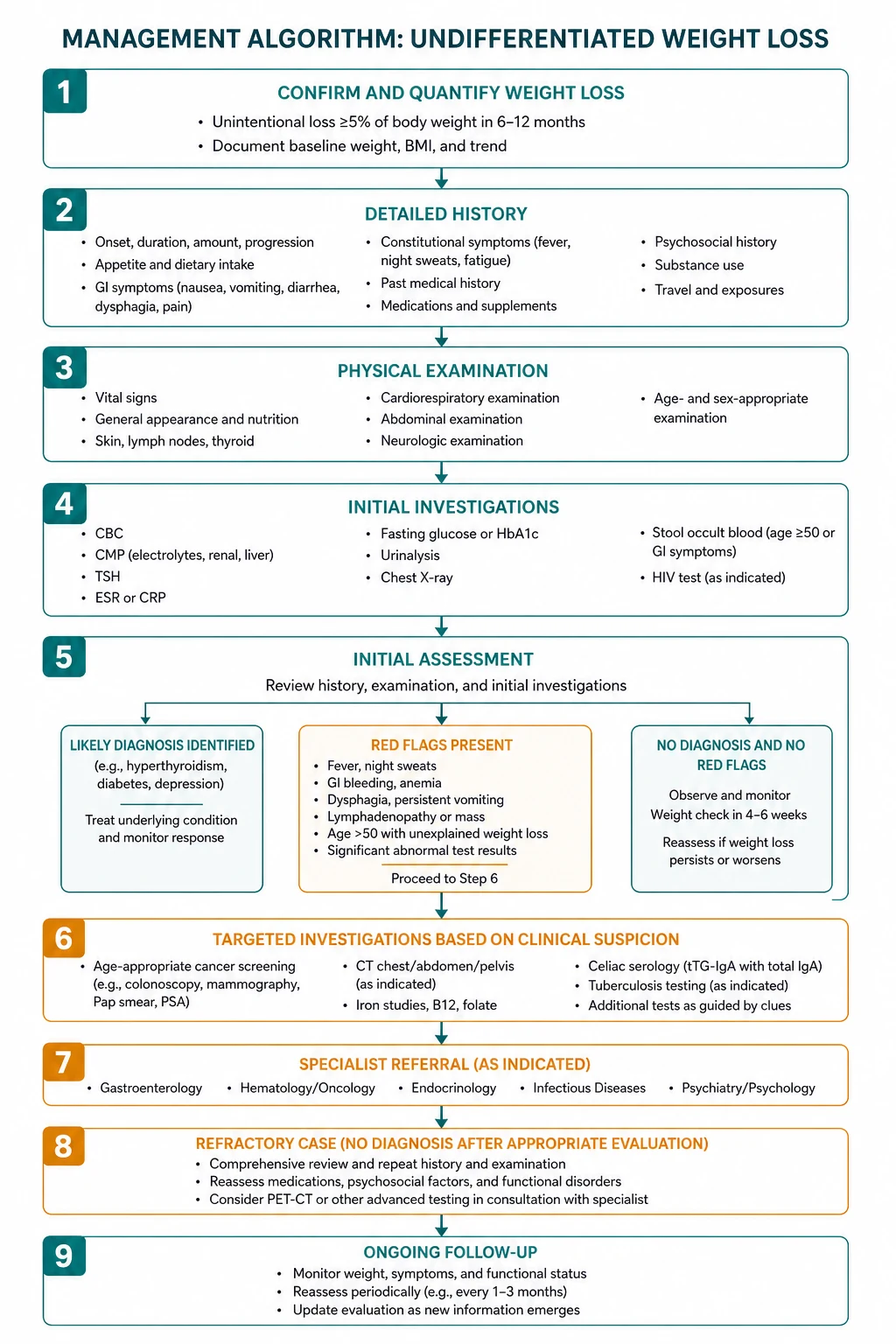
The reproducible sequence for any patient with involuntary weight loss is: [1]
- Confirm the weight loss is real and significant — the threshold for the clinically significant loss is greater than 5 per cent of the usual body weight within 6 months (or greater than 10 per cent within 6 months). The patient self-report is unreliable; the objective documentation from the prior records, the clinic weights, or the clothing size change is essential.
- Ask the two first-minute questions — is the loss intentional or involuntary? Is the appetite preserved (or increased) or lost? The first excludes the dieter and the bariatric surgery patient. The second is the single most powerful discriminator: the weight loss with the preserved appetite points to the hypermetabolic or malabsorptive causes; the weight loss with the anorexia points to the malignancy, the chronic infection, the depression, or the GI obstruction.
- Take a focused history — the amount and the rate, the appetite, the dysphagia and the early satiety, the change in the bowel habit, the thirst and the polyuria, the heat intolerance and the palpitations, the fever and the night sweats, the mood, the functional state (the ADLs, the shopping, the cooking), the drug history (the metformin, the SGLT2 inhibitor, the levothyroxine, the chemotherapy), and the social history.
- Examine systematically — the BMI and the cachexia, the muscle wasting, the pallor, the lymph nodes, the thyroid, the abdominal organomegaly and masses, the PR examination, the skin pigmentation, and the clubbing.
