Phys · geriatric
Polypharmacy and Deprescribing
Also known as polypharmacy · hyperpolypharmacy · deprescribing · potentially inappropriate medications · PIMs · Beers Criteria · STOPP criteria · START criteria · prescribing cascade · medication reconciliation · anticholinergic burden · drug-related problems in older adults
Consultant-physician-depth guide to polypharmacy and deprescribing for FRACP DWE and DCE — definitions of polypharmacy and hyperpolypharmacy, the pharmacokinetic changes of ageing, adverse drug reactions and the prescribing cascade, the Beers Criteria and STOPP/START version 3, medication reconciliation at transitions of care, high-risk medications in older adults, and the systematic deprescribing process with class-specific guidance for PPIs, statins, bisphosphonates, antihypertensives and benzodiazepines.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Polypharmacy and Deprescribing


The answer first
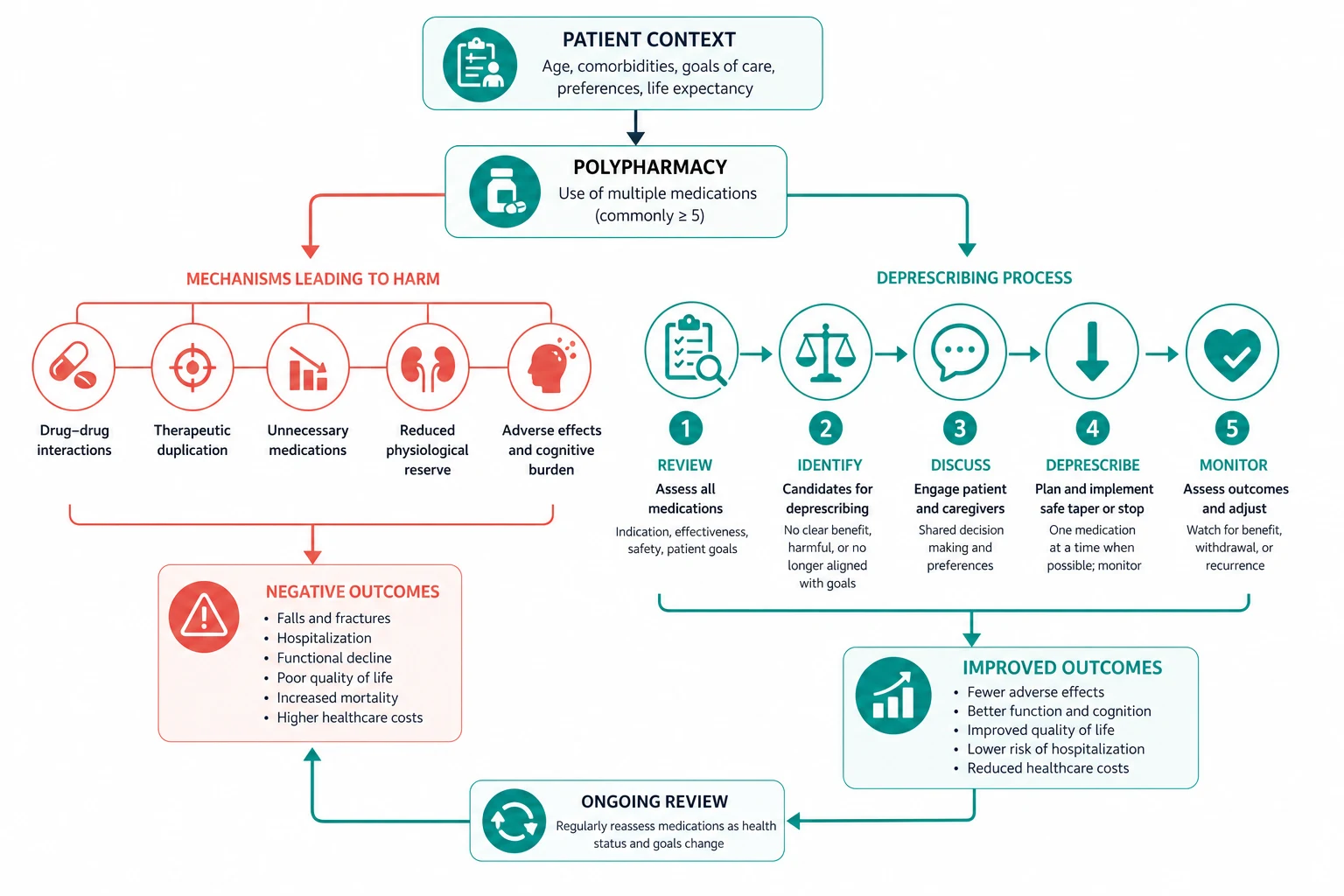
Polypharmacy is the concurrent use of multiple medications — operationally, five or more regular medications. Hyperpolypharmacy is ten or more. The number matters less than the appropriateness: the real target is inappropriate polypharmacy — medications where the potential harms now outweigh the benefits in this patient, at this point, given their goals of care, frailty and life expectancy. [1]
The four rules that determine everything on this topic are: [1]
- Every new symptom in an older patient on multiple medications is an adverse drug reaction until proven otherwise. Before adding a drug, review the list. The prescribing cascade — treating a side effect with a second drug — is the commonest engine of polypharmacy growth.
- Ageing changes pharmacokinetics and pharmacodynamics in ways that increase drug sensitivity. Renal clearance falls (while serum creatinine may look normal because muscle mass is lost), hepatic mass and blood flow decline, body fat increases (prolonging the half-life of lipophilic drugs), and receptor sensitivity rises. Start low, go slow, and review frequently.
- Medications accumulate for predictable reasons — fragmented care, absent reconciliation at transitions, and disease-oriented guidelines that never account for limited life expectancy or competing goals. Every admission and every outpatient review is an opportunity to reconcile and to deprescribe.
