Phys · geriatric
Delirium
Also known as acute confusional state · acute brain failure · acute cognitive decline · postoperative delirium · ICU delirium · hypoactive delirium · hyperactive delirium · terminal delirium · CAM · Confusion Assessment Method · HELP · Hospital Elder Life Program
Consultant-physician-depth guide to delirium for FRACP DWE and DCE — DSM-5 definition, the Confusion Assessment Method, hyperactive versus hypoactive subtypes, neuroinflammatory and cholinergic pathophysiology, the DELIRIUM mnemonic for precipitants, HELP prevention, multicomponent non-pharmacological management, the narrow role of haloperidol, and the differentiation from dementia and depression.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Delirium
The answer first
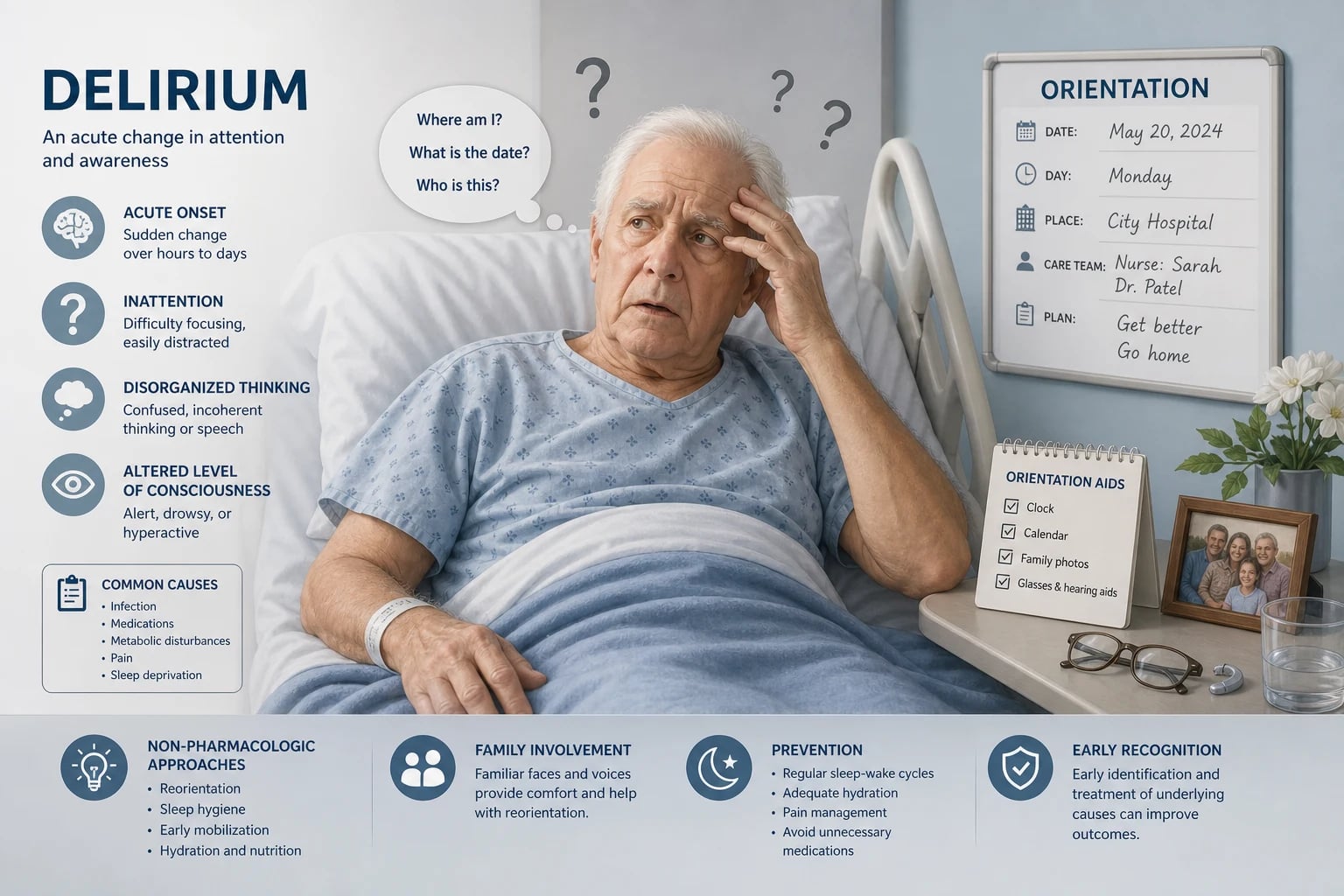
Delirium is an acute, fluctuating disturbance of attention and awareness caused by a medical condition, drug, or withdrawal — it is the behavioural signature of acute brain dysfunction in a medically ill patient. It is the single most common acute neuropsychiatric complication of hospitalisation in older adults, and it is under-recognised in roughly half of cases. [1]
The three rules that determine everything in delirium are: [1]
- Acute confusion is delirium until proven otherwise. Never attribute new confusion to dementia without documenting an acute change from baseline. Dementia is chronic; delirium is acute. The single most useful piece of information is a collateral history from someone who knows the patient's baseline cognition.
- Delirium is multifactorial — search for and treat every precipitant. The patient does not have "a" cause; they usually have several. Infection plus dehydration plus an anticholinergic drug plus urinary retention is a common cluster. The DELIRIUM mnemonic (below) is the structured search.
- The management is non-pharmacological and cause-directed — drugs come last, only for severe distress or danger. The most common management error is reaching for haloperidol before addressing the infection, the dehydration, the pain, the constipation, the drugs, and the environment. [1]
DWE high-yield trap: When asked "best initial management of delirium," the answer is almost always identify and treat the underlying cause with multicomponent non-pharmacological measures — not haloperidol. Haloperidol is reserved for severe agitation with risk to the patient or others, at the lowest effective dose, and must never be given to a patient with Parkinson disease or dementia with Lewy bodies. [1]
Definition — DSM-5
The DSM-5 defines delirium with five criteria. The diagnosis requires all of the core clinical features: [1]
- Disturbance in attention and awareness — reduced ability to direct, focus, sustain, and shift attention. This is the cardinal feature. Attention is tested at the bedside with months of the year backwards, serial sevens, or digit span.
- The disturbance develops over a short period of time (usually hours to a few days), represents an acute change from baseline, and tends to fluctuate in severity during the course of the day. The fluctuation is a key discriminator from dementia — a patient who is lucid in the morning and confused at night has delirium until proven otherwise.
- An additional disturbance in cognition — memory deficit, disorientation, language, visuospatial ability, or perception (hallucinations, illusions).
- The disturbances are not better explained by a pre-existing, established, or evolving neurocognitive disorder (dementia) and do not occur in the context of a severely reduced level of consciousness such as coma. This criterion recognises that delirium can superimpose on dementia, but the acute change itself is not explained by the dementia.
