Phys · haematological
Bleeding Disorders AND Thrombocytopenia
Also known as Bleeding Disorders AND Thrombocytopenia · bleeding disorders and thrombocytopenia
Consultant-physician depth guide to Bleeding Disorders AND Thrombocytopenia for FRACP DWE/DCE preparation — presentation, differentials, investigations, management, complications and exam angles.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
The answer first
Bleeding Disorders AND Thrombocytopenia is managed with an answer-first physician approach: recognise the pattern, exclude dangerous differentials, choose investigations that change action, and deliver a sequenced management plan that accounts for multimorbidity. [1] [2]
The FRACP candidate must be able to open a long-case presentation, defend thresholds, and answer DWE vignettes without hedging. Lead with the decision, then the evidence and the trap. [1]

Clinical spectrum and red flags
Presentations range from incidental or outpatient findings to emergency decompensation. Always ask what would make this urgent today — airway, perfusion, neurological threat, metabolic crisis, infection, or bleeding. [1] [2]
Red flags force same-day action rather than elective pathways. Document them explicitly in the plan. [1]
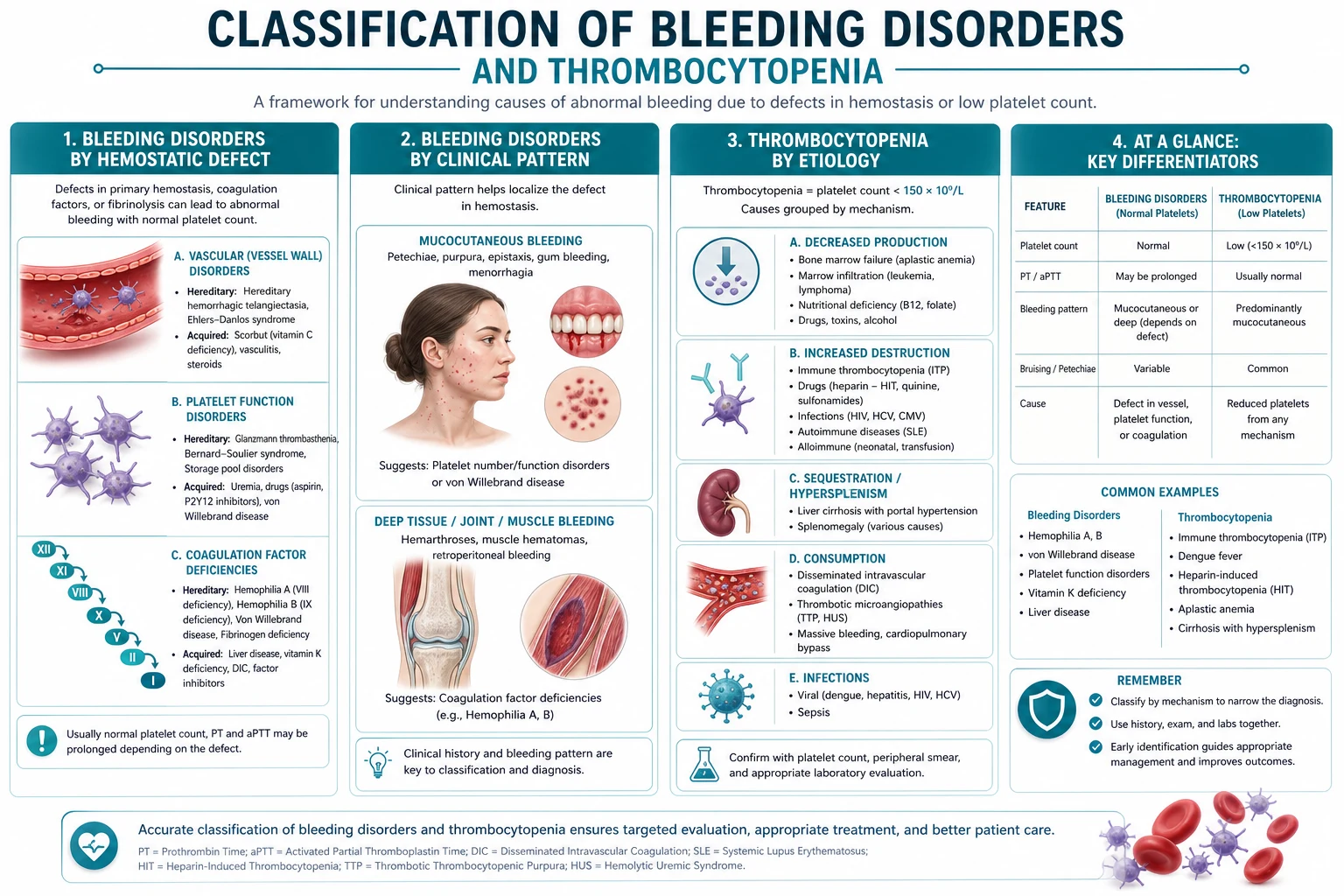
Classification that changes management
Classify by acuity, mechanism, severity and care setting. A useful classification changes investigation choice, initial therapy, disposition or specialist referral — otherwise it is taxonomy without purpose. [1] [2]
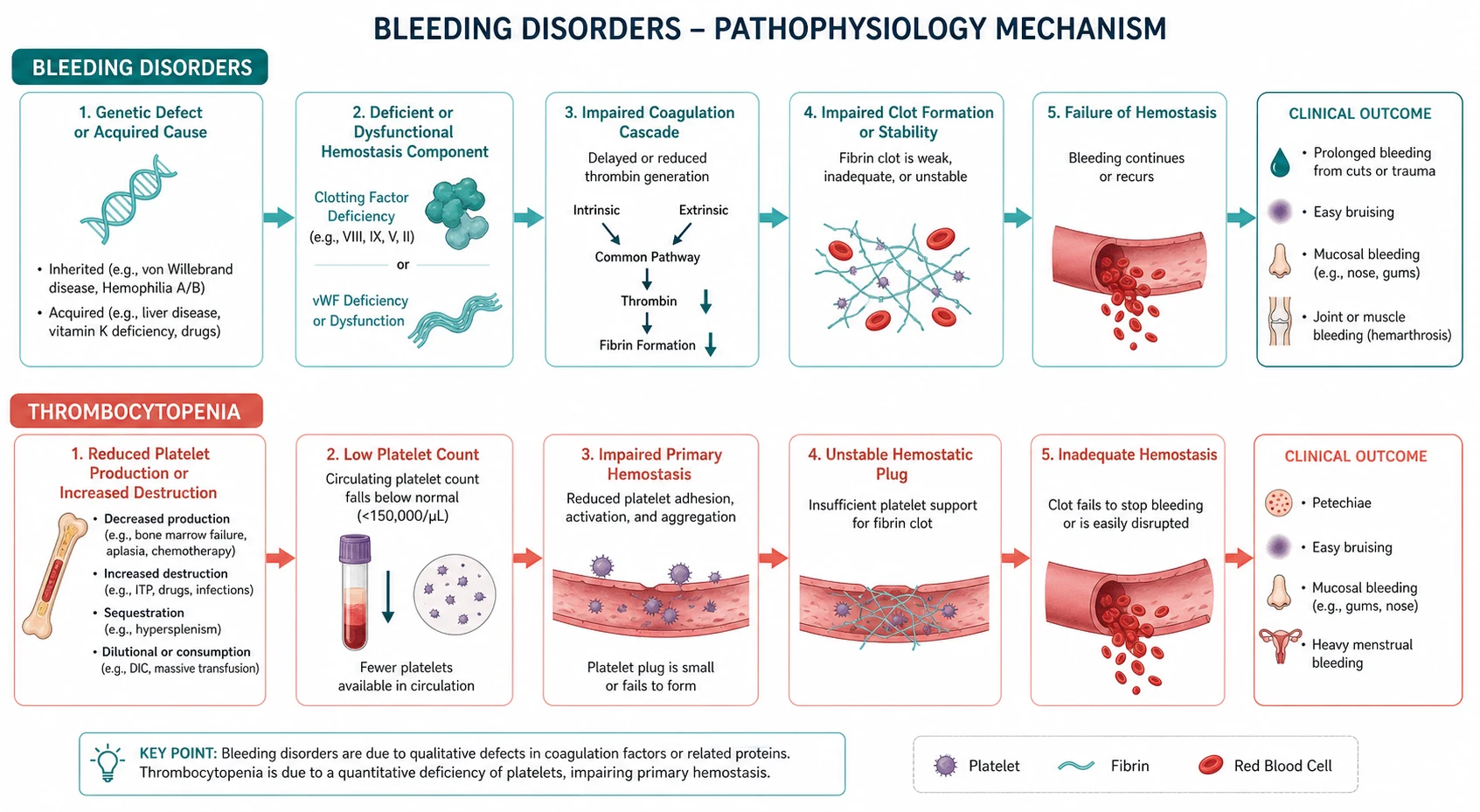
Pathophysiology linked to bedside decisions
Mechanism matters when it predicts treatment response, complications or monitoring. Teach pathophysiology as a bridge to action, not as isolated basic science. [1] [2] [3]
Differentials and discrimination
Build a short differential that includes the common, the dangerous and the commonly missed. For each alternative, name one history clue, one examination clue and one investigation that discriminates. [1] [2]
Investigations
Order tests that change management. State what is required now, what can wait, and what is low-value or harmful. Interpret results in clinical context rather than in isolation. [1] [2]
