Phys · haematological
Iron Deficiency
Also known as iron deficiency anaemia · IDA · microcytic anaemia · hypochromic anaemia · ferritin · transferrin saturation · TSAT · functional iron deficiency · oral iron · intravenous iron · ferric carboxymaltose
Consultant-physician-depth guide to iron deficiency — iron studies interpretation with the ferritin acute-phase caveat, absolute versus functional deficiency, the GI malignancy workup rule, coeliac serology, oral and IV iron with the alternate-day dosing evidence, and iron in heart failure, CKD, IBD and restless legs — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Iron Deficiency
The answer first
Iron deficiency is the commonest cause of anaemia in the world, the most over-investigated-yet-under-diagnosed number on the FBC, and — in an adult man or postmenopausal woman — a malignancy signal first and a haematinic deficiency second [1] [2]. Three rules carry you through almost every DWE question and every clinic letter:
- Diagnose with ferritin and TSAT together, and never trust ferritin alone in inflammation. Ferritin below about 30 µg/L confirms iron deficiency; but ferritin is an acute phase reactant, so in any inflamed patient a "normal" ferritin means nothing — read it beside CRP and transferrin saturation, where TSAT below 20% unmasks deficiency the ferritin is hiding [1] [5].
- Find the cause, and let the demographics choose the scope. Menstrual loss explains iron deficiency in a premenopausal woman until you prove otherwise; in men and postmenopausal women, occult GI blood loss is assumed and bidirectional endoscopy is the standard of care — iron tablets without gastroscopy and colonoscopy is the classic examination and medicolegal failure [5] [6].
- Replace iron physiologically, and match the route to the gut. Oral iron first for most — once daily or alternate days, because each dose spikes hepcidin and blocks the next one. Intravenous iron when the gut cannot absorb it or the loss outruns it: active IBD, bariatric surgery, CKD, heart failure, intolerance or non-response [11] [12] [14].
How iron moves — and why hepcidin runs the system
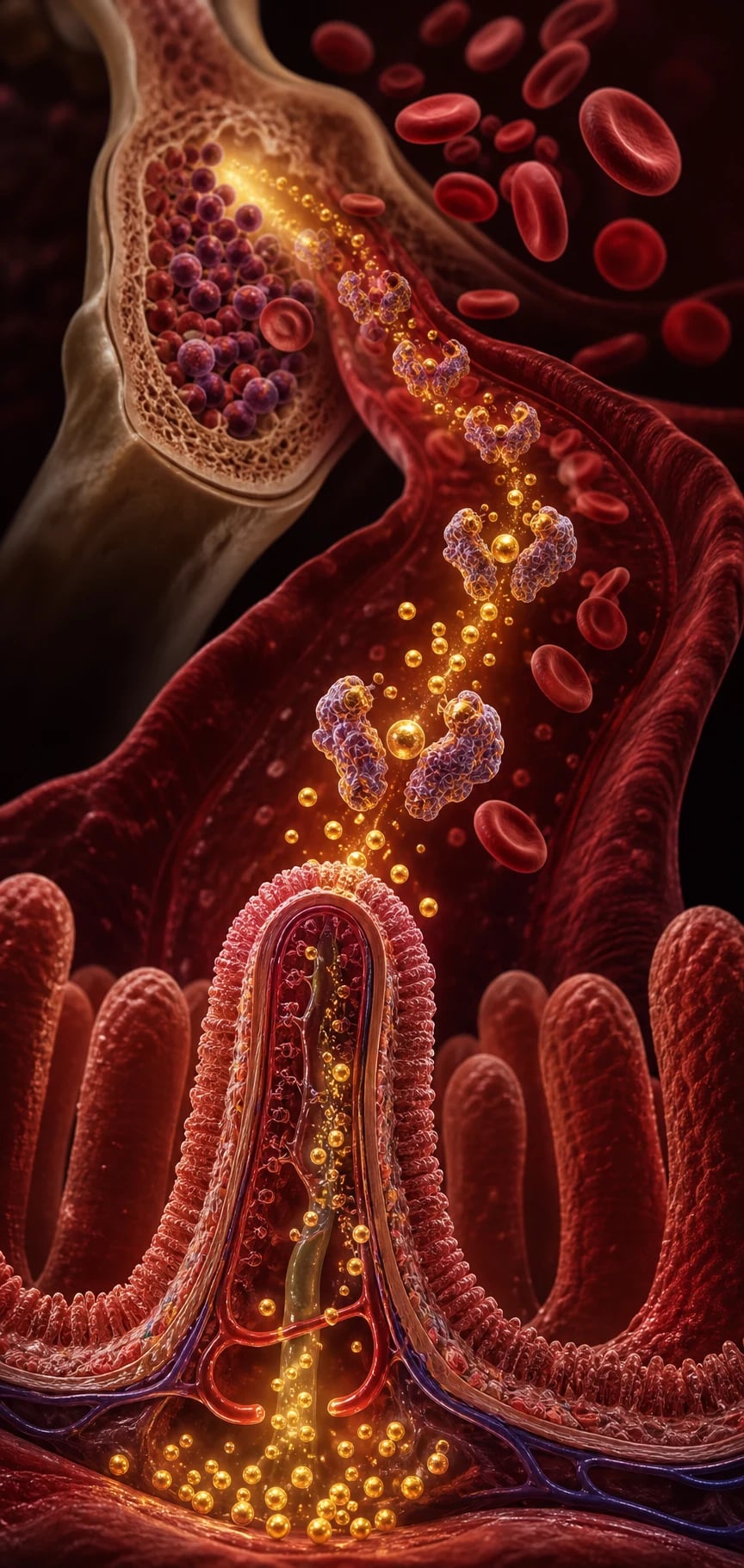
Adults carry about 3–4 g of iron, two-thirds of it in haemoglobin; they lose 1–2 mg a day through shed gut and skin cells and absorb the same amount in the duodenum and proximal jejunum. There is no regulated route of iron excretion — balance is controlled entirely at absorption, which is why any chronic pathological loss, however slow, eventually drains the tank [3] [1].
