Phys · geriatric
Dementia
Also known as major neurocognitive disorder · cognitive impairment · Alzheimer disease · vascular dementia · dementia with Lewy bodies · frontotemporal dementia · mixed dementia · primary progressive aphasia · behavioural variant frontotemporal dementia · mild cognitive impairment · pseudodementia
Consultant-physician-depth guide to dementia for FRACP DWE and DCE — DSM-5 major neurocognitive disorder definition, the five major subtypes (Alzheimer, vascular, Lewy body, frontotemporal, mixed), mild cognitive impairment, cognitive assessment with MoCA and ACE-III, the reversible-cause workup, cholinesterase inhibitors and memantine, the BPSD escalation ladder, the antipsychotic contraindication in Lewy body dementia, driving and capacity, and the differentiation from delirium and depression.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Dementia

The answer first
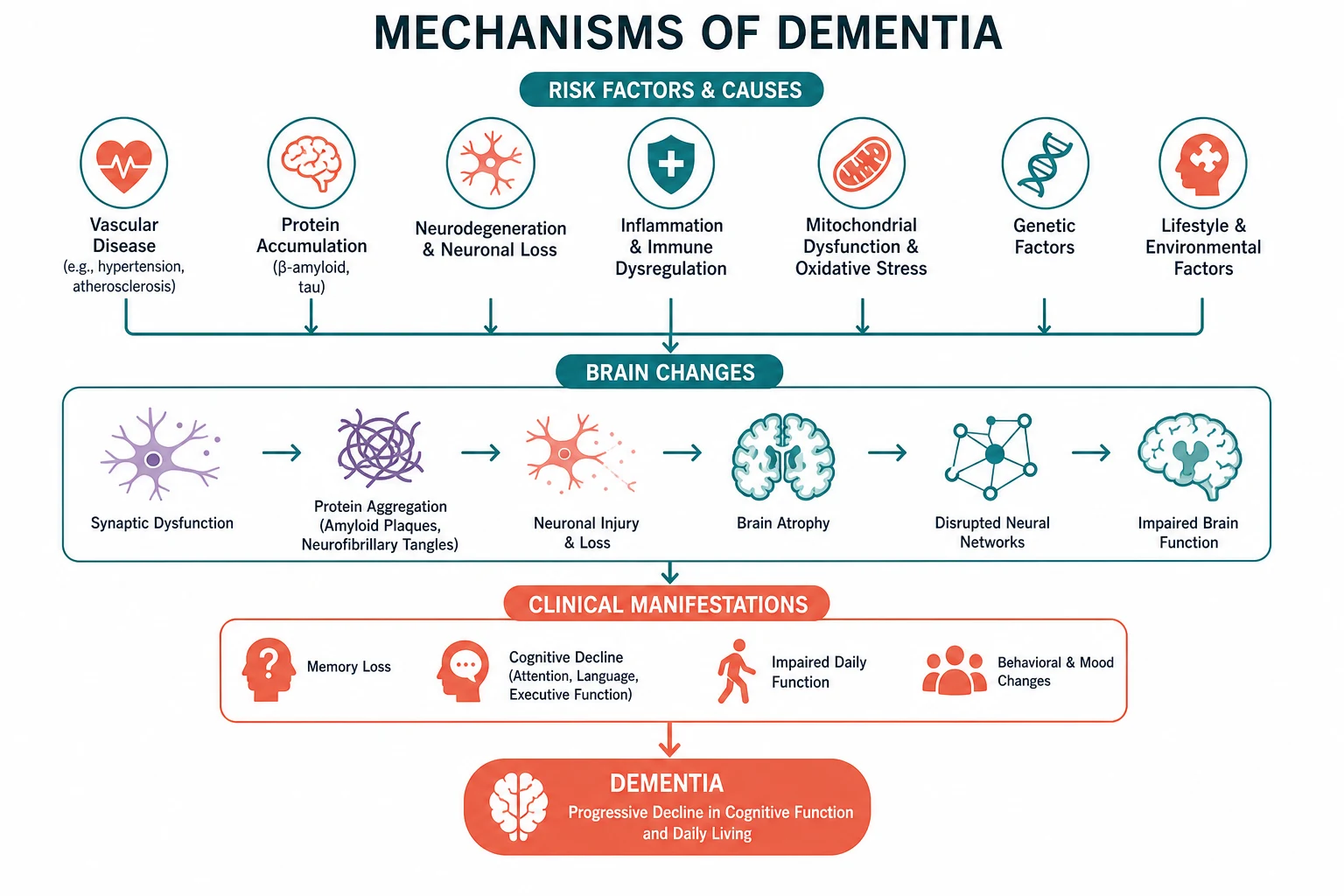
Dementia is a progressive decline in cognition across multiple domains, sufficient to interfere with independence in daily activities, that is not delirium and not explained by another mental disorder. It is not a single disease — it is a clinical syndrome with at least five common underlying pathologies, each with a different course, a different management, and a different set of traps. The most common type is Alzheimer disease, accounting for 60 to 70 percent of cases. [1]
The five rules that determine everything in dementia are: [1]
- It is a clinical diagnosis, anchored by the collateral history. No blood test or scan diagnoses dementia. You make the diagnosis by demonstrating a decline from a documented baseline across multiple cognitive domains, confirmed by a carer who has watched the patient lose function — and by excluding delirium, depression, and the reversible mimics.
- The subtype matters more than the label. "Dementia" is not enough. The subtype — Alzheimer, vascular, Lewy body, frontotemporal, or mixed — determines which drug helps (cholinesterase inhibitors help Alzheimer and Lewy body, not frontotemporal), which drug kills (antipsychotics in Lewy body), and what the family can expect.
- You must exclude the reversible causes before you settle. B12 deficiency, hypothyroidism, depression, normal pressure hydrocephalus, subdural haematoma, and medication burden are the classic reversible mimics — and missing them is the most defensible error in this entire topic. Every dementia workup gets a B12, a folate, a TSH, and an imaging study.
- Management is mostly non-pharmacological. Cognitive enhancers produce a modest, symptomatic benefit that is measured in points on a cognitive scale and months of function — they do not cure or halt disease. The real management is carer education, cognitive stimulation, exercise, social engagement, driving and capacity planning, and the structured management of behavioural and psychological symptoms.