- There is evidence from the history, physical examination, or laboratory findings that the disturbance is a direct physiological consequence of another medical condition, substance intoxication or withdrawal, or exposure to a toxin, or is due to multiple aetiologies. [1]
The key clinical takeaways from the definition: attention is the core domain (not memory — that distinguishes delirium from dementia), onset is acute (hours to days, not months), and the course fluctuates (a red flag for delirium whenever the confusion waxes and wanes). [1]
Exam trap: A common MCQ asks "which feature most distinguishes delirium from dementia" — the answer is acute onset with fluctuating course and impaired attention. A patient with dementia alone has gradual onset, a stable (though declining) course day to day, and relatively preserved attention until late. [1]
The Confusion Assessment Method (CAM)
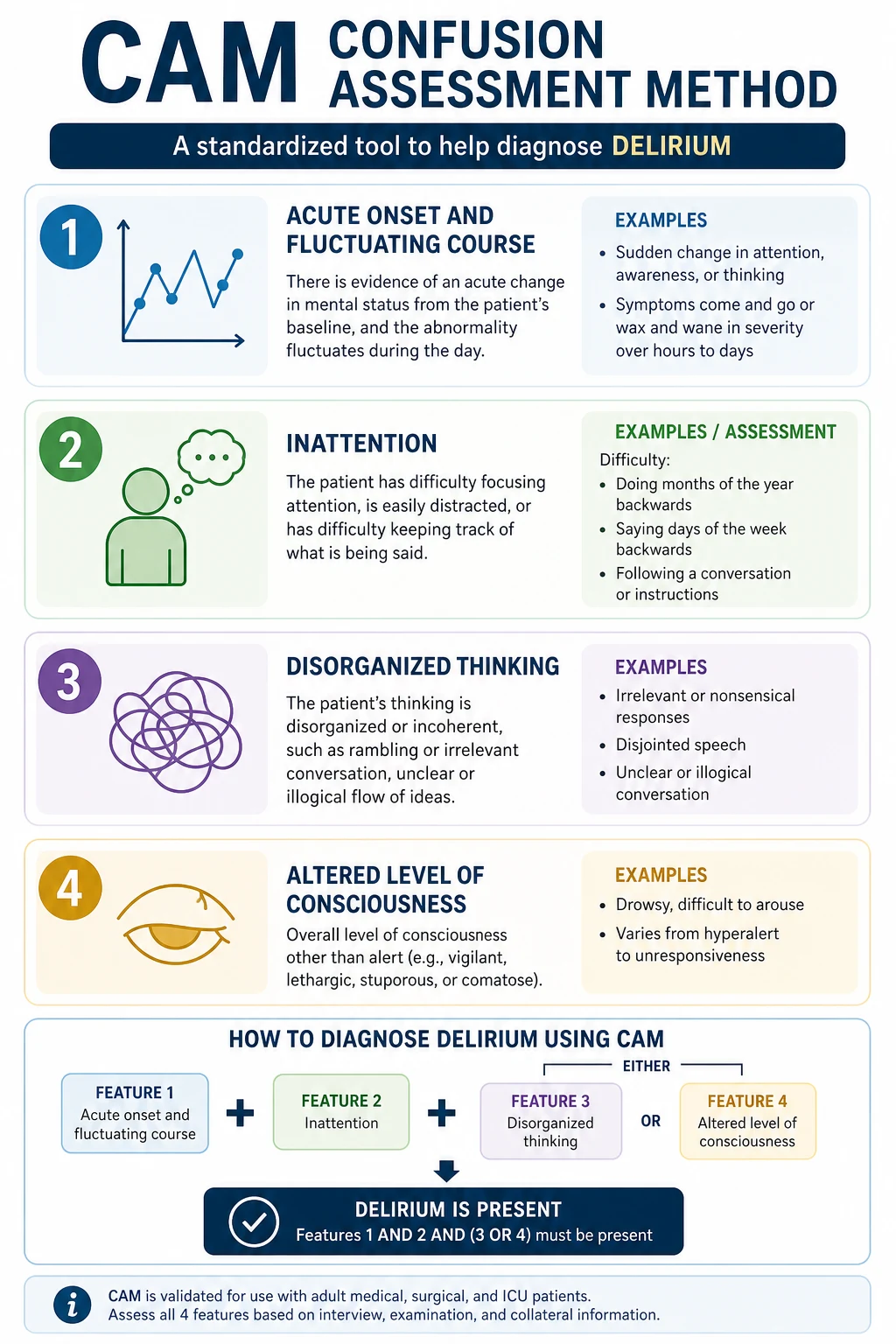
The CAM (Inouye 1990, PMID 2240918) is the most widely validated and used bedside diagnostic instrument for delirium. It has a sensitivity of 94 percent and specificity of 89 percent in the original validation study when administered by trained clinicians. It does not diagnose the cause — it diagnoses the syndrome. [1]
The four features
| Feature | Description | How to assess |
|---|---|---|
| 1. Acute onset and fluctuating course | Information from family or nursing staff that the patient's mental state is acutely changed from baseline AND fluctuates during the day | Ask: "Is the patient acutely confused compared to before? Does it come and go during the day?" Collateral history is essential |
| 2. Inattention | Difficulty focusing attention, easily distracted, difficulty keeping track of what is being said | Ask the patient to recite the months of the year backwards (December, November, October...) — this is the most sensitive bedside test. Errors or losing the thread indicate inattention. Serial sevens or digit span backwards are alternatives |
| 3. Disorganised thinking | Rambling, irrelevant conversation, unclear or illogical flow of ideas, unpredictable switching from subject to subject | Ask a few open questions: "Tell me about your day." "What brought you to hospital?" Listen for disordered, incoherent, or illogical thinking |
| 4. Altered level of consciousness | Anything other than alert — vigilant (hyperalert), lethargic (drowsy but rousable), stuporose, or comatose | Observe the patient. The Richmond Agitation-Sedation Scale (RASS) or the Glasgow Coma Scale eye-opening component formalises this |
The diagnostic rule
The diagnosis of delirium by CAM requires: [1]
Feature 1 AND Feature 2 PLUS either Feature 3 OR Feature 4. [1]
In plain language: acute fluctuating onset with inattention, plus either disorganised thinking or altered consciousness. Features 1 and 2 are mandatory; 3 and 4 are alternative — either one suffices. [1]
DCE short-case trap: The most common error when using CAM at the bedside is to diagnose delirium on the basis of confusion alone without explicitly demonstrating inattention (feature 2). Always test attention formally — months of the year backwards — and document it. Without feature 2, the diagnosis is not CAM-delirium. [1]
The 4AT — a rapid alternative
The 4AT (Shenkin 2014, PMID 24590568) is a validated 2-minute screening tool increasingly used in UK and Australian hospitals because it requires no training and is administered by any clinician. It scores four components: [1]
- Alertness (0 = normal, 4 = clearly abnormal)
- AMT4 — Abbreviated Mental Test-4: age, date of birth, place, current year (0 if all correct, 1 if any error, 3 if untestable)
- Attention — months of the year backwards (0 = achieved, 2 if starts but cannot complete, 4 if cannot start)
- Acute change or fluctuating course (0 = no, 4 = yes) [1]
A score of 4 or more indicates possible delirium. A score of 1 to 3 suggests possible cognitive impairment and warrants fuller assessment. The 4AT is well-suited to routine ward screening on admission and at 72 hours. [1]
Clinical subtypes
Delirium presents in three motoric subtypes, defined by the patient's level of psychomotor activity: [1]
Hyperactive delirium
The patient is agitated, restless, hypervigilant, hallucinating, often pulling at lines, climbing out of bed, shouting. This is the classic, easily recognised "delirious" patient — and the one who is over-treated with sedatives. Hyperactive delirium is associated with alcohol or drug withdrawal, but can occur in any cause. It carries a better prognosis than hypoactive. [1]
Hypoactive delirium
The patient is quiet, lethargic, withdrawn, slow to respond, drowsy, sleeping most of the time, with reduced motor activity. This is the most commonly missed subtype — it looks like "the patient is just tired" or "just old" or "depressed." It is the most dangerous subtype: it carries the worst prognosis, the highest mortality, and the longest recovery, partly because it is missed and untreated, and partly because it reflects more severe underlying illness and cerebral dysfunction. [1]
The clue to hypoactive delirium is a patient who is less responsive than their baseline, who is newly drowsy or withdrawn, or who fails to improve mentally as expected after an acute illness. Any older inpatient who becomes quiet should be assessed with the CAM or 4AT. [1]
Mixed delirium
The patient fluctuates between hyperactive and hypoactive states — agitated at times, somnolent at others. This is the most common subtype overall. The fluctuation itself is a diagnostic clue. [1]
DWE high-yield: The question "a 78-year-old woman on day 4 of admission for pneumonia is noted by the nurses to be drowsy and not eating, previously independent and alert" — the answer is hypoactive delirium, not depression or dementia. The acute onset and reduced level of consciousness are the keys. [1]
Pathophysiology
Delirium is a syndrome, not a disease — there is no single mechanism. The current understanding integrates several interacting hypotheses. Why this matters clinically: it explains why dementia is the strongest risk factor (vulnerable brain), why infection and surgery precipitate it (inflammation), why anticholinergic drugs cause it (cholinergic deficit), and why antipsychotics are a symptomatic tool, not a cure (they do not address the inflammation or the cause). [1]
The neuroinflammatory hypothesis
Systemic inflammation — from infection (pneumonia, urinary tract, bacteraemia), surgery (especially cardiac and orthopaedic), trauma, or pancreatitis — triggers release of pro-inflammatory cytokines (interleukin-1, interleukin-6, tumour necrosis factor alpha). These cytokines signal to the brain via three pathways: direct crossing of a disrupted blood-brain barrier, active transport across the barrier, and signalling through the vagus nerve and circumventricular organs. [1]
Within the brain, the cytokines activate microglia, the resident immune cells. Activated microglia release further inflammatory mediators, causing neuronal dysfunction, synaptic impairment, and altered neurotransmission. This model explains the clinical observation that the severity of the systemic insult correlates with the risk and severity of delirium, and that patients with pre-existing brain disease (dementia, stroke) are more susceptible — their microglia are already primed (the "two-hit" model: a primed brain plus an inflammatory insult). [1]
The cholinergic deficiency hypothesis
Acetylcholine is the neurotransmitter critical for attention, arousal, and cortical processing — exactly the domains impaired in delirium. A cholinergic deficit is central to the syndrome. The evidence: [1]
- Anticholinergic drugs precipitate delirium — oxybutynin, tricyclics, hyoscine, amitriptyline, cyclizine, chlorphenamine, codeine, and many others with antimuscarinic activity. The cumulative anticholinergic burden is a measurable, dose-dependent risk.