- Deprescribing is a planned, supervised, patient-centred process, not a drug-stopping reflex. Identify potentially inappropriate medications, assess each against goals and prognosis, taper where withdrawal or rebound is possible, and monitor. Most deprescribing attempts succeed; the fear of relapse is greater than the reality. [1]
DWE high-yield trap: When asked "best next step" for a frail older patient with falls, confusion, or an adverse drug event on a long medication list, the answer is almost always structured medication review with deprescribing using a validated tool (Beers or STOPP/START) — not adding another drug, not ordering more tests. Adding a drug to treat a side effect is the prescribing cascade and is always the wrong answer. [1]
Definitions
Polypharmacy — the operational thresholds
| Term | Definition | Clinical signal |
|---|---|---|
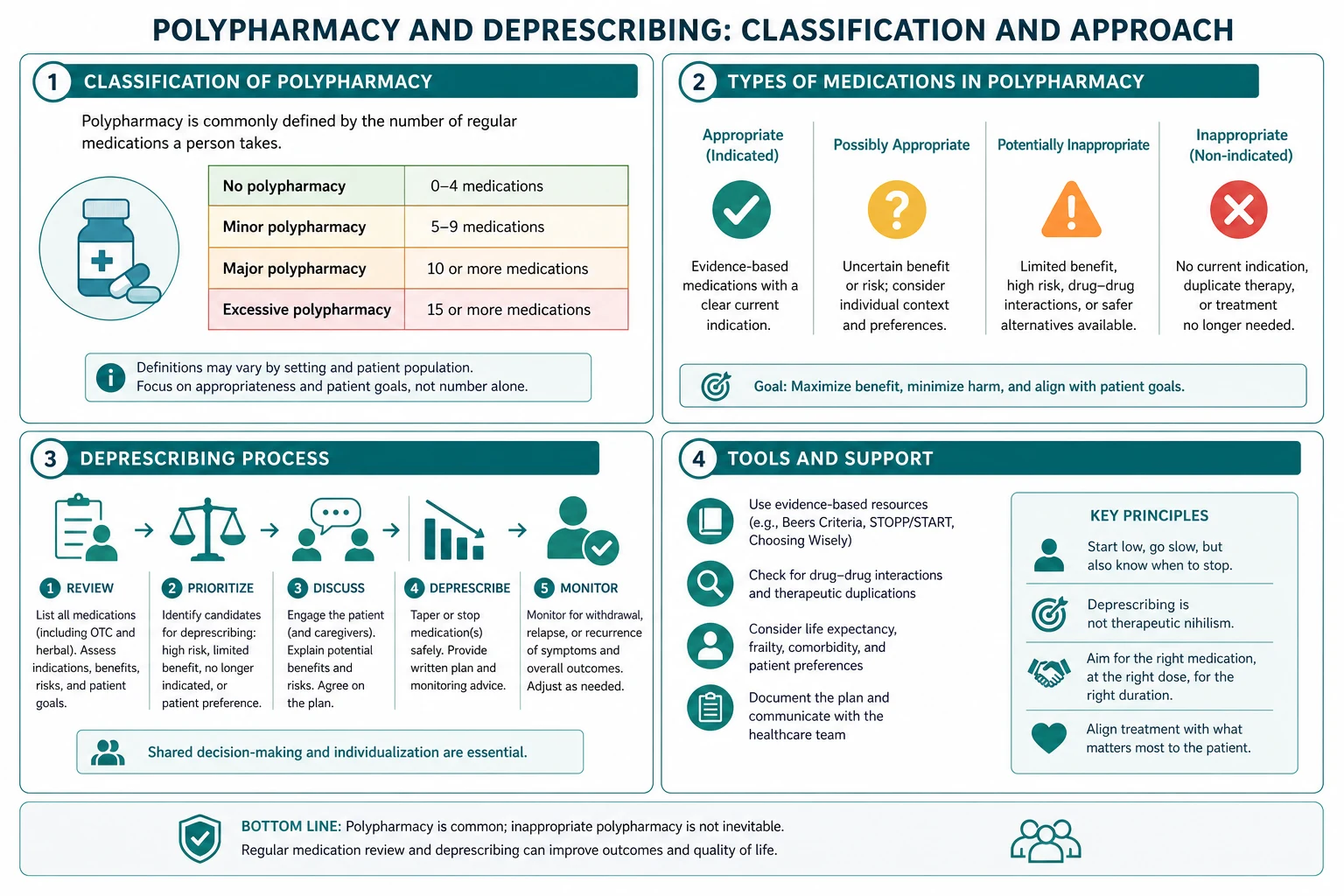
| Polypharmacy | 5 or more concurrent regular medications | Increased risk of adverse drug reactions, interactions and falls; warrants structured review |
| Hyperpolypharmacy | 10 or more concurrent regular medications | High risk; nearly always indicates at least some inappropriate prescribing |
| Inappropriate polypharmacy | Any medication where the potential harms now outweigh the benefits in this patient, at this time, given their goals, frailty and prognosis | The actionable target — a patient can be on one inappropriate drug or ten appropriate ones |
The numerical thresholds (5 and 10) are epidemiological signals, not treatment targets. A patient with heart failure, atrial fibrillation, diabetes and osteoporosis may appropriately take an ACE inhibitor, beta-blocker, mineralocorticoid antagonist, diuretic, anticoagulant, metformin, a statin, and a bisphosphonate — eight drugs, all indicated. The clinical task is to separate appropriate polypharmacy (each drug has a current indication, is effective, tolerated, and aligned with goals) from inappropriate polypharmacy (drugs with no current indication, with harms exceeding benefits, with duplications, or with drug-disease or drug-drug interactions). [1]
Exam trap: The DWE distinguishes polypharmacy (five or more) from hyperpolypharmacy (ten or more). Do not confuse the number with appropriateness — a small number of inappropriate drugs is still a medication-safety problem. [1]
What "deprescribing" means
Deprescribing is the supervised process of tapering or stopping inappropriate medications, guided by a patient-centred evaluation of the current benefits and harms, with the goal of managing polypharmacy and improving outcomes (Scott et al, JAMA Intern Med 2015, PMID 25798731). It is the inverse of prescribing — equally deliberate, equally monitored, and equally patient-centred. It is not the abrupt cessation of all medications, and it is not a nihilistic response to ageing. [1]
Epidemiology
Polypharmacy is near-universal in older adults with multimorbidity, and its prevalence is rising as populations age and single-disease guidelines multiply. [1]
- Older adults in developed countries take a median of 5 medications regularly, rising to 7 to 9 in residential aged care and in hospital.
- Approximately 20 percent of older adults in the community take 10 or more medications (hyperpolypharmacy).
- The prevalence of potentially inappropriate medications by Beers or STOPP criteria in community-dwelling older adults is 20 to 40 percent, and higher in hospital and aged-care settings.
