Phys · geriatric
Falls and Syncope in Older Adults
Also known as falls in older adults · syncope · transient loss of consciousness · vasovagal syncope · carotid sinus hypersensitivity · carotid sinus syndrome · orthostatic hypotension · postural hypotension · drop attack · multifactorial falls · Timed Up and Go test · Otago exercise programme
Consultant-physician-depth guide to falls and syncope in older adults for FRACP DWE and DCE — epidemiology, the multifactorial risk-factor model, the focused assessment (gait, orthostatic BP, cognitive and cardiovascular), the evidence-graded multifactorial intervention bundle (Otago, tai chi, STOPP/START, home safety, pacemaker for cardioinhibitory carotid sinus hypersensitivity), and the ESC 2018 syncope classification (reflex, orthostatic, cardiac; and the TLOC mimics — seizure, hypoglycaemia, drop attack).
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Falls and Syncope in Older Adults

The one-minute answer
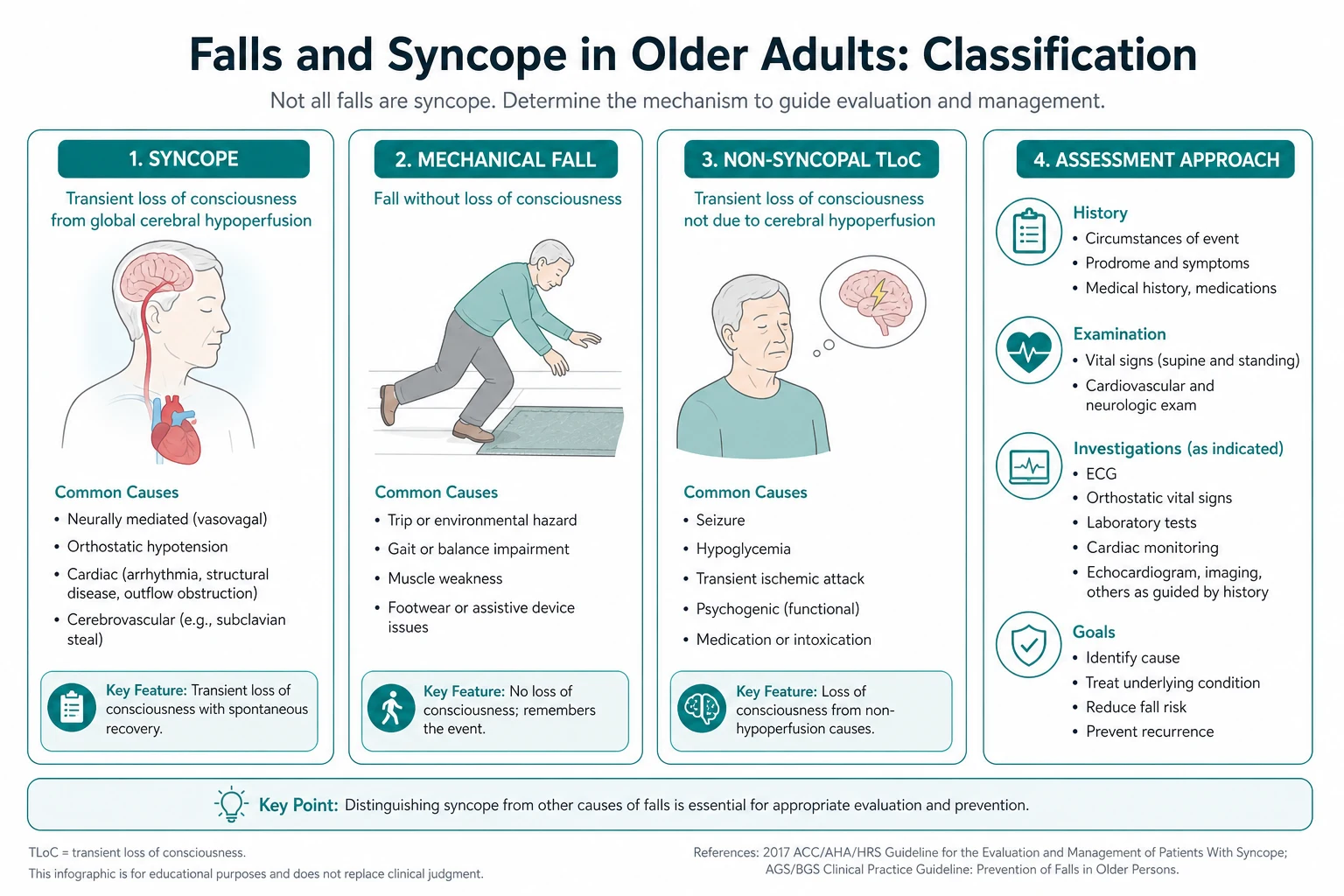
A fall is an unintentional loss of balance that ends on the ground or a lower level. Syncope is a transient loss of consciousness caused by global cerebral hypoperfusion, characterised by rapid onset, short duration, and spontaneous complete recovery. The two overlap in older adults: many older people who have syncope present with an unexplained fall and no recall of losing consciousness, because the witness account is missing or the event was unwitnessed. The job of the physician is to (1) separate syncope from its mimics, (2) find the cause by history and examination rather than by ordering every test, and (3) address the multifactorial risk-factor profile. Falls are the leading cause of injury death in adults over 65, and syncope is the cause in about a third of older patients who fall. The single most useful piece of information is a witnessed account of the event; the single most effective intervention is strength and balance exercise; and the single most dangerous prescribing error is failing to deprescribe the psychotropic, antihypertensive, or anticholinergic drug that is causing the falls. [1]
Why this matters
About 30 percent of people over 65 and 50 percent of those over 80 fall each year; around 5 percent of falls cause a fracture and 1 to 2 percent cause a hip fracture. A hip fracture in an older person carries a one-year mortality of 20 to 30 percent and a high likelihood of losing independent living. Syncope accounts for up to 3 percent of emergency department visits and 1 to 6 percent of hospital admissions. Cardiac syncope has a one-year mortality of 20 to 30 percent and must not be missed — it is the diagnosis that kills. The good news is that the largest part of the problem — multifactorial falls in community-dwelling older adults — is preventable and treatable. Exercise programmes reduce the rate of falls by about 23 percent (Sherrington 2019 Cochrane, PMID 30703272), and a structured medication review alone can prevent falls in a substantial proportion. [1]
