Phys · haematological
Lymphoma — Hodgkin and Non-Hodgkin
Also known as Hodgkin lymphoma · Hodgkin's lymphoma · Hodgkin disease · non-Hodgkin lymphoma · NHL · diffuse large B-cell lymphoma · DLBCL · follicular lymphoma · Burkitt lymphoma · mantle cell lymphoma · marginal zone lymphoma · MALT lymphoma · primary CNS lymphoma · Waldenstrom macroglobulinaemia · lymphoplasmacytic lymphoma
Consultant-physician-depth guide to Hodgkin and non-Hodgkin lymphoma for FRACP DWE and DCE — Reed-Sternberg biology, Ann Arbor and Lugano staging, ABVD and PET-adapted therapy, the International Prognostic Score, DLBCL with R-CHOP and the IPI, follicular lymphoma and FLIPI, Burkitt emergencies, primary CNS lymphoma, marginal zone and mantle cell subtypes, CAR-T therapy for relapsed disease, and the Deauville response system.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Lymphoma — Hodgkin and Non-Hodgkin
The answer first
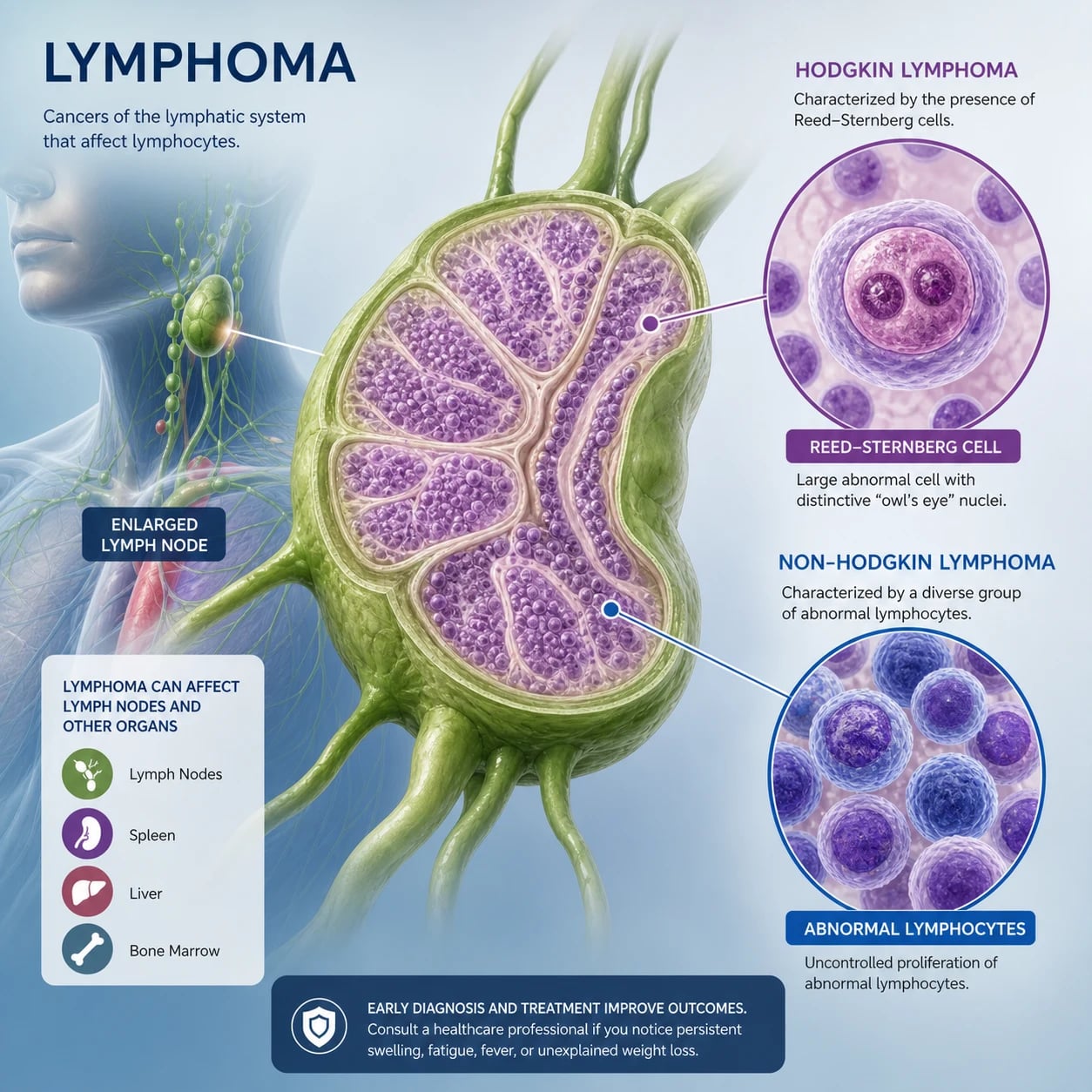
Lymphoma is a clonal proliferation of lymphoid cells that presents most often as painless lymphadenopathy, a mediastinal mass, or an extranodal mass, frequently with the B symptoms of unexplained fever, drenching night sweats, and weight loss. The single most important diagnostic rule: the diagnosis is made on excisional lymph node biopsy, not fine-needle aspiration. Flow cytometry and immunohistochemistry on a whole node preserve architecture; FNA destroys it and misses lymphoma in a meaningful proportion of patients [6].
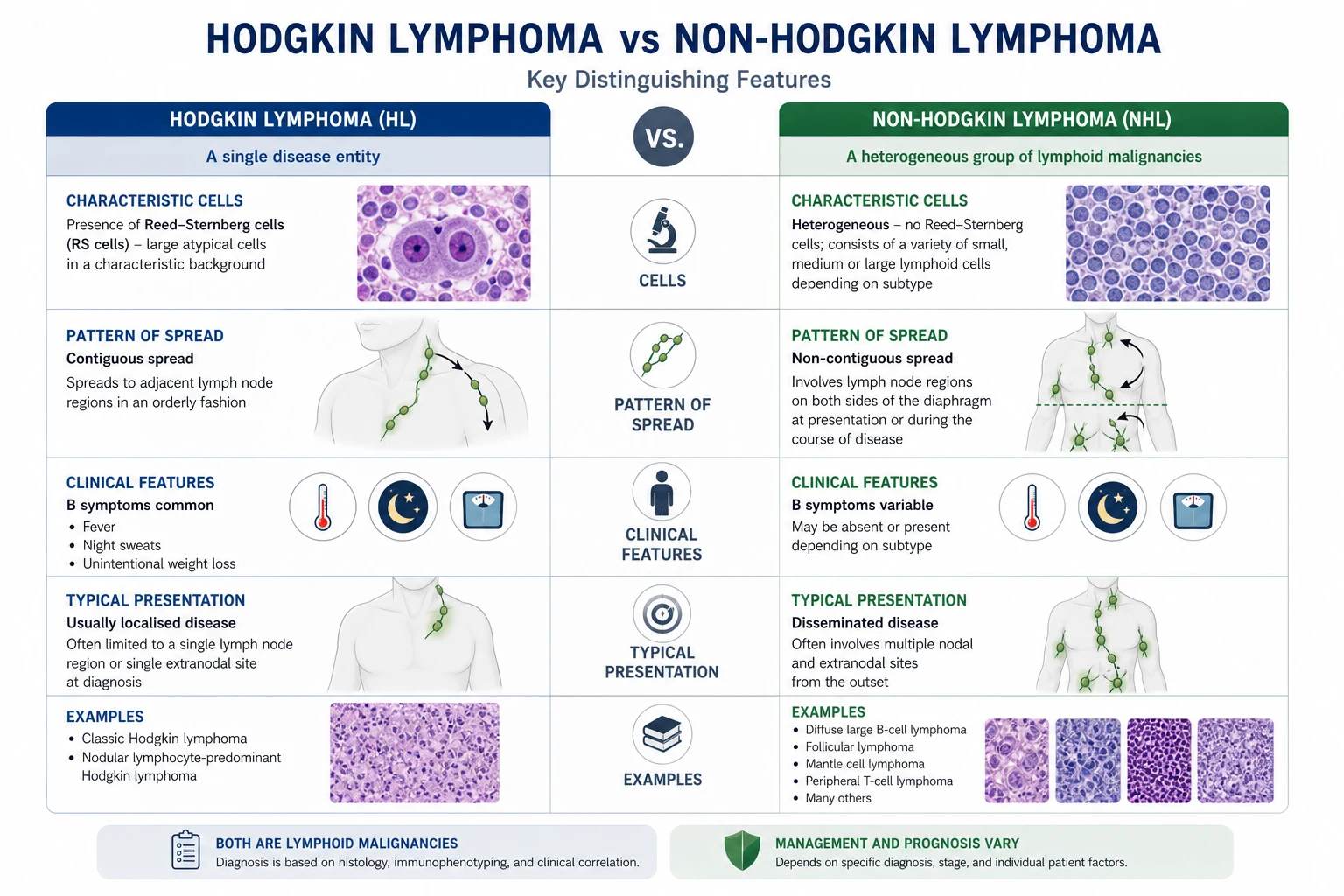
The second rule is a fork in the road that changes everything downstream: Hodgkin versus non-Hodgkin. Hodgkin lymphoma is defined by the Reed-Sternberg cell (a clonal B cell derived from the germinal centre) within an inflammatory background, spreads in a contiguous fashion, is exquisitely chemo-radiosensitive, and is among the most curable of all cancers — five-year survival over 85 per cent in developed countries. Non-Hodgkin lymphoma is heterogeneous: the clinical fork is indolent versus aggressive versus very aggressive, and the management fork is watch-and-wait versus urgent chemoimmunotherapy versus emergency cytoreduction with tumour lysis prophylaxis [6].
Three bedside rules that change outcome: [1]
- Suspected Burkitt or lymphoblastic with high LDH? Start tumour lysis prophylaxis now. Burkitt lymphoma has the fastest doubling time of any human tumour (24 hours) and tumour lysis syndrome can develop spontaneously before chemotherapy is given. Aggressive hydration, rasburicase, and close electrolyte monitoring are started on suspicion [14].
