Phys · haematological
Anaemia — Systematic Workup
Also known as anaemia investigation · low haemoglobin workup · microcytic anaemia · macrocytic anaemia · normocytic anaemia · iron deficiency anaemia · IDA · pernicious anaemia · vitamin B12 deficiency · folate deficiency · haemolytic anaemia · autoimmune haemolytic anaemia · AIHA · hereditary spherocytosis · G6PD deficiency · thalassaemia trait · anaemia of chronic disease · aplastic anaemia · reticulocyte count · iron studies · transfusion threshold · direct antiglobulin test · DAT · Coombs test
Consultant-physician-depth guide to the systematic investigation of anaemia. Covers MCV-based classification (microcytic, normocytic, macrocytic), the reticulocyte count as kinetic discriminator, iron-studies interpretation, the iron deficiency workup in adults (mandatory GI source search), haemolytic anaemia classification, blood-film morphology, transfusion thresholds, and the management of each major cause. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Anaemia — Systematic Workup
The answer first
Anaemia is investigated by a reproducible, two-axis system: the morphological axis (the mean cell volume — microcytic, normocytic, macrocytic) and the kinetic axis (the reticulocyte count — is the marrow responding or not). The registrar who applies these two axes to every low haemoglobin will reach the cause; the one who chases a scatter of tests will miss the GI cancer hiding behind a "simple" iron deficiency. [1]
The mandate in three steps: [1]
- Confirm anaemia and classify by MCV. Take a full blood count and look at the MCV. Is the cell small, normal or large? This is the first branch point.
- Apply the reticulocyte count as the kinetic discriminator. Is the marrow trying to replace the lost cells (reticulocytes high — think haemolysis or bleeding or recovery) or failing to produce them (reticulocytes low — think iron/B12/folate deficiency, marrow failure, chronic disease)?
- Target the cause with the right panel. Iron studies for the microcytic anaemias; B12 and folate for macrocytosis; DAT, LDH and haptoglobin for haemolysis; a blood film for morphology; and a bone marrow biopsy when the marrow itself is suspect. [1]
The single most important principle for the exam: never treat anaemia as the diagnosis. Anaemia is a sign. Iron deficiency anaemia in a man or a postmenopausal woman is GI malignancy until proven otherwise — the iron studies confirm the deficiency, but the endoscopy and colonoscopy find the cause [1].
Overview and definition
Anaemia is a reduction in the haemoglobin concentration below the reference range for age and sex. The World Health Organization thresholds for adults are: men less than 130 g/L, non-pregnant women less than 120 g/L, and pregnant women less than 110 g/L. These cut-offs are physiological — they reflect the point at which oxygen-carrying capacity falls low enough to produce symptoms in a person without cardiorespiratory reserve. A young, fit woman with a haemoglobin of 110 g/L is not "anaemic for her" — she is anaemic by any standard, and she needs a workup. [1]
The clinical problem is not the number but what it means. A haemoglobin of 85 g/L in a chronically iron-deficient 40-year-old woman with menorrhagia is a common, low-acuity problem. The same number in a 68-year-old man with weight loss is colon cancer until excluded. The workup is the same set of tests; the clinical context dictates the urgency and the next step. [1]
Anaemia: defining thresholds
Classification — the MCV is the first branch point
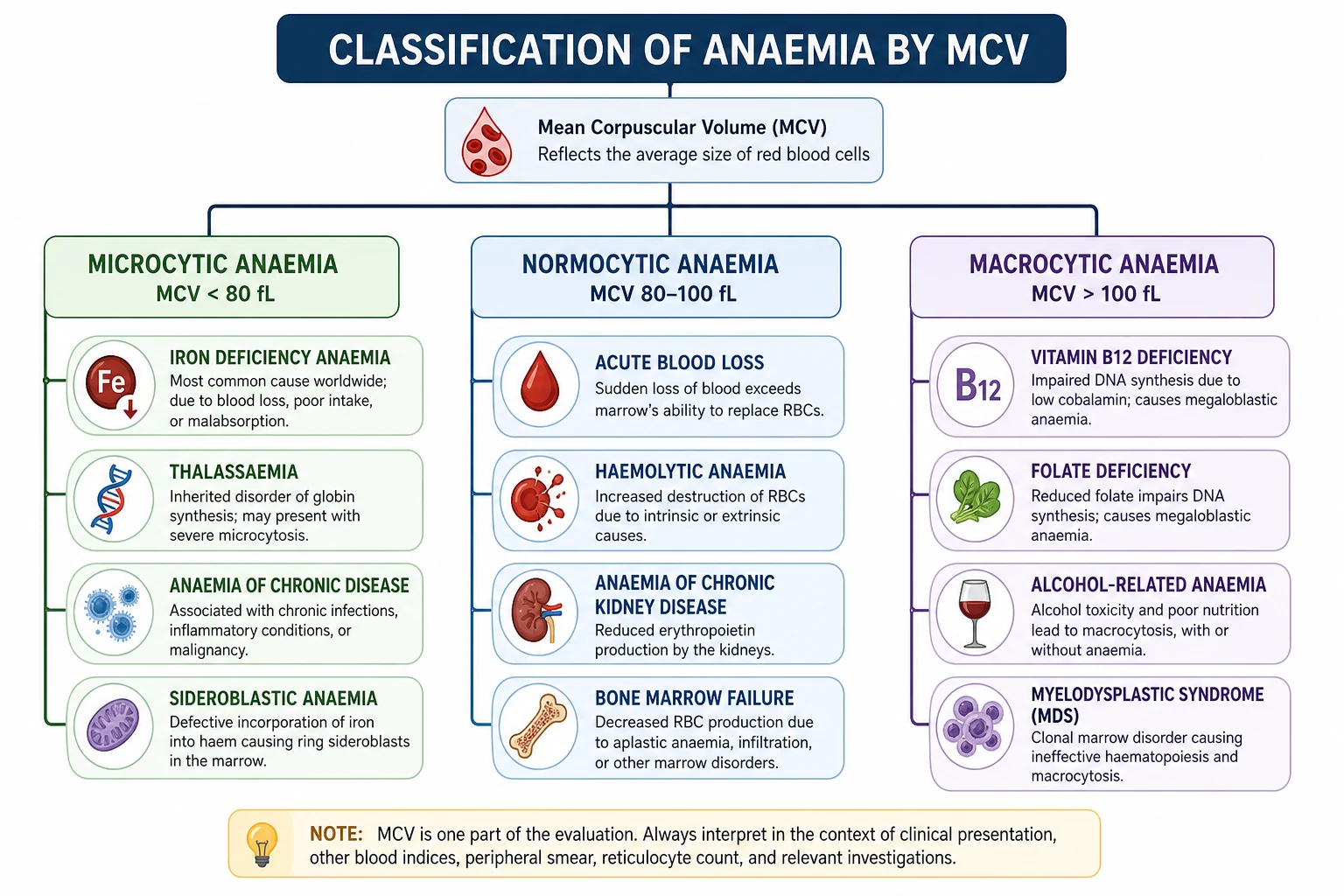
Every anaemia falls into one of three morphological buckets by MCV. The bucket you land in determines the next test and the differential — so state the MCV aloud in the viva before you say anything else. [1]
Microcytic (MCV < 80 fL)
The microcytic anaemias share one mechanism: a failure of haemoglobin synthesis, either because iron is unavailable (iron deficiency, anaemia of chronic disease), because globin is mis-made (thalassaemia), or because the iron cannot be incorporated into the haem ring (sideroblastic, lead poisoning). The cell divides extra times to reach its haemoglobin concentration quota, so each red cell ends up small. [1]