- Antipsychotics are dangerous and should be the last resort, and in Lewy body dementia they are absolutely contraindicated. Atypical antipsychotics increase mortality by about 1.6 to 1.7 times in dementia (Schneider 2005, PMID 16234500), and in Lewy body dementia a single dose can trigger catastrophic rigidity, hyperthermia, and irreversible decline — neuroleptic sensitivity. [1]
DWE high-yield trap: When asked "best initial management of behavioural and psychological symptoms of dementia," the answer is almost always assess for precipitants (pain, infection, constipation, environment, drug), address them, and use non-pharmacological strategies — not an antipsychotic. Risperidone is the only agent subsidised for this indication and only for aggression severe enough to risk the patient or others, time-limited to 12 weeks. [1]
Definition — DSM-5 major neurocognitive disorder
The DSM-5 replaced the term "dementia" with major neurocognitive disorder, though the older term remains in clinical use and in every exam. The diagnosis requires all of the following: [1]
- Evidence of significant cognitive decline from a previous level of performance in one or more domains — complex attention, executive function, learning and memory, language, perceptual-motor, or social cognition — based on both concern from the patient, a knowledgeable informant, or the clinician, and objective impairment on standardised testing.
- The cognitive deficits interfere with independence in everyday activities — the discriminator from mild cognitive impairment. The patient needs help with instrumental activities of daily living (finances, transport, medications, cooking) or, later, basic activities of daily living (dressing, bathing, toileting).
- The deficits do not occur exclusively in the context of delirium. Acute confusion is delirium until proven otherwise, even in a patient with known dementia.
- The deficits are not better explained by another mental disorder — in practice, major depression ("pseudodementia"). [1]
Mild neurocognitive disorder occupies the zone between normal ageing and dementia: a decline in one or more domains that is greater than expected for age and education but does not interfere with independence. This is the clinical diagnosis of mild cognitive impairment (MCI). Patients with MCI progress to dementia at about 10 to 15 percent per year, compared with 1 to 2 percent per year in the general older population (Petersen 2011, PMID 21651394) — which is why MCI is the population targeted by every prevention trial. [1]
Clinical rule: The single most useful piece of information in the dementia assessment is a collateral history from a family member or carer. It establishes the baseline, the onset, the course, and the functional impact — the four facts that separate dementia from delirium, from depression, and from normal ageing. A cognitive test score in isolation is meaningless without it. [1]
The five major subtypes
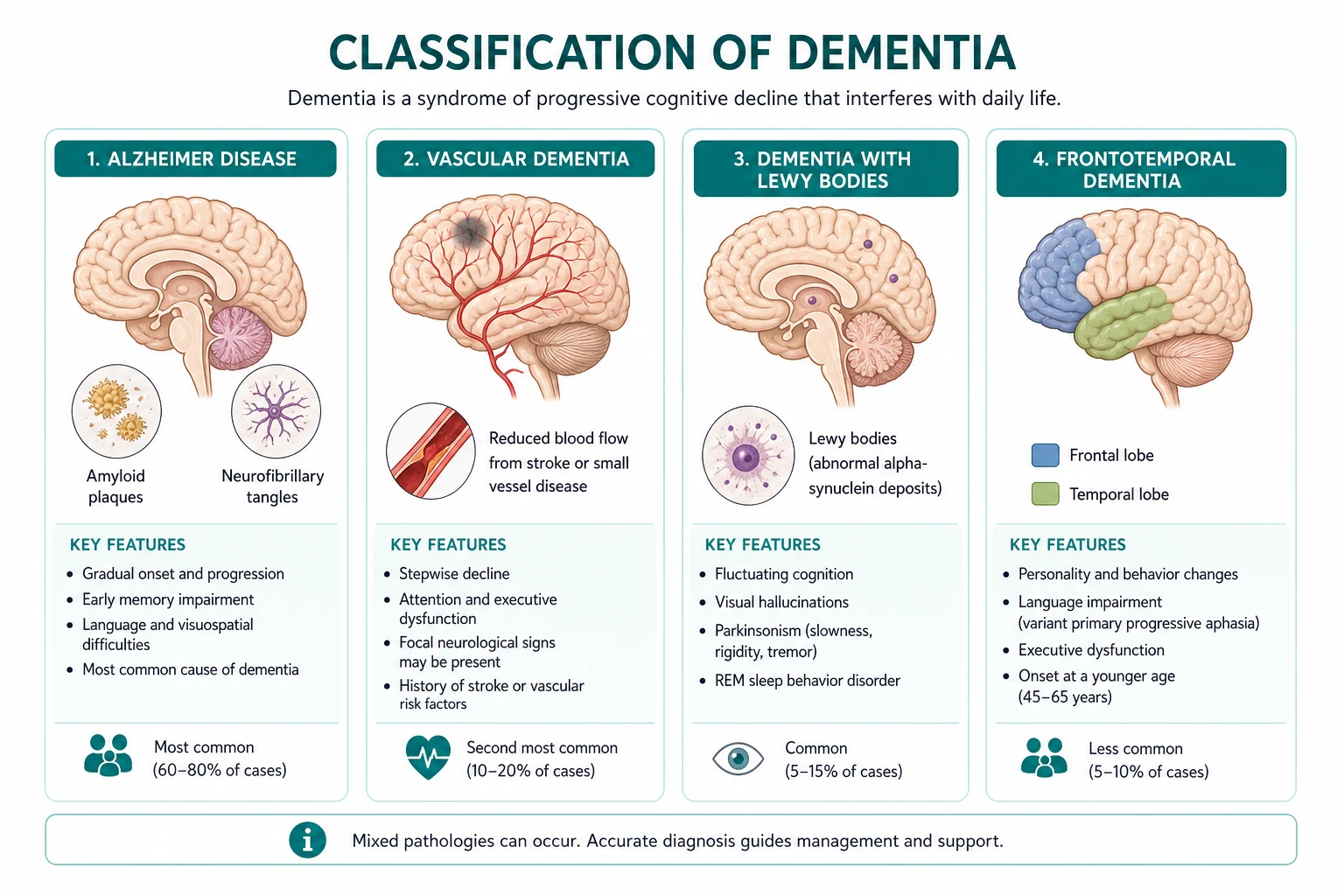

1. Alzheimer disease (60 to 70 percent)
Alzheimer disease is the prototype and the commonest cause. The pathology is amyloid-beta plaque deposition in the extracellular space and intraneuronal neurofibrillary tangles of hyperphosphorylated tau. The pathology begins in the entorhinal cortex and hippocampus — which is why the earliest and most prominent symptom is loss of recent memory — and spreads to the temporoparietal association cortex, producing language difficulty (anomia, then aphasia), visuospatial impairment (getting lost, misplacing objects), and executive dysfunction. [1]
The clinical signature: [1]
- Insidious onset, with gradual progression over years. Family often dates the onset only in retrospect — "it must have started two or three years ago."
- Recent memory loss is the presenting complaint in the amnestic variant — the patient repeats questions, forgets recent conversations, misplaces items, and relies increasingly on lists and carers.
- Naming difficulty (anomia) is an early language sign — the patient circumlocutes ("the thing you write with" for pen).