- Older adults have reduced cholinergic reserve due to age-related neuronal loss, which is one reason age is a risk factor.
- Acetylcholine falls during acute illness and surgery due to reduced synthesis and increased degradation.
- Cholinesterase inhibitors (donepezil, rivastigmine) have been studied for delirium prevention and treatment with mixed results — not recommended routinely, but the rationale is mechanistically sound. [1]
The practical implication: every delirium assessment must include an anticholinergic burden review, and removing anticholinergic drugs is a therapeutic act. [1]
The dopaminergic excess hypothesis
Dopaminergic excess contributes to delirium, particularly the hallucinations, agitation, and psychotic features. This explains: [1]
- Antipsychotics (dopamine antagonists) reduce the agitation and psychosis of delirium — they work symptomatically by blocking D2 receptors.
- Parkinson disease and dementia with Lewy bodies involve dopaminergic deficit (the opposite imbalance), so giving a dopamine antagonist (haloperidol) causes catastrophic worsening — neuroleptic sensitivity.
- Dopamine withdrawal (suddenly stopping levodopa in a Parkinson patient) can precipitate delirium and a neuroleptic-malignant-like syndrome. [1]
The cognitive reserve model
Delirium occurs when the precipitant burden exceeds the brain's reserve. A patient with high cognitive reserve (younger, no dementia, no prior stroke, high education) can tolerate a major insult without delirium; a patient with low reserve (dementia, prior stroke, frailty) develops delirium from a minor insult. This is the "threshold" model: dementia is the single strongest risk factor because it dramatically lowers the threshold. This is also why delirium and dementia are so often superimposed — and why distinguishing them is so difficult (and so important). [1]
Risk factors — predisposing and precipitating
The classic model (Inouye 2006, PMID 16540616; Inouye 2014, PMID 23992774) divides risk factors into predisposing (the vulnerable brain, present before the admission) and precipitating (the acute insult that tips the patient over threshold). Delirium occurs when the combination exceeds the threshold. A highly vulnerable patient (severe dementia) needs only a small precipitant (constipation); a robust patient needs a major insult (severe sepsis, cardiac arrest). [1]
Predisposing factors (the vulnerable patient)
| Factor | Why it matters |
|---|---|
| Older age (over 65, rising steeply over 80) | Reduced cholinergic reserve, reduced cognitive reserve, comorbidity |
| Dementia or cognitive impairment | The single strongest risk factor — 5- to 9-fold increased risk |
| Previous delirium | Indicates a vulnerable brain; high recurrence rate |
| Functional dependence and frailty | Marker of physiological reserve loss |
| Sensory impairment (poor vision, hearing loss) | Reduces environmental input, worsens disorientation |
| Multiple comorbidities (stroke, heart failure, CKD, diabetes) | Each reduces reserve |
| Polypharmacy, especially anticholinergic or psychoactive | Direct neurotoxicity |
| Depression | Reduces reserve, complicates presentation |
| Male sex, dehydration, malnutrition | Identified in multiple risk models |
Precipitating factors (the acute insult)
These are the triggers — and are the target of the search and of prevention. The DELIRIUM mnemonic (below) organises them. The most common in hospitalised older adults are infection (urinary tract, pneumonia), medications (especially newly added anticholinergics, opioids, benzodiazepines), surgery (especially hip fracture and cardiac), metabolic disturbance (hyponatraemia, hypoglycaemia, uraemia, hypoxia), dehydration, and uncontrolled pain or urinary retention. [1]
A critical insight: the precipitants cluster. A postoperative hip fracture patient may have surgery (precipitant) plus opioids for pain (precipitant) plus urinary retention from immobility (precipitant) plus constipation (precipitant) plus an anticholinergic drug given for nausea (precipitant) — five precipitants in one patient. The management must address all of them. [1]
Causes — the DELIRIUM mnemonic
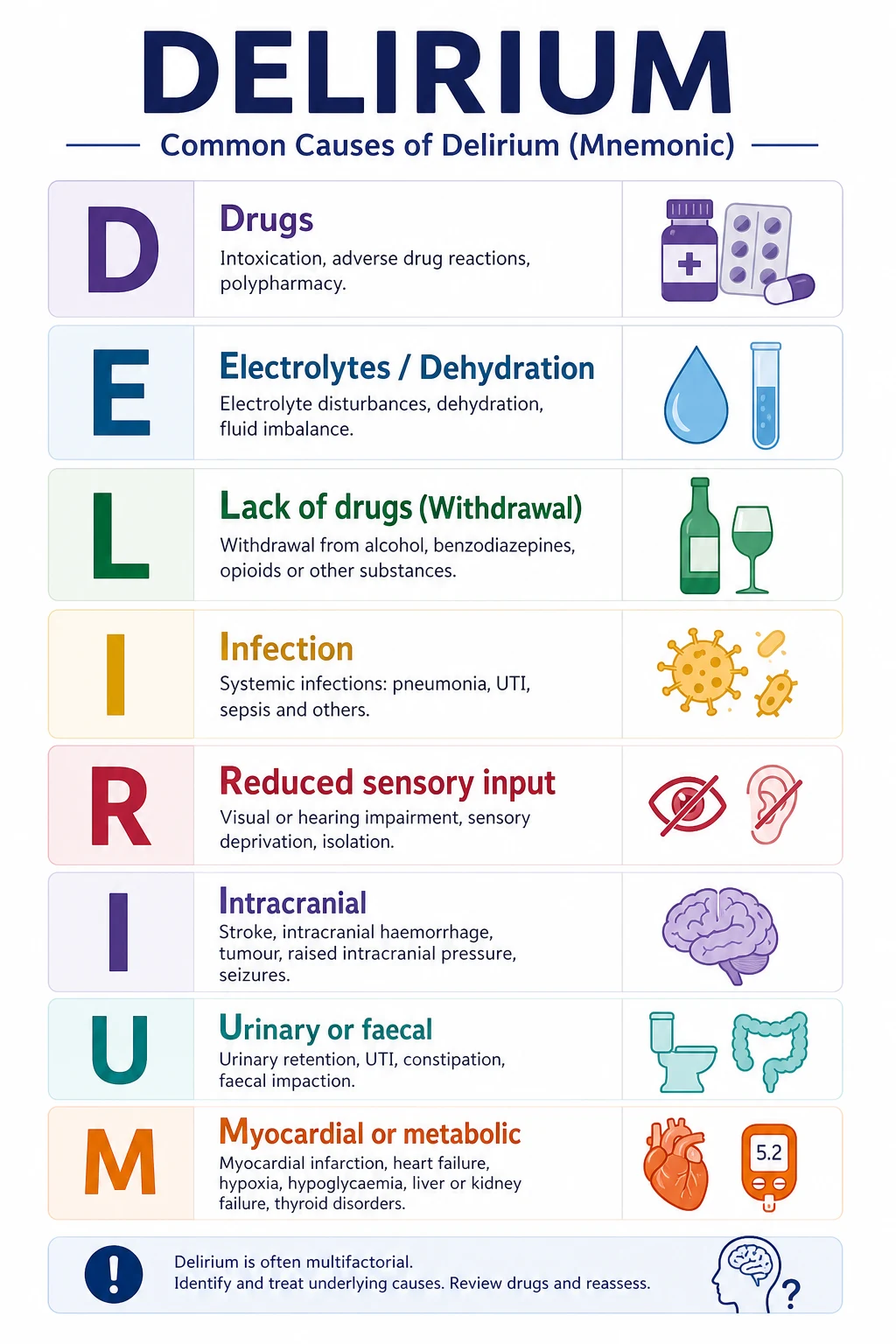
The DELIRIUM mnemonic is a structured, exhaustive framework for the cause search. It is the framework a registrar should run through at the bedside of every delirious patient. Memorise it. [1]
| Letter | Category | Specific causes to search for |
|---|---|---|
| D | Drugs | Anticholinergics (oxybutynin, tricyclics, antihistamines), benzodiazepines, opioids (especially morphine, tramadol), corticosteroids, anticonvulsants, antiparkinsonian drugs, digoxin toxicity, lithium toxicity, withdrawal of chronic benzodiazepine or alcohol |
