Phys · geriatric
Comprehensive Geriatric Assessment and Frailty
Also known as comprehensive geriatric assessment · CGA · geriatric assessment · frailty · frailty phenotype · frailty index · Clinical Frailty Scale · CFS · sarcopenia · EWGSOP2 · Katz index · Lawton IADL scale · Timed Up and Go · MNA-SF · geriatric evaluation and management · GEM
Consultant-physician-depth guide to comprehensive geriatric assessment (CGA) and frailty for FRACP DWE and DCE — the multidimensional interdisciplinary diagnostic process, the four domains (medical, functional, psychological, social), the Katz ADL index, the Lawton IADL scale, the Timed Up and Go test, the Fried frailty phenotype, the Rockwood frailty index, the Clinical Frailty Scale, the EWGSOP2 sarcopenia criteria, the MNA-SF nutrition screen, the 4AT delirium screen, the MoCA and GDS, the CGA delivery models, and the Cochrane meta-analysis evidence for reduced mortality and institutionalisation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Comprehensive Geriatric Assessment and Frailty

The answer first
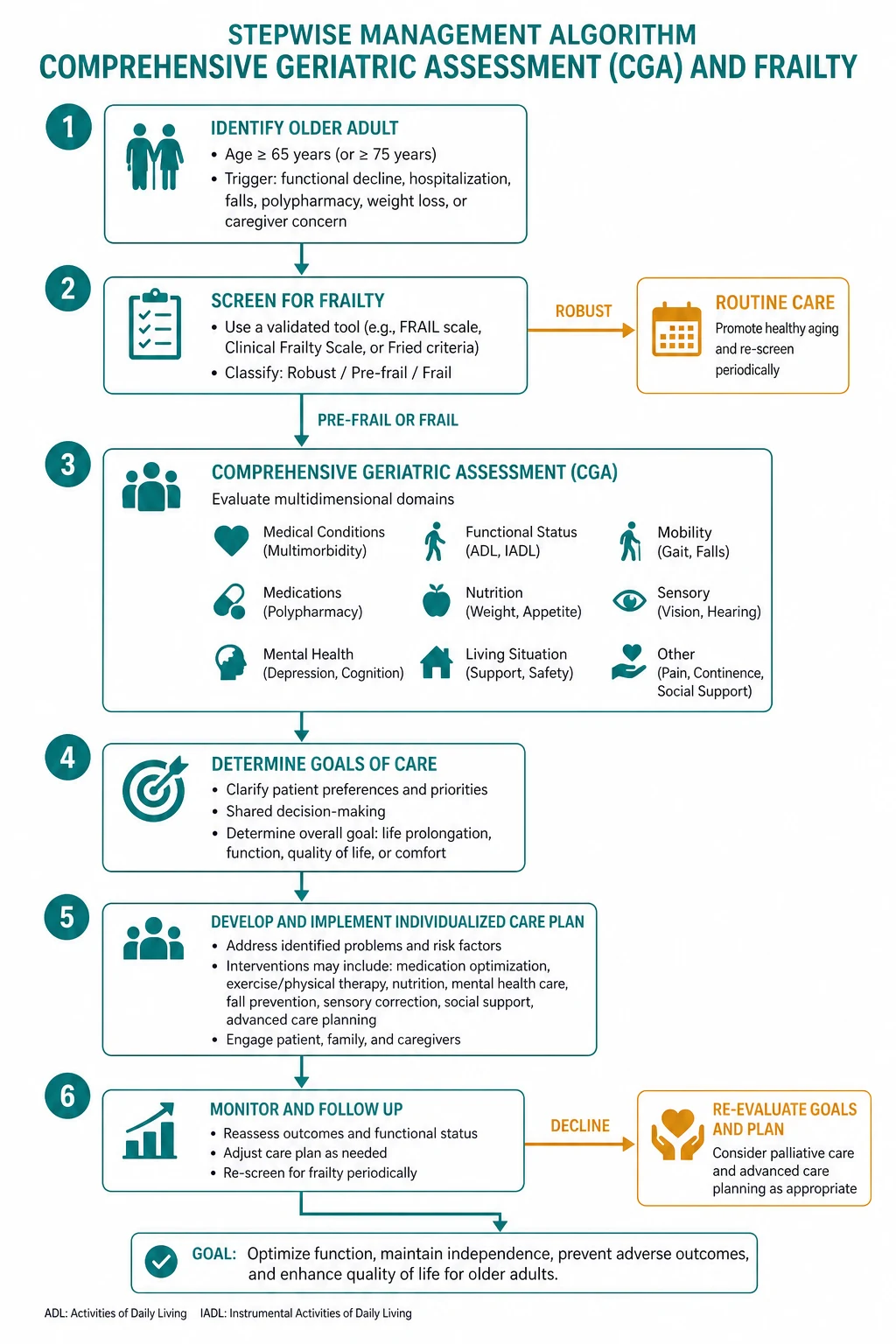
Comprehensive geriatric assessment (CGA) is a multidimensional, interdisciplinary diagnostic and therapeutic process that determines a frail older person's medical, psychological, functional, and social capabilities and limitations, in order to develop a coordinated and integrated plan for treatment and long-term follow-up. It is not a single test — it is a structured assessment, a multidisciplinary team meeting, and a problem list that drives an integrated management plan. [1]
Frailty is a distinct clinical syndrome of increased vulnerability to stressor events, resulting from age-related cumulative decline in multiple physiological systems, such that the ability to cope with everyday or acute stress is compromised. It is not old age, it is not disability, and it is not comorbidity — though all three overlap with it. Frailty is reversible and is the single most important therapeutic target in geriatric medicine. [1]
The five rules that determine everything in this topic are: [1]
- CGA works. The 2017 Cochrane meta-analysis of 29 randomised trials showed that older adults who receive CGA are more likely to be alive and in their own homes at follow-up, and less likely to die or be institutionalised, than those receiving usual care (Ellis 2017, PMID 28898390). The exam expects you to know this evidence base cold.
