Phys · haematological
Acute Leukaemia
Also known as acute myeloid leukaemia · AML · acute lymphoblastic leukaemia · ALL · acute promyelocytic leukaemia · APL · M3 leukaemia · acute leukaemia · blast crisis
Consultant-physician-depth guide to acute myeloid (AML) and acute lymphoblastic leukaemia (ALL) for FRACP DWE and DCE — AML-defining genetic events, APL as an emergency, 7+3 induction versus venetoclax combinations, ELN 2022 risk stratification, paediatric-inspired ALL and measurable residual disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Acute Leukaemia
The answer first
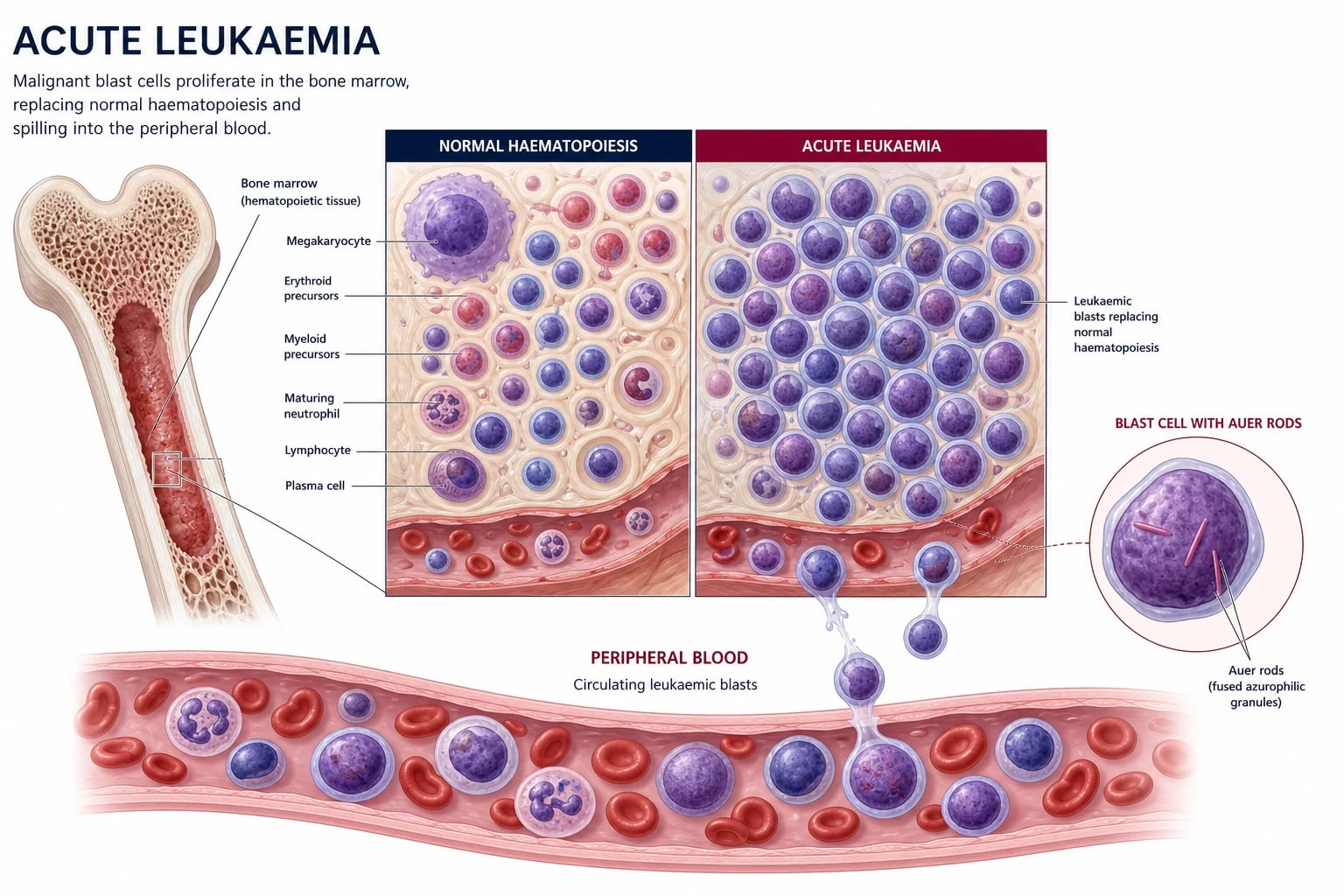
Acute leukaemia is a clonal expansion of immature haematopoietic precursor cells (blasts) that arrests normal marrow function. The patient presents over weeks with the consequences of marrow failure — infection (neutropenia), bleeding (thrombocytopenia, and disseminated intravascular coagulation in acute promyelocytic leukaemia), and fatigue (anaemia). The diagnosis rests on demonstrating 20 per cent or more blasts in the marrow or blood, with subtyping by immunophenotype and genetics [2].