- Visuospatial impairment — getting lost in familiar places, difficulty dressing (dressing apraxia).
- Executive dysfunction — poor judgement, difficulty managing finances or medications, loss of insight.
- Preserved social graces in the early and moderate stages — the patient may converse normally in a brief encounter, masking the deficit. This is why a bedside cognitive test is essential and why a collateral history is irreplaceable.
- Depressive symptoms, apathy, and anxiety are common early behavioural features. Psychosis (hallucinations and delusions, often of theft or infidelity) and aggression emerge later. [1]
Imaging shows hippocampal and temporoparietal atrophy on MRI, with symmetrical temporal horn enlargement. CSF biomarkers (low amyloid-beta 1-42, elevated total tau and phospho-tau) are used in younger-onset or atypical cases, and amyloid-PET is emerging into clinical practice. [1]
2. Vascular dementia (about 20 percent)
Vascular dementia is cognitive impairment caused by cerebrovascular disease. It has two patterns — multi-infarct dementia from large strategic cortical infarcts, and subcortical small-vessel disease from chronic hypertensive vasculopathy producing white matter changes (leukoaraiosis) and lacunar infarcts. [1]
The clinical signature: [1]
- Stepwise or stair-step decline in the multi-infarct pattern — the family describes discrete worsening events ("after his stroke in March, he was never the same, then he had another in August"). This contrasts with the smooth, insidious course of Alzheimer.
- Executive dysfunction predominates in small-vessel disease — slowing of processing speed (bradyphrenia), impaired planning and set-shifting, and reduced fluency — rather than the episodic memory loss of Alzheimer. Memory is relatively spared early.
- Gait disturbance, urinary urgency, and pseudobulbar features (dysarthria, dysphagia, emotional lability) accompany subcortical disease.
- Focal neurological signs may be present — upper motor neuron signs, asymmetric reflexes, a hemiparetic gait.
- Vascular risk factors dominate the history — hypertension, diabetes, atrial fibrillation, prior stroke or transient ischaemic attack, smoking, ischaemic heart disease. [1]
Imaging shows cortical or subcortical infarcts, white matter hyperintensities on T2/FLAIR, and lacunes — the burden of which correlates (imperfectly) with the cognitive deficit. The management is vascular risk factor control — blood pressure, glycaemia, lipids, anticoagulation for atrial fibrillation, smoking cessation — plus a cholinesterase inhibitor, which has modest benefit. [1]
Clinical rule: In practice, pure vascular dementia is uncommon. Most older patients with cerebrovascular disease also have Alzheimer pathology — this is mixed dementia, the most common real-world diagnosis in patients over 80. The treatment addresses both. [1]
3. Dementia with Lewy bodies (about 5 to 10 percent)
Dementia with Lewy bodies (DLB) is an alpha-synucleinopathy — the same protein that drives Parkinson disease — characterised by cortical Lewy body deposition. It is the most clinically distinctive subtype because of its combination of features and its catastrophic pharmacological sensitivity. [1]
The central clinical features (the McKeith 2017 consensus criteria, PMID 28592453): [1]
- Fluctuating cognition — the patient is lucid and coherent one day, confused and disorganised the next, then back to near-baseline. Family describe "good days and bad days." This fluctuation can mimic delirium, and DLB is the dementia that most often presents to acute medicine with a wrong label.
- Recurrent, well-formed, detailed visual hallucinations — often of people or animals in the room, that the patient may or may not find distressing. This is the single most discriminating feature from Alzheimer.
- Spontaneous features of parkinsonism — bradykinesia, rigidity, and a shuffling gait — that appear with or after the dementia (if parkinsonism precedes the dementia by more than one year, the diagnosis is Parkinson disease dementia, not DLB — the "one-year rule").
- REM sleep behaviour disorder — the patient acts out vivid dreams, shouting, punching, or kicking in sleep, sometimes for years before the cognitive symptoms begin. It is now recognised as a highly specific prodromal feature.
- Severe neuroleptic sensitivity — antipsychotic drugs (haloperidol, risperidone, olanzapine) can trigger catastrophic rigidity, hyperthermia, immobility, and irreversible cognitive and physical decline, sometimes after a single dose. This is the single most important pharmacological fact in the entire dementia topic. [1]
Supportive features include autonomic dysfunction (orthostatic hypotension, urinary incontinence, constipation), severe anticholinergic drug sensitivity, depression, anxiety, and delusions. Indicative biomarkers are a low uptake on dopamine transporter (DAT) SPECT, abnormal (low uptake) metaiodobenzylguanidine (MIBG) myocardial scintigraphy, and polysomnographic confirmation of REM sleep without atonia. [1]
Cholinesterase inhibitors are particularly effective in DLB — more so than in Alzheimer — because the cholinergic deficit is profound. Rivastigmine is the agent with the strongest trial evidence. Memantine may help. Antipsychotics are avoided — quetiapine is the least harmful if one is absolutely necessary, but even it carries risk. [1]
4. Frontotemporal dementia (5 to 10 percent, younger onset)
Frontotemporal dementia (FTD) is a group of disorders characterised by frontal and anterior temporal lobe atrophy with underlying tau or TDP-43 proteinopathy. It is the commonest cause of dementia in the under-65 age group, with onset typically between 45 and 65. [1]
The behavioural variant (bvFTD) is the most common: [1]
- Personality and behavioural change is the presenting feature, not memory loss. The family brings the patient in saying "he is not himself" — disinhibited, socially inappropriate, making crude jokes, eating excessively or to excess of specific foods, neglecting personal hygiene, showing loss of empathy and warmth, and displaying repetitive or compulsive behaviours.
- Memory is relatively spared early — which leads to misdiagnosis as a psychiatric disorder (depression, mania, late-onset psychosis, or "midlife crisis").
- Executive dysfunction is present on testing, with relative sparing of episodic memory and visuospatial function.
- The six diagnostic features (Rascovsky 2011 criteria, PMID 21810890): disinhibition, apathy or inertia, loss of sympathy or empathy, perseverative or compulsive behaviour, hyperorality or dietary change, and a dysexecutive neuropsychological profile. Three of six establish "possible bvFTD." [1]
The language variants (primary progressive aphasia): [1]
- Non-fluent variant — effortful, halting speech with apraxia of speech and agrammatism, with preserved comprehension early. Left posterior frontal-insular atrophy.
- Semantic variant — fluent but empty speech with severe loss of word meaning (semantic anomia) and impaired object recognition, with preserved repetition. Left anterior temporal atrophy.
