Phys · geriatric
Elder Abuse and Safeguarding
Also known as elder mistreatment · elder neglect · abuse of older adults · safeguarding older people · financial exploitation of elders · carer abuse · institutional elder abuse · EASI · Elder Abuse Suspicion Index · Hwalek-Sengstock · HSEAST · adult safeguarding
Consultant-physician-depth guide to elder abuse and safeguarding for FRACP DWE and DCE — WHO definition, the six types of abuse (physical, psychological, financial, sexual, neglect, discriminatory), the 1-in-6 prevalence and severe underreporting, risk factors (dementia, carer stress, social isolation), the red flags of abuse, the EASI and Hwalek-Sengstock screening tools, the interview-alone principle, capacity assessment, mandatory reporting by jurisdiction, legal interventions (AVO, tribunal guardianship, financial management), support services, and the ethical balance of autonomy versus protection.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Elder Abuse and Safeguarding

The answer first
Elder abuse is a single or repeated act — or a lack of appropriate action — occurring within any relationship where there is an expectation of trust, which causes harm or distress to an older person (WHO, Toronto Declaration 2002). The perpetrator is almost always someone the older person relies on: an adult child, a spouse, a paid carer, or a person holding a power of attorney. It is vastly under-recognised — approximately 1 in 6 older people in community settings have experienced abuse [1], but only an estimated 1 in 24 cases reach the attention of authorities.
The four rules that govern your response to suspected elder abuse: [1]
- Always interview the patient alone. If a carer or family member is in the room, the patient will not disclose. This is the single most important — and most commonly missed — step in the assessment.
- Assess capacity first. Your management hinges on whether the older person has the capacity to understand the risk, weigh the options, and make and communicate a decision about their safety. A capacitous person has the right to refuse intervention, however unwise that refusal may seem.
- Ensure immediate safety. If the person is in imminent danger, admission to hospital or emergency relocation is justified — capacity permitting, or under the doctrine of necessity if capacity is impaired.
- Report and refer. Know your jurisdiction's mandatory reporting obligations, involve social work and the safeguarding or elder-abuse service early, and document meticulously — your notes may become the evidence in a guardianship tribunal or criminal proceeding. [1]
DWE high-yield trap: When asked "the most appropriate initial step in suspected elder abuse," the answer is almost always interview the patient alone and assess capacity — not "call the police" or "contact the family." If the options include a structured multidisciplinary safeguarding response, that is usually the best next step after safety and capacity are established. [1]
Definition — WHO and the expectation of trust
The WHO definition, adopted in the 2002 Toronto Declaration and reaffirmed in subsequent WHO resolutions, has three components that each carry clinical weight [6]:
- A single or repeated act, or lack of appropriate action. Abuse can be a one-off assault (a slap) or a sustained pattern (daily humiliation, chronic financial drain). The "lack of appropriate action" component captures neglect — the failure to provide care that the person needs and is entitled to.
- Within any relationship where there is an expectation of trust. This is the defining element. Elder abuse is not a random mugging — it is perpetrated by someone the older person depends on or trusts. This includes family members, friends, neighbours, paid carers, and professionals. It explicitly includes financial advisors, attorneys, and guardians. The trust relationship is what makes elder abuse a betrayal, not merely an assault.
- Causes harm or distress to an older person. The harm may be physical, psychological, financial, sexual, or the harm of unmet needs. "Distress" captures the psychological injury even without physical marks. [1]
The age threshold varies — the WHO uses 60 years, some jurisdictions use 65, some use "vulnerable adult" definitions that are not age-bound. In clinical practice, the definition applies to any older person in a relationship of dependency or trust where harm is occurring. [1]
Exam point: The "expectation of trust" criterion distinguishes elder abuse from a stranger assault. An older person robbed by an intruder is a victim of crime, but not (by this definition) of elder abuse. The distinction matters because the safeguarding and legal response is different — and because abuse within a trust relationship is far more common, more insidious, and harder to detect. [1]
Types of elder abuse
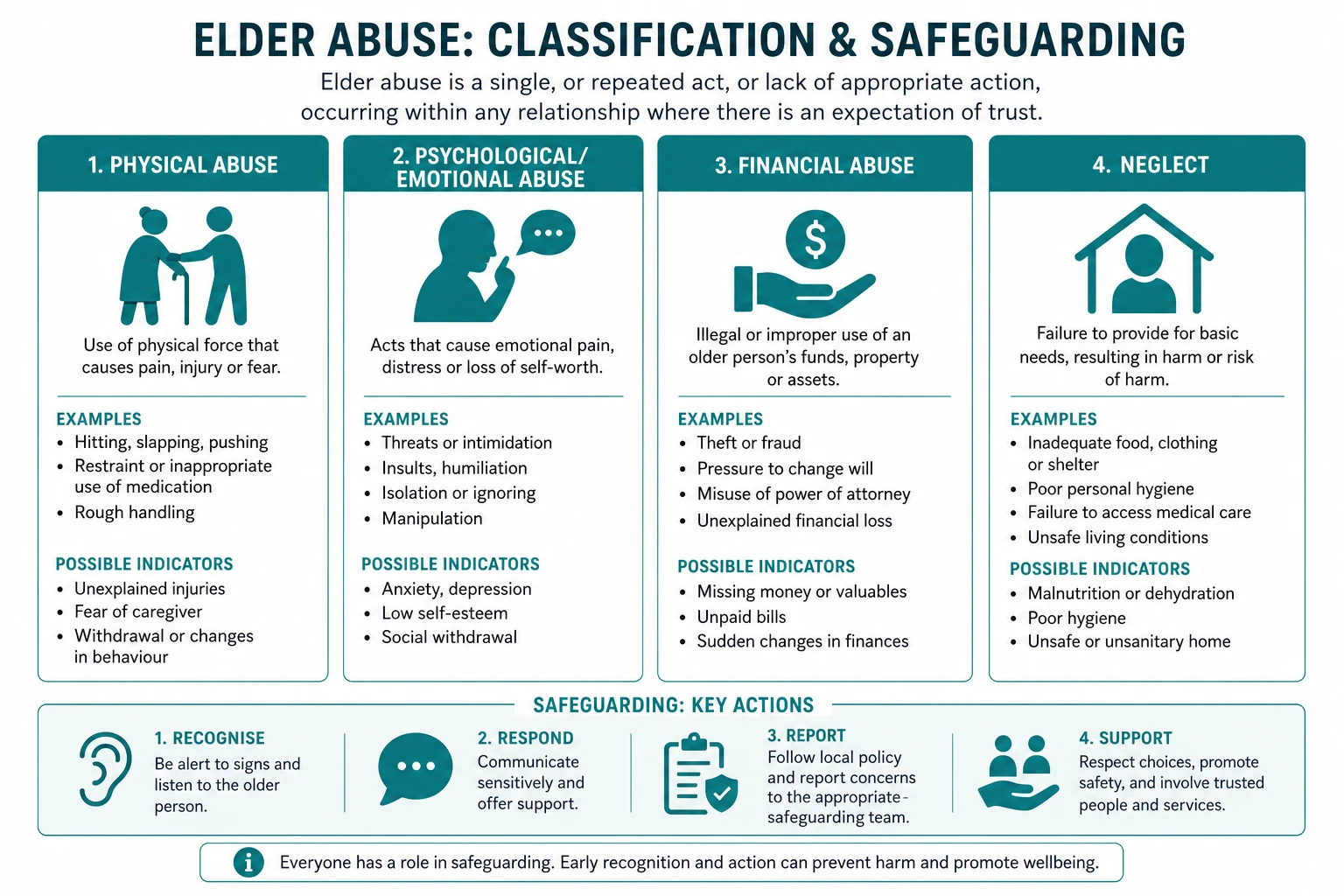

There are six recognised types. In practice, types co-occur — a physically abused woman is almost certainly also being psychologically abused, and a financially exploited man may be neglected as well. [1]
Physical abuse
The intentional infliction of physical pain or injury, or the use of physical restraint that is not clinically justified. Behaviours include hitting, slapping, pushing, shaking, burning, inappropriate use of physical or chemical restraints (over-sedation to keep the patient quiet), and force-feeding. Clinical features: bruises (especially in patterns suggesting grip — upper arms, wrists, neck — or in unusual locations such as inner thighs, axillae, or the trunk), fractures, burns (particularly immersion burns with a "glove and stocking" distribution), lacerations, and bite marks. A key clue is an injury inconsistent with the stated mechanism — a bruise on the upper inner arm attributed to a fall does not fit. [1]
