Phys · general-medicine
Urticaria and Angioedema
Also known as hives · chronic spontaneous urticaria · CSU · chronic idiopathic urticaria · chronic autoimmune urticaria · physical urticaria · dermographism · cold urticaria · angioedema · hereditary angioedema · HAE · C1 inhibitor deficiency · ACE inhibitor angioedema · bradykinin-mediated angioedema · urticarial vasculitis · omalizumab · icatibant · lanadelumab
Consultant-physician guide to urticaria and angioedema: the lesion-duration rule (transient wheals less than 24 hours equals urticaria; persistent lesions with purpura equal urticarial vasculitis), the acute-versus-chronic classification (chronic spontaneous urticaria CSU as a mast-cell autoimmune disease), the pivotal angioedema branch point (with urticaria equals histamine-mediated; without urticaria equals bradykinin-mediated — hereditary angioedema HAE, ACE inhibitor, acquired C1-INH deficiency), the four-step EAACI treatment ladder (standard-dose H1, up to 4-fold H1, omalizumab, ciclosporin), the acute and prophylactic management of HAE (C1-INH concentrate, icatibant, lanadelumab), and the absolute rules that HAE does NOT respond to adrenaline and ACE inhibitors are never rechallenged.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Urticaria and Angioedema

Urticaria (hives) and angioedema are among the most common conditions a physician sees, and they carry two clinical errors that hurt patients: treating all urticaria as an allergy and missing the bradykinin-mediated angioedema that does not respond to adrenaline. This page is built so a registrar facing either a chronic itch or a swollen tongue in the emergency department can act decisively and defend the decision in a viva. [1]
The two questions that decide everything
When a patient presents with wheals, swelling, or both, answer two questions before reaching for any drug. [1]
Question one — is the individual lesion truly urticaria? Urticarial wheals are transient dermal oedema. Each lesion lasts less than 24 hours, resolves completely without bruising or pigmentation, and is intensely pruritic. If a single wheal lasts more than 24 hours, leaves residual purpura, or is painful or burning rather than itchy, the diagnosis is urticarial vasculitis — a leukocytoclastic small-vessel vasculitis, not ordinary urticaria — and the workup changes immediately to skin biopsy and autoimmune screening. This single discriminator is the most-tested fact in the area. [1]
Question two — when there is angioedema, is it with or without urticaria? This is the pivotal branch point. Angioedema with urticaria is histamine-mediated (allergic reaction or chronic spontaneous urticaria) and responds to adrenaline, antihistamines, and corticosteroids. Angioedema without urticaria or pruritus is bradykinin-mediated — hereditary angioedema (C1-INH deficiency), ACE inhibitor-induced angioedema, or acquired C1-INH deficiency — and does NOT respond to adrenaline, antihistamines, or corticosteroids. Giving repeated doses of adrenaline while a bradykinin-mediated airway closes is a documented cause of death. [1]
Definitions and classification

Urticaria
Urticaria is a mast-cell-driven disease of the superficial dermis. Histamine and other mediators increase vascular permeability of the postcapillary venules, producing the superficial wheal (dermal oedema) and surrounding flare. The intense itch is histamine acting on sensory nerve endings. Because histamine is rapidly metabolised and there is no epidermal injury, the lesion resolves completely and quickly — the defining clinical feature. [1]
Classification is by duration and by the presence or absence of a reproducible trigger. [1]
| Type | Duration | Subtype | Comment |
|---|---|---|---|
| Acute urticaria | Less than 6 weeks | — | Usually IgE-mediated (food, drug, sting), infective, or idiopathic; self-limiting; investigation rarely needed |
| Chronic urticaria | More than 6 weeks | Chronic spontaneous urticaria (CSU) | Wheals and/or angioedema arising spontaneously, no external trigger; most are autoimmune |
| Chronic urticaria | More than 6 weeks | Chronic inducible (physical) urticaria | Wheals reproducibly induced by a defined physical stimulus |
CSU was formerly called chronic idiopathic or chronic autoimmune urticaria; the international guideline (Zuberbier 2022) standardised the name to chronic spontaneous urticaria. The "spontaneous" distinguishes it from the inducible urticarias, in which a specific physical trigger can be demonstrated. [1]
The chronic inducible (physical) urticarias
These are defined by their provoking stimulus and confirmed by challenge testing. [1]
- Symptomatic dermographism — wheal on firm stroking of the skin; the most common inducible urticaria; test with a dermographometer or the wooden end of a cotton swab.
- Cold contact urticaria — wheals on cold exposure; test with an ice cube on the volar forearm for 5 to 10 minutes. Warn explicitly about the risk of drowning from cold water immersion — the reaction can progress to anaphylaxis.
- Delayed pressure urticaria — painful deep swelling 4 to 6 hours after sustained pressure (backpack straps, tight footwear, tools); a major cause of occupational disability.
- Solar urticaria — wheals within minutes of sunlight exposure; confirmed by phototesting.