- Logopenic variant — slow speech with word-finding pauses and impaired repetition of long phrases, with relatively preserved comprehension and grammar. Left temporoparietal atrophy, and often an underlying Alzheimer pathology. [1]
Cholinesterase inhibitors do not work in FTD and may worsen behaviour — this is a frequent exam point and a frequent clinical error. Management is symptomatic, centred on behavioural modification, carer education, SSRIs for compulsive or disinhibited behaviour, and the management of motor neuron disease, which coexists in about 10 to 15 percent of FTD patients. [1]
5. Mixed dementia
Mixed dementia — most commonly Alzheimer pathology plus cerebrovascular disease — is the most common real-world diagnosis in patients over 80 and is under-recognised because clinical criteria are designed for the pure subtypes. The patient has features of both — progressive memory loss plus a stepwise component, vascular risk factors, and white matter changes on imaging. Management combines the approaches: a cholinesterase inhibitor plus aggressive vascular risk factor control. [1]
| Feature | Alzheimer | Vascular | Lewy body | Frontotemporal |
|---|---|---|---|---|
| Onset | Insidious | Often stepwise | Insidious, fluctuates | Insidious |
| Course | Gradual, progressive | Stepwise or gradual | Fluctuating day to day | Gradual, progressive |
| Dominant domain | Recent memory | Executive, processing speed | Attention, visuospatial | Behaviour, language |
| Hallmark | Memory loss, naming | Stepwise, focal signs, gait | Hallucinations, fluctuation, parkinsonism | Disinhibition, apathy, PPA |
| Typical age | Over 65 | Over 70 | Over 65 | 45 to 65 |
| Imaging | Hippocampal atrophy | Infarcts, white matter changes | Relatively preserved; DAT-SPECT low | Frontotemporal atrophy |
| Cholinesterase inhibitor | Yes (first-line) | Modest benefit | Yes (particularly effective) | No — may worsen behaviour |
Mild cognitive impairment — the prevention frontier
Mild cognitive impairment is the zone between normal ageing and dementia: objective cognitive impairment on testing, with preserved independence in daily activities, not explained by delirium or another mental disorder. It may be amnestic (memory-predominant, the highest-risk subtype for progression to Alzheimer) or non-amnestic (affecting attention, language, or executive function, more often progressing to vascular or frontotemporal pathology). [1]
The critical number: patients with MCI convert to dementia at about 10 to 15 percent per year (Petersen 2011, PMID 21651394), against a background rate of 1 to 2 percent per year in cognitively normal older adults. This makes MCI the population every prevention trial targets. [1]
Management of MCI is non-pharmacological. Cholinesterase inhibitors do not prevent conversion and are not recommended. The evidence-based interventions are: [1]
- Vascular risk factor control — blood pressure, diabetes, lipids, atrial fibrillation.
- Physical exercise — the single intervention with the most consistent evidence for cognitive benefit.
- Cognitive stimulation and engagement — mentally and socially stimulating activity.
- Hearing and vision correction — untreated hearing loss is now a major recognised modifiable risk factor.
- Sleep assessment — obstructive sleep apnoea and chronic insomnia accelerate decline.
- Depression treatment — depression may be a prodrome, a contributor, or both.
- Medication review — reduce anticholinergic and sedative burden. [1]
The FINGER trial (Ngandu 2015, PMID 25771249) was the landmark randomised trial demonstrating that a two-year multidomain intervention — diet, exercise, cognitive training, and vascular risk monitoring — improved cognition in at-risk older adults. It is the proof-of-concept that dementia is partly preventable. [1]
Prevention — the 12 modifiable risk factors
The 2020 Lancet Commission (Livingston 2020, PMID 32738937) concluded that up to 40 percent of dementia cases could be prevented or delayed by modifying 12 risk factors, which together account for that proportion of population-attributable risk. The 2024 update added two more (uncorrected vision loss and high LDL cholesterol), raising the estimate to 45 percent. [1]
The 12 factors, grouped by life stage: [1]
| Life stage | Risk factor | Population-attributable risk |
|---|---|---|
| Early life | Low education (less than secondary) | 7 percent |
| Midlife | Hearing loss | 8 percent |
| Traumatic brain injury | 3 percent | |
| Hypertension | 2 percent | |
| Obesity | 1 percent | |
| Excess alcohol (more than 21 units per week) | 1 percent | |
| Smoking | 5 percent | |
| Diabetes | 1 percent | |
| Depression | 4 percent | |
| Social isolation | 4 percent | |
| Later life | Air pollution | 2 percent |
Examiner point: The single largest modifiable risk factor is hearing loss in midlife (8 percent population-attributable risk). Hearing aid use is associated with reduced cognitive decline — this is now a public health message, not a niche neurology fact. The exam expects you to know that dementia prevention is not a single drug but a life-course strategy targeting vascular, sensory, lifestyle, and psychosocial factors. [1]
Assessment — the structured cognitive workup

The dementia assessment has four pillars: history (with collateral), cognitive testing, functional assessment, and the exclusion of reversible causes. [1]
1. Collateral history
This is the single most informative element. From the family member or carer, establish: [1]
- The baseline — what was the patient like two to five years ago, in cognition, function, and personality?
- The onset — when did you first notice a change? Was it gradual (Alzheimer, FTD), sudden or stepwise (vascular), or fluctuating from the start (Lewy body)?
- The domains affected — memory, language, navigation, judgement, personality, self-care.
- The functional impact — can they manage finances, medications, transport, cooking, shopping, phone use, housework (IADLs)? Dressing, bathing, toileting, feeding, transferring (ADLs)?
- The behavioural symptoms — agitation, aggression, wandering, hallucinations, delusions, depression, anxiety, apathy, sleep disturbance, eating changes, sexual disinhibition.
- The safety risks — driving, cooking, wandering, financial exploitation, medication errors, falls. [1]
A structured informant questionnaire — such as the IQCODE (Informant Questionnaire on Cognitive Decline in the Elderly) or the AD8 — increases reliability and is recommended. [1]
2. Cognitive testing
| Tool | Time | Cutoff | Strengths | Limitations |
|---|---|---|---|---|
| MMSE | 5 to 10 min | 24 out of 30 | Widely known, tracks decline over time | Insensitive to MCI and executive dysfunction; ceiling effect in educated patients; affected by education, language, culture; copyright restrictions |
| MoCA | 10 to 15 min | 26 out of 30 | Sensitive to MCI (90 percent in original validation); tests executive, attention, language, abstraction, recall, orientation | Education adjustment (add 1 point if 12 years or fewer of education); some practice effect; free for clinical use (licence required for some digital forms) |
| ACE-III | 15 to 20 min | 82 out of 100 | Tests five domains (attention, memory, fluency, language, visuospatial); good at subtype differentiation (FTD vs Alzheimer); single composite score | Longer; less widely known; English-validated primarily |
The MoCA (Nasreddine 2005, PMID 15817019) is the recommended first-line screening tool in the outpatient memory clinic because of its sensitivity to early and mild impairment, particularly in the executive and attentional domains that the MMSE misses. The clock-drawing test (embedded in both MoCA and ACE-III) is a rapid, culture-fair screen for executive and visuospatial function — ask the patient to draw a clock with all the numbers and set the hands to ten past eleven. [1]
Examiner point: A normal MMSE does not exclude early dementia or MCI. The MoCA is the more sensitive tool and is the expected answer when the question is "best cognitive screening test for mild cognitive impairment." [1]
3. Functional assessment
Document IADLs and ADLs explicitly. The loss of IADLs (finances, medications, transport) marks the transition from MCI to dementia. The Lawton IADL scale and the Katz ADL index are the standard tools. [1]
4. Mental state and physical examination
- Mental state: mood (PHQ-9 or GDS for depression screen — to exclude pseudodementia), insight, any thought disorder or hallucinations.