Psychological or emotional abuse
The infliction of mental anguish, fear, or distress through verbal or non-verbal acts. This is the most common type but the hardest to detect because it leaves no physical mark. Behaviours include verbal abuse (name-calling, shouting, belittling), intimidation, humiliation, threats (to institutionalise the person, to harm them, to harm a pet), isolation (preventing contact with family, friends, or services), and treating the person like a child. Clinical features: the patient appears fearful, withdrawn, deferential to the carer, hesitant to speak freely, or depressed. They may flinch, avoid eye contact, or show a marked change in behaviour when the carer enters the room. [1]
Financial or material abuse
The illegal, unauthorised, or improper use of an older person's money, property, or assets. This is the most commonly reported type in many jurisdictions and is particularly associated with cognitive impairment. Behaviours include unauthorised withdrawals from bank accounts, coercion to change a will or property title, misuse of a power of attorney (an attorney is a fiduciary and must act in the person's best interests), pressure to sign documents the person does not understand, theft of cash or valuables, and scam exploitation (the carer may be the scammer, or may fail to protect the older person from scammers). Clinical features: unpaid bills despite adequate income, sudden inability to afford necessities, unexplained transfers or withdrawals, the carer who is "looking after the finances" and will not allow the patient access to their own money, and a mismatch between the person's assets and their living conditions. [1]
Sexual abuse
Non-consensual sexual contact of any kind. This is the least reported type, owing to profound shame and the frequent cognitive impairment of the victim. Behaviours include unwanted touching, coerced nudity, sexual assault, and rape. Clinical features: unexplained genital or anal injury or bleeding, new sexually transmitted infection, bruising on the inner thighs or breasts, torn or stained underclothing, and marked fear or distress during personal care or physical examination. Sexual abuse in residential aged care (resident-to-resident or staff-to-resident) is a particular concern. [1]
Neglect
The failure to fulfil a care obligation, resulting in unmet needs. The critical clinical distinction is between active and passive neglect: [1]
- Active neglect is the deliberate withholding of care. The carer intentionally withholds food, medication, hydration, hygiene, warmth, or medical attention. It is a form of abuse in its own right.
- Passive neglect is the unintentional failure to meet the person's needs, due to carer stress, ignorance, the carer's own illness or cognitive impairment, or inadequate resources. The carer is not malicious but is overwhelmed or untrained. [1]
The distinction matters because the management is different — active neglect may require removal of the carer and legal action, while passive neglect may respond to carer education, respite, and support services. But the harm to the older person is the same regardless of intent, and the threshold for intervention is the same: the person is being harmed. [1]
Clinical features of neglect: malnutrition, dehydration, poor hygiene, infestations (scabies, lice), overgrown nails, untreated pressure injuries (especially in a mobile patient — pressure injuries in a bed-bound patient may be unavoidable despite good care; pressure injuries in a mobile patient suggest neglect), medication non-adherence (the carer is not administering prescribed medications), contractures from lack of positioning or movement, and failure to seek medical attention for treatable conditions. [1]
Discriminatory abuse
Abuse motivated by ageist or other prejudicial attitudes — treating the older person as less deserving of care, dignity, or resources because of their age. This manifests as systematic denial of medical treatment ("they are too old for this"), patronising language ("dearie," "good girl"), institutional practices that strip dignity, and age-based rationing. While harder to prosecute, it underlies much of the systemic neglect that occurs in under-resourced care settings. [1]
DCE long-case rule: When presenting a long case involving suspected abuse, name the type or types explicitly in the problem list — "Problem 1: suspected financial and psychological abuse by the daughter with enduring power of attorney" — so the management plan is structured around the specific harm and the specific perpetrator relationship. [1]
Epidemiology — the hidden epidemic
The landmark systematic review and meta-analysis by Yon et al (2017), covering 52 studies across 28 countries, estimated that 15.7 percent of people aged 60 and older in community settings — approximately 1 in 6 — had experienced some form of abuse in the past year [1]. This represents roughly 141 million older adults worldwide at the time. The US National Elder Mistreatment Study (Acierno et al, 2010) found a past-year prevalence of approximately 10 percent for at least one type of abuse, with financial abuse by family members (5.2 percent) and potential neglect (5.1 percent) the most common [3].