- Order the Tier 1 investigations — the FBC, the U and E, the LFTs including the ALP and the albumin, the TFTs, the glucose and the HbA1c, the CRP, the iron studies, the B12 and the folate, the calcium, the CXR, the urinalysis, the faecal immunochemical test, and the abdominal ultrasound.
- Apply the discriminators — the TSH for the hyperthyroidism, the glucose for the diabetes, the electrolytes for the Addison disease, the FBC and the film for the haematological malignancy, the LFTs and the ALP for the hepatic and the biliary disease, the CXR for the lung and the TB, the faecal immunochemical test and the iron studies for the GI malignancy.
- Proceed to the Tier 2 investigations if the Tier 1 is non-diagnostic — the CT chest abdomen and pelvis for the occult malignancy, the upper GI endoscopy and the colonoscopy (especially in the patient above 50), the coeliac serology, the serum and the urine electrophoresis, and the autoimmune screen.
- Apply the Metalidis rule — if the Tier 1 workup is completely normal, the probability of the malignancy at one year is below 1 per cent, and the 3 to 6 month observation with the repeat weight and the reassessment for the new symptoms is the appropriate strategy. [1]
The single most dangerous error is the investigation without the history. The registrar who orders the CT chest abdomen and pelvis for every patient with the weight loss has substituted the technology for the clinical reasoning. The patient with the weight loss and the preserved appetite needs the TSH and the glucose and the coeliac serology — the CT may be normal. The patient with the weight loss and the hyperpigmentation needs the cortisol and the ACTH — the endoscopy is a distraction. The clinical reasoning directs the investigation, not the reverse. [1]
Viva trap: "What is the single most useful question in the first minute with a patient who has lost weight?" The honest answer is the appetite. "Have you lost your appetite, or are you eating normally or more than usual?" The answer redirects the entire workup. The patient who has lost weight despite eating more has a hypermetabolic or malabsorptive cause; the patient who has lost weight because they cannot eat has an obstructive, an infective, or a psychiatric cause. [1]
The definition of clinically significant weight loss
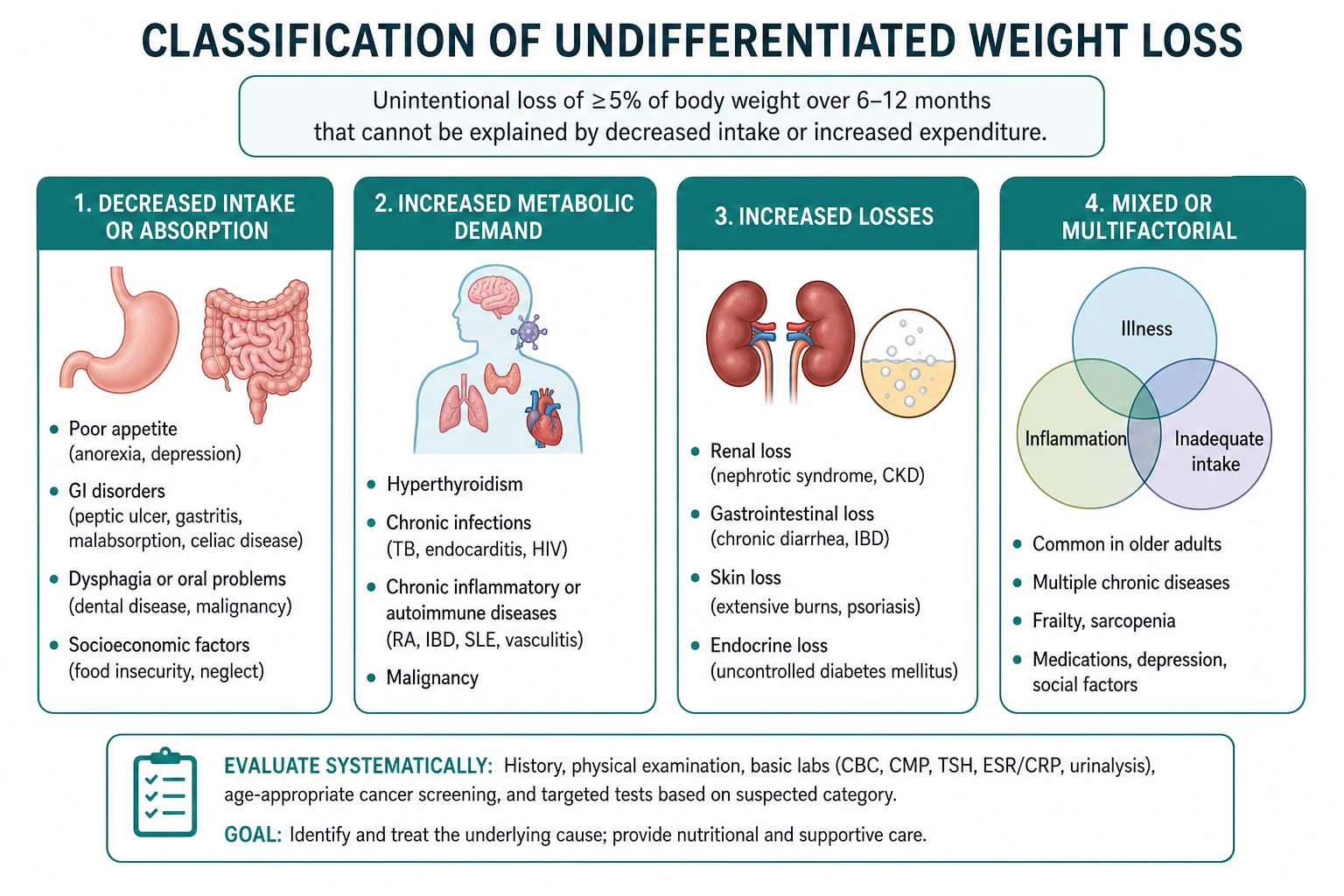
The weight loss is a symptom reported by the patient, but not all reported weight loss is clinically significant. The threshold that mandates the investigation is the loss of greater than 5 per cent of the usual body weight within 6 months (or greater than 10 per cent within 6 months). This threshold is derived from the cohort studies that showed the association between the involuntary loss and the increased morbidity and mortality. [1]
The Wallace 1995 study of 4714 community-dwelling older adults established the clinical significance of the involuntary weight loss: a loss of greater than 4 per cent of the body weight in one year was associated with a doubled mortality risk (the relative risk of death 2.1 in men and 1.6 in women) and an increased rate of the nursing home admission, even after the adjustment for the comorbidities and the baseline BMI [6]. This study is the foundation of the modern threshold and is the reference the examiner expects.