| E | Electrolyte disturbance and dehydration | Hyponatraemia (the most common electrolyte cause), hypernatraemia, hypoglycaemia and hyperglycaemia, hypercalcaemia, uraemia, hepatic encephalopathy, dehydration (often iatrogenic from poor oral intake or diuretics) |
| L | Lack of drugs (withdrawal) | Alcohol withdrawal (delirium tremens), benzodiazepine withdrawal, opiate withdrawal — these require specific treatment with the withdrawn drug class, not antipsychotics |
| I | Infection | Urinary tract infection, pneumonia, cellulitis, bacteraemia, sepsis, intra-abdominal infection (cholecystitis, diverticulitis), meningitis, encephalitis, COVID-19 — the single most common precipitant in hospitalised older adults |
| R | Reduced sensory input | Missing glasses, missing hearing aids, unfamiliar environment, poor lighting, no clock, no window — the hospital environment itself precipitates and perpetuates delirium |
| I | Intracranial / CNS | Stroke (especially right hemisphere and parietal), intracranial haemorrhage (subdural from a fall, intracerebral), subarachnoid haemorrhage, meningitis, encephalitis, seizure (postictal state), non-convulsive status epilepticus, raised intracranial pressure, brain metastases |
| U | Urinary and faecal | Urinary retention (often from anticholinergics or immobility), faecal impaction (constipation from opioids and immobility) — both common, both easily missed, both treatable |
| M | Myocardial and metabolic | Myocardial infarction (especially silent in diabetics and older adults), cardiac failure, arrhythmia (especially atrial fibrillation), hypoxia (from any cause), hypothermia, hyperthermia, thyroid dysfunction (myxoedema madness, thyrotoxicosis), vitamin deficiencies (B1 thiamine in Wernicke, B12, folate), hypoperfusion from any cause |
Clinical rule: Every delirious patient gets a review of this mnemonic. The commonest missed precipitants are urinary retention, constipation, pain, anticholinergic drugs, and occult infection (especially when the fever is blunted in older adults). Do not stop the search at the first cause found — find and treat all of them. [1]
Prevention — the Hospital Elder Life Program (HELP)
Prevention is the most effective strategy for delirium, because treatment of established delirium is unsatisfying. The Hospital Elder Life Program (HELP), developed by Inouye and validated in a landmark randomised trial (PMID 10053175), is the evidence-based multicomponent prevention programme. It reduced delirium incidence from 15.0 percent to 9.9 percent in the original trial, and has been replicated in multiple settings. [1]
HELP targets the six modifiable risk factors for delirium during hospitalisation: [1]
| Risk factor | HELP intervention |
|---|---|
| Orientation and therapeutic environment | Orientation boards, clocks, calendars, frequent reorientation by staff and volunteers, familiar objects from home, a window view |
| Dehydration | Early recognition and oral hydration support, assistance with drinking, fluid charts |
| Sleep deprivation | Sleep hygiene — minimise night-time disruptions (cluster nursing tasks, avoid routine vital signs at night if stable, reduce noise and light), non-pharmacological sleep aids (warm drink, relaxation) rather than sedatives |
| Immobility | Early and frequent mobilisation, ambulation protocols, minimise bed rest, remove catheters and lines that tether the patient |
| Visual impairment | Provide and ensure the patient wears their glasses; magnifiers and large-print material |
| Hearing impairment | Provide and ensure the patient wears hearing aids; portable amplifiers, hearing assist devices; clear communication facing the patient |
The programme uses trained volunteers (often retired community members) to deliver the interventions, supervised by an elder life nurse specialist. It is low-cost, evidence-based, and has been adopted in modified forms worldwide. The principle generalisable to every ward: every older inpatient should have their orientation, hydration, sleep, mobility, vision and hearing actively addressed every day — these are not optional comforts, they are delirium prevention. [1]
Additional preventive measures supported by evidence: [1]
- Medication review — avoid new anticholinergics, benzodiazepines and opioids where possible; reduce polypharmacy.
- Pain control — uncontrolled pain precipitates delirium; paradoxically, adequate analgesia (including regional blocks for hip fracture) reduces delirium.
- Preoperative optimisation — in elective and urgent surgery, address dehydration, anaemia, and polypharmacy first.