The critical epidemiological fact: only an estimated 1 in 24 cases reaches authorities. The reasons for underreporting are systemic and patient-level: [1]
- Shame and stigma — the victim feels embarrassed to admit that their own child is stealing from or hitting them.
- Fear of retaliation or abandonment — the perpetrator may be the only person providing care; disclosure risks institutionalisation or worse treatment.
- Cognitive impairment — the victim may lack the capacity to report, or their account may be dismissed as unreliable.
- Dependency — the victim relies on the perpetrator for food, shelter, or care, and cannot risk the relationship.
- Isolation — there is no one to tell.
- Lack of awareness — the victim, the family, and sometimes clinicians do not recognise the behaviour as abuse.
- Healthcare failure — clinicians do not ask, or ask in front of the carer, or attribute injuries to falls. [1]
In institutional settings the picture is even worse: a systematic review by Yon et al (2019, Eur J Public Health) found that over 64 percent of care home staff admitted to committing some form of abuse in the past year — mostly psychological neglect and rough handling, but with significant rates of physical and financial abuse as well. [1]
The consequence of this hidden epidemic is that elder abuse is associated with increased mortality, accelerated functional decline, depression, anxiety, and institutionalisation, independent of comorbidity and baseline function. The Lachs et al (1998) 13-year prospective cohort study found that elder mistreatment was associated with a dramatically increased risk of death (9 percent survival in mistreated persons versus 40 percent in non-investigated persons), even after adjusting for comorbidity, cognitive status, and social network [4].
Risk factors
Risk factors operate at three levels — the older person, the carer or perpetrator, and the context. The interaction is key: abuse occurs when a vulnerable person, a stressed or malicious carer, and an isolated context converge. [1]
Older-person risk factors
| Factor | Mechanism |
|---|---|
| Dementia and cognitive impairment | The strongest patient-level risk factor. The person may be unable to report, resist, or remember. Behavioural and psychological symptoms of dementia (agitation, aggression, wandering) place enormous stress on carers, increasing the risk of reactive abuse. |
| Functional dependency | The more dependent the person, the greater the carer burden, and the more opportunity for abuse in the intimate care setting. |
| Behavioural disturbance | Aggression, agitation, and resistance to care can provoke a violent or neglectful response from an unsupported carer. |
| Social isolation | Fewer visitors and less community contact mean fewer observers, fewer checks, and fewer opportunities for disclosure. |
| Incontinence | A major driver of carer stress and a specific risk factor for physical and psychological abuse. |
| Communication difficulty | Aphasia, hearing loss, or language barriers make it harder for the person to report or for concerns to be heard. |
| Recent loss | Bereavement of a spouse (who was a protective presence), or loss of a social network, increases vulnerability. |
Carer and perpetrator risk factors
| Factor | Mechanism |
|---|---|
| Carer stress and burnout | Chronic sleep deprivation, physical strain, emotional exhaustion, and lack of respite erode the carer's capacity to cope. Stress alone does not excuse abuse, but it is a modifiable target for prevention. |
| Mental illness | Depression, anxiety, and personality disorders in the carer increase the risk. |
| Substance misuse | Alcohol abuse is one of the strongest carer-level risk factors for physical and psychological elder abuse. Illicit drug use compounds the risk. |
| Financial dependence on the older person | The "reverse dependency" pattern — the adult child who lives with and is financially supported by the parent — is a potent risk factor for financial exploitation and psychological abuse. |
| History of family violence | A carer who has been violent toward a spouse or children is more likely to be violent toward the older person. Intergenerational cycles of abuse apply. |
Contextual risk factors
- Social isolation of both the older person and the carer — fewer external contacts, less scrutiny.
- Shared living arrangement with the carer — the majority of abuse occurs in the home, and shared living increases opportunity.
- Cultural factors — in some cultures, filial expectations of total care without support create unsustainable carer burden; in others, stigma prevents disclosure.
- Inadequate community services — where respite, home care packages, and carer support are scarce or inaccessible, carer burnout is inevitable. [1]
Clinical rule: The highest-risk scenario is an older person with moderate-to-severe dementia, cared for at home by an adult child with alcohol misuse, financial dependence on the parent, and minimal community support. This pattern should prompt active enquiry, not passive observation. [1]
Clinical assessment — the red flags

The diagnosis of elder abuse is clinical — there is no blood test or scan. The assessment rests on pattern recognition, collateral history, and above all a private interview with the patient. The red flags fall into four domains. [1]
Physical signs
- Unexplained or multiple injuries — bruises, fractures, lacerations, burns.
- Injuries in unusual distributions — inner thighs, axillae, neck, upper inner arms (grip patterns), trunk, buttocks. Injuries from a fall are typically on extensor surfaces (knees, shins, forehead, hands); injuries on flexor or protected surfaces raise suspicion.
- Injury patterns suggesting restraint — linear bruises on wrists or ankles, rope marks, wristband abrasions.