Definitions that change the work-up
The ESC 2018 syncope guideline (Brignole, PMID 29562304) defines transient loss of consciousness (TLOC) as a state of real or apparent loss of consciousness with four characteristics — abrupt onset, brief duration, spontaneous full recovery, and loss of postural tone — and divides the causes into: [1]
| Category | Cause | Defining feature |
|---|---|---|
| Syncope | Global cerebral hypoperfusion | The four TLOC features, plus a cerebral mechanism |
| Seizure | Cortical neuronal discharge | Aura, tonic-clonic movements, tongue-biting, incontinence, postictal confusion, slow recovery |
| Apparent TLOC | No real LOC | Cataplexy, drop attack, psychogenic pseudosyncope |
| Rare TLOC | Metabolic, toxic, hypoxaemic | Hypoglycaemia, hypoxia, drug or alcohol intoxication, concussion |
Syncope itself is then subdivided into: [1]
- Reflex (neurally mediated) syncope — vasovagal (the most common in all ages), situational (cough, micturition, defecation, post-prandial), and carotid sinus hypersensitivity.
- Syncope from orthostatic hypotension — autonomic failure (primary neurodegenerative disease, diabetic autonomic neuropathy), drug-induced (the commonest cause in older adults), or volume depletion.
- Cardiac syncope — arrhythmia (brady- or tachy-) and structural heart disease (aortic stenosis, hypertrophic cardiomyopathy, pulmonary hypertension, atrial myxoma, pulmonary embolism). [1]
The discriminating point at the bedside: the cerebral mechanism. Syncope is global hypoperfusion — there is no focal neurological deficit, the recovery is rapid and complete once the patient is horizontal, and there is no postictal state. The work-up that follows depends entirely on which category the history points to. [1]
Epidemiology
- Falls: ~30 percent of community-dwelling adults over 65 fall each year; this rises to 50 percent in those over 80 and is higher again in residential care.
- Consequences: about 10 to 15 percent of falls cause a serious injury; 5 percent cause a fracture; 1 to 2 percent cause a hip fracture.
- Hip fracture: one-year mortality 20 to 30 percent; only about half return to their pre-fracture level of mobility.
- Syncope: accounts for 1 to 3 percent of emergency department attendances and 1 to 6 percent of admissions; the lifetime prevalence is ~40 percent (one vasovagal event).