- Cholinergic urticaria — pinpoint (1 to 3 mm) wheals triggered by a rise in core body temperature (exercise, hot showers, emotion, spicy food).
- Heat contact urticaria, vibratory angioedema (vibration, e.g. jackhammer), and aquagenic urticaria (water contact) are rarer subtypes. [1]
Angioedema
Angioedema is oedema of the deep dermis, subcutaneous tissue, or submucosa — lips, tongue, eyelids, genitalia, bowel wall, and larynx. The skin surface is normal (no wheal). It may accompany urticaria (histamine-mediated) or occur alone (bradykinin-mediated). [1]
Pathophysiology — why the mechanism dictates the treatment
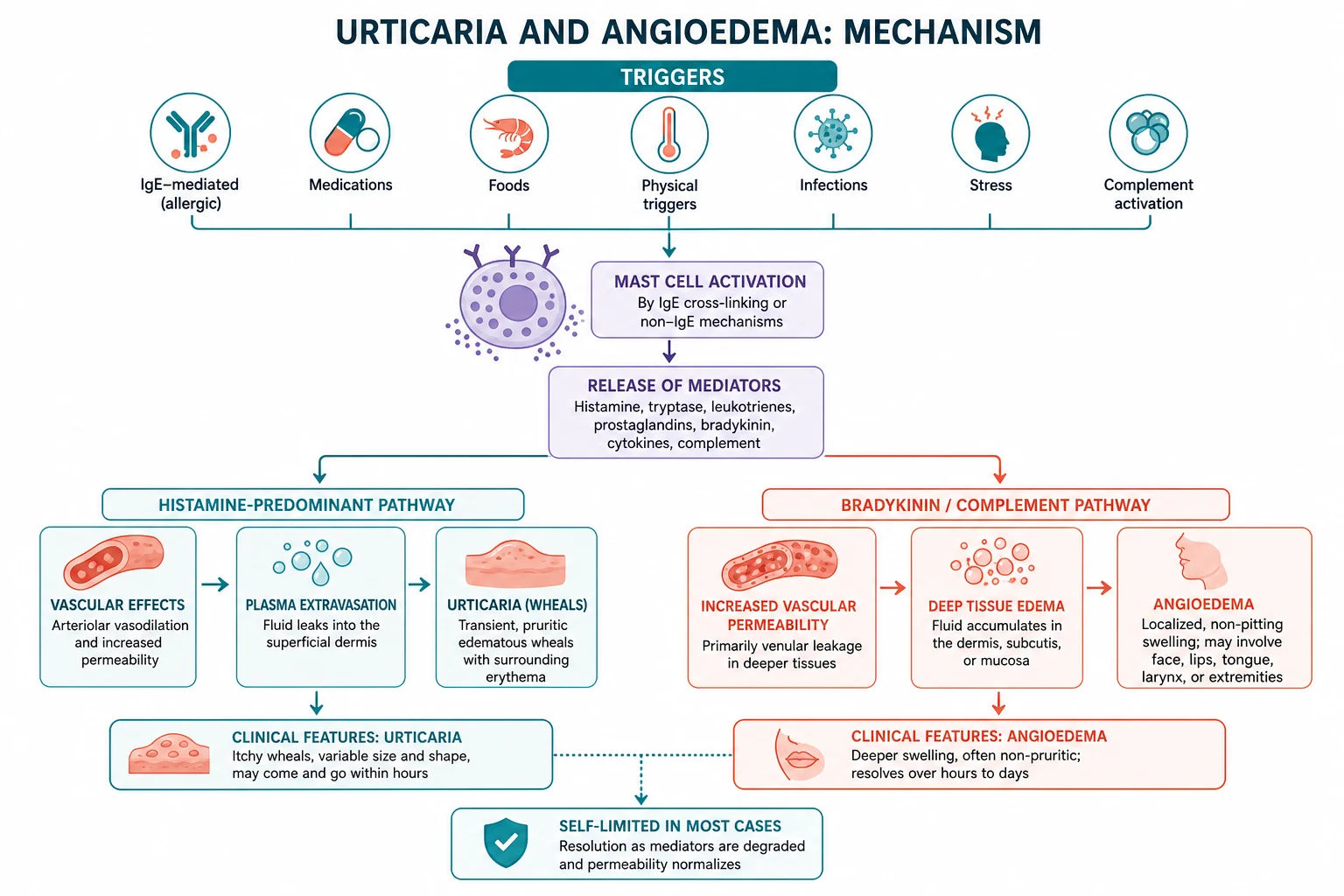
The mast cell in urticaria
The central effector cell is the dermal mast cell. On activation it releases histamine, platelet-activating factor, prostaglandin D2, and leukotrienes, producing vasodilation, increased vascular permeability, and sensory nerve stimulation (itch). In CSU the mast cell is chronically activated not by an external allergen but by an endogenous signal. [1]
Why CSU is an autoimmune disease in many patients
Approximately 30 to 50 per cent of CSU patients have functional IgG autoantibodies directed against the alpha subunit of the high-affinity IgE receptor (FceRI) on mast cells and basophils, or less commonly against IgE itself. These antibodies cross-link the receptor and trigger degranulation, producing chronic mast cell activation. This is the basis for the autologous serum skin test (ASST) — injecting the patient's own serum intradermally produces a wheal-and-flare — and for the response to immunomodulatory therapy such as omalizumab and ciclosporin. The autoimmune subgroup has historically been called chronic autoimmune urticaria. [1]
Why bradykinin-mediated angioedema does not respond to adrenaline
Hereditary angioedema and ACE inhibitor angioedema are driven by bradykinin, not histamine. C1 inhibitor normally serves two inhibitory roles: it checks activated kallikrein (limiting bradykinin generation from high-molecular-weight kininogen) and it checks activated C1 in the classical complement pathway. When C1 inhibitor is deficient (HAE) or when kininase II (angiotensin-converting enzyme) is blocked (ACE inhibitor therapy), bradykinin accumulates and vascular leakage follows. Adrenaline, antihistamines, and corticosteroids do not touch bradykinin — which is why HAE attacks require C1-INH concentrate or a bradykinin B2 receptor antagonist (icatibant). [1]
Why NSAIDs worsen urticaria in a subset
Non-selective NSAIDs (aspirin, naproxen, ibuprofen) inhibit cyclo-oxygenase-1, shunting arachidonic acid down the lipoxygenase pathway and increasing leukotriene (C4, D4, E4) production. Leukotrienes are potent mast cell activators. About 20 to 30 per cent of CSU patients NSAID-exacerbate, and the effect class-shares across non-selective NSAIDs but not COX-2 selective inhibitors. This is a pharmacologic (COX-1) effect, not IgE-mediated. [1]
Clinical features and presentations
Acute urticaria
Acute urticaria is common, often affects a young adult or child, and is usually self-limiting over hours to days. The history usually identifies a trigger: a new drug (beta-lactam antibiotic, NSAID, opiate), a food (peanut, shellfish, egg), an insect sting, or a recent viral or bacterial infection. Most cases resolve without recurrence. Investigation is rarely needed beyond a focused history — routine blood tests, allergy panels, and complement are NOT indicated in straightforward acute urticaria. [1]
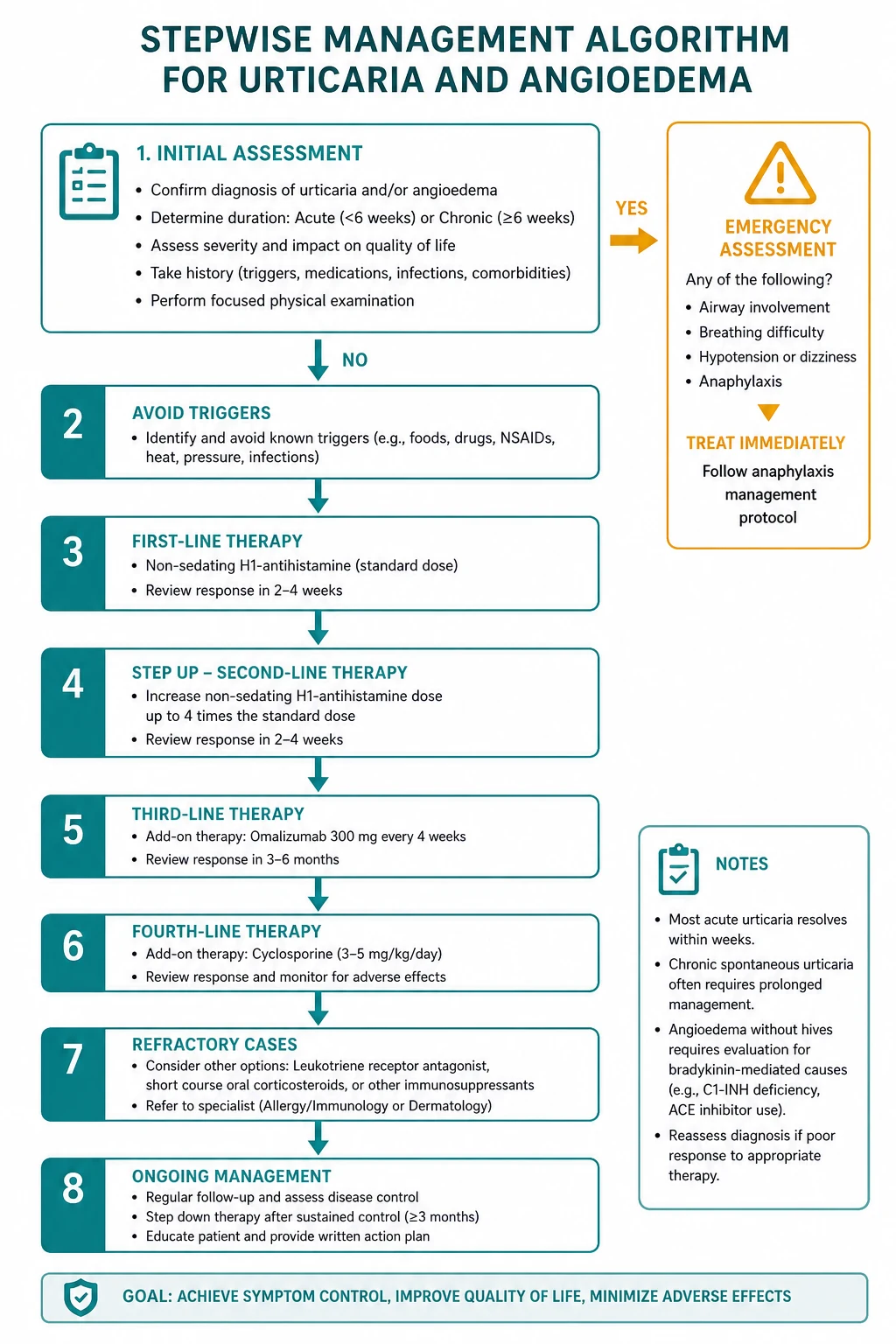
The critical exclusion is anaphylaxis: if the urticarial rash is accompanied by airway, breathing, circulatory, or gastrointestinal involvement within minutes to hours of a trigger, treat as anaphylaxis with intramuscular adrenaline. Isolated urticaria without systemic features is not anaphylaxis. [1]