The objective documentation is essential because the patient self-report is unreliable. The comparison with the prior recorded weights (the GP record, the clinic weights, the hospital admission weights), the clothing size change, and the reported fit of the dentures or the rings all help. The registrar who investigates a subjective loss without the confirmation may subject the patient to the unnecessary testing. [1]
The intentional versus the involuntary
The first branch point is whether the weight loss was intentional. The patient who has dieted, exercised, or undergone the bariatric surgery has the intentional loss, and the malignancy workup is not indicated unless there are the red flags. The patient who has lost weight without trying has the involuntary loss, and the investigation is mandatory. The single question — "Were you trying to lose weight?" — makes the distinction in the first minute. [1]
The two first-minute branch points

The two questions that organise the entire encounter are: [1]
Question one — intentional or involuntary? The dieter, the exerciser, and the bariatric surgery patient have the intentional loss. Everyone else has the involuntary loss and the investigation is indicated. [1]
Question two — appetite preserved or lost? This is the single most powerful discriminator in the history. [1]
- The weight loss with the preserved or the increased appetite points to the hypermetabolic states (the hyperthyroidism, the uncontrolled type 1 diabetes), the malabsorption (the coeliac disease, the chronic pancreatitis, the inflammatory bowel disease, the small intestinal bacterial overgrowth), and the chronic infection (the HIV, the TB). The patient is eating normally or more, but the body is either burning the calories too fast (the hypermetabolic) or not absorbing them (the malabsorption).
- The weight loss with the anorexia (the reduced appetite) points to the malignancy, the chronic infection, the depression, the dementia, the GI obstruction, and the drugs. The patient is eating less, and the weight loss reflects the reduced intake. [1]
The registrar who does not ask about the appetite in the first minute has missed a discriminator that redirects the entire workup. The patient with the weight loss and the preserved appetite needs the TSH and the glucose and the coeliac serology; the patient with the weight loss and the anorexia needs the malignancy workup and the depression screen. [1]
The seven-category differential
The differential of the involuntary weight loss is organised by the system and the mechanism, and the registrar works through the seven categories in turn: the malignancy, the endocrine, the GI, the chronic infection, the psychiatric, the drugs, and the social. [1]
The malignancy
The malignancy is found in 16 to 36 per cent of the cases presenting with the involuntary weight loss, and it is the diagnosis that the patient and the examiner fear most. The solid tumours are the GI malignancies (the oesophageal, the gastric, the pancreatic, the colorectal, the hepatocellular), the lung cancer (especially the small cell and the squamous cell), and the prostate and the ovarian. The haematological malignancies are the lymphoma (both the Hodgkin and the non-Hodgkin), the leukaemia, and the multiple myeloma. [1]
The weight loss in the malignancy is driven by two mechanisms. First, the reduced intake — the anorexia from the tumour cytokines (the tumour necrosis factor alpha, the interleukin 1 and 6), the dysphagia, the early satiety, the pain, and the nausea. Second, the cancer cachexia — the cytokine-mediated syndrome of the skeletal muscle wasting (with or without the fat loss) that cannot be fully reversed by the conventional nutritional support. The Fearon 2011 international consensus defined the cancer cachexia as the weight loss greater than 5 per cent, or greater than 2 per cent in the patient with the BMI below 20 or the sarcopenia [5]. The cachexia differs from the starvation because it preferentially depletes the lean body mass (through the activation of the ubiquitin-proteasome pathway) and it is driven by the inflammatory cytokine cascade, not by the calorie deficit alone.
The endocrine causes
The endocrine causes are the high-yield group because they are common, treatable, and frequently missed. [1]
- The hyperthyroidism — the weight loss with the preserved or the increased appetite, the heat intolerance, the palpitations, the tremor, the anxiety, the sweating, and the increased bowel frequency. The mechanism is the excess T3 that upregulates the basal metabolic rate. The apathetic hyperthyroidism in the older adult presents with the weight loss, the atrial fibrillation, and the depression — without the classic hyperadrenergic features, and is the commonly missed presentation. Always check the TSH in any involuntary weight loss.