| Type | Key features |
|---|---|
| Iron deficiency | Ferritin low, transferrin high, TSAT low; RBC count low, RDW high; most common cause overall; always search for the source |
| Thalassaemia trait | Iron studies normal; RBC count normal or high, RDW normal; Mentzer index (MCV/RBC) less than 13; raised HbA2 in beta-thalassaemia |
| Anaemia of chronic disease | Ferritin normal or high, transferrin low; functional iron deficiency via hepcidin; underlying inflammation, infection, malignancy; CRP raised |
| Sideroblastic / lead | Ring sideroblasts in marrow; basophilic stippling on film; lead: abdominal pain, neuropathy, encephalopathy; iron available but unusable |
Normocytic (MCV 80 to 100 fL)
The normocytic anaemias are the most heterogeneous group — and the group where the reticulocyte count is the discriminator. A high reticulocyte count means the marrow is healthy and losing cells (haemolysis, acute blood loss, recovery after treatment). A low reticulocyte count means the marrow is underproducing (chronic disease, CKD, marrow failure, early mixed deficiency). The two groups look identical on the FBC; the reticulocyte count is what separates them. [1]
- High reticulocyte count (marrow responding): acute blood loss, haemolytic anaemia, recovery after haematinic replacement.
- Low reticulocyte count (marrow failing): anaemia of chronic disease, chronic kidney disease (EPO deficiency), bone marrow failure (aplastic anaemia), early combined iron and B12 deficiency (the two deficits cancel out, producing a normal MCV). [1]
Macrocytic (MCV > 100 fL)
The macrocytic anaemias are split into megaloblastic (B12 and folate deficiency, where DNA synthesis is impaired and the red cell precursor grows large because it cannot divide) and non-megaloblastic (alcohol, liver disease, hypothyroidism, MDS, drug-induced, reticulocytosis). The discriminator is the blood film: megaloblastic anaemia shows hypersegmented neutrophils (six or more lobes), oval macrocytes, and a low reticulocyte count, while a reticulocytosis produces large polychromatic cells that are young red cells, not abnormal ones. [1]
See comparison details in the text above and the figure for this section. [1]
Pathophysiology — why the red cell fails
Iron is absorbed in the duodenum via the divalent metal transporter 1 (DMT1), carried in the blood by transferrin, stored in cells as ferritin, and its absorption and release are controlled by hepcidin — the liver hormone that is the master regulator of iron homeostasis. Hepcidin binds to ferroportin on enterocytes and macrophages, causing its internalisation and degradation; the result is that iron is trapped inside the cells and cannot enter the blood. In inflammation, hepcidin rises — trapping iron in macrophages and producing the anaemia of chronic disease, a functional iron deficiency in which the body has iron (ferritin is normal or high) but cannot mobilise it. [1]
B12 (cobalamin) is a cofactor for two enzymes: methylmalonyl-CoA mutase (in the conversion of methylmalonyl-CoA to succinyl-CoA) and methionine synthase (which remethylates homocysteine to methionine). When B12 is deficient, methionine synthase fails and folate is trapped as methyltetrahydrofolate — the "methylfolate trap" — so that thymidylate and purine synthesis stall and DNA replication is impaired. The red cell precursor grows large but cannot divide, producing a megaloblast. The same biochemical defect affects oligodendrocytes in the central nervous system — producing subacute combined degeneration of the spinal cord, the neurological complication of B12 deficiency that folate deficiency does not produce [2].
Haemolysis shortens the red cell lifespan below the 120-day normal. The marrow can compensate for a red cell lifespan down to about 20 days by increasing output sixfold; once the rate of destruction exceeds this, anaemia develops. The reticulocyte count rises as the marrow pushes out young cells. Whether haemolysis is intravascular (complement-mediated lysis in the circulation — dark urine, low haptoglobin, schistocytes in microangiopathy) or extravascular (macrophage removal in the spleen — jaundice, splenomegaly, spherocytes) determines the clinical picture and the investigations [6].