Chronic spontaneous urticaria
CSU presents as daily or near-daily transient wheals for more than 6 weeks, often with angioedema in about half of patients, intensely pruritic, and worse with NSAIDs, stress, overheating, alcohol, and intercurrent infection. Onset is typically age 20 to 40. The quality-of-life impact is severe — sleep disturbance, anxiety, depression, and reduced work productivity, with health utility scores comparable to coronary artery disease. Thyroid autoimmunity ( Hashimoto thyroiditis, anti-TPO antibodies) is associated in 15 to 25 per cent and should be screened. [1]
Hereditary angioedema
HAE is an autosomal dominant deficiency of C1 inhibitor caused by a mutation in the SERPING1 gene. Onset is in childhood or adolescence (not infancy), with attacks worsening at puberty. Attacks are of non-pitting, non-urticarial, non-pruritic angioedema affecting the extremities, face, genitalia, gastrointestinal tract (severe abdominal pain and vomiting from bowel-wall oedema), and potentially the larynx. Attacks last 2 to 5 days and are triggered by trauma, dental work, emotional stress, menses, oestrogen, and ACE inhibitors. A family history is usually present but de novo mutations account for about 25 per cent of cases. [1]
Two types are recognised. Type 1 (about 85 per cent) has low antigenic and functional C1 inhibitor levels because the defective allele produces a non-secreted protein. Type 2 (about 15 per cent) has a normal or high antigenic level but a dysfunctional protein, so function is low while the antigenic level is normal — this is why the functional C1 inhibitor assay is essential, not the antigenic level alone. [1]
ACE inhibitor-induced angioedema
This is the most common cause of bradykinin-mediated angioedema in adults. It occurs in 0.1 to 0.7 per cent of patients on ACE inhibitors, is more common in Black patients, and typically involves the lips, tongue, face, and upper airway. Although most cases occur within the first month of therapy, attacks can occur years after starting — do not dismiss the diagnosis because the patient has been on the drug for years. The swallow and airway can be compromised. The drug must be stopped permanently and never rechallenged; switch to an angiotensin receptor blocker (which does not inhibit kininase II) or a calcium channel blocker. [1]
Acquired C1 inhibitor deficiency
New-onset angioedema in an older adult with low C4, low C1-INH function, and low C1q (C1q is normal in hereditary HAE) is acquired. It is driven by consumption from a B-cell lymphoproliferative disorder (CLL, lymphoma, monoclonal gammopathy) or by autoantibodies to C1-INH. The C1q level is the discriminator between hereditary and acquired disease in the older adult — and the underlying malignancy must be sought because treating the HAE alone misses the cause. [1]
Differential diagnosis — the discriminating questions
Is it urticaria or something else? Atopic dermatitis (flexural, chronic, lichenification), contact dermatitis (patterned, exposure history), scabies (burrows, web-space involvement, family contacts, nocturnal itch), drug eruptions (maculopapular, not transient), erythema multiforme (target lesions, mucosal involvement), bullous pemphigoid (tense bullae in the elderly, biopsy with immunofluorescence), and mastocytosis (urticaria pigmentosa, positive Darier sign) all enter the differential of a pruritic eruption. [1]
Is it urticaria or urticarial vasculitis? The lesion duration and residual change are the discriminators. CSU wheals last less than 24 hours and resolve completely; urticarial vasculitis wheals last more than 24 hours, are painful or burning, leave bruising or pigmentation, and may be accompanied by arthralgia and low complement. Confirm with a 4 mm punch biopsy of a fresh lesion showing leukocytoclasia. [1]