The journey of a milligram of dietary iron
Reduce
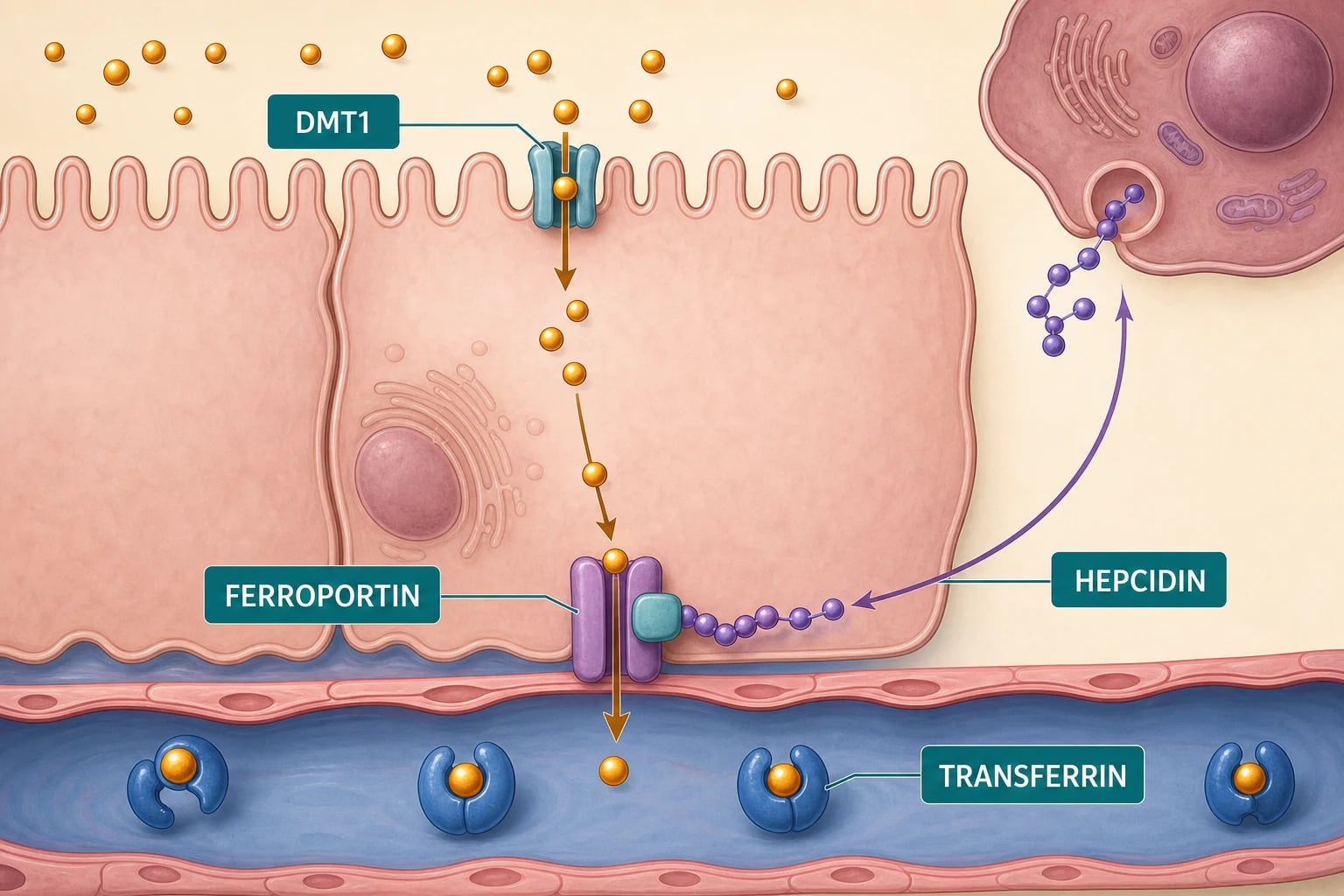
Ferric (Fe3+) iron is reduced to Fe2+ at the brush border by the ferric reductase DCYTB; gastric acid keeps iron soluble
Import
Fe2+ enters the enterocyte through DMT1 (divalent metal transporter 1) on the apical membrane
Export
Fe2+ exits into plasma through FERROPORTIN on the basolateral membrane — the only known cellular iron exporter
Load
Hephaestin re-oxidises Fe2+ to Fe3+, which loads onto transferrin for delivery to marrow, liver and muscle
Regulate
Hepcidin from the liver binds ferroportin and internalises it — switching off iron export from gut cells and macrophages
Hepcidin is the master switch, and it is the molecule that explains half of this topic [3] [4]. When iron stores are full, hepcidin rises, ferroportin is degraded, and iron stays locked inside enterocytes (lost when they are shed) and macrophages. When stores are empty, hepcidin falls and ferroportin opens. The trap for the unwary: inflammation raises hepcidin through IL-6, so in infection, malignancy, autoimmune disease, CKD and heart failure the body deliberately sequesters iron — plasma iron falls, ferritin rises, and marrow erythropoiesis is starved despite adequate total-body stores. That is the engine of the anaemia of chronic disease, and of functional iron deficiency [4].