- Suspected primary CNS lymphoma? Hold the steroids. Corticosteroids lyse lymphoma cells and can make a stereotactic biopsy non-diagnostic. If you give dexamethasone to reduce cerebral oedema before biopsy, the diagnosis may be lost [15].
- DLBCL with kidney, adrenal, testicular, paranasal sinus, or bone marrow involvement? Assess for CNS prophylaxis. CNS relapse in DLBCL is usually fatal. The CNS-IPI identifies patients who benefit from intrathecal or systemic CNS-penetrant prophylaxis [11].
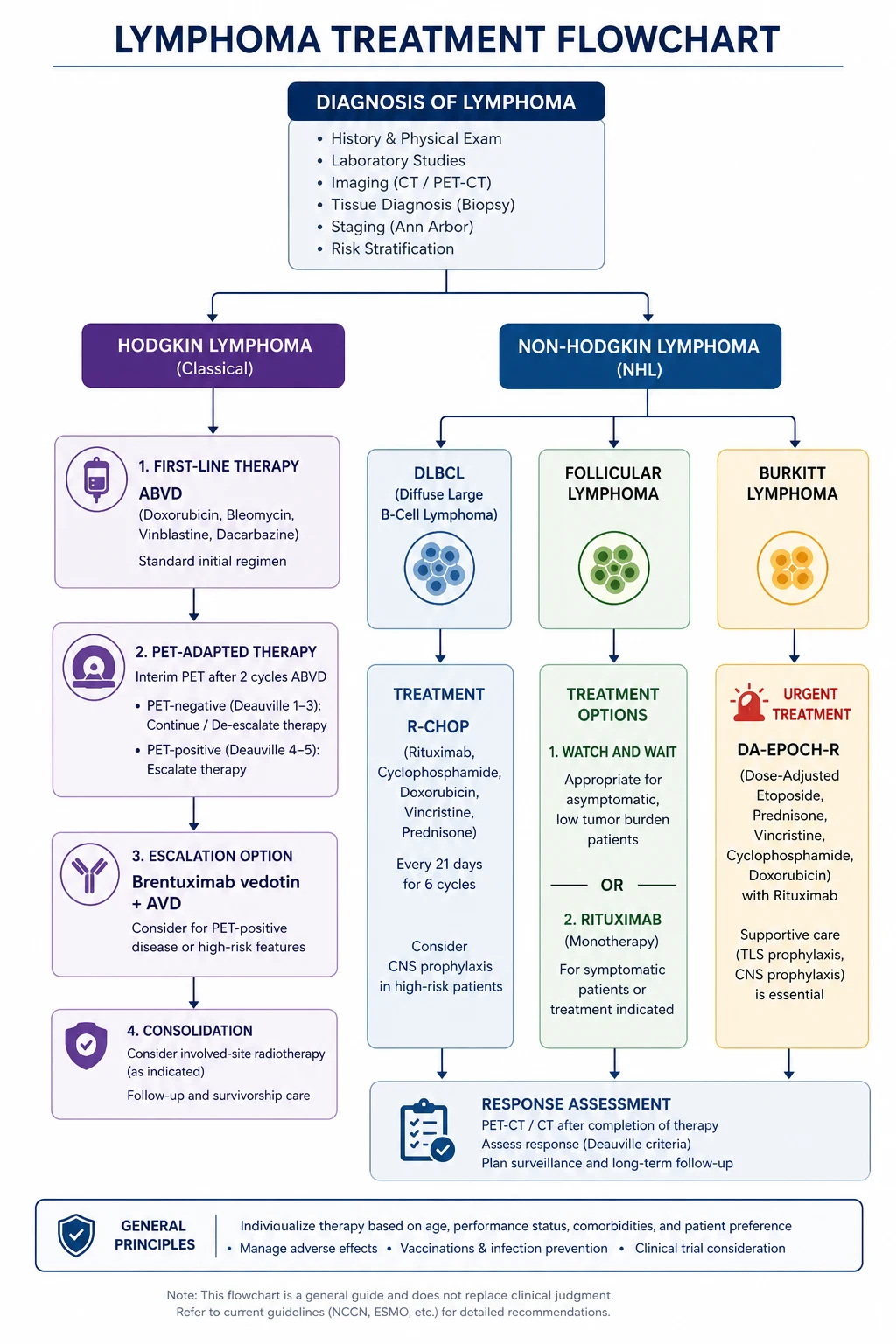
For fit patients with advanced classical Hodgkin lymphoma, the modern backbone is ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine), increasingly modified by interim PET-adapted therapy (escalate if PET-positive after 2 cycles, de-escalate or omit bleomycin if PET-negative) and the newer frontline option of brentuximab vedotin plus AVD [3][4]. For DLBCL — the commonest aggressive NHL — the backbone is R-CHOP (rituximab, cyclophosphamide, doxorubicin, vincristine, prednisone) given every 21 days for 6 cycles [8]. For relapsed DLBCL the paradigm has shifted to CAR-T cell therapy (axicabtagene ciloleucel, tisagenlecleucel) after platinum-based salvage, with curative intent in patients previously deemed incurable [17].
Classification
The two great divisions
Lymphoma is divided first by the presence of the Reed-Sternberg cell — Hodgkin lymphoma — or its absence — non-Hodgkin lymphoma. Within NHL, the practical subdivision is by clinical behaviour: indolent, aggressive, or very aggressive. This single axis determines urgency, intent (palliation versus cure), and the choice of regimen. [1]
| Feature | Hodgkin lymphoma | Non-Hodgkin lymphoma |
|---|---|---|
| Defining cell | Reed-Sternberg (large binucleate B cell with owl-eye nucleoli) in an inflammatory background | Monoclonal lymphoid cells without Reed-Sternberg morphology |
| Pattern of spread | Contiguous, chain to chain | Non-contiguous, haematogenous, extranodal common |
| Extranodal involvement | Less common ( marrow involvement is rare at diagnosis) | Common (GI, skin, CNS, bone, testis) |
| Typical age | Bimodal — young adults (15 to 35) and over 55 | Median 65 for most NHL; subtype-dependent |
| B symptoms | Common, especially drenching night sweats | Common in aggressive subtypes |
| Curability | Highly curable — over 85 per cent 5-year survival | Depends on subtype — DLBCL curable in about 60 to 70 per cent; follicular incurable but indolent |
| Typical chemotherapy | ABVD, escalated BEACOPP, A+AVD | R-CHOP, R-EPOCH, BR, DA-EPOCH-R, CODOX-M/IVAC |
Hodgkin lymphoma — classical and nodular lymphocyte-predominant
Two distinct entities are grouped under Hodgkin lymphoma: [1]
- Classical Hodgkin lymphoma (95 per cent) — Reed-Sternberg cells are CD30-positive, CD15-positive, usually CD20-negative, in a rich inflammatory background of lymphocytes, eosinophils, plasma cells, and fibrosis. The four subtypes are nodular sclerosis (the commonest, particularly in young adults with a mediastinal mass), mixed cellularity (more common in older adults and HIV, often Epstein-Barr virus-associated), lymphocyte-rich, and lymphocyte-depleted (rarest, most aggressive).
- Nodular lymphocyte-predominant Hodgkin lymphoma (5 per cent) — the neoplastic cell is the "popcorn" cell (LP cell), CD20-positive, CD15-negative, CD30-negative. It behaves more like an indolent B-cell NHL, is treated differently (often rituximab-based), and has a higher rate of late relapse and transformation to DLBCL. [1]
Non-Hodgkin lymphoma — by clinical behaviour
| Group | Subtype | Hallmarks |
|---|---|---|
| Indolent | Follicular lymphoma | t(14;18), BCL2; CD10+; relapsing-remitting; median survival over 15 years with modern therapy |
| Indolent | Marginal zone (MALT, nodal, splenic) | Gastric MALT driven by H. pylori; eradication can cure early disease |
| Indolent | Mantle cell lymphoma | t(11;14), cyclin D1; CD5+; biologically aggressive though variable clinically |
| Indolent | Lymphoplasmacytic (Waldenstrom) | MYD88 L265P; IgM paraprotein; hyperviscosity syndrome |
| Indolent | Small lymphocytic lymphoma / CLL | Same disease as CLL; see the CLL topic |
| Aggressive | Diffuse large B-cell lymphoma | Commonest NHL (30 per cent); CD20+; R-CHOP; cell-of-origin (GCB vs ABC) prognostic |
| Aggressive | Primary mediastinal B-cell lymphoma | Young women; mediastinal mass; resembles nodular sclerosis Hodgkin; CD30+ |
| Aggressive | T-cell lymphomas (peripheral, anaplastic large cell) | Heterogeneous; often poorer prognosis; ALK-positive ALCL favourable |
| Very aggressive | Burkitt lymphoma | t(8;14), MYC; "starry sky"; fastest doubling time; endemic (African jaw), sporadic (abdomen), HIV-associated |
| Very aggressive | Lymphoblastic lymphoma (B or T) | T-cell presents with mediastinal mass and CNS disease; overlaps with ALL |
| Special site | Primary CNS lymphoma | Diffuse large B-cell; EBV in immunosuppressed; methotrexate-based |
| Skin | Cutaneous T-cell (mycosis fungoides, Sezary) | Indolent skin patches and plaques; Sezary = erythroderma + circulating Sezary cells |
DWE high-yield: Three lymphomas present with a mediastinal mass in a young adult — nodular sclerosis classical Hodgkin lymphoma, primary mediastinal B-cell lymphoma (PMBCL, in young women), and T-lymphoblastic lymphoma. The discriminating features are age, sex, distribution, CD markers, and the presence or absence of Reed-Sternberg cells. [1]
Pathophysiology
Hodgkin lymphoma — the Reed-Sternberg cell and its microenvironment
The Reed-Sternberg cell is a clonal B lymphocyte that has traversed the germinal centre but lost the ability to produce functional immunoglobulin — it should normally undergo apoptosis but is rescued by constitutive NF-kB and JAK/STAT signalling. The cell is rare within the tumour (often less than 1 per cent of the cellular mass); the bulk of the diseased node is the reactive inflammatory background — T lymphocytes (rosetting around the Reed-Sternberg cell), eosinophils (driven by IL-5), plasma cells, and fibrosis. This microenvironment is what gives Hodgkin lymphoma its characteristic histological pattern and its B symptoms. [1]
In classical Hodgkin lymphoma, Epstein-Barr virus is detected in the Reed-Sternberg cells in about 40 per cent of cases in developed countries (higher in mixed cellularity and HIV-associated disease). EBV expresses latent membrane protein 1 (LMP1), a constitutive CD40 mimic that drives NF-kB and B-cell survival. [1]
DWE conceptual: Why does Hodgkin lymphoma spread contiguously from one lymph node chain to the next, while NHL spreads haematogenously? Because the Reed-Sternberg cell depends on its supportive microenvironment to survive. It cannot seed distant organs without its inflammatory retinue. This contiguity is what made radiotherapy to involved and adjacent fields curative in the pre-chemotherapy era. [1]
Follicular lymphoma — the t(14;14) BCL2 translocation
Follicular lymphoma is the prototypical indolent NHL. The t(14;18) translocation places the BCL2 gene under the immunoglobulin heavy chain enhancer, driving overexpression of BCL2 protein, which blocks apoptosis. The follicle centre B cells accumulate rather than die — the lymph node fills with neoplastic follicles. The patient may have widespread disease at diagnosis but feel entirely well. The natural history is one of relapsing-remitting disease over many years, with eventual transformation to DLBCL in perhaps 2 to 3 per cent of patients per year — transformation presents with rapidly growing disease, high LDH, and a worse prognosis. [1]
Burkitt lymphoma — c-myc dysregulation and the fastest doubling time in oncology
The t(8;14) translocation places the MYC oncogene next to the immunoglobulin heavy chain enhancer, driving relentless proliferation. The tumour has a doubling time of roughly 24 hours, a high growth fraction (Ki-67 close to 100 per cent), and a "starry sky" appearance on histology (the "stars" are macrophages ingesting the apoptotic tumour cells). The three clinical forms are endemic (Equatorial Africa, jaw mass in children, EBV in essentially all cases), sporadic (Western countries, abdominal mass — ileocaecal, ovarian, ovarian — in children and young adults, EBV in about 30 per cent), and HIV-associated. The rapid growth drives both the curability (chemotherapy hits dividing cells) and the danger — spontaneous tumour lysis syndrome is a real risk before any treatment is given [14].