Two bedside rules that change outcome: [1]
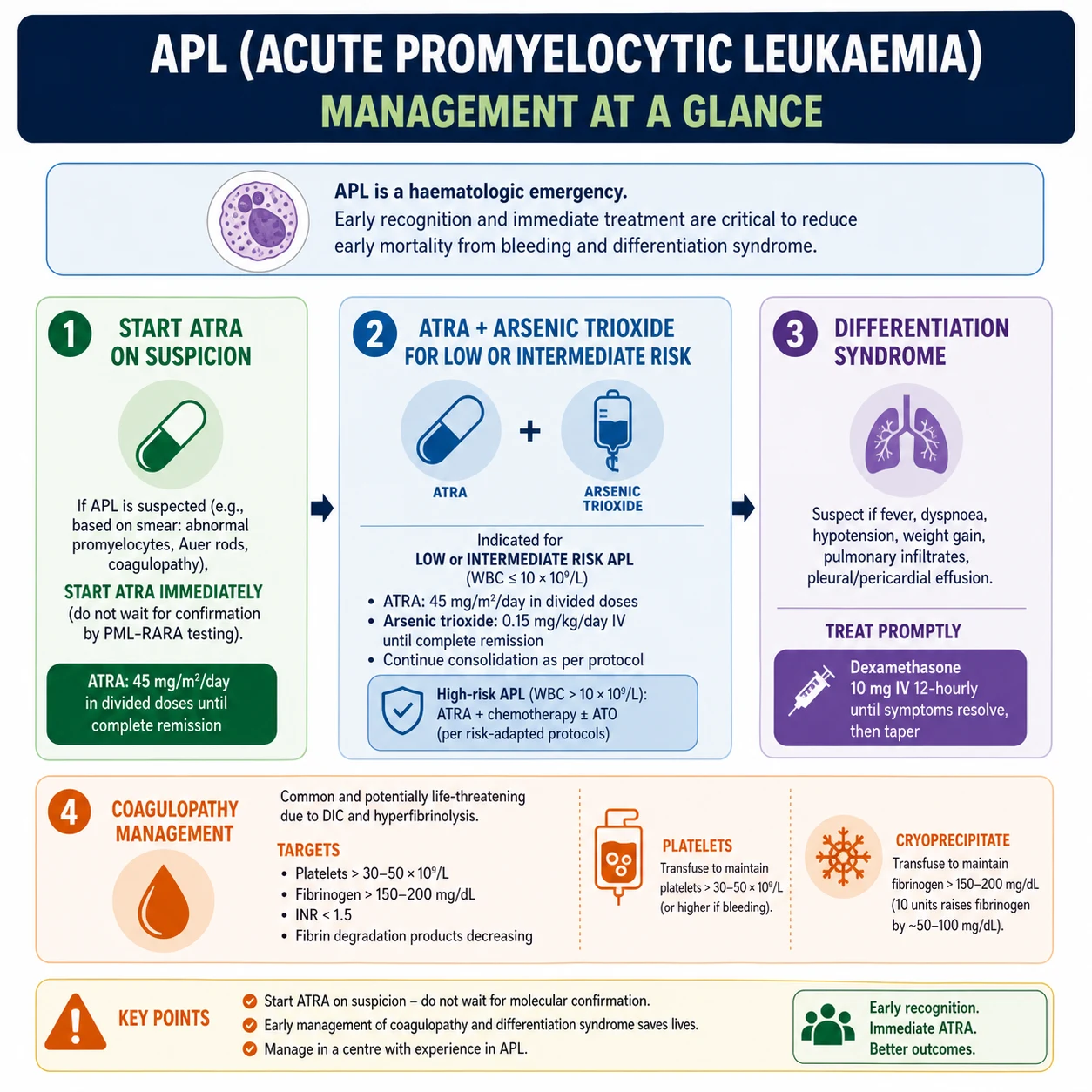
- Suspect APL? Start ATRA now. Acute promyelocytic leukaemia (APL, formerly M3) is the form of AML defined by the t(15;17) PML-RARA fusion. It presents with a bleeding emergency driven by DIC. All-trans retinoic acid (ATRA) reverses the coagulopathy and is started on suspicion — not on cytogenetic confirmation — because the principal danger is early death from cerebral or pulmonary haemorrhage [3].
- New leukaemia plus fever? Treat as neutropenic sepsis within one hour. Cultures then a broad-spectrum antipseudomonal beta-lactam (piperacillin-tazobactam or ceftazidime). The door-to-antibiotic time is a measurable survival determinant.
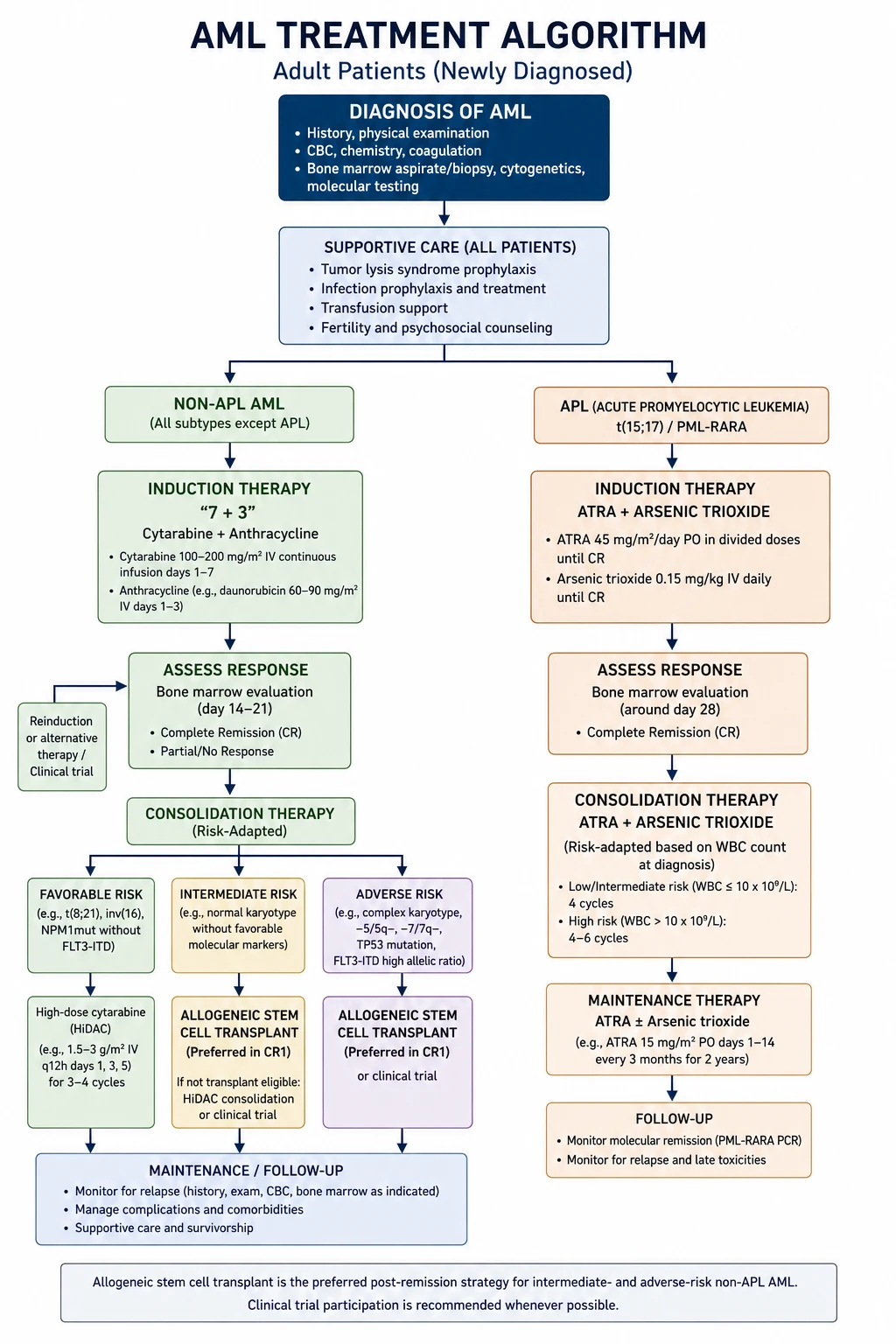
For fit adults with non-APL AML the backbone is 7+3 induction (7 days of cytarabine infusion plus 3 days of an anthracycline, daunorubicin 60 to 90 mg/m2), with midostaurin added for FLT3-mutated disease and the decision to consolidate with chemotherapy or allogeneic stem cell transplant driven by the 2022 European LeukemiaNet (ELN) risk group [1][4][6]. For the older or unfit patient the standard is azacitidine plus venetoclax [5].
For acute lymphoblastic leukaemia (ALL), the adult paradigm has shifted to paediatric-inspired regimens for younger adults (up to about 40 to 45 years), with a tyrosine kinase inhibitor added for Philadelphia-chromosome-positive disease and intrathecal CNS prophylaxis throughout [10][11].