- The number of medications is a continuous risk factor: the probability of an adverse drug event rises with each additional drug, roughly doubling from 5 to 10 medications. [1]
The reason this matters clinically: every extra medication adds independent risk — of an adverse drug reaction, a drug interaction, a fall, cognitive impairment, a hospital admission, and death. Reducing inappropriate medications reduces that risk. This is why deprescribing is a clinical intervention with measurable benefit, not a theoretical preference. [1]
Consequences of polypharmacy
Adverse drug reactions
Adverse drug reactions (ADRs) are the commonest and most measurable harm of polypharmacy. The Kongkaew systematic review (Ann Pharmacother 2008, PMID 18594048) found that approximately 5.3 percent of all hospital admissions were associated with an ADR, and the rate in elderly patients was 10.7 percent (interquartile range 9.6 to 13.3 percent) — roughly double that of younger adults. Cardiovascular drugs (anticoagulants, diuretics, renin-angiotensin system inhibitors) are the most frequently implicated class in adults and older patients. The risk of an ADR in an outpatient older adult is approximately 1 in 6 over a year on multiple medications, and the risk rises steeply with the number of drugs. [1]
Falls
Falls are the leading injury-related cause of death and disability in older adults, and medications are among the most modifiable risk factors. The Woolcott meta-analysis (Arch Intern Med 2009, PMID 19933955) quantified the impact of nine drug classes on falls in adults over 60. The key results: [1]
| Drug class | Odds ratio for a fall |
|---|---|
| Antihypertensives (overall) | 1.24 |
| Diuretics | 1.07 |
| Beta-blockers | 1.01 |
| Benzodiazepines | 1.57 |
| Antidepressants (especially SSRIs, TCAs) | 1.68 |
| Antipsychotics / neuroleptics | 1.59 |
| Opioids | 1.42 |
| Antiepileptics | 1.40 |
| Non-steroidal anti-inflammatory drugs | 1.42 |
The clinical message: psychotropic drugs (benzodiazepines, antidepressants, antipsychotics) and opioids carry the highest falls risk, and they are also the most frequently inappropriate and the most amenable to deprescribing. [1]
Cognitive impairment and delirium
Medications with anticholinergic or sedative properties cause or worsen cognitive impairment and are a leading precipitant of delirium in hospitalised older adults. The anticholinergic burden — the cumulative central antimuscarinic effect of drugs such as oxybutynin, solifenacin, tricyclic antidepressants, first-generation antihistamines, and quetiapine — is associated with impaired attention, reduced executive function, an increased risk of delirium, and accelerated cognitive decline. Reducing anticholinergic burden is one of the highest-yield deprescribing targets in any older patient. [1]
Hospital admissions and mortality
ADR-related hospital admissions are common (approximately 1 in 10 admissions in older adults) and are frequently preventable. Polypharmacy is independently associated with increased all-cause mortality, increased institutionalisation, reduced functional capacity, and reduced quality of life. The relationship is partly direct (drug harms) and partly a marker of multimorbidity and frailty, but the component that is modifiable is the medication list. [1]
Financial burden
Polypharmacy imposes a direct financial cost on patients (out-of-pocket medication costs, which can lead to cost-related non-adherence and rationing) and on health systems (drug acquisition, plus the downstream cost of managing the ADRs and admissions it causes). Deprescribing is a rare intervention that improves outcomes and reduces cost simultaneously. [1]
Causes — how polypharmacy accumulates
Understanding why medications accumulate is the foundation of preventing and reversing polypharmacy. Four mechanisms dominate. [1]
The prescribing cascade
The prescribing cascade — first formally described by Rochon and Gurwitz — is the sequence in which an adverse effect of one drug is misinterpreted as a new medical condition, and a second drug is prescribed to treat it. The second drug may then cause its own adverse effects, triggering a third prescription, and the list grows. [1]
Classic prescribing cascades the exam tests: [1]
| Drug causing the adverse effect | Adverse effect misread as a new disease | Second drug prescribed to treat it | What to do instead |
|---|---|---|---|
| Metoclopramide (D2 antagonist) | Drug-induced parkinsonism (tremor, rigidity, bradykinesia) | Levodopa | Stop the metoclopramide — the parkinsonism is reversible |
| Thiazide or loop diuretic | Gout (diuretic-induced hyperuricaemia) | Allopurinol | Stop or reduce the diuretic if possible; manage the gout |
| NSAID | Hypertension (NSAID-mediated fluid retention and vasoconstriction) | Additional antihypertensive | Stop the NSAID; review the blood pressure |
| Antihypertensive (any) | Dizziness or falls (orthostatic hypotension) | Fludrocortisone or midodrine | Reduce or stop the antihypertensive |
| Donepezil (cholinergic) | Urinary incontinence | Oxybutynin (anticholinergic) | The two drugs pharmacologically oppose each other; address the incontinency non-pharmacologically |
| PPI (long-term) | Hypomagnesaemia causing muscle cramps | Magnesium supplement | Reassess the PPI indication and deprescribe |
The clinical rule: whenever you are about to start a new drug for a new symptom in an older patient, ask whether the symptom could be an adverse effect of a drug they are already taking. If it could, address the first drug before adding the second. [1]
DWE exam trap: A vignette describing an older patient on metoclopramide who develops parkinsonian features and is given levodopa tests the prescribing cascade. The correct answer is stop the metoclopramide (the cause), not escalate the levodopa (the cascade). [1]
Fragmented care
Older adults with multimorbidity see multiple specialists, each focused on a single organ system, each applying a single-disease guideline that does not account for the patient's other conditions, frailty, or life expectancy. The cardiologist adds a fourth antihypertensive for a blood pressure target derived from a trial of robust younger patients; the nephrologist adds an ACE inhibitor; the endocrinologist adds a statin; the rheumatologist adds an NSAID; the psychiatrist adds an SSRI and a benzodiazepine. No single clinician owns or reviews the whole list. The general physician or geriatrician's role is to hold the whole medication regimen and reconcile it against the whole patient. [1]
Absent medication reconciliation at transitions
Every transition of care — admission, transfer between wards, transfer to rehabilitation, and discharge — is a point at which medications are unintentionally changed, duplicated, omitted, or carried forward without review. Up to 60 percent of medication errors and a large proportion of post-discharge ADRs originate at these transitions. Medication reconciliation — the formal process of creating the best possible medication history (BPMH), comparing it against the current orders, and resolving every discrepancy — is a mandated safety standard (ACSQHC Medication Safety Standard) and is the single most effective intervention to prevent transition-related medication errors. [1]
Disease-oriented guidelines that ignore life expectancy