Is the angioedema histamine-mediated or bradykinin-mediated? The presence of urticaria and pruritus, and the response to antihistamines, indicate histamine-mediated disease. Their absence indicates bradykinin-mediated disease (HAE, ACE inhibitor, acquired C1-INH). This is the single most important branch point in the whole topic. [1]
Is it HAE or acquired C1-INH deficiency? HAE begins in childhood, is familial, and has normal C1q. Acquired C1-INH deficiency begins in older adulthood, has no family history, has low C1q, and is driven by a lymphoproliferative disorder or autoantibody. [1]
Is it HAE or ACE inhibitor angioedema in the emergency department? ACE inhibitor angioedema has no family history, no childhood attacks, normal C4, and onset related to the drug. HAE has childhood onset, family history, low C4 between attacks, and abdominal attacks. If unclear, stop the ACE inhibitor permanently and check C4 and C1-INH function in convalescence. [1]
Investigations
Acute urticaria
The diagnosis is clinical. A focused history (new drug, food, infection, sting, recent viral illness) identifies the trigger. Skin-prick testing or specific IgE is only useful if the history implicates a clear IgE-mediated trigger. Routine blood tests, broad allergy panels, and complement are NOT indicated. [1]
Chronic spontaneous urticaria
A limited panel is sufficient: full blood count with differential (to exclude eosinophilia suggesting parasitic infestation or atopy), CRP or ESR (a raised value suggests urticarial vasculitis or systemic disease), and thyroid function with anti-TPO antibodies (because of the 15 to 25 per cent association with thyroid autoimmunity). Extensive allergy testing is NOT indicated because CSU is not an IgE-mediated food or inhalant allergy. [1]
The autologous serum skin test (ASST) and the basophil activation test (CD63 by flow cytometry) confirm the autoimmune subgroup in 30 to 50 per cent, but they rarely change management because the treatment ladder is the same regardless. [1]
Urticarial vasculitis — when and how
Suspect urticarial vasculitis when wheals last more than 24 hours, are painful, leave residual pigment, or are accompanied by arthralgia, fever, or renal disease. Perform a 4 mm punch biopsy of a fresh wheal (less than 24 to 48 hours old) for histology (leukocytoclastic vasculitis) and immunofluorescence. Check complement (C3, C4, CH50) — low complement suggests hypocomplementaemic urticarial vasculitis syndrome. Screen for SLE (ANA, dsDNA) and cryoglobulins. [1]
Hereditary angioedema — the screening test is C4
The screening test for HAE is C4, which is low during and between attacks (because of continuous classical pathway consumption). A normal C4 between attacks effectively excludes HAE. Confirm with C1 inhibitor antigenic level (low in type 1), C1 inhibitor functional level (low in type 1 and type 2 — the essential test), and C1q (normal in hereditary HAE, low in acquired). Genetic testing for SERPING1 confirms and enables family testing. [1]
In a patient with a first attack in adulthood and low C1q, search for a B-cell lymphoproliferative disorder: serum protein electrophoresis, immunoglobulins, lymphocyte subsets, and CT of the chest, abdomen, and pelvis. [1]
The physical urticarias — provocation testing
Match the test to the history: dermographism (dermographometer or firm stroke), cold urticaria (ice cube on the forearm for 5 to 10 minutes), delayed pressure urticaria (weighted shoulder strap for 15 minutes, read at 4 to 6 hours), solar urticaria (phototesting), cholinergic (exercise or hot bath), aquagenic (water compress), vibratory (vortex mixer). [1]