Clinical presentation
The symptoms of anaemia are non-specific because they reflect tissue hypoxia: fatigue, exertional dyspnoea, palpitations, light-headedness, and (with severe or rapid-onset anaemia) chest pain and syncope. The tempo matters: a haemoglobin of 70 g/L that has fallen over months is tolerated; the same value reached in two days from acute haemorrhage is a cardiovascular emergency. [1]
The features beyond fatigue point to the cause: [1]
- Iron deficiency: koilonychia (spoon-shaped nails), angular cheilitis, atrophic glossitis (a smooth, sore, red tongue), pica (craving for ice or starch), restless legs syndrome, and the Plummer-Vinson syndrome (post-cricoid oesophageal web plus iron deficiency plus dysphagia).
- B12 deficiency: the neurological features are the discriminator — peripheral neuropathy (typically symmetric, in the legs), subacute combined degeneration of the cord (loss of vibration and proprioception with extensor plantars from dorsal and lateral column damage), cognitive and mood change, and optic atrophy. Glossitis and mild jaundice from ineffective erythropoiesis may coexist.
- Haemolysis: jaundice (unconjugated hyperbilirubinaemia), dark urine (from haemoglobinuria or urobilinogen), splenomegaly, and pigment gallstones (a history of cholecystectomy at a young age is a clue).
- Marrow failure: the anaemia is accompanied by bruising, mucosal bleeding and recurrent infection from pancytopenia — the triad points to aplastic anaemia, acute leukaemia, or myelodysplasia. [1]
DCE examiner trap: Anaemia in the elderly often presents as confusion, falls, or new heart failure rather than with a classic fatigue complaint. The unwritten rule is: any older patient with new cognitive change, unexplained heart failure, or recurrent falls needs a full blood count. Anaemia is common in this group and its cause is often treatable. [1]
Differential diagnosis — discriminating features
The differential is built from the MCV and reticulocyte count, but within each bucket a small set of features separates the causes. The table below is the viva answer to "how do you distinguish the causes of microcytosis?" [1]
| Feature | Iron deficiency | Thalassaemia trait | Anaemia of chronic disease |
|---|---|---|---|
| RBC count | Low | Normal or high | Low or normal |
| RDW | High | Normal or mildly raised | Normal or mildly raised |
| Mentzer index (MCV/RBC) | Greater than 13 | Less than 13 | Variable |
| Ferritin | Low | Normal or high | Normal or high |
| Transferrin | High | Normal | Low |
| Transferrin saturation | Low | Normal | Low or normal |
| HbA2 | Normal or low | Raised in beta-thalassaemia | Normal |
The Mentzer index (MCV divided by red cell count in millions per microlitre) is a cheap bedside discriminator: a value less than 13 favours thalassaemia trait, and a value greater than 13 favours iron deficiency. It is not definitive — iron studies and Hb electrophoresis are — but it is a high-yield MCQ discriminator and a useful viva shorthand. [1]
For macrocytosis the discriminator is the film and the drug history. Hypersegmented neutrophils and oval macrocytes mean B12 or folate deficiency; round macrocytes with no hypersegmentation mean alcohol, liver disease or hypothyroidism; a high reticulocyte count means a young-cell macrocytosis from haemolysis or recovery. [1]
Clinical and bedside assessment
Begin with a focused history and a focused examination — both should take five minutes and both should be done before the bloods come back. [1]