- Frailty is the unifying concept. The frailty phenotype (Fried 2001, PMID 11253156) and the cumulative deficit model (Rockwood and Mitnitski 2007, PMID 17634318) are the two competing but complementary frameworks. The Clinical Frailty Scale (Rockwood 2005, PMID 16129869) is the bedside tool. You must know all three and their relationship.
- Function is a vital sign. An older person's grip strength, gait speed, and ADL independence predict mortality, institutionalisation, and complication risk more powerfully than most laboratory values. Every CGA measures them.
- Sarcopenia is the muscle substrate of frailty. The EWGSOP2 criteria (Cruz-Jentoft 2019, PMID 31081853) — low muscle strength plus low muscle quantity or quality — make sarcopenia a diagnosable and treatable condition, not an inevitable consequence of ageing.
- The CGA changes the plan. A frailty score of 7 on the Clinical Frailty Scale should change the consent conversation, the perioperative risk assessment, the medication review, the rehabilitation plan, and the goals of care discussion. If it does not change the plan, the assessment was a paperwork exercise, not a CGA. [1]
DWE high-yield trap: When asked "what is the single best predictor of adverse outcomes in an older hospitalised patient," the answer is the Clinical Frailty Scale score on admission — it predicts mortality, length of stay, institutionalisation, and functional decline, and it should be documented in every older patient's chart within 24 hours of admission. [1]
Definition — what CGA is, and what it is not
The formal definition, established by the 1987 US Consensus Development Conference on Geriatric Assessment and adopted by every subsequent guideline, has three non-negotiable elements: [1]
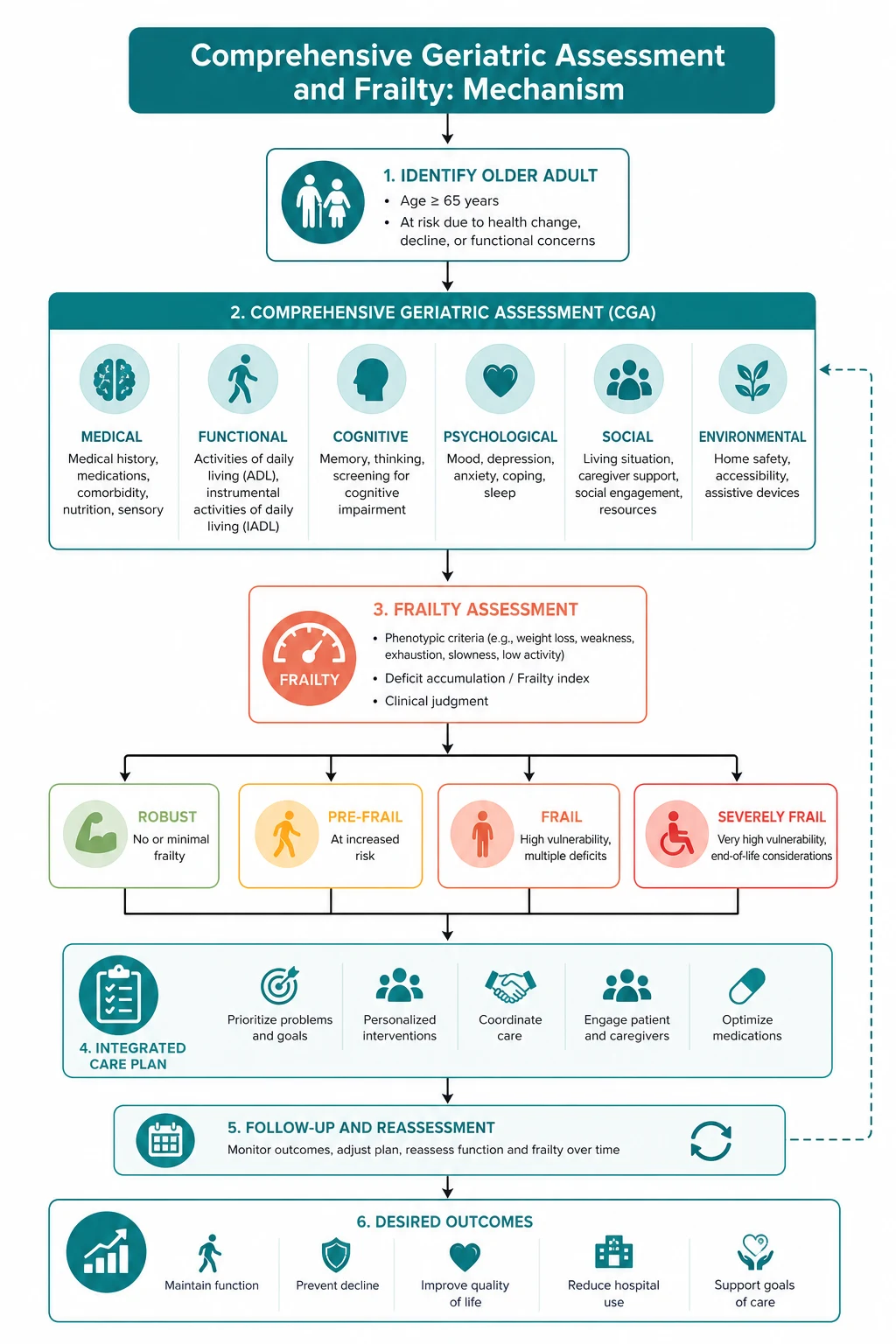
- Multidimensional — it covers at least four domains: medical (comorbidities, polypharmacy, nutrition), functional (ADLs, IADLs, gait, balance, falls), psychological (cognition, mood, delirium), and social (support, finances, living situation, advance care planning).
- Interdisciplinary — it is performed by a team, typically a geriatrician, a specialist geriatric nurse, a physiotherapist, an occupational therapist, a social worker, a pharmacist, and a dietitian, with a structured case conference to synthesise findings into a single plan.