- Reflex syncope is most common in the young and the old (a bimodal distribution); orthostatic and cardiac syncope predominate in older adults. [1]
Pathophysiology — why a fall happens
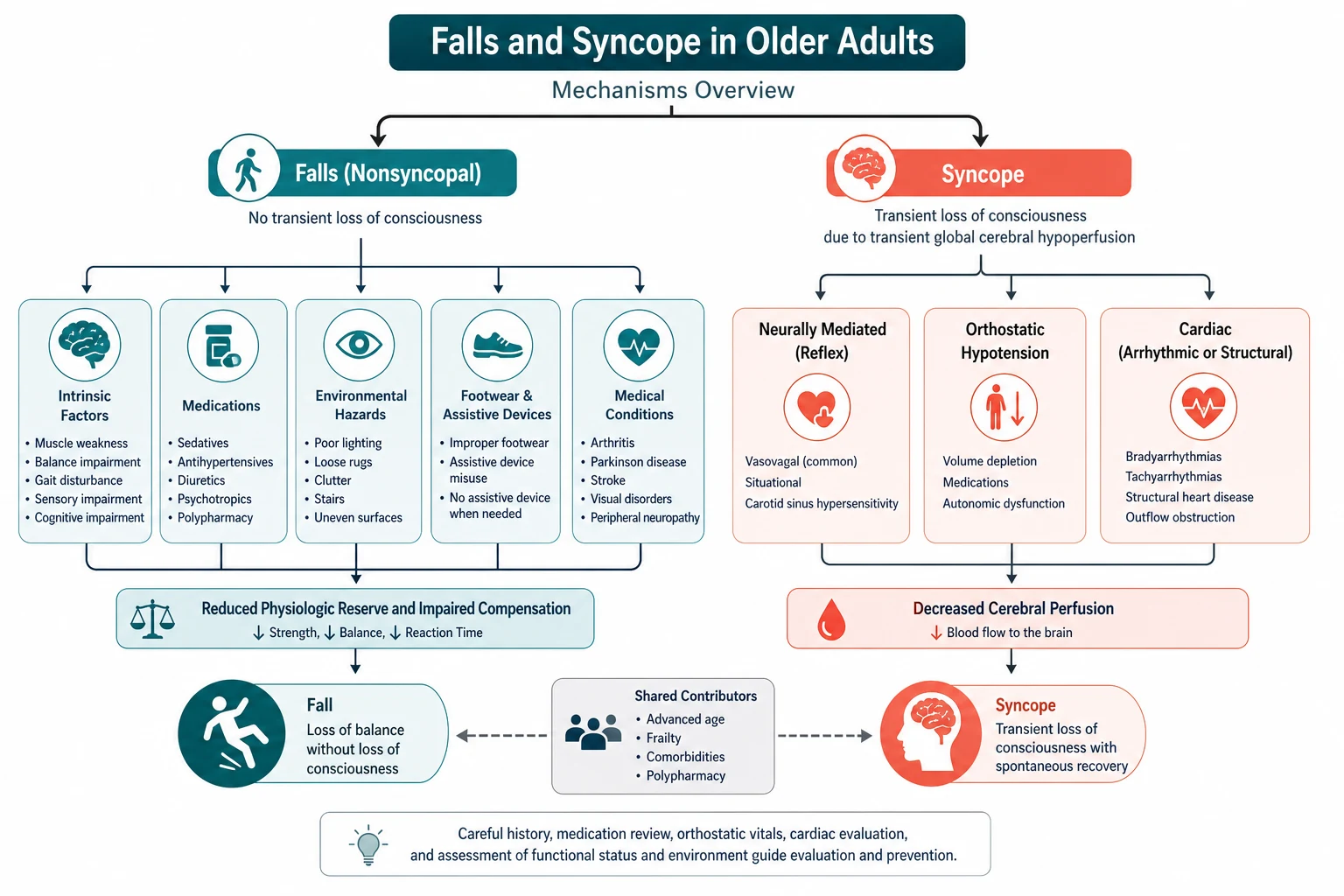
Postural stability requires the continuous integration of sensory input (visual, vestibular, proprioceptive), central processing in the brainstem and cerebellum, and a motor response (the coordinated recruitment of lower-limb and trunk muscles). Ageing reduces the reserve in all three domains — visual acuity and contrast sensitivity fall, vestibular hair cells are lost, proprioceptive fibres thin, reaction time lengthens, muscle mass and strength decline (sarcopenia), and gait becomes slower and more variable. The result is a system that has lost its redundancy — a young person corrects a perturbation without thinking, while an older person needs both attention (which is divided by cognitive impairment or sedating drugs) and strength (which is reduced by disuse or arthritis) to avoid a fall. [1]
The falls-risk equation is therefore: [1]
Falls = (intrinsic vulnerability) × (extrinsic challenge) × (acute insult) [1]
Intrinsic vulnerabilities include age, female sex, cognitive impairment, depression, previous falls, gait and balance impairment, visual impairment, muscle weakness, orthostatic hypotension, and polypharmacy. Extrinsic challenges are environmental hazards (loose rugs, poor lighting, stairs, inadequate footwear) and the medication list. Acute insults are intercurrent illness, infection, dehydration, alcohol, and the context of the activity (reaching, turning, hurrying). A multifactorial intervention is one that addresses several of these factors at once. [1]
Risk factors
| Domain | Risk factor | Why it matters |
|---|---|---|
| Demographic | Age over 80, female sex | Falls and fracture risk rise steeply with age; women have lower bone density and muscle mass |
| History | Previous fall(s) | The single strongest predictor of a future fall — always ask, and ask at every visit |
| Gait and balance | Slow gait, short stride, increased sway, use of a walking aid, abnormal TUG | Objective, measurable, modifiable by exercise |
| Muscle | Sarcopenia, low quadriceps strength, difficulty rising from a chair without arms | The most modifiable risk factor by resistance training |
| Vision | Reduced acuity, cataract, glaucoma, macular degeneration, multifocal glasses outdoors | Impairs contrast sensitivity and depth perception at ground level |
| Cardiovascular | Orthostatic hypotension, carotid sinus hypersensitivity, arrhythmia, valvular heart disease | A cause of syncope masquerading as a fall |
| Neurological | Stroke, Parkinson disease, peripheral neuropathy, cervical myelopathy, normal pressure hydrocephalus | All impair gait and balance |
| Cognitive | Dementia, delirium, depression | Impair judgement, attention, and engagement with prevention |
| Pharmacological | Polypharmacy (4 or more drugs), psychotropics, anticholinergics, antihypertensives | Each psychotropic increases falls risk by ~50 percent |
| Environmental | Loose rugs, poor lighting, no grab rails, slip-on footwear | The home-safety target |
| Functional | ADL impairment, social isolation, fear of falling | Both a consequence and a perpetuator of falls |
The fear of falling deserves a special mention. It develops in up to half of fallers and in many non-fallers; it causes activity restriction, deconditioning, social isolation, depression, and a vicious cycle that INCREASES the future fall risk. It is screened with the Falls Efficacy Scale and treated with a graded re-activation exercise programme. [1]
The focused assessment
History — the circumstances of the event
Ask the patient and, critically, a witness: [1]
- What was the patient doing? — standing up (orthostatic), standing still for a long time (vasovagal), turning the head or looking up (carotid sinus), during exertion (cardiac — red flag), on the stairs or in the bathroom (environmental), at night (nocturia plus dizziness on standing).