- Neurological: focal signs (stroke, tumour), parkinsonism (DLB, Parkinson disease dementia, vascular), gait disorder (normal pressure hydrocephalus, vascular), primitive reflexes (frontal release — grasp, palmar-mental), eye movements (progressive supranuclear palsy).
- General: vascular signs, signs of systemic disease, hearing and vision. [1]
Investigations — exclude the reversible causes
Every dementia workup has one job at its core: exclude the reversible causes and the mimics before settling on a neurodegenerative diagnosis. [1]
First-line investigations (every patient)
| Test | What you are excluding |
|---|---|
| Full blood count | Anaemia, infection |
| Urea, electrolytes, creatinine, calcium, glucose, LFTs | Uraemia, hypercalcaemia, hepatic encephalopathy, diabetes |
| TSH | Hypothyroidism — a classic, reversible mimic |
| Vitamin B12 and folate | B12 deficiency — causes cognitive impairment that may be partially reversible; check even without anaemia or macrocytosis |
| Syphilis serology (TPHA or RPR) | Neurosyphilis — now uncommon but the textbook reversible cause; check in high-risk groups or if the picture is atypical |
| HIV serology (if risk factors) | HIV-associated neurocognitive disorder |
| CT or MRI brain | Structural lesions — tumour, subdural haematoma, normal pressure hydrocephalus — and the atrophy and vascular pattern that support a subtype |
| Urinalysis | Infection (a precipitant of delirium on dementia, and a reversible contributor) |
| ECG | Cardiac comorbidity; baseline before cholinesterase inhibitor (bradycardia risk) |
| Depression screen (GDS or PHQ-9) | Pseudodementia |
Second-line and specialised investigations
| Test | Indication |
|---|---|
| MRI brain (preferred over CT) | Subtype differentiation — hippocampal atrophy (Alzheimer), white matter and lacunes (vascular), frontotemporal atrophy (FTD), posterior atrophy (posterior cortical atrophy, a visual variant of Alzheimer) |
| CSF amyloid-beta and tau | Younger-onset dementia, atypical presentation, or where the diagnosis is uncertain; low amyloid-beta 1-42 with elevated tau supports Alzheimer |
| Dopamine transporter (DAT) SPECT | Distinguishing DLB (low uptake) from Alzheimer (normal) when the clinical picture is ambiguous |
| FDG-PET | Pattern of hypometabolism — temporoparietal (Alzheimer), frontotemporal (FTD), occipital (DLB) |
| Amyloid-PET | Emerging into clinical use; supports Alzheimer pathology; used in workup for anti-amyloid therapy |
| Polysomnography | Confirmation of REM sleep behaviour disorder in suspected DLB |
| Cognitive reserve and neuropsychological testing | Complex or early cases, high-functioning patients, subtype differentiation, medico-legal or capacity assessment |
| Autoimmune encephalitis panel, paraneoplastic antibodies, 14-3-3 protein (CJD) | Rapidly progressive course (weeks to months) — a different differential entirely |
Clinical rule: A rapidly progressive dementia — decline over weeks to a few months — is not typical Alzheimer. It demands urgent MRI and CSF to exclude Creutzfeldt-Jakob disease, autoimmune or paraneoplastic limbic encephalitis, and rapidly progressive Alzheimer or DLB. The course, not the cognitive profile, is the red flag. [1]
Management
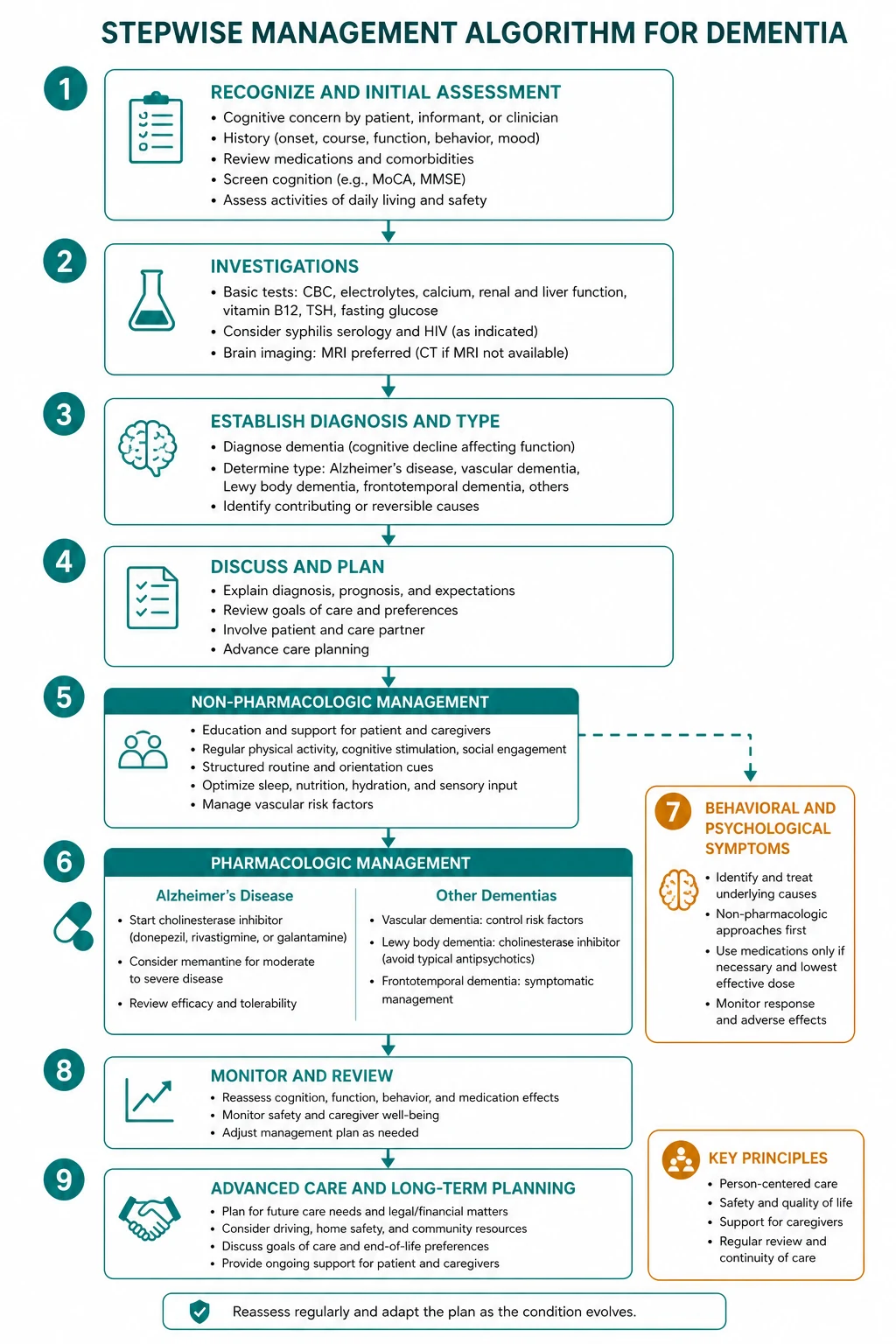

Dementia management is built on five pillars: [1]
- Non-pharmacological foundation — cognitive stimulation, exercise, social engagement, carer education.