- Therapeutic, not just diagnostic — the assessment produces a coordinated and integrated plan for treatment and long-term follow-up. An assessment without a management plan and a follow-up is not a CGA. [1]
What CGA is not: it is not a single clinic visit, not a cognitive screen, not a falls risk assessment, and not a discharge planning checklist. It is the structured, multidisciplinary process that incorporates all of these into a problem list and an integrated plan. [1]
Clinical rule: The exam discriminator between "comprehensive geriatric assessment" and "standard geriatric review" is the interdisciplinary team meeting. The team case conference, where the problems are synthesised into a single plan with shared goals and allocated responsibilities, is what makes the process comprehensive. [1]
The four domains of CGA

1. The medical domain
This is the systematic review of the older person's medical state, with particular attention to the problems that drive functional decline and that are under-diagnosed in routine practice: [1]
- Comorbidities — list every active condition, prioritise them, and identify the interactions. The Charlson Comorbidity Index quantifies the burden and predicts mortality.
- Polypharmacy — five or more regular medications is the standard threshold. Review each drug for indication, benefit, harm, and interaction. The anticholinergic burden and the Drug Burden Index are quantitative measures of the cognitive and functional harm of polypharmacy. Deprescribing is a treatment.
- Nutrition — unintentional weight loss, appetite, dietary intake, swallowing, dentition, and the MNA-SF screen (see below).
- Cognition — screen every older person with the MoCA (or ACE-III if available). Do not rely on bedside impression — the MoCA detects impairment that the interview misses.
- Mood — screen with the 15-item Geriatric Depression Scale. Depression in older adults is under-diagnosed, is a major driver of functional decline and pseudodementia, and is treatable.
- Sensory — vision (Snellen chart, cataracts, macular degeneration) and hearing (whispered voice test, audiometry). Uncorrected sensory loss drives cognitive decline, falls, and social isolation. Always check whether the patient has and wears their glasses and hearing aids.
- Continence — urinary and faecal incontinence, retention, constipation. The most common reversible causes of urinary incontinence are DIAPPERS (Delirium, Infection, Atrophic vaginitis, Pharmaceuticals, Psychological, Excess output, Restricted mobility, Stool impaction).
- Falls and syncope — every older person should be asked about falls in the past year, and a fall with injury or recurrent falls demands a structured assessment (see the falls and syncope topic). [1]
2. The functional domain
Function is the domain that most distinguishes the geriatric assessment from the standard medical review. It has two levels — basic self-care and independent community living — plus the physical performance measures that predict outcomes. [1]
Basic activities of daily living (ADLs) — the Katz index (Katz 1963, PMID 14044222): [1]
The Katz index assesses six basic self-care activities: bathing, dressing, toileting, transferring, continence, and feeding. Each is scored as independent (1 point) or dependent (0 points), giving a total of 0 to 6. A score of 6 indicates full independence; a score of 4 indicates assistance needed; a score of 2 or below indicates severe functional dependency. The Katz index is the standard bedside measure of basic function and predicts mortality, institutionalisation, and the burden of care. [1]
Instrumental activities of daily living (IADLs) — the Lawton scale (Lawton and Brody 1969, PMID 5349366): [1]
The Lawton IADL scale assesses eight higher-order activities necessary for independent living in the community: using the telephone, shopping, food preparation, housekeeping, laundry, transportation, responsibility for medications, and handling finances. Each is scored as independent or dependent. Loss of IADL independence (typically finances first, then medications and transport) marks the transition from robust ageing to functional decline and is often the earliest sign of cognitive impairment or frailty. Note: the Lawton scale was originally validated in women with a modified 6-item version for men, but the 8-item version is now used for both sexes. [1]
| Domain | Instrument | Level | What loss means |
|---|---|---|---|
| Basic self-care | Katz ADL index | Bathing, dressing, toileting, transferring, continence, feeding | Severe dependency, high care needs |
| Community living | Lawton IADL scale | Telephone, shopping, cooking, housekeeping, laundry, transport, medications, finances | Early decline, often first sign of cognitive impairment |
| Physical performance | Timed Up and Go | Rise from chair, walk 3 metres, turn, walk back, sit | Gait under 0.8 m/s or TUG over 12 seconds predicts falls, frailty, and mortality |
| Strength | Grip strength | Dynamometer (Jamar) | Under 27 kg men, under 16 kg women — low strength, probable sarcopenia |
The Timed Up and Go (TUG) test: [1]
Ask the patient to sit in a standard chair with armrests. On the word "go," the patient stands, walks 3 metres at their usual pace, turns, walks back, and sits. Time the task. A TUG of 12 seconds or more predicts falls and identifies gait and balance problems. A TUG of 20 seconds or more indicates severe mobility limitation. The TUG correlates with the Berg Balance Scale and gait speed but takes a fraction of the time — it is the highest-yield single physical performance test in geriatric medicine. [1]
Gait speed — the time to walk 4 metres at usual pace — is another vital sign. A gait speed of under 0.8 metres per second predicts mortality, hospitalisation, and disability. A gait speed of under 0.6 m/s is associated with severe frailty and high falls risk. [1]
