Phys · geriatric
Urinary Incontinence IN Older Adults
Also known as Urinary Incontinence IN Older Adults · urinary incontinence in older adults
Consultant-physician depth guide to Urinary Incontinence IN Older Adults for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
Urinary Incontinence IN Older Adults is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]

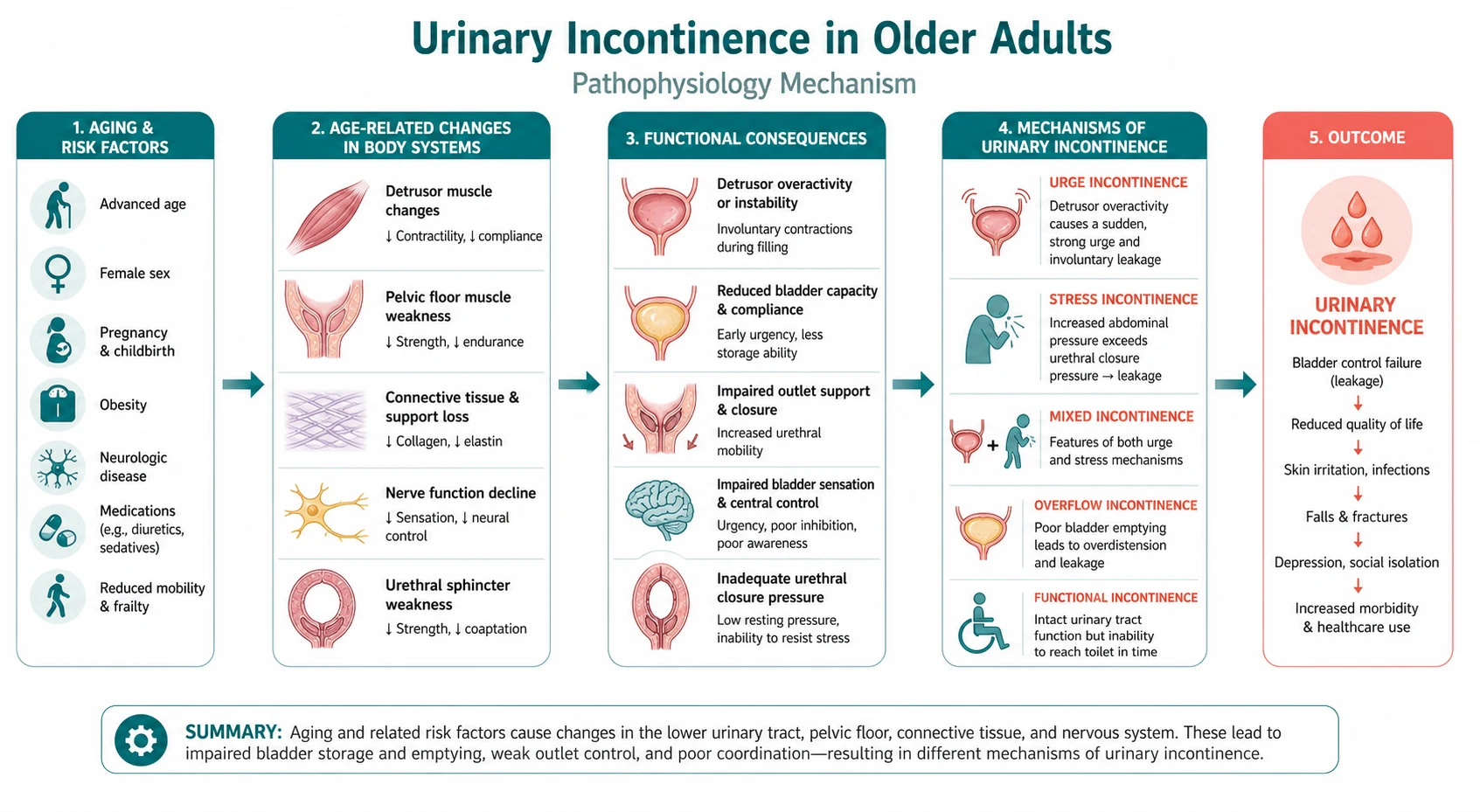
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
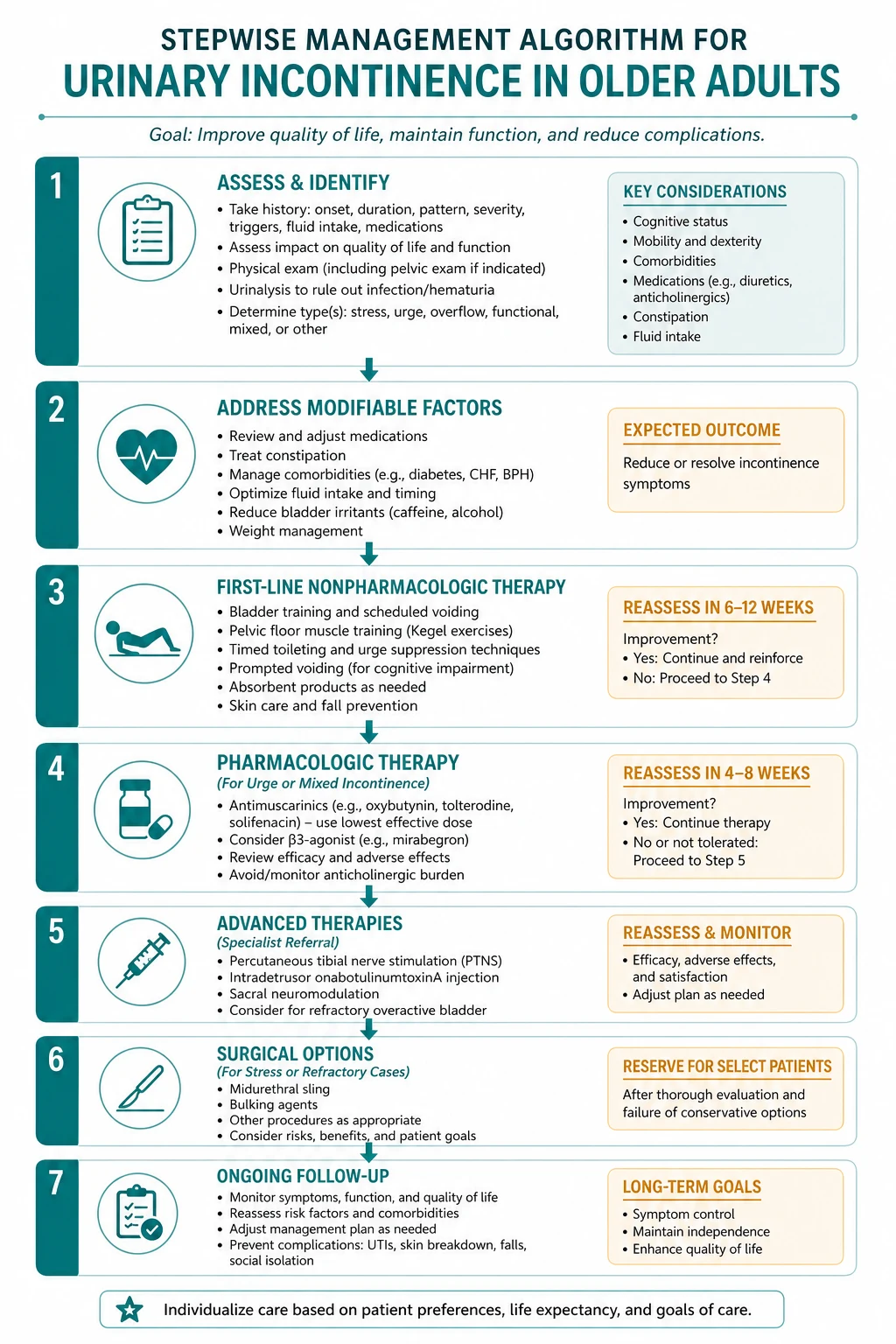
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]
Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Urinary Incontinence IN Older Adults to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Chen SF Modern management of pediatric nocturnal enuresis: Evidence-based treatment and practical guidance Tzu Chi Med J, 2026.PMID 42453518
- [2]Gu M, Choi YS, Sok S Analysis of Characteristics Associated With Advanced-Stage Pressure Injury Classification Among Korean Hospitalised Patients: A Secondary Data Analysis Nurs Open, 2026.PMID 42447083
- [3]Joshi R, Rathi M A Systematic Review With Meta-Analysis on the Role of Pelvic Floor Muscle Exercises on the Severity of Symptoms and Quality of Life in Women With Urinary Incontinence Arch Esp Urol, 2026.PMID 42438870
- [4]Martini S, Schluessel S, Aghamaliyev U, Rippl M, et al. Expert Evaluation of the Perceived Accuracy, Relevance, and Safety of Large Language Model-Generated Patient Information in Geriatrics: Cross-Condition Study JMIR AI, 2026.PMID 42081273
- [5]Banerjee I, Bibi F, Umoessien E, Pradhan R, et al. Quality and associated factors of guideline-concordant primary care referral for urinary incontinence and pelvic organ prolapse: A single centre retrospective observational study Eur J Obstet Gynecol Reprod Biol, 2026.PMID 41849977