Classification
Acute leukaemia is divided by lineage — myeloid (AML) or lymphoid (ALL) — and then by recurring genetic events that determine biology and treatment. The WHO framework requires 20 per cent or more blasts in marrow or blood for the diagnosis of AML, but specific recurring genetic abnormalities (PML-RARA, RUNX1-RUNX1T1, CBFB-MYH11, and some KMT2A rearrangements) are AML-defining regardless of the blast count [2].
AML — AML-defining genetic events (memorise these)
| Genetic lesion | Cytogenetics | Key point | Clinical correlate |
|---|---|---|---|
| PML-RARA | t(15;17) | APL (M3); blocks differentiation at promyelocyte stage | Coagulopathy emergency; ATRA and arsenic responsive; favourable prognosis |
| RUNX1-RUNX1T1 | t(8;21) | Core binding factor (CBF) leukaemia | Favourable; long thin Auer rods; high CD19 expression |
| CBFB-MYH11 | inv(16) or t(16;16) | CBF leukaemia with abnormal eosinophils | Favourable; can present with chloroma |
| KMT2A (MLL) rearrangement | 11q23 (e.g. t(9;11) MLLT3) | Common in therapy-related and infant leukaemia | Adverse in most adults; aggressive biology |
| FLT3-ITD | Molecular (not karyotype) | Most common AML mutation (~25 per cent) | High relapse; add midostaurin (RATIFY) |
| NPM1 mutation | Molecular | Common (~30 per cent) | Favourable when isolated (no FLT3-ITD, no adverse cytogenetics) |
| Biallelic CEBPA | Molecular | ~5 to 10 per cent | Favourable prognosis |
| Monosomy 5 / 5q-, monosomy 7 / 7q-, complex karyotype, TP53 | Cytogenetics | Myelodysplasia-type abnormalities | Adverse prognosis |
DWE high-yield: t(15;17), t(8;21) and inv(16) are AML-defining regardless of blast count. If a vignette gives a young patient with promyelocyte blasts and a bleeding tendency, the answer is APL — start ATRA on suspicion, do not wait for cytogenetics. [1]
ALL — subtype framework
ALL is divided by lineage (B or T) and then by genetics: [1]
- B-ALL: CD19, CD22, CD79a, TdT positive. Key subtypes include BCR-ABL1 (Philadelphia chromosome, rising incidence with age — about 25 per cent of adult ALL and historically adverse), ETV6-RUNX1 (favourable, more common in children), KMT2A rearrangements (adverse), and hyperdiploidy.
- T-ALL: CD3, CD7 positive; often presents with a mediastinal mass and superior vena cava obstruction in a young adult male. Driven by NOTCH1 activation. [1]
Pathophysiology
AML — clonal arrest of myeloid differentiation
AML arises when a haematopoietic stem or early progenitor cell acquires cooperating mutations — a class I mutation (proliferation/survival, e.g. FLT3, RAS) and a class II mutation (differentiation, e.g. PML-RARA, RUNX1-RUNX1T1, NPM1). The myeloid precursor is arrested at an immature stage, accumulates in the marrow, and crowds out normal haematopoiesis. The marrow fails. The patient bleeds, infects and tires. [1]
DWE conceptual: Why does cytarabine (a pyrimidine analogue that inhibits DNA polymerase) require a 7-day continuous infusion? Because it is S-phase specific — it kills only blasts that are actively dividing. The 7-day infusion maximises the fraction of blasts caught in S-phase. Daunorubicin (an anthracycline that intercalates DNA and inhibits topoisomerase II) is given for 3 days alongside it. Together: 7+3. [1]
APL — a differentiation block that is reversible
The t(15;17) translocation fuses the PML gene on chromosome 15 with the RARA retinoic acid receptor gene on chromosome 17. The PML-RARA fusion protein blocks myeloid differentiation at the promyelocyte stage and protects the leukaemic cell from apoptosis. ATRA binds the fusion protein, releases the block and allows the leukaemic promyelocytes to mature into neutrophils that then die naturally. Arsenic trioxide degrades PML-RARA and adds apoptosis. The combination achieves long-term cure in standard-risk disease without chemotherapy [3].
The coagulopathy is mechanistic: leukaemic promyelocytes express tissue factor and annexin II, which drive disseminated intravascular coagulation and hyperfibrinolysis. The dominant clinical phenotype is bleeding — bruising, mucosal haemorrhage, intracranial and pulmonary bleeds — and early haemorrhagic death is the principal danger in the first weeks. [1]
ALL — lymphoid precursor arrest
ALL arises from the clonal expansion of lymphoid precursor cells arrested at the B-cell or T-cell stage. The biology is shaped by fusion genes: BCR-ABL1 (Philadelphia chromosome, from t(9;22)) drives constitutive tyrosine kinase signalling and is the most important adverse lesion in adult ALL; ETV6-RUNX1 and hyperdiploidy are favourable, mainly in children. T-ALL is driven by NOTCH1 activation and often presents with a mediastinal mass. [1]
Clinical presentation
Bone marrow failure (common to AML and ALL)
| Lineage affected | Symptom | Sign |
|---|---|---|
| Neutrophils | Fever, sore throat, recurrent or severe infection | Fever, septic focus, perianal infection, line infection |
| Platelets | Bruising, epistaxis, gum bleeding, menorrhagia | Petechiae, purpura, ecchymoses, fundal haemorrhages |
| Red cells | Fatigue, dyspnoea, angina (in coronary disease) | Pallor, flow murmur, tachycardia |
| Blasts in blood | Sometimes none; occasionally symptoms of leucostasis (see below) | High white cell count on FBC |
The history is short — weeks, not months. This is a key discriminator from chronic leukaemia and from myelodysplasia. [1]
Tissue infiltration (more pronounced in AML and in monocytic/T-ALL subtypes)
- Gum hypertrophy — monocytic AML (M4, M5); the gums are swollen, boggy and bleeding. A high-yield MCQ and a striking bedside sign.
- Skin deposits (leukaemia cutis) — violaceous papules, nodules or plaques. Specific to AML with monocytic differentiation and to some ALL.
- Myeloid sarcoma (chloroma) — a solid green-coloured mass of myeloid blasts, classically in the skin, orbit, bone, or epidural space. Can precede marrow disease.
- Central nervous system — cranial nerve palsies (especially facial nerve), meningism. More common in ALL, in high-count monocytic AML, and at relapse.
- Hepatosplenomegaly and lymphadenopathy — more prominent in ALL than AML.