Management — immediate then definitive
- Stabilise threats to life and organ function. [1]
- Start disease-specific therapy once the working diagnosis is secure enough to act. [1] [2]
- Address complications, drug interactions and monitoring. [1] [2]
- Plan disposition, follow-up intensity and patient education with safety-net advice. [1]

Complications and prognosis
Anticipate early and late complications. Prognosis depends on severity at presentation, speed of effective therapy, comorbidity and adherence to secondary prevention or disease-modifying treatment. [1] [2]
Special populations and multimorbidity
Adjust for pregnancy potential, frailty, CKD, liver disease, immunosuppression and polypharmacy. In older adults, goals-of-care and treatment burden can change the preferred plan even when disease-directed options remain available. [1] [2]
DCE long-case angles
Open with a one-sentence synthesis, then a prioritised problem list, then an integrated plan covering investigations, treatment, prevention and communication. Link Bleeding Disorders AND Thrombocytopenia to cardiovascular risk, infection risk, medications and social context where relevant. [1] [2]
DCE short-case angles
Be prepared to demonstrate or discuss focused examination findings, interpret a key investigation, and counsel on risks, benefits and follow-up in plain language. [1]
Exam traps
- Delaying urgent care because the presentation looks "stable enough". [1]
- Treating a syndrome label without confirming mechanism. [1] [2]
- Forgetting drug interactions and organ-function dosing. [1] [2]
- Omitting safety-net advice and follow-up ownership. [1]
- Quoting thresholds without knowing the source trial or guideline. [1] [2] [3]
References
- [1]Ahn SY, Hong J, Kim JS, Kim SH, et al. Korean expert consensus on the management of thrombotic thrombocytopenic purpura Korean J Intern Med, 2026.PMID 42438901
- [2]Bierlein JG, Kurosch M, Mager R, Sasca D, et al. Acute hemophagocytic lymphohistiocytosis in a patient treated for stone removal via percutaneous nephrolithotomy: a case report and literature review Int J Surg Case Rep, 2026.PMID 42416426