- The new-onset type 1 diabetes — the weight loss with the polyuria, the polydipsia, the nocturia, and the polyphagia. The mechanism is the insulin deficiency that drives the catabolism and the osmotic diuresis. The weight loss can be rapid (over weeks) and the presentation may be the diabetic ketoacidosis. Check the glucose and the ketones urgently.
- The Addison disease (the primary adrenal insufficiency) — the weight loss with the fatigue, the anorexia, the nausea, the postural dizziness, the salt craving, and the characteristic hyperpigmentation of the palmar creases, the buccal mucosa, and the recent scars. The electrolyte pattern is the hyponatraemia and the hyperkalaemia, but it may be normal in the early disease. The undiagnosed Addisonian crisis is fatal. Check the 9 am cortisol, the ACTH, and the synacthen stimulation test in any patient with the clinical suspicion. [1]
The GI causes
The GI causes are the malabsorption, the dysphagia, and the obstruction. [1]
- The coeliac disease — the weight loss with the diarrhoea, the steatorrhoea, the iron deficiency anaemia (the commonest presentation in the adult), the osteoporosis, and the dermatitis herpetiformis. The tTG-IgA is the preferred screening test (check the total IgA simultaneously to exclude the IgA deficiency). The duodenal biopsy confirms.
- The chronic pancreatitis — the weight loss with the chronic epigastric pain radiating to the back, the steatorrhoea (the foul-smelling, oily stools), and the diabetes from the endocrine failure. The history of the alcohol or the gallstones. The faecal elastase is low.
- The inflammatory bowel disease — the weight loss with the diarrhoea, the abdominal pain, the rectal bleeding, and the extraintestinal manifestations (the erythema nodosum, the pyoderma gangrenosum, the axial arthropathy, the primary sclerosing cholangitis). The faecal calprotectin and the colonoscopy with the biopsy.
- The small intestinal bacterial overgrowth — the weight loss with the diarrhoea, the bloating, and the secondary B12 deficiency. The risk factors are the structural abnormality (the blind loop, the fistula, the prior surgery), the motility disorder (the scleroderma, the diabetic autonomic neuropathy), and the immunodeficiency. The hydrogen breath test and the empiric antibiotic trial (the rifaximin).
- The dysphagia and the obstruction — the oesophageal stricture or the malignancy, the gastric outlet obstruction, and the colorectal obstruction cause the weight loss by the mechanical reduction of the intake. [1]
The chronic infection
The chronic infections cause the weight loss through the cytokine-mediated anorexia and the increased metabolic rate from the fever. [1]
- The tuberculosis — the weight loss with the chronic cough, the night sweats, the haemoptysis, and the risk factors (the birth in the endemic country, the household contact, the immunosuppression, the silicosis). The CXR and the sputum for the acid-fast bacilli.
- The HIV — the weight loss with the opportunistic infections, the chronic diarrhoea, the oral candidiasis, and the risk factors. The HIV serology if the risk factors are present.
- The infective endocarditis, the osteomyelitis, and the occult abscess — the weight loss with the fever, the night sweates, the new murmur, and the raised inflammatory markers. The blood cultures, the echocardiogram, and the imaging. [1]
The psychiatric causes
The psychiatric causes are common and frequently missed because the somatic symptoms are attributed to the medical disease. [1]
- The depression — the commonest non-organic cause of the weight loss. The reduced appetite, the anhedonia, the low mood, the early-morning waking, and the fatigue. Screen every patient.
- The anorexia nervosa — the weight loss with the distorted body image, the fear of the weight gain, the amenorrhoea, and the Russell sign. The patient denies the problem, unlike the patient with the organic disease.
- The dementia — the weight loss from the loss of the ability to shop, to cook, and to self-feed (the apraxia of the eating, the forgetting of the meals, and the dysphagia in the later stage). The cognitive assessment and the collateral history.
- The substance use — the alcohol, the stimulants, and the opioids suppress the appetite and alter the metabolism. [1]
The drugs
The drugs are the commonly overlooked cause, and the medication review is the essential part of the workup. [1]
- The metformin — the weight loss through the reduced hepatic gluconeogenesis, the increased insulin sensitivity, and the GI side effects (the nausea, the diarrhoea, the metallic taste).
- The SGLT2 inhibitors (the dapagliflozin, the empagliflozin) — the caloric loss through the glucosuria (approximately 200 to 300 kcal per day).
- The topiramate — the appetite suppression and the taste alteration.
- The levothyroxine in the excess dose — the iatrogenic hyperthyroidism. Check the TSH.
- The chemotherapy — the nausea, the mucositis, and the direct catabolic effect.
- The digoxin at the toxic dose — the anorexia and the nausea. [1]
The social and the economic
The social factors are the common and the correctable cause in the older adult and the socially isolated patient. [1]
- The poverty and the food insecurity — the inability to afford the adequate food.
- The isolation — the loss of the motivation to cook and to eat in the bereaved or the socially isolated patient.