- Testicular swelling — a sanctuary site in ALL. [1]
APL — the coagulopathy emergency
APL often presents with bruising out of proportion to the platelet count, with bleeding from venepuncture sites and gums, and with fundal haemorrhages. The blood count usually shows pancytopenia with a low platelet count, and the film shows promyelocytes (often with heavy granulation and Auer rods). Coagulation shows a low fibrinogen, elevated INR and APTT, and a high D-dimer — the classic DIC pattern. [1]
DCE long-case trap: APL is the form of AML in which early death — usually cerebral or pulmonary haemorrhage — is more dangerous than the leukaemia itself if not managed promptly. The diagnostic question "could this be APL?" must be asked of every new leukaemia presentation, because ATRA is given on suspicion. [1]
ALL-specific features
- Anterior mediastinal mass (T-ALL) — in a young adult male presenting with superior vena cava obstruction (facial plethora, distended neck veins, cough), consider T-ALL alongside lymphoma and thymoma.
- Lymphadenopathy and hepatosplenomegaly — more prominent than in AML.
- CNS disease — cranial nerve palsies at diagnosis; the rationale for CNS prophylaxis throughout treatment.
- Bone pain — especially in the long bones and back; can mimic growing pains in adolescents. [1]
Leucostasis (a hyperleukaemic emergency)
A white cell count over about 100 with symptoms of microvascular plugging: confusion, visual disturbance, dyspnoea, chest pain, priapism. This is most common in AML with a high blast count and in monocytic subtypes, and demands urgent cytoreduction (hydroxyurea, leucapheresis) — not the same as tumour lysis syndrome. APL with a high count is high-risk for early bleeding. [1]
Differential diagnosis of pancytopenia with blasts
| Condition | Discriminating features |
|---|---|
| Acute leukaemia (AML or ALL) | Blasts 20 per cent or more; Auer rods (AML); flow cytometry confirms lineage |
| Myelodysplastic syndrome (MDS) | Blasts below 20 per cent; dysplastic morphology; cytopenias; complex karyotype |
| Aplastic anaemia | Severe pancytopenia with a hypocellular marrow; no blasts; usually no organomegaly |
| Myelofibrosis | Teardrop poikilocytes; dry tap; splenomegaly; reticulin fibrosis on trephine |
| Megaloblastic anaemia | Macrocytosis; hypersegmented neutrophils; low B12 or folate; reversible |
| Metastatic marrow infiltration | Solid cancer history; tear-drop cells; may see circulating nucleated red cells |
| Leukaemoid reaction | Reactive neutrophilia; toxic granulation; high LAP score; no blasts; sepsis or malignancy |
| Chronic myeloid leukaemia (CML) | High white cell count with full spectrum of maturation; basophilia; BCR-ABL positive; low LAP score |
DWE discriminator: Auer rods are pathognomonic for AML. If the film shows blasts with Auer rods, the lineage is myeloid and the diagnosis is AML — do not wait for flow cytometry to act. [1]
Investigations
Essential for every patient with suspected acute leukaemia
| Investigation | Why |
|---|---|
| Full blood count and film | Pancytopenia with blasts; Auer rods (AML); promyelocytes with heavy granulation (APL); baseline counts |
| Coagulation — PT/INR, APTT, fibrinogen, D-dimer | DIC screen — mandatory in APL; baseline for invasive procedures |
| U&E, creatinine, LFTs, LDH, urate, calcium, phosphate | Baseline organ function; tumour burden (LDH, urate); tumour lysis risk |
| Blood cultures, viral serology (HIV, HBV, HCV, CMV) | Sepsis workup; viral co-infections affect conditioning and transfusion |
| Group and screen | Anticipate transfusion; red cell alloantibodies |
| ECG and echocardiogram | Baseline cardiac function before anthracycline; ejection fraction |
| Bone marrow aspirate and trephine | Definitive diagnosis — blast percentage, morphology, immunophenotype, cytogenetics, molecular |
The marrow examination — four layers of information
- Morphology on aspirate smears — blast percentage (20 per cent threshold), Auer rods (myeloid), cytoplasmic features (promyelocyte granulation in APL).
- Immunophenotyping by multiparameter flow cytometry — confirms lineage (myeloid CD13/CD33/MPO versus lymphoid CD19/CD22/CD79a/CD3), identifies leukaemia-associated immunophenotype for later MRD monitoring.
- Conventional karyotyping (cytogenetics) and FISH — the translocations: t(15;17), t(8;21), inv(16), 11q23, monosomy 5 or 7, complex karyotype. AML-defining.
- Molecular testing (next-generation sequencing panel) — FLT3-ITD, FLT3-TKD, NPM1, CEBPA (biallelic), IDH1, IDH2, TP53, RUNX1, ASXL1. These drive risk group (ELN 2022) and direct targeted therapy (midostaurin for FLT3; venetoclax combinations; IDH inhibitors). [1]
DWE high-yield: Every newly diagnosed AML patient must have FLT3 testing at diagnosis because midostaurin improves survival when added to standard chemotherapy (the RATIFY trial) [4]. A delay in testing means a delay in adding the targeted agent.
Lumbar puncture — selective
- ALL: routine at induction and for symptoms; usually combined with intrathecal chemotherapy (methotrexate, cytarabine, hydrocortisone).
- AML: only if symptomatic with CNS signs, or in high-risk monocytic AML, or with high blast count at diagnosis. [1]
Management of AML (non-APL)
Step 1 — Decide on fitness and intent
The decision between intensive and lower-intensity therapy is not driven by age alone but by performance status, comorbidity (cardiac, renal, hepatic), frailty, and patient preference. As a rule of thumb: [1]
- Fit, younger patient (typically under 60 to 65, good performance status, no severe comorbidity) — intensive induction with 7+3.
- Older or unfit patient (poor performance status, significant comorbidity, adverse biology) — lower-intensity therapy with azacitidine plus venetoclax.
- Very frail patient, or patient who declines intensive therapy — supportive (palliative) care with transfusion and symptom control. [1]
Step 2 — Intensive induction: 7+3
The backbone for fit patients is 7+3: [1]
| Drug | Dose | Days |
|---|---|---|
| Cytarabine | 100 mg/m2 per day by continuous intravenous infusion | Days 1 to 7 |
| Daunorubicin | 60 mg/m2 per day IV bolus (90 mg/m2 for patients under 60 in some protocols) | Days 1 to 3 |
The E1900 trial established that high-dose daunorubicin (90 mg/m2) improves complete remission and overall survival versus 45 mg/m2 in younger adults; subsequent trials (UK NCRI AML17) showed 60 mg/m2 and 90 mg/m2 are broadly equivalent for older adults [6].
Targeted additions based on genetics: [1]
- FLT3 mutation — add midostaurin 50 mg twice daily on days 8 to 21 of induction and consolidation (RATIFY showed improved overall survival) [4].
- CD33-positive AML — add gemtuzumab ozogamicin (an antibody-drug conjugate) in fractionated doses (3 mg/m2 on days 1, 4, 7); the ALFA-0701 trial showed improved event-free survival [7].
- IDH1 or IDH2 mutation — IDH inhibitors (ivosidenib, enasidenib) in relapsed disease and now in combinations.