Most evidence-based guidelines are built on trials that excluded older adults with multimorbidity and frailty, and they define benefits in relative terms over horizons (5 to 10 years) that exceed the life expectancy of many of the patients to whom they are applied. A statin for primary prevention takes years to show benefit; a tight glycaemic target (HbA1c under 7 percent) in a frail 85-year-old causes harm (hypoglycaemia, falls) without a realistic prospect of microvascular benefit within their lifetime. Applying disease-by-disease guidelines to a frail patient with limited life expectancy mechanically generates polypharmacy. The antidote is to anchor every prescribing decision to the patient's goals of care, their life expectancy, and their frailty — and to deprescribe when the time-to-benefit exceeds the prognosis. [1]
Pharmacokinetic and pharmacodynamic changes in ageing
Ageing changes how the body handles drugs (pharmacokinetics) and how the body responds to them (pharmacodynamics). These changes increase both the intensity and the duration of drug effect, and they are the physiological basis for the "start low, go slow" principle in older adults. [1]

Renal — reduced clearance, falsely reassuring creatinine
Renal function declines with age: the glomerular filtration rate falls by roughly 0.8 to 1.0 mL/min per year after age 40, so an 80-year-old may have half the GFR of a 30-year-old. The trap is that serum creatinine may remain in the "normal" range despite substantial renal impairment, because muscle mass (the source of creatinine) also declines with age and frailty. A frail 85-year-old woman with a creatinine of 80 micromol per litre may have an eGFR under 45 — and a renally-cleared drug dosed at the "normal" creatinine dose will accumulate and cause toxicity. [1]
Clinical rule: Estimate the GFR in every older patient before prescribing renally-cleared drugs. The 2021 CKD-EPI creatinine equation (Inker et al, NEJM 2021, PMID 34554658) is the current standard and is race-free. Be aware that it is normalised to a body surface area of 1.73 metres squared and may overestimate renal function in small, frail, low-muscle-mass patients. For drugs with a narrow therapeutic index (digoxin, gabapentin, pregabalin, DOACs at the extremes of weight and renal function), consider a cystatin C-based eGFR (less dependent on muscle mass) or a measured creatinine clearance. For drug dosing, the Cockcroft-Gault formula (using actual or estimated creatinine clearance in mL/min) is still used by many references because the original drug trials were based on it. [1]
Drugs that accumulate in renal impairment and commonly cause harm in older adults: digoxin, gabapentin, pregabalin, metformin (lactic acidosis), DOACs (bleeding), lithium, allopurinol, atenolol, sotalol, frusemide (at higher doses), gentamicin, vancomycin, and the water-soluble beta-blockers. [1]
Hepatic — reduced mass and blood flow
Liver mass and hepatic blood flow decline with age (by roughly 20 to 40 percent by age 80). The effect is most pronounced for high first-pass (flow-limited) drugs — such as propranolol, labetalol, verapamil, diltiazem, and morphine — whose clearance depends on hepatic blood flow rather than on hepatic enzyme capacity. Phase I metabolism (oxidation, reduction, hydrolysis — largely cytochrome P450 mediated) becomes slower and more variable with age, while phase II conjugation (glucuronidation, acetylation) is relatively preserved. The clinical consequence: drugs dependent on phase I metabolism (most benzodiazepines, several opioids) have prolonged half-lives and accumulate, while drugs cleared by phase II (lorazepam, oxazepam, temazepam — the "LOT" benzodiazepines; morphine) are relatively unaffected and are preferred when a benzodiazepine or opioid is unavoidable. [1]
Body composition — more fat, less water
With ageing, lean body mass and total body water decline, and body fat increases (from roughly 15 to 30 percent of body weight in men across the adult lifespan, and similarly in women). The pharmacokinetic consequences are predictable: [1]
- Lipophilic drugs (diazepam, flurazepam, amiodarone, fluoxetine, haloperidol, dronedarone) distribute into a larger fat compartment, their volume of distribution increases, and their half-life is markedly prolonged. Diazepam's half-life in an 80-year-old can exceed 80 hours (versus 20 to 40 hours in a younger adult) — this is why diazepam is on every list of inappropriate benzodiazepines in older adults.
- Water-soluble drugs (lithium, digoxin) distribute into a smaller volume, producing higher peak concentrations for a given dose, which raises the risk of early toxicity. [1]
Receptor sensitivity — pharmacodynamic change
Older adults show increased sensitivity to several drug classes even when pharmacokinetics are accounted for — a pharmacodynamic effect: [1]
- CNS depressants (benzodiazepines, opioids, antipsychotics, anaesthetics): greater sedation, greater cognitive impairment, greater falls risk for a given dose. The brain is more sensitive, not just the clearance slower.
- Anticoagulants (warfarin): the INR response to a given warfarin dose is greater in older adults, and the bleeding risk at a given INR is higher — so warfarin doses in older adults are lower.
- Vasoactive drugs (antihypertensives, diuretics): exaggerated blood pressure response, greater orthostatic hypotension.
- Reduced baroreceptor sensitivity: blunted compensatory tachycardia to vasodilatation, increasing orthostatic hypotension and falls. [1]
The combined effect of these pharmacokinetic and pharmacodynamic changes is that older adults experience more drug effect for longer from a given dose. The prescribing rule is: start at 25 to 50 percent of the usual adult dose, titrate slowly to effect, and review frequently. [1]
Assessment tools — Beers Criteria
The AGS Beers Criteria (American Geriatrics Society 2023 updated Beers Criteria, PMID 37139824) is the most widely used US-origin explicit tool for identifying potentially inappropriate medications (PIMs) in adults aged 65 and older. It is updated every three years; the 2023 version is the current standard. It covers five categories of concern. [1]

The five Beers categories
| Category | What it flags | Examples |
|---|---|---|
| 1. PIMs in older adults (generally) | Drugs to avoid in nearly all older adults | Anticholinergics (oxybutynin, hyoscine), benzodiazepines (diazepam, alprazolam), first-generation antihistamines (diphenhydramine, chlorpheniramine), long-acting sulfonylureas (glyburide/glibenclamide), barbiturates, meperidine/pethidine |
| 2. PIMs in specific diseases/syndromes | Drugs to avoid when a particular condition is present | NSAIDs in heart failure or CKD; anticholinergics in dementia or glaucoma; antipsychotics in Parkinson or Lewy body dementia; non-selective beta-blockers in asthma; tricyclics in cardiac conduction disease |
| 3. Medications to use with caution | Drugs that may be appropriate but require careful monitoring | Aspirin for primary prevention in those over 70; diuretics in hyponatraemia; SNRIs; antipsychotics in dementia (behavioural and psychological symptoms) |
| 4. Clinically important drug-drug interactions | Combinations that cause harm | Warfarin plus amiodarone or a macrolide or an NSAID; multiple anticholinergics; ACE inhibitor plus potassium-sparing diuretic |
| 5. Dose adjustment for renal function | Drugs that need dose reduction at low eGFR | Gabapentin, pregabalin, allopurinol, metformin, dabigatran, DOACs, nitrofurantoin (avoid if eGFR under 30) |
The high-yield Beers drugs the exam tests
Memorise these as "drugs to avoid in older adults wherever possible": [1]
- Benzodiazepines (all, especially long-acting — diazepam, chlordiazepoxide, flurazepam) — increased falls, fractures, cognitive impairment, delirium, motor vehicle crashes.