- Family involvement — a family member or carer at the bedside reorients and calms the patient. [1]
Investigations
The investigation of delirium is directed at finding the precipitant(s). There is no single "delirium blood test" — the workup is the cause workup. [1]
First-line investigations (every delirious patient)
| Test | What you are looking for |
|---|---|
| Full blood count | Infection (leucocytosis, neutrophilia), anaemia (a contributor, rarely the sole cause), severe anaemia with hypoperfusion |
| Urea, electrolytes, creatinine | Dehydration (elevated urea, creatinine), hyponatraemia (the commonest electrolyte delirium cause), hypernatraemia, uraemia |
| Glucose | Hypoglycaemia and hyperglycaemia (including HHS) |
| Calcium | Hypercalcaemia (malignancy, hyperparathyroidism), hypocalcaemia |
| Liver function tests | Hepatic encephalopathy (low albumin, elevated bilirubin, prolonged INR), biliary sepsis |
| Thyroid function | Thyrotoxicosis, myxoedema (both can cause delirium) |
| C-reactive protein | Infection, inflammation |
| Urinalysis and urine culture | Urinary tract infection — the single most common infection precipitant. Caution: asymptomatic bacteriuria is common in older adults and in catheterised patients; a positive culture alone does not prove the UTI is the cause. Clinical correlation (symptoms, pyuria, other source excluded) is essential |
| Blood cultures (if febrile or unwell) | Bacteraemia, sepsis |
| Chest X-ray | Pneumonia, heart failure |
| ECG | Silent myocardial infarction (common in older diabetics), arrhythmia |
| Drug levels where indicated | Digoxin, lithium, anticonvulsants — if the patient is on these |
| Arterial or venous blood gas | Hypoxia, hypercapnia, acid-base disturbance — especially if respiratory compromise or sepsis |
Second-line investigations (when first-line is unrevealing or clinically indicated)
| Test | Indication |
|---|---|
| CT brain (non-contrast) | Focal neurological signs, new headache, head trauma (subdural), anticoagulation with confusion, deteriorating level of consciousness, no cause found on first-line workup, or before lumbar puncture. Yield is low in the absence of focal signs or trauma but is usually performed once in an older delirious patient to exclude a structural lesion |
| MRI brain | Suspected acute stroke (especially if CT is normal and stroke is suspected — diffusion-weighted imaging), suspected encephalitis (temporal lobe changes in herpes simplex), suspected non-convulsive status |
| EEG | Suspected non-convulsive status epilepticus (the treatable, easily missed cause of "delirium" that does not resolve), confirming a metabolic encephalopathy (typical generalised slowing), distinguishing delirium from psychiatric disorder (EEG is abnormal in delirium, normal in primary psychiatric) |
| Lumbar puncture | Suspected meningitis or encephalitis (fever, neck stiffness, headache, immunocompromise), after CT if focal signs or depressed consciousness |
| Septic screen (if source occult) | Repeat blood cultures, echocardiogram if endocarditis suspected, abdominal imaging for occult intra-abdominal sepsis |
| Vitamin levels | Thiamine (B1) in suspected Wernicke encephalopathy (alcohol misuse, malnutrition, hyperemesis, bariatric surgery) — give empirically before the result; B12 and folate in selected cases |
| Drug and alcohol screen | Urine drug screen, blood alcohol, if intoxication or withdrawal suspected |
| Troponin | If cardiac cause suspected; interpret with caution as troponin rises in many acute illnesses without acute coronary syndrome |
A practical rule
Do not order every test on every patient. Let the history and examination guide the workup. But every delirious patient gets a collateral history, a full medication review (especially anticholinergic burden), a focused examination (including a rectal examination for faecal impaction and bladder scan for retention), the first-line bloods and urinalysis, and usually a chest X-ray and ECG. Neuroimaging is low-yield in the absence of focal signs or trauma but is often performed once in an older patient to be safe. [1]
Management
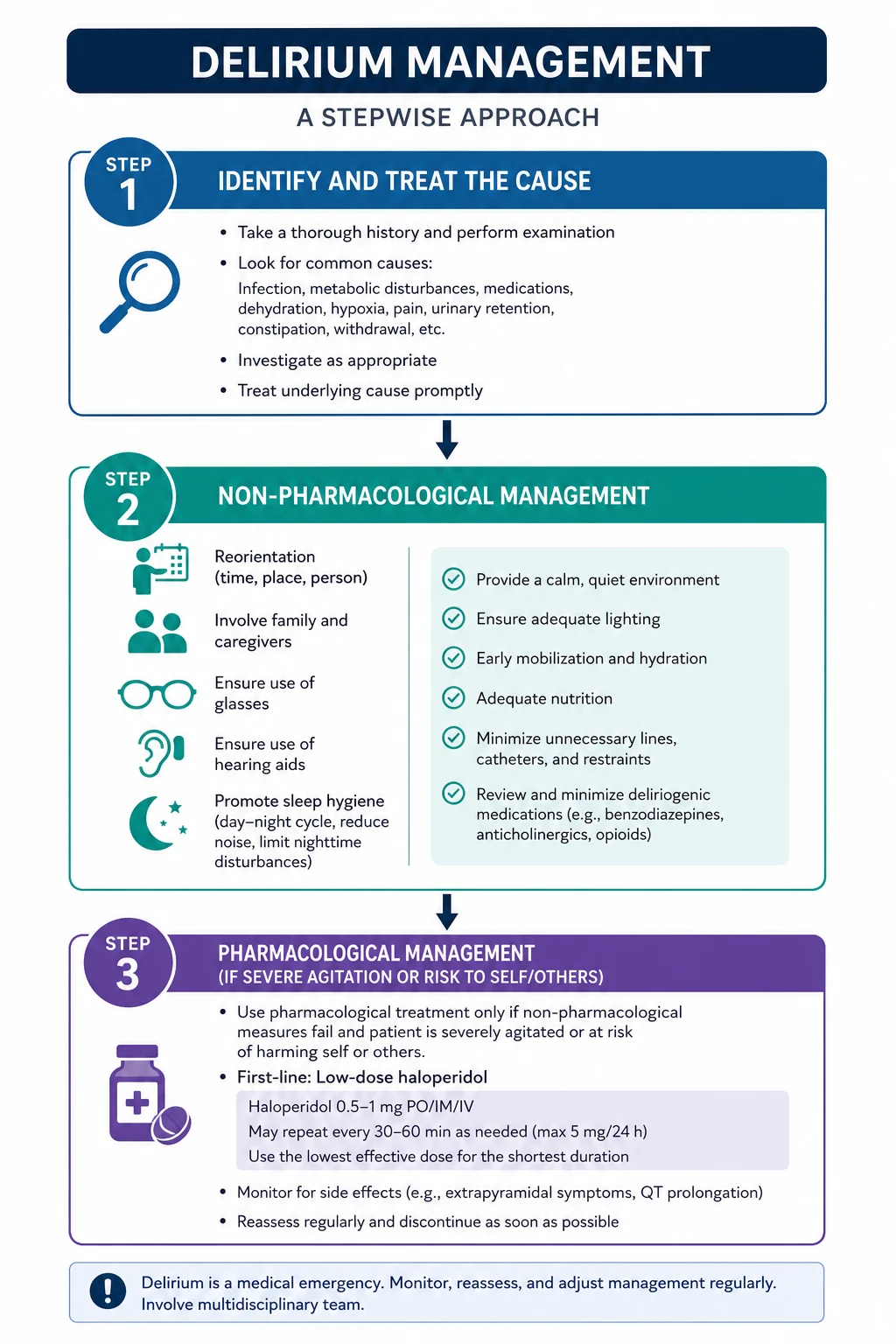
The management of delirium rests on three pillars, in order of priority: [1]
- Find and treat the underlying cause(s) — this is the actual treatment.
- Multicomponent non-pharmacological supportive care — environment, hydration, mobility, sleep, sensory aids, reorientation, family.
- Pharmacological symptom control — reserved for severe distress or danger, lowest effective dose, short duration. [1]
Pillar 1 — Find and treat the cause
This is the single most important intervention. The delirium will not resolve if the cause persists. Run the DELIRIUM mnemonic. Treat the infection, correct the sodium, stop the anticholinergic drug, relieve the urinary retention, treat the pain, soften the constipation, give the thiamine, treat the hypoxia. In most cases, delirium resolves over days to a week once the precipitant is removed. [1]
Caution about the common traps:
- Do not assume a positive urine culture is the cause in a catheterised or asymptomatic patient — search for other sources. Treating asymptomatic bacteriuria does not resolve delirium and causes harm (antibiotic resistance, C. difficile).
- Do not miss pain — uncontrolled pain is a major and under-recognised precipitant. Adequate analgesia reduces delirium. Use paracetamol first, regional techniques where possible (e.g., fascia iliaca block for hip fracture), and minimise opioids.
- Do not miss urinary retention and constipation — both are common, both are easily missed without a bladder scan and a rectal examination, and both are easily treated. [1]
Pillar 2 — Multicomponent non-pharmacological care
This is the HELP-style intervention, applied to every delirious patient regardless of cause. It is the mainstay of management and is often neglected. [1]
| Domain | Intervention |
|---|---|
| Environment | A quiet, well-lit room during the day, dim at night; a clock, calendar and orientation board the patient can see; a window view if possible; minimisation of ward moves; a side room if agitation is severe and disruptive |
| Orientation | Frequent reorientation by all staff (each interaction starts with "Hello Mrs X, my name is Y, I'm a doctor/nurse, it is [day], [date], you are in [hospital name]"); family present as much as possible; familiar objects from home (photos, a blanket) |
| Sensory aids | Ensure the patient wears their glasses and hearing aids at all times — these are frequently removed and lost in hospital, and their absence directly causes and perpetuates delirium |
| Communication | Clear, simple, slow communication; one question at a time; face the patient; do not argue with delusional beliefs — acknowledge and redirect |
| Sleep protection | Minimise night-time disruptions — cluster nursing tasks, avoid routine overnight observations if stable, reduce noise and light, avoid sedatives; a warm drink and relaxation if needed |
| Mobility | Get the patient out of bed and walking as early and as often as possible; minimise bed rest; remove urinary catheters and lines that tether; physiotherapy input |
| Hydration and nutrition | Active oral hydration support; assistance with meals; fluid chart; consider supplementary drinks; treat dry mouth |
| Family and carer involvement | Educate the family about delirium (what it is, that it is not dementia, that it usually resolves); encourage their presence; ask them to bring familiar objects; involve them in reorientation |
Pillar 3 — Pharmacological symptom control
Pharmacological therapy is NOT a treatment for delirium. It is a last-resort symptomatic measure for the small subset of patients in whom the agitation, distress, or behaviour poses a risk to the patient (pulling out essential lines, not receiving treatment, falling) or to others (staff and other patients). The drugs do not shorten the duration of delirium and may prolong it. [1]
When pharmacological therapy is indicated (rarely — estimate 5 to 10 percent of delirious inpatients), the approach is: [1]
First-line — haloperidol:
- Dose: 0.5 mg orally or intramuscularly (intramuscular if the patient will not take oral), repeated after 2 to 4 hours if needed, maximum 5 mg in 24 hours in older adults. In extreme agitation, 0.5 to 1 mg intramuscularly may be given. Start low, go slow, use the lowest effective dose, stop as soon as possible. [1]- Onset: 30 to 60 minutes orally, 10 to 20 minutes intramuscularly.