The aim is complete remission (CR): marrow blasts below 5 per cent, neutrophils at least 1.0 and platelets at least 100, with no extramedullary disease. CR is achieved in 70 to 80 per cent of younger fit adults. [1]
Step 3 — Consolidation and the transplant decision
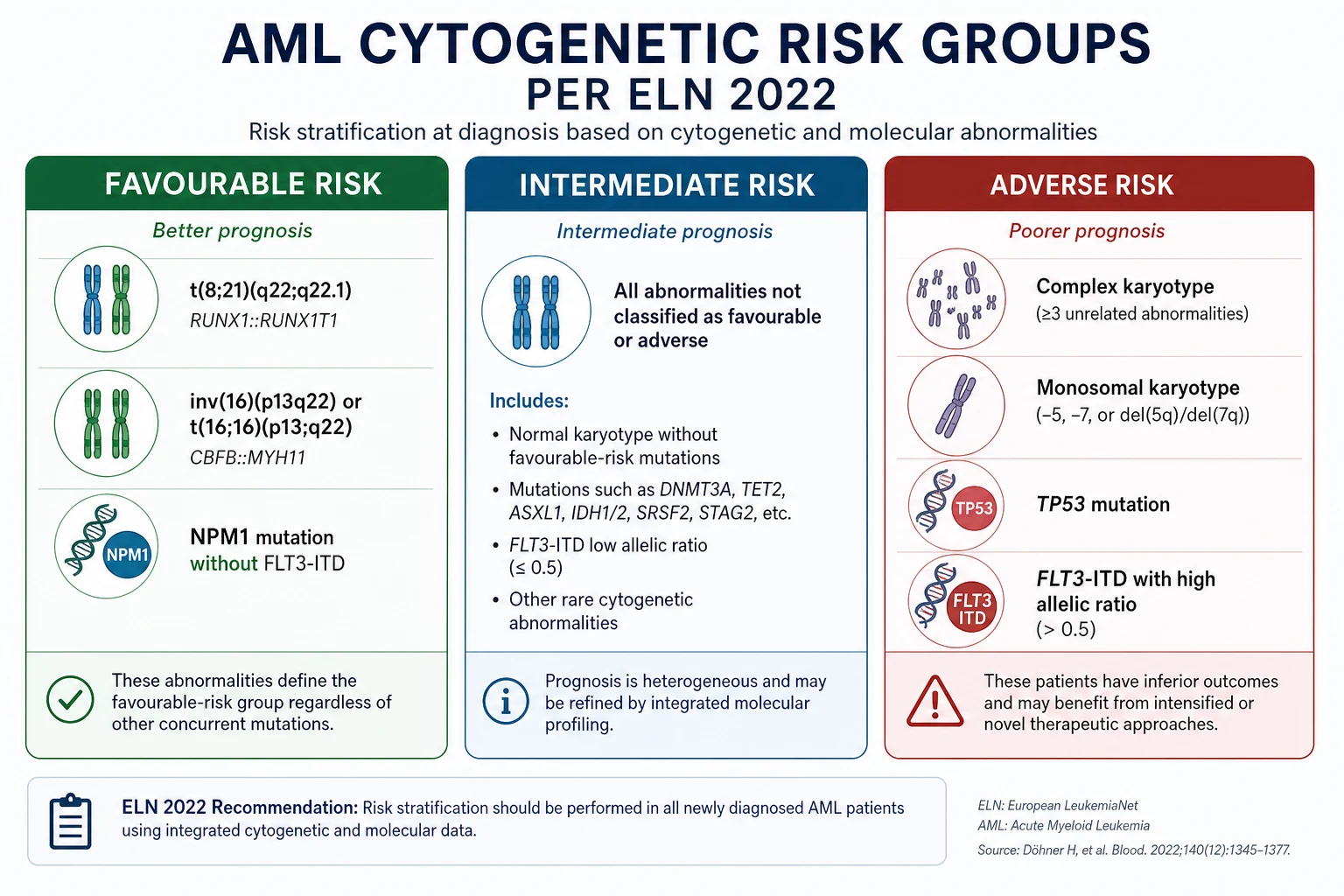
After CR, the consolidation strategy is driven by the ELN 2022 risk group [1]:
| Risk group | Defining features | Strategy |
|---|---|---|
| Favourable | t(8;21), inv(16); NPM1-mutated without FLT3-ITD; biallelic CEBPA | High-dose cytarabine consolidation; no allogeneic HSCT in first CR |
| Intermediate | FLT3-ITD (now intermediate in ELN 2022, regardless of allelic ratio); other mutations/cytogenetics not favourable or adverse | Consider allogeneic HSCT, especially with MRD positivity |
| Adverse | Monosomy 5 or 7, 5q- or 7q-, complex karyotype, TP53 mutation, KMT2A rearrangements, ASXL1/RUNX1, myelodysplasia-related gene mutations | Allogeneic HSCT in first CR if a donor is available |
DWE high-yield (ELN 2022 update): In the 2022 ELN revision, the FLT3-ITD allelic ratio is no longer used. All FLT3-ITD-mutated AML is classified as intermediate risk, regardless of the ratio or the co-presence of NPM1. NPM1-mutated AML is favourable only when FLT3-ITD is absent and no adverse-risk cytogenetic or molecular abnormality is present [1].
Step 4 — Allogeneic stem cell transplant
Allogeneic haematopoietic stem cell transplant (HSCT) offers the only realistic chance of cure in adverse-risk AML, through the graft-versus-leukaemia effect. Donor sources in order of preference: [1]
- HLA-matched sibling donor (best outcomes).
- HLA-matched unrelated donor (from international registries).
- Haploidentical related donor (parent, child, sibling — half-match).
- Umbilical cord blood (especially useful for patients from diverse ethnic backgrounds where matched donors are scarce). [1]
Myeloablative conditioning is preferred in fit younger patients; reduced-intensity conditioning extends HSCT to older patients (into the 60s and sometimes 70s). Complications include graft-versus-host disease, opportunistic infection, and secondary malignancy. [1]
Step 5 — Lower-intensity therapy for the unfit
For patients not fit for 7+3, azacitidine plus venetoclax is the standard of care. The VIALE-A trial showed that the combination improved complete remission (36.7 per cent versus 17.9 per cent) and overall survival (median 14.7 versus 9.6 months) compared with azacitidine alone in previously untreated adults with AML who were ineligible for intensive induction [5]. Cytopenias are the main toxicity; many units reduce the venetoclax duration from 28 to 14 or 21 days in responding patients to limit marrow suppression.
APL — a separate emergency pathway
APL is managed differently from other AML because the bleeding risk dominates. The pathway is: [1]
Immediate (on suspicion — do not wait for cytogenetic confirmation)
- Start ATRA (all-trans retinoic acid) 45 mg/m2 per day in divided doses, immediately on suspicion based on morphology or coagulopathy pattern. [1]2. Send urgent PML-RARA testing (FISH or RT-PCR) to confirm.