Diffuse large B-cell lymphoma — cell-of-origin and the molecular era
DLBCL is heterogeneous. Gene expression profiling divides it into the germinal centre B-cell (GCB) subtype and the activated B-cell (ABC) subtype. The ABC subtype has constitutive NF-kB signalling (often via MYD88, CD79B), a poorer prognosis with R-CHOP, and a higher rate of CNS relapse. The GCB subtype is driven by BCL2 and EZH, often has the t(14;18) translocation, and has a better outcome. The HOVON/LYSA consortium and the now-emerging cell-of-origin assays allow therapy to be tailored — though R-CHOP remains the standard frontline for both in 2026. [1]
Clinical presentation
The lymphadenopathy history — what to ask
When a patient presents with a lump in the neck, axilla, or groin, the questions that discriminate benign from malignant, and lymphoma from other malignancy, are: [1]
- How long has it been there and is it growing? Lymphomatous nodes are typically painless, rubbery, and progressively enlarging over weeks to months. Acute, tender nodes suggest infection. A node present for over 4 to 6 weeks without resolution warrants investigation.
- Where is it and how big is it? Nodes over 1 cm in the cervical chain, over 1.5 cm in the axilla or supraclavicular fossa, or any palpable node in the supraclavicular fossa (Virchow's node — strongly associated with malignancy) demand explanation. A supraclavicular node in a smoker mandates exclusion of lung cancer.
- Are there B symptoms? The classic B symptoms are unexplained fever above 38 degrees Celsius, drenching night sweats (the kind that soak the sheets and force the patient to change), and weight loss of more than 10 per cent of body weight over 6 months. Their presence mandates a search for lymphoma; their absence does not exclude it.
- Is there itch, alcohol-induced pain, or fatigue? Generalised itch and, classically, pain in involved nodes after alcohol ingestion are well-described in Hodgkin lymphoma. Fatigue is common and non-specific.
- Is there a background of immunosuppression? HIV, post-transplant immunosuppression, autoimmune disease (Sjogren, rheumatoid, Hashimoto), and prior chemotherapy all raise the risk of lymphoma. [1]
The examination — every lymph node region and the spleen
A systematic lymphoma examination covers all the major node groups in turn — cervical (including supraclavicular), axillary, epitrochlear, inguinal, popliteal — and then the abdomen for hepatosplenomegaly, the oropharynx for Waldeyer's ring involvement, and the skin for cutaneous deposits. Examine also the testes (a sanctuary site for lymphoma) and perform a brief neurological assessment. Document the size, consistency, mobility, and tenderness of each node — the registrar's careful map is the haematologist's starting point. [1]
Pattern by subtype
| Subtype | Typical presentation |
|---|---|
| Nodular sclerosis Hodgkin | Young adult, cervical and mediastinal nodes, B symptoms, itch |
| DLBCL | Older adult, rapidly enlarging nodal or extranodal mass; any site — gut, bone, skin, brain, testis |
| Follicular | Older adult, widespread painless nodes, often asymptomatic; waxing and waning |
| Burkitt | Child or young adult, rapidly growing abdominal mass (sporadic) or jaw (endemic); high LDH; risk of tumour lysis |
| Primary CNS lymphoma | Immunocompetent older adult or immunosuppressed; focal deficit, seizures, cognitive change; solitary or multiple brain lesions |
| Primary mediastinal B-cell | Young woman, mediastinal mass, superior vena cava syndrome |
| Gastric MALT | Long-standing H. pylori gastritis; epigastric discomfort; diagnosis on endoscopy |
| Mantle cell | Older man, widespread nodes, gut involvement, often aggressive |
| Waldenstrom | Older man, fatigue, neuropathy, hyperviscosity (visual disturbance, headache, mucosal bleeding), IgM paraprotein |
| Mycosis fungoides / Sezary | Chronic skin patches and plaques, eventually tumours and erythroderma; Sezary cells on blood film |
The superior vena cava syndrome — an oncological emergency
A large mediastinal mass (Hodgkin, PMBCL, T-lymphoblastic, germ cell tumour) can obstruct the superior vena cava: facial plethora, distended neck and chest wall veins, conjunctival injection, cough, and dyspnoea, worse when lying flat or bending forward. This is an emergency — arrange urgent imaging and a tissue diagnosis (often via a peripheral node or mediastinoscopy), and involve the haematology or oncology team. Steroids are sometimes given if the airway is compromised, but the principle of histological diagnosis first still holds. [1]
Differential diagnosis of lymphadenopathy
| Cause | Discriminating features |
|---|---|
| Reactive infective | Tender, mobile, short history; viral (EBV, CMV, HIV seroconversion), bacterial, tuberculous |
| Tuberculous lymphadenitis | Painless matted nodes, often cervical (scrofula); systemic symptoms; risk factors (endemic exposure, immunosuppression); needs excisional biopsy with TB cultures |
| Metastatic carcinoma | Hard, fixed nodes; supraclavicular (Virchow) — lung, gastric, breast, prostate, head and neck primary |
| Lymphoma | Painless, rubbery, progressive; B symptoms; systemic exam for hepatosplenomegaly |
| Sarcoidosis | Bilateral hilar lymphadenopathy, erythema nodosum, uveitis; non-caseating granulomas on biopsy |
| HIV-related | Generalised lymphadenopathy, constitutional symptoms, risk factors; high-grade NHL risk |
| Castleman disease | Hyaline-vascular (asymptomatic mass) or multicentric (systemic symptoms, HHV-8 in HIV) |
| Kikuchi-Fujimoto | Self-limiting necrotising lymphadenitis, young Asian women, fever, cervical nodes |
| Rosai-Dorfman | Massive painless cervical lymphadenopathy, young adults, histiocytes with emperipolesis |
DWE discriminator: Painless, progressively enlarging, rubbery cervical lymphadenopathy in a young adult with night sweats is Hodgkin lymphoma until proven otherwise. The first investigation is an excisional lymph node biopsy — not FNA, not a CT scan, not a trial of antibiotics. A node that has not resolved in 4 to 6 weeks, or that grows, or that is accompanied by B symptoms, mandates biopsy. [1]
Investigations
Essential investigations for every patient with suspected lymphoma
| Investigation | Why |
|---|---|
| Excisional lymph node biopsy | The diagnosis. Preserves architecture for histology; allows immunohistochemistry, flow cytometry, FISH for translocations, and conventional cytogenetics. FNA is inadequate for initial diagnosis. |
| Core biopsy or bone marrow biopsy | If no accessible node; for marrow-based disease (CLL/SLL, Waldenstrom, follicular) |
| Full blood count and film | Cytopenias suggest marrow involvement; eosinophilia in Hodgkin; atypical lymphocytes in EBV |
| LDH | Tumour burden marker; elevated LDH is an IPI factor and a tumour lysis risk factor |
| Urea, creatinine, electrolytes, urate, calcium, phosphate | Baseline before chemotherapy; urate and phosphate for tumour lysis assessment |
| Liver function tests and albumin | Hepatic involvement; albumin is an IPS factor in Hodgkin |
| Beta-2 microglobulin | Prognostic in follicular and other NHL |
| ESR and CRP | Non-specific; useful trend marker in Hodgkin |
| HIV serology | All patients — HIV drives lymphoma and changes management |
| Hepatitis B and C serology | Hepatitis B reactivation risk with rituximab — must start antiviral prophylaxis; HCV drives some marginal zone lymphomas |
| EBV serology and PCR | EBV-associated Hodgkin, Burkitt, DLBCL in HIV, NK/T-cell |
| Serum protein electrophoresis, immunoglobulins, free light chains | For suspected Waldenstrom, CLL, myeloma overlap |
| PET-CT | The modern staging standard for FDG-avid lymphomas (Hodgkin, DLBCL, follicular, Burkitt); replaces CT alone for most [6][7] |
| CT neck, chest, abdomen, pelvis with contrast | For non-FDG-avid histologies (some marginal zone, small lymphocytic); always alongside PET for measurement |
| Bone marrow aspirate and trephine | Selective in the PET era — PET-positive marrow involvement in Hodgkin and DLBCL is usually clear on PET; marrow still required for indolent NHL, Waldenstrom, mantle cell, and cytopenic patients |
| Echocardiogram | Baseline cardiac function before anthracycline |
| Fertility referral | Discuss sperm, oocyte, or embryo cryopreservation before chemotherapy |
| Lumbar puncture | For high CNS-risk DLBCL, Burkitt, primary CNS lymphoma, symptoms |
The excisional biopsy — four layers of information
- Histology — architecture (diffuse, follicular, nodular), cell size, mitotic rate, starry-sky pattern. The histological pattern often points to the subtype before any staining.