Examiner point: The single most discriminating physical performance measure in older adults is gait speed. The exam expects you to know the 0.8 m/s threshold and to recognise that a slow gait is a powerful independent predictor of adverse outcomes — frailty, falls, disability, institutionalisation, and mortality. [1]
3. The psychological domain
This domain assesses cognition, mood, and delirium — the three states that most drive functional decline, carer strain, and admission to residential care. [1]
Cognitive screening — the MoCA (Nasreddine 2005, PMID 15817019): [1]
The Montreal Cognitive Assessment is a 30-point screen covering seven domains: visuospatial and executive (clock drawing, trail-making, cube copy), naming, attention (digit span, vigilance, serial sevens), language (sentence repetition, verbal fluency), abstraction, delayed recall (five words), and orientation. A cutoff of 26 out of 30 (with a one-point adjustment for 12 years or fewer of education) has about 90 percent sensitivity for mild cognitive impairment — far superior to the MMSE. The MoCA takes 10 to 15 minutes and is the recommended first-line cognitive screen in the memory clinic and the CGA. [1]
The MMSE remains useful for severity staging and longitudinal tracking but is insensitive to early and executive-predominant impairment. In a CGA, use the MoCA. [1]
Mood screening — the Geriatric Depression Scale (GDS-15): [1]
The 15-item GDS is a yes/no questionnaire designed for older adults (avoiding the somatic items of the PHQ-9 that overlap with physical illness). A score of 5 or more out of 15 suggests depression and warrants a full clinical assessment. The GDS-15 takes 5 minutes, is suitable for patients with mild cognitive impairment, and is the recommended mood screen in the CGA. Always screen mood in any patient with cognitive impairment — depression and dementia coexist in up to 40 percent of cases, and pseudodementia (depression masquerading as dementia) is a reversible mimic. [1]
Delirium screening — the 4AT (Bellelli 2014, PMID 24590568): [1]
The 4AT is a 2-minute rapid screen for delirium with four components: Alertness (normal 0, mild sleepiness 1, drowsy 2, 3-4 if obviously abnormal), AMT-4 (age, date of birth, place, current year — 0 if all correct, 1 if any wrong), Attention (months of the year backwards — 0 if achieves 7 or more, 1 if starts but gets fewer than 7, 2 if cannot start), and Acute change or fluctuating course (0 if no, 1 if yes). A total of 4 or more suggests delirium, with a sensitivity of about 90 percent and specificity of 84 percent. The 4AT is the recommended delirium screen in every hospitalised older person and is a mandatory component of the CGA in the inpatient setting. [1]
Clinical rule: Delirium is the single most common acute cognitive emergency in older hospitalised patients, affecting 20 to 30 percent of medical inpatients and up to 50 percent of postoperative patients. The 4AT should be performed on every older person at admission and at any deterioration — "acutely confused" is delirium until proven otherwise, and delirium is a medical emergency with a mortality of up to 30 percent at 12 months. [1]
4. The social domain
This domain assesses the social, environmental, and financial context that determines whether the older person can be supported safely in the community. It is the domain most often under-assessed by physicians who focus on the medical problems, and it is the domain that most determines discharge destination and the success of the community care plan. [1]
- Social support — who lives with the patient, who visits, who provides care, and who is the emergency contact. Identify the primary carer and assess carer strain — carer burnout is the commonest reason for institutionalisation.
- Finances — pension, savings, private health insurance, eligibility for government-funded home care packages or residential care subsidies. Financial stress drives poor nutrition, medication non-adherence, and inability to access services.
- Living situation — the type of dwelling (house, unit, residential care), the layout (stairs, bathroom access, kitchen), the safety hazards (rugs, cords, poor lighting, lack of grab rails), and the proximity to shops, transport, and family. A home safety assessment by an occupational therapist is a core CGA intervention.
- Advance care planning — the patient's values, goals, and preferences for future care; the existence of an advance care directive; the appointment of a substitute decision-maker (enduring guardian, power of attorney); the preferred place of care and place of death. These conversations should begin early, while the patient retains capacity, and should be revisited with every transition. [1]
Examiner point: The four domains of CGA — medical, functional, psychological, and social — are the structural answer to every CGA question. When asked "describe a comprehensive geriatric assessment," lead with the four domains and name the instrument for each: comorbidities and polypharmacy for medical, Katz and Lawton for functional, MoCA and GDS for psychological, and social support and advance care planning for social. The interdisciplinary team meeting synthesises them into the plan. [1]
Frailty — the two conceptual models
Frailty is the core concept of modern geriatric medicine, and the exam expects you to know the two models, their relationship, and the bedside tool that operationalises them. [1]

Model 1 — the Fried frailty phenotype (physical)
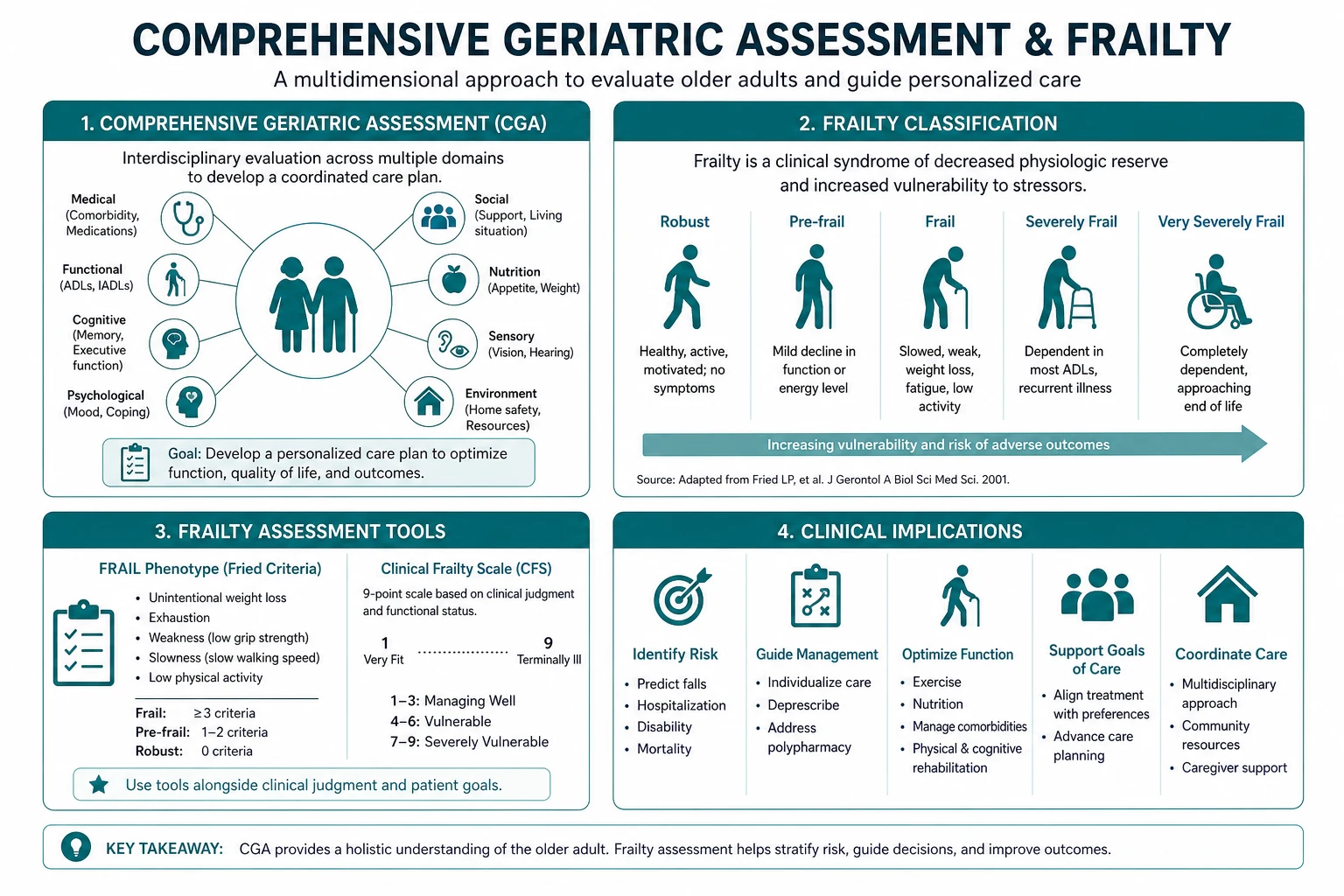
The Fried phenotype, published in 2001 from the Cardiovascular Health Study (Fried 2001, PMID 11253156), defines frailty as a clinical syndrome with three or more of five physical criteria: [1]
- Unintentional weight loss — 10 pounds (4.5 kg) or more, or 5 percent or more of body weight, in the preceding year.