- Pressure injuries in a mobile patient — a Stage 3 or 4 pressure injury in a person who can walk suggests severe neglect of positioning, hygiene, and nutrition.
- Malnutrition and dehydration — weight loss, muscle wasting, loose dentures, dry mucous membranes, without an organic explanation.
- Poor hygiene, infestation, overgrown nails, matted hair — signs that basic care is not being delivered.
- Over-sedation — the patient who is drowsy and unresponsive may be being chemically restrained with unnecessary sedatives or antipsychotics.
- Genital or anal injury, bleeding, or new sexually transmitted infection — raise the possibility of sexual abuse. [1]
History inconsistencies
- Inconsistent histories — the patient and carer give different accounts of how an injury occurred.
- Delayed presentation — an injury or illness that should have been brought to medical attention days or weeks earlier.
- Pattern of recurrent injuries — multiple presentations with injuries, particularly if attributed to falls in a person who is not a recurrent faller.
- Unexplained gap in care — missed medical appointments, unfilled prescriptions, failure to follow through on investigations. [1]
Carer behaviours
- Refusing to leave the room during the clinical interview — this is a major red flag and must be addressed directly.
- Speaking for the patient — answering questions before the patient can, or contradicting the patient's account.
- Controlling behaviour — the carer dominates the consultation, makes decisions for the patient, or physically positions themselves between the patient and the clinician.
- Excessive concern or indifference — the carer who is aggressively attentive (may reflect a need to control the narrative) or, conversely, completely disengaged.
- Apparent financial control — the carer manages all finances and will not allow the patient access to their own money or bank statements. [1]
Environmental and contextual signs
- Poor living conditions relative to the person's known income or assets — squalor, lack of heating, inadequate food, in the home of a person who should be able to afford care.
- Unpaid bills — utilities disconnected, rates unpaid, despite the person having adequate income.
- Missing belongings — jewellery, furniture, or valuables gone from the home.
- Sudden changes to legal documents — a new will, a new power of attorney, or a transfer of property title, particularly when the person's cognition is in question. [1]
DCE exam rule: In any long case involving an older person with an injury, cognitive impairment, or functional decline, you must explicitly state: "I would interview the patient alone to screen for elder abuse, using the EASI or direct enquiry." Failing to mention this is a common exam error. [1]
Screening tools
The Elder Abuse Suspicion Index (EASI)
The EASI (Yaffe et al, 2008, PMID 18928055) is the best-validated physician-administered screening tool for elder abuse [2]. It was developed for use in family practice with cognitively intact older adults (MMSE 24 or above).
Structure — 6 items:
- Questions 1 to 5 are asked of the patient:
- Have you relied on people for any of the following: shopping, banking, or financial matters?
- Has anyone prevented you from getting food, clothes, medication, glasses, hearing aids, or medical care?
- Has anyone been verbally or emotionally cruel to you, or frightened you?
- Has anyone forced you to do things you did not want to do?
- Has anyone taken your money, property, or belongings without your OK?
- Question 6 is completed by the physician (based on clinical observation): 6. Is there evidence of poor compliance, lack of adherence to medication, missed appointments, or other signs of neglect? [1]
Interpretation: A "yes" response to any of questions 2 through 6 raises the index of suspicion and warrants further assessment or referral to social work or a specialist elder abuse service. Question 1 alone (reliance on others) establishes dependency, which is a risk factor, but a "yes" to question 1 alone does not confirm abuse. [1]
Performance: Sensitivity 0.47, specificity 0.75 against a comprehensive social work evaluation. The moderate sensitivity means it will miss cases — it is a screening tool to raise suspicion, not a diagnostic instrument. [1]
Critical limitation: The EASI was validated only in cognitively intact patients (MMSE 24 or above). It cannot be used as a screening tool in moderate-to-severe dementia. In the cognitively impaired patient, screening relies on direct clinical observation, collateral history from multiple sources, and investigation of physical signs. [1]
The Hwalek-Sengstock Elder Abuse Screening Test (HSEAST)
The HSEAST is a 15-item screening instrument that covers physical abuse, psychological abuse, financial exploitation, neglect, and violation of personal rights. It can be self-administered or clinician-administered. It has been more widely used in research than in clinical practice and has a longer administration time than the EASI. Like the EASI, it requires a degree of cognitive intactness for reliable self-report. [1]
When to screen
Screen for elder abuse in any older person presenting with:
- An unexplained injury or recurrent injuries
- Cognitive impairment or behavioural change (especially in the context of a strained carer relationship)
- Evidence of self-neglect or carer neglect
- Unexplained financial difficulties or sudden legal changes
- Depression, anxiety, or social withdrawal in the context of dependency
- Any presentation where the carer behaviour raises your suspicion [1]
DWE exam point: The EASI is validated only in cognitively intact patients. If a DWE question asks about screening for elder abuse in a patient with moderate dementia, the correct answer is clinical observation and collateral assessment — not the EASI. [1]
The interview-alone principle
The single most important — and most commonly omitted — step in the assessment of suspected elder abuse is to interview the patient without the carer present. This is not optional. If the carer or suspected perpetrator is in the room, the patient will not disclose, and the assessment is fundamentally incomplete. [1]
How to achieve this sensitively: [1]
- Explain the routine. Frame it as standard practice: "I always speak to my patients alone for part of the consultation — it helps me understand things from their perspective. I will speak with you afterwards."
- Be firm. If the carer resists, persist: "I understand you are concerned, but I need to speak with Mrs X privately. The nurses can show you to the waiting area."
- Be direct if necessary. If the carer continues to resist, recognise this as itself a red flag and document it. You may need to involve the nurse to escort the carer out.
- Ask open, non-judgemental questions. "How are things at home?" "Do you feel safe?" "Has anyone hurt you or frightened you?" "Has anyone taken your money or belongings?" "Is there anything you are worried about that you have not been able to tell anyone?" Allow silence. Be patient.