History. Ask about the GI tract (change in bowel habit, blood in the stool or vomit, abdominal pain, dysphagia, weight loss), menstrual loss in women (number of days, flooding, clots, intermenstrual bleeding), dietary intake (vegan, restrictive), drug history (NSAIDs, aspirin, anticoagulants, PPIs, metformin, methotrexate, chemotherapy, hydroxycarbamide), surgical history (gastrectomy, bariatric surgery, bowel resection), and family history (thalassaemia, spherocytosis, G6PD deficiency, pernicious anaemia). Ethnic origin matters: beta-thalassaemia is common in Mediterranean, Middle Eastern and South Asian populations; alpha-thalassaemia in South-East Asian and African populations; sickle cell and G6PD deficiency in African, Middle Eastern and Mediterranean populations. [1]
Examination. Look for conjunctival and palmar crease pallor (a quick bedside screen, though sensitivity is low), koilonychia, angular cheilosis and glossitis (iron deficiency), the neurological signs of B12 deficiency (impaired vibration and proprioception in the legs, extensor plantars), jaundice and splenomegaly (haemolysis, hereditary spherocytosis, thalassaemia, lymphoproliferative disease), lymphadenopathy (lymphoma), signs of chronic liver disease (which produces macrocytosis and hypersplenism), and always perform a digital rectal examination with faecal occult blood testing. Pelvic examination is indicated in women with heavy menstrual bleeding. [1]
Investigations — the systematic panel
The first-line panel for any unexplained anaemia is the same, regardless of MCV: [1]
First-line anaemia panel
Full blood count and indices
Hb, MCV, MCH, RDW, RBC count; establish the morphological bucket
Reticulocyte count
The kinetic discriminator — high or low
Blood film
Cell morphology — target cells, spherocytes, schistocytes, sickle cells, hypersegmented neutrophils, blasts
Iron studies
Ferritin, transferrin (or TIBC), transferrin saturation
B12 and folate
Especially if macrocytic; consider methylmalonic acid and homocysteine if borderline
Haemolysis screen
LDH, haptoglobin, bilirubin, DAT (Coombs) — when reticulocytes are high or MCV is normal
Context bloods
CRP, U&E, LFTs, TSH — for chronic disease, CKD, liver disease, hypothyroidism
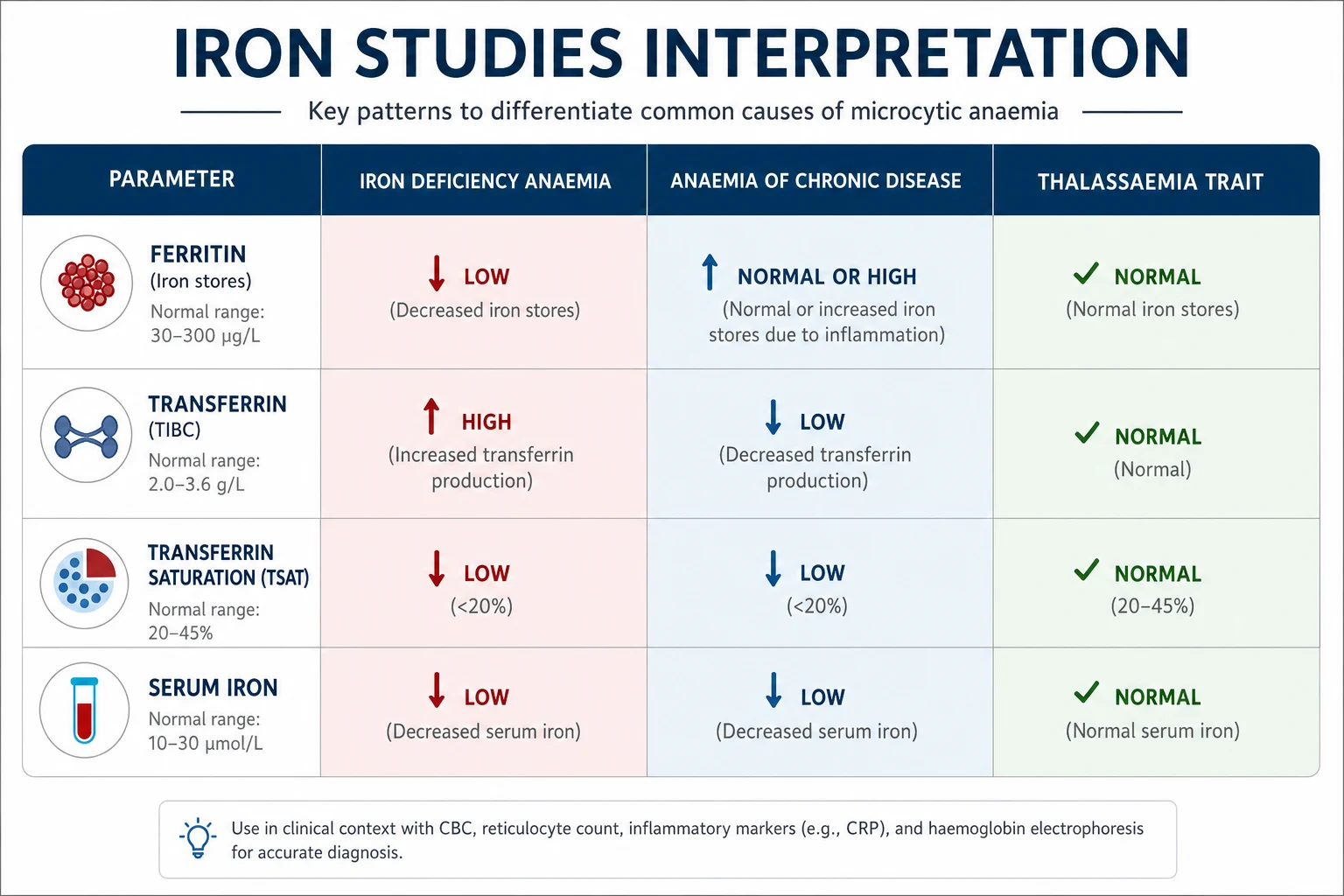
Iron studies interpretation
Iron studies are the core investigation for the microcytic anaemias, and their interpretation is the most tested single skill in this topic. The four patterns to know: [1]
See comparison details in the text above and the figure for this section. [1]
Critical pitfall. Ferritin is an acute phase reactant. In a patient with active inflammation, infection, malignancy or liver disease, a ferritin of 60 g/L does not exclude iron deficiency — in that context the cut-off for deficiency rises to around 100 g/L. A normal or high ferritin in a chronically ill patient with a microcytic anaemia does not close the question; the soluble transferrin receptor (which rises in true iron deficiency but not in anaemia of chronic disease) or a trial of iron may be needed. [1]
The reticulocyte count — the kinetic discriminator
The reticulocyte count tells you whether the marrow is responding. A reticulocyte percentage greater than 2 per cent (or an absolute reticulocyte count greater than 100 x 10^9 per litre) in the face of anaemia means the marrow is trying hard — and the problem is loss or destruction, not production. A low reticulocyte count means the marrow is the bottleneck (iron/B12/folate deficiency, chronic disease, marrow failure, CKD). [1]
The corrected reticulocyte count (reticulocyte percentage multiplied by haematocrit divided by normal haematocrit) corrects for the degree of anaemia and gives a fairer measure of marrow output. The reticulocyte production index (RPI) further corrects for the longer maturation time of reticulocytes released under stress — an RPI greater than 2 indicates an adequate marrow response and points to haemolysis or blood loss. [1]
Blood film morphology — what each cell tells you
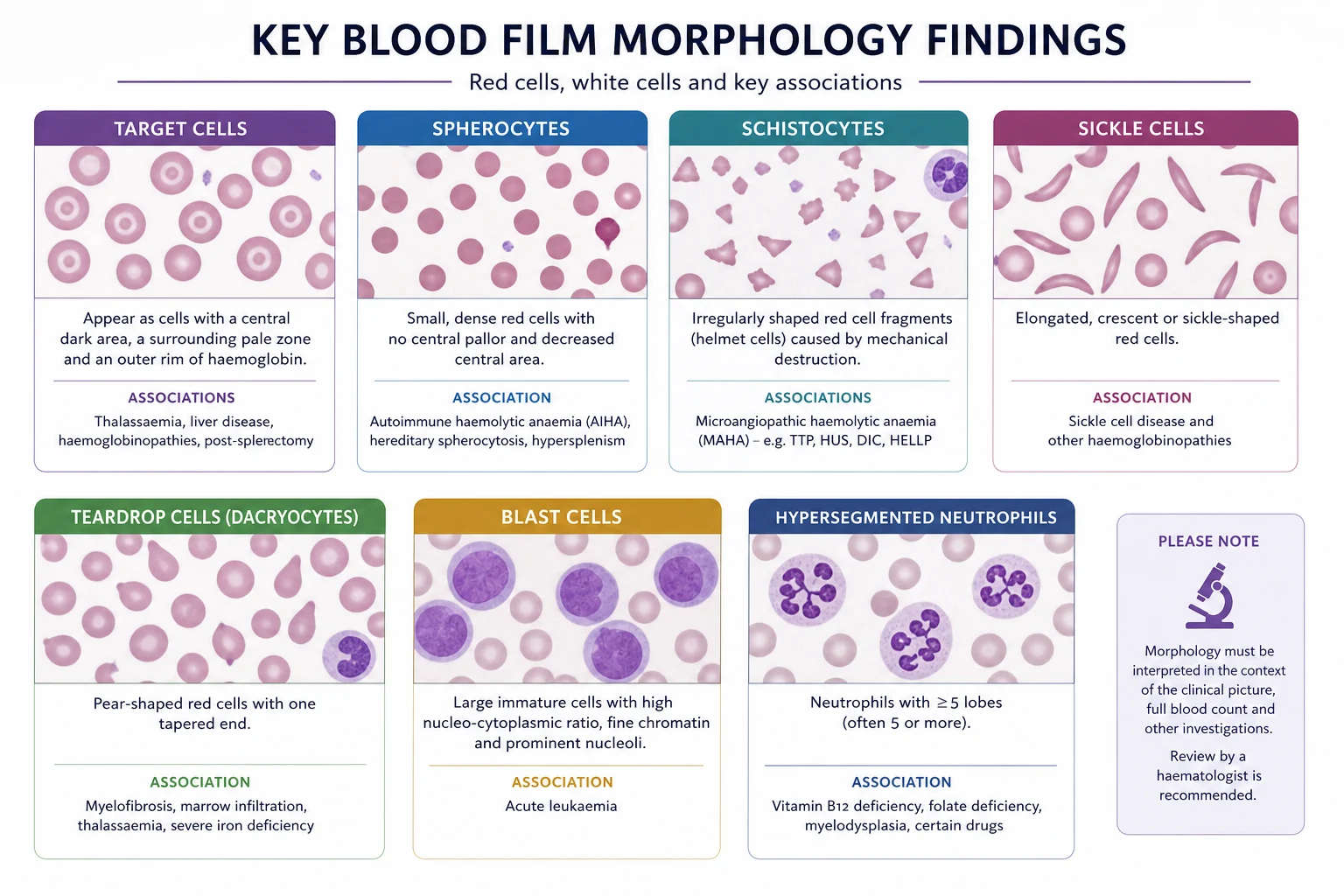