- Cognitive enhancers — cholinesterase inhibitors and memantine, selected by subtype and severity.
- Vascular and comorbidity management — the second disease is as important as the first.
- Behavioural and psychological symptom (BPSD) management — the escalation ladder, with antipsychotics last.
- Advanced care planning, driving, capacity, and carer support — the longitudinal, human work. [1]
Pillar 1 — Non-pharmacological foundation
The evidence-based non-pharmacological interventions are the foundation and should be offered to every patient: [1]
- Cognitive stimulation therapy (CST) — structured group sessions of mentally stimulating activities; the one non-drug intervention with randomised-trial evidence for cognitive benefit in mild to moderate dementia.
- Physical exercise — aerobic and resistance exercise improves cognition, function, mood, and sleep, and may slow decline.
- Social engagement — isolation accelerates decline; day programmes, community groups, and family involvement are therapeutic.
- Carer education and skills training — teaches communication, behavioural management, and structured routines. Carer intervention reduces institutionalisation.
- Hearing and vision correction — hearing aids and glasses reduce cognitive load and improve engagement.
- Environmental modification — orientation aids (clocks, labels, signs), safety modifications (stove alarms, grab rails), and simplification of routines.
- Sleep hygiene and management — bright light therapy, regular daytime activity, avoidance of sedatives. [1]
Pillar 2 — Cognitive enhancers
| Drug | Class | Indication | Starting dose | Titration | Target dose | Key side effects |
|---|---|---|---|---|---|---|
| Donepezil | Cholinesterase inhibitor | Mild, moderate, severe Alzheimer; DLB | 5 mg orally at night | Increase to 10 mg after 4 weeks; 23 mg for advanced | 5 to 10 mg daily (up to 23 mg) | Nausea, diarrhoea, bradycardia, syncope, vivid dreams, weight loss |
| Galantamine | Cholinesterase inhibitor (plus nicotinic modulation) | Mild to moderate Alzheimer | 4 mg twice daily or 8 mg prolonged-release daily | Increase every 4 weeks to 8 mg, then 12 mg twice daily | 8 to 12 mg twice daily (16 to 24 mg prolonged-release daily) | Nausea, vomiting, diarrhoea, bradycardia |
| Memantine | NMDA receptor antagonist (low-affinity, non-competitive) | Moderate to severe Alzheimer; can combine with a cholinesterase inhibitor | 5 mg daily | Increase weekly by 5 mg to 10 mg twice daily (or 20 mg prolonged-release daily) | 10 mg twice daily (20 mg daily) | Dizziness, headache, confusion (usually mild); dose-reduce in moderate-severe renal impairment |
The clinical reality (Birks 2006, PMID 16437532; McShane 2019, PMID 30891742): cholinesterase inhibitors produce a modest, symptomatic benefit — a mean improvement of about 2 to 3 points on the ADAS-cog or 1 to 2 points on the MMSE, sustained for 6 to 12 months before the underlying decline resumes. They do not halt or cure disease. Some patients show a clear functional benefit; others show none; the response is individual and unpredictable. A trial of three to six months, with a structured assessment of function and cognition, is the standard approach, with continuation if there is perceived benefit or stabilisation and discontinuation if there is decline, intolerance, or no effect. [1]
The NICE TA217 algorithm (UK) gates the drugs by severity, using the MMSE: cholinesterase inhibitors for mild (MMSE 10 to 20) and moderate Alzheimer; memantine for moderate (MMSE 10 to 14) and severe (MMSE under 10) Alzheimer, with the option to combine. In Australia (PBS), donepezil, rivastigmine, and galantamine are subsidised for mild to moderate Alzheimer (and rivastigmine for DLB and Parkinson disease dementia), and memantine for moderate to severe Alzheimer; the PBS requires an initial and a continuation assessment. [1]
Subtype-specific prescribing: [1]
- Alzheimer — cholinesterase inhibitor first-line; add or switch to memantine as the disease progresses; combination therapy is common in moderate to severe disease.
- Vascular dementia — cholinesterase inhibitor has modest benefit; the priority is vascular risk factor control. Memantine has a small effect.
- Lewy body dementia — cholinesterase inhibitors are particularly effective (rivastigmine has the strongest evidence); memantine may help; avoid antipsychotics absolutely.
- Frontotemporal dementia — cholinesterase inhibitors do not work and may worsen behaviour (worsened agitation, autonomic side effects); memantine has no established benefit. Management is behavioural and symptomatic.