- Document exact quotes. If the patient discloses, record their words verbatim — this is evidence. "My son hits me when he has been drinking" is more powerful in a legal context than "patient reports being hit." [1]
Capacity assessment
Capacity is the pivot of elder abuse management. The capacity assessment follows the two-stage test and the four functional abilities (understand, retain, use or weigh, communicate), as described by Appelbaum [7].
Why capacity is central:
- If the patient has capacity, they have the right to make decisions about their safety, including the right to refuse intervention and to remain in an abusive situation. The clinician's duty is to inform, support, offer alternatives, and follow up — not to coerce.
- If the patient lacks capacity, the decision is made in their best interests, using substituted judgement, consulting the substitute decision-maker (if they are not the perpetrator), and involving the tribunal if necessary. The doctrine of necessity permits immediate protective action (admission, relocation) to prevent serious harm. [1]
Capacity must be assessed for the specific decision — not globally. A patient with moderate dementia may lack capacity to manage their complex financial affairs but retain capacity to decide where they want to live and who they want around them. The threshold for capacity is higher for high-stakes, complex decisions (signing over a house) than for simpler ones (accepting a home visit from a community nurse). [1]
Assess capacity after addressing any reversible contributors to impaired cognition — delirium from infection, dehydration, or over-sedation must be treated before concluding that the person lacks capacity. [1]
Ethical core: The capacitous older person's right to make "unwise" decisions is legally and ethically protected. An older woman who chooses to stay with a verbally abusive husband because she fears being alone more than she fears the abuse — if she has capacity for that decision — has the right to do so. The response is to support, to reduce the harm, and to keep the door open for future help, not to override her autonomy. This is the hardest and most important ethical principle in elder safeguarding. [1]
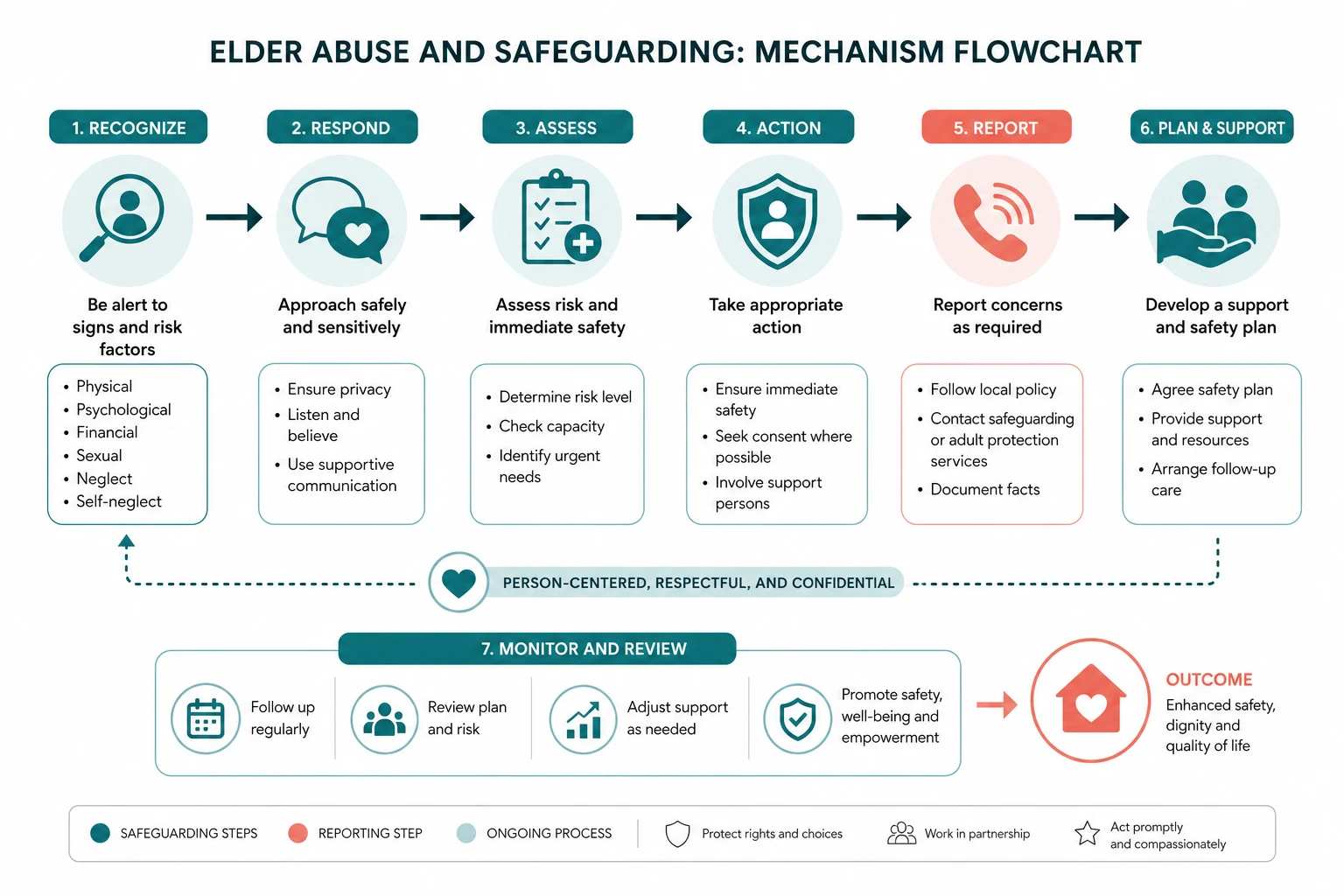
Management — the safeguarding pathway
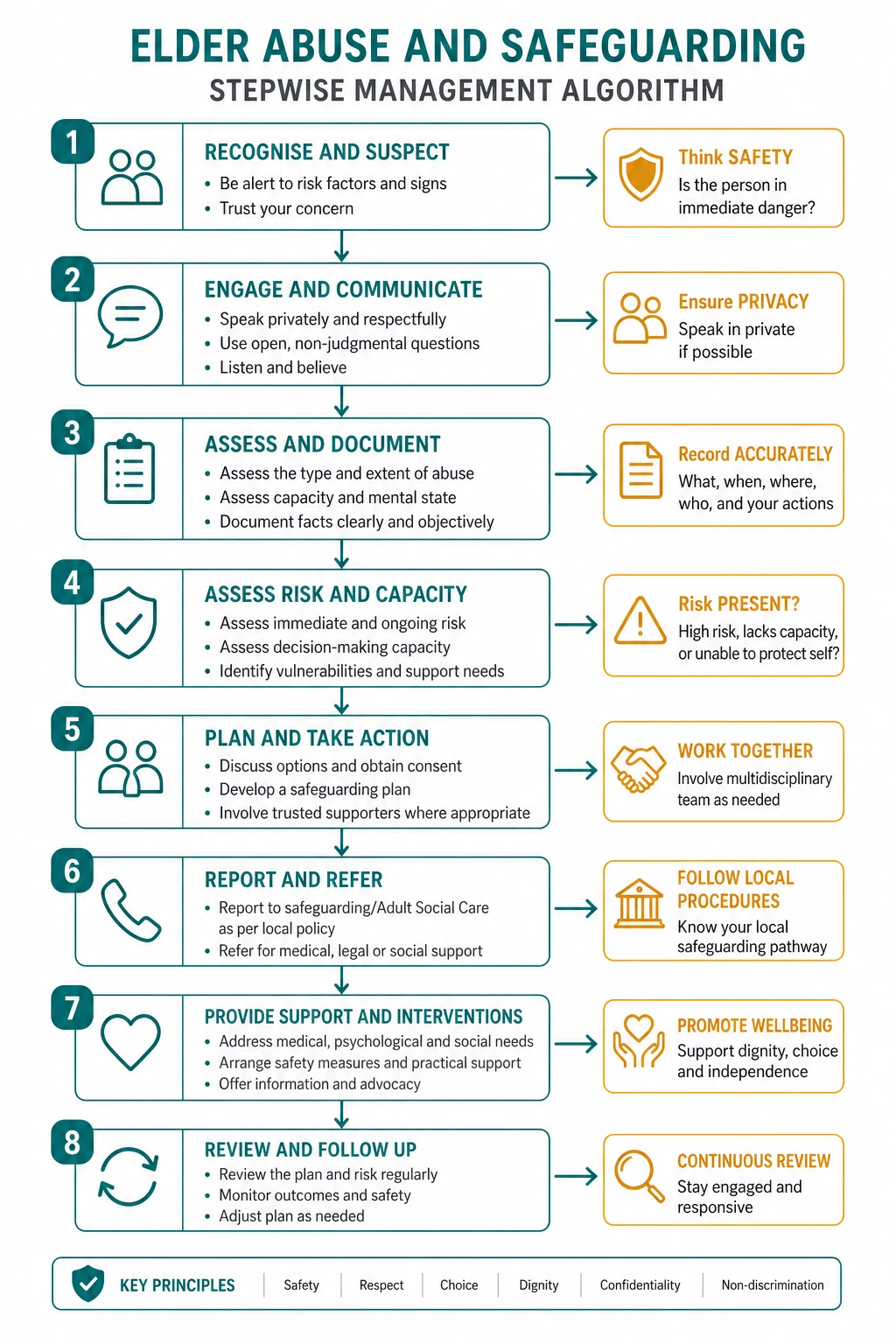

The management of suspected elder abuse follows a structured pathway. The order matters. [1]
Step 1 — Ensure immediate safety