- Anticholinergic drugs (oxybutynin, hyoscine/buscopan, solifenacin, tolterodine, tricyclic antidepressants, first-generation antihistamines, quetiapine) — confusion, dry mouth, constipation, urinary retention, delirium, cognitive decline.
- First-generation antihistamines (diphenhydramine, chlorpheniramine, promethazine) — pronounced anticholinergic effect; use a second-generation agent (cetirizine, loratadine) if an antihistamine is needed.
- Long-acting sulfonylureas (glyburide/glibenclamide) — prolonged hypoglycaemia; prefer gliclazide or a DPP-4 inhibitor in older adults.
- NSAIDs (non-selective and COX-2 inhibitors) — gastrointestinal bleeding, renal impairment, fluid retention, heart failure exacerbation, hypertension.
- Meperidine/pethidine — neurotoxic metabolites (normeperidine) causing seizures and delirium; prefer morphine, oxycodone, or buprenorphine for pain.
- Skeletal muscle relaxants (cyclobenzaprine, baclofen at high dose) — anticholinergic and sedating; limited efficacy. [1]
Assessment tools — STOPP/START criteria (version 3)
The STOPP/START criteria (Screening Tool of Older Persons' Prescriptions / Screening Tool to Alert to Right Treatment), now in version 3 (O'Mahony et al, Eur Geriatr Med 2023, PMID 37256475), is the European-origin explicit tool used widely in the UK, Ireland, Europe and Australasia. It has two complementary halves, which is its key advantage over Beers: it detects both over-prescribing (STOPP — potentially inappropriate medications to stop) and under-prescribing (START — potentially prescribing omissions to start). [1]
Version 3 contains 190 criteria: 133 STOPP criteria and 57 START criteria, a major expansion from version 2 (114 criteria). It is organised by physiological system (cardiovascular, respiratory, gastrointestinal, neurological, renal, etc.), and version 3 has a stronger focus on drug-drug and drug-disease interactions, the geriatric syndromes (dementia, falls, urinary incontinence, constipation), and medications that increase falls risk. [1]
STOPP — potentially inappropriate prescriptions to STOP
STOPP flags medications that are likely to cause harm in older adults because they are:
- Used beyond the recommended duration (e.g., a PPI at full dose for more than 8 weeks without a specialist indication; a benzodiazepine for more than 2 to 4 weeks).
- Used where there is a drug-disease interaction (e.g., a beta-blocker in decompensated heart failure; an NSAID in CKD or heart failure).
- Used where there is a duplicate drug class (e.g., two NSAIDs; two antiplatelets without a clear indication; an ACE inhibitor and an ARB together).
- Used in high-risk combinations (e.g., warfarin plus an NSAID; multiple anticholinergics; an opioid plus a benzodiazepine — the "opioid-benzodiazepine" sedative load that drives falls and respiratory depression). [1]
START — potentially prescribing omissions to START
START flags drugs that are indicated but missing — the other side of appropriateness. Common omissions in older adults:
- An anticoagulant in atrial fibrillation at high stroke risk (CHA2DS2-VASc) without a contraindication.
- A statin in established cardiovascular disease (unless life expectancy is under 1 to 2 years).
- An ACE inhibitor in symptomatic heart failure with reduced ejection fraction.
- A beta-blocker in stable heart failure with reduced ejection fraction.
- Vitamin D and calcium supplementation (and a bisphosphonate where indicated) in confirmed osteoporosis.
- An SGLT2 inhibitor in heart failure with reduced ejection fraction or diabetic kidney disease.
- Influenza and pneumococcal vaccination where indicated. [1]
Beers vs STOPP/START — which to use?
In practice they are complementary and overlapping. Beers is the standard in the US and in many ABIM-style questions; STOPP/START is the standard in the UK, Ireland, Europe and much of Australasia, and it has the advantage of also detecting under-prescribing. For the FRACP DWE and DCE, know both — use STOPP/START as your primary bedside tool (because it covers omissions and is systems-based), and know the key Beers drugs (because they are the highest-yield MCQ targets). Both are explicit criteria: they flag a drug as potentially inappropriate, but the final decision rests on the clinician's judgement of the individual patient. [1]
DCE exam trap: A medication review that only stops drugs and never starts the ones that are missing is incomplete. The START criteria remind you to ask, every time, whether this older patient is missing an indicated drug (anticoagulation in atrial fibrillation, disease-modifying therapy in heart failure, osteoporosis treatment after a fracture). [1]
Medication reconciliation at transitions of care
Medication reconciliation is the formal process of ensuring that the medications the patient is actually taking are correctly and intentionally documented and ordered at every transition — admission, internal transfer, and discharge. It is a patient-safety standard (ACSQHC Standard 4 Medication Safety; NICE NG56 Medicines Optimisation), not an optional nicety, because transition errors are the source of a large proportion of preventable drug harm. [1]
The three steps of reconciliation
- Collect — obtain the best possible medication history (BPMH). This means more than copying the GP referral letter. It means at least two sources (the patient, the GP, the pharmacist, the residential aged-care medication chart, the dispensing records), and it explicitly asks about over-the-counter medications, complementary and herbal medicines, "as needed" medications, topical agents, inhalers, eye drops, and recently stopped medications. The BPMH includes the dose, frequency, route, indication, duration, and adherence for each drug.
- Compare — reconcile the BPMH against the current medication orders (the admission or transfer orders, or the discharge prescription). Identify every discrepancy — an omission, a duplication, a wrong dose, an unintended change.