Reading iron studies like a physician
Order ferritin, transferrin saturation and CRP together — and forget serum iron on its own, which swings with the time of day and crashes with any inflammation [1] [8].
| Test | What it measures | In true (absolute) iron deficiency | The caveat |
|---|---|---|---|
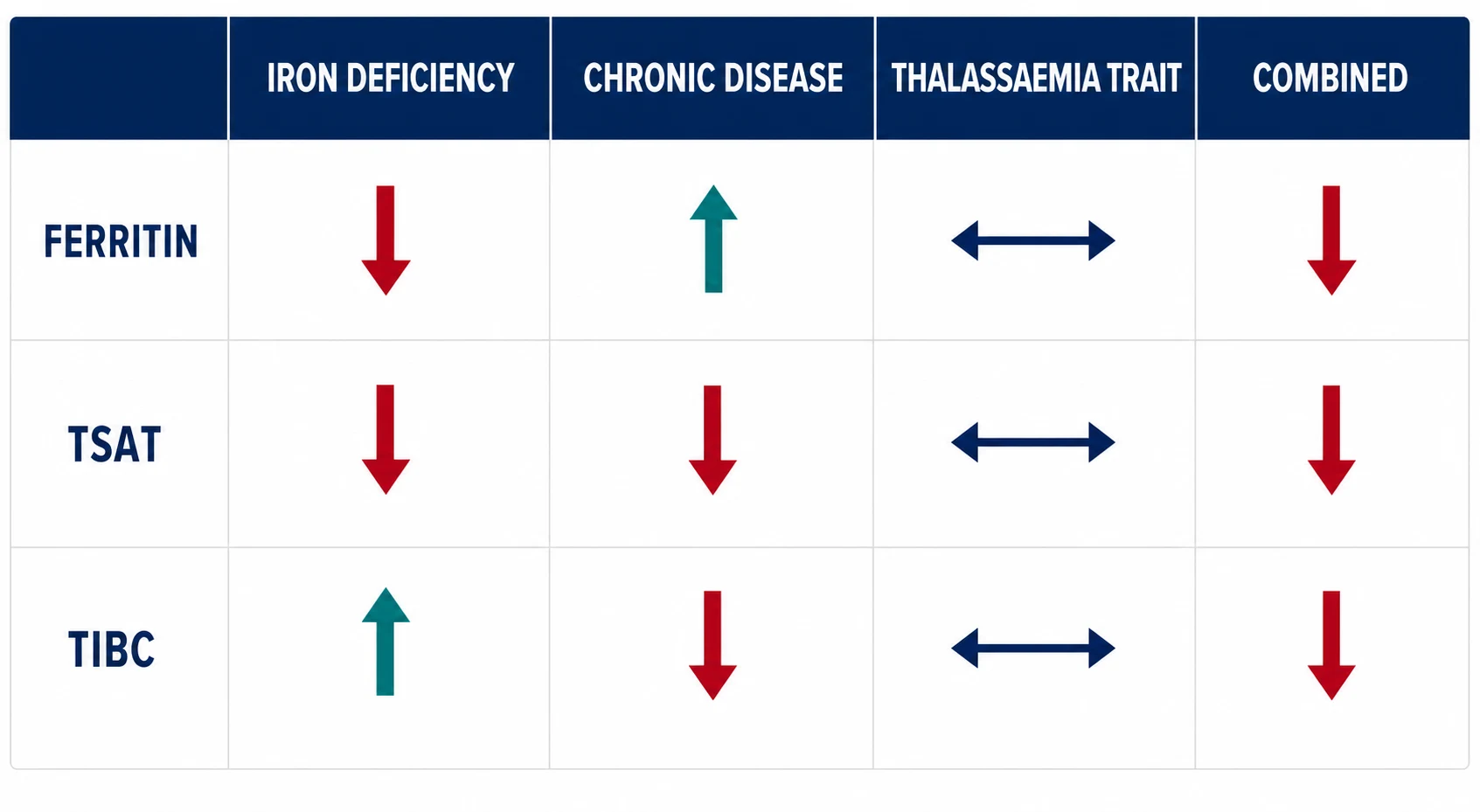
| Ferritin | Body iron stores | Below about 30 µg/L is diagnostic; below 15 is highly specific | Acute phase reactant — rises with inflammation, infection, malignancy, liver disease; can look falsely reassuring [1] [5] |
| TSAT (transferrin saturation) | Iron available for erythropoiesis | Below 20% supports iron-deficient erythropoiesis | Falls in inflammation too — but combined with a raised ferritin it separates functional from absolute deficiency [4] |
| TIBC / transferrin | Iron-carrying capacity (liver makes more transferrin when iron is scarce) | High | Falls in inflammation and malnutrition — the opposite direction to ferritin [1] |
| Soluble transferrin receptor (sTfR) | Cellular iron hunger | High | Largely unaffected by inflammation; the sTfR/log-ferritin index (the CR/IR ratio) above about 2 separates true deficiency from anaemia of chronic disease [9] |
| Reticulocyte haemoglobin (CHr) | Iron delivered to the youngest red cells | Below about 29 pg | The earliest signal of iron-restricted erythropoiesis, and of response to therapy [8] |
| Mentzer index (MCV ÷ RBC count) | Pattern recognition on the FBC | Above 13 favours iron deficiency | Below 13 favours thalassaemia trait — microcytosis with a high red cell count and normal iron studies [10] |
The blood film adds pattern, not proof: microcytic, hypochromic cells with anisopoikilocytosis and pencil (elliptical) cells, a rising RDW as the earliest numerical change, and a reactive thrombocytosis that accompanies blood loss. Severe long-standing deficiency can produce a dimorphic picture if B12 or folate deficiency coexists — which is exactly the combination coeliac disease delivers [1] [2].
Why adults become iron deficient — let the demographics choose the workup
Iron deficiency is never a final diagnosis; it is a question — where is the iron going, or why is none arriving? The answer distribution changes completely with age and sex, and the examiner expects you to say so [2] [5].
| Setting | Mechanism | Typical patient | Workup emphasis |
|---|---|---|---|
| Menstrual loss | Monthly loss exceeding intake (heavy menstrual bleeding) | Premenopausal woman | Quantify the loss; gynaecological review if heavy; GI workup only if red flags, family history, or no menstrual explanation [5] |