- What were the prodromal symptoms? — lightheaded, blurred or tunnel vision, nausea, warmth, sweating, abdominal discomfort, yawning (vasovagal); palpitations (arrhythmia); chest pain or dyspnoea (cardiac); neck movement or tight collar (carotid sinus); no warning at all (cardiac or seizure).
- What did a witness see? — pallor (vasovagal or cardiac), flushing on recovery (vasovagal), brief twitching (syncope can cause myoclonic jerks — this does NOT mean seizure), tongue-biting (seizure), incontinence (seizure, but also syncope), a slow recovery with confusion (seizure), rapid complete recovery on lying flat (syncope).
- How long was the unconsciousness, and how long was the recovery? — syncope is seconds to a minute; seizure is minutes; the postictal confusion of seizure lasts many minutes to hours.
- How often has it happened, and in what settings? — recurrent identical episodes with a clear trigger suggest one mechanism; varied episodes suggest multifactorial risk.
- Past medical history — diabetes (autonomic neuropathy, hypoglycaemia), Parkinson disease (postural instability, OH), dementia (poor judgement), heart disease (arrhythmia, structural disease), stroke, depression.
- Medications — list every drug; flag psychotropics (benzodiazepines, antipsychotics, antidepressants), antihypertensives (especially alpha-blockers, diuretics, combination regimens), anticholinergics (oxybutynin, antihistamines), antiepileptics, opioids, dopaminergic drugs (for Parkinson), and anticoagulants (for the head-injury risk).
- Social history — living situation, ADLs, alcohol intake, driving status. [1]
Examination — gait, balance, vision, orthostatic BP, cognition, and a cardiac and neurological screen
Gait — the Timed Up and Go (TUG) test. Ask the patient to sit in a standard armchair, rise on the word 'go', walk 3 metres at their usual pace to a mark on the floor, turn, walk back, and sit down. Time the task. The original validation (Podsiadlo 1991, PMID 1991946) showed that an independent older adult completes it in less than 10 seconds; a time greater than 12 to 14 seconds indicates impaired mobility and increased fall risk; greater than 30 seconds indicates high dependency. Observe the components: did the patient use their arms to push off (proximal muscle weakness or chair too low), did they need more than one attempt to stand, is the gait shuffling (Parkinson or vascular), wide-based (cerebellar or sensory ataxia), or antalgic (osteoarthritis or a recent fracture), how many steps to turn (more than three is abnormal), and how controlled is the sitting back down? [1]
Balance — the Romberg and tandem gait. Ask the patient to stand with feet together, eyes open, then eyes closed (Romberg — a fall with eyes closed but not open indicates a proprioceptive loss). Ask them to walk heel-to-toe along a straight line (tandem gait — tests balance more than gait). The Berg Balance Scale and the Functional Reach test are longer but more comprehensive alternatives. [1]
Vision — acuity and the glasses. Measure corrected acuity (Snellen); inspect the glasses (bifocal or multifocal lenses increase outdoor falls by impairing edge contrast at the ground). [1]
Orthostatic blood pressure. Have the patient lie supine for 5 minutes; measure the BP and heart rate; ask the patient to stand and measure the BP and heart rate at 1 and 3 minutes. A drop in systolic BP of 20 mmHg or diastolic of 10 mmHg within 3 minutes of standing is orthostatic hypotension (Freeman 2011 consensus, PMID 21431947). The diagnosis requires symptoms (lightheadedness, syncope) — an asymptomatic drop is common in autonomic failure and is not, on its own, a target for treatment. Note the heart rate response: an absent rise with a large drop indicates autonomic failure; an exaggerated rise (greater than 30 beats per minute) is postural tachycardia syndrome (POTS). [1]