- Immunohistochemistry — lineage (CD45 confirms lymphoid; CD3 T-cell; CD20, CD79a B-cell), subtype (CD10 and BCL6 germinal centre; CD5 mantle cell; cyclin D1 t(11;14); CD30 Hodgkin and ALCL; CD15 Hodgkin; ALK in ALCL; CD138 plasma cell).
- Flow cytometry on fresh tissue or blood — confirms clonality (kappa or lambda light chain restriction), defines the immunophenotype, and is highly sensitive.
- Cytogenetics and FISH — t(14;18) follicular (BCL2); t(8;14) Burkitt (MYC); t(11;14) mantle cell (cyclin D1); MYC and BCL2 and BCL6 rearrangements in "double-hit" and "triple-hit" high-grade B-cell lymphoma (a poor prognosis group). [1]
DWE trap: Fine-needle aspiration may diagnose carcinoma but is inadequate for lymphoma because it destroys nodal architecture and limits immunophenotyping. If a patient has had an FNA reported as "atypical lymphoid cells," the correct next step is an excisional biopsy — not a repeat FNA, not a CT scan, not an expectant approach. [1]
PET-CT — the modern staging and response tool
FDG PET-CT is now the standard for staging and response assessment in Hodgkin and most aggressive NHL (DLBCL, follicular, Burkitt, mantle cell) [6][7]. PET is more sensitive than CT alone for nodal and extranodal disease, can upstage (and so change management), and can replace bone marrow biopsy in Hodgkin and many DLBCL patients where PET clearly shows marrow involvement. Response is reported using the Deauville 5-point scale, scored against mediastinal blood pool and liver uptake [7]:
| Score | FDG uptake | Interpretation |
|---|---|---|
| 1 | No uptake | Complete metabolic response |
| 2 | Uptake less than or equal to mediastinum | Complete metabolic response |
| 3 | Uptake greater than mediastinum but less than or equal to liver | Complete metabolic response (or "adequate" in de-escalation trials) |
| 4 | Uptake moderately greater than liver | Residual metabolic disease |
| 5 | Uptake markedly greater than liver, or new lesions | Progressive or new disease |
| X | New areas unlikely to be lymphoma | (e.g. infection, inflammation) |
Scores 1 to 3 are considered a complete metabolic response in routine practice. Scores 4 and 5 (or new FDG-avid lesions) indicate residual or progressive disease. The Deauville score drives interim PET-adapted therapy in Hodgkin (escalate if PET-positive after 2 cycles) and end-of-treatment assessment in DLBCL [4].
Staging — Ann Arbor with Cotswold and Lugano modifications
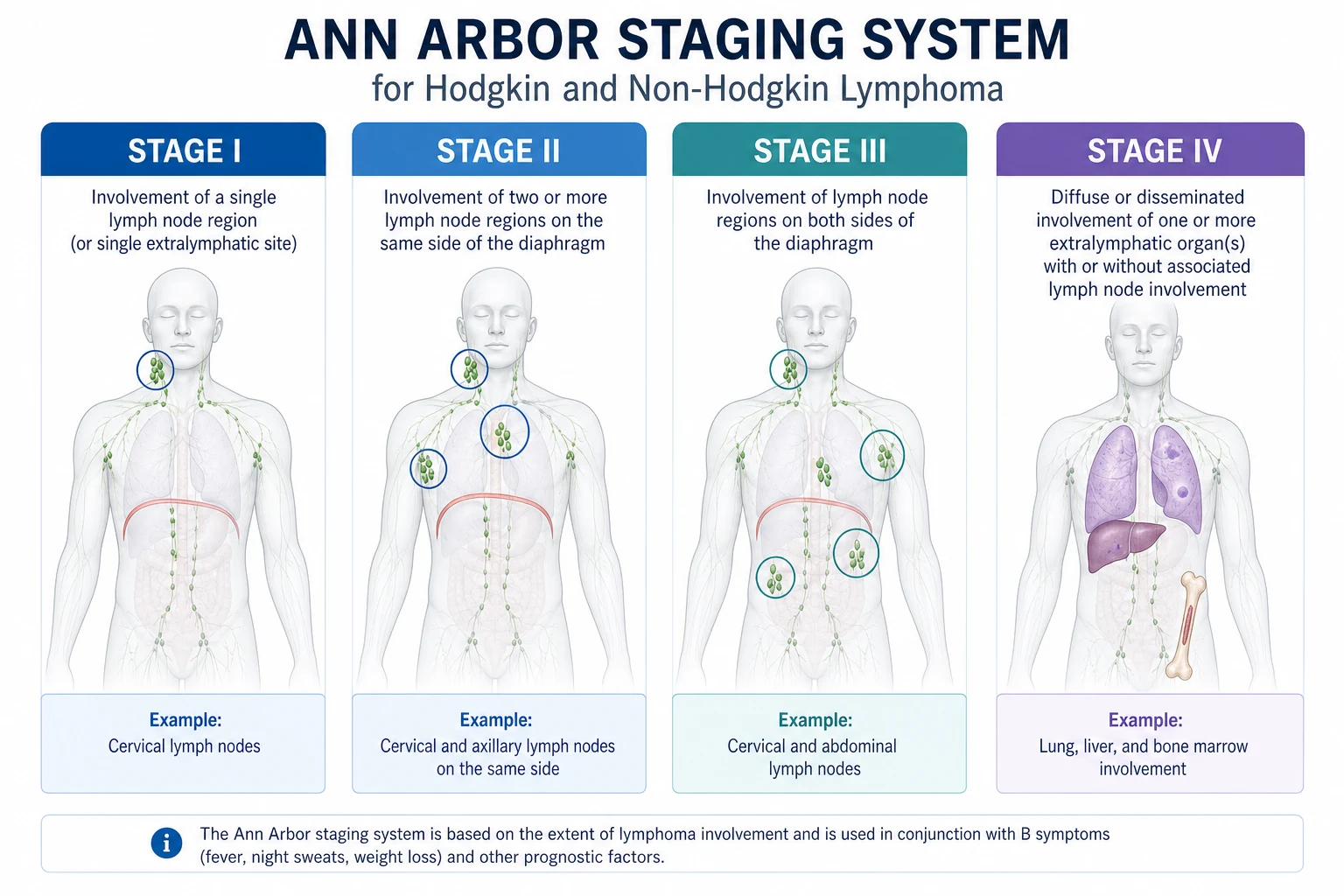
The Ann Arbor staging system, refined at the Cotswold meeting (1989) and again in the Lugano classification (2014), stages lymphoma on the number and location of nodal and extranodal sites [6].
| Stage | Definition |
|---|---|
| I | Single lymph node region (I) or a single extralymphatic organ or site (IE) |
| II | Two or more lymph node regions on the same side of the diaphragm (II), or localised contiguous extralymphatic organ plus nodes on the same side (IIE) |
| III | Node regions on both sides of the diaphragm (III); may include the spleen (IIIS) or a localised extralymphatic organ (IIIE) |
| IV | Diffuse or disseminated involvement of one or more extralymphatic organs (marrow, liver, lung, bone, skin) with or without nodal involvement |
Modifiers: A = no B symptoms; B = B symptoms (unexplained fever above 38, drenching night sweats, weight loss more than 10 per cent in 6 months); E = single contiguous extranodal site; S = splenic involvement; X = bulky disease (a mass over 10 cm or over one-third of the thoracic diameter on CT). [1]
The Lugano classification consolidated staging into limited (stages I and II, non-bulky) and advanced (stages II bulky, III, IV) for treatment decisions. PET-CT is the preferred staging modality for FDG-avid histologies; bone marrow biopsy is no longer required for Hodgkin or DLBCL if PET is clearly negative for marrow involvement [6].
Management of Hodgkin lymphoma
Early-stage favourable Hodgkin (stage I to IIA, non-bulky, no B symptoms)
The standard for favourable early-stage classical Hodgkin is 2 cycles of ABVD followed by 20 Gy involved-site radiotherapy (ISRT) — the GHSG HD10 trial showed this minimal regimen achieved 5-year progression-free survival over 90 per cent with the lowest long-term toxicity [2]. Selected patients (young women, where breast and lung radiation carries a long-term cancer risk) are increasingly treated with chemotherapy alone (typically 4 to 6 cycles of ABVD) if they achieve a complete metabolic response on interim PET, to avoid radiotherapy entirely.