| GI blood loss | Occult bleeding — malignancy, peptic ulceration, NSAIDs, angiodysplasia, oesophagitis, IBD | Man or postmenopausal woman; anyone over 50 | Bidirectional endoscopy — gastroscopy AND colonoscopy [5] [6] |
| Malabsorption | Coeliac disease (villous atrophy of exactly the bowel that absorbs iron), autoimmune atrophic gastritis, H. pylori | Any age; often "refractory" to oral iron | tTG-IgA plus total IgA; consider gastroscopy with duodenal biopsies [7] [13] |
| Bariatric surgery | Roux-en-Y bypasses the duodenum; less acid, less surface | Post-gastric bypass | Expect malabsorption — often needs IV iron; guideline-mandated lifelong micronutrient monitoring [23] |
| Dietary insufficiency | Low bioavailable iron (vegan without planning), cow's-milk excess in toddlers | Vegans, adolescents, pregnancy | Dietary history; replace and counsel — but exclude other drivers in older patients [2] |
| Chronic disease / functional | Hepcidin-mediated sequestration ± reduced absorption | CKD, HF, IBD, malignancy, chronic inflammation | Treat the disease; IV iron where indicated [4] |
| Urinary and pulmonary loss | Intravascular haemolysis (PNH, mechanical valve) shedding haemosiderin; pulmonary haemosiderosis | Rare; hinted by haemoglobinuria or haemoptysis | Urine haemosiderin; haemolysis screen [1] |
The GI malignancy rule — and the workup that follows
The workup sequence for confirmed iron-deficiency anaemia
Confirm and phenotype
FBC and film, ferritin, TSAT, CRP, renal and liver function, B12/folate — establish absolute versus functional deficiency
Screen for coeliac disease
tTG-IgA with total IgA — do it before endoscopy and before any gluten-free diet; if IgA-deficient, use IgG-based serology
Bidirectional endoscopy
Gastroscopy (with duodenal biopsies — coeliac can be seronegative) AND colonoscopy for men and postmenopausal women
If both are negative
Reconsider the diagnosis, the adherence and the losses: menstrual history, NSAIDs, anticoagulants, urinary loss; small-bowel evaluation (capsule endoscopy) for ongoing obscure loss
Replace iron and follow the response
Route chosen by gut function and comorbidity; haemoglobin and ferritin rechecked — a flat response is itself a finding
A few precision points the examiner will probe [5] [7]:
- Coeliac serology belongs in essentially everyone with unexplained iron deficiency — coeliac disease classically presents as iron deficiency anaemia without GI symptoms, because the duodenum it destroys is precisely where iron is absorbed. Tissue transglutaminase IgA with a total IgA; serology can be falsely negative in IgA deficiency and once gluten is withdrawn, so test before dietary change, and take duodenal biopsies at gastroscopy regardless when suspicion persists [7].