- Monitoring: ECG (QT prolongation — haloperidol prolongs the QTc and can cause torsades de pointes, especially in cardiac disease or with other QT-prolonging drugs), extrapyramidal effects, level of consciousness, blood pressure.
- Cautions: Absolute contraindication in Parkinson disease and dementia with Lewy bodies — neuroleptic sensitivity. Relative caution in cardiac disease, prolonged QT, hepatic impairment, epilepsy. [1]
Atypical antipsychotics (alternatives, similar efficacy, different side-effect profile):
- Risperidone 0.25 to 0.5 mg orally.
- Olanzapine 2.5 to 5 mg orally or orodispersible.
- Quetiapine 12.5 to 25 mg orally — preferred in Parkinson disease if an antipsychotic is genuinely unavoidable, with extreme caution, because of the lower dopamine D2 occupancy. [1]
Benzodiazepines — contraindicated in delirium EXCEPT:
- Alcohol withdrawal (delirium tremens) — benzodiazepines (diazepam, lorazepam) are the correct, life-saving treatment. Use a symptom-triggered protocol (CIWA-Ar).
- Benzodiazepine withdrawal — replace and taper the benzodiazepine.
- Seizures or status epilepticus as the cause.
- Catatonia (rare). [1]
Outside these specific indications, benzodiazepines worsen delirium, prolong its duration, cause oversedation, aspiration, falls, and respiratory depression. Do not use lorazepam or diazepam for the agitation of non-withdrawal delirium. [1]
Physical restraint
Physical restraint (bed rails, wrist restraints) is associated with worse outcomes — prolonged delirium, falls and injury, pressure injuries, psychological trauma, and loss of dignity. It should be avoided. If used, it must be the least restrictive measure, time-limited, documented, reviewed regularly, and weaned as soon as possible. One-to-one nursing, environmental modification, and family presence are preferred alternatives. [1]
DWE exam trap: A common MCQ presents an agitated older inpatient and asks for "the best management." The answer is almost always identify and treat the cause, with non-pharmacological measures — not haloperidol, not a benzodiazepine, not physical restraint. Pharmacological and physical measures are last resorts for danger or distress unresponsive to the cause search and non-pharmacological care. [1]
ICU delirium
Delirium in the intensive care unit is nearly universal in mechanically ventilated patients (up to 80 percent) and carries an independent association with longer ICU stay, longer mechanical ventilation, higher mortality, and long-term cognitive impairment resembling traumatic brain injury. [1]
The PAD guidelines (Society of Critical Care Medicine: Pain, Agitation, Delirium) recommend the ABCDEF bundle:
- Assess and manage pain.
- Both spontaneous awakening trials and spontaneous breathing trials (daily interruption of sedation and ventilation). [1]- Choice of analgesia and sedation (prefer opioid-based analgesia and light sedation; avoid benzodiazepines which are independently associated with delirium).
- Delirium assessment (CAM-ICU or ICDSC) and management.
- Early mobility.
- Family engagement. [1]
The evidence for pharmacological treatment of ICU delirium is disappointing. The HOPE-ICU trial (PMID 24461612) found haloperidol did not reduce delirium or coma duration. The AID-ICU trial (PMID 36286254) found haloperidol did not improve days alive and out of hospital at 90 days. Dexmedetomidine, an alpha-2 agonist, is emerging as a preferred agent in ICU because it provides sedation and analgesia without the benzodiazepine-associated delirium risk and may reduce delirium duration — but it is an ICU-specific agent and not used on the general ward. [1]
The principle on the ward remains: treat the cause, provide supportive non-pharmacological care, reserve antipsychotics for severe distress or danger. [1]
Differentiating delirium, dementia, and depression
These three conditions are commonly confused in older adults, with serious consequences. Delirium is the medical emergency that must never be missed. The differentiation is clinical and rests on the temporal pattern, the cognitive domains affected, and the level of consciousness. [1]
| Feature | Delirium | Dementia | Depression |
|---|---|---|---|
| Onset | Acute (hours to days) | Insidious and gradual (months to years) | Subacute (weeks to months) |
| Course | Fluctuating — worse at night, varies through the day | Stable day to day, slowly progressive over months | Stable but diurnal variation (worse in morning, common) |
| Duration | Days to weeks (usually reversible) | Years, progressive | Weeks to months, treatable |
| Attention | Markedly impaired (the cardinal feature) | Preserved until late stage | May be mildly impaired (pseudodementia) but effort-dependent |
| Consciousness | Altered (drowsy, hypervigilant, fluctuating) | Normal (clear) until late | Normal (clear) |
| Orientation | Disoriented, fluctuates | Disoriented (especially time and place), stable pattern | Often correct, or "I don't know" responses |
| Memory | Recent and immediate impaired (registration) | Recent and new learning impaired early; remote late | Variable, inconsistent ("I don't know") |
| Thinking | Disorganised, incoherent, may be delusional | Impoverished, slow | Negative, ruminative, guilty, hopeless |
| Perception | Hallucinations (often visual), illusions | May have hallucinations late (Lewy body) | Intact (unless severe psychotic depression) |
| Psychomotor | Hyperactive, hypoactive, or mixed | Often normal early; apraxia and agnosia later | Retarded (slow) or agitated |
| Speech | Incoherent, rambling, mumbling | Word-finding difficulty, naming deficit | Slow, sparse, low volume |
| Key collateral | Acute change from baseline, fluctuates | Gradual decline over months | Mood change, anhedonia, somatic complaints |
Critical clinical points
- Delirium can superimpose on dementia. The most common scenario is an older patient with known dementia who becomes acutely worse — this is delirium superimposed on dementia, and it must be investigated and treated as delirium. Do not write it off as "the dementia progressing."
- Depression can mimic hypoactive delirium — but depression has a subacute onset over weeks, a stable (not fluctuating) course, normal level of consciousness, and intact attention. The "I don't know" answer pattern and the history of mood change distinguish depression.
- Pseudodementia (depressive cognitive impairment) can mimic dementia but reverses with depression treatment — always screen for depression in a patient with apparent new cognitive impairment.
- Dementia with Lewy bodies has spontaneous fluctuations and visual hallucinations that can mimic delirium — but the fluctuations are chronic (over months), the hallucinations are recurrent, and there is parkinsonism. The distinction is critical because DLB patients have catastrophic neuroleptic sensitivity to haloperidol. [1]
DCE long-case rule: When assessing a confused older patient, your opening statement should distinguish delirium from dementia: "This is Mrs X, an 82-year-old with known Alzheimer dementia, presenting with an acute deterioration from her baseline over 24 hours, with fluctuating confusion and drowsiness. This is delirium superimposed on dementia, and I am investigating the precipitant." [1]
Complications and outcomes
Delirium is not a benign, self-limiting condition. It is an independent marker and mediator of poor outcomes, even after adjusting for age, comorbidity, illness severity, and baseline dementia. The landmark meta-analysis (Witlox 2010, PMID 20664045) established the magnitude of the associations. [1]
Short-term complications
- Prolonged hospital stay — delirious patients stay in hospital roughly twice as long as non-delirious patients with the same admission diagnosis.