Cardiovascular examination. Heart rate and rhythm (atrial fibrillation, bradycardia), murmurs (ejection systolic at the right upper sternal edge radiating to the carotids is aortic stenosis; a dynamic murmur that increases with Valsalva is hypertrophic cardiomyopathy), signs of heart failure. [1]
Neurological examination. Look for parkinsonism (bradykinesia, rigidity, tremor, postural instability), cerebellar signs (nystagmus, dysmetria, dysdiadochokinesia, an ataxic gait), a sensory neuropathy (joint position and vibration sense), proximal myopathy (difficulty rising from a squat), visual fields, and a focused cognitive screen (MoCA or MMSE). [1]
Investigations — only those indicated by the history and examination
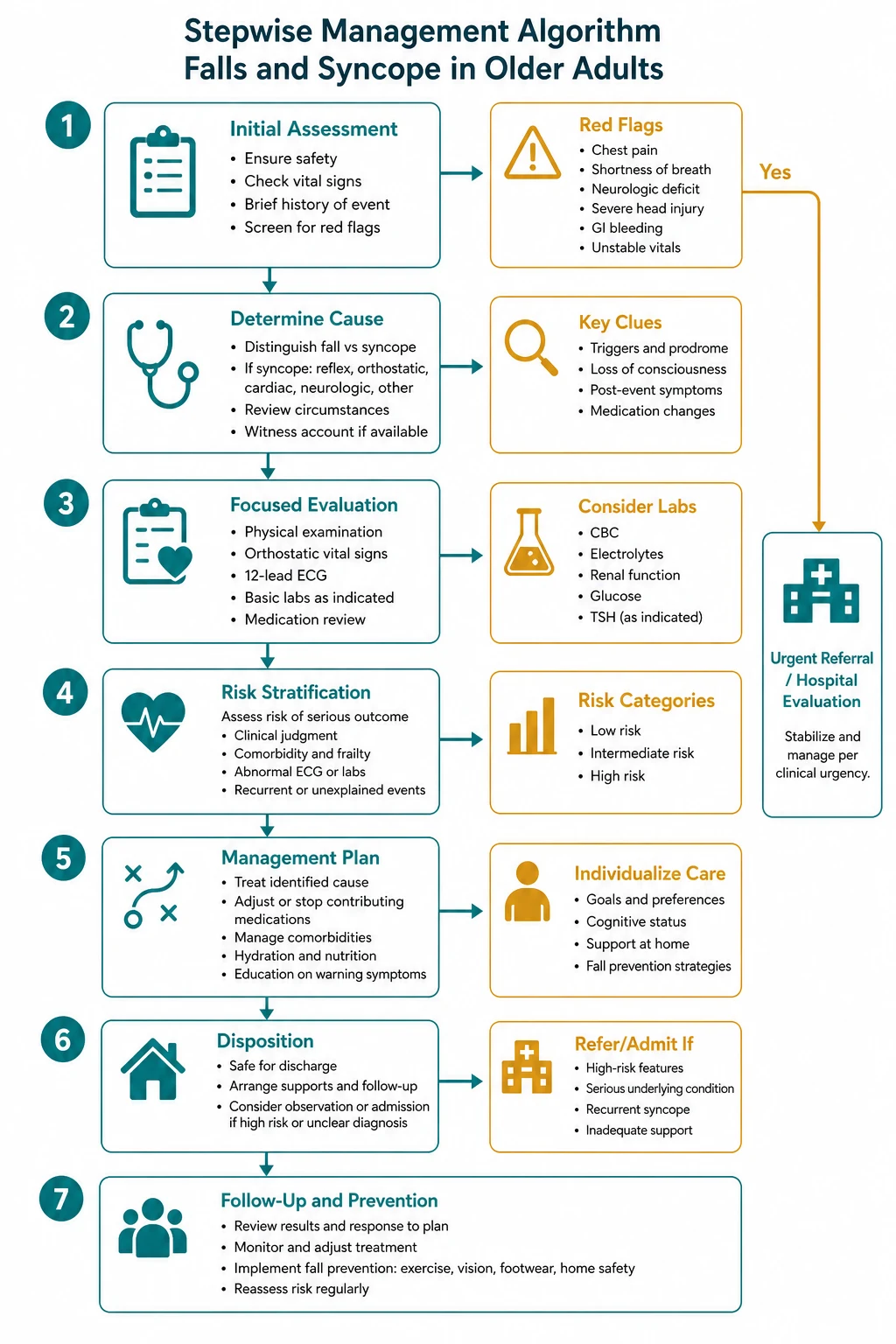
The 2018 ESC syncope guideline (PMID 29562304) is explicit: the initial evaluation is history, physical examination including orthostatic BP, and a 12-lead ECG — and this triad alone yields a suspected or certain diagnosis in 60 to 70 percent of cases. Do NOT order a panel of tests reflexively. [1]

| Test | Indication | Why |
|---|---|---|
| 12-lead ECG | Every patient with syncope; most with unexplained falls | Look for bradycardia, AV block (bifascicular block is a red flag), long QT, Brugada, prior MI, LVH, arrhythmia |
| Orthostatic BP | Every older patient with falls or syncope | Diagnose OH at the bedside |
| Blood glucose | Any patient with possible hypoglycaemia | Hypoglycaemia mimics syncope |
| FBC, U&E, B12, TSH | Selected — anaemia, electrolyte disturbance, reversible causes of cognitive and gait impairment | Targeted, not routine |
| CT head | Head injury on anticoagulant; focal neurology; reduced GCS; suspected subdural; suspected seizure | NOT for unexplained syncope without focal neurology — the yield is very low and the ESC guideline advises against it |
| Echocardiogram | Suspected structural heart disease; abnormal ECG; syncope on exertion | Quantify aortic stenosis, HCM, pulmonary hypertension, LV dysfunction |
| Carotid sinus massage | Unexplained syncope in a patient over 40 compatible with reflex origin; recurrent falls | Contraindicated in recent TIA/stroke or a carotid bruit; reproduce symptoms |
| Tilt table test | Suspected reflex syncope when history is atypical; suspected delayed OH; distinguishing syncope from pseudosyncope | Downgraded in 2018 ESC to a lower class |
| Ambulatory ECG monitoring | Suspected arrhythmic syncope; recurrent unexplained syncope | Choose by frequency — Holter for daily, external loop recorder for weekly, implantable loop recorder for monthly or less frequent |
| EP study | Suspected arrhythmic syncope with structural heart disease or an abnormal ECG | Downgraded in 2018 ESC |
The implantable loop recorder is the highest-yield investigation for recurrent unexplained syncope in older adults after a negative initial work-up — it monitors for up to 3 years, captures the rhythm at the moment of an event, and is cost-effective in this group. [1]
The high-risk cardiac features — do not miss these
The ESC 2018 high-risk features (PMID 29562304) that mandate urgent investigation and admission are: [1]
- Syncope during exertion or while supine
- Palpitations at the time of syncope
- A family history of sudden cardiac death at a young age
- Heart failure or a low LVEF