The role of serum tryptase
A persistently elevated serum tryptase (especially above 20 micrograms per litre) in recurrent unexplained urticaria, angioedema, or anaphylaxis suggests systemic mastocytosis or a clonal mast cell disorder, and warrants bone marrow evaluation (tryptase stain, KIT D816V mutation, CD25). Check tryptase in any adult with recurrent unexplained anaphylaxis, severe or atypical CSU, or a history of a severe reaction to hymenoptera venom. [1]
Management of chronic spontaneous urticaria — the four-step ladder
The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline (Zuberbier 2022) defines a four-step treatment ladder. The steps are cumulative and the patient moves up the ladder if the response at a step is inadequate after 2 to 4 weeks. [1]
Step 1 — standard-dose second-generation H1 antihistamine
Start with a single second-generation non-sedating H1 antihistamine at standard dose daily: cetirizine 10 mg, fexofenadine 180 mg, loratadine 10 mg, desloratadine 5 mg, or bilastine 20 mg. Regular daily dosing (not PRN) is essential. The onset of full effect at each dose is 1 to 2 weeks. [1]
Step 2 — up-titrate the H1 antihistamine up to 4-fold
If standard dose is inadequate, up-titrate the same second-generation agent to up to 4 times the standard dose (off-label but evidence-supported and the standard second step in the international guideline). Cetirizine up to 40 mg, fexofenadine up to 720 mg, loratadine up to 40 mg, desloratadine up to 20 mg, bilastine up to 80 mg daily. This up-titration is the step most often missed — many prescribers stop at standard dose and either declare treatment failure or add a sedating first-generation agent, which the guideline explicitly advises against. [1]
Step 3 — add omalizumab
Add omalizumab (anti-IgE monoclonal antibody) 300 mg subcutaneously every 4 weeks — the licensed, evidence-based, guideline-preferred third step. The ASTERIA I, ASTERIA II, and GLACIAL trials established that 300 mg every 4 weeks significantly reduces itch and wheal activity; about 65 to 70 per cent of patients respond. The drug is well tolerated; the main adverse events are injection-site reactions and headache. The mean time to response is 1 to 2 weeks. [1]
Step 4 — add ciclosporin
Add ciclosporin 2.5 to 4 mg per kg per day orally in two divided doses for 3 to 6 months (off-label, specialist supervised). Monitor blood pressure (weekly initially then monthly), serum creatinine and estimated glomerular filtration rate (every 2 to 4 weeks), electrolytes, and lipids. Reduce the dose if creatinine rises more than 30 per cent from baseline. Ciclosporin is effective in 65 to 70 per cent of refractory patients but is limited by renal toxicity and hypertension, so it is time-limited. For the small minority who remain refractory, other immunomodulators (mycophenolate, methotrexate, azathioprine, intravenous immunoglobulin) are used in specialist centres. [1]
Adjuncts that are no longer routine steps
H2 antihistamines (famotidine 20 to 40 mg twice daily) and the leukotriene antagonist montelukast 10 mg daily provide modest additional benefit in selected patients but are no longer standard steps in the current guideline — they are optional adjuncts. Note that ranitidine has been withdrawn in Australia and the US for NDMA contamination; use famotidine as the H2 alternative. [1]
Systemic corticosteroids — short courses (oral prednisolone 0.5 mg per kg daily for 3 to 7 days) are reserved for severe acute exacerbations as a bridge to definitive therapy. Chronic oral corticosteroids are avoided because of cumulative toxicity (osteoporosis, diabetes, hypertension, infection, adrenal suppression) and are never a maintenance strategy in CSU. [1]