If the patient is in imminent danger (active violence, life-threatening neglect, a perpetrator with immediate access), act to secure safety first. This may mean admission to hospital (the hospital is a place of safety), emergency relocation to alternative accommodation, or calling the police. If the patient lacks capacity and is at serious risk, the doctrine of necessity permits protective action without consent. [1]
Step 2 — Assess capacity
Conduct a structured capacity assessment for the relevant decision (where to live, whether to accept services, whether to report). Treat reversible contributors. Document the assessment formally. [1]
Step 3 — Establish the facts
Take a careful history from the patient (alone), a collateral history (from other family, neighbours, the GP, community services), examine for physical evidence (photograph and document injuries), review the medication chart for inappropriate sedation, and assess the functional, cognitive, and social situation. Consider whether a safeguarding referral for a formal investigation (by social work or a specialist team) is needed. [1]
Step 4 — Involve the multidisciplinary team
Elder abuse is never managed by the physician alone. The core team:
- Social work — coordination, psychosocial assessment, safeguarding referral.
- Elder abuse service or safeguarding team — specialist investigation and intervention.
- Community aged-care services — assessment of the home environment, carer support, respite, home care packages.
- Mental health — for depression, anxiety, and capacity issues in both the patient and the carer.
- Legal services — legal aid, elder law services for financial and property matters.
- Police — if a criminal offence has been committed (physical or sexual assault, major financial fraud). [1]
Step 5 — Legal interventions
The legal toolkit depends on the jurisdiction but includes: [1]
- Apprehended Violence Order (AVO) / Restraining Order — a court order prohibiting the perpetrator from contacting, approaching, or harming the older person. Available in all Australian jurisdictions and the UK (injunctions, restraining orders).
- Guardianship and financial management orders through a tribunal — in Australia, the state civil and administrative tribunal (NCAT in New South Wales, VCAT in Victoria, MCAT, QCAT, SAT, TasCAT, ACTAC, NT CAT). The tribunal can appoint a substitute decision-maker (guardian) for personal and lifestyle decisions, and a financial manager for the person's estate. It can also revoke or review an enduring power of attorney that is being misused.
- Enduring power of attorney review — if the attorney (the financial decision-maker) is the perpetrator, the tribunal can revoke the appointment and substitute an independent manager.