- Mixed dementia — a cholinesterase inhibitor plus vascular risk factor control. [1]
Examiner trap: The most common pharmacology error is prescribing a cholinesterase inhibitor for frontotemporal dementia. It does not help and may worsen the behavioural symptoms. The correct answer for FTD is no cognitive enhancer — manage behaviour with SSRIs, structure, and carer support. [1]
Pillar 3 — Vascular and comorbidity management
In every dementia patient, the second disease is as important as the first. Aggressive management of hypertension (target under 130/80 in most), diabetes (HbA1c individualised, avoiding hypoglycaemia which acutely worsens cognition), atrial fibrillation (anticoagulation unless contraindicated — the dementia patient still benefits from stroke prevention), lipids, heart failure, and chronic kidney disease slows the vascular component of mixed dementia and prevents the strokes that produce stepwise decline. [1]
Medication review is a treatment in itself. The anticholinergic and sedative burden of many older patients' regimens (oxybutynin, tricyclics, antihistamines, benzodiazepines, opioids, antispasmodics) directly worsens cognition. Use the Anticholinergic Burden Scale or the Drug Burden Index and deprescribe systematically. The phrase to use with the family: "One of the most effective treatments for your mother's memory is to stop some of her tablets." [1]
Pillar 4 — BPSD: behavioural and psychological symptoms
Behavioural and psychological symptoms of dementia (BPSD) — agitation, aggression, wandering, hallucinations, delusions, depression, anxiety, apathy, sleep disturbance, sexual disinhibition, and eating problems — affect the majority of dementia patients at some point, are the single commonest driver of institutionalisation and carer breakdown, and are the area where the most prescribing harm is done. [1]
The escalation ladder (the structure every answer must follow): [1]
Step 1 — Search for and treat the precipitant. BPSD is almost never spontaneous. The common precipitants are pain, infection (urinary tract, chest), constipation, urinary retention, hunger or thirst, a change in environment, a drug (newly added anticholinergic, sedative, or opioid, or withdrawal of a long-term drug), sensory deprivation (missing glasses or hearing aids), fear or misunderstanding, and intercurrent delirium. A patient with dementia who becomes agitated is delirious until proven otherwise — the same DELIRIUM mnemonic applies. [1]
Step 2 — Non-pharmacological management. Reassurance, redirection, validation (acknowledge the emotion without arguing with the belief), structured routine, familiar environment, reducing overstimulation (noise, clutter, crowds), one-to-one attention, music, familiar objects, family presence, and the modification of the carer's own approach (slower, calmer, one question at a time). These are the mainstay and should be exhausted before drugs. [1]
Step 3 — Pharmacological treatment, targeted to the symptom, at the lowest dose, for the shortest time. [1]
| Symptom | First-line drug approach | Caution |
|---|---|---|
| Aggression or severe agitation with risk | Risperidone 0.25 to 0.5 mg orally, titrated cautiously, time-limited (PBS restricts to 12 weeks) | Increased mortality and stroke (Schneider 2005, PMID 16234500); review regularly; stop if no benefit; contraindicated in Lewy body dementia |
| Anxiety | SSRI; buspirone in selected cases | Avoid benzodiazepines (worsen cognition, increase falls) |
| Sleep disturbance | Melatonin 2 to 6 mg at night; sleep hygiene; bright light therapy | Avoid benzodiazepines and Z-drugs (zopiclone, zolpidem) — they increase falls, fractures, and cognitive decline |
| Apathy | Cholinesterase inhibitor; structured activity; avoid antipsychotics (worsen) | Stimulants (methylphenidate) are not recommended routinely |
| Wandering | Environmental safety, identification bracelet, GPS tracker, structured activity | No drug has a role |
The dangerous DWE/DCE error: Antipsychotics in dementia carry a black box warning for increased mortality (about 1.6 to 1.7 times placebo; Schneider 2005, PMID 16234500) and an increased risk of stroke. They should be reserved for severe distress or danger, used at the lowest dose for the shortest time (ideally under 12 weeks), reviewed regularly, and stopped if ineffective. In Lewy body dementia, they are absolutely contraindicated — a single dose can trigger catastrophic rigidity, hyperthermia, and irreversible decline (neuroleptic sensitivity). If you must treat psychosis in DLB, use a cholinesterase inhibitor first and quetiapine with extreme caution only if essential. [1]
Pillar 5 — Advanced care planning, driving, capacity, carer support
This is the longitudinal, human work of dementia medicine, and it is where the consultation earns its value. [1]
Advanced care planning should begin early, while the patient still has capacity. Cover: [1]
- Values and goals — what matters most to the patient as the disease progresses.
- Future care preferences — home, supported accommodation, residential care; preferences around hospitalisation and resuscitation.
- Appointment of a substitute decision-maker — enduring power of attorney (financial), enduring guardianship (health and lifestyle), and an advance care directive.
- Review and documentation — revisit at each stage transition and after any acute illness. [1]
Capacity is decision-specific and time-specific. A patient with mild to moderate dementia may retain capacity to make a will, to appoint a power of attorney, and to consent to treatment, while lacking capacity to manage complex finances or to drive safely. The functional test: can the patient understand the relevant information, retain it long enough, weigh it as part of a decision, and communicate the decision? Capacity fluctuates — assess at the best time of day (usually morning), free from intercurrent delirium. [1]
Driving is a high-stakes decision. Dementia impairs the judgement, reaction time, visuospatial function, and attention required for safe driving. In Australia, the patient (and in some states, the doctor) has a legal obligation to report to the licensing authority; most patients require a formal driving assessment (on-road or occupational therapy) as the disease progresses. The conversation should be honest, compassionate, and documented, and should be paired with a plan for alternative transport to preserve autonomy and social engagement. [1]
Carer support is not optional. Carers of dementia patients have high rates of depression, anxiety, sleep disturbance, and physical illness, and carer burnout is the commonest reason for institutionalisation. Offer: [1]
- Education about the disease, the trajectory, and the management.
- Respite — in-home, day-programme, and residential respite.
- Support groups and peer contact.
- Carer assessment — a carer stress scale or the Zarit Burden Interview.
- Psychological support — CBT, counselling, problem-solving therapy.