First-generation sedating antihistamines (promethazine, chlorpheniramine, hydroxyzine) are explicitly NOT recommended for chronic use — they impair cognition, reaction time, and sleep architecture even when the patient does not feel sleepy, and they increase falls in older adults. Reserve them for short-term sedation in severe acute flares only. [1]
Trigger avoidance and lifestyle advice
Advise the patient to avoid non-selective NSAIDs if they exacerbate (a COX-2 selective inhibitor is an alternative if an anti-inflammatory is needed), to avoid ACE inhibitors if a bradykinin-mediated component is suspected, to address stress and sleep, to cool the skin (avoid hot baths and tight clothing), and to identify and treat any thyroid dysfunction. Helicobacter pylori testing and eradication has modest benefit in some CSU patients who are positive and is a reasonable low-risk intervention in refractory disease. Set the expectation that the condition is chronic but usually self-limiting over months to years — about half of patients remit within 1 to 5 years. [1]
Management of hereditary angioedema
Acute attack
For an acute HAE attack the first-line treatments are: [1]
- Plasma-derived C1 inhibitor concentrate (Berinert) 20 units per kg intravenously, or
- Recombinant C1 inhibitor (conestat alfa, Ruconest) 50 units per kg IV (maximum 4200 units), or
- Icatibant 30 mg subcutaneously (a bradykinin B2 receptor antagonist).
- Ecallantide (a kallikrein inhibitor, 30 mg SC in three 10 mg injections) is available in some regions. [1]
Adrenaline, antihistamines, and corticosteroids are NOT effective in HAE. For laryngeal attacks, treat immediately and secure the airway — involve senior anaesthetics and ENT early, prepare for a difficult airway (awake fibre-optic intubation, surgical airway tray at the bedside). For abdominal attacks, opioids control the pain. Home-based self-treatment of acute attacks shortens the time-to-treatment from hours to minutes and improves outcomes. [1]
Long-term prophylaxis
Modern first-line prophylaxis: [1]
- Lanadelumab 300 mg subcutaneously every 2 weeks (then every 4 weeks when stable) — a fully human monoclonal antibody against plasma kallikrein; the HELP trial showed an 87 per cent reduction in monthly attack rate.
- Berotralstat 150 mg orally daily — an oral plasma kallikrein inhibitor; a convenient oral alternative.
- C1 inhibitor concentrate (Cinryze) 1000 units IV every 3 to 4 days for routine prevention. [1]
Attenuated androgens (danazol 50 to 200 mg daily, stanozolol 1 to 2 mg daily) upregulate C1-INH production and are effective but now second-line because of virilisation (hirsutism, acne, irreversible voice deepening in women), menstrual irregularity, hepatotoxicity and hepatic adenoma, dyslipidaemia, and hypertension. They require liver function and lipid monitoring and are contraindicated in pregnancy. [1]
Avoid ACE inhibitors and oestrogen-containing contraception permanently — both raise bradykinin activity and worsen attacks. [1]
Short-term prophylaxis before procedures
Before dental extractions, oral surgery, or airway procedures, give C1 inhibitor concentrate 1000 units IV 1 to 6 hours beforehand — trauma and airway manipulation are classic triggers of laryngeal attacks, and untreated airway manipulation can precipitate fatal laryngeal oedema. For minor procedures, a dose of icatibant held in reserve may be acceptable on specialist advice. Ensure the patient has their on-demand treatment available and wears a medical alert. [1]
Management of ACE inhibitor-induced angioedema
- STOP the ACE inhibitor permanently and NEVER rechallenge — recurrence is common and may be more severe.