Early-stage unfavourable and bulky Hodgkin (stage I to IIB bulky)
The approach is more chemotherapy (typically 4 cycles of ABVD or escalated BEACOPP) plus ISRT, or PET-adapted chemotherapy alone in complete responders. Bulky mediastinal disease has a higher relapse rate with chemotherapy alone and consolidative radiotherapy is often given. [1]
Advanced classical Hodgkin (stage III to IV, or bulky IIB with B symptoms)
The backbone is 6 cycles of ABVD, now commonly PET-adapted — the RATHL trial showed that patients who are PET-negative after 2 cycles of ABVD can safely de-escalate to AVD (omitting bleomycin, reducing pulmonary toxicity) without loss of efficacy, while PET-positive patients are escalated to BEACOPP [4]. The German Hodgkin Study Group prefers escalated BEACOPP for high-risk advanced disease (it produces a lower relapse rate but more acute toxicity and a small excess of secondary leukaemia). The modern alternative frontline regimen is brentuximab vedotin plus AVD (A+AVD) — the ECHELON-1 trial showed a modified progression-free survival advantage over ABVD in stage III or IV disease, and A+AVD is now an FDA-approved frontline option [3].
| Regimen | Drugs | Indication |
|---|---|---|
| ABVD | Doxorubicin (Adriamycin), Bleomycin, Vinblastine, Dacarbazine | Standard frontline for advanced Hodgkin |
| Escalated BEACOPP | Bleomycin, Etoposide, Doxorubicin, Cyclophosphamide, Vincristine, Procarbazine, Prednisone | High-risk advanced disease (GHSG) |
| A+AVD | Brentuximab vedotin plus Doxorubicin, Vinblastine, Dacarbazine | Frontline stage III to IV (ECHELON-1) |
| ISRT | Involved-site radiotherapy, 20 to 30 Gy | Early-stage consolidation; bulky disease |
Relapsed or refractory Hodgkin
The pathway is salvage chemotherapy (e.g. ICE — ifosfamide, carboplatin, etoposide — or GDP — gemcitabine, dexamethasone, cisplatin), then autologous stem cell transplant for chemosensitive disease (the only curative modality for relapsed Hodgkin). For patients who relapse after autologous transplant or who are transplant-ineligible, the modern options are: [1]
- Brentuximab vedotin — an anti-CD30 antibody-drug conjugate carrying monomethyl auristatin E. Highly active in CD30-positive Hodgkin.
- PD-1 blockade — nivolumab or pembrolizumab — Hodgkin Reed-Sternberg cells frequently amplify 9p24.1, the PD-L1/PD-L2 locus, making the tumour exquisitely sensitive to PD-1 blockade. CheckMate 205 and KEYNOTE-087 showed response rates over 65 per cent in relapsed or refractory disease [5]. Pembrolizumab with gemcitabine, vinorelbine, and liposomal doxorubicin is now used as a bridge to autologous transplant in chemorefractory disease, and the tandem autologous transplant plus pembrolizumab maintenance strategy is being explored.
The International Prognostic Score (IPS) for advanced Hodgkin
The Hasenclever IPS, derived from over 5000 patients in the pre-PET era, assigns one point for each of seven adverse factors [1]:
- Serum albumin below 40 g/L
- Haemoglobin below 105 g/L [1]3. Male sex
- Age 45 years or older
- Ann Arbor stage IV
- White cell count 15 or above
- Lymphocyte count below 0.6, or below 8 per cent of white cells, or both [1]
A score of 0 to 1 predicts the best outcome; a score of 4 or more the worst. In the modern era with PET-adapted therapy the IPS discriminates less, but it remains a framework for prognostication and risk-stratified trial entry. [1]
Management of diffuse large B-cell lymphoma
DLBCL is the commonest aggressive NHL and the prototype for R-CHOP. It can arise de novo or by transformation from an indolent lymphoma (follicular, marginal zone, CLL — Richter transformation). [1]
Frontline: R-CHOP
The standard for fit patients with previously untreated DLBCL is R-CHOP given every 21 days for 6 cycles. The pivotal LNH-98.5 trial in elderly patients (60 to 80 years) showed that adding rituximab to CHOP improved complete response, event-free survival, and overall survival without added toxicity [8]. Subsequent data extended R-CHOP to younger fit adults. For non-bulky stage I DLBCL, 3 to 4 cycles of R-CHOP plus ISRT or 6 cycles of R-CHOP alone is appropriate.
| Drug | Dose | Day |
|---|---|---|
| Rituximab | 375 mg/m2 IV | 1 |
| Doxorubicin (hydroxydaunorubicin) | 50 mg/m2 IV | 1 |
| Vincristine (Oncovin) | 1.4 mg/m2 IV (capped at 2 mg) | 1 |
| Prednisone | 100 mg orally | 1 to 5 |
| Cycles every 21 days | 6 cycles (or 3 to 4 for limited stage) | — |
Pegfilgrastim (granulocyte colony-stimulating factor) on day 2 supports neutrophil recovery and maintains dose intensity. Antiviral prophylaxis (entecavir or tenofovir) is mandatory for hepatitis B surface antigen-positive or core antibody-positive patients because rituximab can precipitate fatal HBV reactivation. PJP prophylaxis (co-trimoxazole) is given during and for several months after therapy. [1]
Prognostication — IPI, R-IPI, and NCCN-IPI
The International Prognostic Index (IPI) assigns one point each for age over 60, elevated LDH, ECOG performance status 2 or more, Ann Arbor stage III or IV, and more than one extranodal site. The R-IPI re-stratified the IPI in the rituximab era (very good, good, poor risk groups) [9]. The NCCN-IPI refined the age and LDH cut-offs and the extranodal site definitions for the modern era and discriminates better at the extremes [10]. A high IPI is not a contraindication to curative R-CHOP but prompts discussion of CNS prophylaxis and consideration of a more intensive regimen in selected patients.
CNS prophylaxis
Central nervous system relapse in DLBCL occurs in about 5 per cent overall but is much higher in high-risk groups, and once it occurs it is usually fatal within months. The CNS-IPI (Schmitz, derived from over 2000 patients) integrates the standard IPI with kidney or adrenal involvement; high-risk patients (CNS-IPI 4 to 6 with kidney or adrenal involvement) have a CNS relapse risk approaching 15 per cent and warrant CNS prophylaxis [11]. Additional high-risk features are testicular DLBCL (mandatory intrathecal prophylaxis and contralateral testicular radiotherapy), paranasal sinus, breast, uterine, and bone marrow involvement, double-hit or double-expressor lymphoma, and the ABC cell-of-origin. Prophylaxis is typically with intrathecal methotrexate and cytarabine and/or systemic high-dose methotrexate.
Relapsed DLBCL — salvage, autologous transplant, and CAR-T
The standard pathway for relapsed or refractory DLBCL (after R-CHOP) is platinum-based salvage (R-ICE, R-DHAP, or R-GDP) followed by autologous stem cell transplant in chemosensitive patients — long-term cure in about 50 per cent of those transplanted. For patients who relapse after autologous transplant, who are refractory to salvage, or who are primary refractory after R-CHOP, the standard is now CAR-T cell therapy — the patient's T cells are genetically engineered to express a chimeric antigen receptor targeting CD19, expanded, and reinfused after lymphodepleting chemotherapy. The ZUMA-1 trial of axicabtagene ciloleucel showed an objective response rate of 82 per cent and a complete response rate of 54 per cent in refractory DLBCL, with durable remissions [17]. CAR-T toxicity — cytokine release syndrome (fever, hypotension, hypoxia, treated with tocilizumab and corticosteroids) and immune effector cell-associated neurotoxicity syndrome (ICANS) — requires specialised management. Tisagenlecleucel and lisocabtagene maraleucel are the other approved CD19 CAR-T products. CAR-T is moving earlier in the treatment paradigm — second-line use in primary refractory or early-relapsing DLBCL is now approved.
Management of follicular lymphoma
Follicular lymphoma is the prototypical indolent NHL — median survival in the modern rituximab era exceeds 15 to 20 years. It is generally incurable, and the goal is symptom control, prevention of end-organ damage, and timely intervention for transformation. [1]
Prognostication — FLIPI and FLIPI-2
The FLIPI (Solal-Celigny), derived from over 4000 patients, assigns one point each for age over 60, Ann Arbor stage III or IV, haemoglobin below 120 g/L, more than four nodal sites, and elevated LDH [12]. Risk groups: low (0 to 1 factor), intermediate (2 factors), high (3 or more). The FLIPI-2 incorporates beta-2 microglobulin and the largest nodal diameter and predicts progression-free survival in the rituximab era. The POD24 concept — progression within 24 months of first therapy — is the strongest adverse prognostic marker and identifies patients with a much poorer survival.
Watch-and-wait versus immediate therapy
For asymptomatic patients with low tumour burden and no end-organ threat, watch-and-wait (active surveillance) is a valid strategy. Randomised trials show no survival disadvantage from deferred therapy, and some patients never require treatment. The criteria for starting therapy (the GELF criteria) include symptomatic disease (B symptoms, organ compression, ascites, pleural effusion), splenomegaly over 6 cm, nodal or extranodal masses over 7 cm, cytopenias, or rapid progression. [1]
First-line therapy
For symptomatic or high-burden follicular lymphoma, the standard is rituximab plus chemotherapy — R-CHOP, R-bendamustine (BR), or R-CVP — followed by rituximab maintenance for 2 years (improves progression-free survival). The GALLIUM trial showed that obinutuzumab (a type II anti-CD20 monoclonal antibody) plus chemotherapy followed by obinutuzumab maintenance improved progression-free survival versus rituximab in previously untreated follicular lymphoma [13]. For limited-stage (stage I) disease, involved-site radiotherapy alone is potentially curative. Rituximab monotherapy is appropriate for elderly or frail patients who cannot tolerate chemotherapy. Radiolabelled antibody therapy (90Y-ibritumomab tiuxetan, 177Lu-lilotomab satetraxetan) is used in some centres.
Relapsed follicular lymphoma and transformation
Options for relapse include re-treatment with rituximab-based therapy, lenalidomide plus rituximab, PI3K inhibitors (copanlisib, idelalisib — now used less because of toxicity), the EZH2 inhibitor tazemetostat (for EZH2-mutant disease), and autologous transplant in selected patients. Transformation to DLBCL — suggested by rapid growth, high LDH, hypermetabolic change on PET, and new B symptoms — is biopsy-proven and treated as de novo DLBCL (R-CHOP or similar), though the prognosis is worse. [1]
Marginal zone lymphoma and the H. pylori story
Marginal zone lymphoma is divided into three subtypes: [1]
- Extranodal marginal zone (MALT — mucosa-associated lymphoid tissue) — the commonest, found in the stomach (driven by chronic H. pylori infection), ocular adnexa (Chlamydia psittaci in some regions), salivary gland (Sjogren), thyroid (Hashimoto), lung, and skin. Gastric MALT at an early stage can be cured by H. pylori eradication (triple therapy — a proton pump inhibitor plus amoxicillin plus clarithromycin for 7 to 14 days) — repeat endoscopy at 3 months to assess regression. More advanced disease is treated with radiotherapy, rituximab-based therapy, or chemotherapy.