- A negative gastroscopy does not close the case — and vice versa. Lesions coexist; bidirectional examination is the standard, not a sequence that stops at the first finding [5] [6].
- Faecal occult blood testing does not rule anything out. A negative FOBT has no place in excluding malignancy in iron deficiency — endoscopy is the test [5].
- Young premenopausal women with clear heavy menstrual losses and no red flags can be treated first, but coeliac serology is cheap, non-invasive and commonly positive — do not skip it [5] [7].
Oral iron — done properly
Oral iron is first line for most patients: cheap, effective, and limited mainly by absorption physiology and tolerance [1] [2].
The prescription. Ferrous sulfate 325 mg contains about 65 mg of elemental iron (ferrous gluconate and fumarate differ — prescribe in elemental terms). The modern dosing evidence overturned the old three-times-daily habit: a single 60 mg-plus oral dose triggers a hepcidin surge lasting about 24 hours that blunts absorption of the next dose, so twice- and thrice-daily schedules yield less fractional absorption, not more [11]. In the randomised trials that followed, alternate-day dosing produced higher total iron absorption than consecutive daily dosing, and a single morning dose outperformed split dosing — with fewer side effects, which is usually the real barrier to adherence [12].
| Practical point | What to tell the patient | Why |
|---|---|---|
| Dose | One ferrous sulfate tablet (65 mg elemental iron) once daily — alternate days is a legitimate, evidence-based alternative | Hepcidin surge lasts about 24 hours; spacing doses absorbs more, not less [11] [12] |
| Enhancers | Take on an empty stomach if tolerated; vitamin C (ascorbate) aids absorption | Ascorbate reduces Fe3+ to Fe2+ and counters food inhibition [2] |
| Inhibitors | Separate from tea, coffee, calcium, antacids and PPIs; food halves absorption | Polyphenols chelate iron; acid suppression impairs dissolution [2] [1] |
| Side effects | Nausea, epigastric discomfort, constipation, black stools (harmless) — warn explicitly | GI intolerance is the main cause of non-adherence; alternate-day dosing helps [12] |
| Duration | Continue about 3 months after haemoglobin normalises | Haemoglobin recovers long before stores do — stopping early guarantees relapse [1] |
Intravenous iron — when, and which
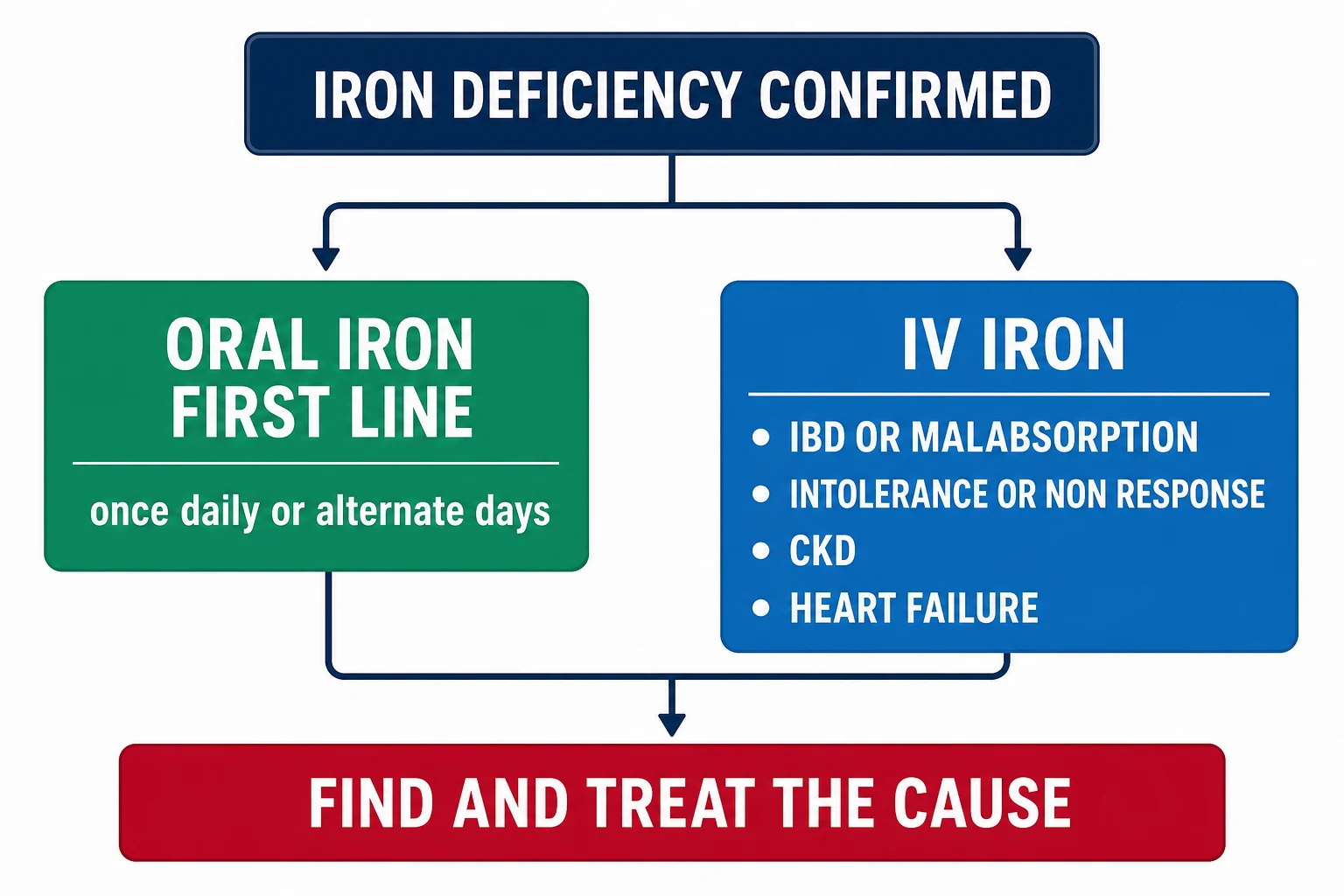
IV iron bypasses the hepcidin-blocked enterocyte and repletes total-body iron in one or two infusions. The art is in the indications, not the infusion [2] [14].
| Indication | The logic |
|---|---|
| Oral iron intolerance or non-adherence (documented) | Commonest everyday reason — but document the trial first |
| Malabsorption — active IBD, untreated coeliac, bariatric surgery | The gut cannot absorb; oral iron is futile and, in active IBD, poorly tolerated and potentially pro-inflammatory at the mucosa — ECCO consensus makes IV iron first line when disease is active [14] [23] |
| Ongoing loss exceeding absorptive capacity | Heavy menstrual bleeding awaiting definitive treatment, hereditary haemorrhagic telangiectasia, chronic GI loss — oral cannot keep pace [2] |