- Self-reported exhaustion — answering "3 or more days" or "moderate to most of the time" to either of two CES-D items on effort and getting going.
- Weakness — grip strength in the lowest 20 percent (adjusted for sex and body mass index), measured with a hand dynamometer.
- Slow walking speed — 15 feet (4.57 metres) in a time in the slowest 20 percent (adjusted for sex and standing height), typically corresponding to under 0.8 m/s.
- Low physical activity — measured by the Minnesota Leisure Time Activity questionnaire, in the lowest 20 percent (men under 383 kcal/week, women under 270 kcal/week). [1]
The classification:
- 0 criteria = robust (fit, no frailty).
- 1 to 2 criteria = pre-frail (an intermediate, potentially reversible state).
- 3 or more criteria = frail. [1]
The phenotype demonstrated, in the original study of over 5000 community-dwelling older adults, that frailty independently predicted incident falls, worsening mobility and ADL disability, hospitalisation, and death over 3 to 7 years of follow-up — after adjusting for comorbidity and disability. This was the key conceptual contribution: frailty is a distinct biological syndrome, not simply the sum of comorbidities or the endpoint of disability. [1]
Model 2 — the Rockwood cumulative deficit model
The cumulative deficit model, developed by Rockwood and Mitnitski (Rockwood and Mitnitski 2007, PMID 17634318), defines frailty as the proportion of accumulated health deficits — symptoms, signs, diseases, disabilities, and laboratory abnormalities — relative to the total number considered. [1]
The frailty index (FI) is calculated by taking a list of at least 30 to 40 health variables (the specific list can vary, provided the variables are associated with health status, increase with age, and do not saturate too early), counting the number present in the individual, and dividing by the total. For example, if 40 deficits are assessed and the patient has 12 present, the FI is 12/40 = 0.30. [1]
The classification:
- FI under 0.08 = fit.
- FI 0.08 to 0.25 = pre-frail (or vulnerable).
- FI over 0.25 = frail.
- FI over 0.7 is a theoretical ceiling — most people do not survive beyond this. [1]
The frailty index has remarkable mathematical properties: the distribution shifts rightward with age, the rate of deficit accumulation is approximately linear at about 3 percent per year, and there is a submaximal limit of about 0.7 beyond which survival is not observed. It predicts mortality, institutionalisation, and functional decline more strongly than chronological age or comorbidity alone. Its strength is that it can be derived from any comprehensive dataset — a CGA, a research database, or an electronic medical record — provided the variables meet the criteria. [1]
The relationship between the two models
The two models measure overlapping but not identical constructs. The Fried phenotype captures the physical and energetic dimension of frailty (weight loss, exhaustion, weakness, slowness, inactivity); the frailty index captures the cumulative burden of disease and deficit. A person can be physically frail by the Fried phenotype with a low deficit count (the "sarcopenic frail" pattern), or can have a high frailty index with few physical signs (the "multimorbid but compensated" pattern). Most older adults show both. For clinical use at the bedside, the Clinical Frailty Scale — derived from the frailty index tradition — is the practical tool. [1]
The Clinical Frailty Scale (CFS)

The Clinical Frailty Scale (Rockwood 2005, PMID 16129869) is a 9-point clinical judgement scale, scored after a brief clinical assessment (the kind a geriatrician performs in 5 to 10 minutes), that summarises the older person's overall fitness and frailty: [1]
| CFS | Label | Clinical description |
|---|---|---|
| 1 | Very fit | Robust, active, energetic, exercise regularly, fittest for age |
| 2 | Well | No active disease symptoms, less fit than category 1, active occasionally |
| 3 | Managing well | Medical problems well controlled, not regularly active beyond routine walking |
| 4 | Vulnerable | Not dependent on others but symptoms limit activities, "slowed up" |
| 5 | Mildly frail | Evident slowing, needs help with high-order IADLs (finances, transport, heavy housekeeping) |
| 6 | Moderately frail | Needs help with all outside activities and with keeping house, help with bathing and minor help with dressing |
| 7 | Severely frail | Completely dependent for personal care, stable, not at high risk of dying within 6 months |
| 8 | Very severely frail | Completely dependent, approaching end of life, could not recover from even minor illness |
| 9 | Terminally ill | Approaching end of life, life expectancy under 6 months without otherwise being evidently frail |
Classification: CFS 1 to 3 = fit; CFS 4 = vulnerable (pre-frail); CFS 5 to 8 = frail; CFS 9 = terminally ill (scored separately). [1]
The CFS predicts mortality, length of stay, institutionalisation, functional decline, and complication risk — including postoperative mortality and delirium — across hospital, surgical, and community settings. It takes under a minute to score, requires no equipment, and is the single highest-yield frailty instrument for routine clinical use. The CFS should be documented in every older patient's chart within 24 hours of hospital admission and is now embedded in the National Early Warning Score (NEWS2) escalation framework in the UK and in the ANZ perioperative and acute medicine pathways. [1]
DWE high-yield trap: The exam expects you to know the Clinical Frailty Scale categories and their prognostic implications. The key thresholds: CFS 5 or above is frail and predicts significantly worse outcomes after surgery, sepsis, and acute illness; CFS 7 to 8 is severe frailty and should trigger a goals-of-care conversation and a consideration of whether aggressive interventions are appropriate. [1]
Sarcopenia — the muscle substrate of frailty
Sarcopenia is the progressive and generalised loss of skeletal muscle mass, strength, and function. It is the muscle-level substrate of the frailty phenotype — the weakness, the slowness, and the low activity of the Fried criteria are largely a consequence of sarcopenia. The EWGSOP2 consensus (Cruz-Jentoft 2019, PMID 31081853) provides the current operational definition and diagnostic algorithm. [1]
The EWGSOP2 criteria: [1]
The EWGSOP2 definition makes muscle strength (measured by grip strength) the primary parameter — because strength declines earlier and faster than mass, and because strength is the stronger predictor of adverse outcomes. [1]
- Probable sarcopenia: low muscle strength (grip strength under 27 kg in men or under 16 kg in women, or a chair stand test of 15 seconds or more for five rises).