- Communicate and decide — for each discrepancy, decide whether it is intentional (a deliberate change) or unintentional (an error), document the decision, communicate the reconciled list to the patient and the next clinician (the GP and the residential facility on discharge), and provide a written medication list to the patient. [1]
The discharge reconciliation — the highest-yield moment
The discharge medication reconciliation is the single most important opportunity to prevent post-discharge harm and to deprescribe. It is the moment to:
- Reconcile the pre-admission, inpatient, and intended discharge lists.
- Stop any medications that were started in hospital for a transient indication (e.g., a PPI started for stress ulcer prophylaxis in ICU; a hypnotic started for sleep on the ward; an antiemetic; a newly added antipsychotic for delirium).
- Resume, hold, or deprescribe each pre-admission medication based on the admission and the new goals.
- Confirm the indication, dose, monitoring plan, and review date for every drug that is continued.
- Provide the patient and the GP with an accurate, up-to-date medication list and a plan for review. [1]
High-risk medications in older adults
Some medications account for a disproportionate share of drug-related harm in older adults because they have a narrow therapeutic index, require individualised dosing, need active monitoring, and have potentially catastrophic adverse effects. The ISMP (Institute for Safe Medication Practices) "high-alert" list and the Beers criteria converge on the same culprits. [1]
| Medication | Why it is high-risk | What to do |
|---|---|---|
| Warfarin | Narrow therapeutic index; bleeding; drug and dietary interactions; greater INR sensitivity in older adults | Review the indication (consider a DOAC if appropriate); monitor the INR; review interacting drugs at every visit |
| Direct oral anticoagulants (DOACs) | Bleeding; renal clearance (apixaban partially, dabigatran heavily); dose errors (under- and over-dosing at the extremes of weight and renal function) | Confirm the indication; dose for renal function and weight; check renal function at least annually and with intercurrent illness; avoid in severe renal impairment where contraindicated |
| Insulin | Hypoglycaemia (the commonest preventable cause of ADR admission); dosing errors; reduced awareness of hypoglycaemia in older adults | Relax glycaemic targets in frailty (HbA1c 7.5 to 8.5 percent); prefer basal insulin; avoid sliding-scale insulin; review at every visit |
| Opioids | Over-sedation, respiratory depression, constipation, falls, delirium; accumulation in renal and hepatic impairment | Start low (morphine 2.5 mg as needed, or oxycodone 2.5 mg); use with a bowel regimen; review regularly; avoid in combination with benzodiazepines |
| Digoxin | Narrow therapeutic index; toxicity (nausea, visual disturbance, arrhythmia) at levels only slightly above therapeutic; accumulation in renal impairment and in older adults (reduced volume of distribution) | Use a lower maintenance dose (62.5 to 125 micrograms daily or less); monitor the level and the renal function; check for hypokalaemia and hypomagnesaemia (which potentiate toxicity) |
| Methotrexate (low dose) | Narrow therapeutic index; renal clearance; fatal toxicity from dosing errors (daily instead of weekly) | Confirm the weekly (not daily) dosing; check renal function, FBC and LFTs; prescribe folic acid; counsel the patient explicitly |
The deprescribing process
Deprescribing is the structured, supervised, patient-centred process of reducing or stopping inappropriate medications. The framework below (Scott et al, JAMA Intern Med 2015, PMID 25798731) is the one to use in the DCE and at the bedside. [1]

Step 1 — Ascertain all drugs in use
Build the complete, verified medication list — the BPMH. This is the medication reconciliation step: every regular and "as needed" drug, the dose, the frequency, the indication, the duration, the adherence, and any over-the-counter and complementary medicines. Without an accurate list, nothing else is reliable. [1]
Step 2 — Identify potentially inappropriate medications
Apply a structured tool — STOPP/START (to catch over- and under-prescribing), Beers (for the high-yield PIMs), and a targeted screen for drugs without a current indication, drugs where the harm now exceeds the benefit, drugs used beyond their recommended duration, duplicate drug classes, and high-risk combinations. Also ask the patient: which medications they believe are helping, which are causing problems, and which they would like to stop — their goals and preferences drive the priorities. [1]
Step 3 — Assess each medication against the current patient
For each flagged drug, weigh the current benefits against the current harms, in the context of:
- The patient's current goals of care (cure, function, symptom control, prolongation of life).
- Their life expectancy and time-to-benefit of the drug (a statin for primary prevention takes 2 to 5 years to show benefit — irrelevant if life expectancy is under 1 year).
- Their frailty (the Clinical Frailty Scale anchors the assessment; a CFS of 7 or more shifts the balance toward symptom-focused care).
- The risk of withdrawal or rebound (benzodiazepines, opioids, beta-blockers, clonidine, SSRIs, corticosteroids, and PPIs need a taper; antihypertensives may need a taper if there is a risk of rebound hypertension).