- Secure the airway — the tongue and larynx may swell rapidly and intubation may be difficult. Involve anaesthetics and ENT early; consider awake fibre-optic intubation or a surgical airway. Do NOT rely on adrenaline or antihistamines as the sole therapy.
- Supportive care and observation for 24 to 48 hours.
- Icatibant and C1-INH concentrate may be used in severe cases (off-label, mixed evidence — the randomised CAMEO trial did not show a significant benefit of icatibant over placebo for the primary endpoint, but individual patients benefit and the drug is used in centres with access).
- Switch hypertension management to an angiotensin receptor blocker (which does not inhibit kininase II) or a calcium channel blocker. Warn the patient that the risk of recurrence persists for weeks to months after stopping (accumulated tissue bradykinin effect) and carry a medical alert. [1]
Complications
Chronic spontaneous urticaria
The dominant morbidity is impaired quality of life — sleep disturbance, anxiety, depression, and reduced work productivity, with health utility scores among the lowest of any skin disease. Treatment-related harms include sedation from first-generation antihistamines (falls and cognitive impairment, especially in older adults) and the cumulative toxicity of corticosteroids if used chronically. Anaphylaxis is NOT a complication of CSU unless there is a separate IgE-mediated trigger. [1]
Hereditary angioedema
Laryngeal oedema causing asphyxiation is the leading cause of death, with historical mortality from upper airway obstruction reported as high as 14 to 33 per cent before modern therapy. Dental work and oral surgery are classic triggers. With modern on-demand therapy and prophylaxis the mortality is markedly reduced, but a fatal outcome from a missed diagnosis in the emergency department remains well documented. [1]
ACE inhibitor angioedema
The swelling can progress to complete upper airway obstruction and death. The risk is highest within the first 30 days of therapy but may occur years later. [1]
Urticarial vasculitis
It may be cutaneous-limited or part of a systemic connective tissue disease (SLE, Sjogren), hypocomplementaemic urticarial vasculitis syndrome (with arthritis, uveitis, glomerulonephritis, and a COPD-like lung disease), or a paraneoplastic process. Systemic involvement carries renal, pulmonary, and cardiovascular morbidity. [1]
The physical urticarias
Cold urticaria can cause drowning. Delayed pressure urticaria is a major cause of occupational disability. Solar urticaria forces severe lifestyle restriction. Cholinergic urticaria limits exercise. Each of these is a preventable harm with counselling and trigger management. [1]
Special situations
Pregnancy. Second-generation H1 antihistamines with the best safety data (loratadine and cetirizine are widely used in pregnancy) are preferred. Omalizumab has reassuring pregnancy registry data and is used when indicated for severe CSU. Ciclosporin is used in pregnancy under specialist supervision for severe disease. Attenuated androgens are absolutely contraindicated in HAE because they are teratogenic; C1 inhibitor concentrate is safe and preferred in pregnant HAE patients for both acute attacks and prophylaxis. [1]
Children. The principles are the same. CSU in children is less common than in adults and an underlying cause (infection, autoimmune) is more often identified. Paediatric weight-based dosing for cetirizine and fexofenadine applies. Omalizumab is licensed for CSU in children aged 12 and over. Avoid first-generation sedating antihistamines because of paradoxical excitation and cognitive effects. [1]
The older adult. Antihistamine choice favours the least sedating and least anticholinergic (fexofenadine, bilastine) because first-generation agents increase falls and cognitive impairment. ACE inhibitor angioedema is more common in older adults on polypharmacy. Always exclude urticarial vasculitis and bullous pemphigoid in the elderly with new-onset pruritic eruptions. Check tryptase to exclude clonal mast cell disease in atypical presentations. [1]
NSAID-exacerbated urticaria. Avoid all non-selective NSAIDs permanently (cross-reactivity is high). A COX-2 selective inhibitor (celecoxib) is tolerated by most in a supervised oral challenge. Paracetamol is usually safe. The NSAID reaction is pharmacologic (COX-1 inhibition), not IgE-mediated. [1]
Guideline anchoring
The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline (Zuberbier 2022) is the current global standard for urticaria classification, diagnosis, and the four-step treatment ladder. The World Allergy Organization (WAO) guideline governs HAE management. The ANZ perspective is led by ASCIA (Australasian Society of Clinical Immunology and Allergy); the UK by BSACI; the US by AAAAAI. The principles are concordant across regions: standard-dose H1, up to 4-fold H1, omalizumab, ciclosporin. The drug doses above are the ANZ-appropriate doses; ranitidine has been withdrawn in Australia and the US (NDMA contamination) and famotidine is the H2 alternative. [1]
Communication
Explain CSU to the patient plainly: "Your immune system is making antibodies that switch on the mast cells in your skin, releasing histamine and producing the wheals and itch. It is not an allergy to a food or something in your environment, and extensive allergy testing is not helpful. The good news is that it usually goes away on its own over months to years, and we have a stepwise treatment that controls the symptoms in almost everyone." [1]
Counsel the patient with HAE about airway risk explicitly: "Your condition can cause the throat to swell, which can block the airway and is life-threatening. If you feel throat tightness, voice change, or swallowing difficulty, take your emergency treatment immediately and call an ambulance. Never let a dentist or surgeon do a procedure without telling them about your condition. Wear a medical alert at all times." [1]
The high-yield exam traps
- Lesion duration is the discriminator. Wheals lasting more than 24 hours, leaving purpura, or painful rather than itchy are urticarial vasculitis — biopsy.