- Confirmed sarcopenia: low muscle strength PLUS low muscle quantity or quality (measured by DEXA appendicular skeletal muscle mass, or by bioimpedance, or by CT or MRI — the DEXA appendicular skeletal muscle mass index under 7.0 kg/m² in men or under 5.4 kg/m² in women is the standard threshold).
- Severe sarcopenia: low strength, low mass, AND low physical performance (gait speed under 0.8 m/s). [1]
Sarcopenia cutoff values: [1]
| Measurement | Men | Women |
|---|---|---|
| Grip strength (probable sarcopenia) | Under 27 kg | Under 16 kg |
| Chair stand (5 rises) | Over 15 seconds | Over 15 seconds |
| ASM mass index (DEXA, confirmed) | Under 7.0 kg/m² | Under 5.4 kg/m² |
| Gait speed (severe sarcopenia) | Under 0.8 m/s | Under 0.8 m/s |
The management of sarcopenia: [1]
- Progressive resistance exercise training — the single most effective intervention. Two to three sessions per week of progressive resistance training (8 to 12 repetitions at 70 to 80 percent of one-repetition maximum, targeting the major muscle groups) increases muscle mass, strength, and function in adults into their 90s. This is the evidence-based cornerstone.
- Dietary protein — 1.0 to 1.2 g/kg/day for healthy older adults, 1.2 to 1.5 g/kg/day for those with sarcopenia or acute illness, distributed across meals. Protein supplementation (20 to 30 g per meal) combined with resistance exercise has additive benefit.
- Vitamin D — supplementation (800 to 1000 IU daily) in deficient patients improves muscle function and reduces falls; the evidence is strongest in deficient older adults.
- Address contributing factors — inflammation, insulin resistance, malnutrition, bed rest, hospitalisation, and drugs (steroids, androgen deprivation). No pharmacological agent is yet approved for sarcopenia, though selective androgen receptor modulators and myostatin inhibitors are under investigation. [1]
Clinical rule: Sarcopenia is not the same as frailty, but they are tightly linked. A frail older patient almost always has sarcopenia. The assessment — grip strength, gait speed, chair stand — and the treatment — resistance exercise, protein, vitamin D — are the practical bridge between the two concepts. [1]
Nutrition screening — the MNA-SF
Malnutrition affects 15 percent of community-dwelling older adults, 30 to 50 percent of hospitalised older patients, and up to 70 percent of residential care residents. It drives frailty, sarcopenia, delayed wound healing, infection, prolonged length of stay, and mortality. The Mini Nutritional Assessment Short Form (MNA-SF) (Rubenstein 2001, PMID 11382797) is the recommended rapid nutrition screen. [1]
The MNA-SF has six items: [1]
- Food intake — has decreased over the past 3 months (0 = severe decrease, 1 = moderate, 2 = no decrease).
- Weight loss — over the past 3 months (0 = more than 3 kg, 1 = does not know, 2 = 1 to 3 kg, 3 = no weight loss).
- Mobility (0 = bed or chair bound, 1 = able to get out of bed but does not go out, 2 = goes out).
- Acute psychological stress or illness in the past 3 months (0 = yes, 2 = no).
- Neuropsychological problems (0 = severe dementia or depression, 1 = mild dementia, 2 = no problems).
- Body mass index (0 = under 19, 1 = 19 to under 21, 2 = 21 to under 23, 3 = 23 or more) — or, if BMI is not available, calf circumference (0 = under 31 cm, 3 = 31 cm or more). [1]
Scoring:
- 12 to 14 — normal nutritional status.
- 8 to 11 — at risk of malnutrition — intervene with dietary counselling, fortified food, oral nutritional supplements.
- 0 to 7 — malnourished — full nutritional assessment and treatment, dietitian referral, consider oral nutritional supplements and appetite stimulants. [1]
The MNA-SF takes under 5 minutes, requires no blood tests, and is the standard nutrition screen in the CGA. A low score should prompt a full nutritional assessment, measurement of body weight and height, and a dietitian review. [1]
The evidence — CGA improves outcomes
The evidence that CGA works is the foundation of the entire field and is the most frequently examined fact in this topic. The 2017 Cochrane systematic review (Ellis 2017, PMID 28898390) pooled 29 randomised trials with over 13,000 participants and found that older adults admitted to hospital who received CGA (compared to usual care) were: [1]
- More likely to be alive and in their own homes at 3 to 12 months follow-up — odds ratio 1.22 (95% CI 1.05 to 1.43). This is the headline result: CGA increases the chance of being alive and independent at home.
- Less likely to be living in a residential care or nursing home — odds ratio 0.78 (95% CI 0.64 to 0.96). CGA reduces institutionalisation.
- Less likely to die during follow-up — the mortality reduction approached but did not reach significance across all studies, but was significant in the higher-quality trials.