- An abnormal ECG — bifascicular block, high-degree AV block, bradycardia less than 40, sustained or non-sustained VT, long QT (greater than 460 ms in men, 480 ms in women), Brugada pattern, epsilon waves of arrhythmogenic RV cardiomyopathy, prior Q-wave infarct, LVH [1]
The bifascicular block trap: an older patient with right bundle branch block plus left anterior (or posterior) fascicular block and unexplained syncope has a high risk of progression to complete heart block. The diagnosis is made by ambulatory monitoring (an implantable loop recorder is often needed), and the treatment is permanent pacing — but only after structural heart disease has been excluded, because bifascicular block in heart failure carries a different prognosis. [1]
Multifactorial intervention
Falls are multifactorial, and the intervention must be too. The AGS/BGS 2011 guideline (PMID 21226685), the Cochrane review of interventions for preventing falls (Gillespie 2012, PMID 22972103), and the Cochrane exercise review (Sherrington 2019, PMID 30703272) all support an individually tailored, multifactorial plan. The components are: [1]

| Intervention | Effect | Evidence |
|---|---|---|
| Strength and balance exercise (Otago, tai chi, supervised balance training) | ~23 percent reduction in fall rate | Sherrington 2019 Cochrane (PMID 30703272); Campbell 1997 Otago (PMID 9366737); Lomas-Vega 2017 tai chi (PMID 28736853) |
| Medication review (STOPP/START, psychotropic and antihypertensive reduction) | Substantial — each psychotropic removed reduces falls | O'Mahony 2015 (PMID 25324330) |
| Home safety assessment by an occupational therapist | Effective in higher-risk groups (prior falls, visual impairment) | Gillespie 2012 Cochrane (PMID 22972103) |
| Vision correction (cataract surgery, single-lens distance glasses outdoors) | Effective; caution with multifocal outdoors | Gillespie 2012 Cochrane (PMID 22972103) |
| Vitamin D supplementation | No benefit for primary prevention; use only if deficient | USPSTF 2018 (PMID 29710141) |
| Foot care and supportive footwear | Modest benefit; podiatry referral | Gillespie 2012 Cochrane (PMID 22972103) |
| Cardiac pacing for cardioinhibitory carotid sinus syndrome | Reduces syncope by half in selected patients | ESC 2018 (PMID 29562304) |
| Orthostatic hypotension treatment — stop causative drugs, increase salt and water, compression garments, fludrocortisone, midodrine | Effective if the diagnosis is drug-induced or neurogenic | Freeman 2011 consensus (PMID 21431947) |
The exercise prescription matters. The Sherrington 2019 Cochrane review (PMID 30703272) found that programs are effective when they challenge balance (not just walking) and provide more than 3 hours per week of exercise; the Otago programme specifically reduced falls by 35 percent in adults over 80 in their own homes (Campbell 1997, PMID 9366737; sustained at 2 years, PMID 10604501). Tai chi reduces the rate of falls by about 19 to 43 percent (Lomas-Vega 2017, PMID 28736853). Group and individual formats both work; programmes delivered by a physiotherapist have a larger effect. [1]
The medication review is one of the highest-yield interventions and is often the only one needed. Apply the STOPP criteria (O'Mahony 2015, PMID 25324330): every benzodiazepine, antipsychotic, antidepressant, anticholinergic, opioid, and excess antihypertensive is a target. The principle is deprescribing — there is rarely a reason to add a drug to a falling patient; there is almost always a reason to remove one. [1]
Syncope management by cause

Reflex (vasovagal) syncope
- Education and reassurance — the prognosis is benign; teach the patient to recognise and act on prodromal symptoms.