- Police prosecution — for criminal acts of assault, sexual abuse, or major fraud. [1]
Step 6 — Mandatory reporting
Mandatory reporting for elder abuse varies by jurisdiction. The clinician must know the local law: [1]
- Australia: There is no universal mandatory reporting of elder abuse in the community. However, the Aged Care Act 1997 (and its 2024 amendments) requires approved providers of residential aged care and home care to report certain incidents — including serious physical or sexual abuse — to the Aged Care Quality and Safety Commission and, for criminal matters, to the police. Individual clinicians working in residential aged care may be required to report under the service's policies and the Act. In the community, reporting is permissive (at professional discretion) rather than mandatory.
- New South Wales has a dedicated pathway through the Ageing and Disability Commission for abuse of older people and adults with disability in community settings, with a reporting helpline.
- UK: The Care Act 2014 places a duty on local authorities to make enquiries (or cause them to be made) whenever an adult is suspected of being at risk of abuse or neglect. There is no universal mandatory reporting duty for individual clinicians, but professional guidance (GMC, NMC) strongly expects safeguarding referrals.
- US: Most states have mandatory reporting laws for elder abuse, typically requiring certain professionals (including physicians) to report suspected abuse to Adult Protective Services. [1]
The confidentiality principle: Patient confidentiality is not absolute. Where a patient lacks capacity and is at serious risk, or where mandatory reporting laws apply, disclosure is justified and may be required. Where the patient has capacity and objects to reporting, the position is more nuanced — respect the patient's wishes unless there is a serious risk to their life or to others, or a legal obligation to report. [1]
Step 7 — Support services
The management is not just legal — it is supportive:
- Carer support and respite — particularly for passive neglect and for carers experiencing burnout. Day respite, in-home respite, residential respite, and carer counselling.
- Community aged-care services — home care packages for personal care, domestic assistance, meal preparation, medication management.
- Financial counselling and legal aid — to recover misappropriated funds, restructure financial arrangements, and obtain legal protection.
- Counselling for the victim — for depression, anxiety, post-traumatic stress, and the complex grief of betrayal by a family member.
- Advocacy — independent advocacy to ensure the older person's voice is heard in safeguarding decisions. [1]
The autonomy-protection dilemma
The central ethical tension in elder safeguarding is the balance between respecting the autonomy of the capacitous older person and protecting the vulnerable from harm. This is the issue that examiners probe hardest. [1]
The capacitous older person who chooses to stay
An older woman with capacity who is being financially exploited by her son may refuse intervention because she does not want her son to get in trouble, or because she fears losing her relationship with him, or because she believes he will change. If her capacity assessment is sound — she understands the exploitation, she can weigh the consequences, and her decision is voluntary — then her autonomy must be respected. The clinician's role is to: [1]
- Ensure she has accurate information about the abuse, the options, and the services available.
- Reduce the harm — e.g., set up direct debits for essential bills so they are paid before funds can be diverted, arrange for a community nurse or aged-care assessment team to visit regularly (providing external observation and support).
- Keep the door open — maintain the relationship, schedule follow-up, and ensure she knows how to access help if she changes her mind.
- Report if legally required — if mandatory reporting applies (e.g., in residential aged care), report despite her objection, but be transparent with her about what you are doing and why. [1]
The non-capacitous older person who cannot protect themselves
If the patient lacks capacity and is being harmed, the duty of protection overrides the (absent) autonomy. The decision is made in their best interests, using substituted judgement (what would they have wanted?), consulting the substitute decision-maker (if not the perpetrator), and escalating to the tribunal if necessary. Immediate protective action is justified under the doctrine of necessity. The principle of the least restrictive intervention applies — support the person to remain at home safely if possible, rather than institutionalising them. [1]
Documentation
Meticulous documentation is both a clinical and a legal act. Your notes may become the evidence in a guardianship tribunal hearing, a criminal prosecution, or a coronial inquest. Document: [1]
- The history in the patient's own words — verbatim quotes.
- The physical findings — a detailed description and a body map or photographs of injuries (with consent or under necessity if capacity is impaired). Include the size, location, colour, and pattern of each injury.
- The capacity assessment — the specific decision, the information given, the four abilities, the conclusion, and the reasoning.
- The collateral history — who was contacted, what they reported.
- The management plan — the safety plan, the referrals made, the legal actions taken or planned, the follow-up arranged.
- Your clinical reasoning — why you suspect abuse, what you have considered and excluded, and what you plan to do next. [1]
Prevention
Prevention operates at three levels: [1]
- Primary prevention — reducing the incidence of abuse. Carer education and support, respite services, screening for carer stress in routine practice, social engagement programs for isolated older adults, public awareness campaigns, financial literacy education, and advance planning (properly executed enduring guardianship and power of attorney documents with safeguards).
- Secondary prevention — early identification and intervention. Screening (EASI in cognitively intact patients), routine enquiry in high-risk settings (aged-care assessments, hospital admissions), mandatory reporting, and rapid multidisciplinary response.
- Tertiary prevention — reducing the harm from established abuse. Safeguarding, legal protection, support services, and follow-up to prevent recurrence. [1]
The evidence base for elder abuse interventions is limited — there are few randomised trials. The strongest evidence is for carer support interventions (respite, education, counselling, skills training), which reduce carer stress and may reduce abuse. There is also evidence for multidisciplinary team approaches and for financial education and protective measures [5]. More research is needed, and a number of trials are ongoing.
Guidelines and regional differences
- WHO — The Toronto Declaration on the Prevention of Elder Abuse (2002) and the WHO global status report on violence prevention provide the international framework. The WHO calls elder abuse "a violation of human rights and a significant cause of personal injury, illness, lost productivity, isolation and despair."