- [6]Zhong CC, Chen M, Yang Z, Li Z, et al. Adoption of the Reference Framework for Preventive Care for Older Adults: a study of primary care physicians Fam Med Community Health, 2026.PMID 41807019
- [7]Xi Y, Yao T, Zhang C, Zhuang T Effectiveness of safety care and clinical nursing pathway in patients undergoing cardiovascular intervention: a randomized controlled trial Perioper Med (Lond), 2026.PMID 42469924
- [8]Marks FJ, Walters SJ, Sutton L, Jacques RM What statistical methods are more appropriate for predicting recruitment at the design stage of a randomised controlled trial? Trials, 2026.PMID 42469922
- [9]Hajiaqaei M, Mohammadi A Transcranial random noise stimulation (tRNS) over the left dorsolateral prefrontal cortex ameliorates emotion dysregulation and executive function: a single-blind, randomized, sham-controlled clinical trial BMC Psychol, 2026.PMID 42469906
- [10]Santos E, Bradfield Strydom M, Perelmuter S, Schloss J Postpartum health-seeking behaviours, awareness and experiences of Genitourinary Syndrome of Lactation Midwifery, 2026.PMID 42456325
- [11]Javanmardifard S, Gheibizadeh M, Shirazi F, Zarea K, et al. Managing the silent burden: a grounded theory study on urinary incontinence in older women BMC Geriatr, 2026.PMID 42426641
- [12]Milutinović D, Kennaway B, Stojković E, Baturan B, et al. Knowledge, attitudes, and predictors of urinary incontinence and overactive bladder as components of lower urinary tract symptoms among female healthcare professionals Front Glob Womens Health, 2026.PMID 42416371