- Nodal marginal zone — rarer; treated as for follicular.
- Splenic marginal zone — splenectomy or rituximab; associated with hepatitis C. [1]
Mantle cell lymphoma
Mantle cell lymphoma is defined by the t(11;14) translocation, which places cyclin D1 under the immunoglobulin enhancer, driving overexpression. The cells are CD5-positive, CD20-positive, cyclin D1-positive. It affects older men, often with widespread nodes, gut involvement (lymphomatous polyposis), and marrow disease. Biologically aggressive though clinically heterogeneous; the MIPI (Mantle Cell Lymphoma International Prognostic Index) stratifies risk. Treatment in younger fit patients is intensive — R-hyper-CVAD alternating with high-dose methotrexate and cytarabine, or Nordic regimen — followed by autologous stem cell transplant consolidation in first remission. Older or less fit patients receive BR (bendamustine-rituximab) or R-CHOP. The BTK inhibitors (ibrutinib, zanubrutinib, acalabrutinib), bortezomib, and lenalidomide are active in relapsed disease. Median survival in the modern era has improved to 5 to 10 years depending on risk. [1]
Burkitt lymphoma — an emergency
Burkitt lymphoma is the fastest-growing human tumour, and its management is an oncological emergency. Presentation is with a rapidly enlarging mass — the ileocaecal or abdominal mass in sporadic Burkitt (Western, children and young adults), the jaw or facial bone mass in endemic Burkitt (Equatorial Africa, children), or nodal disease in HIV-associated Burkitt. LDH is typically very high, and tumour lysis syndrome may be present at diagnosis or develop within hours of starting therapy. [1]
Tumour lysis prophylaxis — start before chemotherapy
For any patient with Burkitt or lymphoblastic lymphoma, or any high-burden high-LDH lymphoma, start tumour lysis prophylaxis before chemotherapy: [1]
- Aggressive intravenous hydration — 3 L/m2 per day, goal urine output at least 100 mL/m2 per hour.
- Rasburicase (recombinant urate oxidase) — breaks down existing uric acid. Preferred over allopurinol in high-risk and established tumour lysis because allopurinol only prevents new urate formation. Dose 0.15 to 0.2 mg/kg daily. Contraindicated in G6PD deficiency (causes haemolysis).
- Allopurinol for moderate risk; rasburicase for high risk and established tumour lysis.
- Frequent monitoring — potassium, phosphate, calcium, creatinine, urate every 4 to 6 hours for the first 48 hours; treat hyperkalaemia, hyperphosphataemia, hypocalcaemia (do not correct calcium unless symptomatic — it worsens calcium phosphate deposition). [1]
Treatment
Modern Burkitt treatment is short, intensive, multi-agent chemotherapy with CNS prophylaxis — DA-EPOCH-R (dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, rituximab) at the National Cancer Institute achieved outstanding outcomes with lower toxicity than historical regimens [14], while the CODOX-M/IVAC regimen (Magrath) remains widely used for high-risk disease. All patients receive intrathecal CNS prophylaxis. HIV-associated Burkitt is treated with the same regimens alongside antiretroviral therapy. Five-year survival exceeds 80 to 90 per cent in children and young adults; the prognosis falls with age and comorbidity.
Primary CNS lymphoma
Primary CNS lymphoma is a diffuse large B-cell lymphoma confined to the brain, spinal cord, leptomeninges, or eyes, with no systemic disease. It is uncommon in the immunocompetent (median age 65) but much more frequent in the immunosuppressed (HIV, post-transplant), in whom it is almost always Epstein-Barr virus-associated. Presentation is with a focal neurological deficit, seizures, cognitive or personality change, or ocular symptoms (vitreal deposits). Imaging typically shows a solitary, homogeneously enhancing periventricular mass (often adjacent to the ventricle, suggesting origin from the subependymal B cells). [1]
The biopsy-first rule — avoid steroids
The cardinal management rule in suspected primary CNS lymphoma is to avoid corticosteroids before stereotactic biopsy unless the patient has life-threatening cerebral oedema or impending herniation. Steroids lyse lymphoma cells — a dramatic radiographic response within 24 to 48 hours — but they can render the biopsy non-diagnostic, leaving the patient without a tissue diagnosis. If steroids have been given and the biopsy is non-diagnostic, a period of steroid washout with repeat imaging and biopsy may be required [15].
Treatment
The standard is high-dose methotrexate-based polychemotherapy (typically the MATRix regimen — methotrexate, cytarabine, thiotepa, rituximab — for fit patients up to age 70), followed by consolidation with autologous stem cell transplant or, in older or less fit patients, whole-brain radiotherapy [15]. The IELSG32 trial established MATRix as the most effective induction combination. Whole-brain radiotherapy is effective but carries a significant risk of late neurocognitive decline, particularly in older patients; it is now often deferred or used only in the relapsed setting. Median survival in the modern era is 3 to 5 years, with long-term survival in some fit patients.
Primary mediastinal B-cell lymphoma
PMBCL arises from thymic medullary B cells, affects young women (median age 35), and presents with a bulky anterior mediastinal mass with superior vena cava syndrome, dyspnoea, cough, and sometimes pleural or pericardial effusions. Histologically and molecularly it overlaps with nodular sclerosis classical Hodgkin lymphoma (both share 9p24.1 amplification and PD-L1 overexpression). It is CD20-positive, CD30 variably positive, and may be confused with Hodgkin. Treatment is DA-EPOCH-R for 6 cycles or R-CHOP followed by involved-site radiotherapy — with PET-adapted radiotherapy in those who do not achieve complete metabolic response. Pembrolizumab is active in relapsed disease (PD-L1 overexpression makes it sensitive to checkpoint blockade). Prognosis is excellent — 5-year survival over 90 per cent in modern series. [1]
T-cell lymphomas
Peripheral T-cell lymphomas are heterogeneous and generally carry a worse prognosis than B-cell NHL. Key subtypes: [1]
- Peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS) — the commonest; aggressive; treated with CHOP or similar; 5-year survival 30 to 40 per cent.
- Anaplastic large cell lymphoma (ALCL) — CD30-positive; ALK-positive ALK in young patients has an excellent prognosis (5-year survival over 70 per cent) with CHOP or CHOEP; ALK-negative ALCL is worse. Brentuximab vedotin (anti-CD30) is active. Systemic ALCL must be distinguished from primary cutaneous ALCL (indolent, skin-limited).
- Angioimmunoblastic T-cell lymphoma — presents with generalised nodes, B symptoms, skin rash, autoimmune features; aggressive; often EBV-associated.
- Extranodal NK/T-cell lymphoma, nasal type — Asian and South American predominance; EBV-driven; destructive nasal or midline facial lesions; treated with asparaginase-based regimens and radiotherapy.
- Cutaneous T-cell lymphoma — mycosis fungoides and Sezary syndrome — an indolent epidermotropic T-cell neoplasm. Mycosis fungoides progresses through patches, plaques, and tumours over years to decades. Sezary syndrome is the leukaemic variant — erythroderma, generalised lymphadenopathy, and clonal Sezary cells (cerebriform T cells) on the blood film. Treatment is skin-directed (topical steroids, phototherapy, radiotherapy) and systemic (brentuximab, mogamulizumab, histone deacetylase inhibitors) for advanced disease. [1]
Waldenstrom macroglobulinaemia
Waldenstrom macroglobulinaemia is a lymphoplasmacytic lymphoma producing a monoclonal IgM paraprotein. The MYD88 L265P somatic mutation is present in over 90 per cent of cases and is a diagnostic discriminator from other IgM-producing disorders [16]. Clinical features are driven by the paraprotein: hyperviscosity syndrome (visual disturbance, headache, mucosal bleeding, neurological symptoms — serum viscosity over 4 centipoise, IgM usually over 30 g/L), cryoglobulinaemia, cold agglutinin disease, peripheral neuropathy (anti-MAG), and renal amyloidosis. Diagnosis is on marrow (over 10 per cent lymphoplasmacytic infiltrate), serum IgM paraprotein, and the MYD88 mutation. Treatment is with rituximab-based therapy (BR, DRC — dexamethasone, rituximab, cyclophosphamide), proteasome inhibitors (bortezomib — but avoid in neuropathy), BTK inhibitors (zanubrutinib, ibrutinib — highly active given the MYD88-driven NF-kB signalling), or venetoclax. Plasmapheresis is used for symptomatic hyperviscosity (visual disturbance, bleeding, neurological) — it removes the IgM rapidly while chemotherapy takes effect. Watch-and-wait is reasonable for asymptomatic patients.