- Physical counter-pressure manoeuvres — leg-crossing, arm-tensing, hand-gripping; raise BP and prevent syncope if applied early in the prodrome.
- Adequate salt and fluid intake — 2 to 3 litres of fluid and 3 to 5 g of salt per day if no contraindication. [1]- Tilt training — prolonged standing against a wall daily; modest evidence.
- Avoid triggers — prolonged standing, hot environments, large meals, alcohol.
- Beta-blockers are NOT recommended as first line (recent trials are negative and the 2018 ESC does not support them); midodrine is used in selected refractory cases; permanent pacing is reserved for older patients with a dominant cardioinhibitory response and recurrent severe syncope refractory to other measures. [1]
Carotid sinus hypersensitivity
- Carotid sinus hypersensitivity is the asymptomatic reproduction of a reflex by carotid sinus massage (asystole greater than 3 seconds or a systolic drop greater than 50 mmHg); it is common in older adults and is not, on its own, a diagnosis.
- Carotid sinus syndrome is the diagnosis when the massage reproduces the patient's spontaneous symptoms. The dominant cardioinhibitory type is treated with a permanent dual-chamber pacemaker, which halves the recurrence of syncope.
- Avoid tight collars, and advise care with head turning. [1]
Orthostatic hypotension
- Stop the causative drug — alpha-blockers, diuretics, antihypertensives, tricyclics, antipsychotics, dopaminergics. This single intervention resolves OH in a large proportion of older patients.
- Increase salt and water — 2 to 3 litres of fluid and up to 10 g of salt per day (caution in heart failure). [1]- Compression garments — abdominal and lower-limb compression reduce venous pooling; waist-high stockings are more effective than below-knee.
- Rise slowly — sit on the edge of the bed for several minutes before standing; elevating the head of the bed by 10 to 20 cm reduces nocturnal diuresis and supine hypertension.
- Fludrocortisone 0.1 mg orally daily, titrate to 0.2 mg twice daily — a mineralocorticoid that expands volume; monitor for supine hypertension, oedema, hypokalaemia, and heart failure. [1]- Midodrine 2.5 to 5 mg three times daily — an alpha-1 agonist; contraindicated in ischaemic heart disease; the last dose should be before late afternoon to avoid supine hypertension.
- Droxidopa 100 to 600 mg three times daily — a noradrenaline prodrug approved for neurogenic OH; effective in primary autonomic failure (MSA, Parkinson disease, PAF).
- Supine hypertension is the unsolved paradox of treating OH — treat the standing hypotension during the day and accept a degree of supine hypertension at night, or use a short-acting antihypertensive at bedtime. [1]
Cardiac syncope
- Treat the underlying cause — permanent pacing for sinus node dysfunction and high-grade AV block; ICD or catheter ablation for ventricular arrhythmia; aortic valve replacement for severe symptomatic aortic stenosis; septal reduction therapy for HCM.
- The prognosis is driven by the underlying heart disease, not by the syncope itself. [1]
Common exam traps and pitfalls
- The reflex test panel trap. Ordering CT head, carotid Dopplers, EEG and Holter on every patient with syncope. The initial evaluation is history, examination, orthostatic BP, and ECG — and that triad alone yields the diagnosis in 60 to 70 percent of cases (ESC 2018, PMID 29562304). Tests are then targeted to the suspected cause.
- The bifascicular block trap. Missing bifascicular block on ECG in an older patient with unexplained syncope. This is a high-risk finding indicating intermittent complete heart block and warrants ambulatory monitoring and pacing if syncope is unexplained.
- The asymptomatic orthostatic drop trap. Treating a number rather than a symptom. The diagnosis of OH requires symptoms — an asymptomatic drop is common in autonomic failure and is not a target for treatment (Freeman 2011, PMID 21431947).
- The beta-blocker for vasovagal trap. Beta-blockers were once recommended for vasovagal syncope; recent randomised trials are negative and the 2018 ESC does not recommend them as first line.
- The carotid sinus hypersensitivity trap. Diagnosing carotid sinus hypersensitivity from carotid sinus massage alone. The asymptomatic reflex is present in up to 40 percent of older adults; only the reproduction of spontaneous symptoms makes it a diagnosis (carotid sinus syndrome).
- The vitamin D for falls trap. The 2018 USPSTF (PMID 29710141) found no net benefit of routine vitamin D for primary fall prevention. Use it for documented deficiency only.
- The 'dementia caused the fall' trap. Assuming all falls in dementia are due to cognitive impairment. A patient with dementia on an antipsychotic may be falling because of the drug — and stopping it is the intervention.