- Correct coagulopathy aggressively — keep platelets over 30 to 50, fibrinogen over 1.5 g/L using cryoprecipitate, and INR and APTT near normal with fresh frozen plasma. Transfuse to haemoglobin over 80 g/L.
- Avoid invasive procedures (intramuscular injections, arterial lines, unnecessary lumbar punctures) while coagulopathic.
- Admit to a monitored bed with haematology, transfusion and intensive care as a single team. [1]
Risk-stratified treatment (the Sanz classification) [8]
| Risk group | WCC | Platelets | Treatment |
|---|---|---|---|
| Low / intermediate | Up to 10 | Any | ATRA plus arsenic trioxide (chemotherapy-free); long-term cure in most patients [3] |
| High | Over 10 | Any | ATRA plus arsenic plus chemotherapy (anthracycline-based, e.g. idarubicin); higher relapse and bleeding risk |
The Lo-Coco trial established that ATRA plus arsenic trioxide (without chemotherapy) was non-inferior and indeed superior to ATRA plus chemotherapy in low-to-intermediate risk APL, with 2-year event-free survival of 97 per cent and complete remission in essentially all evaluable patients [3]. This transformed APL from the most lethal to the most curable form of adult AML.
Differentiation syndrome — recognise and treat
Differentiation syndrome (formerly retinoic acid syndrome) occurs in the first 3 weeks of ATRA or arsenic as the leukaemic promyelocytes differentiate and release cytokines. The clinical picture is a systemic inflammatory response: [1]
- Fever
- Dyspnoea with pulmonary infiltrates
- Weight gain and peripheral oedema
- Pleural or pericardial effusion
- Hypotension
- Acute kidney injury [1]
Treatment is immediate dexamethasone 10 mg intravenously twice daily, started on clinical suspicion rather than waiting for confirmation [9]. Hold ATRA or arsenic if severe. Provide supportive care — oxygen, diuresis, ventilatory support as needed.
DWE discriminator: A patient on ATRA for APL develops fever, dyspnoea and bilateral pulmonary infiltrates on day 10. The answer is dexamethasone immediately for differentiation syndrome — not antibiotics alone. Sepsis is in the differential and broad antibiotics are reasonable as well, but the differentiating-agent syndrome is the diagnosis that must be treated within hours. [1]
Acute lymphoblastic leukaemia (ALL)
ALL is the commonest childhood cancer but adult ALL carries a far worse prognosis — driven by a higher proportion of adverse cytogenetics (especially the Philadelphia chromosome, which rises from rare in children to about 25 per cent in adults and over 50 per cent in older adults) and lower tolerance of the intensive schedules that cure children. [1]
Induction
The backbone in adults has shifted to paediatric-inspired regimens for adolescents and young adults (up to about 40 to 45 years). These regimens — pioneered by groups such as GRAALL — use higher cumulative doses of the agents that work in children: vincristine, corticosteroids (dexamethasone preferred over prednisolone for CNS penetration), L-asparaginase, and anthracycline, with more prolonged maintenance and CNS prophylaxis. The GRAALL-2003 study showed improved complete remission (94 per cent versus 88 per cent) and improved event-free survival and overall survival in adults up to 60 years compared with historical adult regimens, with the benefit concentrated in patients under 45 [10].
Toxicity is the price — osteonecrosis of the hip and knee (especially in adolescents on corticosteroids), hepatotoxicity from asparaginase (with coagulation disturbance from antithrombin depletion), pancreatitis, thrombosis, and allergic reactions. [1]
Philadelphia-positive ALL — add a tyrosine kinase inhibitor
About a quarter of adult ALL carries the BCR-ABL1 fusion (t(9;22), the Philadelphia chromosome). Historically this carried a dismal prognosis. The addition of a tyrosine kinase inhibitor — imatinib first, then dasatinib (more potent, better CNS penetration) — to chemotherapy transformed outcomes. The most recent paradigm is a chemotherapy-free strategy of dasatinib plus blinatumomab (a bispecific T-cell engager targeting CD19) — the D-ALBA study reported 18-month disease-free survival of about 95 per cent and is changing practice in older Ph-positive patients [11].
Consolidation, CNS prophylaxis and maintenance
- Consolidation cycles continue the intensive block-then-recovery pattern, often with high-dose methotrexate and cytarabine.
- CNS prophylaxis — intrathecal chemotherapy (methotrexate, cytarabine, hydrocortisone) is given throughout treatment because the CNS is a sanctuary site that standard systemic therapy penetrates poorly. Without CNS prophylaxis, CNS relapse was common; with it, relapse is rare.
- Maintenance — daily 6-mercaptopurine and weekly methotrexate for 2 to 3 years, an essential component of the paediatric-inspired approach. [1]
Stem cell transplant in ALL
Allogeneic HSCT in first complete remission is considered for high-risk biology: Philadelphia-positive ALL (though this is shifting as TKI-plus-blinatumomab outcomes improve), hypodiploidy, KMT2A rearrangements, MRD positivity at end of induction, and primary refractory disease. [1]
Measurable (minimal) residual disease
Measurable residual disease (MRD) — the detection of leukaemia below the threshold of morphology — is the strongest predictor of relapse in both AML and ALL. Methods: [1]
- Multiparameter flow cytometry (MPF) — detects leukaemia-associated immunophenotype at sensitivities of 1 in 1000 to 1 in 10,000.
- Molecular assays — RT-PCR for fusion transcripts (PML-RARA, RUNX1-RUNX1T1, CBFB-MYH11, BCR-ABL1) and for NPM1; IG/TCR clonality for ALL; NGS-based assays at sensitivities of 1 in a million.
- Timing — at end of induction (the most important timepoint), then at consolidation milestones. [1]
MRD positivity at end of induction in AML or ALL is an indication to escalate — allogeneic HSCT, or in Ph-positive ALL a switch in therapy (blinatumomab, inotuzumab). MRD negativity is the modern goal of induction, not just morphological complete remission. [1]
Supportive care
Supportive care is not an afterthought — it is the difference between survival and death in acute leukaemia, and a registrar who delivers it well is the patient's best advocate. [1]
Neutropenic sepsis — the door-to-antibiotic rule
Fever in a neutropenic patient (neutrophils below 0.5, or under 1.0 and falling) is neutropenic sepsis until proven otherwise. The protocol: [1]
- Recognise — single oral temperature over 38.3, or sustained over 38.0 for an hour. Do not wait for a focus.
- Culture — blood cultures (peripheral and from each lumen of any central line), urine, sputum, swab any obvious focus including the perianal area.
- Empiric antibiotic within one hour — piperacillin-tazobactam 4.5 g IV every 6 to 8 hours (or ceftazidime, or meropenem in unstable patients). Add vancomycin if there is line infection, haemodynamic instability, mucositis, or local MRSA prevalence.