- More likely to experience improved cognition — a secondary outcome that supports the multidimensional benefit. [1]
The critical caveat — the model matters. The Cochrane review distinguished between two CGA models:
- CGA delivered on a dedicated geriatric evaluation and management (GEM) unit or ward — where the geriatric team controls the admission and the care plan — showed consistent and significant benefits (alive at home, reduced mortality, reduced institutionalisation).
- CGA delivered by a consultation team — where a geriatric team advises the primary treating team but does not control the care — showed no significant benefit. [1]
The clinical and exam point: CGA works when it is delivered in a model where the geriatric team has control of the care — the dedicated GEM ward, the orthogeriatric service, the geriatric outpatient clinic with direct follow-up. A consult that is filed and ignored is not CGA. [1]
CGA delivery models
| Model | Setting | Evidence | Key feature |
|---|---|---|---|
| Inpatient GEM unit | Acute or subacute ward | Strongest evidence — reduced mortality, institutionalisation, improved function | Geriatric team controls admission and care plan |
| Inpatient consultation team | Acute ward | Weaker evidence — no consistent benefit | Advice given to primary team, no control of care |
| Outpatient CGA clinic | Community | Moderate evidence — improved function, reduced hospitalisation, benefits depend on follow-up | Direct, ongoing geriatric follow-up |
| Orthogeriatrics / perioperative | Surgical ward | Strong evidence (hip fracture) — reduced mortality, length of stay, complications, improved return to function | Geriatrician co-manages surgical patients |
| Hospital at home / acute CGA at home | Community | Emerging evidence — non-inferior to inpatient for selected patients | Avoids hospital-acquired deconditioning |
Orthogeriatrics deserves special mention as the exam-favourite model. The hip fracture population is overwhelmingly frail and elderly, and the orthogeriatric model — co-management by orthopaedic surgery and geriatric medicine, with rapid comprehensive assessment, early surgery, early mobilisation, and structured rehabilitation — has demonstrated reduced 30-day and 1-year mortality, reduced length of stay, reduced complications (delirium, pressure injuries, pneumonia, venous thromboembolism), and improved return to independent mobility. Every patient over 65 with a fragility fracture should receive a CGA and be managed under an orthogeriatric model; this is now the standard of care in ANZ, the UK, and most of the developed world. [1]
The CGA process — how to do it
The CGA is a structured process with five steps: [1]
Step 1 — Screening and referral. Identify the frail older person who will benefit. The trigger is any of: age over 75, a recent fall or fragility fracture, functional decline (new difficulty with ADLs or IADLs), polypharmacy, cognitive decline, unplanned hospital admission, or a CFS of 5 or above. In the acute setting, the CFS on admission is the trigger. [1]
Step 2 — The multidimensional assessment. A structured assessment across the four domains, using the validated instruments. This is typically performed over one or more sessions by the geriatrician, the specialist nurse, the physiotherapist (gait, balance, strength, falls risk), the occupational therapist (ADL and IADL performance, home safety), the social worker (social support, finances, services), the pharmacist (medication review, deprescribing), and the dietitian (nutrition assessment). Each contributes a structured report. [1]
Step 3 — The interdisciplinary team meeting. The team meets, synthesises the findings into a single prioritised problem list, and develops a coordinated and integrated management plan with shared goals and allocated responsibilities. This is the step that makes the process "comprehensive" — without the team meeting, it is a collection of individual assessments. [1]
Step 4 — Implementation. The plan is delivered — medication changes, rehabilitation, exercise programme, home modifications, community services, carer support, advance care planning, follow-up appointments. The plan is communicated to the patient, the family, the general practitioner, and the community team. [1]
Step 5 — Follow-up and reassessment. The CGA is not a one-off event. The plan is reviewed at intervals, the functional and cognitive measures are repeated, and the plan is adjusted as needs change. The Cochrane evidence shows that the benefit depends on ongoing follow-up, not on a single assessment. [1]
Clinical rule: The single most important determinant of whether a CGA changes outcomes is whether the geriatric team has control of the care plan and provides ongoing follow-up. A consultative assessment that is filed and ignored does not work — the Cochrane review is explicit on this. The exam expects you to know that the GEM ward model (team control) outperforms the consult model (advice only). [1]
The CGA in the long case — the integrated plan
In the DCE long case, the frail older patient with multiple comorbidities is the archetypal scenario, and the CGA is the framework for the integrated management plan. The structure: [1]
1. The opening statement (SASPOP) — Symptoms, Age, Sex, Presentation, Occupation, Problems. Lead with the patient as a person, then the problem list. [1]
2. The problem list — numbered, prioritised, with each problem's specific assessment and plan. The CGA structure ensures you do not miss a domain. A typical frail long case might have: [1]
- Frailty (CFS 6, with sarcopenia, recent functional decline).
- Falls (two falls in 6 months, one with a wrist fracture; TUG 18 seconds, orthostatic hypotension).
- Polypharmacy (12 regular medications, high anticholinergic burden, two potentially inappropriate).
- Cognitive impairment (MoCA 21, likely mild cognitive impairment or early dementia).
- Depression (GDS-15 score 7).
- Malnutrition (MNA-SF score 9, weight loss 4 kg in 3 months).
- Sensory impairment (uncorrected hearing loss, missing hearing aid).