- The feasibility and burden of the monitoring the drug requires. [1]
Prioritise: stop the highest-harm, lowest-benefit drugs first; the ones the patient most wants to stop; the ones with the easiest taper; and the ones with the clearest evidence of harm. [1]
Step 4 — Plan the cessation — taper or stop
Communicate the plan to the patient, the family, the GP, the pharmacist, and the residential facility. For most drugs, a taper is safer and better tolerated than an abrupt stop. Provide a written deprescribing plan, document the indication for each change, and set a review date. [1]
Step 5 — Monitor for withdrawal, rebound, and return of the original condition
Review the patient at a defined interval (1 to 4 weeks for most deprescribing; sooner for high-risk drugs). Ask about withdrawal symptoms (anxiety, insomnia, agitation for benzodiazepines; tachycardia, hypertension, angina for beta-blockers; symptomatic relapse for any drug stopped). If symptoms recur, decide with the patient whether to restart at a lower dose, switch, or accept the symptom — the decision is shared, not unilateral. Most deprescribing attempts succeed without the symptom returning — the evidence consistently shows that the fear of relapse is greater than the reality. [1]
Deprescribing specific classes
Proton pump inhibitors (PPIs)
PPIs are among the most over-prescribed drugs in older adults. They are frequently started in hospital for stress ulcer prophylaxis (an ICU indication), for an acute gastrointestinal bleed, or for dyspepsia, and then continued indefinitely without a reassessment of the indication. Long-term PPI use is associated with an increased risk of hypomagnesaemia (and associated fractures and arrhythmias), vitamin B12 deficiency, Clostridioides difficile infection, community-acquired pneumonia, and an increased risk of osteoporotic fracture. [1]
When to deprescribe: Stop if there is no current specialist indication (severe reflux oesophagitis, Barrett oesophagus, a bleeding risk on dual antiplatelet or anticoagulant therapy, Zollinger-Ellison syndrome). Most patients on a PPI for more than 8 weeks without a specialist indication can have it tapered to the lowest effective dose or stopped, with a step-down (daily to alternate day to on-demand) or a switch to an H2 antagonist for rebound symptoms. Rebound acid hypersecretion occurs for up to 2 to 4 weeks; warn the patient and manage with antacids or on-demand therapy. [1]
Statins
Statins are highly effective for secondary prevention (established cardiovascular disease) and reduce mortality in that group, regardless of age. For primary prevention, the benefit depends on the absolute cardiovascular risk and the time horizon. The time-to-benefit for a statin in primary prevention is approximately 2 to 5 years for a cardiovascular event and longer for mortality. [1]
When to deprescribe: Consider stopping a statin when the life expectancy is under 1 year (end-of-life, advanced dementia, metastatic cancer), or when the statin is causing symptomatic adverse effects (myalgia, fatigue, cognitive symptoms) that are impairing quality of life in a patient in whom the primary-prevention benefit is marginal. Stopping a statin in the last year of life is one of the most evidence-supported deprescribing decisions and is associated with improved quality of life without a signal of harm. In a patient with established cardiovascular disease and a reasonable life expectancy, continue the statin. [1]
Bisphosphonates
Bisphosphonates accumulate in bone and have a persistent anti-resorptive effect after cessation. Long-term use (over 5 years, especially over 10 years) is associated with rare but serious harms: atypical femoral fractures and osteonecrosis of the jaw, in addition to the more common upper gastrointestinal effects. [1]
When to deprescribe: Offer a "drug holiday" after 5 years of oral bisphosphonate therapy (alendronate, risedronate) or 3 years of intravenous zoledronic acid in a patient whose fracture risk has improved and whose bone mineral density is stable. Reassess the fracture risk (bone mineral density, FRAX, and the trend in bone turnover markers) at 2 to 3 years during the holiday; restart if the risk rises. The drug holiday is not indefinite deprescribing — it is a structured pause with a defined reassessment. [1]
Antihypertensives
Tight blood pressure control can harm frail older adults through orthostatic hypotension, falls, syncope, and reduced cerebral perfusion presenting as dizziness or cognitive change. The SPRINT trial demonstrated benefit from intensive control (SBP under 120 mmHg) in selected robust older adults, but excluded frail patients and those in residential care, and the trial's intensive arm would be unsafe in many real-world frail patients. [1]
When to deprescribe: Reduce antihypertensives when the SBP is under 130 mmHg in a frail patient, when there is symptomatic orthostatic hypotension, when the patient has had a fall or a syncope episode, or when the goals of care have shifted toward comfort and function rather than long-term cardiovascular risk reduction. Reduce one agent at a time, monitor the blood pressure and the symptoms, and review. In a frail patient, a target SBP of 130 to 150 mmHg is often more appropriate than the 120 to 130 mmHg target of a robust younger patient. [1]
Benzodiazepines and Z-drugs
Benzodiazepines and the Z-drugs (zolpidem, zopiclone) are among the highest-priority deprescribing targets in older adults: they are associated with falls, fractures, cognitive impairment, delirium, motor vehicle crashes, and dependence, and the evidence for benefit (in insomnia and anxiety) is weak in this group. [1]
When to deprescribe: Aim to deprescribe in every older patient on a benzodiazepine or Z-drug, unless there is a compelling current indication (a severe, treatment-resistant anxiety disorder; alcohol withdrawal; a seizure disorder) that has been explicitly weighed against the harms. [1]
How to deprescribe: Taper slowly — reduce the dose by 10 to 25 percent every 1 to 2 weeks, using a long-acting benzodiazepine (diazepam) to substitute for a short-acting one if needed, and combine with cognitive behavioural therapy for insomnia (the most effective single intervention for chronic insomnia). Warn the patient about withdrawal symptoms (anxiety, insomnia, agitation, tremor, perceptual disturbance) and rebound. A slow, supervised taper succeeds in the majority of older patients. [1]
Antipsychotics for behavioural and psychological symptoms of dementia
Antipsychotics (risperidone, quetiapine, olanzapine) are sometimes used for the behavioural and psychological symptoms of dementia (BPSD), but they carry a black-box warning for increased mortality in dementia, and they cause sedation, falls, extrapyramidal effects, and stroke. The evidence for benefit is modest and limited to severe distress or danger. [1]
When to deprescribe: Initiate a non-pharmacological management plan (person-centred care, identification and treatment of unmet needs, environmental modification) as the first-line treatment of BPSD. If an antipsychotic has been started for an acute episode, set a review date (usually 3 months) with the explicit plan to taper and stop if the symptoms have settled. Regularly scheduled attempts to taper and stop antipsychotics in BPSD succeed in a substantial proportion of patients. [1]
Anticholinergic burden — a dedicated target
The anticholinergic burden is the cumulative central antimuscarinic effect of all the drugs a patient is taking. Each drug contributes a load (scored 0 to 3 on the Anticholinergic Burden Scale or the Anticholinergic Cognitive Burden Scale); the total burden predicts cognitive impairment, delirium, falls, and mortality. A total score of 3 or more is high risk and is a trigger for review. [1]
High-burden drugs to look for in every older patient: oxybutynin (the highest), solifenacin, tolterodine, hyoscine, amitriptyline and other tricyclics, diphenhydramine and chlorpheniramine (first-generation antihistamines), quetiapine, clozapine, paroxetine, and codeine (at high doses). The deprescribing strategy: identify every drug contributing to the burden, prioritise the highest-burden ones, and switch to lower-burden alternatives where an alternative is needed (mirabegron for oxybutynin; an SSRI other than paroxetine for depression; a second-generation antihistamine for a first-generation one; non-pharmacological measures for the underlying symptom where possible). [1]
Shared decision-making in deprescribing
Deprescribing is a shared decision, not a unilateral clinician act. The patient (and their family or carer) must understand:
- Why each medication was originally started and what it was intended to achieve.
- Whether it is still achieving that, or whether the balance of benefit and harm has shifted.
- What the alternatives are — including accepting the symptom, using a non-pharmacological approach, or switching to a safer drug.