- Reassess at 48 to 72 hours — escalate or de-escalate based on cultures and response; add antifungal (liposomal amphotericin or an echinocandin) for persistent fever.
- ICU early if haemodynamically unstable. [1]
Tumour lysis syndrome
Rapid blast lysis releases potassium, phosphate and urate. Prevent with: [1]
- Aggressive intravenous hydration (3 L/m2 per day, goal urine output at least 100 mL/m2 per hour).
- Allopurinol 300 mg daily for lower-risk, or rasburicase (a recombinant urate oxidase, 0.15 to 0.2 mg/kg) for high-risk (high tumour burden, high white cell count, high LDH, renal impairment) or established tumour lysis syndrome.
- Frequent monitoring — potassium, phosphate, calcium, creatinine, urate every 4 to 6 hours for the first 48 hours.
- Renal replacement therapy for refractory hyperkalaemia, symptomatic hypocalcaemia, volume overload, or anuric AKI. [1]
DWE trap: Allopurinol inhibits xanthine oxidase (reducing urate production) but does nothing for the existing urate load; rasburicase breaks down existing uric acid and is preferred for high-risk or established TLS. Allopurinol is contraindicated (or dose-reduced) with azathioprine and 6-mercaptopurine (shared metabolism). [1]
Transfusion
- Red cells to keep haemoglobin over 70 to 80 g/L (higher if symptomatic or with ischaemic heart disease). [1]- Platelets to keep above 10 (prophylactic), above 20 (febrile), above 30 to 50 (active bleeding or before procedures, and in APL).
- Irradiated blood products for patients who will have, are having, or have had allogeneic HSCT, and after purine analogue therapy, to prevent transfusion-associated graft-versus-host disease.
- CMV-negative products for CMV-negative transplant candidates. [1]
Psychological and social support
A new leukaemia diagnosis is a catastrophe. Early input from a clinical psychologist, social work, and a named haematology clinical nurse specialist is part of standard care. Fertility preservation must be discussed before chemotherapy for any patient of reproductive age. [1]
Prognosis
AML — driven by age, fitness and genetics
- Overall 5-year survival in adults is about 30 per cent, but ranges from over 60 per cent in younger fit patients with favourable-risk disease (t(8;21), inv(16), NPM1-mutated without FLT3-ITD) to under 10 per cent in older unfit patients with adverse genetics (TP53-mutated, complex karyotype, monosomy 7).
- APL is the exception — 5-year overall survival of 80 to 90 per cent with modern ATRA-plus-arsenic protocols [3].
- Prognostic markers — age, performance status, white cell count at diagnosis, cytogenetic and molecular risk group (ELN 2022), and MRD status at end of induction.
ALL — driven by age, genetics and MRD
- Overall 5-year survival in adults is about 40 per cent, with younger patients on paediatric-inspired regimens approaching 60 to 70 per cent and older patients with Ph-positive disease historically much worse (now improved with TKI and blinatumomab).
- MRD negativity at end of induction is the single strongest predictor of relapse-free survival. [1]
DCE long-case approach
Opening statement (SASPOP)
"This is Mrs R, a 64-year-old retired teacher who presents with a four-week history of fatigue, easy bruising and two episodes of fever, found on blood count to have a pancytopenia with circulating blasts and on marrow to have acute myeloid leukaemia with an NPM1 mutation and a normal karyotype. Her main problems are the leukaemia itself (favourable-risk by ELN 2022, but only if no FLT3-ITD co-exists), the immediate risk of neutropenic infection, her coexisting type 2 diabetes and ischaemic heart disease that constrain anthracycline dosing, the psychosocial shock of the diagnosis on her and her family, and the question of whether she is a candidate for curative-intensive versus lower-intensity therapy. My priorities are to confirm the molecular profile (FLT3 status), control infection, transfuse to safe thresholds, and engage the haematology multidisciplinary team and the patient in a shared decision on induction." [1]
Structured problem list
- Newly diagnosed AML — confirm molecular risk (FLT3 status pending), decide intensive versus lower-intensity therapy.
- Marrow failure — anaemia, thrombocytopenia, neutropenia; transfuse and treat infection.
- Comorbidity — ischaemic heart disease (limits anthracycline), type 2 diabetes (worsened by steroids and infection).
- Psychosocial — shock of diagnosis; family communication; fertility (if relevant); work and finance.
- Long-term — fertility, late cardiac toxicity, secondary malignancy, survivorship. [1]
Integrated management plan
- Confirm diagnosis and risk — complete the molecular panel (FLT3-ITD and TKD, NPM1, CEBPA); HLA type the patient and any siblings in case HSCT is needed.
- Induction — 7+3 with daunorubicin 60 mg/m2 (lower than 90 given her cardiac history) and cytarabine, with midostaurin if FLT3 mutated. [1]3. Cardiology input — echocardiogram baseline, careful cumulative anthracycline dosing, consider liposomal anthracycline or alternative if ejection fraction low.
- Diabetes — sliding scale insulin during induction; expect steroid hyperglycaemia.
- Supportive care — irradiated blood products, neutropenic precautions, tumour lysis prophylaxis, antimicrobial prophylaxis per local protocol (aciclovir, fluconazole, PJP prophylaxis).
- Communication — break the news with the haematologist and nurse specialist; written summary; named contact; offer fertility referral if applicable; psychological support.
- Post-remission — consolidation by risk group; allogeneic HSCT only if intermediate with MRD positivity or adverse-risk. [1]
DCE short-case approach: examination of the haematology patient
Instruction: "Examine this patient's general systems." [1]
Systematic routine
- End of bed — pallor, bruising pattern, body habitus, whether on oxygen or attached to lines. Look for the cachexia and lethargy of marrow failure.
- Hands — pallor of palmar creases, bruising and petechiae, nail-bed infarcts, splinter haemorrhages. Pulse: tachycardia of anaemia or sepsis, irregularity of atrial fibrillation.
- Mouth — gum hypertrophy (monocytic AML), oral candidiasis, herpetec ulceration, mucositis from chemotherapy, petechiae on the hard palate, dental sepsis.
- Skin — leukaemia cutis (violaceous nodules), bruising, ecchymoses, line insertion sites, perianal sepsis.
- Lymph nodes — cervical, axillary, supraclavicular, epitrochlear, inguinal. Prominent in ALL.
- Abdomen — hepatosplenomegaly (more prominent in ALL than AML), masses, ascites.
- Chest — signs of pneumonia in the neutropenic patient, mediastinal signs (SVC obstruction in T-ALL).
- Nervous system — cranial nerves (especially facial nerve palsy — CNS leukaemia), fundoscopy (retinal haemorrhage of thrombocytopenia or leukaemic infiltration), meningism.