The blood film is the single most informative test in haematology — it converts a number into a shape. The high-yield morphologies: [1]
| Morphology | Diagnosis it points to |
|---|---|
| Target cells | Thalassaemia, liver disease, post-splenectomy, HbC |
| Spherocytes | Hereditary spherocytosis, autoimmune haemolysis (warm) |
| Schistocytes (fragments) | Microangiopathic haemolysis — DIC, TTP/HUS, HELLP, mechanical valve |
| Sickle cells | Sickle cell disease |
| Teardrop cells (dacrocytes) | Myelofibrosis, severe megaloblastic anaemia, marrow infiltration |
| Basophilic stippling | Lead poisoning, sideroblastic anaemia, thalassaemia |
| Hypersegmented neutrophils (6+ lobes) | B12 or folate deficiency (megaloblastic) |
| Howell-Jolly bodies | Post-splenectomy, hyposplenism, severe megaloblastic anaemia |
| Blast cells | Acute leukaemia, myelodysplasia, severe infection |
| Heinz bodies (supravital stain) | G6PD deficiency, oxidant haemolysis |
Haemolysis screen
When the reticulocyte count is high and the DAT is requested, the haemolysis panel is: raised LDH, low haptoglobin, raised unconjugated bilirubin, raised reticulocyte count, and a positive or negative DAT. A low haptoglobin (less than 0.3 g/L) is the most sensitive single marker of intravascular haemolysis; a raised LDH reflects red cell destruction and is also raised in megaloblastic anaemia (ineffective erythropoiesis) and in malignancy. [1]
The direct antiglobulin test (DAT, or Coombs test) detects antibody or complement bound to the surface of the patient's red cells. A positive DAT with IgG is warm autoimmune haemolytic anaemia; a positive DAT with C3d (complement) alone is cold agglutinin disease; a negative DAT points to a non-immune cause — hereditary spherocytosis, G6PD deficiency, microangiopathy, or a haemoglobinopathy [6].
Bone marrow biopsy — when and why
Bone marrow biopsy is not a first-line test, but it is indicated for: unexplained pancytopenia; a persistently unexplained macrocytosis or leucoerythroblastic film; suspected acute leukaemia, myelodysplasia, myelofibrosis, or aplastic anaemia; staging of lymphoma or solid tumours; and an anaemia that fails to respond to appropriate therapy. The trephine biopsy (not just the aspirate) is essential for assessing cellularity — the key discriminator between aplastic anaemia (markedly hypocellular) and myelodysplasia (hypercellular with dysplasia). [1]
Management — resuscitation and transfusion
The immediate question in any anaemic patient is not "what is the cause" but "is this patient sick now?" Resuscitation precedes diagnosis. Assess for haemodynamic instability, ongoing bleeding, ischaemia (chest pain, ECG changes), and high-acuity features (shock, altered mental status). If any are present, transfuse and resuscitate first, then investigate. [1]
Transfusion thresholds — the restrictive strategy
Modern transfusion practice is restrictive: transfuse only when the haemoglobin is at or below a threshold that is lower than most clinicians once assumed. The evidence underpinning this is the TRICC trial (Hebert, NEJM 1999), which showed that a restrictive strategy (transfuse when Hb less than 70 g/L, target 70 to 90 g/L) was at least as safe as a liberal strategy (transfuse when Hb less than 100 g/L, target 100 to 120 g/L) in critically ill adults, and was better for the less-acutely-ill and the younger patients [3]. The FOCUS trial extended this to older patients with cardiovascular disease undergoing hip-fracture surgery: a liberal threshold (100 g/L) did not improve outcomes over a restrictive threshold (80 g/L or symptoms) [4]. The AABB guideline (Carson, 2012) consolidated the evidence into a recommendation: a restrictive threshold of 70 to 80 g/L for hospitalised, stable patients, with a higher threshold of around 80 g/L for those with cardiovascular disease [5].