- The inability to cook or to shop — the functional limitation from the arthritis, the visual impairment, the frailty, or the transport difficulty.
- The dental problems — the ill-fitting dentures, the dental decay, and the periodontal disease that reduce the intake.
- The elder abuse — the neglect, the financial abuse, and the psychological abuse. [1]
The history
The history is the single most informative part of the weight loss workup, and the structured approach covers: [1]
- The amount and the rate — how much weight, over how long, objectively documented from the records. The greater than 5 per cent in 6 months is the significant loss. The rapid loss (over weeks) has a higher probability of the malignancy, the hyperthyroidism, or the type 1 diabetes.
- The appetite — the preserved or the increased appetite points to the hypermetabolic or malabsorptive; the reduced appetite points to the malignancy, the infection, the depression, or the obstruction. This is the single most important discriminator.
- The GI symptoms — the dysphagia, the odynophagia, the early satiety, the abdominal pain, the change in the bowel habit, the rectal bleeding, the steatorrhoea, and the nausea. Each symptom redirects the workup (the dysphagia to the endoscopy, the steatorrhoea to the malabsorption).
- The endocrine symptoms — the thirst and the polyuria (the diabetes), the heat intolerance and the palpitations (the hyperthyroidism), the cold intolerance and the fatigue (the hypothyroidism, the Addison disease), the postural dizziness (the Addison disease).
- The systemic symptoms — the fever, the night sweats, and the pruritus (the malignancy, the lymphoma, the chronic infection, the TB). The fatigue and the functional decline.
- The mood — the low mood, the anhedonia, the sleep disturbance, and the loss of interest. Screen for the depression with the PHQ-2 or the direct question.
- The functional and the social history — the activities of the daily living (the shopping, the cooking, the cleaning), the living situation (the alone, the supported, the residential care), the finances, and the transport. The social causes are the common and the correctable contributors.
- The drug history — the metformin, the SGLT2 inhibitors, the topiramate, the levothyroxine, the chemotherapy, and the over-the-counter and the recreational drugs. The dose and the recent changes. [1]
The examination
The examination is systematic and covers the whole body: [1]
- The general inspection — the cachexia (the temporal wasting, the hollow cheeks, the prominent bones), the pallor (the anaemia), the muscle wasting (the proximal myopathy of the hyperthyroidism), and the agility.
- The hands — the clubbing (the malignancy, the IBD, the cirrhosis), the koilonychia (the iron deficiency), the palmar erythema (the chronic liver disease), the pulse (the atrial fibrillation of the hyperthyroidism), and the tremor (the fine rapid tremor of the hyperthyroidism).
- The mouth and the neck — the oral candidiasis (the immunosuppression, the HIV), the angular cheilitis (the iron or the B12 deficiency), the glossitis (the B12 or the folate deficiency), the dental decay and the dentures, the goitre (the hyperthyroidism), and the lymphadenopathy (the Virchow node of the gastric cancer, the cervical and the supraclavicular nodes of the lung cancer and the lymphoma).
- The chest — the crackles (the heart failure, the malignancy), the wheeze (the COPD, the asthma), the consolidation (the pneumonia), and the apical signs (the TB).
- The abdomen — the cachexia (the scaphoid abdomen), the hepatomegaly (the metastases, the cirrhosis), the splenomegaly (the lymphoma, the portal hypertension), the palpable mass (the gastric, the colonic, the pancreatic, the ovarian), the ascites (the ovarian cancer, the peritoneal carcinomatosis), and the PR examination (the rectal mass, the prostate, the melaena).
- The skin — the hyperpigmentation of the Addison disease, the dermatitis herpetiformis of the coeliac disease, the striae and the thin skin of the Cushing syndrome, and the track marks of the substance use.
- The breast and the pelvic examination — in the woman with the unexplained weight loss, the breast examination (the breast cancer) and the pelvic examination (the ovarian cancer) are part of the complete assessment.
- The functional and the cognitive assessment — the gait, the balance, the grip strength, the ADLs, the MMSE or the MoCA, and the depression screen. [1]
The Tier 1 investigations

The Tier 1 panel is the set of investigations that every patient with the significant involuntary weight loss should have: [1]
- The full blood count — the anaemia (the iron deficiency of the GI malignancy and the coeliac disease, the normocytic anaemia of the chronic disease), the leukaemia, the leukocytosis (the infection, the inflammation), and the lymphocytosis (the CLL, the lymphoma).
- The urea and electrolytes — the hyponatraemia and the hyperkalaemia of the Addison disease, the renal failure of the multiple myeloma and the systemic disease.
- The liver function tests — the metastatic disease, the chronic liver disease, the alcohol, and the infiltrative disease. The ALP and the LDH are part of the Hernandez malignancy prediction score.
- The albumin — the nutritional state and the chronic disease (a late and non-specific marker).
- The calcium — the hypercalcaemia of the malignancy (the myeloma, the bone metastases, the paraneoplastic) and the malabsorption.
- The glucose and the HbA1c — the diabetes (especially the new-onset type 1).
- The thyroid function tests — the hyperthyroidism (the suppressed TSH, the raised free T4) and the hypothyroidism. Always check the TSH.
- The C-reactive protein — the malignancy, the chronic infection, and the inflammation. The CRP is the non-specific marker of the organic cause.