- Falls — from agitation, wandering, impaired judgement, and the sedative effects of the drugs used to treat the delirium.
- Pressure injuries — from immobility, poor nutrition, and incontinence during the delirious episode.
- Aspiration pneumonia — from impaired swallow and reduced level of consciousness.
- Institutionalisation — many delirious patients cannot return home and require new residential or supported care. [1]
Mortality
Delirium is independently associated with increased mortality. In-hospital mortality of delirious patients is roughly double that of matched non-delirious patients. The one-year mortality after a delirium episode is high — up to 40 to 50 percent in some series, depending on setting (highest in ICU and palliative care, lower in elective surgical patients). The mortality reflects both the severity of the precipitating illness and the independent contribution of the delirium itself. [1]
Persistent cognitive impairment — delirium as a brain insult
This is the most important long-term consequence and the subject of intense research. Delirium is not merely a marker of a vulnerable brain — it may itself cause brain damage. Evidence: [1]
- Patients who experience delirium are at markedly increased risk of subsequent dementia, even if they had no prior cognitive impairment.
- In patients with existing dementia, each episode of delirium accelerates the cognitive decline.
- Delirium that persists beyond the acute illness ("persistent delirium" or "chronic delirium") occurs in up to 30 to 45 percent of patients at discharge and predicts long-term cognitive decline and institutionalisation.
- The mechanism may be neuronal injury from sustained neuroinflammation, accelerated neurodegeneration, or a "delirium-dementia" vicious cycle. [1]
Other long-term complications
- Post-traumatic stress disorder and psychological distress — patients who recall their delirium (especially ICU and hyperactive delirium with hallucinations) commonly describe frightening, traumatic experiences. This is now recognised and deserves acknowledgement and explanation.
- Functional decline and loss of independence — the delirious episode often marks a step-down in baseline function that does not fully recover.
- Caregiver burden and institutionalisation — the family carries the consequences; many delirious patients never return home. [1]
Special situations
Postoperative delirium (especially hip fracture and cardiac surgery)
Postoperative delirium occurs in 15 to 53 percent of older patients after hip fracture repair and 20 to 50 percent after cardiac surgery. The precipitants are a combination of the anaesthetic and surgical insult, pain, opioids, inflammation, immobility, and the underlying vulnerability (most hip fracture patients have some cognitive impairment). Prevention (HELP-style), adequate pain control (including regional blocks), early mobilisation, and medication minimisation are key. The American Geriatrics Society guideline on postoperative delirium (2015) emphasises multicomponent non-pharmacological prevention as the single most effective strategy. [1]
Terminal (palliative) delirium
Delirium in the last days to weeks of life is extremely common — up to 80 percent in the final days. The precipitants are often multifactorial and irreversible (organ failure, opioid metabolites, brain metastases, hypercalcaemia). The goals shift: symptom comfort, sedation for distress, and family support. Haloperidol remains first-line for agitation; low-dose benzodiazepines may be added for terminal agitation that is refractory. The family must be counselled that the delirium reflects the dying process and that the priority is comfort, not reversal. [1]
Alcohol withdrawal (delirium tremens)
This is a specific delirium subtype requiring specific treatment. It is the only delirium in which benzodiazepines are the correct first-line agent. The presentation (tremor, agitation, hallucinations, autonomic hyperactivity, seizures) reflects central nervous system hyperexcitability from chronic gamma-aminobutyric acid (GABA) downregulation and glutamate upregulation. Treatment is with a symptom-triggered benzodiazepine protocol (CIWA-Ar-guided diazepam or lorazepam), thiamine (to prevent Wernicke encephalopathy), and supportive care. Antipsychotics (haloperidol) may be added for refractory hallucinations but do not treat the withdrawal and may lower seizure threshold. Untreated severe alcohol withdrawal has a mortality of 5 to 15 percent. [1]
The DCE short case — cognitive assessment
A cognitive assessment short case (typically PACES Station 5 or a DCE short case on the general medicine or geriatric rotation) tests the structured assessment of attention, orientation, memory, language, and executive function, and the ability to distinguish delirium from dementia and depression. [1]
Structured routine (examiner instruction: "Assess this patient's cognition")
- Establish rapport and baseline — confirm identity, explain the assessment, ensure glasses and hearing aids are on, ensure the patient is comfortable and not in pain. Ask: "How are you today? Can you tell me your full name, your age, and where we are?"
- Alertness — observe the patient's level of consciousness. Is the patient alert, drowsy, hypervigilant, fluctuating? This is the first domain of the 4AT.
- Attention — the cardinal domain. Ask the patient to recite the months of the year backwards (December, November, October, September, August, July, June, May, April, March, February, January). Record errors. Alternatively, serial sevens (100, 93, 86, 79, 72, 65) or digit span backwards (start with 3 digits, extend to 5 to 7).
- Orientation — time (day, date, month, year, season), place (hospital name, floor, city, country), person (name, date of birth). Document each item.
- Registration and recall — name three objects (apple, table, penny), ask the patient to repeat, then recall after 3 to 5 minutes.
- Language — naming (watch, pencil, a complicated object), repetition ("no ifs, ands, or buts"), comprehension (three-step command: "take this paper in your right hand, fold it in half, and put it on the floor"), reading and writing (a sentence), fluency.
- Executive function — clock-drawing test ("draw a clock face, put in all the numbers, and set the hands to ten past eleven") — tests planning, visuospatial function, and frontal-executive function. Interlocking pentagons (MMSE).
- Visuospatial — copy a cube or interlocking pentagons.
- Mood and insight — "How is your mood? Do you feel low?" Assess insight into the cognitive difficulty.
- Collateral history — always ask, or note the need to obtain, a collateral history from a family member or the treating team regarding the baseline and the onset. [1]
Formal cognitive tools
- Mini-Mental State Examination (MMSE) — 30-point screen; now superseded by MoCA for sensitivity to mild impairment but still widely used.
- Montreal Cognitive Assessment (MoCA) — 30-point; more sensitive than MMSE to mild cognitive impairment; tests executive function, attention, language, abstraction, recall, orientation (normal is 26 or above).
- 4AT — the rapid delirium screen (score 4 or more suggests delirium).
- Abbreviated Mental Test-4 (AMT-4) — age, date of birth, place, year — the attention subcomponent of the 4AT. [1]
Presentation template
"I performed a cognitive assessment on this 82-year-old woman. She is drowsy and fluctuating in alertness. Attention is markedly impaired — she cannot recite the months of the year backwards and loses the thread after two months. She is disoriented in time (thinks it is 1998) and place (cannot name the hospital). Registration is intact but recall is impaired at 3 minutes. Language and executive function are impaired — her clock-drawing shows perseveration and disorganisation. Her mood appears flat. A collateral history from her daughter confirms an acute change over the last 24 hours from her baseline of mild Alzheimer dementia. These findings are consistent with delirium superimposed on dementia. I would now investigate the precipitant — I have ordered a full septic screen, electrolytes, urinalysis, chest X-ray and ECG, and I am reviewing her medications for anticholinergic burden." [1]
Discussion from signs
- Acute onset, fluctuating alertness, inattention, disorientation, impaired clock-drawing = delirium, possibly superimposed on dementia.
- Stable, gradually progressive cognitive impairment with preserved attention early = dementia.
- Subacute mood change, anhedonia, "I don't know" answers, normal attention, normal alertness = depression (pseudodementia if cognitive impairment present).
- Fluctuating cognition with visual hallucinations and parkinsonism over months = dementia with Lewy bodies. [1]
Common exam traps
- Reaching for haloperidol first — the answer to "best management of delirium" is almost always identify and treat the cause with non-pharmacological measures, not a drug.
- Missing hypoactive delirium — the quiet, drowsy patient is the most dangerous presentation; always apply the CAM or 4AT to any older inpatient who is less responsive than baseline.