| CKD — especially on dialysis or an ESA | Functional deficiency; KDIGO-permitted thresholds; PIVOTAL showed proactive IV iron in dialysis patients reduced ESA requirements and transfusions without a safety signal [15] [16] |
| Heart failure with reduced ejection fraction | Symptomatic and hospitalisation benefit independent of anaemia — see the trial section below [17] [18] [19] |
| Need for rapid repletion | Late-pregnancy third trimester, preoperative optimisation with limited time, severe symptomatic deficiency [2] |
Products differ in carbohydrate shell and therefore in dose per visit: ferric carboxymaltose and ferric derisomaltose allow large single doses (about 15–20 mg/kg, commonly 1000 mg); iron sucrose and iron polymaltose require smaller repeated doses. Calculate the total deficit (haemoglobin deficit plus stores — the Ganzoni formula), give it, and recheck in 4–8 weeks [2] [14].
Infusion reactions are usually minor complement-activation–type events — flushing, chest or back tightness, arthralgia — that settle when the infusion is paused and restarted slowly; true anaphylaxis is rare with modern preparations, but infusions belong where resuscitation is available [14].
Iron in heart failure — the evidence block examiners quote
Iron deficiency affects roughly half of HFrEF patients, worsens exercise capacity and outcomes independently of anaemia, and has its own treatment evidence — which is why this is now a cardiology topic wearing a haematology coat [17] [18].
The trial definition of iron deficiency in heart failure is deliberately inflammation-aware: ferritin below 100 µg/L, or ferritin 100–300 µg/L with TSAT below 20% [17].
| Trial | Population | Intervention | Result | What it changed |
|---|---|---|---|---|
| FAIR-HF (2009) | Chronic HFrEF with iron deficiency, with or without anaemia | IV ferric carboxymaltose vs placebo | Improved patient global assessment, NYHA class and quality of life — including in non-anaemic patients | Established that iron deficiency itself, not just anaemia, is a treatment target [17] |
| AFFIRM-AHF (2020) | Hospitalised for acute HF, LVEF below 50%, iron deficient | IV ferric carboxymaltose at discharge and maintenance | Reduced recurrent HF hospitalisations; the composite with cardiovascular death narrowly missed significance | IV iron became part of the post-discharge checklist [18] |
| IRONMAN (2022) | HFrEF with iron deficiency, ambulatory UK population | IV ferric derisomaltose vs usual care | Fewer recurrent HF admissions and cardiovascular deaths, directionally consistent with AFFIRM-AHF (COVID-disrupted follow-up) | Extended the evidence to a second product and a health-system setting [19] |
Iron in chronic kidney disease — functional deficiency in its purest form
CKD concentrates every mechanism in this topic: inflammation-driven hepcidin elevation, reduced absorption, blood loss on dialysis, and an erythropoiesis-stimulating agent consuming iron faster than stores can release it. The result is the textbook functional iron deficiency — ferritin normal or high, TSAT low [4] [8].