Supportive care
Hepatitis B reactivation — the rituximab rule
Every patient about to receive rituximab (or any anti-CD20 therapy) must have hepatitis B surface antigen, core antibody, and (ideally) HBV DNA tested. Reactivation of hepatitis B during or after rituximab can cause fulminant hepatic failure and death. Surface antigen-positive patients need antiviral prophylaxis (entecavir or tenofovir) started before chemotherapy and continued for at least 12 to 18 months after the last rituximab dose. Core-antibody-positive, surface-antigen-negative patients need monitoring with HBV DNA and prophylaxis if HBV DNA becomes positive. [1]
Neutropenic sepsis
Fever in a neutropenic patient (neutrophils below 0.5, or under 1.0 and falling) after chemotherapy for lymphoma is neutropenic sepsis until proven otherwise — cultures then empiric antipseudomonal antibiotic within one hour (piperacillin-tazobactam 4.5 g IV, or meropenem 1 g IV if unstable). G-CSF support and dose modification may be needed for subsequent cycles. Refer to the acute leukaemia page for the full door-to-antibiotic protocol. [1]
Tumour lysis syndrome
Rapid lysis releases potassium, phosphate, and urate, causing hyperkalaemia, hyperphosphataemia, hypocalcaemia, and acute kidney injury. Prevent with aggressive hydration, rasburicase (high-risk), allopurinol (moderate risk), and frequent electrolyte monitoring — especially in Burkitt, lymphoblastic, and high-burden high-LDH lymphomas. Treat established tumour lysis with rasburicase, aggressive hydration, treatment of hyperkalaemia (calcium gluconate for cardiac instability, insulin-dextrose, potassium binders, dialysis for refractory cases). [1]
Infusion reactions and cytokine release syndrome
Rituximab, obinutuzumab, and CAR-T infusions can cause infusion reactions or cytokine release syndrome. Rituximab reactions (fever, rigors, hypotension, bronchospasm) are reduced by premedication (paracetamol, antihistamine, corticosteroid) and starting the infusion slowly. CAR-T cytokine release syndrome (fever, hypotension, hypoxia, multi-organ dysfunction) is managed with tocilizumab (anti-IL-6 receptor) and corticosteroids; ICANS with corticosteroids and supportive care. [1]
Fertility preservation
Every patient of reproductive age should be offered fertility preservation before chemotherapy — sperm cryopreservation for men (rapid, single sample), oocyte or embryo cryopreservation for women (requires a 2 to 3 week ovarian stimulation cycle, which may delay chemotherapy). The fertility specialist and the haematologist should coordinate timing. [1]
Prognosis
Hodgkin lymphoma
Five-year overall survival is over 85 per cent in developed countries — over 95 per cent for early-stage favourable disease and over 80 per cent for advanced disease with modern PET-adapted therapy. The leading cause of death in long-term Hodgkin survivors is not the lymphoma itself but the late effects of treatment — secondary malignancies (breast cancer from radiotherapy, lung cancer, secondary leukaemia and myelodysplasia from chemotherapy), cardiovascular disease (anthracycline cardiomyopathy, radiation-accelerated coronary and carotid disease), pulmonary fibrosis (bleomycin), hypothyroidism (cervical radiotherapy), and infertility. Long-term survivorship care is a discipline in its own right. [1]
DLBCL
Five-year overall survival with R-CHOP is about 60 to 70 per cent overall — better for low-IPI disease (over 80 per cent) and worse for high-IPI disease (under 50 per cent). Primary refractory DLBCL (progressive disease during or within 12 months of R-CHOP) carries a particularly poor prognosis; CAR-T therapy has transformed this group. [1]
Follicular lymphoma
Median overall survival in the rituximab era exceeds 15 to 20 years. Progression within 24 months of first therapy (POD24) identifies a high-risk group with median survival 5 years. Transformation to DLBCL occurs in perhaps 2 to 3 per cent per year. [1]
Burkitt lymphoma
Five-year survival exceeds 80 to 90 per cent in children and young adults with modern therapy; the prognosis falls with age, high LDH, and CNS involvement. [1]
Late effects and survivorship

The lymphoma survivor is a long-case archetype. The high-yield late effects to screen for are: [1]
- Secondary malignancy — breast cancer (after thoracic radiotherapy for Hodgkin in young women — annual MRI from 8 years post-treatment or age 40, whichever first), lung cancer (especially in smokers who received radiotherapy), acute leukaemia and myelodysplasia (after alkylating agents and topoisomerase inhibitors — usually within 5 to 10 years).
- Cardiovascular disease — anthracycline cardiomyopathy (cumulative dose, often after doxorubicin or epirubicin; echocardiographic surveillance), accelerated coronary and carotid atherosclerosis after mantle or mediastinal radiotherapy, valvular disease (radiation).
- Pulmonary fibrosis — bleomycin lung (especially with smoking, age, and high cumulative dose; can present years later with exertional dyspnoea and interstitial changes).
- Endocrine — hypothyroidism (cervical radiotherapy, annual TSH), hypogonadism, premature menopause (alkylating agents).
- Infertility — alkylating agents (cyclophosphamide, procarbazine, mechlorethamine) cause gonadal damage; discuss before treatment.
- Psychological — anxiety, depression, fear of recurrence; a named clinical nurse specialist and access to psychological support are part of standard care.
- Vaccination — pneumococcus, influenza, COVID-19, hepatitis B, Haemophilus influenzae; re-vaccination after splenectomy or anti-CD20 therapy (rituximab impairs vaccine response for 6 to 12 months — re-vaccinate after B-cell recovery). [1]
DCE long-case approach
Opening statement (SASPOP)
"This is Mr J, a 34-year-old software engineer who presents with a three-month history of painless enlarged cervical and supraclavicular lymph nodes, drenching night sweats, and 8 kilograms of unintentional weight loss, found on excisional biopsy to have nodular sclerosis classical Hodgkin lymphoma with bulky mediastinal involvement and Ann Arbor stage IIBX disease. His main problems are the lymphoma itself (bulky stage II disease with B symptoms — managed with PET-adapted ABVD chemotherapy), the acute impact of the diagnosis on his young family and his work, the question of fertility preservation before chemotherapy, his coexisting asthma (which affects bleomycin tolerance), and the long-term survivorship plan (secondary malignancy screening, cardiac and pulmonary surveillance). My priorities are to complete staging with PET-CT and baseline bloods, to address fertility preservation before starting chemotherapy, to engage the haematology multidisciplinary team and the patient in a shared decision on ABVD versus A+AVD, and to institute a structured survivorship plan." [1]
Structured problem list
- Newly diagnosed classical Hodgkin lymphoma, stage IIBX (bulky) — PET-adapted ABVD or A+AVD; ISRT for residual disease.
- B symptoms and bulky mediastinal disease — confirm no airway compromise; assess for superior vena cava syndrome.
- Fertility preservation — refer before chemotherapy for sperm cryopreservation.
- Coexisting asthma — optimise; bleomycin pulmonary toxicity risk.
- Psychosocial impact — diagnosis on the patient, his partner, and their two young children; employer liaison.
- Long-term survivorship plan — secondary malignancy (breast in a young woman, but this patient is male — lung, leukaemia), cardiac (anthracycline), pulmonary (bleomycin), endocrine, psychological surveillance. [1]
Integrated management plan
- Confirm diagnosis and stage — review the excisional biopsy histology and immunohistochemistry (CD30, CD15, CD20 status); complete PET-CT staging; baseline bloods including LDH, albumin, full blood count, HIV and hepatitis B and C serology; baseline echocardiogram and pulmonary function tests.
- Fertility preservation — urgent referral for sperm cryopreservation before chemotherapy; document the discussion and the patient's decision.
- Frontline therapy — PET-adapted ABVD (6 cycles) is the standard; A+AVD is an alternative based on ECHELON-1 [3][4]. Interim PET after 2 cycles (Deauville 1 to 3 — continue; Deauville 4 to 5 — escalate to BEACOPP or switch). Consolidative ISRT for bulky residual disease or PET-positive end-of-treatment.
- Supportive care — antiemetics, pegfilgrastim, PJP prophylaxis (co-trimoxazole), antiviral prophylaxis if hepatitis B core antibody positive; tumour lysis prophylaxis for high-burden disease.
- Survivorship — structured late-effects plan: annual TSH, echocardiographic surveillance at 2 and 5 years, pulmonary function if symptomatic, dermatology and breast or lung cancer screening as appropriate, psychological support, return-to-work plan, vaccination review.
DCE short-case approach: examination of the lymph node regions
Instruction: "Examine this patient's cervical, axillary, and inguinal lymph nodes, and the abdomen for organomegaly." [1]
Systematic routine
- End of bed — observe for cachexia, pallor, jaundice, clubbing, and any visible masses. Note any Hickman line or port, the side-effects of chemotherapy (alopecia, mucositis), or radiation tattoos.
- Cervical nodes — examine from behind, in sequence: submental, submandibular, pre-auricular, post-auricular, occipital, tonsillar, upper cervical, middle cervical, lower cervical, posterior triangle, supraclavicular (Virchow). Use the pads of the index and middle fingers, with a rolling motion in both axes. Document the size, shape, consistency (soft, rubbery, hard), mobility, and tenderness of each node.
- Axillary nodes — examine with the patient's arm supported. Central, apical, lateral, pectoral, subscapular. Support the patient's right arm with your left hand and examine the right axilla with your right hand, and vice versa.
- Epitrochlear nodes — support the elbow at 90 degrees, examine the medial aspect above the medial epicondyle (suggests lymphoma or secondary syphilis).
- Inguinal nodes — horizontal and vertical groups; the horizontal group drains the lower abdominal wall, external genitalia, and anal canal; the vertical group drains the lower limb.
- Abdomen — inspect, palpate for hepatosplenomegaly (use the radial border of the right index finger, breath in, move towards the costal margin incrementally; turn slightly to the patient's right to feel the spleen). Percuss Traube's space (dullness suggests splenomegaly).
- Oropharynx — look for Waldeyer's ring involvement (tonsillar enlargement) and mucosal involvement; examine the skin for cutaneous deposits or plaques (mycosis fungoides).
- Testes — examine for testicular masses (testicular lymphoma, a sanctuary site).
- Complete the examination — examine the chest (mediastinal masses, pleural effusion), briefly the neurological system (paraneoplastic or CNS involvement), and offer to perform a fundoscopic examination and to check the blood pressure. [1]
Presentation template
"I examined Mr J, a 34-year-old man who looks comfortable at rest. He has a 2 cm rubbery, mobile, non-tender right supraclavicular node and a 1.5 cm left cervical chain node; the epitrochlear, axillary, and inguinal nodes are not palpable. The abdomen reveals a spleen palpable 3 cm below the costal margin; the liver is not enlarged. The chest is clear. There is no pallor, jaundice, or clubbing. These findings are consistent with lymphadenopathy with splenomegaly — in a young man with cervical and supraclavicular nodes and B symptoms, the differential includes Hodgkin lymphoma, non-Hodgkin lymphoma, and tuberculous lymphadenitis. I would specifically arrange an excisional lymph node biopsy for histology, immunohistochemistry, and mycobacterial culture." [1]
Key DWE MCQ patterns
- Painless cervical lymphadenopathy in a young adult with night sweats — excisional biopsy, not FNA.