- The iron studies, the ferritin — the iron deficiency anaemia of the GI malignancy and the coeliac disease.
- The vitamin B12 and the folate — the malabsorption and the nutritional deficiency.
- The chest X-ray — the lung cancer, the TB, the lymphoma, the heart failure, and the metastases.
- The urinalysis — the glycosuria (the diabetes), the proteinuria (the myeloma, the diabetic nephropathy).
- The faecal immunochemical test (FIT) — the GI malignancy, especially in the patient above 50.
- The HIV serology — if the risk factors are present.
- The abdominal ultrasound — the liver metastases, the pancreatic mass, the hepatocellular carcinoma, the ovarian mass, and the lymphadenopathy.
- The depression screen — the PHQ-2 or the GDS-15. [1]
The Hernandez prediction score
The Hernandez 2003 study of 306 patients with the involuntary weight loss without the specific symptoms derived the clinical prediction score for the malignancy [2] [3]. The five variables are:
- An elevated alkaline phosphatase.
- An elevated lactate dehydrogenase (LDH).
- A low albumin (below 40 g per litre).
- An elevated white blood cell count.
- An age above 80 years. [1]
The presence of two or more variables significantly increases the probability of the malignancy and should prompt the Tier 2 imaging (the CT chest abdomen and pelvis) and the endoscopic evaluation. The score has been validated in some but not all the subsequent studies — the Baicus 2014 PLoS One study did not confirm the score [8] — but it remains a useful framework for the malignancy risk assessment.
The Tier 2 investigations
The Tier 2 investigations are indicated when the Tier 1 panel is abnormal and a cause is suspected, or when the Tier 1 is normal but the weight loss persists or the patient has the red flags. [1]
- The CT chest, abdomen, and pelvis — the single most informative investigation for the occult malignancy. It identifies the pancreatic cancer, the lung cancer, the lymphoma, the renal cell carcinoma, the ovarian cancer, the metastatic disease, and the primary tumour.
- The upper GI endoscopy and the colonoscopy — indicated in the patient above 50, in the patient with the GI symptoms, and in the patient with the iron deficiency anaemia. The duodenal biopsy during the upper GI endoscopy screens for the coeliac disease. The bidirectional endoscopy identifies the oesophageal, the gastric, and the colorectal malignancies.
- The coeliac serology — the tTG-IgA and the total IgA. The positive tTG-Iga requires the duodenal biopsy confirmation (the villous atrophy, the crypt hyperplasia, the intraepithelial lymphocytosis — the Marsh classification).
- The serum and the urine electrophoresis — the serum paraprotein and the Bence Jones protein of the multiple myeloma. The serum free light chains are the more sensitive test.
- The autoimmune screen — the ANA, the dsDNA, and the extractable nuclear antigens for the connective tissue disease.
- The faecal calprotectin — the inflammatory bowel disease.
- The faecal elastase — the chronic pancreatitis and the exocrine pancreatic insufficiency. [1]
The Metalidis rule — the observation after the normal workup
The Metalidis 2008 prospective study of 101 patients with the involuntary weight loss showed that a completely normal baseline evaluation (the history, the examination, the FBC, the biochemistry, the inflammatory markers, the CXR, the abdominal ultrasound, and the urinalysis) had a 99 per cent negative predictive value for the malignancy at the one-year follow-up [4]. The recommendation is the 3 to 6 month observation with the repeat weight measurement and the re-evaluation if the new symptoms develop. The undirected invasive testing in this setting (the PET scan, the repeated endoscopy, the exploratory laparotomy) has a low yield and a significant complication rate.
DWE high-yield: The most testable fact about the workup of the unexplained weight loss is the Metalidis evidence: a completely normal Tier 1 workup has a 99 per cent negative predictive value for the malignancy at one year, and the 3 to 6 month observation is the appropriate strategy. The registrar who orders the PET scan after the normal CT and the normal endoscopy has not understood the evidence. [1]
The nutritional assessment and the management

The management of the involuntary weight loss is the treatment of the underlying cause — the weight loss is a symptom, not a diagnosis, and the nutritional support is a bridge to the definitive treatment. [1]
The nutritional assessment
The nutritional state is assessed with: [1]
- The MUST (the Malnutrition Universal Screening Tool) or the MNA (the Mini Nutritional Assessment for the older adult) — the validated screening tools.
- The BMI — below 18.5 is the underweight, below 20 in the older adult is the concern.
- The weight change — the greater than 5 per cent in 3 months is the significant loss.
- The mid-upper arm circumference and the grip strength — the functional markers of the nutritional state.
- The biochemistry — the low albumin (a late and non-specific marker), the low prealbumin (a more sensitive marker of the acute state). [1]
The management ladder
The nutritional support follows the ladder: [1]
- The oral nutritional supplementation — the high-calorie, high-protein supplements (for example Fortisip 200 mL providing 300 kcal and 12 to 18 g of protein, 2 to 3 bottles per day), the food fortification (the cream, the butter, the cheese added to the normal meals), the small frequent energy-dense meals, and the dietitian referral.
- The enteral feeding — the nasogastric tube for the short-term, the PEG (the percutaneous endoscopic gastrostomy) for the long-term (more than 2 to 3 weeks). Indicated for the dysphagia (the motor neuron disease, the oesophageal stricture, the head and neck cancer) and the inadequate oral intake despite the supplementation.