- Australia — The National Plan to Respond to the Abuse of Older Australians (Council of Attorneys-General, 2019) coordinates a national response. State-based tribunals (NCAT, VCAT, QCAT, etc.) handle guardianship and financial management. The Aged Care Act 1997 (substantially amended in 2024) governs residential and home care safeguarding, with mandatory incident reporting to the Aged Care Quality and Safety Commission. The Ageing and Disability Commission (NSW) provides a reporting pathway for community-based abuse.
- UK — The Care Act 2014 provides the statutory framework for adult safeguarding. The core principle is "making safeguarding personal" — focusing on the outcomes the person wants, not what the professional thinks is best. Local authorities have a duty to make enquiries. Safeguarding Adults Boards coordinate the multi-agency response. There is no universal mandatory reporting duty for clinicians.
- US — Most states have mandatory reporting laws for elder abuse, requiring physicians and other professionals to report to Adult Protective Services. The Elder Justice Act (2010) provides federal support for elder abuse prevention and prosecution. [1]
Regional drug difference relevant to this topic: There are no drug-dose differences between regions. However, the use of chemical restraint (antipsychotics, benzodiazepines) in aged care is regulated in Australia by the Aged Care Quality Standards and the requirement for informed consent, periodic review, and documentation — and its inappropriate use (for staff convenience rather than clinical indication) is itself a form of abuse. [1]
Communication and shared decision-making
The communication priorities in elder abuse are: [1]
- Establish trust and safety. The patient may never have disclosed before. A warm, unhurried, non-judgemental approach is essential.
- Use the patient's language. Many older people do not use the word "abuse" to describe what is happening to them. Ask: "How are things at home?" "Do you feel safe?" "Is anyone hurting or frightening you?" "Is anyone taking your money?"
- Validate and acknowledge. If the patient discloses, acknowledge their courage: "Thank you for telling me. I know that was difficult. What you are describing is not OK, and there are things we can do to help."
- Respect the patient's wishes where possible. Even when you disagree with their decision, respect it (if they have capacity) and keep the door open.
- Communicate the plan. Explain what you are going to do, who you are going to involve, and what the patient can expect. Avoid jargon. Ensure the patient has a way to contact you or the team.
- Address the family. Where safe and appropriate, involve the family in the plan — but never confront the suspected perpetrator in a way that endangers the patient. [1]
Common exam traps
- Failing to interview the patient alone. This is the most common DCE error. Always state it explicitly.
- Over-riding a capacitous patient's autonomy. The capacitous person has the right to refuse help. The correct answer is support and follow-up, not coercion or institutionalisation.
- Using the EASI in moderate dementia. The EASI is validated only in cognitively intact patients (MMSE 24 or above). In dementia, rely on clinical observation and collateral.
- Assuming the carer is always reliable. The carer who accompanies the patient may be the perpetrator. A high index of suspicion and a private interview are essential.
- Missing financial abuse. Financial abuse is the most under-recognised type. Ask about it directly — "Who manages your money?" "Has anyone asked you to sign anything you did not understand?" "Have there been any changes to your will or your bank accounts?"
- Confusing mandatory reporting with patient confidentiality. Know your jurisdiction's law. In many settings, the duty to report (or to make a safeguarding referral) overrides confidentiality — but be transparent with the patient about what you are disclosing and why. [1]
References and further reading
Yon Y, Mikton CR, Gassoumis ZD, Wilber KH. Elder abuse prevalence in community settings: a systematic review and meta-analysis. Lancet Glob Health 2017;5:e147-e156 (PMID 28104184). Yaffe MJ, Wolfson C, Lithwick M, Weiss D. Development and validation of a tool to improve physician identification of elder abuse: the Elder Abuse Suspicion Index (EASI). J Elder Abuse Negl 2008;20:276-300 (PMID 18928055). Acierno R, Hernandez MA, Amstadter AB, et al. Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: the National Elder Mistreatment Study. Am J Public Health 2010;100:292-297 (PMID 20019303). Lachs MS, Williams CS, O'Brien S, Pillemer KA, Charlson ME. The mortality of elder mistreatment. JAMA 1998;280:428-432 (PMID 9701077). Pillemer K, Burnes D, Riffin C, Lachs MS. Elder abuse: global situation, risk factors, and prevention strategies. Gerontologist 2016;56 Suppl 2:S194-S205 (PMID 26994260). Lachs MS, Pillemer K. Elder abuse. Lancet 2004;364:1263-1272 (PMID 15464188). Appelbaum PS. Clinical practice: assessment of patients' competence to consent to treatment. N Engl J Med 2007;357:1834-1840 (PMID 17978292). WHO — Elder abuse (fact sheet, 2022). Toronto Declaration on the Prevention of Elder Abuse (2002). National Plan to Respond to the Abuse of Older Australians (Council of Attorneys-General, 2019). UK Care Act 2014 (statutory guidance). [1]
References
- [1]Yon Y, Mikton CR, Gassoumis ZD, Wilber KH Elder abuse prevalence in community settings: a systematic review and meta-analysis Lancet Glob Health, 2017.PMID 28104184
- [2]Yaffe MJ, Wolfson C, Lithwick M, Weiss D Development and validation of a tool to improve physician identification of elder abuse: the Elder Abuse Suspicion Index (EASI) J Elder Abuse Negl, 2008.PMID 18928055
- [3]Acierno R, Hernandez MA, Amstadter AB, et al. Prevalence and correlates of emotional, physical, sexual, and financial abuse and potential neglect in the United States: the National Elder Mistreatment Study Am J Public Health, 2010.PMID 20019303
- [4]Lachs MS, Williams CS, O'Brien S, Pillemer KA, Charlson ME The mortality of elder mistreatment JAMA, 1998.PMID 9701077
- [5]Pillemer K, Burnes D, Riffin C, Lachs MS Elder Abuse: Global Situation, Risk Factors, and Prevention Strategies Gerontologist, 2016.PMID 26994260
- [6]Lachs MS, Pillemer K Elder abuse Lancet, 2004.PMID 15464188
- [7]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292