KDIGO's thresholds are deliberately permissive compared with the general population: for adults with CKD, a trial of iron is recommended when TSAT is at or below 30% and ferritin at or below 500 µg/L and a haemoglobin rise is desired — oral for some non-dialysis patients, IV for dialysis patients and for most in practice [15] [16].
Two trials anchor the practice [15] [16]:
- FIND-CKD (non-dialysis CKD, 2014): IV ferric carboxymaltose achieved haemoglobin targets faster and more often than oral ferrous sulfate, with no increase in adverse events — the evidence that IV beats oral once CKD impairs absorption [15].
- PIVOTAL (maintenance haemodialysis, 2019): proactive high-dose iron sucrose was at least as safe as reactive low-dose dosing on cardiovascular outcomes, while reducing ESA doses and transfusion requirements — the trial that ended the fear of liberal IV iron on dialysis [16].
Restless legs, and iron deficiency without anaemia
Restless legs syndrome is a brain iron-deficiency disorder: CNS iron handling is abnormal even when peripheral stores look adequate, which is why the treatment thresholds differ from haematology's [22].
The IRLSSG task force recommendations give the examinable numbers: check a ferritin in every RLS patient; trial oral iron when ferritin is at or below 75 µg/L, and consider IV ferric carboxymaltose when ferritin is 75–100 µg/L or when oral iron fails or is not tolerated — with IV iron particularly favoured in moderate-to-severe RLS [22]. The same logic — iron as a cofactor worth replacing in its own right — underlies treating fatigue, pica and hair loss in iron deficiency without anaemia: repletion is reasonable, response is the arbiter, and the cause still needs finding [2].
Expected response — and the systematic non-responder workup
Set expectations explicitly, for patients and for examiners [1]:
What a successful course of iron looks like
When the haemoglobin has not moved by 3–4 weeks of apparently adequate oral iron, resist the urge to just switch formulations. Work the differential systematically — this is a complete SAQ answer by itself [13]:
The oral-iron non-responder
Confirm the diagnosis
Re-read the iron studies with CRP — is this really iron deficiency, or thalassaemia trait, sideroblastic change, or anaemia of chronic disease?
Confirm the dose got in
Adherence (side effects?), timing with tea/PPIs/food, formulation in elemental-iron terms
Look for ongoing loss
Quantify menstrual loss; ask about NSAIDs, anticoagulants, haematuria; reconsider the GI tract if endoscopy was incomplete
Look for malabsorption
Coeliac serology if not done, autoimmune atrophic gastritis (B12, parietal cell antibodies), H. pylori, bariatric anatomy, active IBD
Consider the rare
IRIDA (TMPRSS6 — microcytosis from childhood, family history, high-normal hepcidin physiology), and marrow disease if other lineages are involved
Act
Switch to IV iron while the cause hunt completes — non-response to oral iron is itself an IV indication
Transfusion — almost never the answer
Iron-deficiency anaemia develops over months; the cardiovascular system has compensated; and the patient has an iron deficit, not a blood-volume deficit. Transfusion in chronic iron deficiency buys a few weeks of haemoglobin at the price of alloimmunisation, volume load and a false sense of completion — and it treats none of the cause [1].
The narrow legitimate indications: haemodynamic compromise, severe angina or cardiac ischaemia, imminent surgery, or symptoms so severe that the weeks oral iron needs are unsafe — and even then, one unit, reassess, and start definitive iron replacement alongside [1]. In the exam, "transfuse for Hb 78 in a stable iron-deficient patient" is a distractor, not an answer; patient blood management principles make iron therapy the treatment and transfusion the exception [1] [2].
DCE angles — how this topic is examined live

The long case is iron deficiency as an entry point, not a diagnosis. The archetype: a postmenopausal woman (or older man) referred with fatigue and Hb 78 g/L, ferritin 12 µg/L — whose colonoscopy finds a caecal cancer. The examiner's arc moves from your diagnostic discipline (did you scope both ways, did you screen for coeliac, did you stage and refer) to your management synthesis (iron repletion around surgery, follow-up intervals, recurrence surveillance, the family conversation). Own the narrative: "iron deficiency was the presenting problem; the cancer was the diagnosis; the iron plan and the cancer plan ran in parallel" [5] [6].