- Practical help — community aged care packages, home modification, financial advice. [1]
Differentials — the four distinctions
The dementia diagnosis requires the exclusion of four mimics: [1]
1. Delirium. Acute, fluctuating, inattention, altered consciousness — versus chronic, progressive, preserved early attention, normal consciousness until late. The single most important question: is this an acute change from the patient's baseline? If yes, it is delirium until proven otherwise, even in a patient with known dementia (delirium superimposed on dementia is the commonest inpatient scenario). The collateral history and the CAM settle it. [1]
2. Depression (pseudodementia). Depression in older adults can produce cognitive impairment that mimics dementia — the "pseudodementia" problem. The distinguishing features: [1]
| Feature | Depression (pseudodementia) | Dementia |
|---|---|---|
| Onset | Subacute, over weeks to months | Insidious, over months to years |
| Course | Diurnal variation (often worse in morning) | Stable or slowly progressive |
| Patient effort | Gives up easily, answers "I don't know", poor effort | Tries hard, makes errors, confabulates |
| Orientation | Usually preserved | Often impaired |
| Attention | Usually preserved | Often impaired (late) |
| Memory | Variable, inconsistent | Consistently impaired, recent worse than remote |
| Biological features | Prominent (low mood, anhedonia, sleep, appetite, weight) | May coexist but less central |
| GDS / PHQ-9 | Strongly positive | May be positive |
The trap: depression and dementia coexist in up to 40 percent of cases, and depression may be a prodrome of dementia. The clinical rule is to screen for and treat depression in every patient with cognitive impairment and to reassess cognition after the mood has improved. The old teaching "give an SSRI and see if the cognition improves" is not sufficient — treat the depression, but continue to monitor for the dementia. [1]
3. The reversible causes. B12 deficiency, hypothyroidism, neurosyphilis, HIV, normal pressure hydrocephalus, subdural haematoma, depression, medications (anticholinergics, sedatives, polypharmacy), alcohol-related cognitive impairment, and sleep apnoea. These are excluded by the first-line workup above. Normal pressure hydrocephalus deserves special mention — the triad of gait disturbance (typically a magnetic, shuffling, broad-based gait), urinary incontinence, and cognitive decline (executive-predominant), with communicating hydrocephalus on imaging and a positive lumbar drain or tap test. It is partially reversible with shunting, and it is missed when attributed to Alzheimer, Parkinson, or vascular disease. [1]
4. Age-related cognitive decline and the worried well. Some older patients present with subjective memory complaints but normal testing — the "worried well." Reassurance, baseline testing, lifestyle advice, and follow-up are appropriate. The risk of progression to MCI and dementia is higher than in the general population, so do not dismiss them — review annually. [1]
Prognosis and the natural history
The median survival from diagnosis of dementia is about 4 to 8 years, but this varies widely by subtype, age at onset, and comorbidity. Alzheimer disease runs a course of 8 to 12 years from first symptom to death; vascular dementia is highly variable; Lewy body dementia has a slightly shorter survival; frontotemporal dementia runs 6 to 10 years (shorter if motor neuron disease coexists). [1]
The trajectory of functional loss is broadly predictable, moving from IADL loss (finances, transport, medications) through ADL loss (dressing, bathing, toileting) to complete dependency, loss of mobility, loss of swallowing, and death — most commonly from aspiration pneumonia, but also from other infections, pressure injuries, and the complications of immobility (Mitchell 2009, PMID 19828530). [1]
The family should be prepared for the late-stage complications: recurrent infections, weight loss, dysphagia, contractures, pressure injuries, seizures (in 10 to 20 percent of advanced Alzheimer), and the eventual transition to palliative care. The decision to withhold antibiotics or hospitalisation in advanced dementia, made in advance and with the family, is a recognised and ethical component of end-of-life care. [1]
How this is examined
DWE MCQ
The DWE tests dementia through clinical vignettes that probe: [1]
- Subtype discrimination — a younger patient with personality change (FTD), an older patient with fluctuating cognition and visual hallucinations (DLB), a stepwise decline with focal signs (vascular), a patient with memory loss and naming difficulty (Alzheimer).
- The best cognitive screening test — the MoCA, not the MMSE, for MCI.
- The reversible-cause workup — B12, TSH, and imaging in every case.
- The pharmacology — cholinesterase inhibitors for Alzheimer and DLB, memantine for moderate to severe, no cognitive enhancer for FTD.
- The BPSD trap — non-pharmacological first, risperidone only for severe aggression time-limited, absolute contraindication to antipsychotics in DLB.
- The dangerous drug — an antipsychotic in a patient who turns out to have DLB.
- The rapidly progressive course — the differential changes to CJD, autoimmune encephalitis. [1]
DCE long case
The long case will be a multi-morbid elderly patient with dementia plus cardiac failure, atrial fibrillation, diabetes, falls, polypharmacy, and a recent admission with delirium. You will be expected to present a structured problem list, an integrated management plan that addresses each problem, and a thoughtful discussion of capacity, driving, and the family. The dementia is the thread that runs through the whole case. [1]
DCE short case
The short case will ask you to perform a cognitive assessment. You will be expected to present a systematic routine — alertness, attention (months of the year backwards), orientation, registration and recall, language, clock-drawing, executive function, mood, insight — and to present the findings, the likely subtype, and the differential. The MoCA or ACE-III structure is the model. [1]
Key references
Livingston G, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020;396:413-446 (PMID 32738937). Nasreddine ZS, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc 2005;53:695-699 (PMID 15817019). Petersen RC. Clinical practice: mild cognitive impairment. N Engl J Med 2011;364:2227-2234 (PMID 21651394). Birks J. Cholinesterase inhibitors for Alzheimer's disease. Cochrane Database Syst Rev 2006 (PMID 16437532). McShane R, et al. Memantine for dementia. Cochrane Database Syst Rev 2019 (PMID 30891742). Schneider LS, et al. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis. JAMA 2005;294:1934-1943 (PMID 16234500). McKeith IG, et al. Diagnosis and management of dementia with Lewy bodies: fourth consensus report of the DLB Consortium. Neurology 2017;89:88-100 (PMID 28592453). Rascovsky K, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain 2011;134:2456-2477 (PMID 21810890). Hsieh S, et al. Validation of the Addenbrooke's Cognitive Examination III in frontotemporal dementia and Alzheimer's disease. Dement Geriatr Cogn Dis Extra 2013;3:172-181 (PMID 23949210). Ngandu T, et al. A 2 year multidomain intervention (FINGER): a randomised controlled trial. Lancet 2015;385:2255-2263 (PMID 25771249). Mitchell SL, et al. The clinical course of advanced dementia. N Engl J Med 2009;361:1529-1538 (PMID 19828530). Guideline sources: NICE TA217 (cognitive enhancers in Alzheimer), NICE NG97 (dementia assessment, management and support), WHO Global action plan on dementia 2017-2025. [1]
References
- [1]Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission Lancet, 2020.PMID 32738937
- [2]Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment J Am Geriatr Soc, 2005.PMID 15817019
- [3]Petersen RC Clinical practice. Mild cognitive impairment N Engl J Med, 2011.PMID 21651394
- [4]Birks J Cholinesterase inhibitors for Alzheimer's disease Cochrane Database Syst Rev, 2006.PMID 16437532
- [5]McShane R, Westby MJ, Roberts E, et al. Memantine for dementia Cochrane Database Syst Rev, 2019.PMID 30891742
- [6]Schneider LS, Dagerman KS, Insel P Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials JAMA, 2005.PMID 16234500
- [7]McKeith IG, Boeve BF, Dickson DW, et al. Diagnosis and management of dementia with Lewy bodies: Fourth consensus report of the DLB Consortium Neurology, 2017.PMID 28592453
- [8]Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia Brain, 2011.PMID 21810890
- [9]Hsieh S, Schubert S, Hoon C, et al. Validation of the Addenbrooke's Cognitive Examination III in frontotemporal dementia and Alzheimer's disease Dement Geriatr Cogn Disord, 2013.PMID 23949210
- [10]Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial Lancet, 2015.PMID 25771249
- [11]Mitchell SL, Teno JM, Kiely DK, et al. The clinical course of advanced dementia N Engl J Med, 2009.PMID 19828530