- Angioedema without urticaria is bradykinin-mediated. HAE, ACE inhibitor, acquired C1-INH. No response to adrenaline, antihistamines, corticosteroids.
- HAE does not respond to adrenaline. Give C1-INH concentrate or icatibant. Do not let the airway close while giving repeated adrenaline.
- ACE inhibitor angioedema can occur years after starting. Stop permanently, never rechallenge.
- Up to 4-fold H1 antihistamine is the second step in CSU. Do not stop at standard dose and do not add a sedating first-generation agent.
- C4 is low in HAE between attacks. A sensitive screening test. C1q distinguishes hereditary (normal) from acquired (low).
- The functional C1-INH assay is essential. Type 2 HAE has a normal antigenic level — measure function, not just antigen.
- Cold urticaria and drowning. Warn the patient explicitly; never swim alone; carry adrenaline.
- First-generation antihistamines impair cognition in chronic use. Use second-generation agents.
- Extensive allergy panels are not indicated in CSU. It is autoimmune or intrinsic mast cell activation, not IgE-mediated food allergy. [1]
References
- Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The international EAACI/GA2LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy 2022;77:734-766. PMID 34536239.
- Maurer M, Rosen K, Hsieh HJ, et al. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria (ASTERIA II). N Engl J Med 2013;368:924-935. PMID 23432142.
- Zuraw BL. Hereditary angioedema. N Engl J Med 2008;359:1027-1036. PMID 18768946.
- Bas M, Greve J, Stelter K, et al. A randomized trial of icatibant in ACE-inhibitor-induced angioedema. N Engl J Med 2015;372:418-425. PMID 25629740.
- Sinert R, Levy P, Bernstein JA, et al. Randomized trial of icatibant for ACE inhibitor-induced upper airway angioedema (CAMEO). Ann Emerg Med 2017;70:559-570. PMID 28552382.
- Cicardi M, Banerji A, Bracho F, et al. Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema (FAST). N Engl J Med 2010;363:532-541. PMID 20818888.
- Banerji A, Riedl MA, Bernstein JA, et al. Effect of lanadelumab compared with placebo on prevention of hereditary angioedema attacks: a randomized clinical trial (HELP). JAMA 2018;320:2108-2121. PMID 30480729.
- Kaplan AP. Chronic spontaneous urticaria: pathogenesis and treatment considerations. Allergy Asthma Immunol Res 2017;9:477-482. PMID 28913986. [1]
References
- [1]Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria Allergy, 2022.PMID 34536239
- [2]Maurer M, Rosen K, Hsieh HJ, et al. Omalizumab for the treatment of chronic idiopathic or spontaneous urticaria N Engl J Med, 2013.PMID 23432142
- [3]Zuraw BL Clinical practice. Hereditary angioedema N Engl J Med, 2008.PMID 18768946
- [4]Bas M, Greve J, Stelter K, et al. A randomized trial of icatibant in ACE-inhibitor-induced angioedema N Engl J Med, 2015.PMID 25629740
- [5]Sinert R, Levy P, Bernstein JA, et al. Randomized Trial of Icatibant for Angiotensin-Converting Enzyme Inhibitor-Induced Upper Airway Angioedema J Allergy Clin Immunol Pract, 2017.PMID 28552382
- [6]Cicardi M, Banerji A, Bracho F, et al. Icatibant, a new bradykinin-receptor antagonist, in hereditary angioedema N Engl J Med, 2010.PMID 20818888
- [7]Banerji A, Riedl MA, Bernstein JA, et al. Effect of Lanadelumab Compared With Placebo on Prevention of Hereditary Angioedema Attacks: A Randomized Clinical Trial JAMA, 2018.PMID 30480729
- [8]Kaplan AP Chronic Spontaneous Urticaria: Pathogenesis and Treatment Considerations Allergy Asthma Immunol Res, 2017.PMID 28913986