- [3]Banerjee P, Allsup D, Uglow E, Hauff C, et al. A case of immune thrombocytopenia complicated by catastrophic antiphospholipid antibody syndrome and subsequent intramuscular haemorrhage J Med Case Rep, 2026.PMID 42415122
- [4]Zhou X, Liu Y, Zhang P, Shan N Precision targeting of CD38 in immune thrombocytopenia: Mechanistic foundations and therapeutic implications Eur J Pharmacol, 2026.PMID 41905452
- [5]Mingot-Castellano ME, Álvarez Román MT, Bastida JM, Butta N, et al. Navigating the Hemostatic Balance: Anticoagulation and Antiplatelet Therapy in Patients with Thrombocytopenia J Clin Med, 2026.PMID 41899195
- [6]Doan HN, Chang MC Comparative Effectiveness of Unstable Versus Stable Resistance Training on Lower Limb Strength, Mobility, and Fear of Falling in Older Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials Am J Phys Med Rehabil, 2026.PMID 42468010
- [7]Liu HW, Tsai TL Virtual Reality-assisted Physiotherapeutic Training for Patients With Knee Osteoarthritis: A Systematic Review and Meta-analysis Am J Phys Med Rehabil, 2026.PMID 42468005
- [8]Osborne AK, Brown RD, Sillence E Effects of Social Media Narratives on Affective and Behavioral Responses to Menopause Content: Randomized Online Experimental Study JMIR Form Res, 2026.PMID 42467962
- [9]Nishikawa K, Suto T, Shinagawa S, Takamine S, et al. Early postoperative onset of immune thrombocytopenia in rheumatoid arthritis with concomitant systemic lupus erythematosus: A case report Mod Rheumatol Case Rep, 2026.PMID 42421261
- [10]Kono A, Watanabe M, Sasaki Y, Noguchi Y, et al. [Immune-mediated thrombotic thrombocytopenic purpura with recurrent remission achieved by fresh frozen plasma transfusion and steroid therapy without plasma exchange] Rinsho Ketsueki, 2026.PMID 42419982
- [11]Pustake M, Patel S, Gomez J, Gaur S, et al. Secondary thrombotic thrombocytopenic purpura with features of Evans syndrome in a patient with SLE BMJ Case Rep, 2026.PMID 42425608
- [12]Goto T, Kitagawa J, Sakaida Y, Shimazu R, et al. [Transient acquired thrombotic thrombocytopenic purpura developed during bortezomib, lenalidomide, and dexamethasone therapy for multiple myeloma] Rinsho Ketsueki, 2026.PMID 42419983