Restrictive transfusion thresholds (AABB 2012)
The exceptions to the restrictive strategy are the patient who is actively bleeding, the patient with acute coronary syndrome (where the threshold may be higher — the TRICC and FOCUS evidence does not apply directly), and the patient with severe symptomatic anaemia. In heart failure with severe anaemia, transfuse a single unit at a time, slowly, with diuretic cover to avoid precipitating pulmonary oedema. [1]
Management — definitive, by cause
Iron deficiency
The treatment of iron deficiency anaemia is iron replacement plus a search for and treatment of the cause. Oral ferrous sulfate 200 mg three times daily (or every other day, which improves absorption and tolerance by avoiding hepcidin upregulation) for three to six months — long enough to replete stores, not just to correct the haemoglobin. A reticulocyte response should be evident within 7 to 10 days, and the haemoglobin should rise by about 20 g/L over three weeks. Alternative oral salts (ferrous fumarate, ferrous gluconate) are equally effective if sulfate is not tolerated; avoid slow-release formulations, which are poorly absorbed. [1]
Intravenous iron is indicated when oral iron is not tolerated, not absorbed (inflammatory bowel disease, post-bariatric surgery, coeliac disease), or insufficient (ongoing blood loss, chronic kidney disease, perioperative optimisation, heart failure with iron deficiency). Ferric carboxymaltose and ferric derisomaltose allow large single-dose infusions over 15 to 20 minutes; iron polymaltose and iron sucrose are alternatives. The modern preparations have a low anaphylaxis rate and a test dose is no longer routinely required for ferric carboxymaltose. [1]
Iron deficiency workup in adults — the mandatory GI search
B12 deficiency
Replace with intramuscular hydroxocobalamin. The standard regimen for neurological involvement or pernicious anaemia is 1 mg IM on alternate days for two weeks (or until symptoms stop improving), then 1 mg IM every two to three months for life. For dietary B12 deficiency without malabsorption, a maintenance oral dose of 50 to 150 micrograms daily between meals may suffice, but the IM route is preferred when compliance or absorption is uncertain. The first-dose response is a reticulocytosis within 5 to 7 days and a fall in the (initially low) potassium as new cells take up potassium — monitor potassium in severe deficiency. Hypokalaemia is a recognised early complication of B12 (or folate) replacement [2].
Folate deficiency
Replace with oral folic acid 5 mg daily for four months (long enough to correct the deficiency and rebuild stores). Exclude B12 deficiency first, because folate replacement alone in a B12-deficient patient can precipitate or accelerate subacute combined degeneration of the spinal cord — the folate corrects the blood picture but not the neurological defect, while the B12 deficiency continues to damage the cord. In pregnancy, prophylactic folic acid 400 micrograms daily before conception and for the first trimester prevents neural tube defects; a higher dose of 5 mg daily is used in women at high risk (epilepsy on enzyme-inducers, prior affected pregnancy, diabetes, BMI above 30). [1]
Autoimmune haemolytic anaemia (AIHA)
The first-line treatment of warm AIHA is prednisolone 1 to 1.5 mg/kg/day, tapered over months as the haemoglobin recovers and the DAT normalises. About 80 per cent respond initially, but relapse is common; rituximab is the preferred second-line agent and is now used earlier in severe or refractory disease [6]. Splenectomy is reserved for refractory cases. Cold agglutinin disease does not respond to corticosteroids — it is managed with cold avoidance, rituximab (with or without bendamustine), and complement inhibitors (sutimlimab). Transfusion in AIHA is difficult: the autoantibody may make crossmatching unreliable, and transfused cells may be destroyed as fast as the patient's own — transfuse only if symptomatic or haemodynamically unstable, and use the least incompatible unit.
Hereditary spherocytosis
Folate supplementation supports the chronically haemolysing marrow. Splenectomy is curative for the haemolysis and is indicated for symptomatic moderate or severe disease, but it must be preceded by vaccination (pneumococcal, meningococcal, Haemophilus influenzae type b) and followed by lifelong penicillin V prophylaxis (250 to 500 mg twice daily), because the asplenic patient is at high risk of overwhelming post-splenectomy infection. In children, splenectomy is delayed until after age 6 if possible to reduce the infection risk [8].