The short case is the anaemia examination. Hands first — koilonychia (spoon-shaped, concave nails) and brittle nails; then eyes — conjunctival pallor; then mouth — angular cheilitis and glossitis (a smooth, depapillated, sore tongue); then look for the cause and the consequences — tachycardia and a flow murmur, abdominal masses or scars, a dialysis fistula, dermatitis herpetiformis, and the dysphagia history that suggests a post-cricoid web [1] [2].
Exam traps, collected
References
- [1]Camaschella C. Iron-deficiency anemia N Engl J Med, 2015.PMID 25946282
- [2]Lopez A, Cacoub P, Macdougall IC, et al. Iron deficiency anaemia Lancet, 2016.PMID 26314490
- [3]Ganz T. Systemic iron homeostasis Physiol Rev, 2013.PMID 24137020
- [4]Camaschella C, Nai A, Silvestri L. Iron metabolism and iron disorders revisited in the hepcidin era Haematologica, 2020.PMID 31949017
- [5]Snook J, Bhala N, Beales ILP, et al. British Society of Gastroenterology guidelines for the management of iron deficiency anaemia in adults Gut, 2021.PMID 34497146
- [6]Rockey DC, Cello JP. Evaluation of the gastrointestinal tract in patients with iron-deficiency anemia N Engl J Med, 1993.PMID 8179652
- [7]Ludvigsson JF, Bai JC, Biagi F, et al. Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology Gut, 2014.PMID 24917550
- [8]Thomas DW, Hinchliffe RF, Briggs C, et al. Guideline for the laboratory diagnosis of functional iron deficiency Br J Haematol, 2013.PMID 23573815
- [9]Punnonen K, Irjala K, Rajamäki A. Serum transferrin receptor and its ratio to serum ferritin in the diagnosis of iron deficiency Blood, 1997.PMID 9028338
- [10]Mentzer WC Jr. Differentiation of iron deficiency from thalassaemia trait Lancet, 1973.PMID 4123424
- [11]Moretti D, Goede JS, Zeder C, et al. Oral iron supplements increase hepcidin and decrease iron absorption from daily or twice-daily doses in iron-depleted young women Blood, 2015.PMID 26289639
- [12]Stoffel NU, Cercamondi CI, Brittenham G, et al. Iron absorption from oral iron supplements given on consecutive versus alternate days and as single morning doses versus twice-daily split dosing in iron-depleted women: two open-label, randomised controlled trials Lancet Haematol, 2017.PMID 29032957
- [13]Hershko C, Camaschella C. How I treat unexplained refractory iron deficiency anemia Blood, 2014.PMID 24215034
- [14]Dignass AU, Gasche C, Bettenworth D, et al. European consensus on the diagnosis and management of iron deficiency and anaemia in inflammatory bowel diseases J Crohns Colitis, 2015.PMID 25518052
- [15]Macdougall IC, Bock AH, Carrera F, et al. FIND-CKD: a randomized trial of intravenous ferric carboxymaltose versus oral iron in patients with chronic kidney disease and iron deficiency anaemia Nephrol Dial Transplant, 2014.PMID 24891437
- [16]Macdougall IC, White C, Anker SD, et al. Intravenous Iron in Patients Undergoing Maintenance Hemodialysis N Engl J Med, 2019.PMID 30365356
- [17]Anker SD, Comin Colet J, Filippatos G, et al. Ferric carboxymaltose in patients with heart failure and iron deficiency N Engl J Med, 2009.PMID 19920054
- [18]Ponikowski P, Kirwan BA, Anker SD, et al. Ferric carboxymaltose for iron deficiency at discharge after acute heart failure: a multicentre, double-blind, randomised, controlled trial Lancet, 2020.PMID 33197395
- [19]Kalra PR, Cleland JGF, Petrie MC, et al. Intravenous ferric derisomaltose in patients with heart failure and iron deficiency in the UK (IRONMAN): an investigator-initiated, prospective, randomised, open-label, blinded-endpoint trial Lancet, 2022.PMID 36347265
- [20]Wolf M, Chertow GM, Macdougall IC, et al. Randomized trial of intravenous iron-induced hypophosphatemia JCI Insight, 2018.PMID 30518682
- [21]Schaefer B, Tobiasch M, Viveiros A, et al. Hypophosphataemia after treatment of iron deficiency with intravenous ferric carboxymaltose or iron isomaltoside-a systematic review and meta-analysis Br J Clin Pharmacol, 2021.PMID 33188534
- [22]Allen RP, Picchietti DL, Auerbach M, et al. Evidence-based and consensus clinical practice guidelines for the iron treatment of restless legs syndrome/Willis-Ekbom disease in adults and children: an IRLSSG task force report Sleep Med, 2018.PMID 29425576
- [23]Allied Health Sciences Section Ad Hoc Nutrition Committee, Aills L, Blankenship J, et al. ASMBS Allied Health Nutritional Guidelines for the Surgical Weight Loss Patient Surg Obes Relat Dis, 2008.PMID 18490202