- Giving haloperidol to a patient with Parkinson disease or dementia with Lewy bodies — potentially catastrophic neuroleptic sensitivity; use quetiapine with extreme caution if an antipsychotic is unavoidable.
- Using benzodiazepines for non-withdrawal delirium agitation — they worsen and prolong delirium; reserved for alcohol or benzodiazepine withdrawal, seizures, and catatonia.
- Assuming a positive urine culture is the cause — asymptomatic bacteriuria is common in older adults and catheterised patients; correlation with symptoms, pyuria and exclusion of other sources is required.
- Writing off acute confusion in a known dementia patient as "dementia progressing" — acute change is delirium until proven otherwise, even in a patient with established dementia; investigate and treat.
- Confusing DLB with delirium — chronic fluctuating cognition with visual hallucinations and parkinsonism over months is DLB; the distinction matters because of neuroleptic sensitivity.
- Stopping the cause search at the first precipitant — delirium is multifactorial; find and treat every precipitant (the DELIRIUM mnemonic).
- Using physical restraint as a first-line measure — associated with worse outcomes; one-to-one nursing, environmental modification, and family presence are preferred.
- Forgetting to reassess at 48 to 72 hours — if delirium is not improving, the precipitant search is incomplete; look again, especially for occult infection, drug causes, retention, constipation, and pain. [1]
Guidelines and regional deltas
- NICE Clinical Guideline CG103 (2010, updated 2023) — Delirium: prevention, diagnosis and management. The UK primary guidance. Recommends multicomponent risk-factor intervention for prevention, the CAM or 4AT for diagnosis, and the principle that antipsychotics should be reserved for patients who are distressed or a risk to themselves or others, at the lowest effective dose for the shortest possible duration.
- Australian Commission on Safety and Quality in Health Care (ACSQHC) — Delirium Clinical Care Standard (2021). The ANZ primary guidance. Emphasises that delirium is a medical emergency, that all older at-risk patients should be screened on admission, that the underlying cause is identified and treated, and that a multicomponent non-pharmacological approach is the mainstay. Reduces reliance on antipsychotics and physical restraint.
- American Geriatrics Society (AGS) Clinical Practice Guideline for Postoperative Delirium in Older Adults (2015). US guidance emphasising multicomponent non-pharmacological interventions for prevention, and caution with antipsychotics (which carry an FDA black-box warning for increased mortality in older adults with dementia when used long-term, though short-term use in delirium is different).
- Society of Critical Care Medicine (SCCM) PADIS guidelines — for ICU delirium, the ABCDEF bundle, with dexmedetomidine emerging as a preferred agent. [1]
Regional drug differences: Haloperidol is the first-line antipsychotic for delirium worldwide, available orally and parenterally. In ANZ and the UK, the FDA black-box warning (increased mortality in elderly dementia patients treated with antipsychotics) is noted but does not preclude short-term use in delirium — the warning applies to chronic use in dementia, not acute use in delirium. The Beers Criteria (American Geriatrics Society) lists antipsychotics and benzodiazepines as potentially inappropriate in older adults, reinforcing caution. Dexmedetomidine is widely available in ICU settings in ANZ, UK, and US. [1]
Communication and shared decision-making
Delirium is frightening for the patient, the family, and the staff. The communication priorities: [1]
- Explain what delirium is — to the family, in plain language: "Your mother has delirium, which is a temporary disturbance of the brain caused by the illness and the hospital stay. It is not a permanent loss of her mind. It usually improves over days to weeks as we treat the underlying problem."
- Acknowledge the fear — the patient who remembers hallucinations may be traumatised; the family seeing a loved one agitated and unrecognising them is distressed. Acknowledge this and offer support.
- Discuss the role and risks of medication — if an antipsychotic is being considered, explain why (to settle severe distress or danger, not to treat the delirium itself), the dose, the monitoring, the plan to stop as soon as possible, and the specific risks (sedation, falls, extrapyramidal effects, QT prolongation).
- Encourage family involvement — ask the family to be present, to bring familiar objects, to assist with reorientation, feeding, and reassurance. Their presence is therapeutic.
- Discuss the prognosis honestly — most delirium resolves, but some persists; there is an increased risk of longer-term cognitive impairment. Set realistic expectations without catastrophising.
- Initiate advance care planning — an episode of delirium in a patient with dementia is a natural trigger to discuss goals of care, substitute decision-makers, and future preferences. [1]
Long-term outcomes and follow-up
Most delirium resolves over days to weeks once the precipitant is treated, but a significant proportion persists. Follow-up after a delirium episode should include: [1]
- Cognitive reassessment at 1 to 3 months to detect persistent cognitive impairment or new dementia, with onward referral to memory services if needed.
- Functional reassessment — many patients have a step-down in baseline function; rehabilitation, physiotherapy, and occupational therapy support recovery.
- Medication review — ensure precipitating drugs (anticholinergics, benzodiazepines) have been removed or deprescribed.
- Risk modification — address the modifiable risk factors to prevent recurrence (optimise vision and hearing, manage comorbidity, minimise polypharmacy, encourage activity and social engagement).
- Family education and support — explain the episode, the risk of recurrence, the warning signs, and the importance of seeking early medical review for any acute illness. [1]
The recurrence rate of delirium is high — patients who have had one episode are at markedly increased risk of future episodes. Each episode may accelerate cognitive decline. Prevention of recurrence is as important as treatment of the index episode. [1]
References and further reading
Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med 1990;113:941-948 (PMID 2240918). Inouye SK, Bogardus ST, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients. N Engl J Med 1999;340:669-676 (PMID 10053175). Inouye SK. Delirium in older persons. N Engl J Med 2006;354:1157-1165 (PMID 16540616). Witlox J, Eurelings LSM, de Jonghe JFM, et al. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA 2010;304:443-451 (PMID 20664045). Inouye SK, Westendorp RGJ, Saczynski JS. Delirium in elderly people. Lancet 2014;383:911-922 (PMID 23992774). Shenkin SD, Fox C, Godfrey M, et al. Delirium detection in older adults and the validation of the 4AT in acute medicine. Age Ageing 2014;43(suppl_1):i23 (PMID 24590568). Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomised, double-blind, placebo-controlled trial. Lancet Respir Med 2013;1:515-523 (PMID 24461612). Oddi A, Taekker Janssen L, Luta C, et al. Haloperidol for the treatment of delirium in critically ill patients (AID-ICU). N Engl J Med 2022;387:2322-2332 (PMID 36286254). NICE Clinical Guideline CG103 — Delirium: prevention, diagnosis and management (2010, updated 2023). Australian Commission on Safety and Quality in Health Care — Delirium Clinical Care Standard (2021). [1]
References
- [1]Inouye SK, van Dyck CH, Alessi CA, et al. Clarifying confusion: the confusion assessment method. A new method for detection of delirium Ann Intern Med, 1990.PMID 2240918
- [2]Inouye SK, Bogardus ST, Charpentier PA, et al. A multicomponent intervention to prevent delirium in hospitalized older patients N Engl J Med, 1999.PMID 10053175
- [3]Inouye SK Delirium in older persons N Engl J Med, 2006.PMID 16540616
- [4]Witlox J, Eurelings LSM, de Jonghe JFM, et al. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis JAMA, 2010.PMID 20664045
- [5]Inouye SK, Westendorp RGJ, Saczynski JS Delirium in elderly people Lancet, 2014.PMID 23992774
- [6]Shenkin SD, Fox C, Godfrey M, et al. Validation of the 4AT, a new instrument for rapid delirium screening: a study in 234 hospitalised older people Age Ageing, 2014.PMID 24590568
- [7]Page VJ, Ely EW, Gates S, et al. Effect of intravenous haloperidol on the duration of delirium and coma in critically ill patients (Hope-ICU): a randomised, double-blind, placebo-controlled trial Lancet Respir Med, 2013.PMID 24461612
- [8]Oddi A, Taekker Janssen L, Luta C, et al. Haloperidol for the Treatment of Delirium in ICU Patients N Engl J Med, 2022.PMID 36286254