- DLBCL with kidney and adrenal involvement — assess for CNS prophylaxis (CNS-IPI).
- Suspected Burkitt with high LDH — start tumour lysis prophylaxis with rasburicase before chemotherapy.
- Suspected primary CNS lymphoma — avoid steroids before stereotactic biopsy.
- DLBCL refractory after R-CHOP — CAR-T cell therapy (axicabtagene ciloleucel) after platinum salvage.
- Follicular lymphoma, asymptomatic, low burden — watch-and-wait; no survival disadvantage from deferred therapy.
- Hepatitis B core antibody positive patient about to receive rituximab — antiviral prophylaxis (entecavir or tenofovir) to prevent reactivation.
- Interim PET after 2 cycles of ABVD for advanced Hodgkin, Deauville 1 to 2 — continue ABVD (or de-escalate to AVD).
- Waldenstrom with hyperviscosity and visual disturbance — urgent plasmapheresis.
- Gastric MALT, early stage, H. pylori positive — H. pylori eradication therapy; repeat endoscopy at 3 months. [1]
Common exam traps
- "Could this be primary CNS lymphoma?" — avoid steroids before biopsy. The reflex to give dexamethasone for a brain mass must be resisted.
- Excisional biopsy, not FNA — for suspected lymphoma, the diagnosis needs architecture. A candidate who orders an FNA will fail the question.
- Hepatitis B before rituximab — reactivation is fatal. Surface antigen, core antibody, and HBV DNA must be checked; prophylaxis is mandatory if positive.
- CNS prophylaxis in DLBCL — the CNS-IPI is underused. A candidate who omits CNS risk assessment in a high-IPI DLBCL with kidney or testicular involvement has missed an exam point.
- Tumour lysis before chemotherapy — Burkitt and lymphoblastic lymphoma need prophylaxis before treatment, not after the first cycle.
- Hodgkin in a young woman — radiotherapy fields and chemotherapeutic choice affect breast cancer and fertility risk; involve the fertility team before chemotherapy.
- Watch-and-wait in follicular lymphoma — counterintuitive but correct for asymptomatic low-burden disease; some candidates wrongly feel they must always treat.
- Deauville 3 is a complete metabolic response in routine practice (it is "inadequate" only in some de-escalation trials).
- Reed-Sternberg cells are CD30-positive and CD15-positive, CD20 usually negative — this immunophenotype distinguishes Hodgkin from NHL.
- Burkitt t(8;14), follicular t(14;18), mantle cell t(11;14) — the three translocations are a frequent written question. [1]
Communication and shared decision-making
"I would sit with the patient and their family in a quiet room with the haematologist and a clinical nurse specialist. I would explain in plain language what lymphoma is — a cancer of the lymphoid cells — and what the immediate plan is. I would acknowledge the shock explicitly and give them space. I would set out the options honestly — for Hodgkin, the high probability of cure with PET-adapted ABVD or A+AVD, balanced against the late effects of treatment; for DLBCL, the goal of cure with R-CHOP and the role of CAR-T if it relapses; for follicular, the often-counterintuitive choice of watch-and-wait for asymptomatic disease. I would address fertility before any chemotherapy — for a young man this is a single semen sample; for a young woman it requires coordination with a fertility specialist and may delay chemotherapy by a few weeks. I would document the shared decision, give written information and a named contact, and arrange follow-up within days. I would address finances, work, family, and the psychological burden — a lymphoma diagnosis reshapes every domain of life, and the registrar who acknowledges that is the one the patient trusts." [1]
References
[1] Hasenclever D, Diehl V. A prognostic score for advanced Hodgkin's disease (IPS). N Engl J Med 1998.
[2] Engert A, Plutschow A, Eich HT, et al. Reduced treatment intensity in early-stage Hodgkin's lymphoma (GHSG HD10). N Engl J Med 2010.
[3] Connors JM, Jurczak W, Straus DJ, et al. Brentuximab vedotin with chemotherapy for stage III or IV Hodgkin's lymphoma (ECHELON-1). N Engl J Med 2018.
[4] Johnson P, Federico M, Kirkwood A, et al. Adapted treatment guided by interim PET-CT scan in advanced Hodgkin's lymphoma (RATHL). N Engl J Med 2016.
[5] Ansell SM, Lesokhin AM, Borrello I, et al. PD-1 blockade with nivolumab in relapsed or refractory Hodgkin's lymphoma (CheckMate 205). J Clin Oncol 2018.
[6] Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol 2014.
[7] Barrington SF, Mikhaeel NG, Kostakoglu L, et al. Role of imaging in the staging and response assessment of lymphoma: consensus of the ICML Imaging Working Group. J Clin Oncol 2014.
[8] Coiffier B, Lepage E, Briere J, et al. CHOP plus rituximab versus CHOP alone in elderly DLBCL (LNH-98.5). N Engl J Med 2002.
[9] Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) for DLBCL treated with R-CHOP. Blood 2007.
[10] Zhou Z, Sehn LH, Radford JW, et al. An enhanced International Prognostic Index (NCCN-IPI) for DLBCL in the rituximab era. Blood 2014.
[11] Schmitz N, Zeynalova S, Nickelsen M, et al. CNS International Prognostic Index for CNS relapse in DLBCL treated with R-CHOP. J Clin Oncol 2016.
[12] Solal-Celigny P, Roy P, Colombat P, et al. Follicular lymphoma international prognostic index (FLIPI). Blood 2004.
[13] Marcus R, Davies A, Ando K, et al. Obinutuzumab for first-line treatment of follicular lymphoma (GALLIUM). N Engl J Med 2017.
[14] Dunleavy K, Pittaluga S, Shovlin M, et al. Low-intensity therapy in adults with Burkitt's lymphoma (DA-EPOCH-R). N Engl J Med 2013.
[15] Ferreri AJM, Cwynarski K, Pulczynski EJ, et al. MATRix regimen for primary CNS lymphoma (IELSG32). Lancet Haematol 2016.
[16] Treon SP, Xu L, Yang G, et al. MYD88 L265P somatic mutation in Waldenstrom's macroglobulinaemia. N Engl J Med 2012.
[17] Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene ciloleucel CAR T-cell therapy in refractory large B-cell lymphoma (ZUMA-1). N Engl J Med 2017.
Lugano Classification; NCCN B-cell Lymphoma Guidelines; HSANZ/eviQ Lymphoma Protocols; British Society for Haematology Lymphoma Guidelines. [1]
References
- [1]Hasenclever D, Diehl V A prognostic score for advanced Hodgkin's disease. International Prognostic Factors Project on Advanced Hodgkin's Disease N Engl J Med, 1998.PMID 9819449
- [2]Engert A, Plutschow A, Eich HT, et al. Reduced treatment intensity in patients with early-stage Hodgkin's lymphoma N Engl J Med, 2010.PMID 20818855
- [3]Connors JM, Jurczak W, Straus DJ, et al. Brentuximab Vedotin with Chemotherapy for Stage III or IV Hodgkin's Lymphoma N Engl J Med, 2018.PMID 29224502
- [4]Johnson P, Federico M, Kirkwood A, et al. Adapted Treatment Guided by Interim PET-CT Scan in Advanced Hodgkin's Lymphoma N Engl J Med, 2016.PMID 27332902
- [5]Ansell SM, Lesokhin AM, Borrello I, et al. Nivolumab for Relapsed/Refractory Classic Hodgkin Lymphoma After Failure of Autologous Hematopoietic Cell Transplantation: Extended Follow-Up of the Multicohort Single-Arm Phase II CheckMate 205 Trial J Clin Oncol, 2018.PMID 29584546
- [6]Cheson BD, Fisher RI, Barrington SF, et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification J Clin Oncol, 2014.PMID 25113753
- [7]Barrington SF, Mikhaeel NG, Kostakoglu L, et al. Role of imaging in the staging and response assessment of lymphoma: consensus of the International Conference on Malignant Lymphomas Imaging Working Group J Clin Oncol, 2014.PMID 25113771
- [8]Coiffier B, Lepage E, Briere J, et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma N Engl J Med, 2002.PMID 11807147
- [9]Sehn LH, Berry B, Chhanabhai M, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP Blood, 2007.PMID 17105812
- [10]Zhou Z, Sehn LH, Radford JW, et al. An enhanced International Prognostic Index (NCCN-IPI) for patients with diffuse large B-cell lymphoma treated in the rituximab era Blood, 2014.PMID 24264230
- [11]Schmitz N, Zeynalova S, Nickelsen M, et al. CNS International Prognostic Index: A Risk Model for CNS Relapse in Patients With Diffuse Large B-Cell Lymphoma Treated With R-CHOP J Clin Oncol, 2016.PMID 27382100
- [12]Solal-Celigny P, Roy P, Colombat P, et al. Follicular lymphoma international prognostic index Blood, 2004.PMID 15126323
- [13]Marcus R, Davies A, Ando K, et al. Obinutuzumab for the First-Line Treatment of Follicular Lymphoma N Engl J Med, 2017.PMID 28976863
- [14]Dunleavy K, Pittaluga S, Shovlin M, et al. Low-intensity therapy in adults with Burkitt's lymphoma N Engl J Med, 2013.PMID 24224624
- [15]Ferreri AJM, Cwynarski K, Pulczynski EJ, et al. Chemoimmunotherapy with methotrexate, cytarabine, thiotepa, and rituximab (MATRix regimen) in patients with primary CNS lymphoma: results of the first randomisation of the International Extranodal Lymphoma Study Group-32 (IELSG32) phase 2 trial Lancet Haematol, 2016.PMID 27132696
- [16]Treon SP, Xu L, Yang G, et al. MYD88 L265P somatic mutation in Waldenström's macroglobulinemia N Engl J Med, 2012.PMID 22931316
- [17]Neelapu SS, Locke FL, Bartlett NL, et al. Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma N Engl J Med, 2017.PMID 29226797