- Social — lives alone, daughter visits weekly, at risk of institutionalisation, no advance care directive. [1]
3. The integrated plan — addresses each problem, but also identifies the interactions and the shared goals. The plan is not eight separate treatments — it is a coordinated package: a medication review that reduces falls risk and improves cognition; a resistance exercise and nutrition programme that addresses frailty, sarcopenia, falls, and mood; a community package that supports function and reduces carer strain; and an advance care planning conversation that respects the patient's values. [1]
4. The insight and communication — the examiner wants to see that you understand the patient's perspective, that you can prioritise the problems in order of urgency and importance, and that you can communicate the plan to the patient and the family with empathy and realism. [1]
The CGA in the short case — the functional assessment
The DCE short case on geriatric medicine frequently asks for a focused functional assessment — the gait, the ADLs, and the physical performance. The systematic routine: [1]
1. Observe the patient — posture, muscle bulk (temporal wasting and thenar wasting suggest sarcopenia), gait initiation, turn, and stability. Watch the patient walk to and from the chair — the gait is the most informative single observation. [1]
2. The Timed Up and Go test — explain, demonstrate, time. A TUG over 12 seconds is abnormal and indicates increased falls risk. [1]
3. The gait speed — time over 4 metres. Under 0.8 m/s is abnormal and predicts adverse outcomes. [1]
4. The grip strength — if a dynamometer is available, measure both hands. Under 27 kg (men) or 16 kg (women) suggests probable sarcopenia. [1]
5. The chair stand test — time five rises from a chair without using the arms. Over 15 seconds suggests lower extremity weakness. [1]
6. The functional inquiry — ask explicitly about each ADL (bathing, dressing, toileting, transferring, continence, feeding) and each IADL (telephone, shopping, cooking, housekeeping, laundry, transport, medications, finances). Document the Katz and Lawton scores. [1]
7. The falls and continence inquiry — falls in the past year, injuries, frequency, urinary and faecal continence. [1]
8. The cognitive and mood screen — a brief MoCA or a clock-drawing test, and a mood question, if time permits. [1]
The presentation template: [1]
"This 82-year-old woman has a slow, cautious gait with a widened base and reduced stride length. Her Timed Up and Go is 16 seconds (abnormal, over 12 seconds), her gait speed over 4 metres is 0.6 m/s (abnormal, under 0.8 m/s), and her grip strength is 14 kg in the dominant hand (low, below the 16 kg threshold for women, suggesting probable sarcopenia). She is independent in basic ADLs (Katz 5 out of 6 — she needs assistance with bathing) but has lost independence in two IADLs (transport and finances, Lawton 6 out of 8). She has fallen twice in the past 6 months. The pattern is of mild to moderate frailty, with sarcopenia and early functional decline, and a significantly increased falls risk. Her Clinical Frailty Scale score is 5 (mildly frail). My plan is a structured falls assessment, a resistance exercise and protein supplementation programme, a medication review, and a home safety assessment." [1]
How this is examined
DWE MCQ
The DWE tests CGA and frailty through clinical vignettes and knowledge questions that probe: [1]
- The definition of CGA — the three elements (multidimensional, interdisciplinary, therapeutic) and the four domains.
- The frailty models — the Fried phenotype (the five criteria, the 3-or-more threshold), the frailty index (the deficit ratio, the 0.25 threshold), and the Clinical Frailty Scale (the 9 points, the prognostic implications).
- The functional instruments — the Katz ADL (the six activities, the 0 to 6 score), the Lawton IADL (the eight activities), the Timed Up and Go (the 12-second threshold), and gait speed (the 0.8 m/s threshold).
- The EWGSOP2 sarcopenia criteria — low strength (under 27 kg men, under 16 kg women) plus low mass, with the severe category adding low gait speed.
- The CGA evidence — the Cochrane meta-analysis result (alive at home, reduced institutionalisation), and the model distinction (GEM ward works, consultation does not).
- The MNA-SF — the screening tool, the cutoffs, the management. [1]
DCE long case
The long case is the archetypal frail older patient with multiple comorbidities — falls, cognitive impairment, polypharmacy, malnutrition, functional decline, carer strain, and a question of goals of care. You will be expected to present a structured CGA (the four domains), a prioritised problem list, an integrated management plan, and a thoughtful discussion of advance care planning. The CGA framework is the structure that earns the marks. [1]
DCE short case
The short case will ask for a functional assessment — gait, physical performance, ADLs, IADLs, falls risk. You will be expected to perform the Timed Up and Go, to observe and interpret the gait, to score the Katz and Lawton, to assess grip strength and gait speed if available, and to present the findings with a Clinical Frailty Scale score and a management plan. [1]
Key references
Fried LP, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001;56:M146-M156 (PMID 11253156). Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci 2007;62:722-727 (PMID 17634318). Rockwood K, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005;173:489-495 (PMID 16129869). Ellis G, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev 2017;CD006211 (PMID 28898390). Cruz-Jentoft AJ, et al. Sarcopenia: revised European consensus on definition and diagnosis (EWGSOP2). Age Ageing 2019;48:16-31 (PMID 31081853). Katz S, et al. The index of ADL: a standardized measure of biological and psychosocial function. JAMA 1963;185:914-919 (PMID 14044222). Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 1969;9:179-186 (PMID 5349366). Rubenstein LZ, et al. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol A Biol Sci Med Sci 2001;56:M366-M372 (PMID 11382797). Bellelli G, et al. Validation of the 4AT, a new instrument for rapid delirium screening. Age Ageing 2014;43:496-502 (PMID 24590568). Nasreddine ZS, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-699 (PMID 15817019). Guideline sources: ANZSGM Position Statement on CGA, NICE NG97 (cognitive domain), BGS CGA Toolkit, Dalhousie Clinical Frailty Scale. [1]
References
- [1]Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype J Gerontol A Biol Sci Med Sci, 2001.PMID 11253156
- [2]Rockwood K, Mitnitski A Frailty in relation to the accumulation of deficits J Gerontol A Biol Sci Med Sci, 2007.PMID 17634318
- [3]Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people CMAJ, 2005.PMID 16129869
- [4]Ellis G, Gardner M, Tsiachristas A, et al. Comprehensive geriatric assessment for older adults admitted to hospital Cochrane Database Syst Rev, 2017.PMID 28898390
- [5]Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis Age Ageing, 2019.PMID 31081853
- [6]Katz S, Ford AB, Moskowitz RW, et al. STUDIES OF ILLNESS IN THE AGED. THE INDEX OF ADL: A STANDARDIZED MEASURE OF BIOLOGICAL AND PSYCHOSOCIAL FUNCTION JAMA, 1963.PMID 14044222
- [7]Lawton MP, Brody EM Assessment of older people: self-maintaining and instrumental activities of daily living Gerontologist, 1969.PMID 5349366
- [8]Rubenstein LZ, Harker JO, Salva A, et al. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF) J Gerontol A Biol Sci Med Sci, 2001.PMID 11382797
- [9]Bellelli G, Morandi A, Davis DHJ, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people Age Ageing, 2014.PMID 24590568
- [10]Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019