- The 'echo for all syncope' trap. Echocardiography is indicated only when there is clinical or ECG suspicion of structural heart disease. [1]
Multi-morbidity and polypharmacy — the long-case reality
The falls long case is almost always multi-morbid. The patient who falls in clinic is the one with osteoarthritis (gait impairment), dementia (poor judgement), polypharmacy (drug-induced OH), Parkinson disease (postural instability), diabetes (autonomic neuropathy), visual impairment (cataracts), and cardiovascular disease (arrhythmia). The skill is to construct a single, integrated, feasible plan that addresses them all rather than a list of siloed referrals. The medication review comes first — it is the single most impactful intervention in many older patients and it is free. The exercise prescription comes second — strength and balance training is the best-evidenced non-pharmacological intervention. The home safety assessment comes third. The investigation for a specific cardiac cause comes fourth, and only in patients with the red-flag features. [1]
Communication and shared decision-making
- Frame falls as a treatable geriatric syndrome, not an inevitable part of ageing — this shifts the conversation from fatalism to action and improves adherence.
- Discuss the fear of falling explicitly — patients restrict activity believing it is protective, when the opposite is true. Negotiate a graded re-activation plan.
- The driving discussion is delicate — older patients with syncope or unexplained falls may be unsafe; this is both a capacity and a legal issue (reporting to the licensing authority varies by Australian state). Pair the conversation with a plan for alternative transport.
- The medication review needs explicit discussion of risk versus benefit — patients and prescribers overestimate the benefit of long-term benzodiazepines and underestimate the falls risk.
- Carer involvement — the family is the source of the collateral history and the enabler of the home-safety plan; engage them early. [1]
Long-term outcomes, follow-up and surveillance
- Reassess the fall risk profile at each visit (every 3 to 6 months) — risk factors accumulate and change.
- Review the medication list at every visit; deprescribe wherever possible.
- Reassess the TUG and the orthostatic BP at each visit; both are objective, quick, and track the response to intervention.
- For recurrent syncope after a negative work-up, an implantable loop recorder is the next step — it captures the rhythm at the moment of an event and is cost-effective in this group.
- For the patient with a hip fracture, the post-fracture period is a high-risk window — secondary prevention (osteoporosis treatment, falls prevention, and a home-safety review) is mandatory and is often missed. [1]
Key citations
- Brignole M, et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur Heart J 2018;39:1883-1948 (PMID 29562304).
- Panel on Prevention of Falls in Older Persons, AGS/BGS. Summary of the updated clinical practice guideline for prevention of falls in older persons. J Am Geriatr Soc 2011;59:148-157 (PMID 21226685).
- Sherrington C, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev 2019 (PMID 30703272).
- Gillespie LD, et al. Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev 2012 (PMID 22972103).
- Campbell AJ, et al. Randomised controlled trial of home-based exercise to prevent falls in elderly women. BMJ 1997;315:1065-1069 (PMID 9366737).
- Campbell AJ, et al. Falls prevention over 2 years: a randomised controlled trial in women 80 years and older. Age Ageing 1999;28:513-518 (PMID 10604501).
- Lomas-Vega R, et al. Tai chi for risk of falls: a meta-analysis. J Am Geriatr Soc 2017;65:2037-2043 (PMID 28736853).
- Grossman DC, et al. Interventions to prevent falls in community-dwelling older adults: USPSTF recommendation statement. JAMA 2018;319:1696-1704 (PMID 29710141).
- O'Mahony D, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing 2015;44:213-218 (PMID 25324330).
- Podsiadlo D, Richardson S. The timed 'Up and Go': a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991;39:142-148 (PMID 1991946).
- Freeman R, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res 2011;21:69-72 (PMID 21431947). [1]
References
- [1]Brignole M, Moya A, de Lange FJ, et al. 2018 ESC Guidelines for the diagnosis and management of syncope Eur Heart J, 2018.PMID 29562304
- [2]Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons J Am Geriatr Soc, 2011.PMID 21226685
- [3]Sherrington C, Fairhall NJ, Wallbank GK, et al. Exercise for preventing falls in older people living in the community Cochrane Database Syst Rev, 2019.PMID 30703272
- [4]Gillespie LD, Robertson MC, Gillespie WJ, et al. Interventions for preventing falls in older people living in the community Cochrane Database Syst Rev, 2012.PMID 22972103
- [5]Campbell AJ, Robertson MC, Gardner MM, Norton RN, Tilyard MW, Buchner DM Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women BMJ, 1997.PMID 9366737
- [6]Campbell AJ, Robertson MC, Gardner MM, Norton RN, Buchner DM Falls prevention over 2 years: a randomized controlled trial in women 80 years and older Age Ageing, 1999.PMID 10604501
- [7]Lomas-Vega R, Garrido-Jaute MV, Rus A, Del-Pino-Casado R Tai Chi for Risk of Falls. A Meta-analysis J Am Geriatr Soc, 2017.PMID 28736853
- [8]Grossman DC, Curry SJ, Owens DK, et al. Interventions to Prevent Falls in Community-Dwelling Older Adults: US Preventive Services Task Force Recommendation Statement JAMA, 2018.PMID 29710141
- [9]O'Mahony D, O'Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P STOPP/START criteria for potentially inappropriate prescribing in older people: version 2 Age Ageing, 2015.PMID 25324330
- [10]Podsiadlo D, Richardson S The timed Up & Go: a test of basic functional mobility for frail elderly persons J Am Geriatr Soc, 1991.PMID 1991946
- [11]Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome Clin Auton Res, 2011.PMID 21431947