- How the deprescribing will be done — the taper, the timeline, the monitoring, and the plan if the symptom returns. [1]
Many patients and families hold strong beliefs about their medications — that a drug is "keeping me alive", that stopping it is "giving up", or that every drug prescribed by a doctor must be permanent. These beliefs are often the biggest barrier to deprescribing, and they are addressed by a clear, respectful, goals-anchored conversation, not by a form. The conversation is the intervention. [1]
DCE long-case integration — the patient with polypharmacy and frailty
The DCE long case frequently features an older patient with multimorbidity and a long medication list — the archetypal "polypharmacy and frailty" case. The integration the examiner wants is a structured medication review that addresses every drug in the context of the whole patient, not disease by disease in isolation. [1]
The structured approach
- Build the verified medication list (BPMH) — every drug, dose, frequency, indication, duration, adherence, and recent changes.
- Apply STOPP and START systematically — list every potentially inappropriate medication and every prescribing omission.
- Apply Beers to catch the high-yield PIMs (benzodiazepines, anticholinergics, long-acting sulfonylureas, NSAIDs, first-generation antihistamines).
- Assess the renal function and dose-adjust every renally-cleared drug.
- Assess the anticholinergic burden and plan to reduce it.
- Anchor each decision to goals, prognosis and frailty (Clinical Frailty Scale).
- Prioritise the changes, taper where needed, set review dates, and communicate to the patient, the GP, and the pharmacist.
- Schedule a follow-up to monitor for withdrawal, rebound, and symptomatic change. [1]
The presentation
Present the medication review as an integrated part of the problem list — "Problem 7: polypharmacy with 14 regular medications, of which 4 are potentially inappropriate by STOPP/START and 2 are contributing to a high anticholinergic burden; my plan is to stop the oxybutynin and switch to mirabegron, taper and stop the temazepam over 4 weeks, stop the glyburide and switch to gliclazide, reassess the PPI and the statin in the context of her frailty and goals, and start the missing anticoagulant for her atrial fibrillation after discussing the bleeding risk with her and her son." [1]
DCE short case — the bedside medication review
Examiner instruction: "This 82-year-old man is in hospital with a fall. Please review his medications at the bedside." [1]
The routine
- Obtain and verify the list — ask the patient, check the drug chart, and (critically) ask the family or the GP for the pre-admission list, including over-the-counter and complementary medicines. Ask specifically about "as needed", topical, inhaler, and eye-drop medications.
- For each drug, ask: Is there a current indication? Is it working? Is it causing harm? Is the dose correct for the renal function and the age? Is it on the Beers or STOPP list? Is there a safer alternative? Could it be stopped?
- Check the renal function and dose-adjust the renally-cleared drugs.
- Assess the falls risk from medications — benzodiazepines, antipsychotics, antidepressants, opioids, antihypertensives (the Woolcott classes).
- Assess the anticholinergic burden and flag the high-burden drugs.
- Check for prescribing omissions (START) — is there an indicated drug missing?
- Present the plan — prioritised, with tapers and review dates, and communicated to the patient and the team. [1]
DWE exam trap: The most common DCE short-case error is to review medications one by one without a structured tool. Always name the tool you are using (STOPP/START or Beers), always check the renal function, and always ask about omissions as well as excesses. [1]
Exam traps and high-yield discriminators
- The prescribing cascade is the highest-yield concept. A vignette in which a new symptom appears in a patient on a known causative drug, and a new drug is added to treat it, is always testing the cascade. The correct answer is to address the first drug.
- A "normal" creatinine does not mean normal renal function in a frail older adult. Always estimate the GFR before dosing renally-cleared drugs, and prefer cystatin C if the muscle mass is very low.
- Benzodiazepines, anticholinergics and antipsychotics are the highest-yield deprescribing targets and appear in nearly every polypharmacy question. Know the harm profile and the taper.
- STOPP detects over-prescribing; START detects under-prescribing. A review that only stops drugs is incomplete. Always ask whether an indicated drug is missing (anticoagulation in atrial fibrillation; disease-modifying therapy in heart failure; osteoporosis treatment after a fracture).
- Statins and intensive glycaemic control are the classic examples of disease-oriented guidelines that cause harm when applied to frail patients with limited life expectancy. Know the time-to-benefit and the deprescribing thresholds.
- Medication reconciliation at transitions is the highest-yield systems-level intervention. Know the three steps: collect (BPMH), compare, communicate.
- The deprescribing process is patient-centred and supervised — never abrupt, never unilateral, always with a review plan. The fear of relapse is greater than the reality; most deprescribing succeeds.
- PPIs started in hospital are frequently continued indefinitely — this is a common error to spot in a medication review. Reassess the indication and taper. [1]
Key references
American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 2023;71(7):2052-2081 (PMID 37139824). O'Mahony D, O'Sullivan D, Byrne S, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med 2023;14(4):625-632 (PMID 37256475). Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing. JAMA Intern Med 2015;175(5):827-834 (PMID 25798731). Kongkaew C, Noyce PR, Ashcroft DM. Hospital admissions associated with adverse drug reactions: a systematic review of prospective observational studies. Ann Pharmacother 2008;42(7):1017-1025 (PMID 18594048). Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med 2009;169(21):1952-1960 (PMID 19933955). Inker LA, Eneanya ND, Coresh J, et al. New creatinine- and cystatin C-based equations to estimate GFR without race. N Engl J Med 2021;385:1737-1749 (PMID 34554658). NICE guideline NG56 — Medicines optimisation (2015). Australian Commission on Safety and Quality in Health Care — Medication Safety Standard. Australian Medicines Handbook — Aged Care and Dosing in Renal Impairment. [1]
References
- [1]American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [2]O'Mahony D, O'Sullivan D, Byrne S, O'Connor MN, Ryan C, Gallagher P STOPP/START criteria for potentially inappropriate prescribing in older people: version 3 Eur Geriatr Med, 2023.PMID 37256475
- [3]Scott IA, Hilmer SN, Reeve E, et al. Reducing inappropriate polypharmacy: the process of deprescribing JAMA Intern Med, 2015.PMID 25798731
- [4]Kongkaew C, Noyce PR, Ashcroft DM Hospital admissions associated with adverse drug reactions: a systematic review of prospective observational studies Ann Pharmacother, 2008.PMID 18594048
- [5]Woolcott JC, Richardson KJ, Wiens MO, et al. Meta-analysis of the impact of 9 medication classes on falls in elderly persons Arch Intern Med, 2009.PMID 19933955
- [6]Inker LA, Eneanya ND, Coresh J, et al. New Creatinine- and Cystatin C-Based Equations to Estimate GFR without Race N Engl J Med, 2021.PMID 34554658