Aplastic anaemia
Aplastic anaemia is immune-mediated marrow failure producing pancytopenia and a hypocellular marrow. Allogeneic haematopoietic stem cell transplantation is the curative treatment for younger patients (under 40 to 50 years) with a matched sibling donor. For older patients or those without a donor, immunosuppressive therapy with horse antithymocyte globulin (ATG) plus ciclosporin, often combined with eltrombopag, is first-line; about 60 to 70 per cent respond. Supportive care with transfusions and anti-infective cover is essential while awaiting response. [1]
Specific subtypes — the high-yield diagnoses
G6PD deficiency
Glucose-6-phosphate dehydrogenase deficiency is the most common human enzymopathy, X-linked and affecting hundreds of millions worldwide. The enzyme generates NADPH through the pentose phosphate pathway; without it, red cells cannot maintain reduced glutathione and are destroyed by oxidative stress. The classic triggers are fava beans (broad beans), infections, and oxidant drugs — primaquine, dapsone, rasburicase, sulphonamides, nitrofurantoin, and certain analgesics. The haemolysis is episodic and acute, with jaundice, dark urine (haemoglobinuria) and a falling haemoglobin; the film shows bite cells and Heinz bodies (denatured haemoglobin on a supravital stain). Methylene blue, the usual treatment for methaemoglobinaemia, is contraindicated — it is an oxidant and will worsen the haemolysis [7]. The acute episode is managed with withdrawal of the trigger, supportive care, and transfusion if severe. The enzyme assay is unreliable during an acute episode because the most deficient (oldest) cells have been destroyed — test several weeks after recovery.
Anaemia of chronic disease
The anaemia of chronic disease (also called anaemia of inflammation) is the second most common anaemia after iron deficiency. It is driven by inflammatory cytokines (IL-6 in particular) that raise hepcidin, trapping iron in macrophages and enterocytes and producing a functional iron deficiency. The iron studies show a normal or high ferritin, a low transferrin, and a low transferrin saturation — the mirror image of iron deficiency. The treatment is of the underlying condition; intravenous iron may help in selected cases (such as inflammatory bowel disease or heart failure), and erythropoiesis-stimulating agents are used in CKD-associated anaemia. [1]
Sickle cell disease and thalassaemia
Sickle cell disease and the thalassaemias are covered in their own dedicated topics; in the workup of anaemia they appear as causes of chronic haemolytic anaemia with characteristic films — sickle cells, target cells, and (in sickle disease) Howell-Jolly bodies from autosplenectomy. Thalassaemia trait is asymptomatic microcytosis — the trap is treating it with iron and producing iron overload. [1]
Complications and pitfalls
The classic errors in the anaemia workup, each of which can fail a viva or harm a patient: [1]
- Treating ferritin in isolation. A normal or high ferritin does not exclude iron deficiency in inflammation — use the soluble transferrin receptor, the TSAT, or a therapeutic trial if in doubt.
- Folate without B12. Giving folate to a B12-deficient patient corrects the blood but allows the subacute combined degeneration to progress — always check B12 first or treat both together.
- Methylene blue in G6PD deficiency. The standard methaemoglobinaemia treatment is an oxidant; in G6PD deficiency it worsens the haemolysis. Use ascorbic acid instead.
- Transfusing autoimmune haemolysis liberally. The autoantibody cross-reacts with donor cells; transfuse only when necessary and accept the "least incompatible" unit.
- Missing a mixed deficiency. Iron deficiency plus B12 deficiency can produce a normal MCV — the two size effects cancel out. A macrocytosis that normalises after iron replacement is a clue that B12 deficiency was masked.
- Closing the iron deficiency workup at the iron study. The iron study confirms the deficiency; the endoscopy and colonoscopy find the cancer. Do not stop at the iron study in a man or a postmenopausal woman. [1]
Prognosis and disposition
The prognosis of anaemia is the prognosis of its cause. Iron deficiency from a benign, treatable source (menorrhagia, peptic ulcer, coeliac disease) has an excellent prognosis once the cause is addressed. Iron deficiency from a colorectal cancer carries the prognosis of the cancer. Pernicious anaemia treated early is fully compatible with normal life; the neurological deficit may not fully reverse if treatment is delayed. Aplastic anaemia has a high untreated mortality but a good outlook with transplant in young patients or immunosuppression in older patients. Hereditary spherocytosis is cured by splenectomy, with the proviso of lifelong infection risk. [1]
Disposition: most anaemia workup is outpatient. Admit for symptomatic severe anaemia (heart failure, ischaemia, haemodynamic instability), for acute haemolysis, for pancytopenia with bleeding or infection, and for any anaemia where the diagnostic pathway (bone marrow biopsy, transfusion) needs inpatient monitoring. [1]
Special populations
Pregnancy. The threshold for anaemia falls (less than 110 g/L) and iron demand rises. Oral iron is first-line; IV iron is used when oral iron is not tolerated or not absorbed, particularly in the third trimester when the time to delivery is short. Erythropoietin is avoided in pregnancy unless there is a specific indication (renal disease). [1]
Chronic kidney disease. Anaemia in CKD is from EPO deficiency and is managed with intravenous iron and erythropoiesis-stimulating agents (ESAs), targeting a TSAT above 20 per cent and ferritin above 100 to 200 micrograms per litre, and a haemoglobin of 100 to 115 g/L — higher targets are associated with cardiovascular harm. [1]
Heart failure. Iron deficiency is common in heart failure (present in up to 50 per cent) and worsens symptoms regardless of whether anaemia is present. Intravenous ferric carboxymaltose improves symptoms and exercise capacity in heart failure with iron deficiency, with or without anaemia — a finding that has brought iron repletion into the heart failure management pathway. [1]
The elderly. Anaemia is not a normal consequence of ageing. Any older patient with a new anaemia needs a full workup — the yield of treatable and serious causes (iron deficiency, B12 deficiency, CKD, myelodysplasia, GI malignancy) is high. [1]
Evidence, guidelines and regional differences
The British Society of Gastroenterology guideline (Goddard, Gut 2011) is the standard reference for the iron deficiency workup in adults and is the source of the "always investigate a GI source in men and postmenopausal women" rule [1]. The British Society for Haematology publishes the standard UK guidance on the investigation and management of macrocytosis, hereditary spherocytosis, and autoimmune haemolysis. In ANZ, the National Blood Authority Patient Blood Management Guidelines (2011, updated) endorse the restrictive transfusion strategy and emphasise patient blood management as a system — treat the cause of anaemia before surgery rather than transfusing perioperatively. In the United States, the AABB guideline (Carson, 2012) is the standard reference for transfusion thresholds [5].