- The parenteral nutrition — reserved for the severe malabsorption (the short bowel syndrome, the severe Crohn disease with the intestinal failure), the intestinal obstruction, and the prolonged nil-by-mouth status after the major GI surgery. Never the first-line because of the line-sepsis, the metabolic, and the hepatobiliary risks. [1]
The appetite stimulants
The appetite stimulants (the megestrol acetate, the dexamethasone) are reserved for the palliative phase and the short-term use. They increase the appetite and produce the modest weight gain (predominantly the fat and the fluid) but do NOT improve the survival, the lean body mass, or the functional outcome, and they carry the significant risks (the thromboembolism, the immunosuppression, the adrenal suppression, the myopathy). The Gaddey and Holder 2014 review is explicit: the appetite stimulants are not recommended for the non-palliative weight loss [1].
The refeeding syndrome
The refeeding syndrome is the potentially fatal complication of the rapid re-nutrition in the chronically malnourished patient. The insulin surge from the carbohydrate load drives the intracellular shift of the phosphate, the potassium, and the magnesium, producing the hypophosphataemia, the hypokalaemia, the hypomagnaesaemia, the fluid retention, the cardiac arrhythmia, the heart failure, the respiratory failure, and the death. [1]
The high-risk patient is the one with: [1]
- A BMI below 16.
- An unintentional weight loss greater than 15 per cent in the preceding 3 to 6 months.
- A minimal intake for more than 10 days.
- The low baseline potassium, phosphate, or magnesium.
- The alcohol use disorder. [1]
The prevention is the slow refeeding (5 to 10 kcal per kg per day, increasing over 4 to 7 days), the thiamine (200 to 300 mg orally daily, or 100 mg intravenously daily, for the first 7 to 10 days, given before the first feed), and the close electrolyte monitoring (the phosphate, the potassium, and the magnesium daily for the first week, with the supplementation as needed). The NICE refeeding guideline is the reference. [1]
The cancer cachexia
The cancer cachexia is the cytokine-mediated syndrome of the skeletal muscle wasting that cannot be fully reversed by the conventional nutritional support. The Fearon 2011 international consensus framework classifies the cachexia into: [1]
- The precachexia — the early stage with the anorexia and the altered metabolism, but without the significant weight loss.
- The cachexia — the weight loss greater than 5 per cent, or greater than 2 per cent with the BMI below 20 or the sarcopenia.
- The refractory cachexia — the advanced stage with the ongoing weight loss, the poor performance status, and the short life expectancy, where the cancer is no longer responsive to the treatment. [1]
The management is the treatment of the underlying cancer, the nutritional support to the extent that it improves the quality without the burden, the symptom control (the antiemetics, the analgesics, the laxatives), the corticosteroid or the progestogen in the palliative phase, and the palliative care approach. The forced feeding in the refractory cachexia causes the distress (the nausea, the bloating) without the reversal of the wasting. [1]
The special situations
The older adult
In the older adult (above 65), the comprehensive geriatric assessment is the framework. The commonest causes shift toward the malignancy, the depression, the dementia, the medication side effects, the chronic disease, and the social factors. The polypharmacy review (the metformin, the digoxin, the levothyroxine excess, the cholinesterase inhibitors), the elder abuse screen, the dental and the swallow assessment, and the functional and the social support are the essential components. The goal is the cause identification, the nutritional optimisation, and the preservation of the function and the independence [1] [7].
The patient with the weight loss and the normal Tier 1 workup
The Metalidis evidence supports the 3 to 6 month observation with the repeat weight and the reassessment for the new symptoms. The undirected invasive testing has the low yield and the significant complication rate. The honest communication with the patient — "the normal tests are reassuring, the chance of the cancer is very low, we will monitor you closely" — is the essential component. [1]
The advanced dementia
The PEG feeding in the advanced dementia does NOT improve the survival, the nutritional state, the pressure ulcer healing, or the aspiration risk (the evidence from the multiple cohort studies and the Cochrane review). The careful hand-feeding, the oral hygiene, the comfort feeding, and the palliative approach are the recommended management. The decision about the artificial nutrition and hydration at the end of life is one of the most ethically complex in the clinical medicine and requires the careful discussion with the family and the multidisciplinary team. [1]
The exam traps
- The weight loss treated as the diagnosis rather than the symptom. The appetite stimulant or the nutritional supplement without the diagnostic workup delays the identification of the malignancy, the hyperthyroidism, or the Addison disease.
- The appetite not assessed in the first minute. The weight loss with the preserved appetite points to the hypermetabolic or the malabsorptive; the weight loss with the anorexia points to the malignancy, the infection, the depression, or the obstruction.
- The missed Addison disease. The weight loss with the fatigue, the postural dizziness, and the hyperpigmentation is the Addison disease until proven otherwise. The undiagnosed Addisonian crisis is fatal.
- The missed depression. The depression is the commonest non-organic cause and is frequently missed. The simple screen identifies it.
- The over-investigation after the normal workup. The Metalidis evidence supports the 3 to 6 month observation. The PET scan after the normal CT and the normal endoscopy is not supported.