- Testes — in male patients with ALL, examine the testes (a sanctuary site). [1]
Presentation template
"I examined Mrs R, a 64-year-old woman who looks pale and tired. She has widespread petechiae on the lower limbs and hard palate and several large ecchymoses on the arms. The mouth shows gum hypertrophy with bleeding on the gingival margins. There is no lymphadenopathy. The abdomen reveals a spleen tip palpable, no hepatomegaly. The chest is clear. Fundoscopy shows a few flame haemorrhages. These findings are consistent with marrow failure and a coagulopathy — in a patient with circulating blasts, this picture with gum hypertrophy suggests acute myeloid leukaemia with a monocytic component, and I would specifically ask whether acute promyelocytic leukaemia has been excluded given the bleeding, because APL requires immediate ATRA." [1]
Key DWE MCQ patterns
- Suspected APL with bleeding — start ATRA immediately on suspicion, do not wait for cytogenetics.
- New AML with fever — neutropenic sepsis protocol; empiric antipseudomonal beta-lactam within one hour.
- Patient on ATRA develops fever and pulmonary infiltrates — differentiation syndrome; give dexamethasone immediately.
- AML with a FLT3-ITD mutation — add midostaurin to induction (RATIFY).
- Unfit older AML patient — venetoclax plus azacitidine (VIALE-A), not intensive 7+3.
- Young adult with Ph-positive ALL — add a tyrosine kinase inhibitor (dasatinib preferred); consider dasatinib plus blinatumomab in older adults.
- APL with low fibrinogen — correct with cryoprecipitate to fibrinogen over 1.5 g/L; platelet target over 30 to 50. [1]8. Adverse-risk AML (TP53, complex karyotype, monosomy 7) — allogeneic HSCT in first complete remission.
- Leucostasis with confusion in AML and WCC over 100 — urgent cytoreduction (hydroxyurea and/or leucapheresis), not antibiotics alone.
- AML with 18 per cent marrow blasts but t(8;21) — still AML; core binding factor leukaemia is AML-defining regardless of blast count. [1]
Common exam traps
- "Could this be APL?" must be asked of every new leukaemia. ATRA on suspicion.
- Differentiation syndrome vs sepsis — both can have fever and infiltrates; treat both, but steroids for differentiation syndrome must not be delayed.
- ELN 2022 — FLT3-ITD allelic ratio is gone; do not use it to stratify.
- NPM1 is favourable only if isolated — coexisting FLT3-ITD or adverse cytogenetics override it.
- Age alone does not decide fitness for induction — performance status and comorbidity do.
- Paediatric-inspired ALL regimens work in adults up to about 45, but toxicity (osteonecrosis, pancreatitis, thrombosis) is higher.
- 20 per cent blasts is the threshold for AML, except for AML-defining genetic abnormalities.
- Irradiated blood products for HSCT patients and after purine analogues.
- Allopurinol is not rasburicase — rasburicase breaks down existing urate; allopurinol prevents new formation. Use rasburicase for high-risk or established TLS. [1]
Communication and shared decision-making
"I would sit with the patient and their family in a quiet room with the haematologist and a nurse specialist. I would explain in plain language what leukaemia is — a cancer of the blood-forming cells of the marrow — and what the immediate plan is. I would acknowledge the shock explicitly and give them space. I would set out the options honestly — intensive therapy with curative intent, lower-intensity therapy with venetoclax, or supportive care — and explain that the choice depends on the leukaemia's biology, their overall health, and what matters most to them. I would document the shared decision, offer written information and a named contact, and arrange follow-up within days. I would address fertility, finances, work, and family — a leukaemia diagnosis affects every domain of life, and the registrar who acknowledges that is the one the patient trusts." [1]
References
[1] Dohner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 ELN recommendations. Blood 2022.
[2] Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the WHO classification of myeloid neoplasms and acute leukemia. Blood 2016.
[3] Lo-Coco F, Avvisati G, Vignetti M, et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med 2013.
[4] Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus chemotherapy for AML with a FLT3 mutation (RATIFY). N Engl J Med 2017.
[5] DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and venetoclax in previously untreated AML (VIALE-A). N Engl J Med 2020.
[6] Fernandez HF, Sun Z, Litzow MR, et al. Anthracycline dose intensification in AML (E1900). N Engl J Med 2009.
[7] Castaigne S, Pautas C, Maître C, et al. Gemtuzumab ozogamicin in de-novo AML (ALFA-0701). Lancet 2012.
[8] Sanz MA, Lo Coco F, Martín G, et al. Risk stratification in APL. Blood 2008.
[9] Sanz MA, Montesinos P. How we prevent and treat differentiation syndrome in APL. Blood 2014.
[10] Huguet F, Leguay T, Raffoux E, et al. Paediatric-inspired therapy in adults with Ph-negative ALL (GRAALL-2003). J Clin Oncol 2009.
[11] Martinelli G, et al. Dasatinib plus blinatumomab in Ph-positive ALL (D-ALBA). N Engl J Med 2020.
ELN 2022 AML Recommendations; WHO 2016 Myeloid Classification; NCCN AML Guidelines; HSANZ/eviQ AML and ALL Protocols. [1]
References
- [1]Dohner H, Wei AH, Appelbaum FR, et al. Diagnosis and management of AML in adults: 2022 recommendations from an international expert panel on behalf of the ELN Blood, 2022.PMID 35797463
- [2]Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia Blood, 2016.PMID 27069254
- [3]Lo-Coco F, Avvisati G, Vignetti M, et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia N Engl J Med, 2013.PMID 23841729
- [4]Stone RM, Mandrekar SJ, Sanford BL, et al. Midostaurin plus Chemotherapy for Acute Myeloid Leukemia with a FLT3 Mutation N Engl J Med, 2017.PMID 28644114
- [5]DiNardo CD, Jonas BA, Pullarkat V, et al. Azacitidine and Venetoclax in Previously Untreated Acute Myeloid Leukemia N Engl J Med, 2020.PMID 32786187
- [6]Fernandez HF, Sun Z, Litzow MR, et al. Anthracycline dose intensification in acute myeloid leukemia N Engl J Med, 2009.PMID 19776406
- [7]Castaigne S, Pautas C, Maître C, et al. Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study Lancet, 2012.PMID 22482940
- [8]Sanz MA, Lo Coco F, Martín G, et al. Definition of relapse risk and role of nonanthracycline drugs for consolidation in patients with acute promyelocytic leukemia: a joint study of the PETHEMA and GIMEMA cooperative groups Blood, 2000.PMID 10942364
- [9]Sanz MA, Montesinos P How we prevent and treat differentiation syndrome in patients with acute promyelocytic leukemia Blood, 2014.PMID 24627526
- [10]Huguet F, Leguay T, Raffoux E, et al. Pediatric-inspired therapy in adults with Philadelphia chromosome-negative acute lymphoblastic leukemia: the GRAALL-2003 study J Clin Oncol, 2009.PMID 19124805
- [11]Foà R, Bassan R, Vitale A, et al. Dasatinib-Blinatumomab for Ph-Positive Acute Lymphoblastic Leukemia in Adults N Engl J Med, 2020.PMID 33085860