The evidence base for the restrictive transfusion strategy is one of the strongest in all of medicine: TRICC (1999) in the ICU, FOCUS (2011) in hip-fracture surgery, and the TRISS trial in septic shock all converge on the same conclusion — less transfusion is at least as good as more, and sometimes better [3] [4]. The trials have changed practice globally.
For B12 deficiency, the move towards oral high-dose cobalamin in selected patients (dietary deficiency, no malabsorption) is a regional variation — the IM route remains the ANZ and UK standard for pernicious anaemia and any deficiency with neurological features [2].
Exam pearls
- State the MCV first. Every viva answer to "investigate this anaemia" opens with the MCV. Microcytic, normocytic or macrocytic — then refine.
- The reticulocyte count is the kinetic discriminator. High means the marrow is working and cells are being lost or destroyed; low means the marrow is the problem.
- Ferritin is an acute phase reactant. A normal ferritin does not exclude iron deficiency in a sick patient. The cut-off rises to around 100 g/L in inflammation. [1]4. The B12 versus folate discriminator is neurological. Subacute combined degeneration is B12, never folate.
- Men and postmenopausal women with iron deficiency get a GI workup. Coeliac serology, OGD, and colonoscopy — no exceptions unless an obvious non-GI cause is found and excluded.
- The DAT separates immune from non-immune haemolysis. Warm AIHA (IgG) responds to steroids; cold agglutinin disease (C3d) does not — use rituximab.
- Transfuse restrictively. 70 g/L in the stable patient, 80 g/L in cardiac disease, individualise in acute coronary syndrome. [1]8. Never give folate alone to a B12-deficient patient. Check B12 first or treat both together.
- Methylene blue is contraindicated in G6PD deficiency. Use ascorbic acid for methaemoglobinaemia instead.
- A normal MCV does not exclude a deficiency. Iron deficiency and B12 deficiency can cancel each other out; the film and the indices may both look normal. Check both if the clinical picture suggests deficiency. [1]
References
[1] Goddard AF, James MW, McIntyre AS, Scott BB. Guidelines for the management of iron deficiency anaemia. Gut 2011;60(10):1309–1316. The British Society of Gastroenterology consensus — the source of the rule that every adult man and postmenopausal woman with iron deficiency anaemia is investigated for a GI source.
[2] Stabler SP. Clinical practice. Vitamin B12 deficiency. N Engl J Med 2013;368(2):149–160. The definitive modern clinical-practice review of B12 deficiency — causes (pernicious anaemia, terminal ileum disease, metformin, vegans), the megaloblastic picture, subacute combined degeneration, and hydroxocobalamin replacement.
[3] Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. N Engl J Med 1999;340:409–417. The TRICC trial — the landmark study that established the restrictive transfusion strategy (threshold Hb less than 70 g/L) as at least as safe as the liberal strategy in critically ill adults.
[4] Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011;365:2453–2462. The FOCUS trial — extended the restrictive strategy to older patients with cardiovascular disease undergoing hip-fracture surgery; no benefit from a liberal (100 g/L) over a restrictive (80 g/L or symptomatic) threshold.
[5] Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB. Ann Intern Med 2012;157:49–58. The consolidated AABB recommendation — restrictive threshold of 70 to 80 g/L in stable inpatients, 80 g/L in cardiovascular disease, with clinical judgement for acute coronary syndrome.
[6] Jager U, Barcellini W, Broome CM, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: recommendations from the First International Consensus Meeting. Blood Rev 2020;34:100648. The international consensus on AIHA — monospecific DAT mandatory, corticosteroids first-line for warm AIHA, rituximab for cold agglutinin disease and refractory warm disease.
[7] Luzzatto L, Nannelli C, Notaro R. Glucose-6-phosphate dehydrogenase deficiency. Blood 2020;136(11):1225–1240. The modern review of G6PD deficiency — genetics, pathophysiology (NADPH and glutathione), oxidative triggers, the Heinz body film, and the absolute contraindication to methylene blue.
[8] Manciu S, Maranduca MA, Tanase DM, et al. Hereditary spherocytosis — diagnosis, surgical treatment and outcomes. A literature review. Chirurgia (Bucur) 2017;112(2):110–116. The surgical review of hereditary spherocytosis — membrane protein defects, EMA binding test, splenectomy, and the importance of vaccination and penicillin prophylaxis.
Goddard BSG guideline 2011; Stabler NEJM 2013; Hebert TRICC NEJM 1999; Carson FOCUS NEJM 2011; Carson AABB Ann Intern Med 2012; Jager AIHA consensus Blood Rev 2020; Luzzatto G6PD Blood 2020; Manciu HS Chirurgia 2017. [1]
References
- [1]Goddard AF, James MW, McIntyre AS, Scott BB Guidelines for the management of iron deficiency anaemia Gut, 2011.PMID 21561874
- [2]Stabler SP Clinical practice. Vitamin B12 deficiency N Engl J Med, 2013.PMID 23301732
- [3]Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group N Engl J Med, 1999.PMID 9971864
- [4]Carson JL, Terrin ML, Noveck H, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery N Engl J Med, 2011.PMID 22168590
- [5]Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: a clinical practice guideline from the AABB* Ann Intern Med, 2012.PMID 22751760
- [6]Jager U, Barcellini W, Broome CM, et al. Diagnosis and treatment of autoimmune hemolytic anemia in adults: Recommendations from the First International Consensus Meeting Blood Rev, 2020.PMID 31839434
- [7]Luzzatto L, Nannelli C, Notaro R Glucose-6-phosphate dehydrogenase deficiency Blood, 2020.PMID 32702756
- [8]Manciu S, Maranduca MA, Tanase DM, et al. Hereditary Spherocytosis - Diagnosis, Surgical Treatment and Outcomes. A Literature Review Chirurgia (Bucur), 2017.PMID 28463670