- The refeeding syndrome. The severely malnourished patient who is rapidly refed develops the fatal electrolyte disturbance. The slow refeeding, the thiamine, and the electrolyte monitoring prevent it.
- The cancer cachexia treated as the starvation. The forced feeding in the refractory cachexia causes the distress without the benefit. The management is the treatment of the cancer and the palliative approach.
- The appetite stimulant as the substitute for the cause treatment. The megestrol and the dexamethasone are reserved for the palliative phase. The non-palliative use is not supported.
- The self-reported weight loss accepted without the objective documentation. The self-report is unreliable. The prior records, the clinic weights, and the clothing size change are the confirmation.
- The missed elder abuse. The unexplained weight loss in the older adult is the marker of the abuse. The safeguarding screen and the mandatory reporting are the duty of the clinician. [1]
Key takeaways for the exam
- The threshold: greater than 5 per cent in 6 months is the significant loss and mandates the investigation.
- The first-minute questions: intentional or involuntary? Appetite preserved or lost?
- The seven categories: malignancy, endocrine, GI, chronic infection, psychiatric, drugs, social.
- The Tier 1 panel: FBC, U and E, LFTs, TFTs, glucose and HbA1c, CRP, iron studies, B12 and folate, calcium, CXR, urinalysis, faecal immunochemical test, abdominal ultrasound, depression screen.
- The Tier 2: CT CAP, upper GI endoscopy and colonoscopy, coeliac serology, serum and urine electrophoresis, autoimmune screen.
- The Metalidis rule: the normal Tier 1 workup has a 99 per cent negative predictive value for the malignancy; the 3 to 6 month observation is appropriate.
- The Hernandez score: the elevated ALP, the elevated LDH, the low albumin, the elevated white cell count, and the age above 80; the two or more variables increase the malignancy probability.
- The Fearon cachexia: the weight loss greater than 5 per cent, or greater than 2 per cent with the BMI below 20 or the sarcopenia.
- The refeeding syndrome: the slow refeeding, the thiamine, the electrolyte monitoring in the high-risk patient.
- The management principle: treat the cause; the nutritional support is the bridge. [1]
References
- Gaddey HL, Holder K. Unintentional weight loss in older adults. Am Fam Physician 2014;89(9):718-722. PMID 24784334.
- Hernández JL, Riancho JA, Matorras P, González-Macías J. Clinical evaluation for cancer in patients with involuntary weight loss without specific symptoms. Am J Med 2003;114(8):631-637. PMID 12798450.
- Hernández JL, Matorras P, Riancho JA, González-Macías J. Involuntary weight loss without specific symptoms: a clinical prediction score for malignant neoplasm. QJM 2003;96(9):649-655. PMID 12925720.
- Metalidis C, Knockaert DC, Bobbaers H, Vanderschueren S. Involuntary weight loss. Does a negative baseline evaluation provide adequate reassurance? Eur J Intern Med 2008;19(5):355-359. PMID 18549937.
- Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus. Lancet Oncol 2011;12(5):489-495. PMID 21296615.
- Wallace JI, Schwartz RS, LaCroix AZ, Uhlmann RF, Pearlman RA. Involuntary weight loss in older outpatients: incidence and clinical significance. J Am Geriatr Soc 1995;43(4):329-337. PMID 7706619.
- Moriguti JC, Moriguti EK, Ferriolli E, et al. Involuntary weight loss in elderly individuals: assessment and treatment. Sao Paulo Med J 2001;119(2):72-77. PMID 11276170.
- Baicus C, Rimbas M, Baicus A, Caraiola S. Cancer and involuntary weight loss: failure to validate a prediction score. PLoS One 2014;9(4):e95286. PMID 24762986. [1]
References
- [1]Gaddey HL, Holder K Unintentional weight loss in older adults Am Fam Physician, 2014.PMID 24784334
- [2]Hernández JL, Riancho JA, Matorras P, González-Macías J Clinical evaluation for cancer in patients with involuntary weight loss without specific symptoms Am J Med, 2003.PMID 12798450
- [3]Hernández JL, Matorras P, Riancho JA, González-Macías J Involuntary weight loss without specific symptoms: a clinical prediction score for malignant neoplasm QJM, 2003.PMID 12925720
- [4]Metalidis C, Knockaert DC, Bobbaers H, Vanderschueren S Involuntary weight loss. Does a negative baseline evaluation provide adequate reassurance? Eur J Intern Med, 2008.PMID 18549937
- [5]Fearon K, Strasser F, Anker SD, et al. Definition and classification of cancer cachexia: an international consensus Lancet Oncol, 2011.PMID 21296615
- [6]Wallace JI, Schwartz RS, LaCroix AZ, Uhlmann RF, Pearlman RA Involuntary weight loss in older outpatients: incidence and clinical significance J Am Geriatr Soc, 1995.PMID 7706619
- [7]Moriguti JC, Moriguti EK, Ferriolli E, et al. Involuntary weight loss in elderly individuals: assessment and treatment Sao Paulo Med J, 2001.PMID 11276170
- [8]Baicus C, Rimbas M, Baicus A, Caraiola S Cancer and involuntary weight loss: failure to validate a prediction score PLoS One, 2014.PMID 24762986